
Abstract
Background:
Isolated ankle syndesmosis disruption (without fibula fracture) causes acute pain and may cause chronic instability and pain. The aim of the present study was to evaluate the outcomes after anterior inferior tibiofibular ligament (AITFL) anatomical fixation using anchor sutures for unstable isolated syndesmosis disruption without fibular fractures.
Methods:
This study assessed 22 athletes who were diagnosed with unstable isolated syndesmosis disruption with a positive external rotation test, had more than 2-mm diastasis on ultrasound, and had complete AITFL rupture on magnetic resonance imaging between 2004 and 2020. Eighteen patients (82%) were elite-level athletes, and the remaining 4 were recreational athletes. Twelve patients (55%) were injured by an external rotation force. The athletes underwent open anatomical suture anchor fixation between the AITFL attachment sites, the fibula and tibia. The mechanism of injury, return-to-play time, and Foot and Ankle Outcome Score (FAOS) were evaluated.
Results:
All athletes returned to previous play except 1 retired elite athlete. Twenty-two athletes returned to jogging, team training, and official game play at an average of 62, 89, and 102 days, respectively. The final average follow-up FAOS symptom, pain, daily activity, sports activity, and quality of life scores were 98, 97, 100, 99, and 97, respectively. Two athletes were reinjured, and 1 required reoperation in the follow-up period.
Conclusion:
Athletes with isolated syndesmosis disruption had a high likelihood to return to their previous activity level after suture anchor augmentation.
Level of Evidence:
Level IV, case series.
Introduction
Ankle syndesmosis injuries can be categorized as either (1) ankle fracture dislocation with syndesmosis disruption, such as with Maisonneuve fractures, external rotation-type fibular fractures, or posterior malleolar fractures, or (2) syndesmotic ligamentous disruption without fractures. Syndesmotic ligamentous disruption without fracture is disruption of the anterior inferior tibiofibular ligament (AITFL) without fracture and has been termed “high ankle sprain” or “isolated syndesmotic injury” to distinguish it from the more common lateral ankle sprain or medial deltoid ligament sprain. In athletes, syndesmotic injury is very common, accounting for 7% to 25% of acute ankle sprains.2,5,7,25 Although isolated syndesmosis injury can produce instability, radiography can be normal, making diagnosis of syndesmotic injury in these cases very challenging. Therefore, dynamic and functional assessment is important for the diagnosis of unstable syndesmosis injuries. The natural history of isolated syndesmosis injury treated nonoperatively involved a prolonged period of pain, precluding return to sports (~3 months), and an unknown rate of chronic disabling syndesmosis instability. Recently, acute surgical repair of the torn ligament with suture and suture anchors has been reported in an attempt to shorten time to return to play (RTP), which is double that of lateral ankle injuries, and reduce the rate of chronic syndesmosis instability. 3
As chronic syndesmosis problems may lead to significant functional deficit and osteoarthritic change, early diagnosis of unstable syndesmosis and appropriate treatment are very important. The classic syndesmotic fixation technique for unstable syndesmosis employs transsyndesmotic screws in a 1- or 2-screw technique. However, transsyndesmotic screw fixation has several disadvantages, such as screw removal, inaccurate reduction, limitation of physiologic syndesmosis motion, screw breakage, late syndesmotic diastasis after removal, and disused osteoporosis. To overcome these drawbacks, transsyndesmotic suture-button fixation, which does not require removal, appeared to be a good alternative. However, transsyndesmotic suture-button fixation alone did not provide adequate rotational stability for syndesmosis in a biomechanical study. 12 Thus, Shoji et al 19 recommended using additional suture tape augmentation along the AITFL plane.
Lee et al 12 proposed an endoscopic anatomical syndesmotic fixation technique that used suture tape and bioscrews from the anterior surface of the fibula to the distal surface of the distal tibia over the AITFL. This technique ensures direct anatomical fixation for “open book”–type anterior syndesmotic disruption. Moreover, Kim 9 reported more satisfactory outcomes for unstable syndesmosis disruption using AITFL fixation with knotted and knotless suture anchors than for transsyndesmotic screw fixation.
The aim of the present study was to evaluate the outcome of AITFL open anatomical suture anchor fixation for unstable isolated syndesmotic disruptions without fracture in athletes.
Methods
Patients
Ninety-four patients underwent anatomical syndesmosis suture anchor fixation of an unstable syndesmosis disruption after high ankle sprain at our institute from 2014 to 2020. Among those, patients who (1) were athletes; had (2) a positive external rotation test (squeeze test positive), (3) AITFL rupture and tibiofibular widening greater than 2 mm on ultrasonography, (4) positive jump or taping test (functional test), (5) confirmed complete rupture of AITFL on magnetic resonance imaging (MRI), and (6) tibiofibular diastasis greater than 4 mm on endoscopic or open assessment (obturator swing test positive); (7) underwent open anatomical fixation with suture anchors between the AITFL attachment sites of the fibula and tibia; and (8) had more than 1 year of follow-up were included in this retrospective study. After excluding patients who had (1) a history of previous ankle fracture or ankle operation, (2) underlying systemic pathology, (3) combined chronic ankle and syndesmotic instability, (4) combined posterior malleolar fracture, (5) combined foot fracture, and (6) tibiofibular diastasis less than 2 mm on endoscopic assessment (probe test positive, obturator swing test negative) 10 and (7) were nonathletes, 22 athletes were included in this study. There was no control group. Data were obtained from the medical records, radiograph findings, and evaluation results of patients. Indications for operation included unstable syndesmosis disruption on physical examination, ultrasound dynamic findings, and complete AITFL tear on MRI. The protocol for performing the operation is shown in Figure 1. All athletes underwent clinical and radiological follow-up at a mean of 18.0 months postoperatively. The study protocol was approved by our institutional review board (CMHCTC-19-003), and consent forms were obtained from all patients.
