
Abstract
Background:
Using a total contact orthosis (TCO) is an effective method to offload in diabetic patients with foot neuropathy. However, the redistribution of peak plantar pressure is mostly observed during level walking, which may differ from other walking activities. The aim of this study was to investigate the plantar pressure from 4 regions of the foot during different walking activities (level walking, ramp ascending, ramp descending, stair ascending, and stair descending) in neuropathic diabetic patients with and without a TCO.
Methods:
Sixteen neuropathic diabetic patients aged 40 to 60 years with calluses and hallux valgus were included in this study and were provided with TCOs made up of multifoam, Plastazote, and microcellular rubber. The plantar pressure and contact area with the TCO and without the TCO were recorded using the Pedar X system during different walking activities.
Results:
A significant reduction of plantar pressure during different walking activities at the toes and forefoot regions was observed while walking with the TCO compared with walking without the TCO (control condition). Plantar pressure increased at the midfoot region when walking with the TCO, and no significant difference was observed at the hindfoot region between the control and TCO conditions. Furthermore, maximum contact area was observed during level walking with the TCO compared with other walking activities.
Conclusion:
The TCO significantly reduced and redistributed the peak plantar pressure from the sites where the ulceration rate is higher at the toes and forefoot compared with the other regions of the foot.
Level of evidence:
Therapeutic level II, lesser quality randomized controlled trial
Excessive peak plantar pressure is the most common cause of ulceration in the presence of foot deformity or neuropathy. Foot deformities result in an abnormal gait pattern, and neuropathy also causes abnormal plantar pressure.1,4,21,31,34 Prolonged abnormal plantar pressure at a specific site increases the chance of ulceration. 11 It has been reported that 67% of all lower extremity amputations were preceded by diabetic foot ulceration. 36 Even though an ulcer had healed completely through medical therapy, the chance of reulceration was still high (30%-40%) within the first year after healing.6,28,35 Diabetic foot ulcerations and amputations are serious complications linked to diabetes and have an effect on the individual and also on society. 32 The lifetime incidence of foot ulceration is 25% of those with diabetes.8,37 Callus formation is usually caused by shear forces between the footwear and the foot under the bony prominences where the pressure leads to breakdown of the skin. 16 Repetitive peak dynamic plantar pressures considerably increase the possibility of foot ulcers in patients with peripheral neuropathy. 31
Plantar pressure usually changes with different activities in healthy individuals without foot abnormalities. 21 Stair walking is a common activity that requires a higher demand than level walking. During stair descending, the reduction of peak plantar pressure occurs from the hindfoot compared with level walking. However, incline walking increases the forefoot plantar pressure but reduces the hindfoot plantar pressure.12,30 Level walking may not reflect plantar pressure during other walking activities, especially in patients with gait impairments.5,22 Plantar pressure measurements give important information for the design of an insole that can reduce the peak plantar pressure. 33 In a clinical setup, diabetic patients are provided with a customized total contact orthosis (TCO).3,23 The effectiveness of a TCO is based on the reduction of the peak plantar pressure during different walking activities from the sites where a high rate of ulceration and reulceration occurs.7,16,30
It was reported that high plantar pressure can be minimized through the use of a TCO in combination with stable shoes. 10 Several studies compared the load distribution of a custom-made insole with a prefabricated insole. The custom-made insole was considerably better compared with the prefabricated insole in terms of plantar pressure distribution and contact area. 25 We found very few studies that investigated the effectiveness of a TCO in diabetic patients. There is still limited information regarding different walking activities and the effectiveness of a TCO in the diabetic population.
With an understanding of a specific activity that results in higher plantar pressure and the regions of the foot where high plantar pressure occurs, the load distribution can be managed effectively through a TCO. A positive approach toward management of diabetic foot ulceration through a TCO by understanding the activities can reduce the number of foot complications and lower limb amputations. The aim of this study was to investigate the plantar pressure at 4 regions of the foot during different walking activities (level walking, ramp ascending, ramp descending, stair ascending, and stair descending) in diabetic neuropathic patients with and without a TCO.
Materials and Methods
Patient Recruitment
The sample size of 16 neuropathic diabetic patients was determined by the inference of means method (comparing two independent samples). The patients were informed of the details of the research after approval from the research ethics committee of the Faculty of Medicine (EC-58-161-20-2). All participants read and signed the informed consent. The inclusion criteria were age 40 to 60 years, type 2 diabetes, history of having calluses on the forefoot or hindfoot at the time of evaluation, having forefoot deformity (ie, hammer toes, mallet toes, or hallux valgus), blood pressure not exceeding 140/90 mm Hg, having insensate or diminished sensation noted with a 10-g monofilament, and able to walk independently at least 10 m at a self-selected speed. The patients were excluded if they had foot ulcerations, joint surgery of the lower limb or the presence of an unhealed open wound at the time of the experiment, a partial or total amputation, ischemic heart disease, or unable to understand instructions given during the study protocol.
