
Abstract
Brachymetatarsia is a rare congenital condition characterized by a shortened metatarsal, most commonly affecting the fourth metatarsal bone and in some cases affecting multiple metatarsal bones. Etiology is unclear but is thought to be caused by premature closure of the metatarsal physis resulting from endocrine, congenital, or acquired conditions. 1 Its hallmark is metatarsal shortening greater than 5 mm related to the normal metatarsal parabola. 13 Usually, symptoms involve cosmetic concerns because of a dorsally displaced corresponding toe and painful callosities under adjacent normal metatarsal heads. Metatarsalgia is a common medical condition present in many foot disorders other than brachymetatarsia and refers to pain in the forefoot under metatarsal heads. 3 An accurate analysis of possible causes behind this symptom is crucial to address the problem adequately. An altered forefoot parabola, 9 as seen in brachymetatarsia, with abnormal progression of the center of pressure during the gait cycle is a common cause. 8 Treatment strategies involve conservative measures like orthotics or wider toe-box shoes, but surgical treatment is indicated when these fail. 4 The surgical goal is to remove forefoot overload and relieve pain by restoring the involved metatarsal and forefoot cascade length. 2
Forefoot reconstruction can be accomplished by lengthening the shortened metatarsal. The 2 main techniques used for this purpose are distraction osteogenesis using external fixation 6 or 1-stage metatarsal lengthening using autologous bone graft. 4 Typically, technique selection is mandated by the amount of lengthening required. When metatarsal lengthening required is less than 15 mm, the 1-stage approach can be used, with bone graft interposition and internal fixation. If lengthening of more than 15 mm is needed, progressive lengthening is recommended because of the potential soft tissue and neurovascular damage with acute lengthening of more than 15 mm. However, this technique is associated with a long duration of treatment, difficulties maintaining alignment during the distraction, pin tract infection, difficulty with shoe wear, and patient cooperation. 4
In extensive cases, an alternative to distraction osteogenesis is lengthening the shortened metatarsal to the maximum of 15 mm in a 1-stage procedure with autologous bone graft and associating it with a shortening procedure to the adjacent metatarsals to obtain the desired metatarsal parabola. The latter can be performed by open surgery with shortening procedures like Weil/triple osteotomies 11 or by minimally invasive procedures like distal metatarsal metaphyseal osteotomy (DMMO), with reasonable patient satisfaction, functional improvement, and low complication rates. 5
This article aims to describe the surgical technique of 1-stage metatarsal lengthening using autologous bone graft associated with DMMO for the adjacent metatarsals to restore a standard forefoot parabola for the treatment of brachymetatarsia.
Indications
Metatarsal lengthening should be considered for patients with brachymetatarsia and associated metatarsalgia of the adjacent normal rays, usually with painful plantar hyperkeratosis and patients with cosmesis concerns due to a dorsally displaced toe or asymmetric forefoot (Figure 1). When the desired lengthening approaches 15 mm, a DMMO can be added on multiple metatarsals at the distal diaphyseal-metaphyseal junction to balance the axial and coronal plane metatarsal formula, with a lesser chance of producing an elevation of the metatarsal head as compared with diaphyseal osteotomies.2,12 The need for lengthening the shortened metatarsal or shortening the incongruent long metatarsals is calculated as described by Maestro et al, 9 taking special care with congruency and progression of the central metatarsals and trying to balance M1 = M2 or M2 > M1, 1 to 3 mm.

Abnormal metatarsal parabola due to bilateral brachymetatarsia (left M1-M4-M5 and right M4). The left side needs approximately M4 2.2-cm lengthening to restore foot parabola, exceeding the theoretical limit for a 1-stage lengthening procedure.