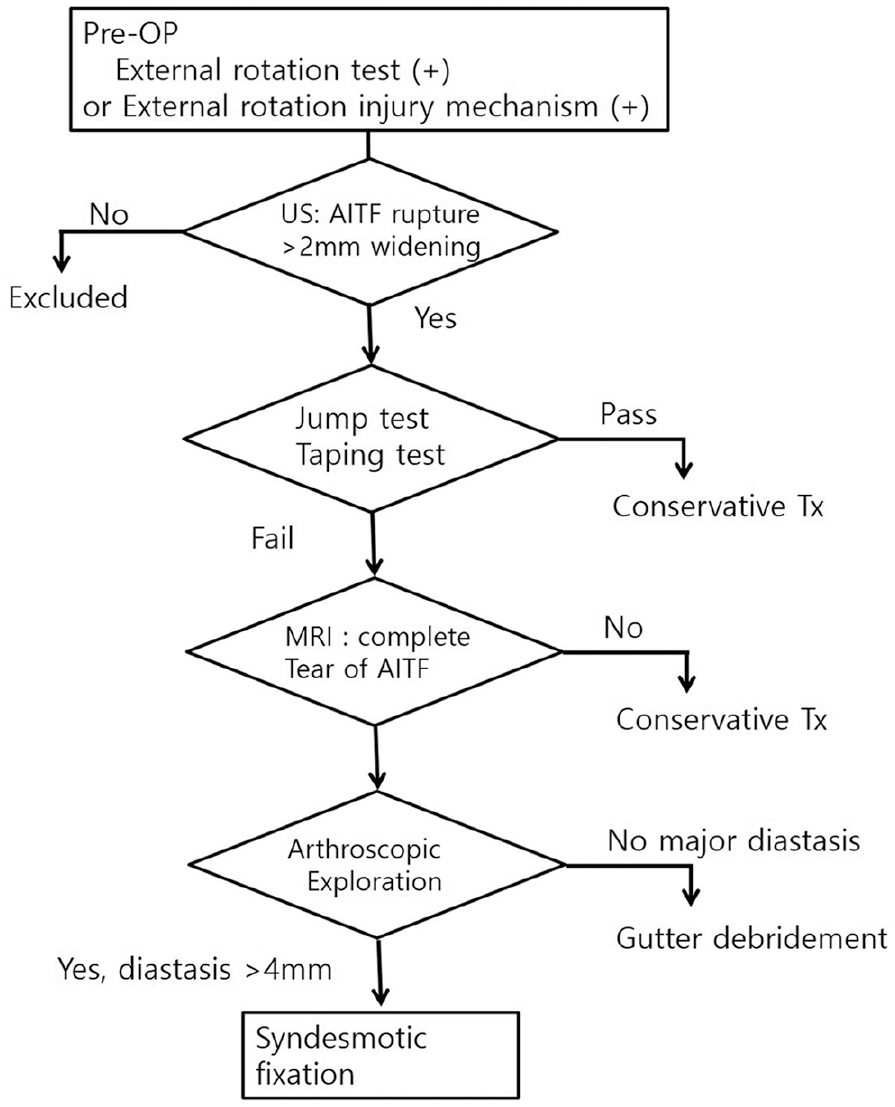
Operative decision-making protocol for isolated syndesmosis disruption. AITF, anterior inferior tibiofibular; Tx, treatment.
Preoperative Evaluation Tests
The external rotation test is the most valuable method for the diagnosis of syndesmosis disruption.13,17,23 With the knee in 90 degrees of flexion, the examiner applies an external rotation moment at the ankle, like the mechanism of injury. The squeeze test was performed by compressing the fibula to the tibia above the ankle joint. The inability of the patient to perform a double-leg jump over 30 cm is considered to indicate a positive functional test result. The “stabilization test” is performed by tightly taping the patient’s leg just above the ankle joint in an attempt to stabilize the syndesmosis. 23 If toe raises, walking, and/or jumping are less painful upon taping, the test is considered positive.
The syndesmosis disruptions were graded as West Point classification IIB (functional test positive, ultrasonography positive) or III (diagnosed definitely on radiography).3,5,8
Operation
Patients were placed in a semilateral position. A pneumatic tourniquet was applied at the thigh level to allow free examination of the syndesmotic stability. We evaluated the syndesmosis stability with arthroscopic exploration by an anteromedial and anterolateral portal. We placed a 2.9-mm obturator (component of the endoscope sheath) within the tibiofibular diastasis and swung it. Fixation was indicated for diastasis greater than 4 mm.
An anterolateral linear skin incision of approximately 4 cm was made at the distal tibiofibular joint. The superficial peroneal nerve was preserved, the distal transcrural fascia and anterolateral joint capsule were dissected, and the ruptured AITFL was exposed. Syndesmosis fixation was initiated when more than 4 mm of widening on the stress test showed positive results (can be omitted if it is confirmed by endoscopy). The ruptured AITFL remnant was preserved to maintain contact with both ends. A 3.0-mm suture anchor (BioComposite SutureTak; Arthrex, Naples, FL) was inserted into the fibular AITFL attachment site, and a retrieved No. 2 FiberWire suture was fixed with appropriate tension at the distal tibial attachment site in the anatomical direction of the AITFL using a 3.5 knotless anchor (BioComposite PushLock; Arthrex) (Figures 1 and 2). Stability was confirmed by the external rotation test and the postoperative wound was closed.
