
Abstract
Background:
There have been no studies evaluating the usefulness of grayscale radiographs in extremity fractures. We aimed to compare the ability and reliability of traction radiographs vs traction grayscale inversion radiographs to detect fracture fragment and comminution zones in comminuted tibia pilon fractures.
Methods:
Plain radiographs and grayscale inversion images of 60 patients with Orthopaedic Trauma Association/AO Foundation type C3 fracture were evaluated by 20 observers (15 orthopaedic surgeons and 5 radiologists) after traction had been applied. The anterolateral, posterolateral, and medial malleolar fragments, as well as the lateral, central, and medial column comminution zones, were identified by all physicians. Computed tomography scan images were used as the “gold standard” against which plain radiographs and grayscale inversion image interpretation were measured. Intra- and interobserver reliability and correct identification of fracture fragments and comminution zones were evaluated.
Results:
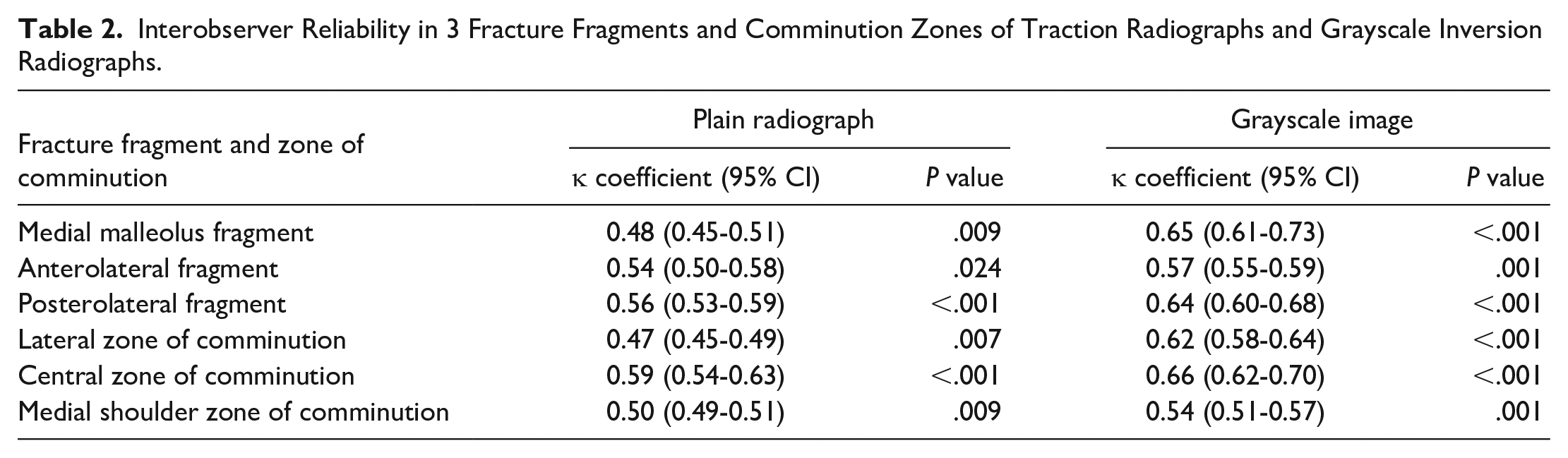
The interobserver reliability for 3 of the fracture fragments and comminution zones on the traction plain radiographs was moderate, whereas it was substantial on traction grayscale inversion radiographs. The lateral comminution zones (P = .001) and presence or absence of posterolateral fragments (P < .001) were significantly better identified in grayscale inversion radiographs compared to standard radiographs.
Conclusion:
After traction was applied, we found grayscale inversion radiographs are superior to plain radiographs in the identification of posterolateral fragment and lateral zone of comminution in comminuted intraarticular pilon fractures.
Level of Evidence:
Level III, retrospective case series.
