
Abstract
Background:
The management of pain in patients with foot and ankle pathology can be challenging. Cumulative data suggest that, in addition to nociceptive mechanisms, other neuropathic mechanisms can contribute to pain in a subset of people with orthopedic conditions, and can be found in 10.5% to 53% of patients with chronic pain, depending on the location of the pathology. Preoperative diagnosis of neuropathic pain (NP) can potentially change decision making and management of foot and ankle pathologies.
Methods:
We used a validated patient-reported pain questionnaire (painDETECT) as a cross-sectional study to investigate the prevalence of NP symptoms in a population of patients undergoing foot and ankle surgery. A total of 533 patients were prospectively included and completed the painDETECT questionnaire.
Results:
Sixty-six patients (12.4%) were classified as having a component of NP symptoms according to their painDETECT score. Current smokers (23.2%) had a significantly higher rate of developing NP symptoms than current nonsmokers (11.1%) (P = .016). The location of the pathology and obesity had a moderate effect on the prevalence of NP symptoms. Patients with ankle-level pathology, excluding tarsal tunnel syndrome, had a marginally increased risk of having NP symptoms (15.4%) compared to patients with forefoot pathologies, excluding Morton’s neuroma (7.5%, P = 0.06). Obesity also had a moderate effect on the NP risk, with 15.6% risk of NP symptoms for patients with BMI of 30 or more compared to 10% risk for patients with a BMI of less than 30 (P = .06). Patients with NP symptoms reported significantly higher levels of current pain (7.2 vs 4.6, P < .001).
Conclusion:
A considerable number of patients with foot and ankle problems requiring surgery had a neuropathic component of pain. Evaluation of their risk factors and level of pain may help with the diagnosis, decision making, and pain control. Further research is needed to evaluate the effect of preoperative NP on the short- and long-term results of surgeries.
Level of Evidence:
Level II, prospective cohort survey study.
Introduction
The management of pain in patients with foot and ankle pathology can be challenging. Cumulative data suggest that in addition to nociceptive mechanisms, other neuropathic mechanisms can contribute to pain in a subset of people with osteoarthritis.11,12,20
Clinically, nociceptive pain evoked during moving or loading of a joint, or in certain activities, that may develop eventually into pain at rest or at night and even may progress, in certain individuals, to a referred pain, hyperalgesia and allodynia. Neuropathic pain (NP) is that pain which is not mechanical and has the features of nerve irritation. Neuropathic mechanism includes peripheral sensitization, central sensitization, reduced descending inhibition, and atrophy of cortical areas. 4
These mechanisms can develop due to direct irritation or injury to the peripheral nerve itself or through chronic sensitization and nerve modulation. Heterogeneous pain mechanisms may explain variable responses to recommended pain therapies.
A recent general-population health survey done in the United States found that as high as 15.7% of the patients reporting to have pain and 10% of all the responders had a probable NP with a higher tendency in certain ethnic groups (blacks and Hispanic). 2 The study of NP in orthopedic conditions has started with focusing mainly in osteoarthrosis (OA) of the knee1,5,7,14,16 and spinal pathologies15,23 but has now progressed to evaluate the prevalence and the implications of NP in other common orthopedic conditions including hip lesions, 13 rotator cuff tear, 9 carpal tunnel syndrome, 18 etc. These studies have found up to 34% of the patients with knee OA have NP, 10.5% of the patients with carpal tunnel syndrome, 15.8% with rotator cuff tears, and as high as 53% of patients with chronic back pain. A recent study found a prevalence of 23% of NP following open reduction internal fixation (ORIF) of ankle fractures. 17 Furthermore, it was shown the patients with NP had inferior results following total knee arthroplasty (TKA), with significantly higher visual analog scale (VAS) pain scores and lower pain detection thresholds, 10 though another study with similar inferior results for patients with NP found that the presence of preoperative NP did not predict higher pain scores postoperatively. 5
Accurate classification of pain phenotype using clinically feasible tools has the potential to improve pain management. The painDETECT score is one of several methods to clinically diagnose NP. 6 It is a patient-report questionnaire that was developed to identify NP and validated for the use in patients with back pain. The painDETECT was later used in several other pain locations including the hip, 13 knee, 14 and wrist. 18 It was also translated to more than 23 languages and was validated for these versions for general use and not specifically for back pain. 21 A modified painDETECT version for the use of knee pain was validated by Hochman et al.7,8 The purpose of this study is to examine the prevalence of neuropathic pain symptoms in patients presenting for foot and ankle surgery and identify certain conditions with highly reported frequencies of NP.