Contraindications
Active infection, insufficient vascular perfusion, and the inability to comply with postoperative management are specific contraindications to this surgical technique. 2 In the presence of significant arthritis and stiffness in the associated metatarsophalangeal joints (MTPJs), there is a concern to use DMMO because of the observed increased risk of nonunion in this situation (motion then predominantly occurs at the osteotomy site rather than the MTPJ). 12
Operative Technique
The patient is positioned supine with the feet on the operating table under regional anesthesia. The affected foot is prepared and draped, and a pneumatic tourniquet to obtain a blood-free working area and hemostasis is used. Appropriate perioperative antibiotics are administered as per local guidelines. A 4-cm-long dorsal longitudinal incision is made over the proximal metaphysis of the affected metatarsal. When 2 metatarsals are involved, only 1 median incision is made over the corresponding web-space. Z-plasty elongates the extensor tendon, and the metatarsal shaft and proximal metaphysis are exposed subperiosteally.
The flexor tendon of the affected toe is cut percutaneously at the level of the proximal phalanx of the affected toe. This maneuver prevents hyperflexion deformity after lengthening the metatarsal bone due to increased flexor pulling.
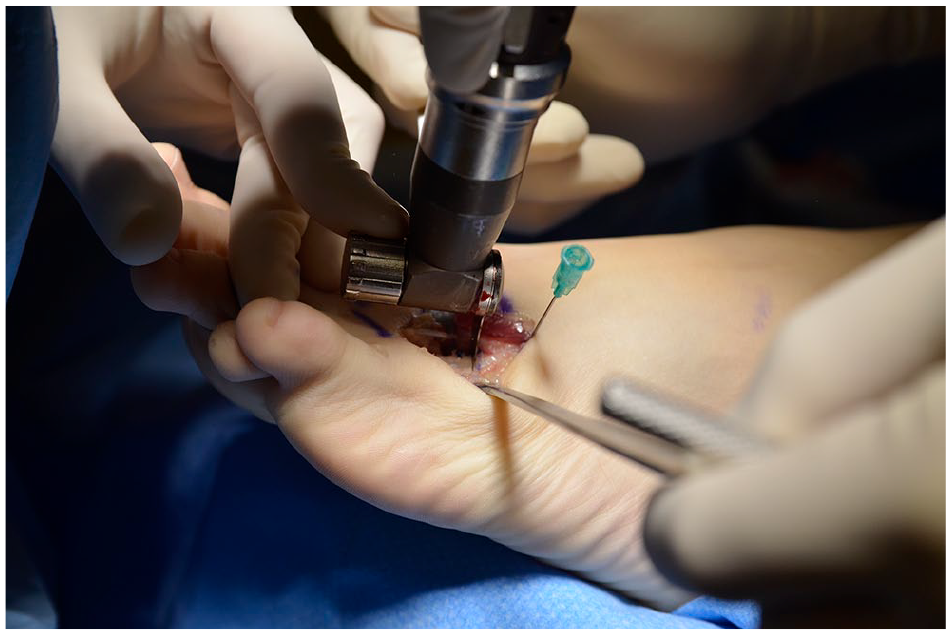
The proximal metaphyseal bone is selected as the osteotomy site given its increased healing capacity and enough room for at least 2-point fixation in the proximal metatarsal segment. First, a transverse osteotomy of the proximal metatarsal is performed using an oscillating saw (Figure 2). Then, an intramedullary 1.6-mm Kirschner wire (K-wire) is passed from the osteotomy site through the metatarsal shaft from proximally to distally up to the toe (Figure 3) and then in a retrograde fashion to cannulate the proximal metatarsal segment. This stabilization technique is beneficial when distraction is performed to prevent deformities in flexion or extension of the metatarsal and the toe as the K-wire drives the lengthening direction.
