
Abstract
Background:
This study was designed to compare the findings of noninvasive arterial testing in patients with and without diabetic foot pathology.
Methods:
The ABI (ankle brachial index), TBI (toe brachial index), and great toe pressures were measured in 207 patients. PAD (peripheral artery disease) was defined as an ABI < 0.91 on either extremity or a TBI < 0.7.
Results:
PAD was identified in 103 of the 207 patients (49.8%), 80 patients with diabetic foot pathology and 23 patients with nondiabetic foot pathology. Although patients with diabetic foot pathology were 1.4 times more likely to have PAD compared to patients without diabetic pathology, this increased risk was not statistically significant (OR 1.41 [95% CI 0.75-2.64], P = .28). Patients with PAD and diabetic foot pathology were 4.9 times more likely to have ischemia (toe pressure < 60 mm Hg) than patients with PAD and nondiabetic foot pathology (OR 4.93 [95% CI 1.35-17.94], P < .05). Patients on dialysis had a 7.3 times increased likelihood of having PAD compared to patients not on dialysis (OR 7.3 [95% CI 1.6-33.6], P < .01). Patients with absent pedal pulses were 4.9 more likely to have PAD than patients with normal pulses (OR 4.9 [95% CI 2.6-9.4], P < .0001). PAD was identified in 97 of 188 patients (51.6%) with peripheral neuropathy compared to 6 of 19 patients (31.5%) without peripheral neuropathy (OR 2.31 [95% CI 0.84-6.33], P = .10).
Conclusions:
Combining the ABI with TBI improved the ability to diagnose PAD in diabetic patients because the ABI has high specificity (low false positives) and the TBI has high sensitivity (low false negatives). The TBI was more reliable in patients with noncompressible arteries, medial artery calcinosis and/or neuropathy. Due to the relative incompressibility of calcified distal arteries in patients with DM, the ABI may be within normal limits in patients with PAD. This false negative result may lead surgeons to assume that normal perfusion is present.
Level of Evidence:
Level III, comparative study.
The prevalence of peripheral artery disease (PAD) in patients aged ≥ 40 years with diabetes mellitus (DM) is estimated to be 10% compared to 5% in the general population, and the prevalence increases with advancing age. 16 One study reported that 16% of diabetic patients had PAD at the time of diagnosis, and an additional 24% developed PAD during a period of surveillance that averaged 11 years. 24 In high risk groups such as patients with diabetic foot ulcers (DFU), the prevalence of PAD approaches 50%. 33
The measurement of the ankle brachial index (ABI) is a commonly used, simple method to diagnose PAD and estimate the cardiovascular risk profile in patients with DM.16,32 The ABI has been validated against angiographically confirmed disease. 1 In 2003, a consensus statement authored by the American Diabetes Association recommended that a screening ABI be obtained in diabetic patients over the age of 50 years, and in patients < 50 years of age with risk factors such as hypertension, hyperlipidemia, tobacco use, and diabetes duration of more than 10 years. 1 Subsequently, a task force from the American College of Cardiology Foundation and the American Heart Association was created in collaboration with the Societies of Cardiovascular Angiography and Interventions, Interventional Radiology, Vascular Medicine and Vascular Surgery to develop an update on the guidelines for the management of PAD. This update, published in 2011, also recommended using the ABI to screen for PAD in high risk groups such as diabetic patients over the age of 50. 34 In addition, the Trans-Atlantic Inter-Society Consensus (TASC II) working group, representing societies from Africa, Asia, Australia, North America, and South America also recommended similar screening programs. 30
Most authors consider the normal range of ABI to be from 0.91 to 1.30, with values above 1.3 representing poorly compressible vessels. 32 Other authors state that values as high as 1.4 may be the upper limit of normal. 3 It has been demonstrated that DM is the dominant risk factor for an ABI > 1.4 and that occlusive disease is highly prevalent in diabetic patients with noncompressible vessels. 3 Approximately 85% of patients with an ABI > 1.4 have findings of occlusive PAD, prompting some authors to recommend that these findings should be considered PAD equivalents. 3
An ABI ≤ 0.90 remains the most common and consensual threshold for diagnosing PAD. A population based 7-year follow up study of patients with Type 1 and 2 DM demonstrated an 8-fold (700%) increased risk of lower extremity amputation in patients with an ABI ≤ 0.90. 2 In some patients, ankle systolic pressure can’t be measured due to medial artery calcinosis, a condition that commonly occurs in patients with DM, end-stage renal disease and/or peripheral neuropathy.32,34 Medial artery calcinosis results in arterial wall stiffness, potentially leading to a false elevation of the systolic pressure at the level of the ankle. 20 In the setting of noncompressible ankle arteries or patients with an abnormally high ABI, measurement of the toe brachial index (TBI) is recommended to fully assess for PAD.2,34 Toe vessels are less susceptible to medial artery calcinosis and TBI < 0.7 is considered abnormal and indicative of PAD.19,38 In the presence of medial artery calcinosis and/or neuropathy, toe pressure measurement is considered more sensitive than ABI in diagnosing PAD.8,43
Foot and ankle surgeons often treat patients with DM, including nondiabetic foot problems such as tendinopathy, ligament injuries, and trauma to the foot and ankle. In addition, foot and ankle surgeons often encounter patients with complications of DM such as DFU, Charcot neuroarthropathy (CN), and diabetic foot infections. The aim of this study was to evaluate the results of noninvasive arterial testing and to determine the prevalence of PAD in diabetic patients with diabetic foot pathology versus diabetic patients with common nondiabetic foot pathologies.
