
Abstract
Background:
The association between forefoot and hindfoot position for planus and cavus feet is fundamental to the treatment of these deformities. However, no studies have evaluated the association between hindfoot alignment and first metatarsal (M1) axial rotation. Understanding this possible relationship may help to understand the deformity and improve patient care. The purpose of this study is to determine a correlation between hindfoot alignment and metatarsal rotation as assessed by weightbearing computed tomography (WBCT).
Methods:
Patients who underwent weightbearing plain radiography (WBPR) and WBCT between 2015 and 2018 were evaluated. Hindfoot alignment was measured with the calcaneal moment arm (CMA). M1 rotation was measured using the Kim and Saltzman angles. Patient subgroups were created according to the severity of valgus/varus hindfoot alignment. Statistical analyses were performed to evaluate for association between variables.
Results:
Among the 196 patient feet included in the study, the average CMA was 6.0 ± 16.2 mm. The average Kim and Saltzman angles were 7.7 ± 12.9 degrees and 2.8 ± 13.1 degrees, respectively. The average Meary angle was 182.0 ± 11.9 degrees. A moderately strong association was found between the CMA and the Saltzman (r = 0.641, P < .01) and Kim angles (r = 0.615, P < .01). Hindfoot valgus was associated with M1 pronation and hindfoot varus with M1 supination. Additionally, inverse relationships between the Meary angle and the Saltzman (r = −0.600, P < .01) and Kim angles (r = −0.529, P < .01) were identified.
Conclusion:
In this well-defined cohort, we found substantial correlation between hindfoot alignment and M1 rotation. Hindfoot valgus was associated with M1 pronation, and hindfoot varus was associated with M1 supination. Surgeons correcting cavovarus/planovalgus deformities should be aware of this association and evaluate the need for first-ray derotation.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Compensatory forefoot supination resulting from hindfoot valgus in the setting of pes planovalgus deformity is a well-described phenomena.6,17,24,27 This is further reinforced by the observation that recurrence of operatively corrected hallux valgus is associated with progressive planovalgus deformity. 17
Although these relationships between forefoot and hindfoot position exist, to our knowledge no investigation has been performed to query a potential association between hindfoot alignment and first metatarsal (M1) axial rotation. M1 axial rotation in the coronal plane can manifest as “pronation” when the plantar aspect of the M1 faces toward the second metatarsal, and “supination” when the plantar aspect of the bone faces away from the second metatarsal.29,35,36 M1 pronation has been recognized as a component of hallux valgus deformity,5,7,9,20,23,25,32,35 and may contribute to poor outcomes and recurrence following operative intervention of this pathology.3,17,20,30 Conti et al examined multiple methods of measuring M1 axial rotation in patients undergoing a Lapidus bunionectomy and reported a statistically significant decrease in M1 pronation postoperatively. They also demonstrated the importance of using a consistent method of measuring M1 axial rotation, as different reference points can yield significantly different results. 8 M1 rotation, in either direction, may also be associated with hindfoot varus and valgus deformity and could influence operative management and outcomes. For example, a patient with a pes planovalgus deformity may also have a symptomatic bunion with M1 malrotation that may possibly benefit from a derotational procedure in addition to a flatfoot reconstruction.
The purpose of this investigation is to determine the strength of a potential relationship between hindfoot alignment and M1 axial rotation in patients with mild, moderate, and severe hindfoot valgus and varus deformity. We hypothesize that (1) patient feet with a hindfoot valgus alignment will be associated with an M1 pronation deformity and (2) patient feet with a hindfoot varus alignment will be associated with an M1 supination deformity.
Methods
After obtaining internal review board (IRB) approval, electronic health records (EHRs) collected over a period of 42 months were retrospectively assessed between June 2015 and December 2018. All patients who received a weightbearing computed tomography (WBCT) imaging study during this period were reviewed. WBCT was indicated by the provider on a case-by-case basis to improve accuracy of clinical diagnosis following initial weightbearing plain radiographs (WBPRs). WBPRs were obtained prior to WBCT for all of these patients based on requirements by insurance providers. Ultimately, 761 consecutive WBCT images (pedCAT, CurveBeam LLC, Warrington, PA; medium view, 0.3-mm slice thickness, 0.3-mm slice interval, kVp 120, mAs 22.62) were assessed and any duplicate patient feet were subsequently omitted (n = 30). Additionally, patients who did not have anteroposterior and lateral foot WBPR taken within 6 months of the WBCT, or had surgery or an injury between image acquisition dates, were excluded (n = 125). Exclusion criteria were applied to the residual 606 feet. Patient feet with signs of previous operations (osteotomy, arthrodesis, arthroplasty), hardware in place, dysmorphia, partial amputations, and trauma were excluded from the study (n = 331). Following these omissions, the residual 275 feet of 262 patients were considered for inclusion.