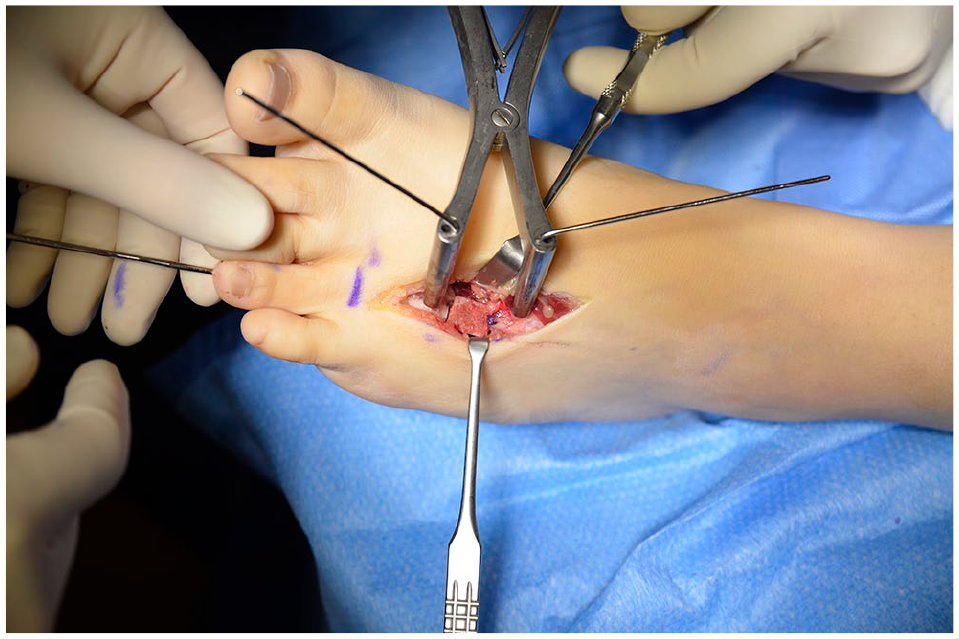
After the correct position of the intramedullary K-wire is confirmed, osteotomy distraction using a bone spreader is initiated, allowing enough time for soft tissue to adapt to the lengthening process (Figure 4). Typically, we wait after progressing on each mark on the bone spreader for about 3 to 5 minutes, taking the entire lengthening process about 20 to 30 minutes. 7
At this stage, a tricortical iliac bone graft 20 mm long is obtained. 7 To avoid soft tissue stress, the bone graft, prepared according to the preoperative planning, is never more extensive than the gap that could be created during distraction. We tailor the iliac crest graft to match the metatarsal segment, and a groove is carved on it over the cancellous bone face to “sit” over the K-wire (Figure 5). After this, the bone spreader is released, and the bone graft sits tightly between the 2 metatarsal fragments and over the K-wire (Figure 6). Then, the bone graft is secured with a straight or L-shaped 2.7 plate, with at least 2 screws at each segment (Figure 7).
The extensor tendon Z-plasty is now sutured elongated as much as needed depending on the new metatarsal length. The distal end of the K-wire is bent just beyond the tip of the toe and cut, allowing maintenance of toe alignment.
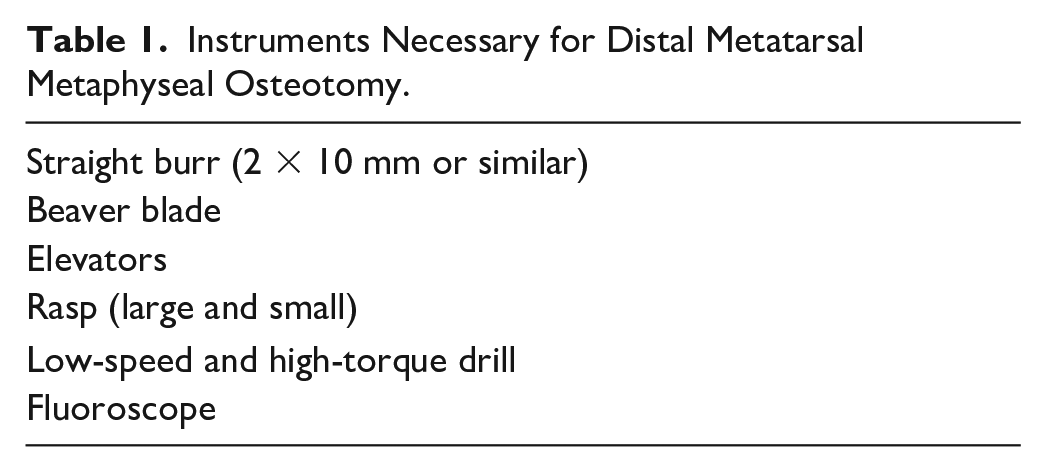