Methods
After approval by our Institutional Review Board, the database of an academic foot and ankle practice was utilized to identify patients with DM. Electronic medical records were then reviewed to identify those patients with DM who underwent noninvasive arterial testing for PAD during the timeframe of January 1, 2011, through December 1, 2014. Patients were excluded from this study if they had incomplete studies that did not include bilateral measurements of the ABI, TBI and absolute great toe pressures. Patients with a great toe amputation that precluded measurement of the toe pressure were also excluded. All patients had a vascular examination which included palpation of the dorsalis pedis and posterior tibial pulses, and these pulses were characterized as palpable or nonpalpable. Peripheral neuropathy was assessed using the Michigan Neuropathy Screening Index which includes an assessment of monofilament examination, vibratory sensation testing, Achilles reflexes, presence of deformity and the presence of ulceration. 40 Demographic data were recorded.
An ABI of 0.91 to 1.40 was considered normal and values > 1.4 were defined as noncompressible.3,9,25,30 The highest systolic pressure of the dorsalis pedis or posterior tibial pulse was used to calculate the ABI. A normal TBI was defined as ≥ 0.70.3,17-19,25,30,42 The diagnosis of PAD was based on an ABI ≤ 0.9 on either side or a TBI < 0.70.11,18,24,30 Utilizing these 2 values as a threshold for diagnosing PAD, Hoyer et al 18 reported a positive predictive value of 91.0% and negative predictive value of 92.6%. Doppler waveforms that were triphasic or biphasic were considered normal and monophasic waveforms were considered abnormal. Patients were divided into 2 groups based on their foot and ankle pathology (diabetic vs nondiabetic). Based on the results of noninvasive arterial testing, the prevalence of PAD in patients with foot pathology related to complications of DM (DFU, CN, diabetic foot infection or neuropathic fractures) was compared to the prevalence of PAD in patients with common foot pathology (flatfeet, plantar fasciitis, tendonitis, and ligament sprains) unrelated to complications of DM. The severity of PAD was defined according to toe pressure measurement as described by Mills et al 28 and includes 4 grades of ischemia. This consensus statement by the Society of Vascular Surgery described no ischemia (grade 0) with toe pressures ≥ 60 mm Hg, mild ischemia (grade 1) with toe pressures of 40-59mm Hg, moderate ischemia (grade 2) with toe pressures of 30-40 mm Hg, and severe ischemia (grade 3) with toe pressures < 30 mm Hg.
Statistical Analysis
