
Abstract
Background:
Autologous grafting is widely used in orthopedic surgery because of its high osteogenic capacity, immunologic compatibility, for the absence of risk of disease transmission, and for not requiring a bone bank. The posterior-superior calcaneal tuberosity is an option for obtaining a cortical and cancellous structural bone. This study aims to describe the operative technique and complications observed at the donor site of the posterior-superior calcaneal tuberosity.
Methods:
Patients who underwent graft harvesting from the posterior-superior calcaneal tuberosity were retrospectively evaluated by pain outcomes, imaging tests, and intra- and postoperative complications.
Results:
Twenty patients with a median age of 69 years (range 48-77) and follow-up of 16 months (12-26) were assessed. Median postoperative pain at the donor site was 0 (0-6), with 2 patients reporting persistent local pain. No case of Achilles tendon rupture or intra- or postoperative calcaneal fracture were identified. One patient developed a superficial infection that was quickly resolved using oral antibiotic therapy.
Conclusion:
The posterior-superior calcaneal tuberosity is an alternative source of autologous graft with low donor site morbidity.
Level of Evidence
Level IV, case series.
Introduction
The use of bone graft in orthopedic surgeries is widespread to fill cavities, bone defects, and pseudoarthrosis, as well as to correct deformities, among other indications.3,7,9,20
When bone grafts are from the patient’s own body (autologous), they are usually harvested from the tibia, fibula, or iliac crest. 8 These 3 bones provide structured cortical grafts. Bone grafting is common; in the United States alone, it is estimated that 200 000 grafting procedures are performed each year. 19
In 2012, Sanhudo 15 described the technique of harvesting an autologous bone block graft from the posterior-superior calcaneal tuberosity. The study shows some advantages of this technique, such as preparation in the same operative field and the possibility of using the same anesthesia as that of the primary procedure. Additionally, the bone structure at the calcaneal tuberosity is especially useful in surgeries that require a rigid and tricortical graft.
This study aims to evaluate the donor site complications observed in a consecutive series of patients undergoing autologous graft harvesting from the posterior-superior calcaneal tuberosity.
Materials and Methods
This is a retrospective case series study based on data collected from patients’ medical records and on a prospective face-to-face clinical evaluation. The sample included 22 patients consecutively, and 2 case was not included due to loss of follow-up. The study was approved by the local ethics committee and followed the Declaration of Helsinki and the Guidelines for Good Clinical Practice.
Participants underwent operative treatment using the posterior-superior tuberosity as the autologous graft donor site between January 2017 and January 2020. All procedures were performed by the same medical team, at the same medical center. The graft was used at the same operative time to treat foot and ankle disorders.
The inclusion criteria were as follows: (1) patients who underwent operative treatment using the technique of autologous graft harvesting from the posterior-superior calcaneal tuberosity and (2) patients who agreed with and signed the study informed consent form at the time of follow-up.
The exclusion criteria were as follows: patients with neuropathy, previous or current skin lesions in the graft region, previous degenerative lesions, and surgeries or sequelae of fractures in the foot or ankle.
Outcome Measures
This study assessed clinical and imaging outcomes. The clinical evaluation was performed at the last consultation using the visual analog scale (VAS) directed at the graft donor as well as by evaluating the healing process and complications.
In cases where patients reported pain at the donor site, a magnetic resonance imaging (MRI) was ordered and independently evaluated by 2 radiologists specialized in the musculoskeletal field (G.D., J.P.B.C.L.). Feet radiograph was ordered according to routine consultations (Figure 1).