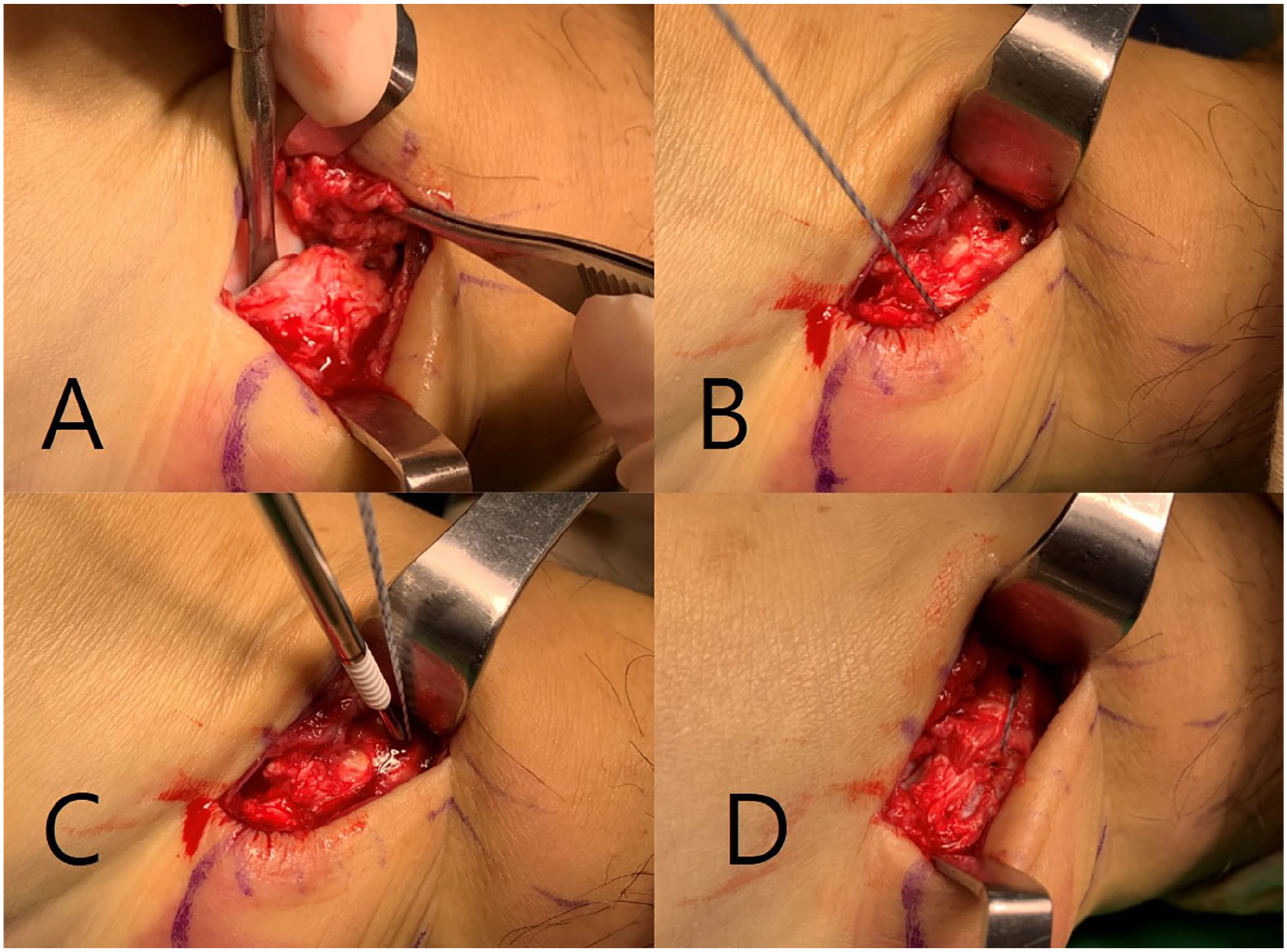
(A) We rechecked the intraoperative stability of injured syndesmosis. (B, C) We fixed the unstable syndesmosis with bone-to-bone anchoring using a suture anchor and knotless anchor along the anterior inferior tibiofibular ligament. (D) Final image of the anterior inferior tibiofibular ligament anatomical fixation using anchor sutures.
Postoperative Care
Postoperatively, the patients were immobilized with a posterior splint. After 2 weeks, the splint was changed to a short leg cast, and the patients were allowed weightbearing as tolerated. At 4 weeks, the cast was removed and changed to an air brace, and range of motion exercises with strengthening and proprioceptive training were initiated. In most cases, stability was evaluated using ultrasonography at 4 and 8 weeks. If athletes showed good stability on ultrasonography (tibiofibular distance within 1 mm), we permitted running. Full RTP progression was permitted according to each athlete’s individual progression. No removal procedures were required.
Clinical Assessment
A follow-up examination was conducted using the Foot and Ankle Outcome Score (FAOS), which includes scores for symptoms, pain, active daily living, sports activity, and quality of life. 18 RTP time was collected from the elite team trainer or by telephone survey of athletes. The definitions of RTP were as follows: “jogging,” athletes could perform high-intensity rehabilitation, including jogging, jump, and plyometric exercise; “team training,” athletes could participate in full RTP with their team; and “official match,” athletes could participate in a match against a competing team. In cases that lacked official games because it was the off-season, the official game day was considered a scrimmage game with an opposing team. Reinjury or postoperative complications were evaluated.