Hindfoot alignment of each foot was first assessed using a standardized and reliable WBCT method, where 3 authors (R.L., C.A., A.B.) measured the calcaneal moment arm (CMA) (Figure 1). 2 CMA was determined by measuring the horizontal distance between the most inferior aspect of the calcaneus identified on axial cross-sectional imaging and an extended line representing the longitudinal axis of the tibia on coronal cross-section in millimeters. Directionality of the CMA was denoted with positive values for valgus and negative values for varus. 31 The subsequent distribution of cohort CMA values was established. In an attempt to evaluate M1 rotation in patients with hindfoot malalignment, 6 subgroups were created dependent on their severity of hindfoot position: (1) moderate valgus (12.9-19.7 mm), (2) moderate varus (−0.8 to −7.6 mm), (3) substantial valgus (>19.7-33.3 mm), (4) substantial varus (<−7.6 to −21.2 mm), (5) severe valgus (>33.3 mm), and (6) severe varus (<−21.2 mm). Similar to Wang et al, 37 the moderate subgroups (1 and 2) were defined as possessing CMA values between 0.5 and 1 SD away from the cohort mean. The substantial subgroups (3 and 4) had CMA values between 1 and 2 SD away from the cohort mean. The severe subgroups (5 and 6) possessed CMA values >2 SD away from the cohort mean. Patient feet with CMA values within 0.5 SD above or below the cohort mean (6.1 mm valgus) were excluded, as this study’s aim was to investigate patient feet with hindfoot malalignment (n = 79). These patients with neutral hindfoot alignment were examined in a separate study. 34
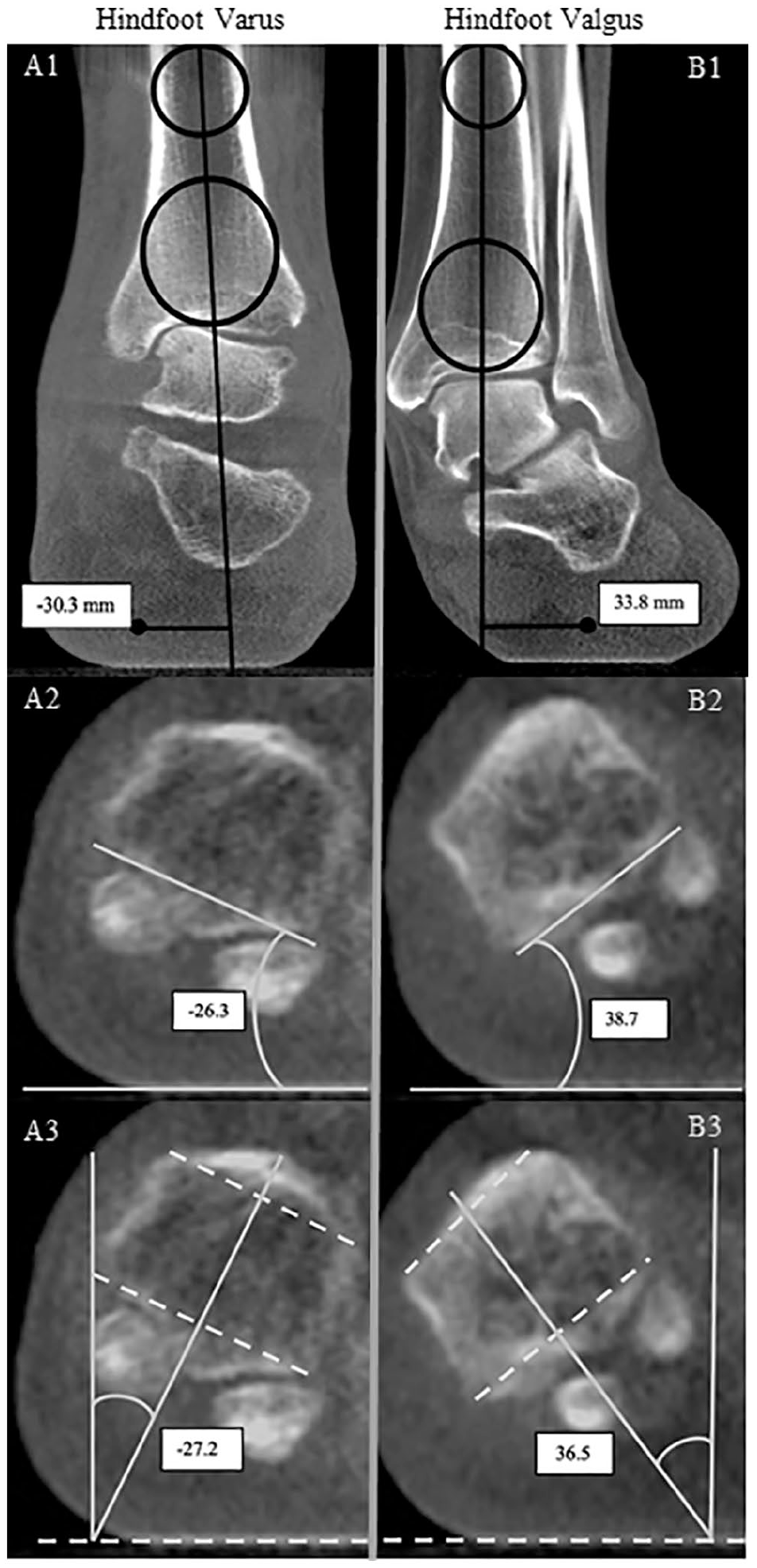
Coronal weightbearing computed tomography scans of (A) a 58-year-old woman with hindfoot varus and (B) a 61-year-old man with hindfoot valgus (B) visualizing hindfoot alignment using the calcaneal moment arm measurement (A1, B1). Measurement of first metatarsal axial rotation is illustrated using the Saltzman angle (A2, B2) and Kim angle (A3, B3). Images A/B 2 and 3 are measured in degrees. Varus alignment and supinated angulation are represented as negative values.
Following group allocation of the remaining 196 feet, 2 observers, including a musculoskeletal radiologist (R.L., observer A) and a foot and ankle–trained orthopaedic surgeon (N.B., observer B) independently accessed and measured the M1 axial rotation of each patient foot demonstrated on coronal view WBCT. Both observers used a standardized, reliable method to identify the same coronal WBCT slice. 