Methods
This was a cross-sectional study investigating the prevalence of NP symptoms in a population of patients undergoing foot and ankle surgery at a private, multicenter institution in an urban/suburban location. All patients presenting at their preoperative visit prior to foot and ankle surgery with one of our institution’s fellowship-trained foot and ankle surgeons were prospectively enrolled. The presence of preoperative NP symptoms was assessed using the English version of the original painDETECT, patient-reported pain questionnaire, that was developed to identify NP. 6 Patient demographics, diagnosis, comorbidities, and functional scores were also prospectively collected. Patients with a nerve pain-related diagnosis (tarsal tunnel syndrome, neuromas) were excluded from the study.
The painDETECT questionnaire is composed of 9 questions contributing to a neuropathic pain score ranging from 0 to 38 (Table 1). A painDETECT score of 0-12 indicates “a neuropathic pain component is unlikely (less than 15%)”; a score of 13-18 indicates “ambiguous, however a neuropathic pain component can be present”; and a score of 19-38 indicates “a neuropathic component is likely (more than 90%).” For our study, a painDETECT score of less than 18 was considered “nociceptive” and a score of 18 or more was considered “neuropathic” (NP).
painDETECT Neuropathic Pain Screening Questionnaire.
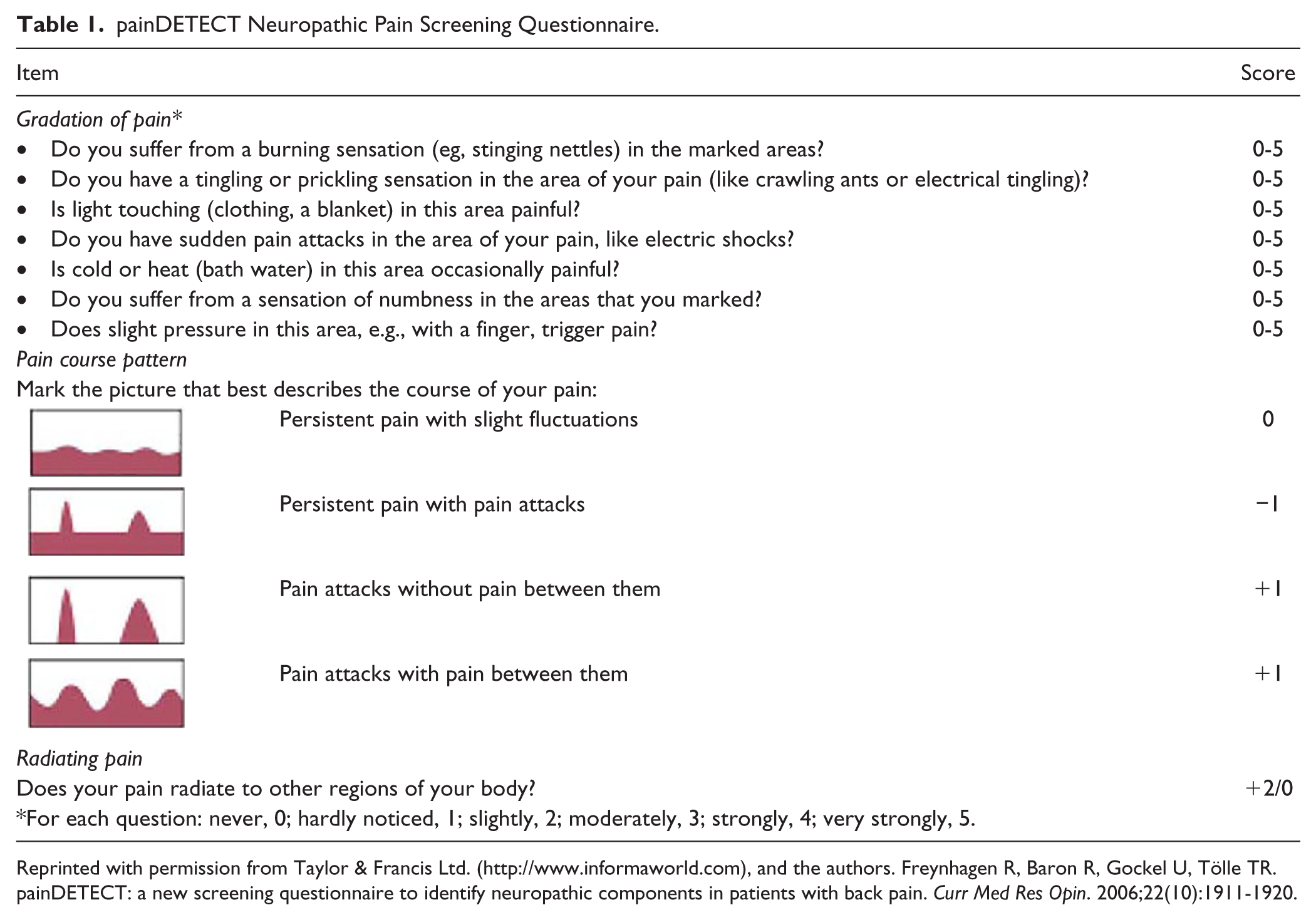
Reprinted with permission from Taylor & Francis Ltd. (http://www.informaworld.com), and the authors. Freynhagen R, Baron R, Gockel U, Tölle TR. painDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin. 2006;22(10):1911-1920.