TCO Fabrication
A certified prosthetist and orthotist took foam impressions of the feet of the patients to make positive plaster molds. The foam was compressed to capture the foot and medial longitudinal arch with the knee at 90 degrees and a neutral subtalar joint. The positive mold was modified according to the blueprint obtained from the standing subject bearing equal weight on both feet. The TCO was fabricated using multifoam as the top layer, Plastazote (Streifeneder ortho production GmbH, Emmering, Germany) as the second layer, and microcellular rubber as the final stabilizing layer. The TCO was then fitted inside the sport shoe with a 0.5-cm heel height. Similar shoes were given to each patient to minimize the experimental variation.
Plantar Pressure Assessment
Patients were asked to perform 3 walking activities: level walking for 10 m, walking on an inclined surface (8.34 degrees) for 4 m, and 10 steps (step height 17.5 cm and 29 cm in depth) of stair walking. Two conditions were set up: the control condition without the TCO and with the TCO. Three rounds of each walking activity were performed without the use of a walking aid or handrail. Patients had 10 minutes to rest after each walking activity. The plantar pressure was recorded using the Pedar-X system (Novel GmbH, Munich, Germany), which was composed of 2.6-mm-thick insoles (size W = Asian shoe size 26-26.5 and size X = Asian shoe size 27-27.5) and the Pedar A/D converter. Each of the Pedar insoles was calibrated to zero before starting the experiment by asking the patients to stand on the left leg first and followed by standing on the right leg for 6 to 9 seconds for each leg. Then the patients were asked to walk for a round to get familiar with the TCO and Pedar insoles before recording the data. We defined the foot into 4 regions: toes, forefoot, midfoot, and hindfoot (Figure 1). The Pedar-X system had an inbuilt threshold of 15 kPa that resulted in a cutoff value in pressure recording to reduce the noise while recording the in-shoe data. Appropriately sized Pedar insoles were placed in each shoe of the patients and the data were sampled at 100 Hz.
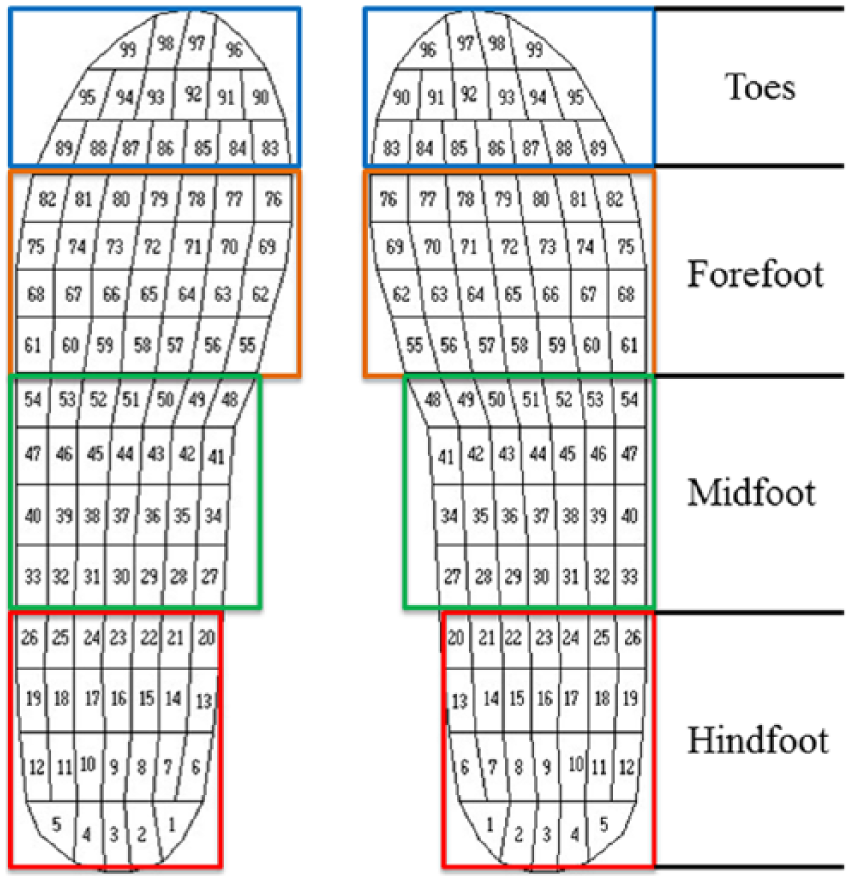
Regions of the foot.
Data and Statistical Analysis
The plantar pressure and contact area were obtained from the Novel Database Essential software version 12.3 (Novel GmbH, Munich, Germany). Furthermore, the force-time integral (area under the curve) was analyzed using our in-house computer algorithm. The descriptive statistics of data were presented as mean and standard deviation. The statistical analysis was done using Prism 5.0 Windows version (GraphPad Software, San Diego, California, USA). The paired t test was used to assess the plantar pressure and derived parameters between the control condition and with the TCO. The statistical significance for the test was set at P < .05. Furthermore, we calculated a Cohen’s d effect size to confirm the magnitude of differences between the conditions. 9
Results
The demographic data of the patients are shown in Table 1. The body mass index indicated that our patients were in a range of overweight. The patients had a long mean duration of diabetes (8.37 ± 4.50 years), and some patients had a big toe callus, metatarsal head (forefoot) callus, or hallux valgus deformity. All patients performed completely the 3 walking tasks without pause.