After assessing normality using the Shapiro–Wilk test, descriptive statistical analyses were conducted to determine frequencies (%) of categorical variables, mean and standard deviation of normally distributed continuous variables, and median and interquartile range of nonnormally distributed continuous variables. Frequency distributions of categorical variables between individuals with and without PAD, and individuals with and without diabetic foot pathology were compared using Pearson’s chi-square tests or Fisher’s exact tests, when appropriate. Two-sample t tests were used to determine differences between groups for normal continuous data, and Wilcoxon–Mann–Whitney tests were used to determine differences between groups for nonnormal continuous data. All tests were conducted with a significance level of .05. Associations between independent variables and dichotomous outcome variables were assessed using univariate logistic regression. Odds ratios (OR) with corresponding 95% confidence intervals (CI) were used to illustrate the magnitude of these associations. All analyses were conducted using SAS version 9.4 statistical analysis software (SAS Institute Inc, Cary, NC).
Results
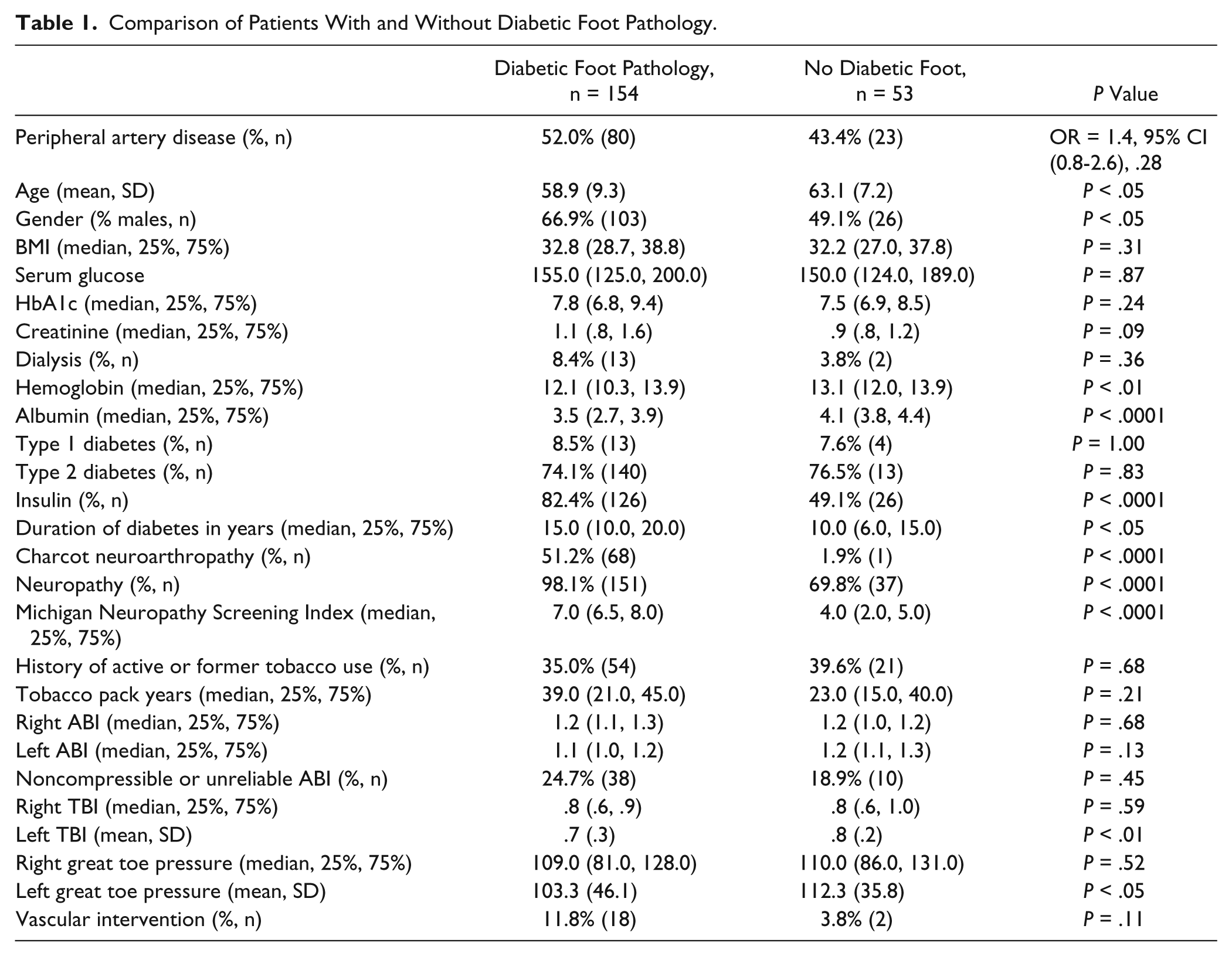
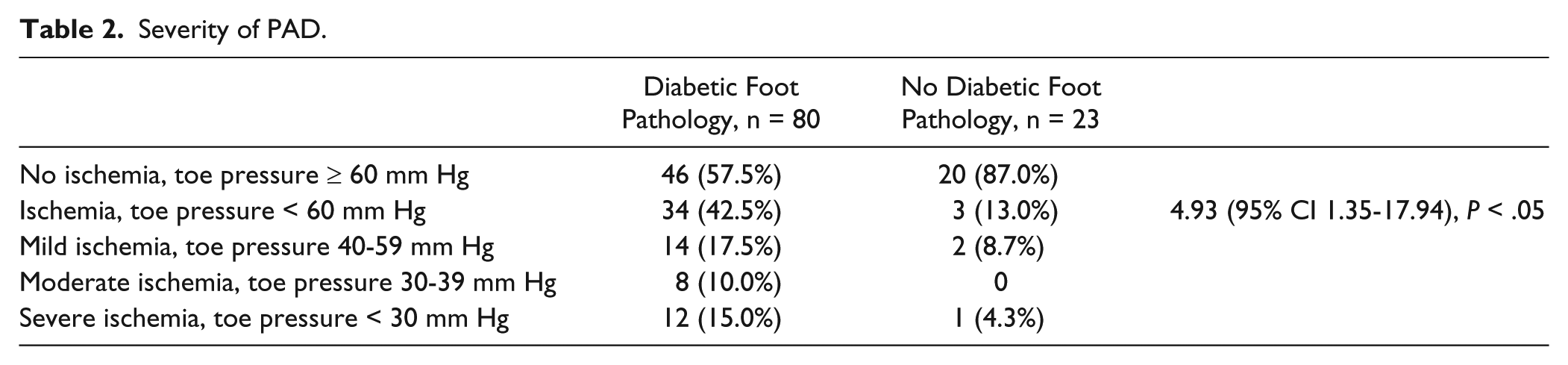
Two hundred seven diabetic patients were included in our study. PAD was identified in 103 of the 207 patients (49.8%). Of the 103 patients diagnosed with PAD, 80 patients had diabetic foot pathology and 23 patients had nondiabetic foot pathology. A comparison of demographic data, laboratory data, diabetes status, comorbidities and results between patients with and without diabetic foot pathology is illustrated in Table 1. Although patients with diabetic foot pathology were 1.4 times more likely to have PAD compared to patients without diabetic pathology, this increased risk was not statistically significant (OR 1.41 (95% CI 0.75-2.64), P = .28). No significant differences were present between the 2 groups with regard to measurement of the right and left ABIs, right TBI, and measurement of the right great toe pressures, although patients with diabetic foot pathology had a significantly lower left TBI (P < .01) and left great toe pressure (P < .05) than patients without diabetic foot pathology (Table 1). Thirty-four of the 80 patients (43%) with PAD and diabetic foot pathology had ischemia as defined by Mills et al 28 (mild ischemia in 14 patients, moderate ischemia in 8 patients and severe ischemia in 12 patients) and 46 did not have ischemia. Three of the 23 patients (13%) with PAD and nondiabetic foot pathology had ischemia (mild ischemia in 2 patients, none with moderate ischemia and 1 with severe ischemia) and 20 patients did not have ischemia. Patients with PAD and diabetic foot pathology were 4.9 times more likely to have ischemia than patients with PAD and nondiabetic foot pathology (OR 4.93 [95% CI 1.35-17.94], P < .05) (Table 2).