Statistical Analysis
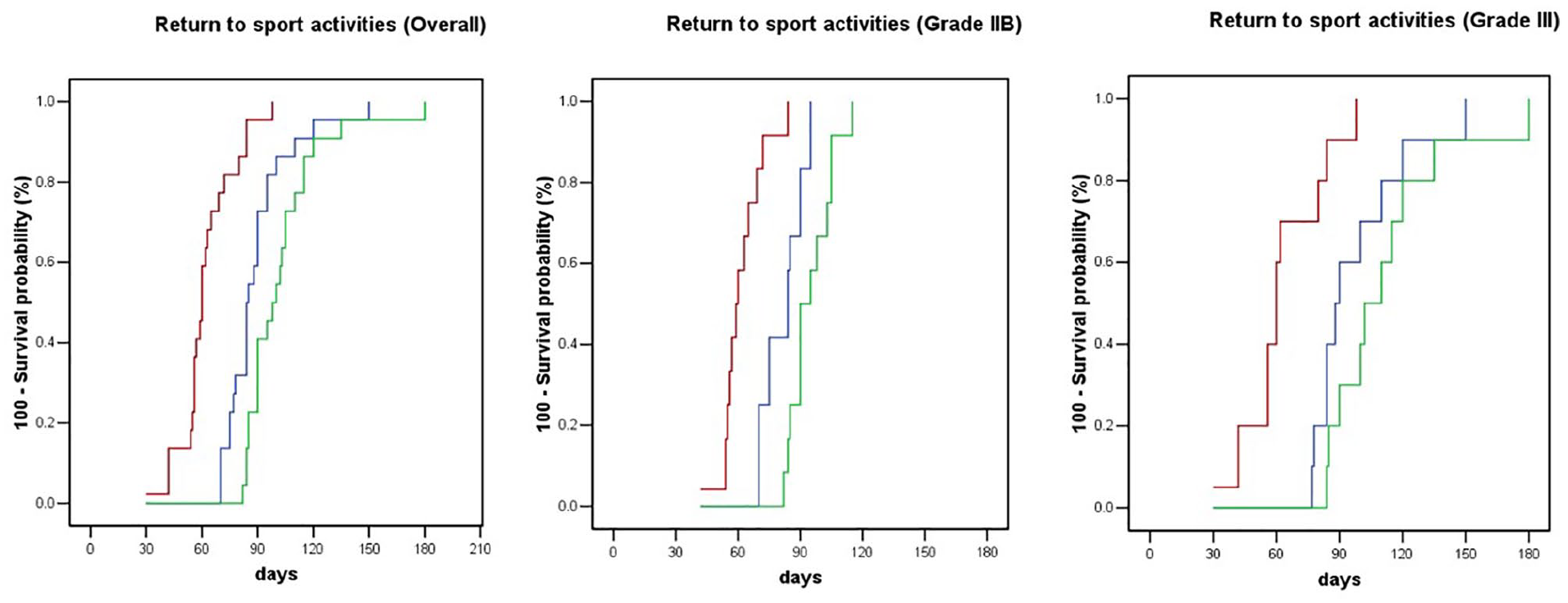
Statistical analysis was performed with SPSS version 18.0 (SPSS Inc, Chicago, IL). A Mann-Whitney U test was performed to compare the RTP times between West Point grades IIB and III and between athletes younger than and athletes older than 25 years of age. 4 Pearson’s correlation was performed to evaluate the correlation between age, weight, height, and RTP time. A Kaplan-Meier curve was calculated using 3 different RTP categories (jogging, team training, official match).
Results
A total of 22 eligible patients (20 males, 2 females) with a mean age of 23.2 (range, 15-43) years at the time of operation were enrolled (Table 1). All operations were performed within 2 weeks after the trauma day (average, 9 days: SD, 5.1 days). Of the 22 patients, 20 (91%) patients were elite-level professional athletes, while 2 (9%) were engaged in sports at a recreational level. The athletes’ sports included soccer (n = 20), basketball (n = 1), and handball (n = 1). The injury occurred because of an external rotation force in 12 (55%) athletes and extreme plantarflexion in 6 (27%) athletes. Other