34 With this common coronal plane established, M1 axial rotation (pronation/supination) was measured using methods proposed by Saltzman et al 30 and Kim et al. 20 Implementing the method introduced by Saltzman et al, 30 a line was drawn touching the inferior, outer profile of the tibial and fibular sesamoid sulci; the angle created between this line and a line representing a horizontal reference provided the amount of M1 rotation present (Figure 1). With the Kim et al method, a line was drawn that connected the medial and lateral corners of the superior M1 head. A similar line was drawn connecting the inferior corners. A third line was then drawn that bisected the half-way point of the first 2 lines. The angle formed between the bisecting line and a line perpendicular to a horizontal reference quantified the amount of M1 rotation present. 20 The observers showed excellent reliability using both of these methods in a prior study. 34 Pronation was defined as positive rotation, whereas supination was negative.
For the secondary analysis of this investigation, further measurements including the hallux valgus angle, intermetatarsal angle, interphalangeal angle, and Meary angle 26 were collected by the observers using WBPR following the methods proposed by Coughlin et al. 11 Additionally, the M1 head lateral edge shape was evaluated as described by Okuda et al. 28 This proposed method involves the assessment of an anteroposterior radiograph and the classification of the M1 lateral head shape as angled, intermediate, or round. Previous literature suggests that a round lateral head shape may be associated with M1 pronation.28,38 Initial cohort overlap and repeat measurements on half of the observers’ respective cohorts following an appropriate washout period of 4 weeks were incorporated into the study to generate data for interobserver and intraobserver reliability calculations for the lateral edge parameter.
Statistical Analysis
The intraobserver and interobserver reliability values were determined by calculating the kappa values on the basis of multirater kappa. Multirater kappa summarizes the strength of agreement for all possible comparisons between the observers including the same and mixed types of experience levels. 33 Kappa values were calculated for assessment of the lateral head round sign. 28 The kappa statistics were used as the chance-corrected measurement of agreement and was interpreted according to the definitions of Landis and Koch. 22 A Shapiro-Wilk normality test was performed to determine if the data were normally distributed. Spearman coefficient was used for correlation of nonparametric data. An analysis of variance test and a Kruskal Wallis test were used for the comparison of continuous parametric and nonparametric data, respectively. Post hoc comparisons between the 6 CMA subgroups were performed with the use of Tukey honestly significant difference (HSD) test. Comparisons of noncontinuous variables were performed with a Pearson chi-squared test. A P value of <.05 was considered significant in all tests. All data were analyzed using IBM SPSS Statistics, version 26.0 (IBM, Armonk, NY).