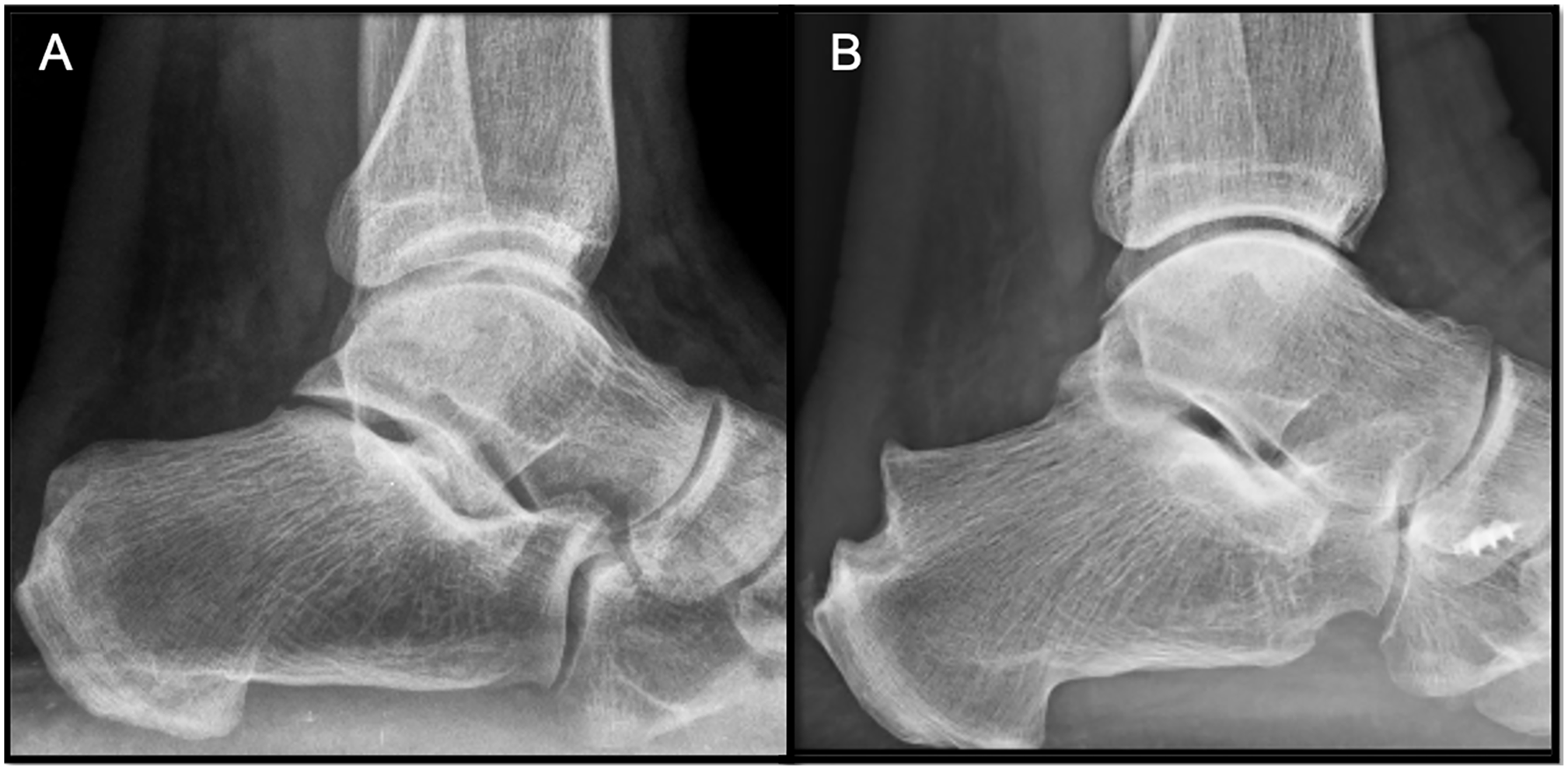
(A) Preoperative radiograph. (B) Radiograph of the posterior-superior calcaneal tuberosity graft harvesting site 1 year after the surgery.
Operative Technique and Postoperative Care
The patients underwent the operative procedure in the supine position, with lateral tilt after placing a cushion below the ipsilateral gluteus. Spinal anesthesia was performed with sedation in all cases.
After setting up the sterile fields, a tourniquet was inflated. The technique consists of making a vertical incision of approximately 3 cm, in most cases in the lateral region, in the topography of the posterior-superior calcaneal tuberosity (Figure 2).

Vertical incision in the topography of the posterior-superior calcaneal tuberosity.
The Achilles tendon is identified with care not to detach it. The graft harvest area is then marked with the electrocautery, and a bone saw is used to perform the osteotomy (Figure 3).

Graft identification and preparation for osteotomy.
A delicate chisel is used to harvest the graft; then, the region must be cleaned with a saline solution (Figure 4). The subcutaneous tissue was closed using a 3-0 Vicryl suture, whereas the skin was closed using a 4-0 nylon suture.