Comparison of Patients With and Without Diabetic Foot Pathology.
Severity of PAD.
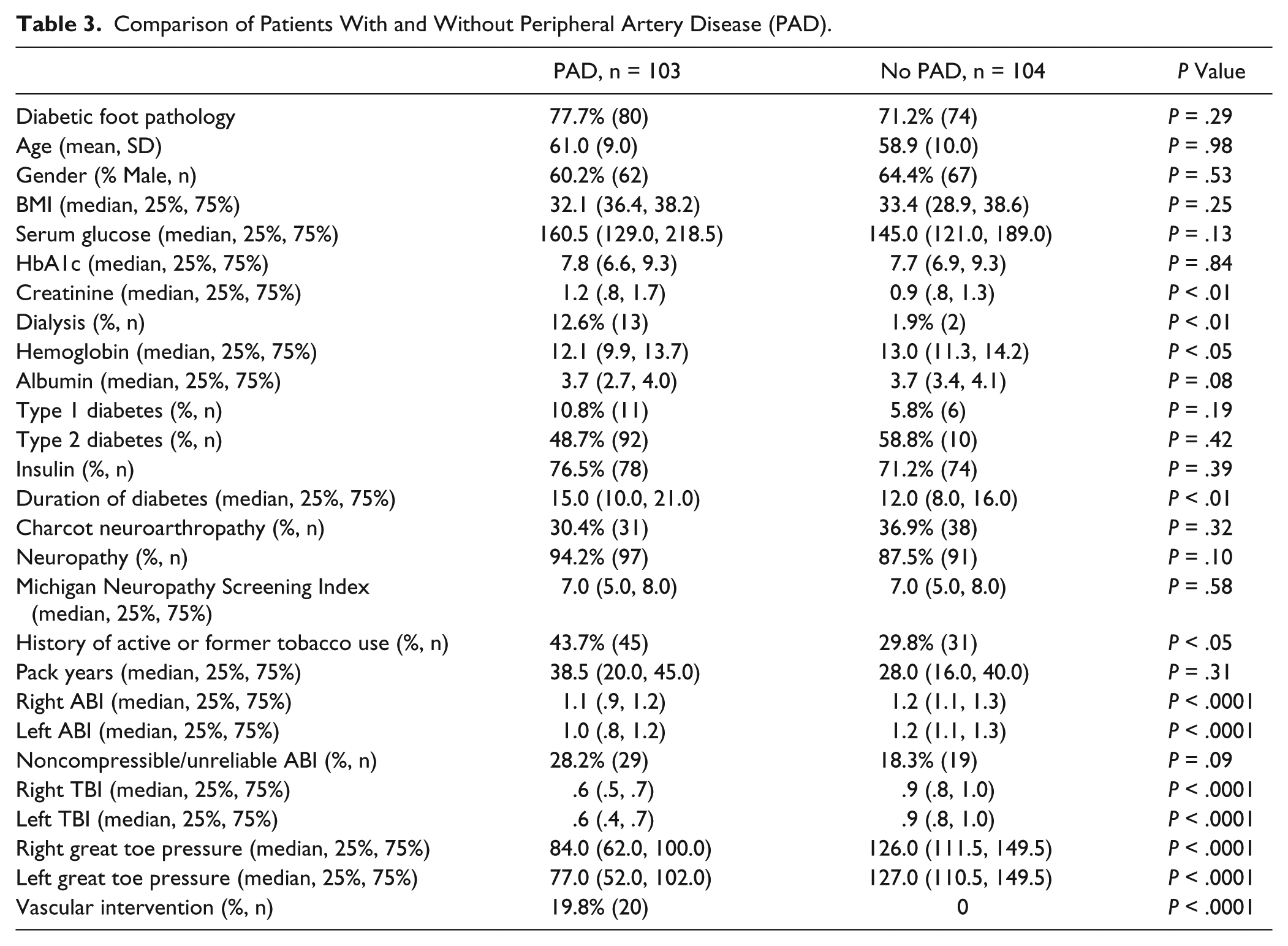
Patients with PAD had lower values on measurement of ABI, TBI, and absolute great toe pressures than patients without PAD. Table 3 illustrates the differences when comparing diabetic patients with and without PAD. Forty-eight of 207 (23%) diabetic patients had noncompressible vessels or unreliable ABIs. Although patients with PAD were 1.8 times more likely to have a noncompressible ankle pressure/unreliable ABI than patients without PAD, this difference did not reach statistical significance (OR 1.75 [95% CI 0.91-3.38], P = .09). Forty-five of 48 patients (94%) with noncompressible vessels/unreliable ABI had peripheral neuropathy compared to 143 of 159 patients (90%) without noncompressible vessels/unreliable ABI (OR 1.67 [95% CI 0.47-6.02], P = .42). Twenty of the 103 patients (19.4%) with PAD underwent vascular intervention with either endovascular or open surgery. Eighteen of 80 (22.0%) of patients with PAD and diabetic foot pathology underwent vascular intervention compared to 2 of 23 (8.7%) patients with PAD and nondiabetic foot pathology (OR 3.05 [95% CI 0.65-14.25], P = .16). Forty-four of 103 (42.7%) of patients diagnosed with PAD had normal bilateral ABIs (0.91-1.40) and the diagnosis of PAD was made on a TBI < 0.70. PAD was identified in 97 of 188 patients (51.6%) with peripheral neuropathy compared to 6 of 19 patients (31.5%) without peripheral neuropathy (OR 2.31 [95% CI 0.84-6.33], P = .10).