Patients with and without NP symptoms were compared via Student t tests on continuous variables, such as the pain scores, age, and BMI. Categorical variables, such as the prevalence of NP symptoms among different foot and ankle procedures (bony vs soft tissue, elective vs trauma) and procedural regions (ankle, hindfoot, midfoot, forefoot) were compared via chi-square and Fisher exact tests. A multivariate logistic regression was used to identify significant factors associated with higher rates of NP symptoms. Receiver operating characteristic curves were generated to determine which reported level of current pain (0 to 10) was best at predicting which patients had components of neuropathic pain.
Results
Rather than testing for overall prevalence of NP symptoms in our population, we utilized an A-prior sample size calculation to appropriately power our study in order to detect NP symptoms by patient variables. This calculation determined we would need 506 patients to have just more than 80% power to detect a significant rate difference of 10% at P < .05 for any 2 conditions. A total of 533 patients were prospectively included in the present study and completed the painDETECT questionnaire. With this sample size, the current cross-sectional study has greater than 99% power to detect a neuropathic pain prevalence as low as 11%, the rate of NP symptoms detected in a previous study utilizing the painDETECT questionnaire, 16 and greater than 80% power to detect a significant rate difference of 10% at P <.05 for any 2 conditions. Sixty-six patients (12.4%) were classified as having a component of neuropathic pain according to their painDETECT score. Results are outlined in Table 2.
Neuropathic Pain According to Patients’ Demographics, Medical History, and Their Foot and Ankle Pathology. a
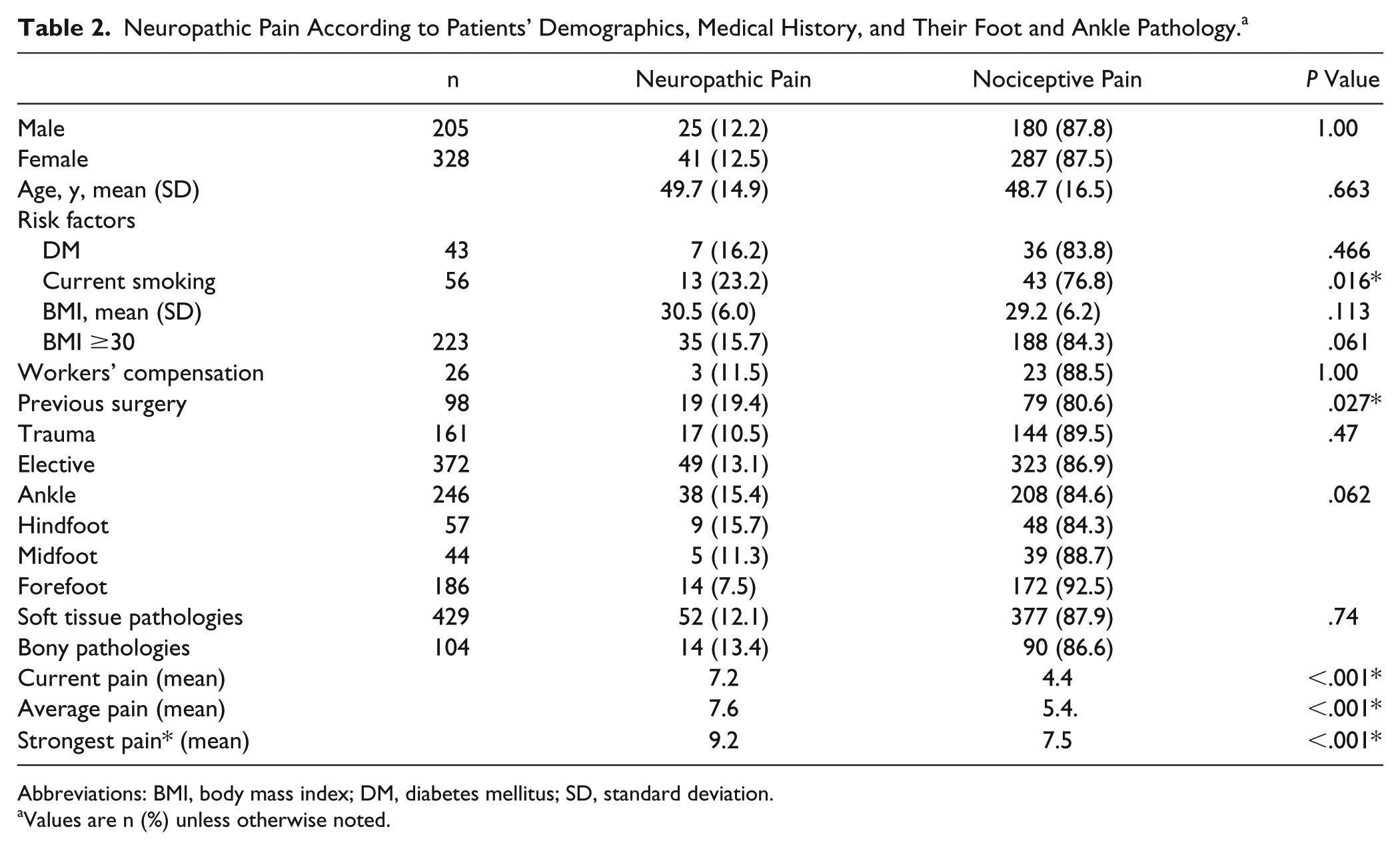
Abbreviations: BMI, body mass index; DM, diabetes mellitus; SD, standard deviation.
Values are n (%) unless otherwise noted.