Results
Baseline demographic and imaging information of the included 186 patients and 196 feet are described in Table 1. The average age of all patients was 52.6 ± 18.1 years. The cohort was 62% male and the laterality of feet were evenly represented. All patients underwent WBPR and WBCT within 3 months of each other. The average CMA in the cohort was +6.0 ± 16.2 mm (valgus group: +19.0 ± 5.9 mm; varus group: –10.3 ± 8.2 mm). The average Saltzman angle and Kim angles (representing M1 axial rotation) were 2.8 ± 13.1 degrees (valgus group: 8.9 ± 10.3 degrees; varus group: –4.8 ± 12.2 degrees) and 7.7 ± 12.9 degrees (valgus group: 13.3 ± 10.9 degrees; varus group: 0.8 ± 11.9 degrees), respectively. The average Meary angle was 182.0 ± 11.9 degrees (valgus group: 176.3 ± 11.2 degrees; varus group: 189.2 ± 8.3 degrees), with greater than 180 degrees representing an apex dorsal measurement (Table 1).
Descriptive Summary of Baseline Demographic and Imaging Information. a
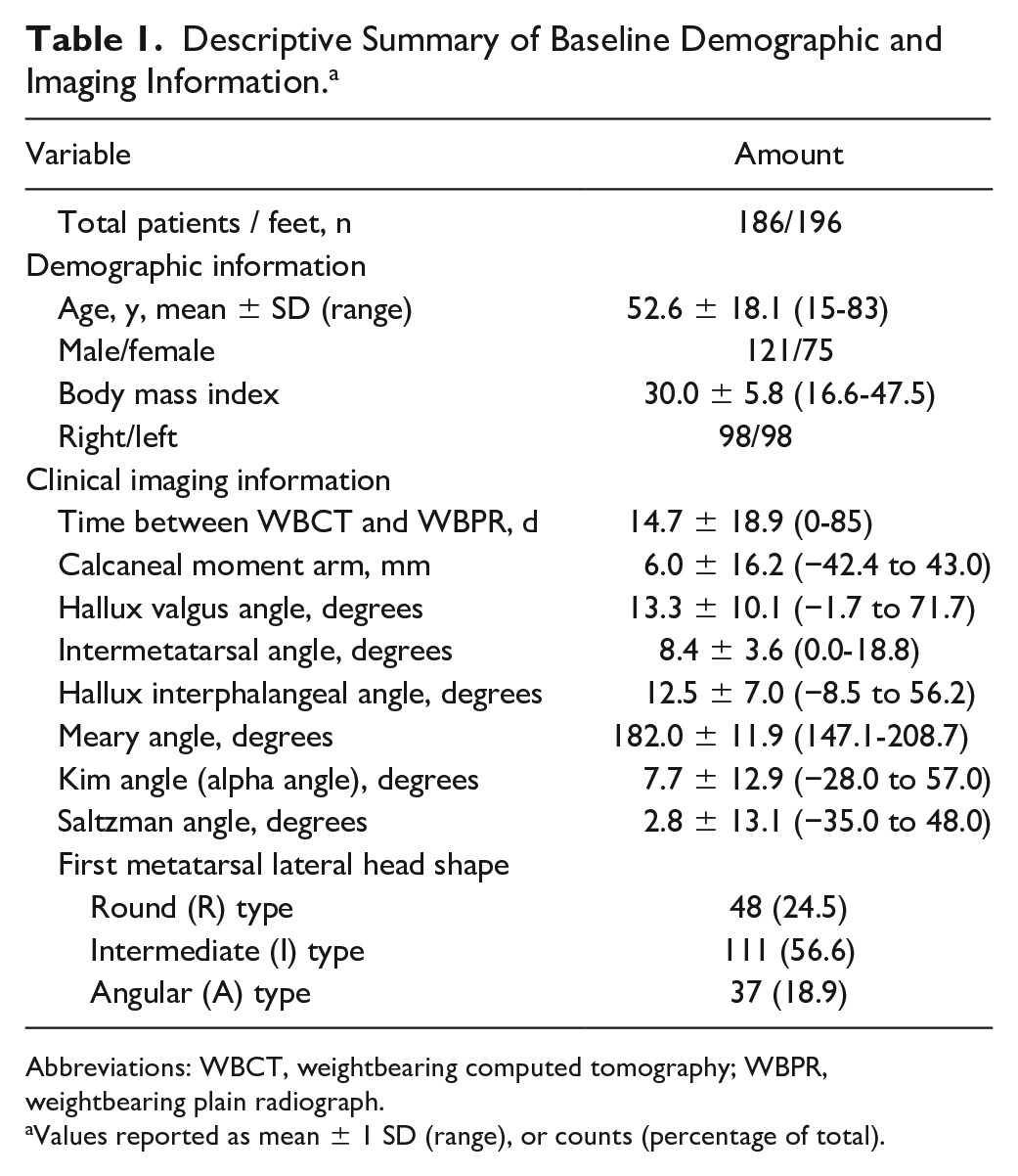
Abbreviations: WBCT, weightbearing computed tomography; WBPR, weightbearing plain radiograph.
