
Abstract
Background:
Operative management of chronic exertional compartment syndrome of the tibialis anterior muscle compartment (ant-CECS) usually involves the use of a fasciotome. Collateral tissue damage such as hematoma and nerve damage may occur during the procedure. The current report assessed the feasibility and safety of an alternative tool for the operative management of ant-CECS.
Methods:
The system had a speculum-like hollow tube that was inserted via a 2-cm skin incision and allowed for the protected advancement of a fasciotome. The device was tested in patients with bilateral ant-CECS. Symptoms were prospectively scored before and after surgery using a 5-category verbal rating scale (VRS). Fourteen patients (age 26 ± 10 years) were analyzed. Complications and operative efficacy were determined using physical examination and questionnaires after 21 (range = 16-25) months.
Results:
Technical operative success rate was 100% (28/28 legs). Operation time was 10 ± 2 minutes per leg (range = 6-14). Perioperative complications were not observed. One superficial wound infection was treated nonoperatively. Significant reductions in pain (–2.2 ± 1.1 on 5-point VRS, P < .001), tightness (–1.9 ± 1.6, P = .01), cramps (–1.4 ± 1.6, P = .009), muscle weakness (–1.6 ± 1.2, P < .001), and altered sensibility (–1.3 ± 1.4, P = .005) were registered 21 months postoperatively.
Conclusion:
This fasciotome was simple to use and allowed for a safe fasciotomy in patients with leg ant-CECS. A randomized controlled trial comparing the present device with a widely used fasciotome was under way at the time of writing of this study.
Level of evidence:
Level IV, case series
Introduction
In 1 of 8 young individuals with exercise-induced leg pain, symptoms are due to a chronic exertional compartment syndrome (CECS). 27 In athletes, this portion may even be higher. 8 Leg CECS is usually found in the anterior (ant-CECS, 40%-60%) or deep flexor (dp-flex-CECS, 30%-50%) compartments.10,28 Typically, patients experience exercise-induced pain that is alleviated by a period of rest.4,39 Other symptoms are tightness, cramps, muscle weakness, and diminished sensibility.14,25 Diagnosis is confirmed with a dynamic intracompartmental pressure measurement (ICP). A pressure ≥30 mm Hg 1 minute after a standardized provocative treadmill test or ≥20 mm Hg 5 minutes thereafter are widely used cut-off points for the diagnosis.26,35,40
Once diagnosed, patients with CECS initially undergo nonoperative treatment but often to no avail.7,45 Most recalcitrant patients opt for operative intervention. During surgery, the fascia is ether split (fasciotomy) or a strip is removed (fasciectomy).1,3,6 Several operative techniques and devices have been proposed.10,51 In previous times, the operative management of ant-CECS involved a 10- to 15-cm longitudinal incision. 23 With the introduction of a fasciotome, Due and Nordstrand reduced the size of the skin incision to 2 to 3 cm. 11 A fasciotome is essentially a metal rod that is mounted with a vertically placed small knife that splits the fascia subcutaneously. This technique is termed “semi-blind” as advancement of the tip of the fasciotome does not occur under direct vision.
Complications such as superficial peroneal nerve damage have prompted physicians to explore alternative approaches such as an endoscopically assisted technique allowing visualization of anatomical structures at risk. 24 Feasibility was demonstrated in cadaveric legs as well as in patients.18,20,36 However, cosmesis may not be improved as total incision size was larger whereas operation time was possibly longer. 19 Clinical data on these endoscopic techniques are scarce, and more research is necessary to determine whether endoscopic assisted techniques are superior compared to nonendoscopic approaches in patients with ant-CECS.21,50
Literature concerning efficacy and complication rates after operative treatment of ant-CECS is heterogeneous in terms of outcome. Success ranged from 63% to 100%.1,9,12,15,17,22,29,30,34,37,41,42,45,47 Complication rates including muscle and nerve damage varied from 5% to 17%. However, only 6 of 13 retrospective studies reported on the incidence of complications.1,9,12,15,17,22,29,30,34,37,41,42,45,47 Prospectively obtained complication rates range from 0% to 11%.13,33,38,43,46
The options for operative treatment of ant-CECS may leave room for improvements. The present study aimed to answer whether an alternative fasciotome was simple to use, safe, and effective in the treatment of ant-CECS. If so, it would be worthwhile to test this tool in a randomized controlled trial.
Methods
The Department of Sports Medicine of Máxima Medical Center, Veldhoven, The Netherlands, serves as a national referral center for sports related injuries. In recent years, considerable expertise has been gained in exercise-related pain syndromes, including vascular syndromes in cyclists and CECS.32,44,48,49 In the year of 2013, a total of 221 patients suspected of having CECS were referred for an ICP measurement.