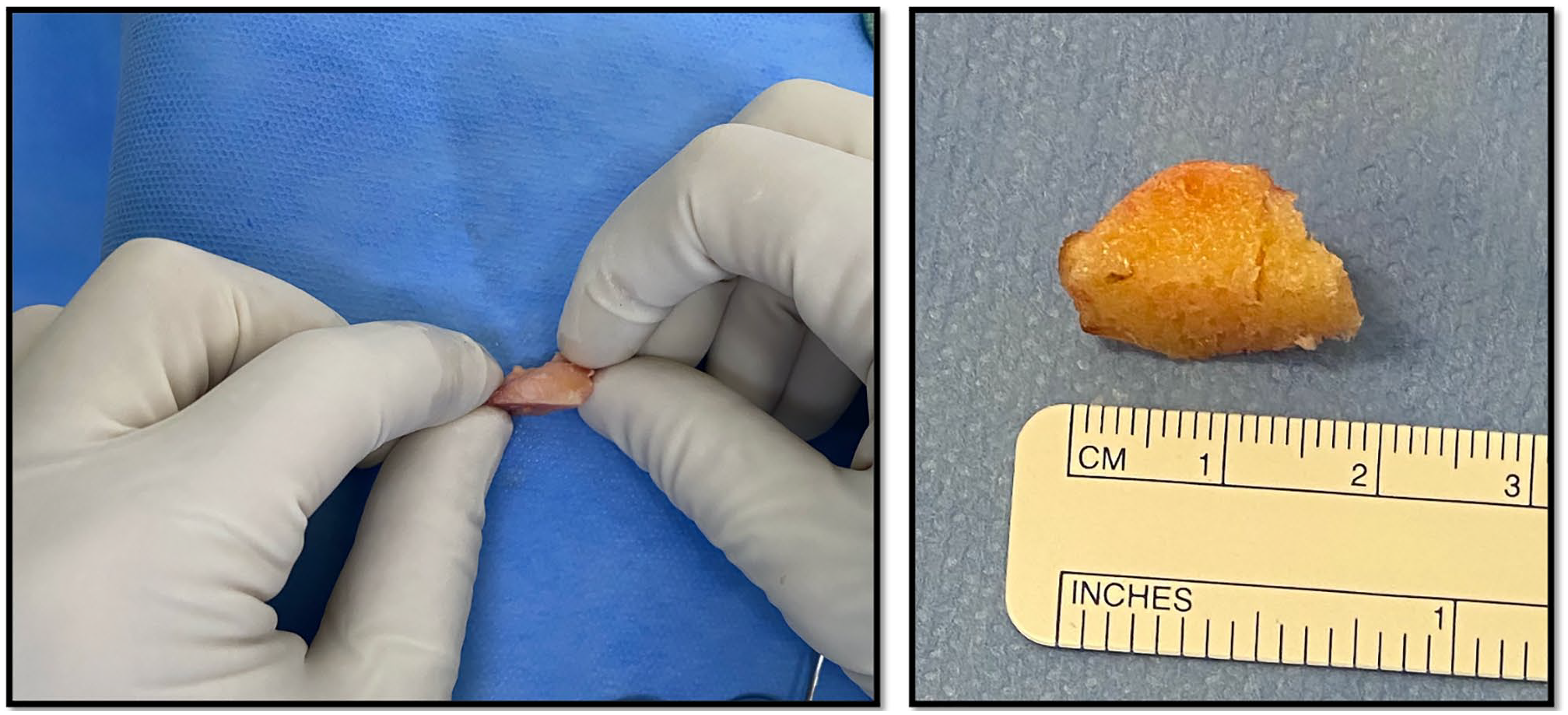
Autologous bone graft from the posterior-superior calcaneal tuberosity.
Postoperative care was the same as for any other surgery. Immediate weightbearing restrictions varied according to the primary procedure to which the patient was submitted.
Statistical Data Analysis
Statistical analysis was performed using the Stats package of software R. 17 The continuous variables were calculated by mean, median, standard deviations and range, while their proportion calculated the categorical ones. A description of the maximum and minimum values was included.
Results
The participants were mostly female (95%), with a mean age of 67.35 and a standard deviation of 6.82, ranging from 48 to 77 years. The left side was most commonly affected (55%), 18 of 20 (90%) patients were nonsmokers, 4 of 20 (20%) had diabetes mellitus, and 2 of 20 (10%) had rheumatoid arthritis (Table 1.)
Sample Characteristics and Postoperative Results.