If lengthening needed to restitute metatarsal parabola is deemed to be more than 15 mm, a shortening procedure to the adjacent metatarsals is done by a DMMO (Figure 8). The instruments needed are listed in Table 1. Fluoroscopy is used to confirm the correct position of the osteotomy site on the metatarsal (MT) neck. Then, a 0.5-cm longitudinal incision is made with the beaver blade in the lateral intermetatarsal space at the side considered to perform the osteotomy. A slight rasp is then inserted and slid along the plantar and dorsal aspect of the metatarsal neck, and the periosteum is separated over a small area.2,12
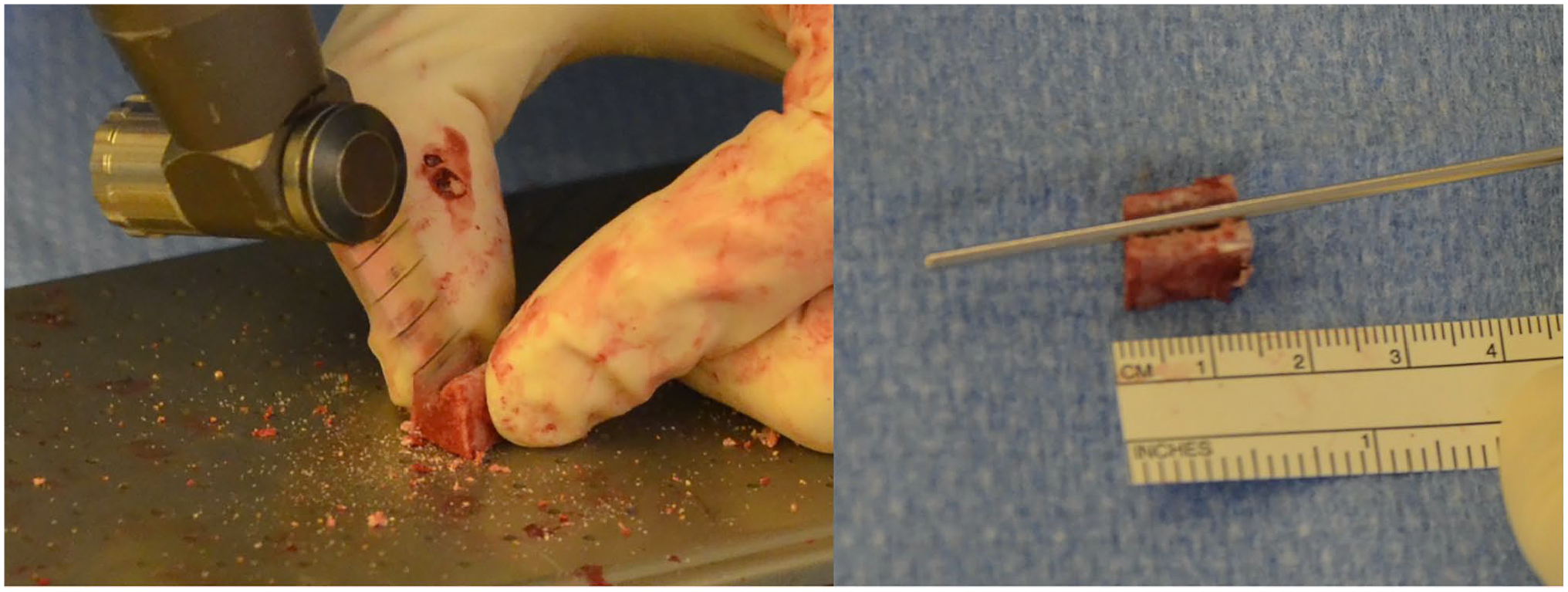
The straight 2-mm × 10-mm burr is introduced into the area cleared from the periosteum at the metatarsal neck, typically at the dorsal neck surface. The metatarsal head is held between the thumb and index finger. The osteotomy is performed in a cutting angle of usually 45 degrees relative to the long axis of the MT and a dorsal-distal to proximal-plantar direction to get enough shortening as in a Weil osteotomy. Once the osteotomy is completed, the surgeon will feel reduced resistance to metatarsal head movement. Confirmation under fluoroscopic imaging is made, placing gentle traction to the involved toe. The same procedure is repeated in the adjacent metatarsal bones as needed. Wounds are closed with a 4/0 monofilament suture and the forefoot is wrapped with an MT strap using a self-adhesive bandage.