Demographic Data of Patients.
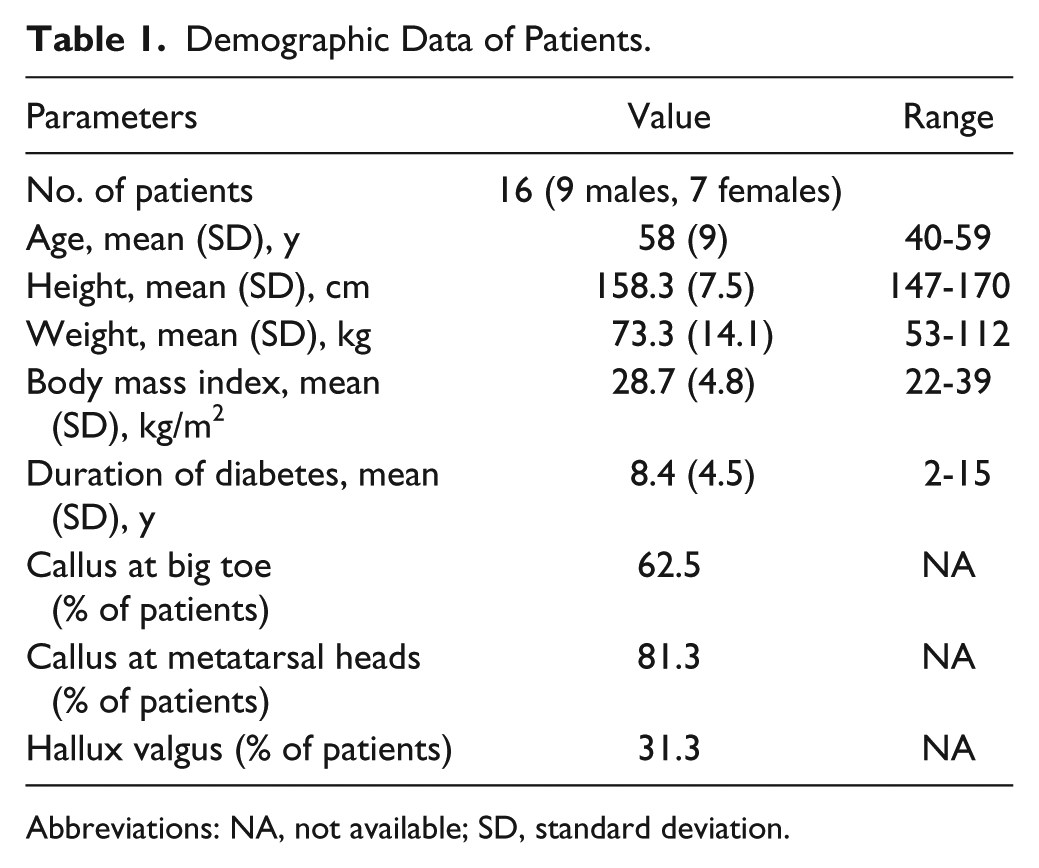
Abbreviations: NA, not available; SD, standard deviation.
Figure 2 presents the peak plantar pressure during different walking activities in the control condition and with the TCO. During level walking with the TCO, the peak plantar pressures in the forefoot and toe regions were significantly reduced about 26% and 24%, respectively, compared with the control condition (P < .01) (Figure 2A). During ramp ascending and ramp descending with the TCO, there were significant differences for the toes and forefoot regions (P < .01 and P < .001) (Figure 2B,C). The same results were found while wearing the TCO for stair ascending and stair descending (P < .01 and P < .001, respectively) (Figure 2D,E). Furthermore, in each walking activity, we found that wearing the TCO significantly increased peak plantar pressure at the midfoot compared with a control condition (P < .05 and P < .001). Table 2 shows the Cohen’s d effect sizes and the t test P values of peak plantar pressure differences between 2 conditions in 4 regions of the foot in each activity. The effect sizes were medium to very large for 3 regions of the foot (toes, forefoot, and midfoot). The t test of these 3 regions showed a significant difference in each walking activity.