mechanisms were supination and eversion (Table 1). All athletes returned to play at their previous activity level. During the follow-up period, only 1 elite-level athlete retired due to older age even though he participated in an official game in the season. The average periods required to resume jogging, return to team training, and participate in official game play were 62.0, 89.3, and 102.9 days, respectively (Table 2). The final mean FAOS was 98.4, and mean scores for individual components were as follows: symptoms, 98.0; pain, 98.0; active daily living, 100.0; sports activity, 99.3; and quality of life, 97.1 (Table 2).
Patients’ Demographic Data. a
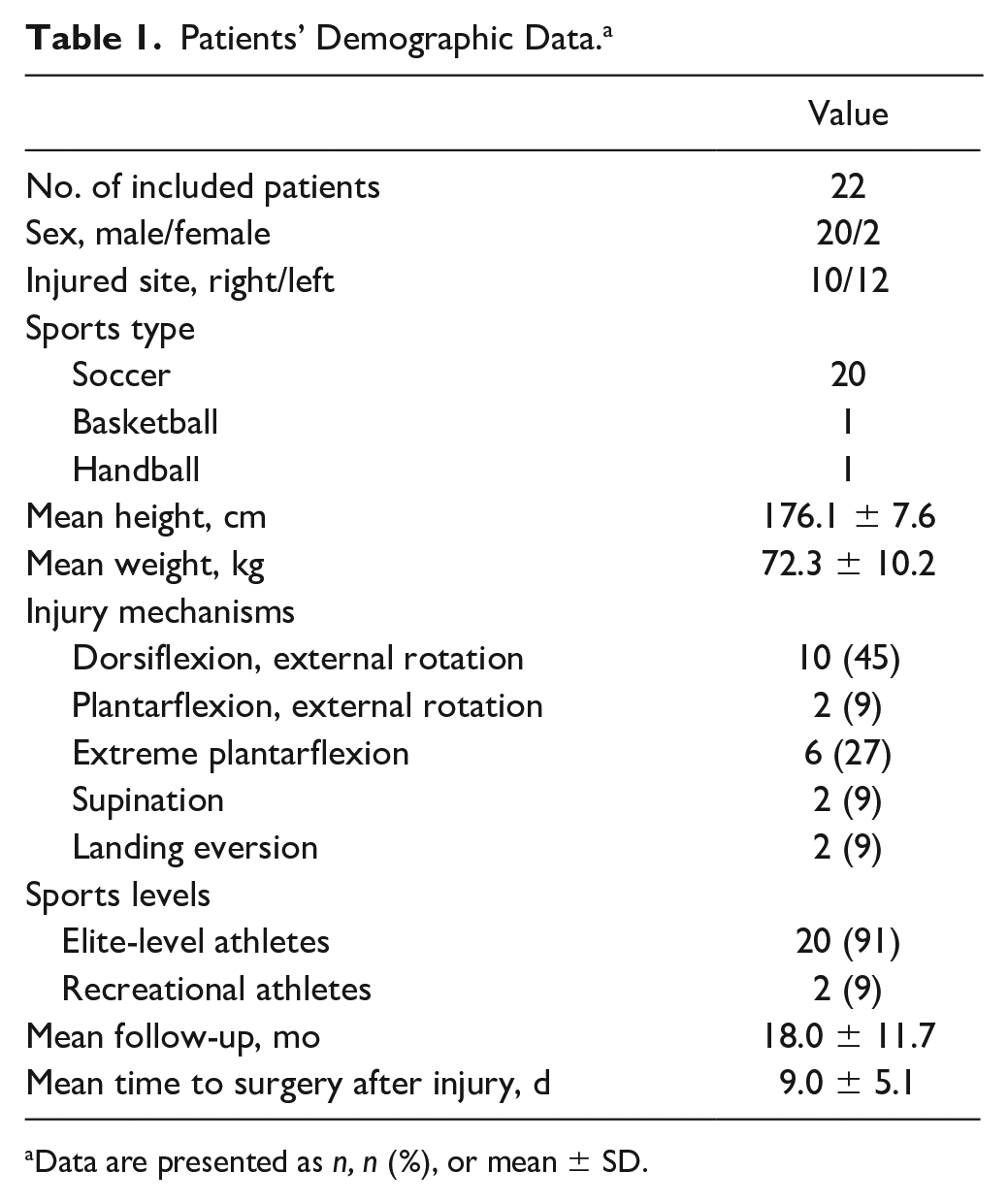
Data are presented as n, n (%), or mean ± SD.
Postoperative Clinical Assessment. a
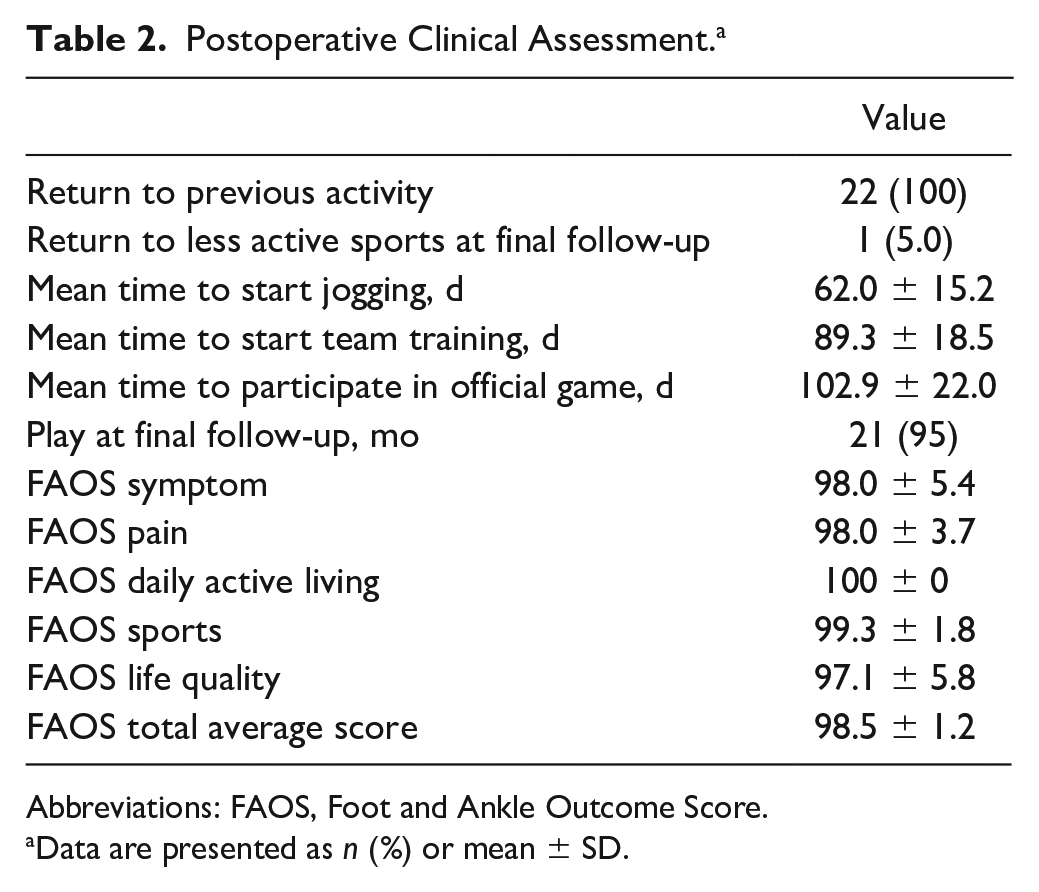
Abbreviations: FAOS, Foot and Ankle Outcome Score.
Data are presented as n (%) or mean ± SD.
We did not observe a difference in RTP between West Point injury grades IIB and III (Table 3), and we could not confirm a difference in the RTP between the athletes older than and the athletes younger than 25 years of age (Table 4, Figure 3).