Metatarsal osteotomy with oscillating saw.

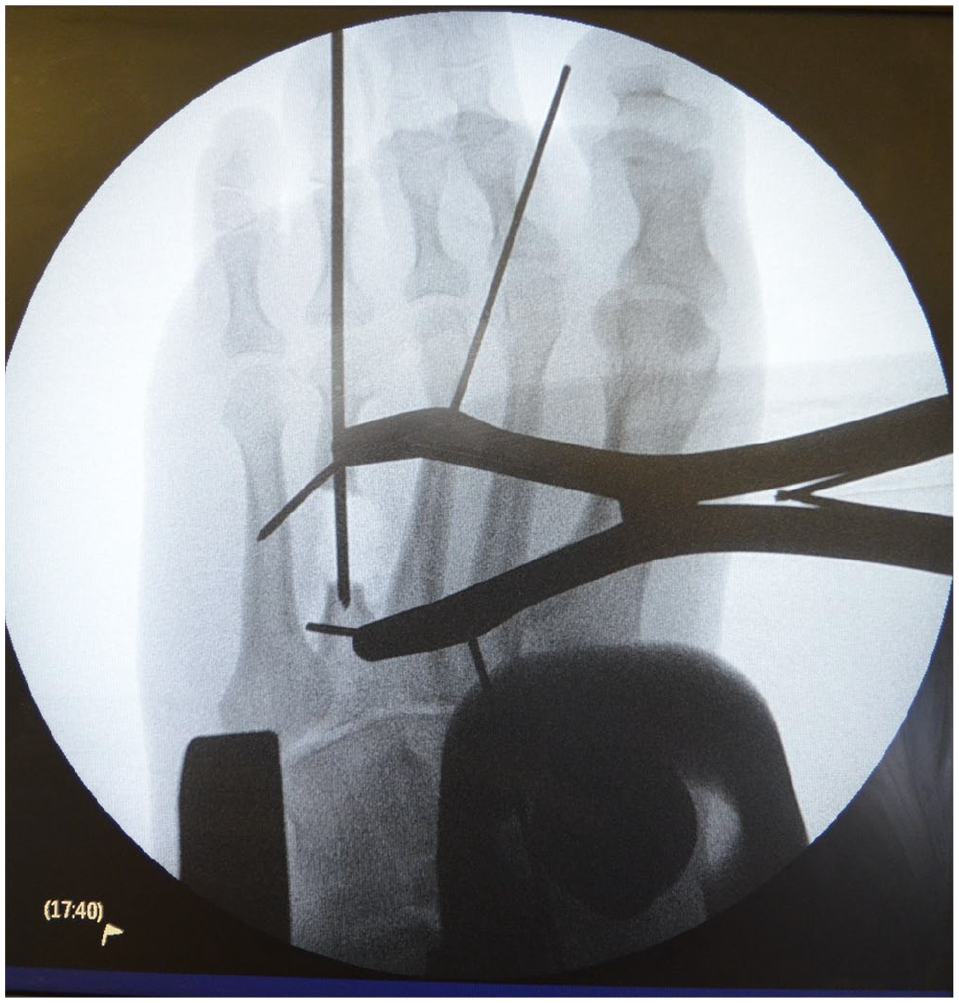
K-wire insertion through metatarsal shaft.
Metatarsal lengthening process with a bone spreader.
Iliac crest bone graft preparation to adapt the lengthened space.
Bone graft siting over K-wire.

Bone graft plate fixation over lengthened metatarsal.