Comparison of Patients With and Without Peripheral Artery Disease (PAD).
Diabetic patients with end-stage renal disease on dialysis (13 of 103 patients, 14.4%) had a 7.3 times increased likelihood of having PAD compared to diabetic patients not on dialysis (2 of 104 patients, 1.9%) (OR 7.3 [95% CI 1.6-33.6], P < .01). Patients with absent pedal pulses were 4.9 times more likely to have PAD than patients with normal pulses (OR 4.9 [95% CI 2.6-9.4], P < .0001). In all, 57% (59 of 103 patients) with PAD had biphasic or triphasic wave forms and 43% (44 of 103 patients) had monophasic wave forms. All patients without PAD had biphasic or triphasic wave forms. An OR and P value could not be calculated because none of the patients without PAD had monophasic wave forms.
Discussion
Foot and ankle surgeons are likely to encounter patients with DM during the scope of their practice, largely due to the increasing prevalence of DM. Even surgeons who are not interested in diabetic foot pathology will be exposed to diabetic patients with fractures, tendon disorders, ligament sprains and overuse syndromes. Consequently, surgeons need to be aware of the methods for diagnosing PAD in patients with DM prior to embarking on reconstructive surgery. Some risk factors for postoperative complications in diabetic patients, such as neuropathy, are generally not modifiable. Other risk factors such as active tobacco use, poor glycemic control, and PAD are potentially modifiable, and these variables should be optimized in diabetic patients prior to undergoing elective foot and ankle surgery. The ABI is a widely used screening test to detect significant PAD in patients with DM although the reliability of detecting PAD is decreased in patients with end-stage renal disease, medial artery calcinosis and peripheral neuropathy. The sensitivity of the ABI is reported to be only 53% in diabetic patients with neuropathy, although the specificity is 95%. 43 In other words, an ABI < 0.91 is diagnostic of PAD while a normal or high ABI does not exclude the diagnosis of PAD. Increased arterial wall stiffness secondary to medial artery calcinosis has been observed in diabetic patients with normal ABIs.22,35 Patients with impaired glucose tolerance (ie, “prediabetes”) have also been demonstrated to manifest increased arterial wall stiffness. 35 Insulin resistance and the metabolic syndrome have also been shown to be associated with increased arterial wall stiffness. 39 There appears to be universal agreement on the lower limit of a normal ABI (0.91), however, the lower limit of a normal value for TBI is less well defined with values ranging from 0.61 to 0.76.4,21,31,41
Patients with diabetes and PAD may not manifest symptoms of claudication due to peripheral neuropathy and decreased activity. Examination of the peripheral pulses may be unreliable in patients with PAD, especially in patients with DM.4,43 Studies of healthy volunteers have demonstrated that 8.1% of dorsalis pedis pulses and 2.9% of posterior tibial pulses were not palpable. 21 The posterior tibial pulse is the most difficult to palpate, most likely due to its deep retromalleolar location, and this can be particularly difficult in diabetic patients with soft tissue swelling associated with peripheral edema, acute soft and osseous trauma, diabetic foot infections and/or CN. 7 Even among vascular surgeons, there is only moderate interobserver agreement when assessing the dorsalis pedis (mean Kappa value 48) and posterior tibial (mean Kappa value 53) pulses. 27 The palpability of pulses in patients with DM is lower at most ABI levels when compared to patients without DM. 27 This is likely in large part due to the presence of medial artery calcinosis which decreases vessel wall motion with the cardiac cycle. A recent study of patients with lumbar spinal stenosis demonstrated that 14% of patients with a normal posterior tibial pulse and 11% of patients with a normal dorsalis pedis pulse had abnormal noninvasive arterial assessment. 21 Approximately 30% of patients with diminished, but present pedal pulses had abnormal ABI and/or TBI measurements. Conversely, approximately one-third of patients without PAD had an abnormal tactile pedal pulse examination. 21 Therefore, the utilization of only pedal pulses for diagnosing PAD may lead to both false positive and false negative results.21,43 The sensitivities and specificities of the dorsalis pedis and posterior tibial pulses for diagnosing PAD were 60% and 64%, and 68% and 70%, respectively, in this study. 21 Our results indicate that the inability to palpate the pedal pulses increased the likelihood of PAD by nearly 400% (OR = 4.9).