Values reported as mean ± 1 SD (range), or counts (percentage of total).
Association Between First Metatarsal Axial Rotation and Hindfoot Alignment
There was a statistically significant association between hindfoot alignment (measured with CMA) and the Saltzman (r = 0.641, P < .01; Figure 2), and Kim angles (0.615, P < .01; Table 2). Subgroup analysis revealed that hindfoot valgus deformity was associated with M1 pronation that increased in severity as the hindfoot valgus deformity worsened (P < .01; Table 3). Conversely, hindfoot varus deformity was associated with M1 supination that increased as the hindfoot varus deformity worsened (Table 3, P < .01).
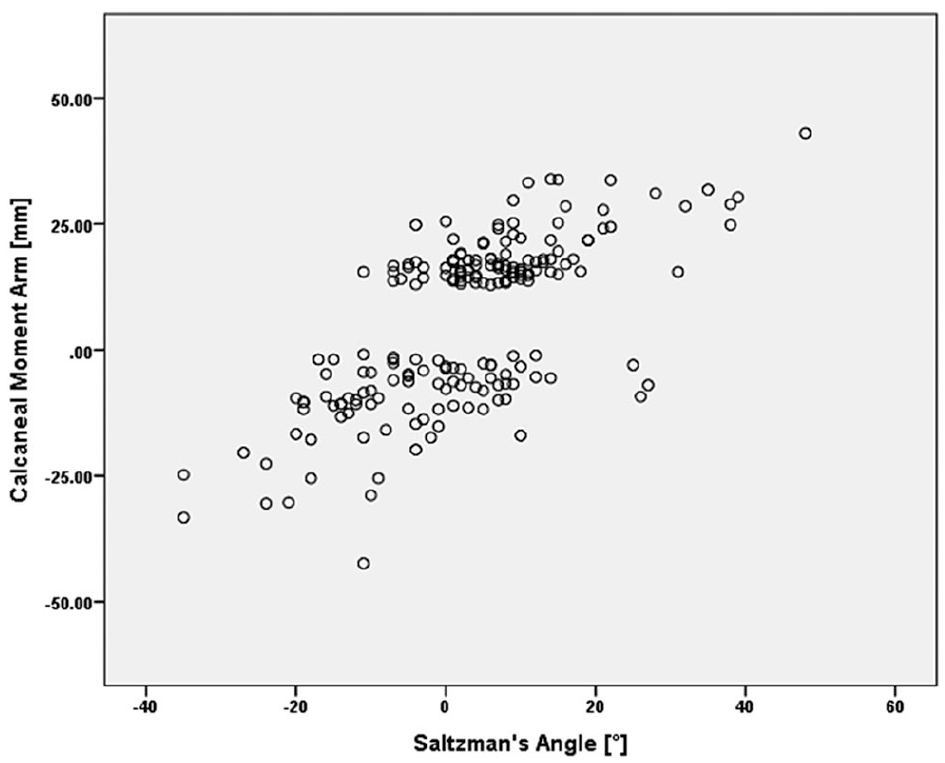
Correlation plot of first metatarsal rotation using the Saltzman et al 30 angle and the calcaneal moment arm (positive values indicate valgus calcaneal moment arm, negative values indicate varus calcaneal moment arm) with a correlation coefficient of 0.64 (P < .01). The gap seen on the graph is related to the patients who were excluded for possessing a normal calcaneal moment arm (mean ± 0.5 standard deviation).