Patient Selection
The present study entailed a portion of all patients (n = 123) who were evaluated by the department of sports medicine between January 1 and June 30, 2013, with leg complaints that were suggestive for a CECS. Study inclusion criteria were bilateral leg symptoms associated with ant-CECS and a positive ICP measurement (ICP ≥ 30 mm Hg 1 minute after a standardized provocative test, or ICP ≥ 20 mm Hg after 5 minutes). Patients with combined CECS syndromes (ant and dp-flex n = 8, ant and peroneal n = 4, peroneal and dp-flex n = 1) were excluded, as were dp-flex (n = 12), CECS of forearms (n = 6), peroneal (n = 1), recurrent ant-CECS (n = 4), and unilateral ant-CECS (n = 2). Patients that were operated in a different hospital (n = 7) were also excluded (Figure 1).
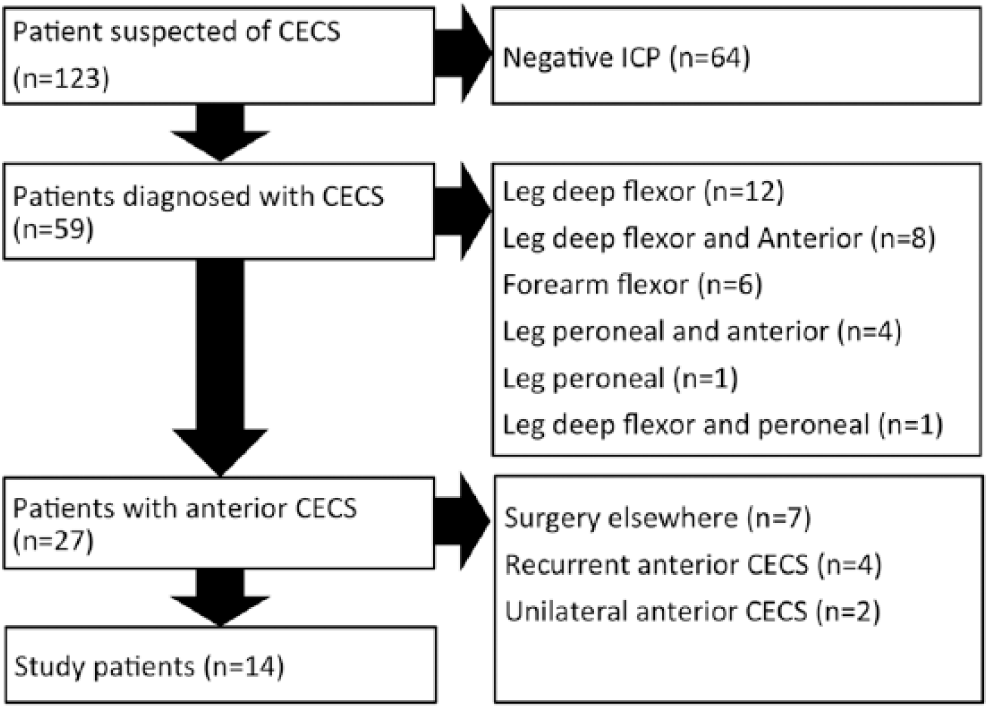
Patient selection. All patients were evaluated for possible CECS during a 6-month time period in a high-volume institution. CECS, chronic exertional compartment syndrome; ICP, intracompartmental pressure measurement.
During the 6-month study period, 14 patients with bilateral ant-CECS fulfilled study criteria. Provocative sports are depicted in Table 1. Median duration of symptoms prior to operation was almost 3 years. Two patients had previously received surgery for dp-flex CECS.
Characteristics of Patients Undergoing Surgery for Tibialis Anterior Muscle Chronic Exertional Compartment Syndrome (n = 14).