Keywords
Grayscale inversion is a simple transformation of plain radiographs that provides dark structures on a bright background instead of standard bright-on-dark presentation, 14 and it is a readily accessible tool in picture archiving and communication system (PACS). It is simple and readily accessible and does not require additional radiation exposure. In addition, it does not increase diagnostic and treatment costs.
Usefulness of grayscale inversion radiographs has been evaluated in different areas of medicine. Park et al 10 assessed the efficacy of grayscale inversion rib series for the detection of rib fractures after minor chest trauma. They reported an increased accuracy for rib fracture detection when conventional and inverted grayscale radiographs are combined. In their study, Lungren et al 7 evaluated the usefulness of grayscale images in the detection of pulmonary nodules. They reported a higher sensitivity for grayscale inversion radiographs than the plain radiographs. Also, the effectiveness of inverted grayscale radiographs was studied in the evaluation of proximal junctional kyphosis and spinopelvic parameters in the adult population.12,14 It has been suggested that grayscale inversion view is a more reliable tool than standard radiographs for the evaluation of proximal junctional kyphosis. 14 In addition, it was reported that grayscale images provided improved intra- and interobserver reliabilities in the measurement of spinopelvic alignment when compared with standard radiographs. Recently, Misir et al 9 analyzed the effectiveness of traction radiographs in pilon fractures. They reported that traction radiographs are less reliable than computed tomography (CT) in terms of fracture fragment and comminution zone identification. There have been no studies regarding the usefulness of grayscale inversion radiographs in the detection of fracture fragments and comminution zones in periarticular fractures.
In this study, we aimed to compare the ability and intra- and interobserver reliability of traction radiographs and grayscale inversion radiographs to detect fracture fragment and comminution zones that present on CT images in comminuted tibia pilon fractures.
Materials and Methods
The study was started after approval from the Uludag University Clinical Research Ethics Committee (approval number: 2020-12/13, approval date: August 7, 2020). The inclusion criteria for the study were (1) patients who were admitted for Orthopaedic Trauma Association (OTA)/AO Foundation (AO) type C3 pilon fracture (2) between January 2018 and June 2020, (3) who were skeletally mature (≥18 years old) at the date of admission and (4) available plain radiographs and CT images after ankle spanning external fixator applied. Exclusion criteria were (1) patients under 18 years old, (2) open fracture, (3) previous ankle surgery, and (4) inadequate radiological records. Patient selection process is shown in Figure 1. After inclusion and exclusion criteria were applied, 60 patients’ radiological records were evaluated.