Correlation Coefficients and Statistical Significance Between Single Radiographic Parameters and Demographics in 196 Feet. a
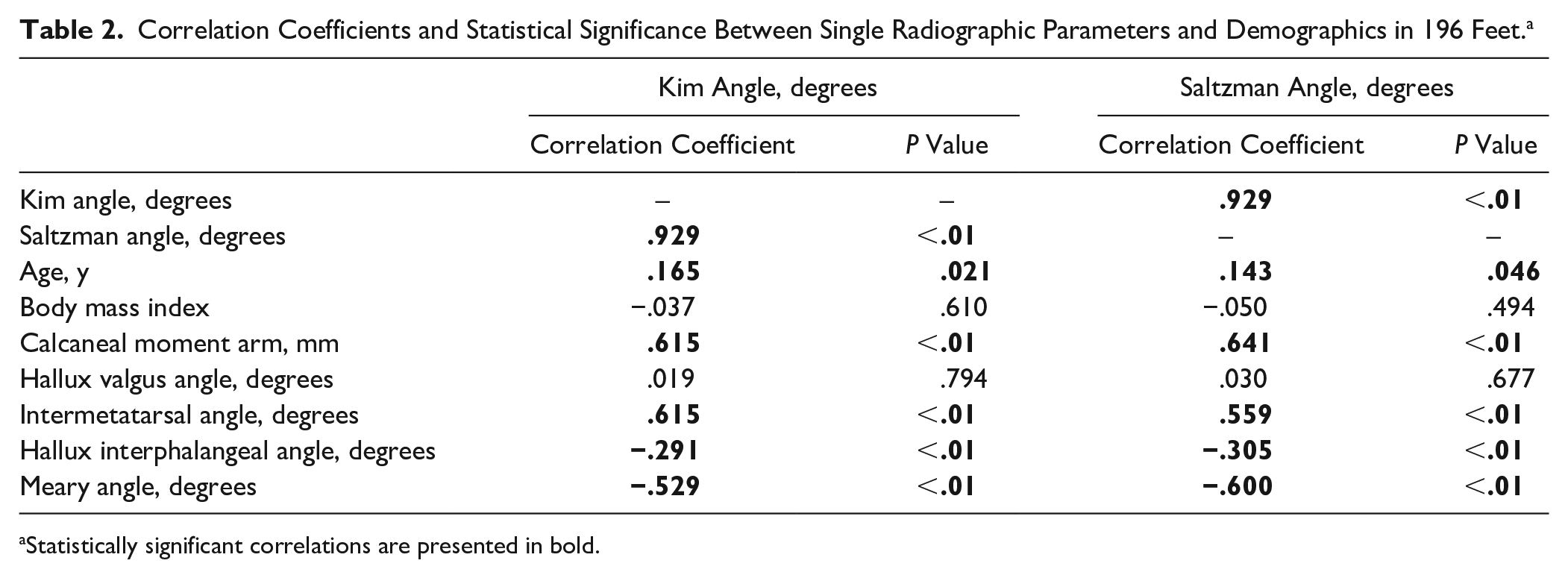
Statistically significant correlations are presented in bold.
Post Hoc Comparisons and Tukey Honestly Significance Difference Test of the 6 Subgroups Stratified by Calcaneal Moment Arm. a
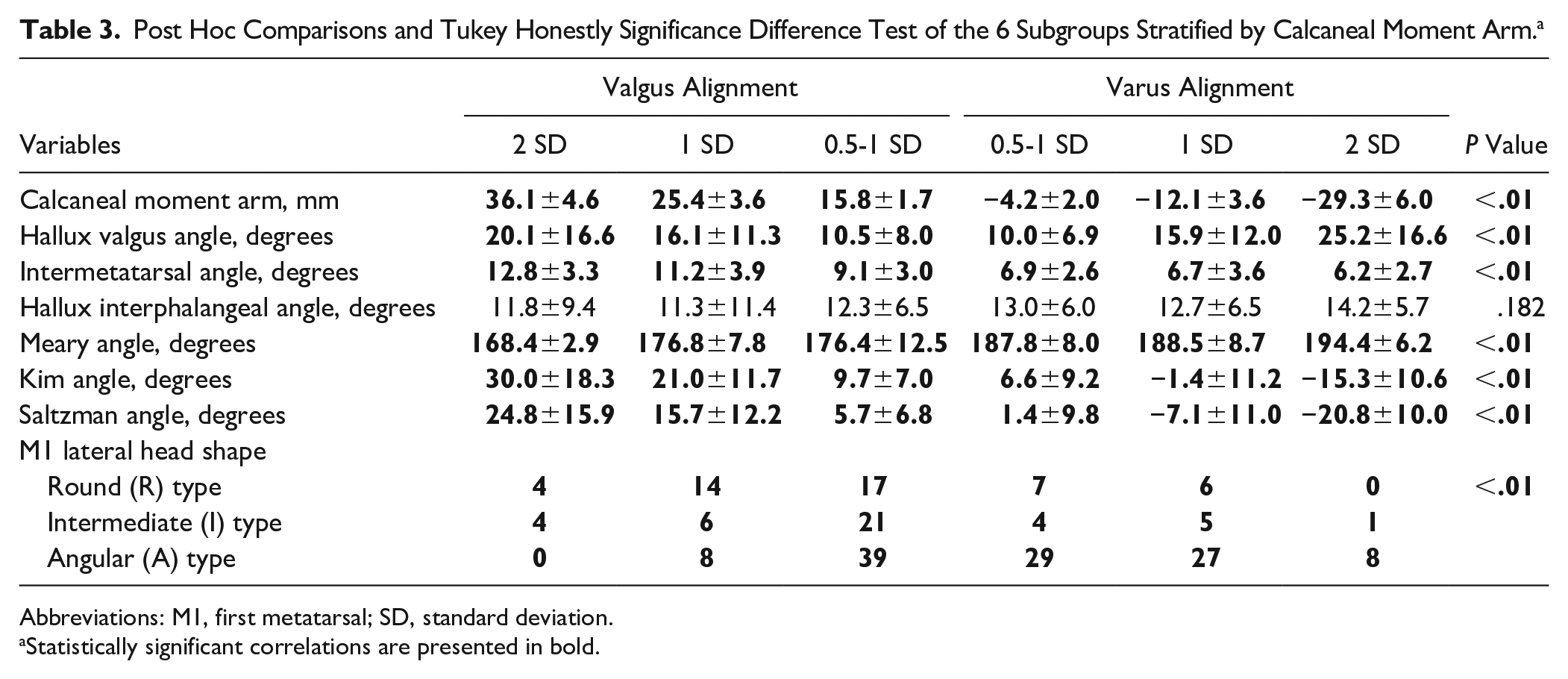
Abbreviations: M1, first metatarsal; SD, standard deviation.