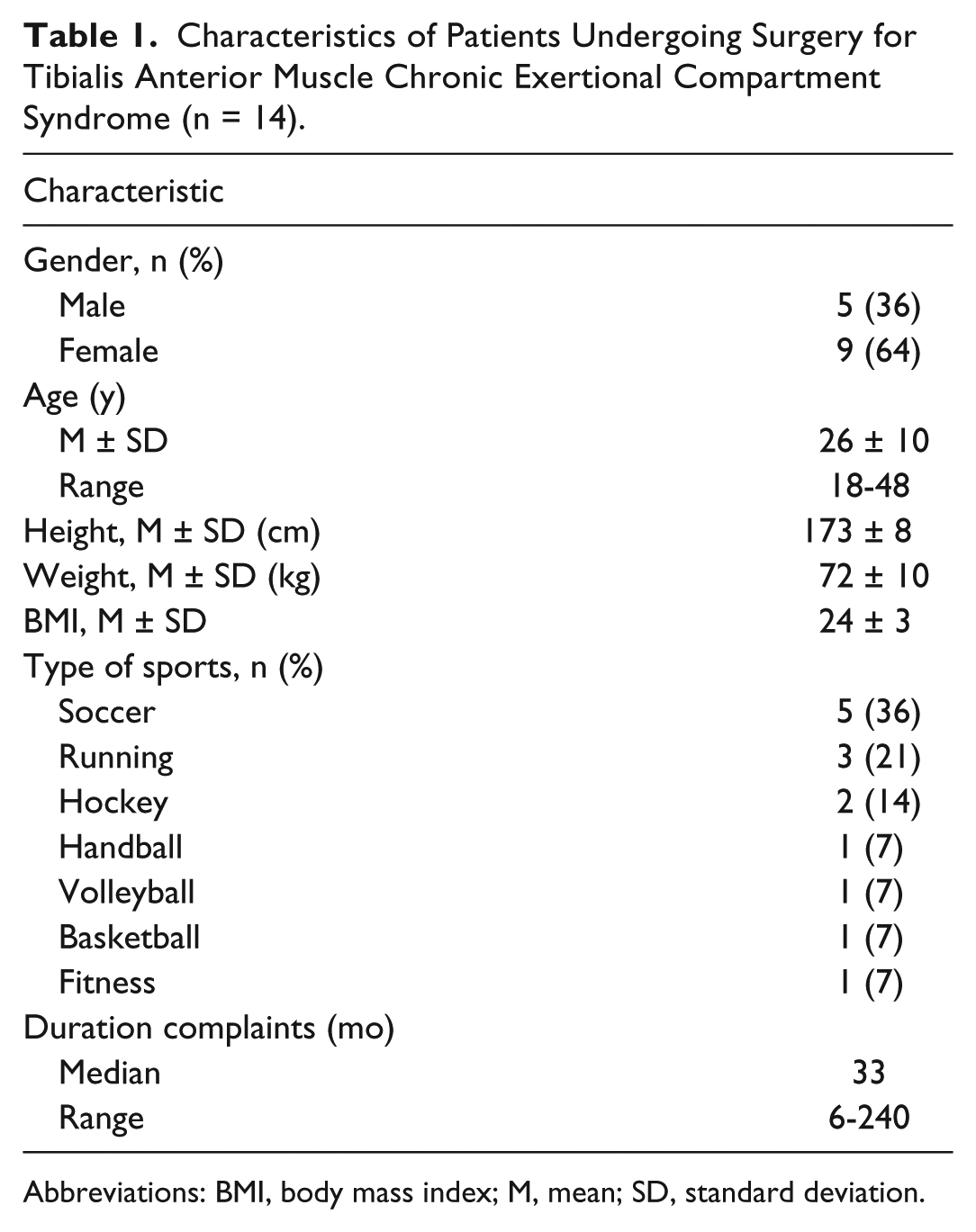
Abbreviations: BMI, body mass index; M, mean; SD, standard deviation.
Diagnosis and Intracompartmental Pressure Measurement
Two investigators (M.C. and A.H.) with ample experience (over 1500 procedures) performed the ICP measurements using a slit catheter (Stryker Instruments, Kalamazoo, MI). Patients were lying supine with the ankle joint in 20 degrees of plantarflexion and the knee in 10 to 30 degrees of flexion. The leg was positioned horizontally with the tibialis anterior margin in neutral position. Before needle introduction, a 1-cm2 portion of overlying skin was infiltrated using 2 mL of 1% lidocaïne. The needle containing the catheter was inserted horizontally at the junction of the proximal and middle thirds of the anterior aspect of the leg. A perceptible “pop” is usually experienced upon piercing of the fascia.
After the needle was removed while leaving the tip of the flexible catheter in the compartment, patients were instructed to evert and dorsiflex the foot against resistance as a test for correct catheter placement. After the catheter was flushed once with saline, resting pressures were measured. The arterial line manometer was subsequently disconnected and the catheter end was taped to the skin. The exercise protocol depended on the patients’ physical ability and on the activity subjectively provoking the symptoms. In most patients, symptoms were elicited during treadmill running starting with an 8 km/h speed and an 8% inclination during 5 minutes. If symptoms remained absent, heel walking or uphill walking tests were used as an additional provocation. Patients were encouraged to continue until symptoms were maximal. After ensuring the catheter was still functional and in the correct position, pressures were again recorded in a supine position immediately after cessation, and after 1 and 5 minutes.
The sports physician communicated to the patient whether history and levels of ICP were consistent with the diagnosis of ant-CECS. If patients opted for surgery, they received an appointment for an operative outpatient visit. All patients were counseled by the senior author (M.S.), a surgeon with extensive experience in the operative treatment of CECS (>250 operations). Complications and the department’s historical success rates of ant-CECS surgery using the technique proposed by Due and Nordstrand were discussed with the patients. They were also informed on the characteristics of the alternative operative tool and its method of action was demonstrated. All patients consented either verbally or in writing to undergo the procedure using the alternative tool. None of the patients opted for a Due and Nordstrand procedure when given the alternative for the current technique.