Comparison of RTP in Athletes Older Than and Athletes Younger Than 25 Years of Age. a
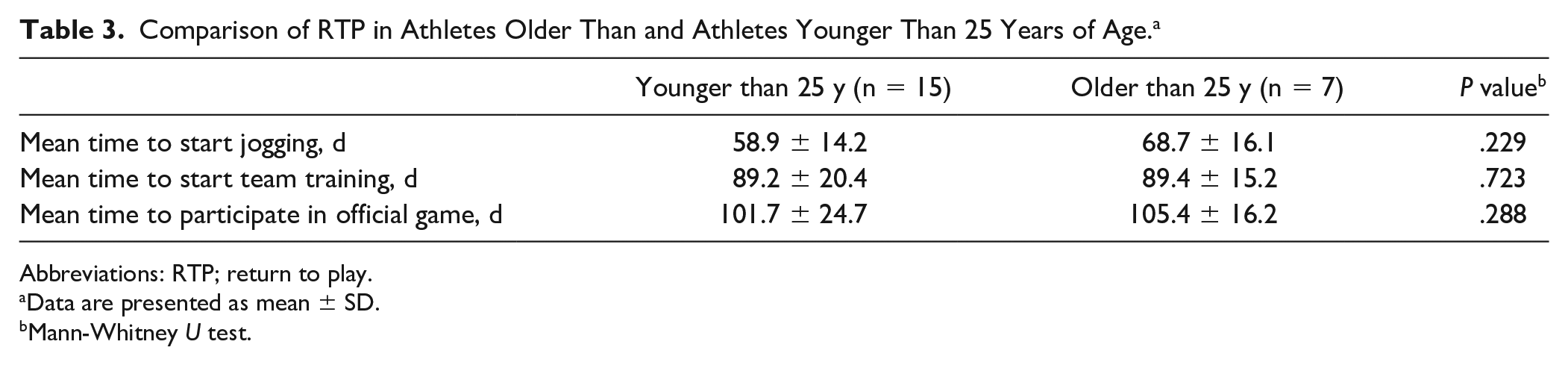
Abbreviations: RTP; return to play.
Data are presented as mean ± SD.
Mann-Whitney U test.
Return to Play According to Overall and West Point Grade IIB and III Injuries. a
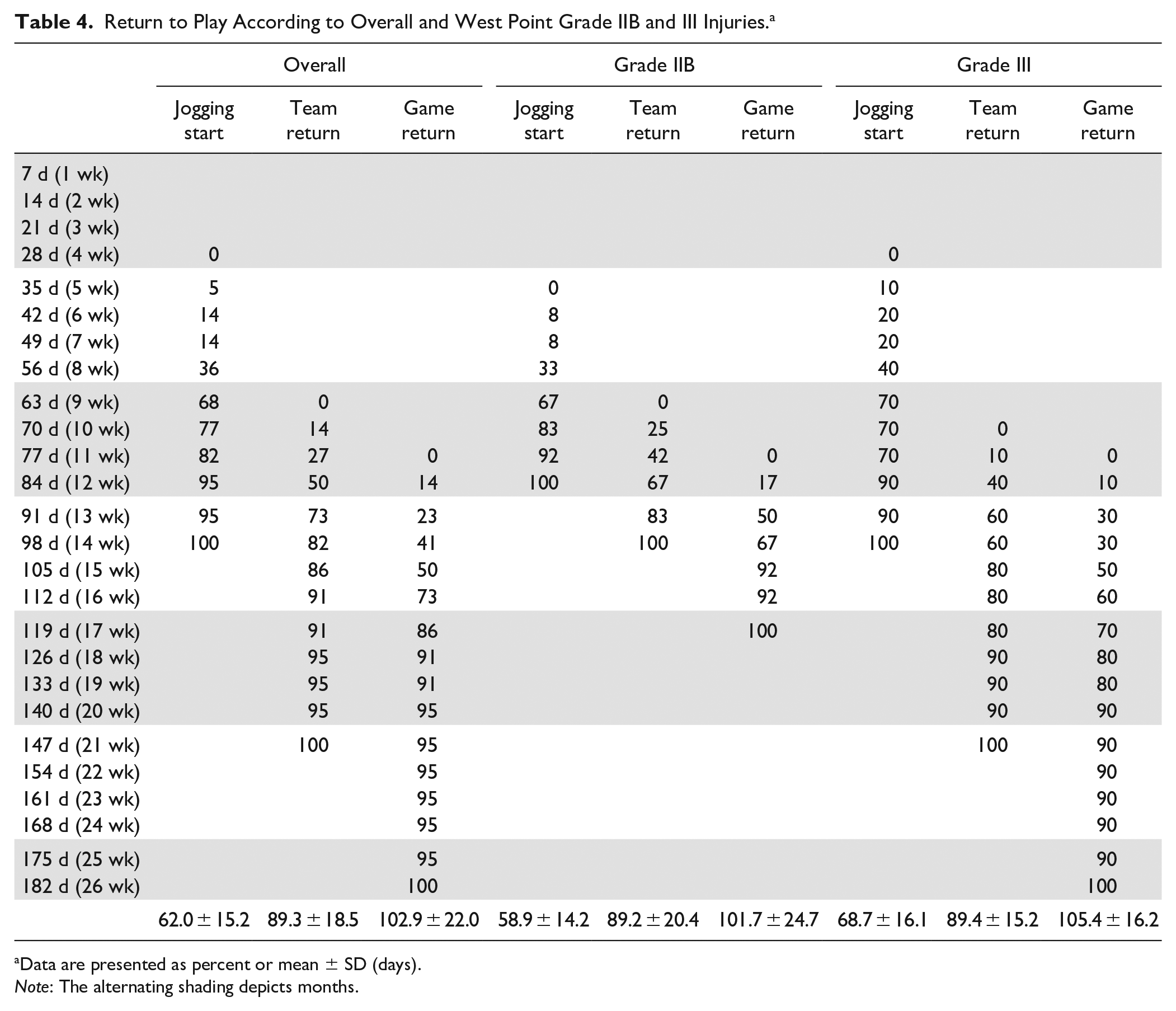
Data are presented as percent or mean ± SD (days).