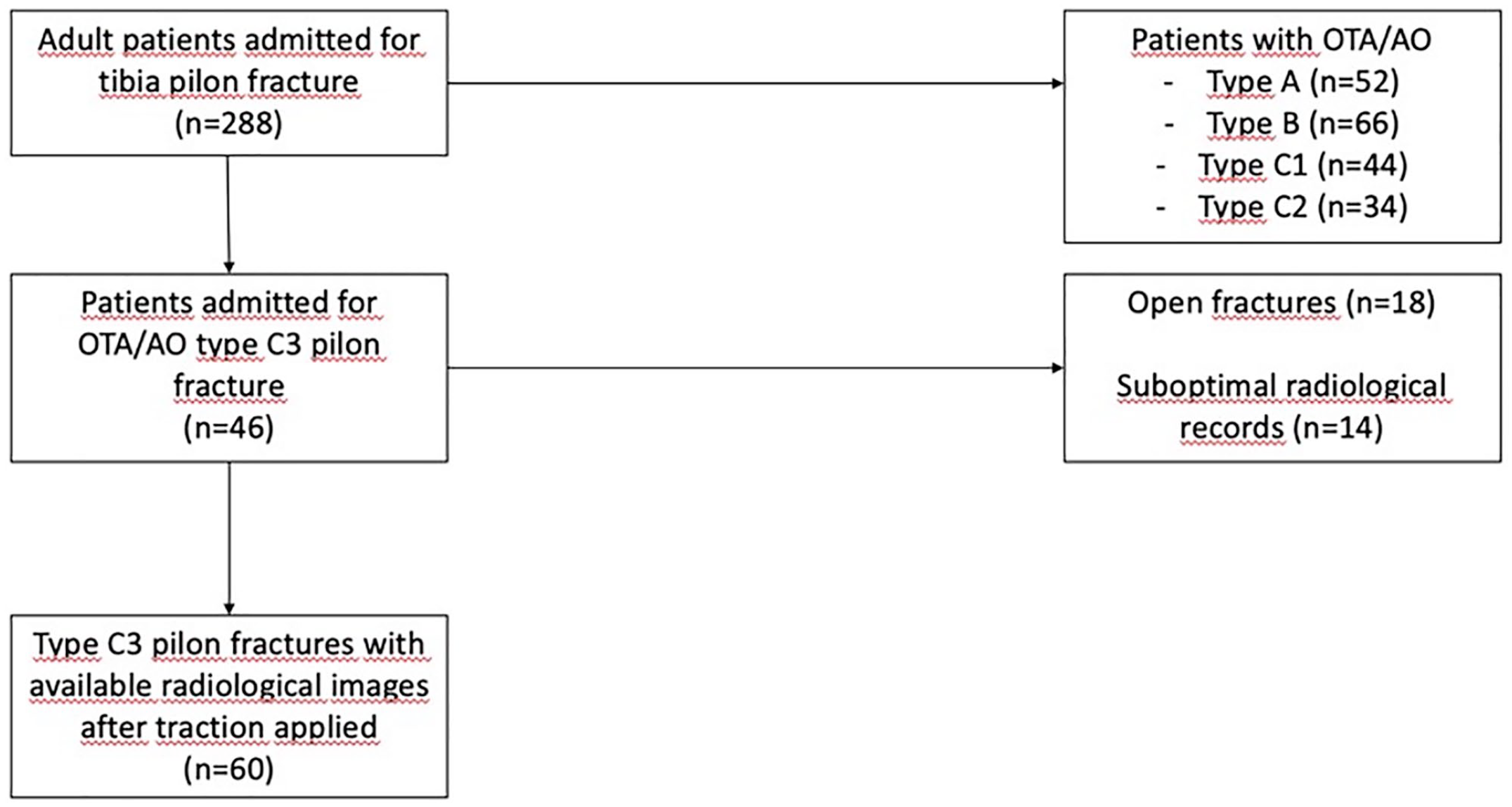
Flowchart of the patient selection process. OTA/AO, Orthopaedic Trauma Association/AO Foundation.
The traction radiographs included 2 standardized anteroposterior (AP) and lateral images taken with a spanning external fixator applied. Traction images were performed under general or regional anesthesia in the operating room. All images were obtained using a radiographic image intensifier (Shimadzu Collimator R 300; Shimadzu Corporation) at a distance of 51 cm and were stored in the PACS. CT scans were from 5 cm above the ankle joint to the subtalar joint. CT scans were obtained before skeletal traction application, at the emergency service.
Three presentations were prepared with the PACS system. The first presentation contained AP and lateral traction radiographs, and the second presentation contained AP and lateral views of the inverted grayscale images. The order of the images was randomized, and the name of the patients and postoperative radiographs were hidden.
Twenty observers (5 orthopaedic trauma surgeons, 10 general orthopaedic surgeons, and 5 radiologists) were selected as participants. All participants systematically evaluated the images in the same dark room, and a high-resolution monitor based on the first author’s (G.E.) instructions and opportunity to use the PACS system tools were provided. They were asked to identify (1) the presence or absence of a posterolateral, anterolateral, or medial malleolus fragment and (2) the presence or absence of a lateral, central, or medial shoulder zone of comminution. Comminution was defined as the areas where the fracture fragments were less than 10 mm in diameter and gaps between reduced fragments. 2 Accurate identification of fracture fragments and comminution zones (gold-standard decision) was made according to the decisions obtained using CT images at the beginning of the study from the absolute agreement created by the joint decision of a trauma surgeon, a general orthopaedic surgeon, and a radiologist. The evaluations made by the observers on traction radiographs and grayscale radiographs were compared with the gold-standard decisions. Accuracy was determined for the individual fracture fragments and comminution zones. Plain radiographs, grayscale inversion views, and CT image examples of 2 patients are shown in Figure 2 and Figure 3.