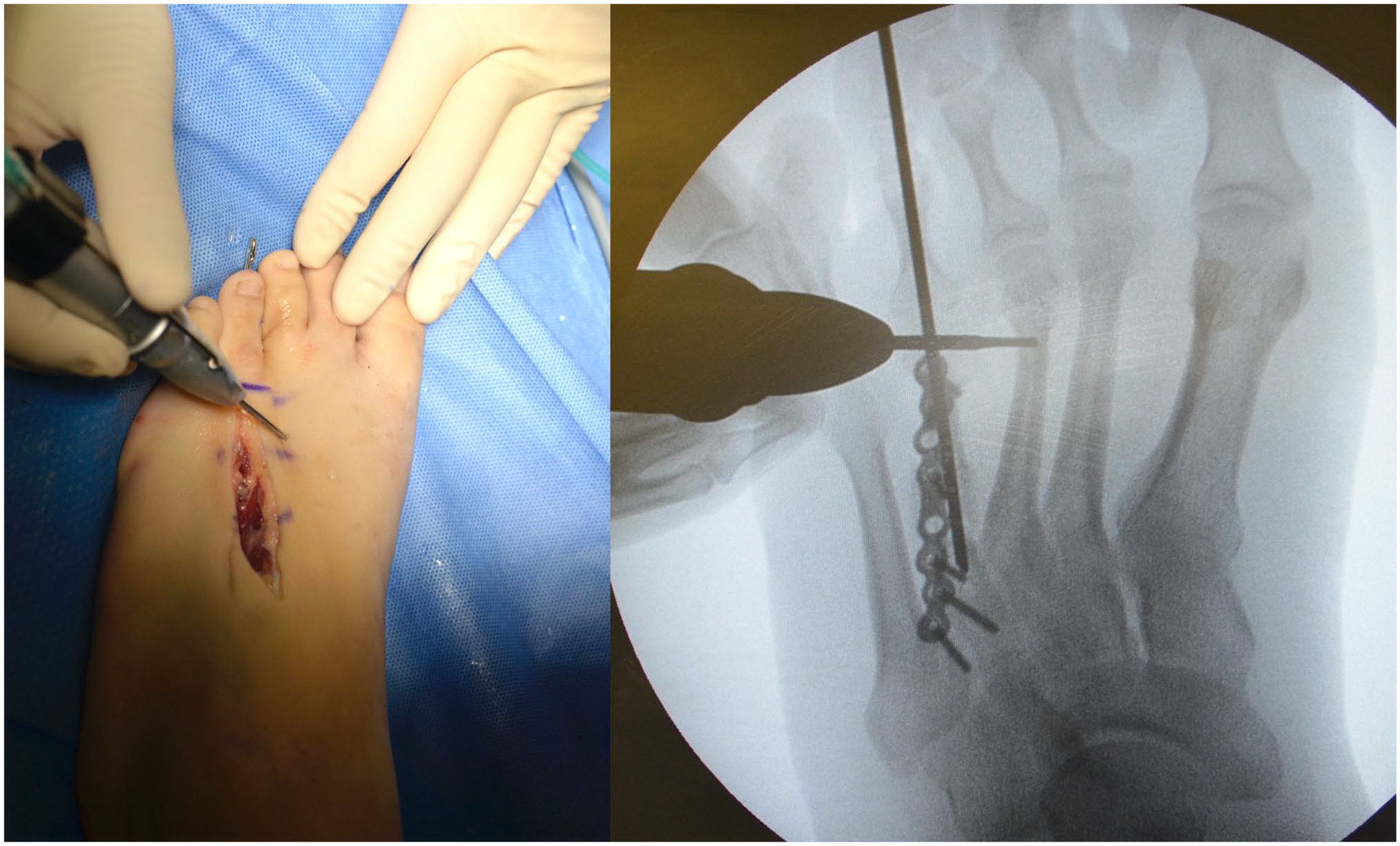
DMMO over adjacent metatarsal necks to recover adequate metatarsal parabola.
Instruments Necessary for Distal Metatarsal Metaphyseal Osteotomy.
Postoperative Management
After surgery, immediate weightbearing is encouraged in a rigid sole shoe, expecting that the osteotomized metatarsal heads reorganize according to the weightbearing pattern of the patient. Metatarsal lengths are set upon weightbearing and tension of the surrounding soft tissue structures. 10 Crutches are provided to provide stability. Six weeks after surgery, the K-wire is removed, and the patient is allowed to use other types of shoes. Physical therapy is initiated 3 weeks after surgery for gait rehabilitation and after K-wire removal, preventing toe flexion deformity and rigidity. Further outpatient consultation usually occurs at 10 and 15 weeks with periodical radiographic review to confirm complete graft union, which generally takes place around 16 weeks (Figures 9 and 10).