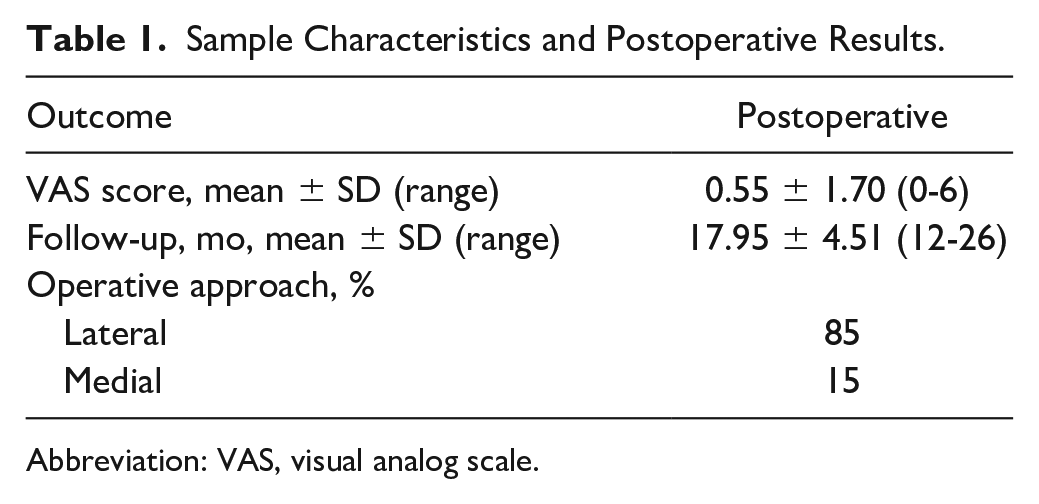
Abbreviation: VAS, visual analog scale.
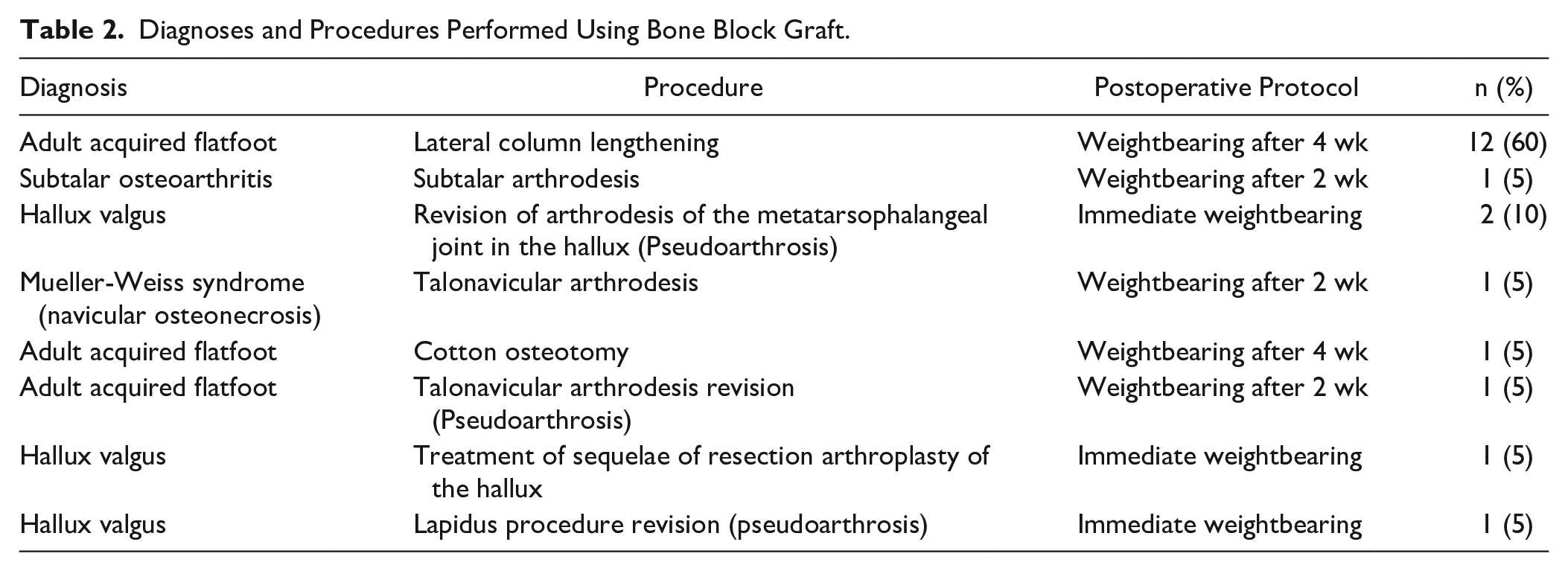
Table 2 shows the primary operative procedures that required graft harvesting, as well as the diagnoses and postoperative protocol.
Diagnoses and Procedures Performed Using Bone Block Graft.