Description of Technique
The fasciotome (FascioMax) consisted of 2 components. The first part was a speculum-type stainless steel instrument (Figure 2). By manipulating the handle, the 2 semi-circular blades either open or close, thus forming a 30-cm-long, 5-mm-wide (inner diameter) hollow tube. The second part was a stainless steel fasciotome consisting of a thin metal rod holding a small vertically placed knife (Figure 2). In essence, it was a thinner version of the fasciotome proposed by Due and Nordstrand. 11 When closed, the tube acted as a sheath in which the fasciotome was advanced towards the end (Figure 2).
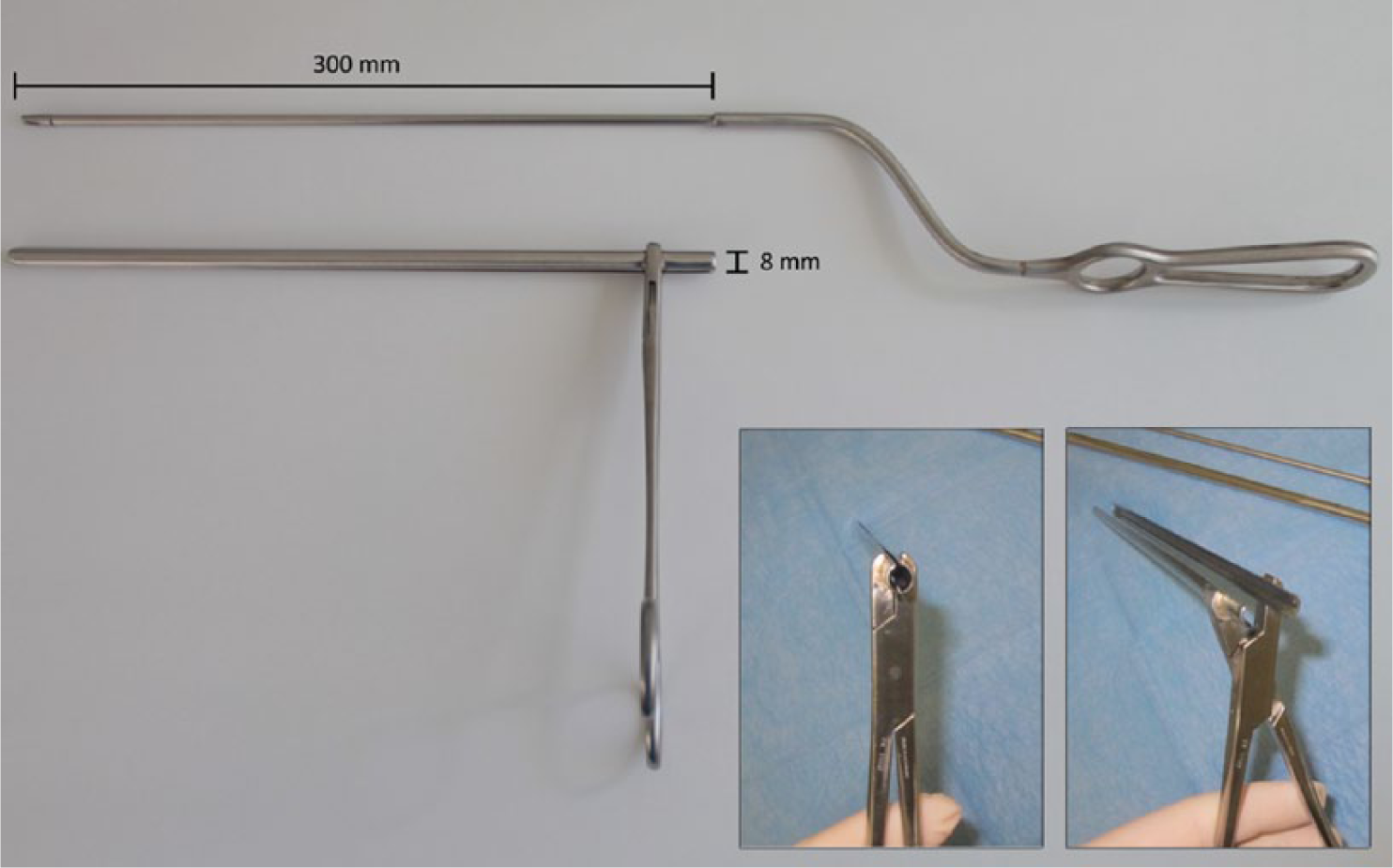
The fasciotome consists of 2 separate parts. The first part is a speculum-type instrument with a handle, lock, and 2 long blades. Tips of the blades are blunt, so tissue damage is minimized during advancement. By manipulating the handle, the 2 semicircular blades either open up or close, thus forming a 30-cm-long hollow tube in which the second part, a small vertical knife mounted on a thin metal rod, can be advanced.