Calcification of the pedal arteries is a common finding in patients with DM, although 40% of patients admitted to a well-respected diabetic foot unit did not have radiographic evidence of calcification. 6 PAD was found in 60% of patients with calcification of the pedal arteries, while PAD was identified in 30 % of patients who did not have calcification. 6 The predictive variables associated with medial artery calcinosis included duration of DM > 20 years (OR 2.1), retinopathy (OR 2.2), albuminuria (OR 3.3), and PAD (OR 4.2). 6 The relationship between peripheral neuropathy and pedal artery calcification has also been established. 23 Overt medial artery calcinosis is more common in diabetic patients with peripheral neuropathy, and this may be related to sympathetic denervation.8,15 Since there is a significant association between medial artery calcinosis and diabetic neuropathy, the TBI may be more useful as a screening test in this group of patients since peripheral neuropathy and medial artery calcinosis do not appear to have a significant influence on the TBI.23,29,43
Combining the ABI with TBI improves the ability to diagnose PAD because the ABI has high specificity (low false positives) and the TBI has high sensitivity (low false negatives). The mean difference between the ABI and TBI is less than 0.4 in patients with normal and low ABIs, however this gradient rises dramatically in patients with an elevated ABI due to noncompressibility (mean gradient of 0.85). 8 The TBI is more reliable than ABI in diabetic patients with noncompressible arteries and/or peripheral neuropathy.8,43 The arteries of patients with DM can be more diseased than the ABI would indicate due to medial artery calcinosis and a falsely elevated ABI. As illustrated in this study, PAD was diagnosed in 43% of patients with a normal ABI based on the finding of an abnormal TBI. Our study also demonstrated that monophasic Doppler wave forms were universally associated with PAD; however PAD can be present in patients with biphasic or triphasic wave forms.
An ABI ≤0.90 is not only indicative of PAD but also associated with a 3- to 6-fold increased risk of mortality. 10 In patients with DM, elevated ABIs > 1.3 are also associated with higher risk for cardiovascular death than an ABI ranging from 0.91 to 1.3. 20 A low TBI is also associated with increased cardiovascular risk in patients with and without DM. 20 The Society for Vascular Surgery recently released guidelines which state that an ABI > 0.8 in patients with DFU is unlikely to require revascularization to achieve healing, although they state that measurement of toe pressures in diabetic patients is mandatory. 28 Another study reported that an absolute toe pressure of > 55 mm Hg has been correlated with wound healing in patients with DFU. 30 For diabetic patients with foot ulcers or gangrene, critical limb ischemia was defined as an ankle pressure of < 70 mmHg or toe pressure < 50 mm Hg. 30 While some patients may demonstrate clear signs of critical limb ischemia, other patients present with a lesser degree of vascular impairment with absolute toe pressures of 50-69 mmHg. At the current time, we are unaware of any guideline that indicates what toe pressure is needed to achieve high rates of healing in elective, reconstructive foot and ankle surgery. Several authors have used a great toe pressure of < 45 mmHg to indicate poor healing potential of DFU and amputations.5,13,36 Other authors have used a great toe pressure threshold of ≥ 55 mmHg to indicate adequate perfusion for healing of DFU.4,10,30 Our current protocol in patients with a nonhealing DFU or patients undergoing elective surgery is to obtain vascular surgery consultation for ABIs < 0.91 or TBIs < 0.7 and for noncompressible arteries (ABI > 1.4) with a TBI < 0.7 (Figure 1). In general, our vascular consultants expect primary healing of DFUs or elective surgical wounds if toe pressure is ≥ 55mm Hg. Communication between the vascular surgeon and foot and ankle surgeon is paramount, since the magnitude of the surgical procedure may dictate what path to follow. For instance, PAD in a patient undergoing a percutaneous Achilles tendon lengthening might be approached differently than PAD in a patient undergoing a major Charcot reconstruction.
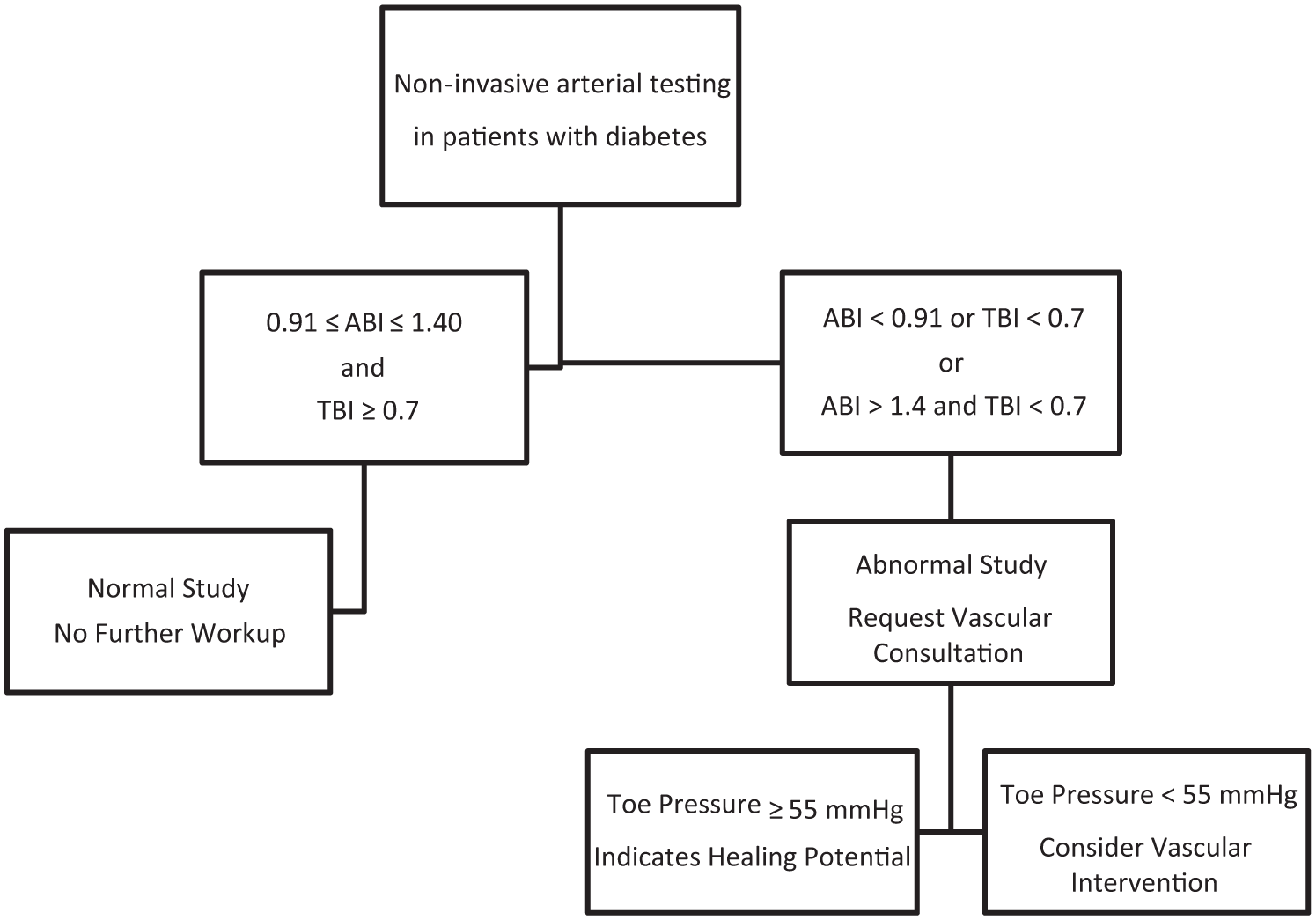
Algorithm depicting non-invasive arterial testing in patients with diabetes.