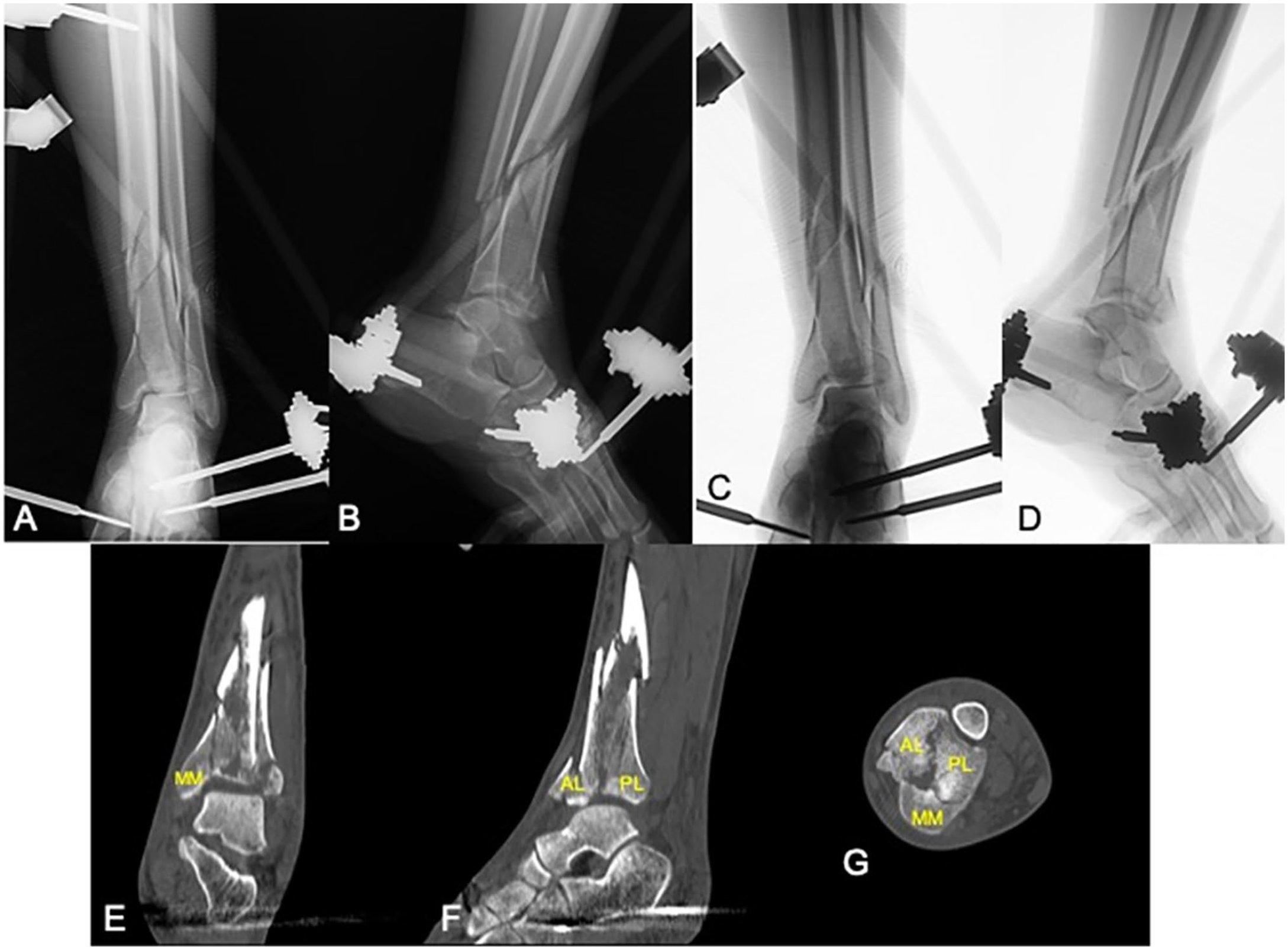
(A, B) Traction radiographs (anteroposterior [AP] and lateral), (C, D) grayscale inversion radiographs (AP and lateral), and (E) coronal, (F) sagittal, and (G) axial computed tomography (CT) images of a patient without significant comminution. As shown on the CT images, medial malleolus (MM), anterolateral (AL), and posterolateral (PL) fragments were requested to be marked on the traction radiographs, inverted grayscale radiographs, and CT images.