Note: The alternating shading depicts months.
The overall periods for return to jogging, team training, and official game play were 62.0, 89.3, and 102.9 days, respectively.
There was no significant correlation between RTP and age, height, or weight. A strong correlation was found between team training day and official match day (r = 0.94, P < .000), and it was found that in athletes with rapid RTP team training, the official match day was also faster; however, early jogging did not appear to affect return to team training or official game play (Table 5).
Pearson’s Correlation Between Age, Height, Weight, Jogging Day, Team Training Day, and Official Match Day. a
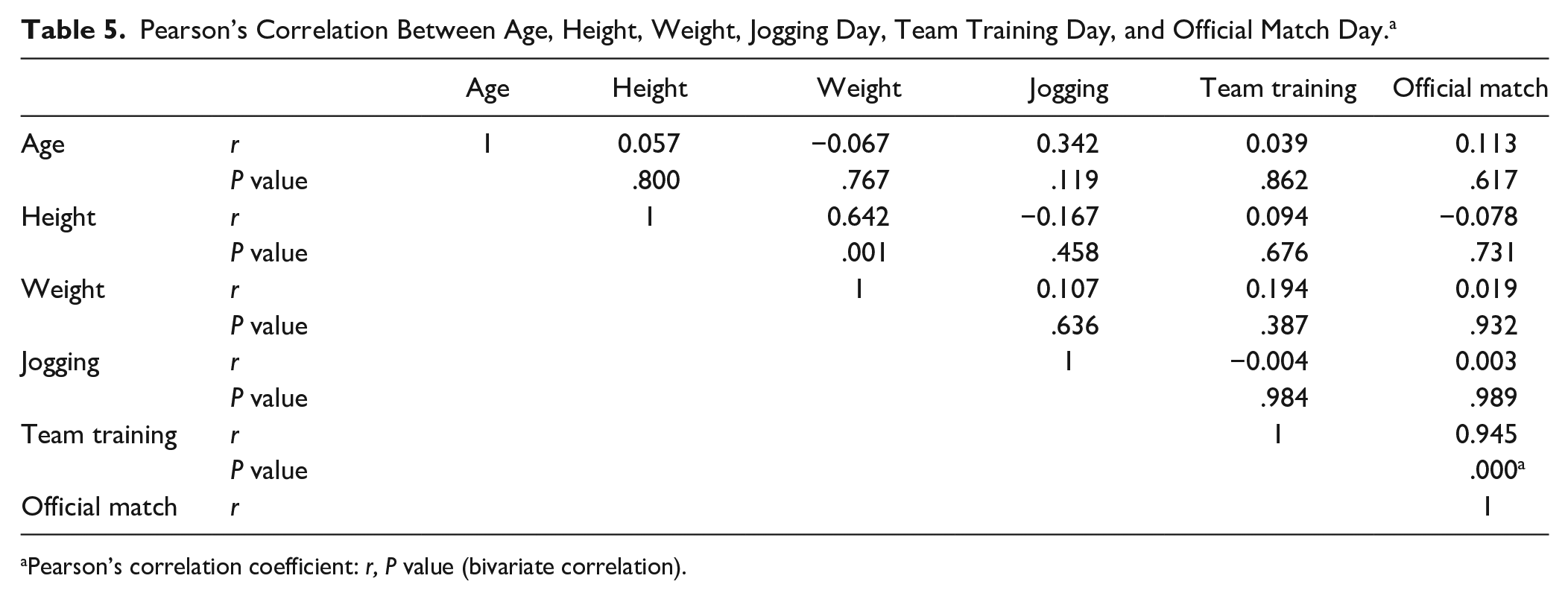
Pearson’s correlation coefficient: r, P value (bivariate correlation).
Two elite-level soccer players were reinjured at the end-of-season game. One elite handball player experienced an eversion sprain but was able to return to participation in 2 weeks with conservative treatment. Another elite soccer player was diagnosed with redisruption of the AITFL in the left ankle when he crossed toward the goal post from left. He experienced another injury with the same mechanism of dorsiflexion and external rotation 8 months after the operation, requiring syndesmosis allograft reconstruction including anterior talofibular ligament repair. Six months later, he returned to official game play. None of the patients showed major complications, including infection or superficial peroneal nerve injury.
Discussion
Syndesmosis injuries can require prolonged recovery for athletes in terms of rehabilitation. In this study employing AITFL open anatomical suture anchor fixation for unstable isolated syndesmotic disruptions without fracture, the mean RTP time after which the athletes could participate in an official game was 14.6 weeks at the 18-month follow-up, and the athletes could resume jogging at 8.9 weeks and athletic training at 12.7 weeks after operation.
Wright et al 25 reported that national hockey players with syndesmosis injuries required a mean time to RTP of 45 (range, 6-137) days versus the 1.4 (range, 0-6) days required for lateral sprains. Furthermore, delayed diagnosis or operative stabilization (>6 months) results in significantly worse outcomes. 4 Thus, treatment methods should be determined precisely based on anatomical and functional stability. According to the West Point Ankle Grading System, conservative treatment is performed in patients with grade I and IIA injuries, which are anatomically or functionally stable, while operative stabilization should be performed in grade IIB and III cases, which comprise cases of anatomically and functionally unstable syndesmosis. 4
Conventional operative methods include transsyndesmotic screw fixation and the suture-button fixation technique. For transsyndesmotic screw fixation, Steinmetz et al 20 reported that the mean RTP time was 10 weeks, and Taylor et al 21 reported a RTP time of 6 weeks. Following suture-button fixation, Calder et al 3 reported that the mean RTP time was 9.3 weeks, while Naqvi et al 15 reported that the mean RTP time was 11.2 weeks. However, these studies did not provide a detailed definition of RTP, which prohibited a direct comparison to our results.