The contour of the tibialis anterior muscle was marked onto the skin using an operative marker. A tourniquet was not used. After sterile exposure, a 2- to 2.5-cm longitudinal skin incision was made approximately 3 cm lateral to the medial margin of the tibia at the transition zone between the middle and distal thirds of the tibialis anterior muscle. The incision was made approximately halfway along the line from the fibular head to the lateral malleolus (3A). The superficial crural fascia was bluntly freed of overlying fatty tissue. A 2-cm-wide subcutaneous tunnel immediately superficial to the crural fascia was created bluntly toward the knee joint and the ankle joint using scissors (Figure 3B). The exit site of the superficial peroneal nerve penetrating the crural fascia was located lateroinferior from this tunnel, so nerve identification was not performed. Following a 1.5- to 2-cm longitudinal fascial incision (3C), the upper blade of the speculum was carefully advanced in the subcutaneous tunnel toward the knee superficially to the muscle’s fascia (Figure 3D). The tips of the instrument were positioned at least 5 cm away from the fibular head so the common peroneal nerve was not damaged (Figure 3D). Once the correct position of the instrument was confirmed by transcutaneous palpation (Figure 3D), the fasciotome was introduced (Figure 3F) and advanced into the hollow tube that was formed by the 2 blades (Figure 3G). The fascia was thus opened in a controlled fashion. The distal portion of the crural fascia (approximately 4-5 cm toward the ankle joint) was cut under direct visual inspection using a small retractor and scissors (Figure 3H). Completeness of the fasciotomy was confirmed by palpating medial and lateral fascial edges (Figure 3I). Once confirmed, the skin was closed in one layer. (This procedure and a fasciotomy according to Due and Nordstrand are shown in more detail in a short video available as an online electronic supplement.) Patients received compressive stockings day and night for 14 days. They were instructed to refrain from sports during this time period, but normal ambulation was recommended.
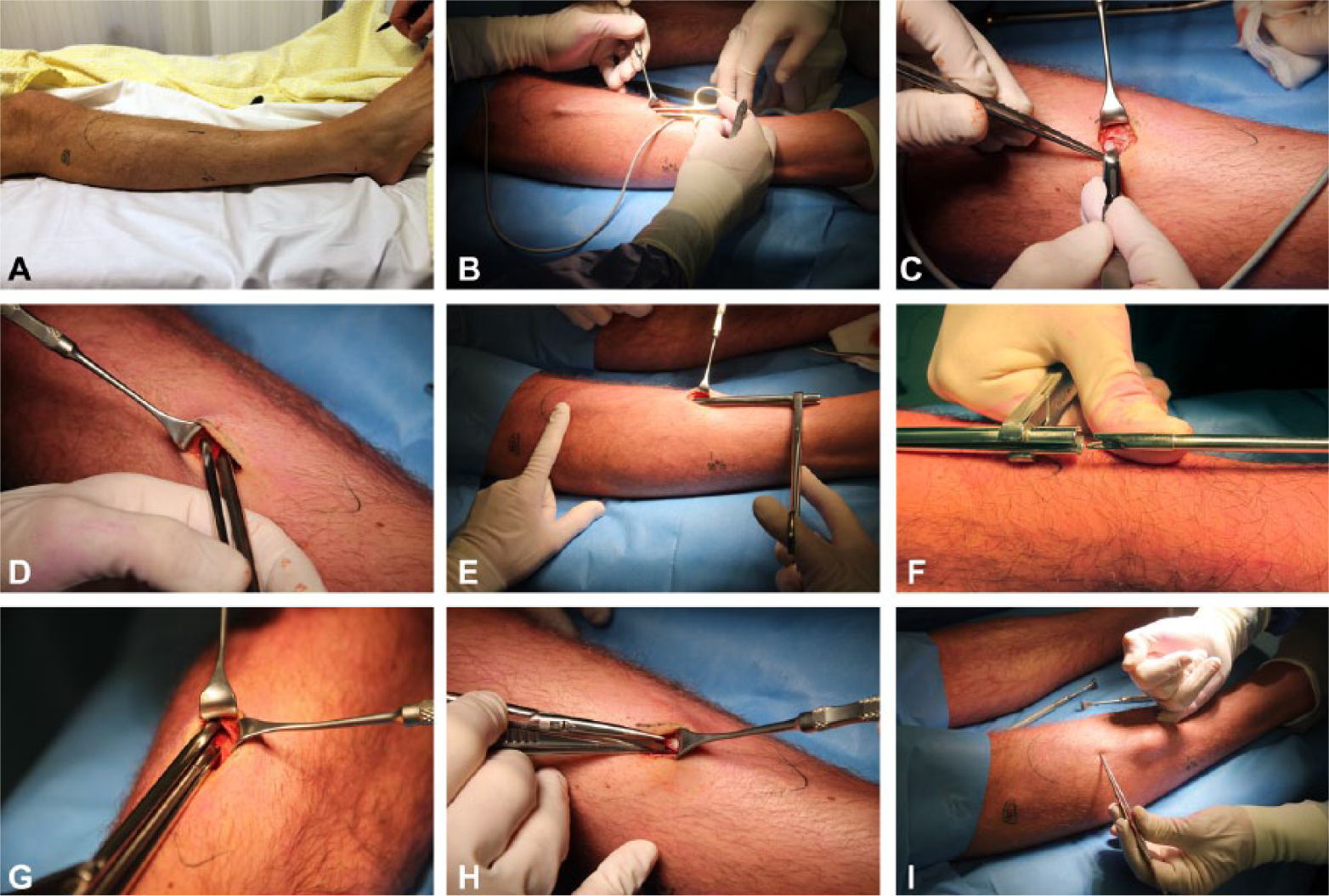
Intraoperative view of the procedure. In all images, the knee is located on the left. (A) A 2-cm incision is made halfway along the line from the fibular head to lateral malleolus, approximately 3 cm lateral to the tibia. (B) A subcutaneous tunnel is created via the skin incision. (C) A 1.5- to 2-cm incision is made in the crural fascia. (D) The 2-bladed instrument is inserted. The deepest blade is located just underneath the fascia covering the muscle compartment, while the superficial blade is positioned