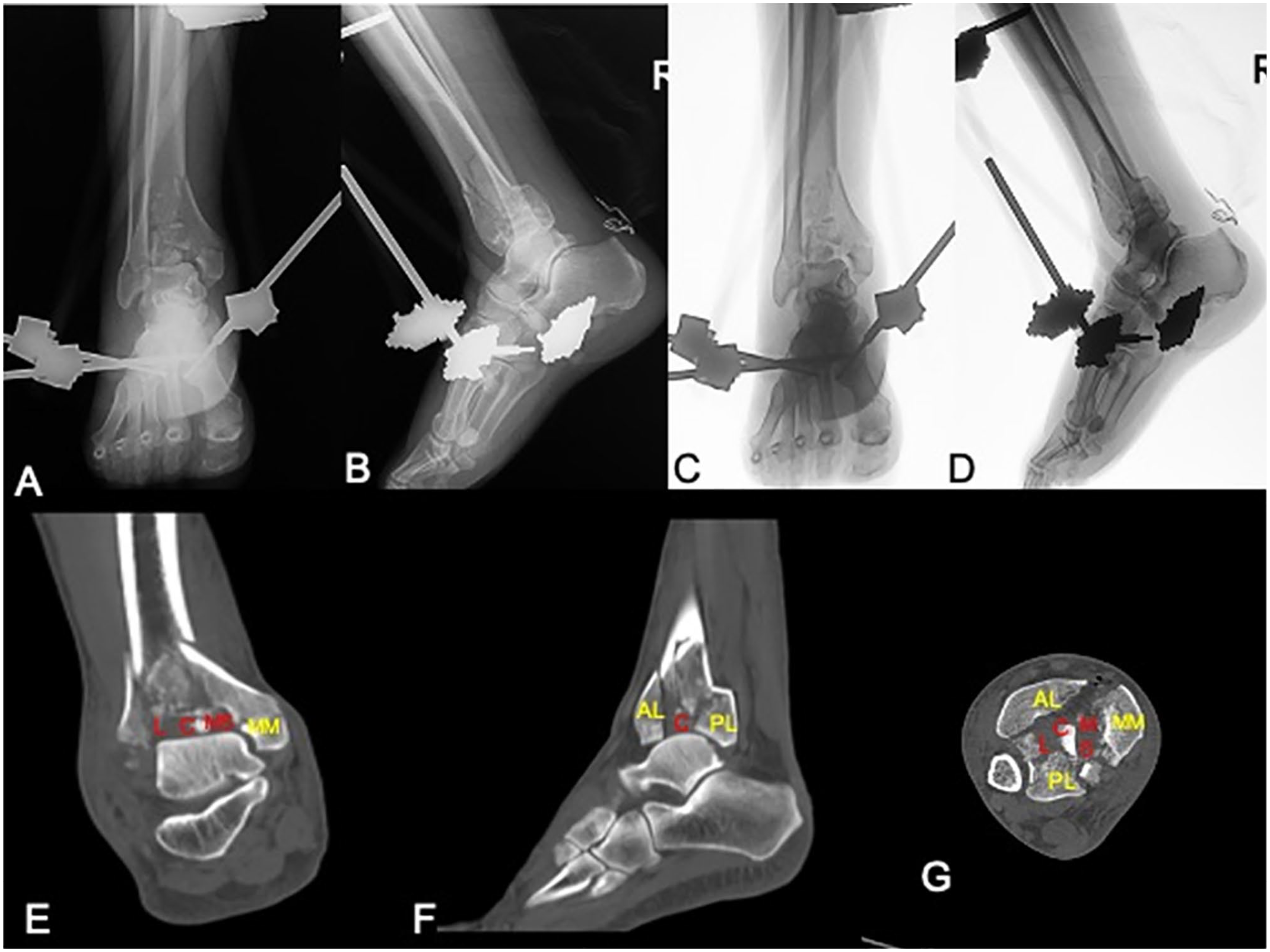
(A, B) Traction radiographs (anteroposterior [AP] and lateral), (C, D) grayscale inversion radiographs (AP and lateral), and (E) coronal, (F) sagittal, and (G) axial computed tomography (CT) images of a patient with significant comminution. As shown on the CT images, medial malleolus (MM), anterolateral (AL) and posterolateral (PL) fragments, and lateral (L), central (C), and medial shoulder (MS) comminution zones were requested to be marked on the traction radiographs, inverted grayscale radiographs, and CT images.
The observers were first asked to evaluate the plain radiographs. Then, they evaluated the second presentation, which contained grayscale images. All participants completed the presentations twice within a 2-week interval. The order of cases was randomized before the second evaluation and before the third evaluation for each participant.
Statistical Analysis