Recently, D’Hooghe et al 4 reported that isolated unstable syndesmosis injury treated by suture-button fixation had a mean RTP time to field rehabilitation of 5.3 weeks, to team training of 10.3 weeks, and to first official match of 14.7 weeks postoperatively. This is very similar to our results and provides important information to sports medicine doctors and athlete trainers. They reported that risk factors for worse outcomes were age older than 25 years and West Point grade III injuries. However, our results showed no correlations to age or injury severity.
For ideal syndesmotic stability, 3 factors must be confirmed: stable fixation during ligament recovery and initial joint movement; corrective reduction; and normal biomechanical movement. 14 Currently, syndesmotic fixation techniques include 3 categories: (1) syndesmotic screws, (2) suture-button construct, and (3) anatomical repair of syndesmotic ligaments. 5
Transsyndesmotic screws’ rigid fixation remains the gold standard for syndesmotic injury with or without fibular fracture; however, it has the disadvantage of restricted physiologic motion of the ankle and malreduction.16,19 Zhan et al 26 reported that open and anatomical repair of syndesmosis has better functional outcomes than transsyndesmotic screw fixation. In addition, there were significantly fewer malreductions in the anatomical repair group.
Our technique makes it easy to ensure the stability of syndesmosis, which has more anatomical fixation via the upper surface of the AITFL. Open reduction and tibiofibular suture anchor fixation can avoid malreduction of the syndesmosis because the knotless anchoring on the tibia reduces the syndesmosis automatically in the absence of posterior tibiofibular ligament injury. We used the expression “closed book” reduction because the mechanism of injury was similar to that of “open book” reduction.
Suture-button fixation also yields proper reduction and stability, with the advantage of not requiring routine removal.11,22 However, Forsythe et al 6 reported that suture-button fixation with a transverse plane could not maintain anatomical reduction. Moreover, Shoji et al 19 found that the fibular external rotation angle increased significantly in single suture-button fixation with dorsiflexion, inversion, and external rotation forces. Several studies have shown that the transsyndesmotic suture-button technique with AITFL anatomical suture tape fixation (Arthrex) achieved dynamic stability similar to that of an intact cadaver compared with suture-button fixation alone.22,24
Shoji et al 19 reported that when ankle dorsiflexion and inversion were performed, the tibiofibular diastasis and fibular rotational angle were more stable in the group that received additional anatomical suture tape fixation than in the group that underwent only suture-button fixation. Interestingly, in their research, the group with fixation by transsyndesmotic suture button with AITFL suture tape and that with AITFL suture tape alone show almost similar outcomes in terms of physiologic ankle stability. The anatomical AITFL fixation alone technique also yielded appropriate results in terms of stability, mechanical movement, and proper tibiofibular reduction.
In our study, we used knot and knotless suture anchors instead of suture tape because the bioscrews required for fixation were quite large. Furthermore, our technique required fixation on both sides of the bone, unlike repair or suture on a ligament. As in the previous study, the mean pullout strength of the suture anchor was good enough to endure the force applied to the distal syndesmosis during normal ankle movements.1,9 Our outcomes suggest that syndesmosis suture anchor fixation alone is sufficient for management of acute isolated syndesmosis injury.
Finally, surgery using suture anchor offers an economic advantage over other operative techniques. The cost of the suture anchor implant is usually more than $600, while the suture anchor used in this study costs approximately $180, resulting in a total cost of approximately $360 for 2 suture anchors. Although this procedure is more expensive than screw fixation, it does not carry the risk of screw breakage or removal.
The limitations of this study include its comparatively short follow-up and small sample size. Because of the retrospective design, this study lacked comparisons with a control group. However, we only included athletes and excluded individuals with several kinds of associated injuries. Further studies with a longer follow-up period and a larger sample size may be necessary in the future. The definition of RTP is an important factor to compare and analyze the usefulness of operative methods for athletes. However, it was difficult to make objective comparisons because the criteria for RTP varied among studies. Thus, it is necessary to set standard criteria for RTP in the future.
Conclusion
Our study showed that isolated syndesmosis disruption in athletes who underwent tibiofibular knotless anchor fixation had good clinical outcomes. In short-term follow-up, 95% of the athletes returned to their sport at their preinjury level. The average times to return to running, team training, and official game play were 62.0, 89.3, and 102.9 days, respectively.
Supplemental Material
sj-docx-1-fai-10.1177_10711007211015188 – Supplemental material for Suture Anchor Augmentation for Acute Unstable Isolated Ankle Syndesmosis Disruption in Athletes
Supplemental material, sj-docx-1-fai-10.1177_10711007211015188 for Suture Anchor Augmentation for Acute Unstable Isolated Ankle Syndesmosis Disruption in Athletes by Jin Su Kim and Hyuck Soo Shin in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_10711007211015188 – Supplemental material for Suture Anchor Augmentation for Acute Unstable Isolated Ankle Syndesmosis Disruption in Athletes
Supplemental material, sj-pdf-1-fai-10.1177_10711007211015188 for Suture Anchor Augmentation for Acute Unstable Isolated Ankle Syndesmosis Disruption in Athletes by Jin Su Kim and Hyuck Soo Shin in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jin Su Kim, MD, PhD, is a training instructor at a cadaver workshop hosted by Arthrex Corporation. However, for this study, an Arthrex Corporation product was chosen because it offered the advantage of allowing knotless bone fixation. We have recently also used the Raptor and Q-fix products from Smith & Nephew Corporation. No benefits in any form were received or will be received from a commercial party related directly or indirectly to the subject of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
A supplemental video for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.