There was no difference in the prevalence of NP symptoms relative to the age, sex, or specific diagnosis. Current smokers (23.2%) had significantly higher rate of developing NP symptoms than current nonsmokers (11.1%) (P = .016), whereas former smokers (12.0%) had the same risk as lifetime nonsmokers (10.8%). Patients with a prior history of foot and ankle surgery had nearly double the risk to have NP symptoms than patients without a history of surgery in the same foot (19.4% vs 10.8%, P = .027).
In regard to procedural region, patients with ankle-level pathology, excluding tarsal tunnel syndrome, had a marginally increased risk of having NP symptoms (15.4%) compared to patients with forefoot pathologies, excluding Morton neuroma (7.5%, P = .06). Patients scheduled for elective surgery trended to have an increased risk of having NP symptoms compared to patients scheduled for trauma surgery, but the difference did not meet the criteria for statistical significance (13.2% vs 10.5%, P = .062).
Obesity also had a moderate effect on the NP risk, with 15.6% risk of NP symptoms for patients with BMI of 30 or more compared to 10% risk for patients with a BMI of less than 30 (P = .06). Interestingly, diabetes mellitus (DM) showed no effect on the risk for NP, with 16% of DM patients having NP symptoms and 12.0% of non-DM patients having NP symptoms. Patients being treated for a workers’ compensation (WC)-related problem also had no effect on the rate of NP symptoms, with 11.5% of WC patients having NP symptoms compared to 12.4% of non-WC patients.
Bivariate logistic regressions identified BMI of 30 or more (P = .011), current smokers (P = .011), previous foot and ankle surgery (P = .022), and ankle-level pathology (P = .014) as being significant predictors of having increased rates of NP symptoms. A multivariate logistic regression incorporating these significant factors identified current smokers (odds ratio [OR] =2.10, P = .043), previous foot and ankle surgery (OR=1.84, P = .046), and ankle-level pathology (OR=1.99, P = .041) all as having higher odds of having NP symptoms.