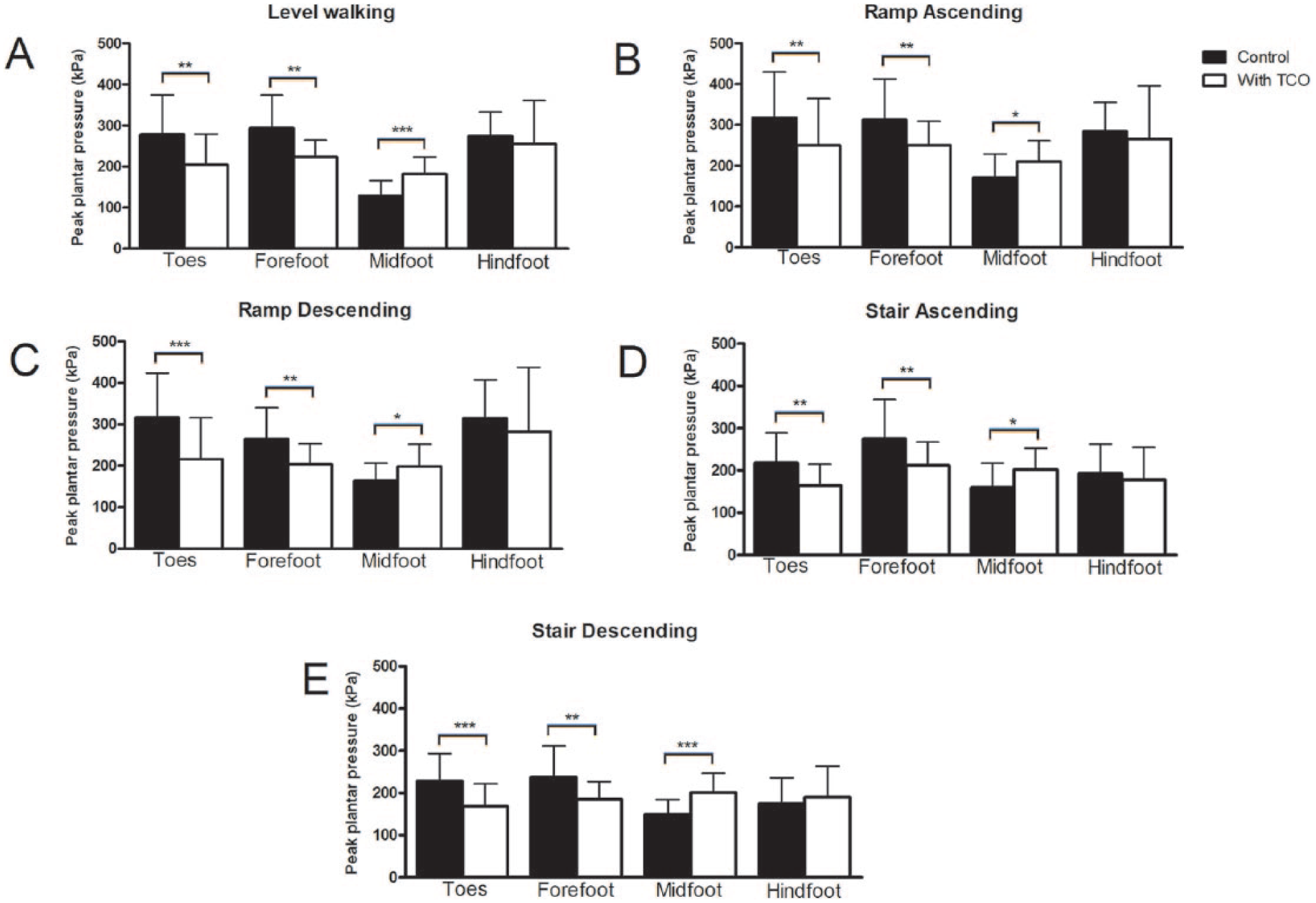
Peak plantar pressure during different walking activities in 2 conditions with the total contact orthosis (TCO) and without the TCO (control) of 4 foot regions: toes, forefoot, midfoot, and hindfoot. Significant differences between conditions are displayed with *P < .05, **P < .01, and ***P < .001.
Cohen’s d Effect Sizes and t Test P Values of the Peak Plantar Pressure Differences Between Two Conditions: With the TCO and Without the TCO (Control) During LW, RA, RD, SA, and SD for 4 Foot Regions.