The descriptive statistics used were mean, standard deviation, median, lowest and highest value, frequency, and ratio. Intraobserver and interobserver reliability for the identification of fracture lines and comminution zones on traction radiographs and inverted grayscale radiographs were calculated using Fleiss κ coefficients. Values were assigned in the following manner: poor (0.01-0.20), fair (0.21-0.40), moderate (0.41-0.60), substantial (0.61-0.80), and nearly perfect (0.81-1.00) based on the strength of agreement. The χ2 test was used for qualitative independent analysis, while the McNemar test was used for qualitative dependent analysis. A P value <.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS software (version 22 for Windows; SPSS, Inc).
Results
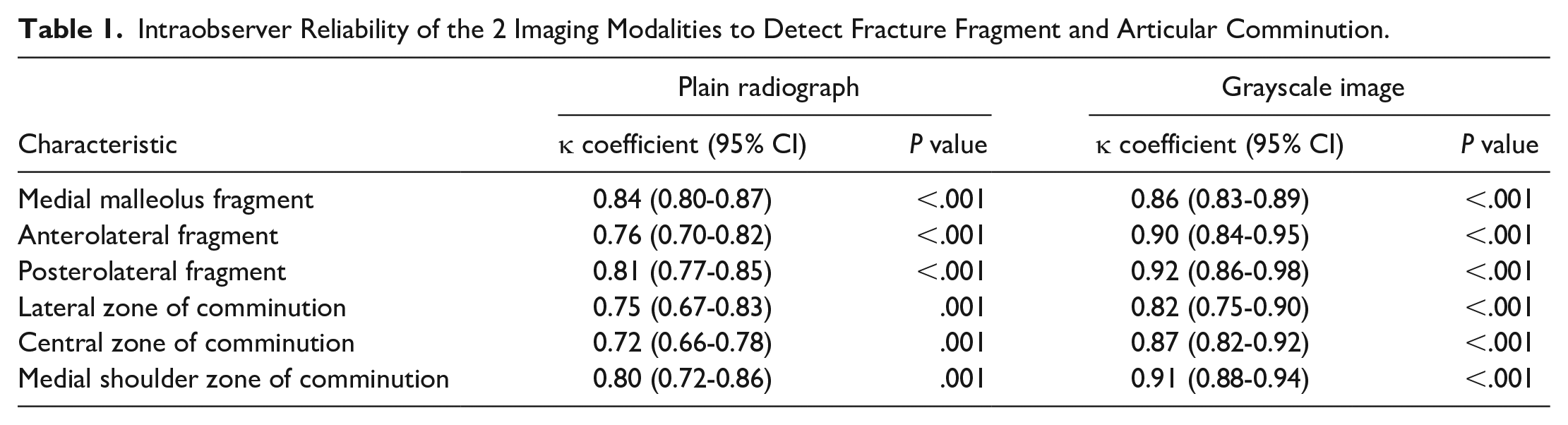
There was high intraobserver and moderate interobserver reliability in the identification of fracture fragments and comminution zones. The intra- and interobserver reliability of the 2 imaging modalities to detect specific fracture fragments or zone of comminution are summarized in Tables 1 and 2.