As an additional part of the painDETECT survey, patients with NP symptoms reported significantly higher levels of current pain (7.2 vs 4.6, P < .001) and average pain level in the past 4 weeks (7.6 vs 5.4, P < .001). A cut-off value current pain score of 7 and higher for patient-reported current pain was the best at predicting patients with NP symptoms according to receiver operating characteristic curve analysis, with a sensitivity of 70.3% and specificity of 75.1%.
Discussion
In this study, we prospectively collected data assessing the presence of NP symptoms in patients with foot and ankle pathologies. The overall rate of NP symptoms was lower than previously published for hip, 1 knee,8,14,16 and lower back, 15 and similar to other reports of NP in carpal tunnel 18 and rotator cuff 9 pathologies. We did find a much lower rate of NP symptoms compared to a recent study following ORIF of ankle fracture. 17 However, after delineating our finding according to reason for surgery, we found a similar rate for patients with a history of foot/ankle surgery, who had double the NP symptoms rate compared to native feet and ankles.
The location of the pathology also seems to have an effect on the rate of NP symptoms. Looking at the previous reports, and according to our findings as well, the more proximal the pathology, the higher the rates of NP symptoms. As mentioned earlier, the rates of NP in patients with lower back pain was as high as 53%, 34% for knee osteoarthritis, and 12.4% in our study. Even within the foot and ankle region, the rate of NP in the ankle and hindfoot regions was higher than the midfoot and forefoot (15.5%, 11.4%, and 7.5% for combined ankle/hindfoot, midfoot, and forefoot, respectively). We did not find an explanation for this finding, though we think it is part of the peripheral sensitization mechanism and the fact that the more proximal the location of the pathology, the more nerves cross the area and can be sensitized.
Regarding the effect of preoperative NP on postoperative function and pain, there is only limited data. A recent prospective study of 50 patients undergoing total knee arthroplasty found a higher level of short-term, postoperative pain in the patients with the presence of preoperative NP symptoms. 10 Similar results were found in another prospective study following total knee arthroplasty. 5
The results of our study suggest that a significant amount of foot and ankle patients, both for acute injuries and chronic conditions, have NP symptoms. The implication of that on their results is yet to be evaluated. Nevertheless, according to our study, a current pain level of VAS higher than 7 should alert the physician to check for NP.
We additionally found risk factors for NP symptoms like obesity, smoking, pathologies in the ankle level, and prior surgery. A higher VAS score in the NP patients was ubiquitous in most of the studies we reviewed. A higher BMI was found in other studies in the patients with NP. 1 Ko et al found smoking to be related to NP. 9 Although diabetes itself is a risk factor for development of peripheral neuropathy in about 50% of the patients with diabetes and up to 26% for painful peripheral neuropathy, 19 we did not find higher prevalence of NP symptoms in this group of patients. This finding can be explained to some degree by our patient selection and management of patients with uncontrolled diabetes or documented neuropathy.3,22
Conclusions
A considerable number of patients with foot and ankle problems requiring surgery had a neuropathic component of pain. We believe this should be evaluated preoperatively and taken into account when deciding on an operative intervention and pain management before and after the operation. We found risk factors and variables related to NP symptoms, some of which are reversible, like smoking and obesity, and some of which are related to the centrality of the pathology or the presenting level of pain. We believe that the painDETECT is a good research tool, but reviewing with every patient for the presence of allodynia, dysesthesia, rest pain, or radiating pain should be enough and is a good clinical practice. Further research is yet to be done to evaluate the effect of preoperative NP symptoms on the short- and long-term results of surgeries.
Supplemental Material
FAI838302-ICMJE – Supplemental material for Prevalence of Neuropathic Pain Symptoms in Foot and Ankle Patients
Supplemental material, FAI838302-ICMJE for Prevalence of Neuropathic Pain Symptoms in Foot and Ankle Patients by Eliezer Sidon, Ryan Rogero, Elizabeth McDonald, Annemarie Daecher, Rachel Shakked, David I. Pedowitz, Daniel Fuchs, Joseph N. Daniel and Steven M. Raikin in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.