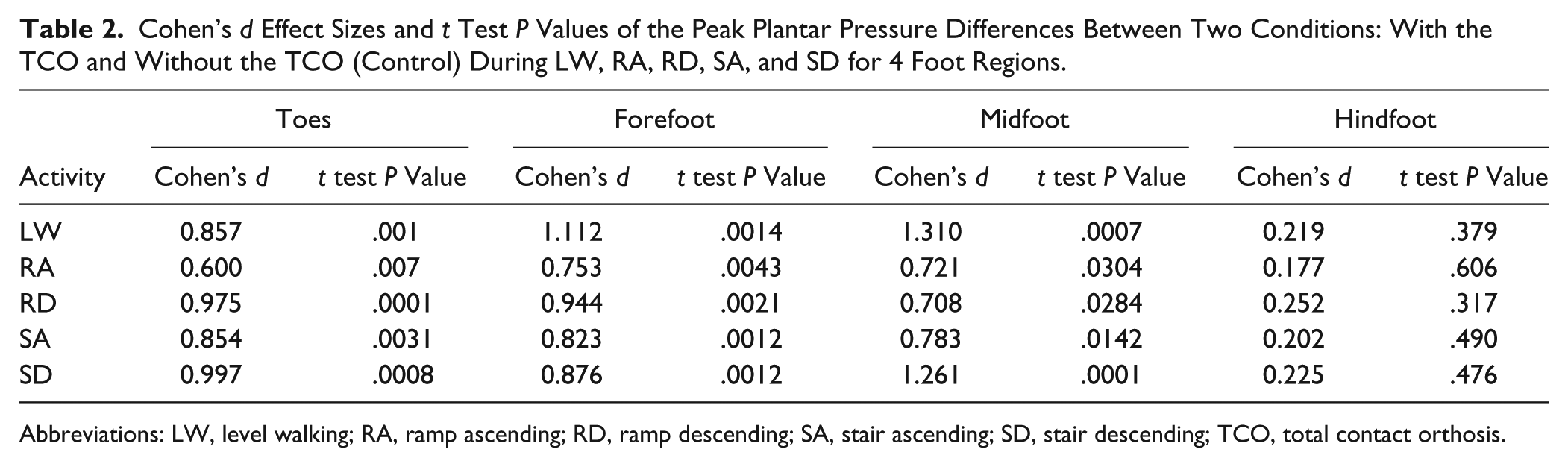
Abbreviations: LW, level walking; RA, ramp ascending; RD, ramp descending; SA, stair ascending; SD, stair descending; TCO, total contact orthosis.
Plantar pressures in each region for 3 walking activities are shown in Figure 3. For the control condition in the toes region, it was revealed that both ascending and descending ramp walking had a peak plantar pressure higher than other walking activities (Figure 3A). In the forefoot region, the peak plantar pressure in the control condition was highest during ramp ascending, whereas the peak plantar pressure was lowest in stair descending (Figure 3B). In the midfoot region, the peak plantar pressure during level walking was the lowest compared with other walking activities in both conditions (Figure 3C). In the hindfoot region for both conditions, ramp descending had the highest peak plantar pressure among the walking activities, whereas it was the lowest during stair walking (Figure 3D). Furthermore, it was noticed that stair walking had the lowest peak plantar pressure among the walking activities in the toes, forefoot, and hindfoot regions. Whether wearing the TCO or not, it showed a similar trend of peak plantar pressure in every region.
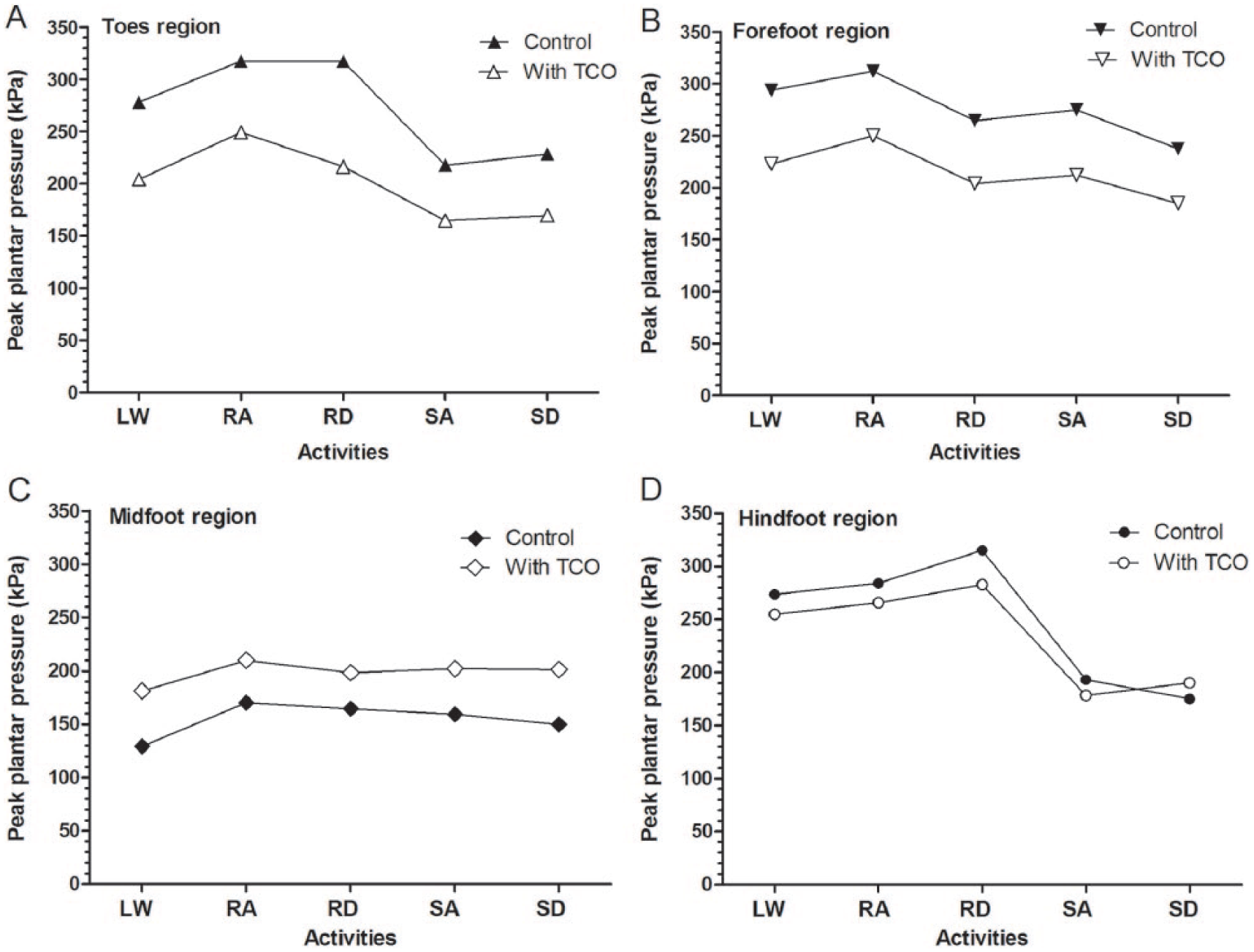
Plantar pressure during level walking (LW), ramp ascending (RA), ramp descending (RD), stair ascending (SA), and stair descending (SD) for 4 foot regions: (A) toes, (B) forefoot, (C) midfoot, and (D) hindfoot in 2 conditions: with total contact orthosis (TCO) and without TCO (control).