Two patients (10%) reported pain in the graft region. In both cases, the pain was not exclusive to the donor site, but a diffuse pain in the foot, including that region. Both patients underwent a magnetic resonance imaging (MRI) examination: one showed mild insertional tendinopathy with no sign of rupture and edema in the graft donor bed; the other, on the other hand, showed no inflammatory changes in the Achilles tendon and its region, except for a slight thickening.
In this series, 1 patient developed a superficial operative wound infection, which resolved with oral antibiotic therapy. We had no deep infections requiring operative debridement, no Achilles tendon ruptures or intra- or postoperative calcaneal fracture.
Discussion
Autologous bone graft is considered the gold standard of bone grafting because it contains osteogenic, osteoinductive, and osteoconductive properties. Further, there is a complete histocompatibility, with no risk of disease transmission.9,12
One of the most common sites for autologous bone graft harvesting is the iliac crest region with varying reports of complication rates. Shin et al 16 found good long-term results, with low complication rates. However, Kim and colleagues 10 reported 16.5% of patients reporting more severe pain at the iliac crest graft harvesting site than at the primary operative site after 1 year of follow-up.
In a case series involving 19 patients, Feeney described the harvesting of a tricortical graft from the calcaneus. Unlike this study, the 1.5 × 1.5 × 3-cm bone block was harvested from a region close to the halfway point between the calcaneal tendon insertion and the subtalar joint. No patient developed symptoms at the donor site at the end of the follow-up, but they had 2 calcaneal fractures requiring treatment with cast immobilization. 6 By harvesting the graft from the tuberosity very close to the Achilles tendon insertion, similar to a calcaneoplasty, we obtained a much shorter lever arm, thus reducing the fracture risk. In this procedure, the concern is the risk of avulsion, but no patient had this complication. Similarly, studies in which calcaneoplasty has been performed to treat Haglund’s Syndrome, Achilles avulsion is rare and typically only after tendon manipulation for insertional tendinopathy was performed during the procedure.4,18
In our study, 2 of 20 (10%) of patients reported continued pain. These patients did not report pain exclusively at the graft harvesting site, but a diffuse pain in the foot, probably from the primary operative procedure. The MRI examinations did not show any specific injury to the Achilles tendon or to other local structures that could have been affected by the graft harvesting procedure. Only 1 of the cases involved mild tendinopathy, with no substantial injuries.
Our sample presented a patient with a superficial infection at the operative site, which was resolved using oral antibiotic therapy. When comparing it with the complications already described on iliac graft harvesting, such as gait abnormalities, infection, sensory changes, and cosmetic dissatisfaction, 11 it appears that calcaneal graft harvesting is a less morbid procedure.
Another advantage of using autologous bone graft from the posterior-superior calcaneal tuberosity is that the procedure is performed in the same operative field. Two studies have shown that postoperative pain is less common when using a graft from the same area as that of the primary procedure, especially in foot and ankle surgeries; moreover, anesthetic blocks can be performed to control the postoperative pain.2,14
The tibia region is another common region for autologous bone graft. Low complications in this area have substantial evidence in the literature; however, a major disadvantage is the recommendation to prevent local weightbearing and postpone walking until the tibia defect is partially consolidated in order to prevent a possible fracture.1,5,13 In our small case series, we did not restrict weightbearing based on the harvesting of a graft from the calcaneus.
The size of bone grafts from the posterior-superior calcaneal tuberosity is restricted. The maximum dimension that can be harvested is up to the region of the Achilles tendon’s insertion, so as to avoid the risk of disinsertion. In cases where large amounts of graft are needed, another donor site should be deemed a safer option.
The study has some limitations. Our sample size is relatively small, and the follow-up time is short. Graft harvesting was performed by a team specialized in foot and ankle surgery and may have a steep learning curve for orthopedic surgeons unfamiliar with the anatomy of the area. The grafts were used exclusively in procedures in the same foot, and not in other areas, favoring a confusing factor in the results. Finally, the autologous graft used in this study was not compared with other classic autologous graft donor sites, such as the iliac crest or the tibia region.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007211032665 – Supplemental material for Low Donor Site Morbidity Associated With Tricortical Calcaneal Bone Graft
Supplemental material, sj-pdf-1-fai-10.1177_10711007211032665 for Low Donor Site Morbidity Associated With Tricortical Calcaneal Bone Graft by Gabriel Ferraz Ferreira, João Henrique Almeida Costa, Giancarlo Domingues, João Paulo Bacellar Costa Lima, José Antônio Veiga Sanhudo and Miguel Viana Pereira Filho in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.