Statistically significant correlations are presented in bold.
Association Between First Metatarsal Axial Rotation and Intermetatarsal Angle
There was a significant association between M1 axial rotation and the intermetatarsal angle (Kim angle: r = 0.615, P < .01; Saltzman angle: r = 0.559, P < .01). This suggests that as the intermetarsal angle increases, the amount of M1 pronation increases as well (Table 3).
Association Between First Metatarsal Axial Rotation and Meary Angle
There was a statistically significant inverse relationship between the Meary Angle and M1 axial rotation, measured by the Saltzman angle (r = −0.600, P < .01) and the Kim angle (r = −0.529, P < .01; Table 2). This suggests that as the Meary angle decreases (<180 degrees is apex plantar), as seen in a pes planus deformity, M1 pronation increases (Table 3).
Association Between Hindfoot Alignment and Intermetatarsal Angle
Subgroup analysis revealed a statistically significant association between hindfoot alignment and IMA. Patients with hindfoot valgus alignment had increasing IMA as the hindfoot valgus deformity worsened (P < .01; Table 3). Furthermore, patients with hindfoot valgus alignment had significantly higher IMA compared to those with hindfoot varus alignment (P < .01; Table 3).
Association Between Hindfoot Alignment and First Metatarsal Head Shape
Subgroup analysis revealed a statistically significant association between hindfoot alignment and the M1 head round sign. Patients with hindfoot valgus alignment had a significantly higher proportion of M1 heads characterized as round, rather than angular, compared to those with hindfoot varus alignment. Conversely, patients with hindfoot varus alignment were found to have a higher proportion of M1 heads characterized as angular, rather than round (Table 3).
Discussion
The results of this investigation confirm our hypothesis that there is a correlation between hindfoot alignment and M1 axial rotation. We report a significant, moderately strong association between hindfoot valgus alignment and M1 pronation. Additionally, we report a significant, moderately strong association between hindfoot varus alignment and M1 supination. Although these findings do not demonstrate causation, they do suggest an association with some pes planovalgus deformities and M1 pronation, as well as the converse: an association with some pes cavovarus deformity and M1 supination.