The force-time integrals in the control and with the TCO conditions during different activities are shown in Figure 4A. There were no significant differences while the patients walked with the TCO and without the TCO. The highest force-time integral was found during stair walking compared with other walking activities.
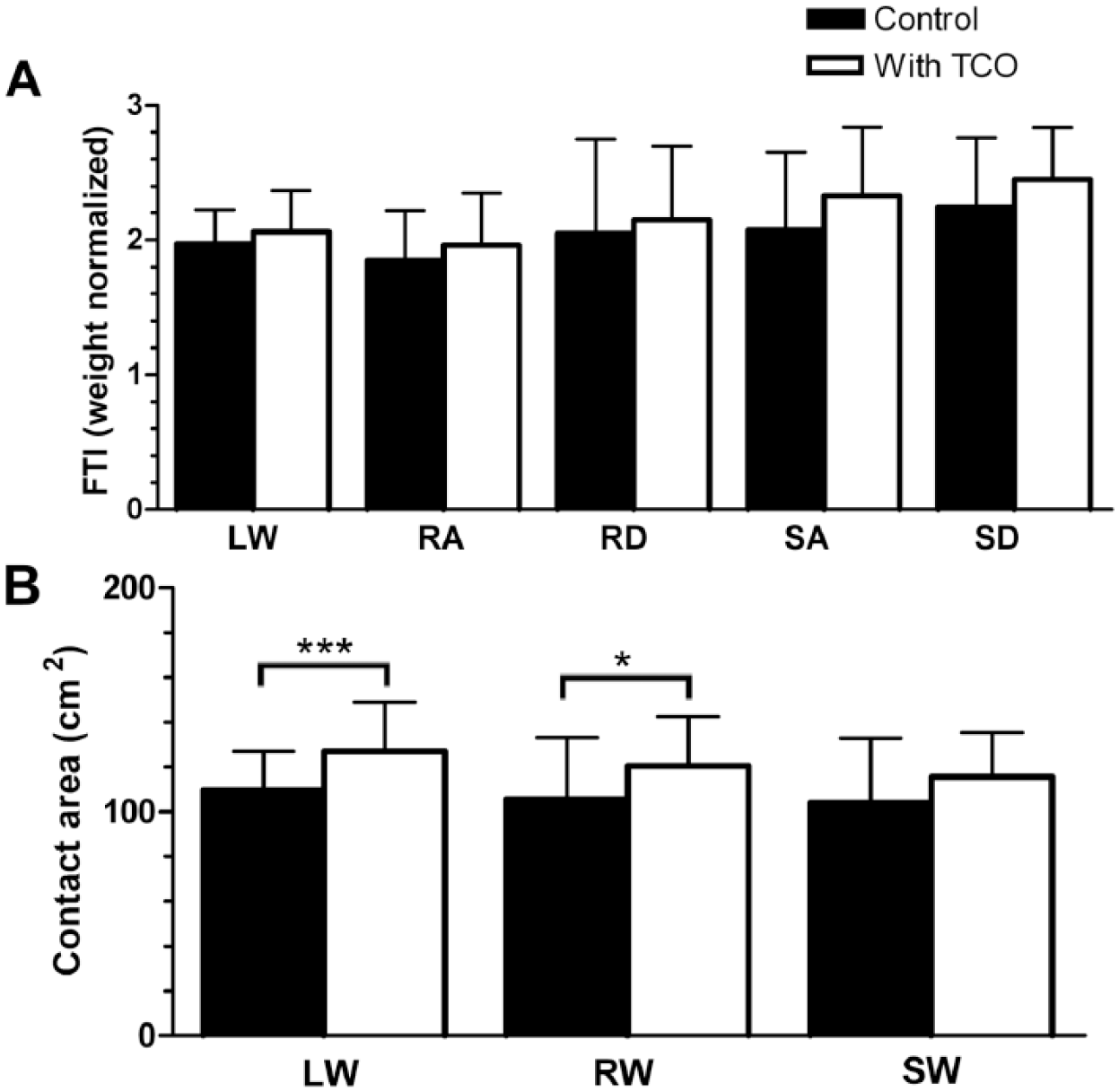
Force-time integral (FTI) during and contact area for level walking (LW), ramp walking (RW), ramp ascending (RA), ramp descending (RD), stair walking (SW), stair ascending (SA), and stair descending (SD) in 2 conditions: with total contact orthosis (TCO) and without TCO (control). Significant differences between conditions are displayed with *P < .05 and ***P < .001.