The decision to proceed with angiography is individualized, since the use intravascular contrast is not benign in patients with diabetic nephropathy. The pathoanatomy of PAD in diabetic patients tends to involve the profunda femoris artery and the infrapopliteal vessels at the popliteal trifurcation. 12 The distribution of the distal PAD is often amenable to endovascular or open bypass reconstruction when indicated. We feel that optimal management of these complex patients requires a multidisciplinary approach, often employing the skills of vascular surgeons, cardiologists, hospitalists, infectious disease specialists, and endocrinologists.
Our results are similar to the recent Eurodiale study that found that 49% of patients presenting for DFU had PAD. 33 A surprising finding of our series was the high rate of PAD observed in patients without diabetic foot disease. There is no an apparent explanation for this finding other than to acknowledge that 78% of these patients had peripheral neuropathy, a complication of DM that is associated with PAD.
This study had several limitations that need to be acknowledged. The most obvious limitation was the retrospective nature of this study, and the accuracy of our data was dependent on the accuracy of our electronic medical records. Our health care system was composed of many hospitals and an attempt has been made to standardize the vascular laboratories. Despite this, a potential for variation in the testing existed which could have introduced measurement bias. Our study cohort was largely composed of patients with complicated diabetes and the prevalence of PAD reported in this study may not be representative of diabetic patients in general.26,37 Our patients with nondiabetic foot problems had a high prevalence of peripheral neuropathy, and consequently, the rate of PAD may be higher than normally seen in a general diabetic foot population. Therefore, readers should interpret our results with this limitation in mind. Not all authors believe that measurement of toe pressure and calculation of the TBI is the optimal method for assessing PAD in patients with DM. Calcification of the metatarsal or digital arteries may make the toe pressure measurement inaccurate, although this is less likely in the digits. 14 Measurement accuracy of the TBI may be potentially limited because the digital arteries of the great toe may be susceptible to vasoconstriction and increased response to colder room environment. 20 Toe pressures reflect perfusion of the forefoot, and it is possible that perfusion of the midfoot and hindfoot may not be accurately assessed. We also recognize that the ABI and TBI reflect the macrovascular anatomy, and that microcirculatory abnormalities with changes such as arteriovenous shunting are not detected with these tests. Our results did not identify a significant difference in the prevalence of PAD, and consequently, this study is underpowered to definitively state that no real differences exist in the prevalence of PAD between patients with and without diabetic foot pathology. To definitively state that there was not a significant difference in the prevalence of PAD, 482 diabetic patients in each group would be necessary to achieve 80% power with an α of .05. Our results identified a significant decrease in the left TBI and left great toe pressure in patients with established diabetic foot pathology. We do not have a good explanation for this isolated finding affecting only the left side. Although the prevalence of PAD was not significantly different, the severity of PAD was worse in patients with diabetic foot pathology as compared to patients with nondiabetic foot pathology (Table 2). Thirty-four of 80 (42.5%) patients with PAD and diabetic foot pathology had ischemia compared to 3 of 23 (13%) patients with PAD and nondiabetic foot pathology (P < .05). Diabetic patients diagnosed with PAD may not have enough obstruction to warrant intervention as illustrated by the fact that over 60% of diabetic foot patients and 87% of nondiabetic foot patients did not meet the threshold of ischemia as described by Mills et al. 28
Although peripheral neuropathy was associated with a 2.3 increased likelihood of being diagnosed with PAD, this increased risk was not statistically significant (OR 2.31 [95% CI 0.84-6.33], P = .10). Despite this lack of statistical significance, we feel that this increased risk of PAD was clinically meaningful in diabetic patients with peripheral neuropathy, and foot and ankle surgeons should have heightened suspicion for PAD in patients with neuropathy. Similarly, foot and ankle surgeons should be aware of the increased risk of PAD in patients with end-stage renal disease on dialysis.