in the subcutaneous tunnel between the fascia and the skin. (E) The fascia is grasped between the 2 blades by closing the handle; the position of the tip of the instrument is checked via transcutaneous palpation. (F) The fasciotome is introduced into the tube. (G) The protective tube may be opened slightly to visualize the position of the fasciotome in relation to the crural fascia. (H) Toward the ankle, the crural fascia is opened under direct visual inspection using scissors. (I) Completeness of the fasciotomy is confirmed by palpating medial and lateral fascial edges using the fifth finger that is inserted via the skin incision.
Postoperative Outpatient Visit
Two weeks postoperatively, patients were interviewed and physically examined by the senior author at the outpatient department. Complications due to tissue damage such as hematoma, tunnel infection, loss of sensibility, or infection were tabulated. Instructions on rehabilitation were then provided. A last telephone contact occurred once thereafter, usually 6 to 8 weeks postoperatively.
Questionnaire
Each patient completed a questionnaire just prior to the ICP measurement. Pain, tightness, cramps, muscle weakness, and diminished sensibility were scored using a verbal rating scale (VRS). Patients judged each symptom as extremely severe (4 points), severe (3 points), moderate (2 points), mild (1 point), or absent (0 points). This scale is known to allow for statistical analysis. 5 Postoperatively, current functional status and symptoms were determined using similar symptom questionnaires.
Statistical Analysis
Data are expressed as mean ± standard deviation when normally distributed, or as median and range if not normally distributed. Mean pre- and postoperative symptoms were compared using a paired-samples t test. For all tests, P ≤.05 was considered significant.
This study was conducted in accordance with the World Medical Association Declaration of Helsinki (Brazil, October 2013). Study design and protocol were reviewed and approved by the Medical Ethics Committee of Máxima Medical Center.
Results
Mean ICP at rest was 20 ± 8 mm Hg. Immediately after the standardized provocative test, it increased to 46 ± 12 mm Hg. One and 5 minutes after cessation, pressures again declined to 41 ± 12 mm Hg and 34 ± 7 mm Hg, respectively (Figure 4).
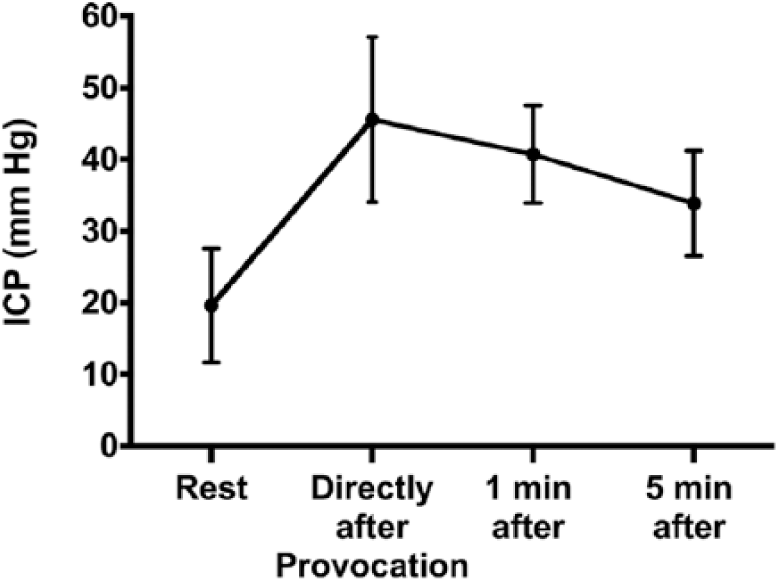
Tibialis anterior muscle intracompartmental pressure (ICP) in patients (n = 14) with chronic exertional compartment syndrome. Readings were obtained during rest, and directly, 1 minute, and 5 minutes after a standardized provocative treadmill test. Dots represent mean pressure values (n = 14); error bars represent standard deviations.