The contact area was highest for level walking, which was less during stair walking (Figure 4B). A significant difference in the contact area between the control condition and with the TCO was observed during level walking and ramp walking (P < .001 and P < .05), whereas the contact area also increased when wearing the TCO in other walking activities, but it was not statistically significantly different. Pressure mapping indicated there was a redistribution of peak plantar pressure and an increase in the contact area in each activity when using the TCO, as the examples show in Figure 5.
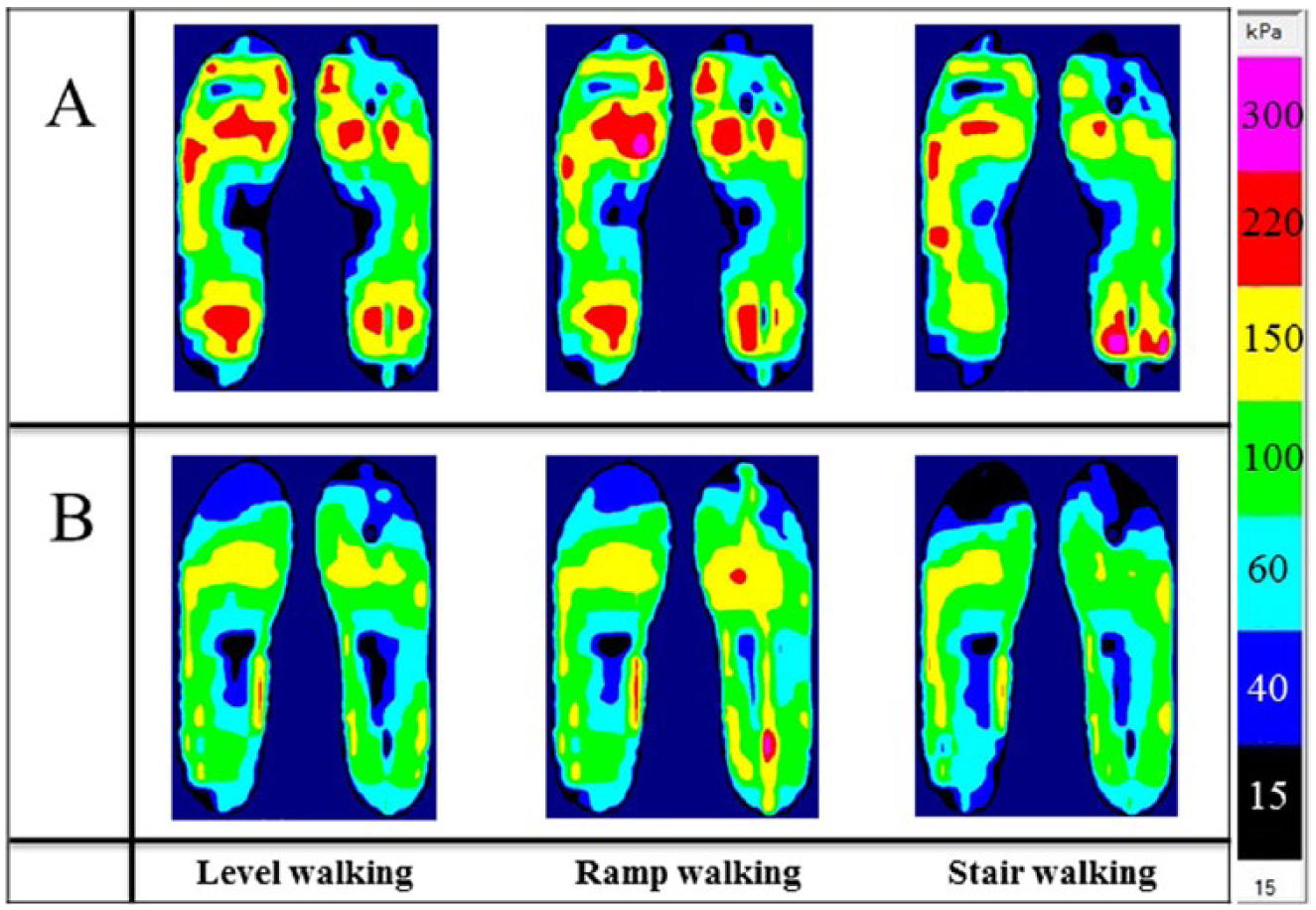
Pressure mapping during level walking, ramp walking and stair walking in a control condition (A) and with a total contact orthosis (B) from a single representative patient.