Intraobserver Reliability of the 2 Imaging Modalities to Detect Fracture Fragment and Articular Comminution.
Interobserver Reliability in 3 Fracture Fragments and Comminution Zones of Traction Radiographs and Grayscale Inversion Radiographs.
The accuracy of observers’ assessment regarding the presence or absence of posterolateral fragment was 62% with use of plain radiographs and 77% with use of the grayscale inversion images (P < .001). The accuracy regarding the anterolateral fragment presence was 72.5% in the grayscale inversion radiographs and 80% in the traction radiographs (P = .125). We also found no difference in the accuracy of the diagnosis of a medial malleolar fragment on traction plain radiographs vs traction grayscale inversion radiographs. (50% vs 47%, P = .191) (Table 3).
Accuracy Rates for Fracture Fragment and Zone of Comminution Identification on Plain Traction Radiographs and Grayscale Inversion Radiographs. a
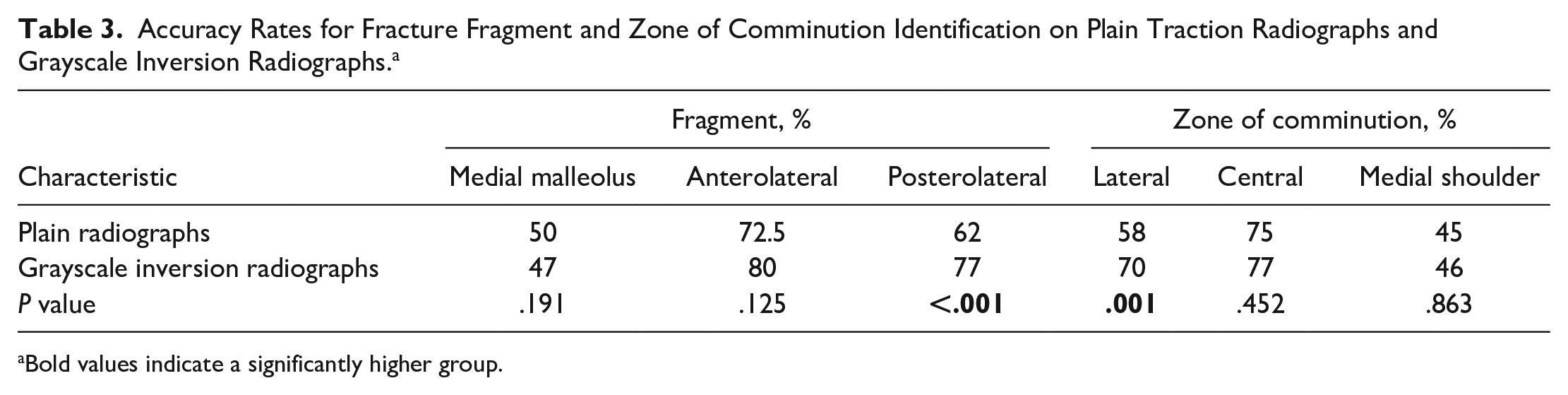
Bold values indicate a significantly higher group.