Conclusion
Despite the limitations cited above, foot and ankle surgeons should be aware of the current guidelines and recommendations from national and international consensus groups regarding noninvasive arterial testing in patients with DM (see Table 4). Patients with diabetic foot pathology should be anticipated to have more severe PAD than patients without diabetic foot pathology. Due to the relative noncompressibility of calcified distal arteries in patients with DM, the ABI may be within normal limits in patients with PAD. This false negative result may lead surgeons to assume that normal perfusion is present even in patients with palpable pulses. Medial artery calcification decreases the sensitivity of the ABI for detecting both PAD and death from cardiovascular diseases in patients with DM. The importance of measuring toe pressures and calculating the TBI cannot be overestimated, particularly in diabetic patients with peripheral neuropathy and end-stage renal disease.20,30 We recommend vascular consultation for ABIs < 0.91 or TBIs < 0.7 and for noncompressible arteries (ABI > 1.4) with a TBI < 0.7. Diabetic patients with absolute great toe pressures < 55 mm Hg may benefit from arteriography prior to major reconstructive surgery.
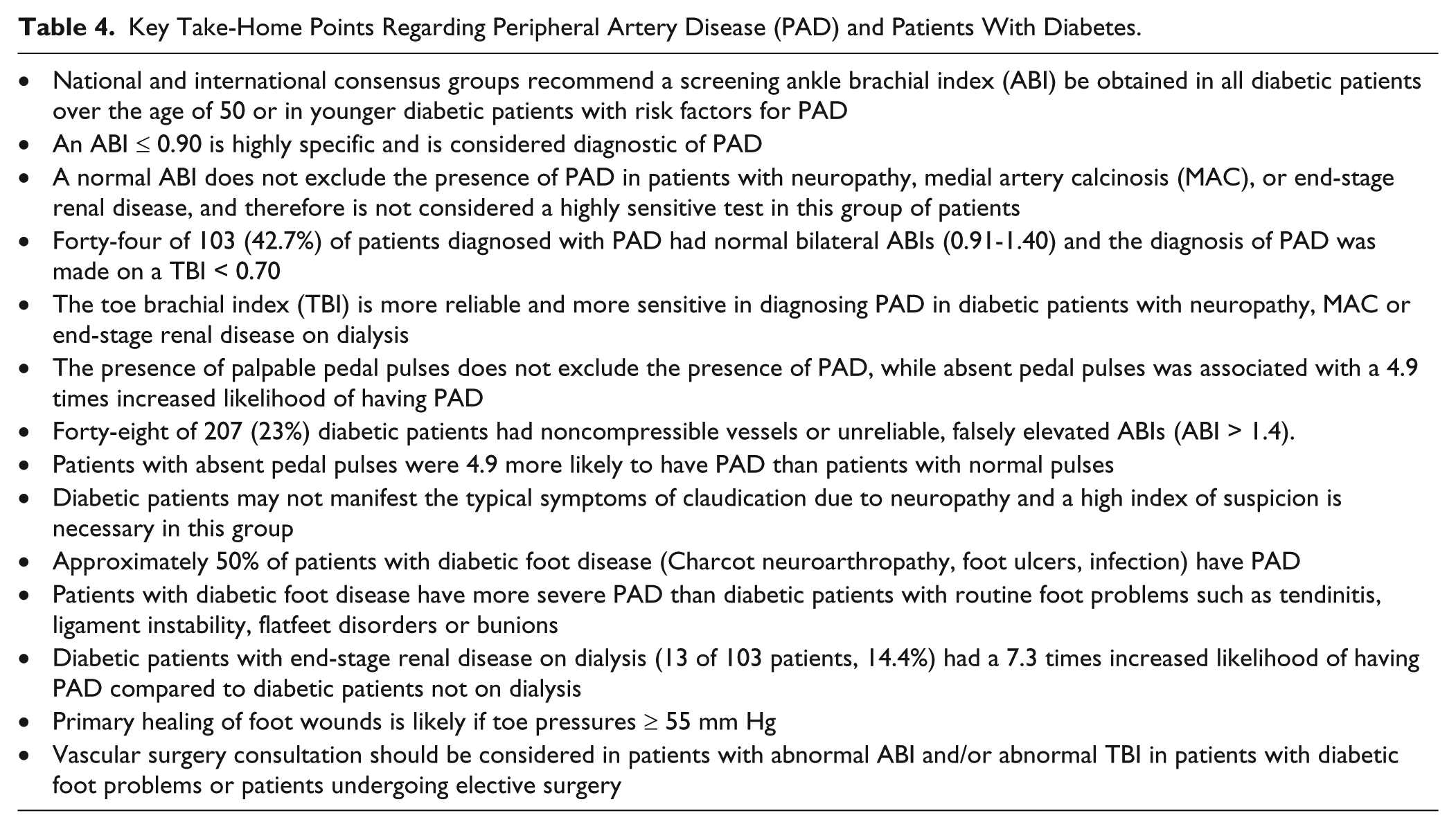
Key Take-Home Points Regarding Peripheral Artery Disease (PAD) and Patients With Diabetes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.