Radiographic progression of patient in Figure 1 after M4 one-stage lengthening and M2 to M3 distal metatarsal metaphyseal osteotomy (DMMO) preoperatively to 1 year postoperatively. Notice restoration of metatarsal parabola and complete fusion of both lengthening and DMMO.
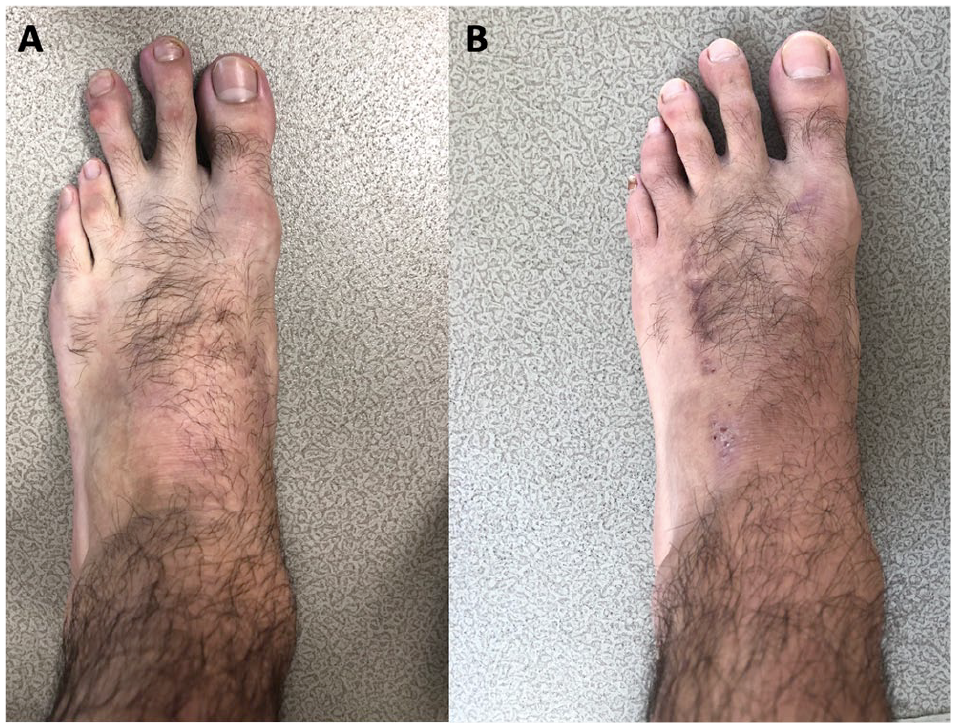
Clinical appearance (A) preoperatively and (B) 1 year postoperatively.
Conclusion
Restoring altered forefoot parabola is paramount to resolving metatarsalgia due to brachymetatarsia by removing focal overload. Doing so in a 1-stage procedure seems appropriate for patients with this condition, especially when the length discrepancy is less than 15 cm. When length discrepancy is more than 15 mm, the patient could be at risk of neurovascular damage if the lengthening process is not made in a progressive fashion. Most commonly, distraction osteogenesis through external fixation is the method of choice in such a scenario, despite being highly unpleasant to patients. As reported in this article, the alternative way is to lengthen the shortened metatarsal with an autologous bone graft up to the maximum recommended length (15 mm). Judicious shortening of the adjacent metatarsals upon necessity to restore metatarsal parabola by DMMO seems to be an excellent option to avoid neurovascular damage or phalangeal shortenings in healthy toes.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007211039526 – Supplemental material for One-Stage Lengthening and Minimally Invasive Distal Metatarsal Metaphyseal Osteotomy (DMMO) for Brachymetatarsia
Supplemental material, sj-pdf-1-fai-10.1177_10711007211039526 for One-Stage Lengthening and Minimally Invasive Distal Metatarsal Metaphyseal Osteotomy (DMMO) for Brachymetatarsia by Felipe Chaparro, Raul Espinoza, Manuel J. Pellegrini, Giovanni Carcuro and Cristian Ortiz in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.