In assessing specific comminution zones, the correct definition of the medial shoulder and central zones of comminution was similar in the traction plain radiographs (45% and 75%, respectively, P = .863) and the traction grayscale inversion radiographs (46% and 77%, respectively, P = .452). However, the correct definition of lateral comminution zone was better in the traction grayscale inversion radiographs (70%) than in the traction plain radiographs (58%, P = .001) (Table 3).
Discussion
The most important findings of this study were that grayscale inversion images provide more accuracy than plain radiographs to detect a posterolateral fragment and identify the lateral zone of comminution. The possible explanation of the superiority of the grayscale image may be that optimal contrast perception is obtained when looking a dark image in the bright background. 1
Correct identification of fracture patterns is crucial for preoperative planning in the management of pilon fractures. CT is widely used in evaluating pilon fractures, and some authors recommend its routine use.2,8 Leonetti and Tigani 6 proposed a new classification system based on CT that is simple, is reliable, and has a higher prognostic value than classic classification systems. Although CT scan provides detailed information about fracture patterns and degree of articular communion, it has a high dose of radiation and increases costs of treatment. 11 Konda et al 5 reported the same performance with ultra-low-dose CT in fracture management. However, ultra-low-dose CT is not accessible in most cases. The findings obtained in this study show that grayscale images that can be easily obtained from direct radiographs can be helpful in identifying fracture fragment and comminution zones.
In the presence of posterolateral fragment, reduction and temporary fixation of the posterolateral fragment is recommended as the first step of the articular reduction. 13 Guan et al 3 reported satisfactory results with the use of the combined posterolateral and anterior approach which posterior cortical reduction takes the first place. Ketz and Sanders 4 conclude that proper reduction of the posterolateral fragment is a reference point for the remainder of the surgery. Therefore, recognition of the posterolateral fragment is very important for deciding the overall treatment plan, choice of surgical approach, and selection of implants. We have found that grayscale images have a higher sensitivity to detect posterolateral fragments compared to plain radiographs. When CT is not available or a high dose of radiation is a concern, such as for pregnancy, grayscale inversion radiographs may be useful in the correct identification of the posterolateral fragment.
In our study, the intraobserver reliability in the identification of the fracture fragments and comminution zones was high, and interobserver reliability was moderate. Our results were similar to the literature. Misir et al 9 reported that the interobserver reliability in the identification of the 3 specific fracture fragments and comminution zones was moderate.
This study has some limitations. First, the most complicated type of pilon fracture pattern was evaluated. Only 1 type of fracture pattern was included in the study. Analyses including other types of pilon fractures could provide additional information on the usefulness of grayscale inversion radiographs. Second, 3-dimensional CT reconstruction was not used. More advanced studies may be performed by comparing 3-dimensional CT with other modalities that we used. Third, oblique views were not used, and these views may be helpful for evaluating the anterior lateral cortex of the tibia. Fourth, we think that posterolateral fragment assessment was better with the evaluation of the lateral x-ray because AP x-ray images were obscured by the fibula and talus. This is a disadvantage of x-ray.
Conclusion
Grayscale inversion radiographs are found to be superior to plain radiographs in the identification of posterolateral fragment and lateral zone of comminution in comminuted intra-articular pilon fractures. A combination of traction and grayscale inversion radiographs can be used reliably and cost-effectively in the fracture fragment and comminution zone identification. Despite the findings of this study, CT remains the gold-standard imaging modality to understand the morphology of pilon fractures.
Supplemental Material
sj-docx-1-fai-10.1177_10711007211049247 – Supplemental material for Comparison of Computed Tomography, Traction, and Inverted Grayscale Radiographs for Understanding Pilon Fracture Morphology
Supplemental material, sj-docx-1-fai-10.1177_10711007211049247 for Comparison of Computed Tomography, Traction, and Inverted Grayscale Radiographs for Understanding Pilon Fracture Morphology by Gokay Eken and Abdulhamit Misir in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.