In the last decade, WBCT became a well-established imaging method to assess alignment and different pathologies of the foot and ankle.12-15,25 However, only few other studies have used imaging to evaluate the relationship between hindfoot and forefoot alignment. Kim et al 19 retrospectively evaluated WBPRs of 163 patients and compared patients with juvenile hallux valgus to a control cohort to determine whether a pes planovalgus deformity was associated with juvenile hallux valgus. Although they reported no association between hindfoot alignment and juvenile hallux valgus, they reported significantly more midfoot pronation (based on naviculocuneiform overlap) in the juvenile hallux valgus cohort compared to the control cohort. Unlike our study, Kim et al did not evaluate for an association between hindfoot alignment and M1 axial rotation. In addition, they evaluated patients with open physes whereas our cohort had a significantly higher mean age. Unlike Kim et al, our study did find a statistically significant association between hindfoot alignment and intermetatarsal angle (IMA), suggesting an association between hindfoot valgus and hallux valgus deformities. Finally, Kim et al only evaluated WBPR, while we used WBPR and WBCT for our investigation. In addition, Yoshioka et al 39 utilized simulated WBCT to evaluate the forefoot alignment of 10 patients (20 feet) with a hindfoot valgus deformity compared with that of 10 healthy controls (20 feet). They reported significantly increased M1 and fifth metatarsal pronation in the hindfoot valgus group compared with that of the healthy controls. They also reported significantly increased fifth metatarsal plantarflexion relative to the M1 in the hindfoot valgus group compared with that of the healthy controls. This likely represents a forefoot supination/varus deformity commonly seen in a planovalgus deformity. Similar to our study, they reported increased M1 pronation in patients with hindfoot valgus deformity. However, their method of measurement for pronation was different from ours, as they created a 3-dimensional computerized model and used a Eulerian coordinate system. Furthermore, they reported on a relatively small cohort of 20 patients. In addition, we included patients not only with hindfoot valgus but also hindfoot varus. Finally, Yoshioka et al 39 used simulated weightbearing CT, rather than true WBCT. These factors may account for some of the discrepancies between our results and theirs. Conti et al preoperatively and postoperatively examined multiple methods of measuring M1 axial rotation in patients undergoing a Lapidus bunionectomy for hallux valgus and reported a statistically significant decrease in M1 pronation postoperatively. They also reported a significant lack of correlation between different methods of measuring M1 rotation that varied regarding the modality and reference point for measurement. This demonstrates the importance of using a consistent method of measuring M1 axial rotation, as different reference points and modalities can yield significantly different results. Similar to our study, Conti et al uses WBCT to evaluate M1 axial rotation. However, they did not evaluate for any association between hindfoot alignment and M1 axial rotation. Furthermore, their cohort of 30 patients was significantly smaller than ours. 8
Although many other hindfoot/forefoot interactions, including compensatory changes, have been well described previously,6,17,24,27 this is the first study, to our knowledge, to report a correlation between hindfoot alignment and M1 axial rotation using true WBCT. Compensatory forefoot supination/varus has been demonstrated in the setting of a planovalgus deformity and often is partially corrected with an opening wedge medial cuneiform osteotomy (Cotton osteotomy).1,4,7,10,16,18 Furthermore, forefoot driven hindfoot varus in a cavovarus foot may be treated partially with a dorsiflexion M1 osteotomy. 21 Both these approaches correct sagittal plane deformities without appreciation of a potential rotatory abnormality of the first metatarsal. If such a deformity does exist, the approach to these types of medial column corrections could be modified with a derotational osteotomy or arthrodesis at the time of correction to improve forefoot loading.
There are multiple limitations with this study that deserve mention. First, this was a retrospective review of extant images from a large database of patients with varying presenting problems. We excluded many patients to obtain the set of images to do this analysis and were very stringent about the inclusion and exclusion criteria. However, it is still possible that patients may have presented with a foot deformity that was not accounted for within the parameters we evaluated and present an unrecognized confounding variable. Second, the mean axial rotation and hindfoot alignment values were only measured using the methods discussed above, and therefore these results may not be generalizable to other measurement methods. Third, and importantly, this study did not evaluate for causation and we cannot determine whether the hindfoot deformity led to the forefoot deformity or vice versa. In addition, we cannot determine whether correcting the hindfoot or forefoot malalignment would correct the other deformity, or whether they would each require correction. Further clinical investigation will also be needed to assess whether these newly recognized moderately strong associations will have meaningful clinical impact. Finally, patients with severe deformities and pain may modify their foot position when standing to avoid discomfort, potentially confounding our results on WBCT.
In conclusion, there is substantial correlation between hindfoot alignment and M1 rotation. Hindfoot valgus was associated with M1 pronation, and hindfoot varus was associated with M1 supination. The implications for clinical care of these findings remain unknown at this time; however, surgeons caring for these patients should be aware of a potential association when performing complex multilevel reconstructive procedures.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007211033514 – Supplemental material for Association Between Hindfoot Alignment and First Metatarsal Rotation
Supplemental material, sj-pdf-1-fai-10.1177_10711007211033514 for Association Between Hindfoot Alignment and First Metatarsal Rotation by Neil Bakshi, Jesse Steadman, Matthew Philippi, Christopher Arena, Richard Leake, Charles L. Saltzman and Alexej Barg in Foot & Ankle International
Footnotes
Neil Bakshi, MD and, Jesse Steadman, BS, equally contributed to the development of this project.
Author Note
The investigation was performed at the Department of Orthopaedics, University of Utah, Salt Lake City, UT, USA.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alexej Barg, MD, reports other from WBCT Society, personal fees from Medartis, other from Springer Publisher, outside the submitted work. Charles L. Saltzman, MD, reports being the Editor-In-Chief of Foot & Ankle International. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.