The fasciotome was easily introduced and advanced with mild resistance. Correct positioning of the tips relative to the fibular head (approximately 5 cm distal to) was easily confirmed by transcutaneous palpation. Splitting of the fascia occurred with the first attempt. The technical success rate as judged by intraoperative palpation of both edges of the split fascia via the 2-cm incision was 100%. Operation time (“skin to skin”) was 10 ± 2 minutes per leg (range = 6-14).
Two weeks postoperatively, there were no cases of disturbed wound healing, hematoma, subcutaneous tunnel complications, or nerve injuries (n = 28 legs). One patient had used a 7-day course of antibiotics for superficial infection of the incision as advised by his general practitioner. Thus, the overall complication rate was 3.6% (1/28 legs).
Symptoms were assessed preoperatively (n = 14) and postoperatively (n = 13, loss to follow up = 1). Before the operation, the 2 principal symptoms during exercise were pain and tightness. Less prominent symptoms were cramps, muscle weakness, and diminished sensibility. Self-reported recovery was 4 weeks (mean; range = 1-8). All symptoms were greatly attenuated during follow-up evaluation, both at very short term (median = 4 months, range = 3-9; n = 13, response rate = 93%) and after a longer period (median = 21 months, range = 16-25; n = 13, response rate = 93%). Twenty-one months postoperatively, mean levels of pain had decreased by 2.2 ± 1.1 (5-point VRS, P < .001), and levels of tightness had dropped by 1.9 ± 1.6 (P = .001). Cramps (–1.4 ± 1.6, P = .009), muscle weakness (–1.6 ± 1.2, P < .001), and diminished sensibility (–1.3 ± 1.4, P = .005) were also significantly attenuated (Figure 5).
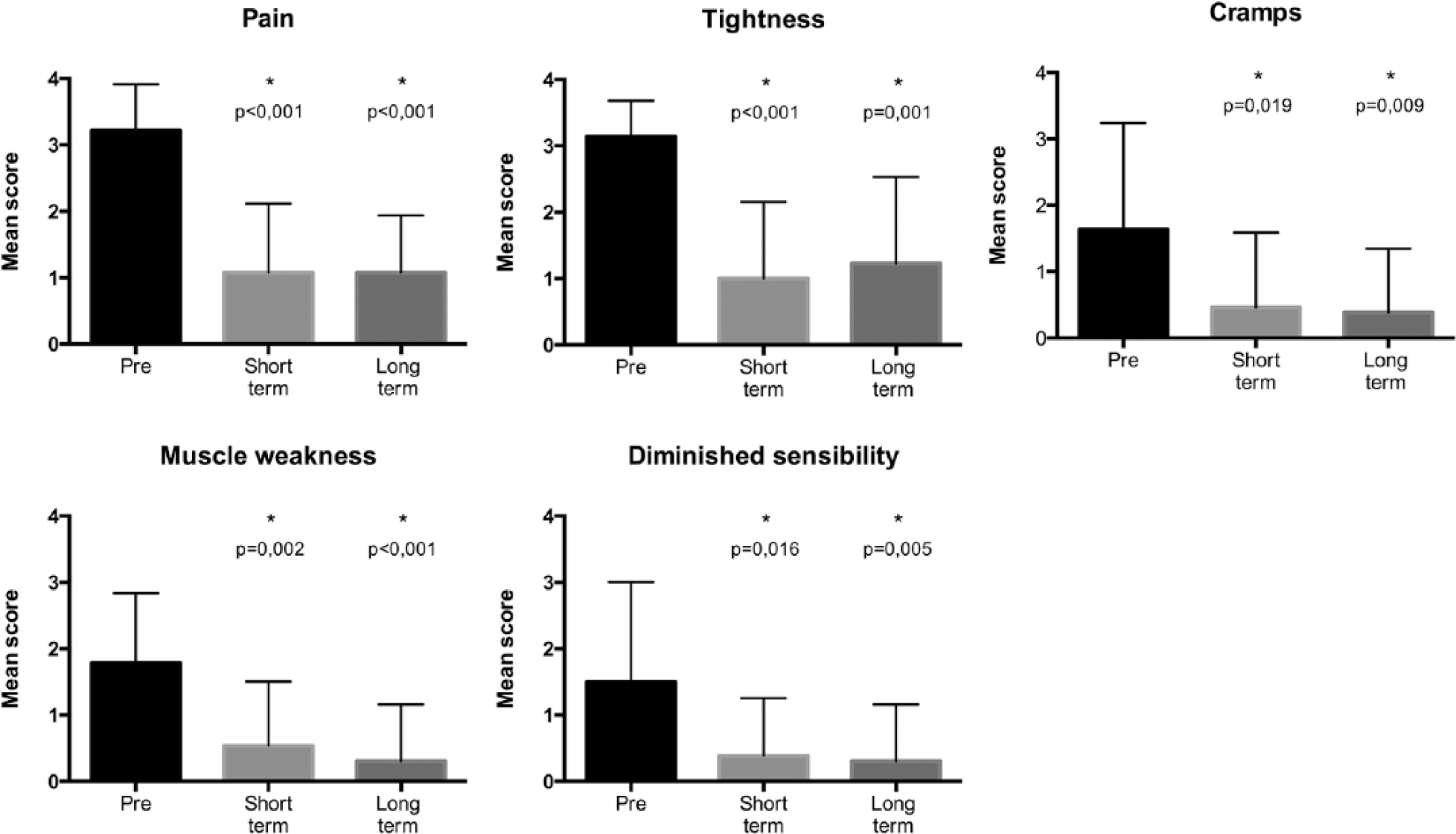
Symptoms in patients before (pre, n = 14), 5 months (very short term, n = 13), and 21 months (longer follow-up, n = 13) after a fasciotomy. Symptoms associated with CECS were scored as extremely severe (4 points), severe (3 points), moderate (2 points), mild (1 point), or no symptoms (0 points). Bars represent mean values, and error bars depict standard deviation. *Significant reduction compared to mean preoperative score.