Discussion
Diabetic patients with neuropathy experience a higher plantar pressure compared with patients without a neuropathy and compared with healthy individuals.2,24,33 In this study, we found that the toes and forefoot regions had the highest peak plantar pressures during level walking and ramp walking in the control condition. When using the TCO, the peak plantar pressure in the toes region was reduced by 32% during ramp descending and by 24% during level walking. The midfoot region showed an increased peak plantar pressure with the TCO in every walking activity. However, the TCO reduced the peak plantar pressure at the heel region during ramp descending by 10%. These findings provided quantitative assessment results for plantar pressure reduction using the TCO.
During normal gait, the foot acts as a flexible body during initial contact for shock absorption and then acts as a rigid body to propel the body forward. However, the pathological feet with hallux valgus tend to disturb the forward propulsion of the body during the terminal stance phase of the gait cycle, which results in a high peak plantar pressure at the big toe and metatarsal heads. Therefore, using the TCO in that case can be beneficial because our study clearly showed that the TCO could significantly reduce plantar pressure in the toes and forefoot regions in level walking.
As shown in our study, it was expected that different walking activities resulted in a variation of peak plantar pressure in each foot region. During level walking and ramp walking, toes and forefoot regions had higher plantar pressure for both control and with TCO conditions, which is in concordance with previous investigations.14,21 Furthermore, our study showed that level walking in the control condition had a higher peak plantar pressure than stair ascending and stair descending in the toes, forefoot, and hindfoot regions, but Rao and Carter 29 reported that level walking in healthy adult women had higher peak pressures in all regions, including the midfoot. Ramp ascending increased forefoot peak plantar pressure and was reduced at the hindfoot in healthy individuals, whereas the opposite effect was observed during ramp descending. 13 Our results showed a similar trend while walking without the TCO with diabetes. Peak plantar pressure at the hindfoot region during level walking, stair ascending, and stair descending was reduced compared with ramp descending where the peak plantar pressure was the highest in healthy individuals.17,20,27 We obtained similar results for peak plantar pressure in diabetic patients.
The custom-made orthoses can redistribute the plantar pressure by maximizing the total contact area, and they are more effective than shoes only. Other studies reported that the peak plantar pressure could be reduced by 30% to 40% using the TCO with an increased contact area of the whole foot.3,18,19 The arch support and metatarsal pads in combination shift the pressure from hindfoot and forefoot to midfoot and prevent the foot from pronation.7,15,26 In our study, we also found that peak plantar pressure increased in the midfoot region, whereas the peak plantar pressure in other regions was reduced when using the TCO during all walking activities.
Our results indicate that the TCO allowed a significant increase in the contact area and redistribution of the peak plantar pressure from the metatarsal heads to the metatarsal shaft that provided support at the medial arch of the foot during all activities performed from 4 regions of the foot. The present study also contributes toward the proper management of diabetic foot ulceration.
There are several limitations in our study. We focused only on the initial stage of diabetic foot with no ulceration, which might not completely represent the diabetic foot conditions. Only 4 regions of the foot could be masked due to the available version of the software. Therefore, we could not determine plantar pressure on the lateral and medial sides of the midfoot region. The TCOs were fabricated from materials available in our prosthetics and orthotics unit. The walking activities in this study were representative of activities but may not represent the situations that the patients encounter in their daily lives. Furthermore, customized casting conditions could affect the TCO fabrication and the pattern of pressure redistribution.
Conclusion
Using a TCO in diabetic, neuropathic patients reduced and redistributed plantar pressures from the toes and forefoot to the metatarsal shafts and midfoot during walking activities. Ramp walking resulted in higher peak pressures than in other walking activities in both the control condition and with the TCO. Further studies that focus on the later stages of diabetic neuropathy, other daily activities, and the offloading effectiveness of a TCO are necessary for the design and fabrication of TCOs.
Footnotes
Acknowledgements
We thank the primary care unit (PCU of Songklanagarind Hospital) for providing the patients after initial screening and also to the volunteers who willingly participated in our study. We also acknowledge the Prosthetics and Orthotics Unit of Songklanagarind Hospital for allowing us to use the fabrication facilities and Ms. Tuanjit Na Rungsri and Ms. Suwicha Techapoowapat for very useful advice on the fabrication of the TCO. We thank our research assistants, Mr. Manatsunai Kuna, Ms. Atitaya Sookkasem, and Ms. Sirinthon Nunthong, for their contributions on the experiments. Last, we thank Mr. Glenn Shingledecker for English editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Graduate School of Prince of Songkla University. The Faculty of Medicine, Prince of Songkla University EC-58-161-20-2.