Almost 2 years postoperatively (median, 21 months), 31% of the patients (n = 4) judged their clinical outcome as excellent, 31% (n = 4) as good, 23% (n = 3) as fair, 8% (n = 1) as poor, and 8% (n = 1) as bad. All patients had resumed a type of sports activity, although 2 patients had abandoned their original sport (soccer). The one patient who judged her postoperative result as “poor” was able to continue her sport at a reasonable level, although with complaints. She was later diagnosed with medial tibial stress syndrome during follow-up. The patient who judged his postoperative result as “bad” was treated for Achilles tendinopathy. However, pain in the decompressed anterior compartment was absent in these patients who rated the result as “poor” and “bad.”
Discussion
The aim of the present study was to test an alternative technique for the operative treatment of patients with ant-CECS. The technique was minimally invasive but allowed for optimal tissue protection. The results indicate that this tool (FascioMax) was simple, safe, and effective for the treatment of ant-CECS. Performance and handling of the current instrument were thoroughly assessed during the trial. The fasciotome performed as expected during each of the 28 operative procedures. Introduction into the tissue tunnel and advancement along the fascial plane were not difficult. Splitting of the fascia was successful in all patients. A second introduction of the device or additional skin incisions was not required. Removal of the instrument was smooth in all patients. Clinically relevant bleeding was not encountered. These findings indicate that the tool was simple to use.
All patients had a 2-week postoperative follow-up ensuring that all potential complications were identified. One wound infection that was treated successfully with antibiotics resulted in a 3.6% minor complication rate (1/28 legs). Signs of an absorbed hematoma were occasionally observed. Major complications such as major hematoma, deep tissue infection, or superficial peroneal nerve damage did not occur. In the literature, complication rates up to 17% have been reported. These include major complications that required operative intervention.1,9,12,15,17,22,29,30,34,37,41,42,45,47
Cardinal symptoms were significantly reduced at 5 and 21 months postoperatively. Furthermore, all patients were able to engage in sports. Literature concerning the clinical results of operative treatment for ant-CECS is very heterogeneous in terms of clinical outcome. Therefore, it is impossible to compare present efficacy rates with previous studies. Only a randomized controlled trial would allow for a comparison of efficacy. Nevertheless, the results of the present trial indicate that this technique effectively reduced symptoms associated with the presence of ant-CECS.
The present study has limitations. First, the absolute diagnostic value of ICP measurements is debated in recent literature.16,31 However, the role of ICP measurements in our hospital was to confirm a diagnosis that is predominantly based on a characteristic medical history and physical examination as judged by exceedingly experienced sports physicians (evaluated >1500 patients suspected with CECS). Moreover, a recent systematic review emphasized that an ICP ≥30 mm Hg 1 minute after provocation along with a convincing history is highly suggestive of CECS. 2 In the present study, all patients demonstrated both a highly suggestive medical history and an ICP ≥30 mm Hg 1 minute after provocation. Second, patients were counseled before the operative procedure by the surgeon (M.S.) who participated in the development of the alternative fasciotome and performed all operative procedures. Although counseling was performed on the basis of current knowledge, his behavior may have prompted patients to opt for the new tool. Furthermore, the senior author was the only person to register potential complications. Although patients were instructed to report complications in the postoperative questionnaire, this may potentially have influenced study results. Finally, the present study was purely observational and had no control intervention. However, a randomized controlled trial would only be worthwhile if the alternative tool was found to be safe in the present pilot study.
In conclusion, the described fasciotome was a simple, safe, and effective tool for the operative management of patients with chronic exertional compartment syndrome of the tibialis anterior muscle compartment of the leg. Data of the present safety and feasibility study were so encouraging that a randomized controlled trial comparing the new technique (FascioMax) and the technique according to Due and Nordstrand was initiated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.