
Abstract

Keywords
Introduction
Lesser tarsometatarsal (TMT) arthritis—whether from a degenerative or traumatic origin—can lead to chronic pain and disability. 2 Patients may require operative intervention, most commonly TMT arthrodesis, after failing nonoperative therapies. 2 Although there is a storied history of studies about first metatarsal fusions, there are far fewer with regard to the lesser TMT joints.
With an overall nonunion rate ranging from 3% to 8%, and as high as 11.4% in other studies, determining proper management for TMT arthritis can be a challenging problem.2,6 Although many fixation options exist—including plates, screws, Kirscher wires, and staples with or without autologous vs allograft bone graft—no construct has proven superior to others in lowering nonunion rates. 6 One specific technique, first described by Cloward in neurosurgery literature for acute fractures of the cervical spine, entails the use of a bone dowel and for an interbody fusion. 3 This technique has since been adapted to various areas of the human body, including the foot and ankle literature. 2 For instance, Johnson and Johnson 5 described the use of an autologous iliac crest bone dowel graft supplemented by cross-wire fixation for the treatment of posttraumatic TMT arthritis. Similarly, Withey et al 8 described techniques that used this autologous interbody for lesser TMT fusion with a staple construct made from Kirschner wires and compression plating.
Continuous compression devices (CCDs) have promising biomechanical data, 1 but no study has specifically evaluated their efficacy in achieving adequate postoperative union for lesser TMT fusions.6,7 Additionally, bone marrow aspirate concentrate (BMAC) has also shown promise in the care of bone defects and nonunion. 5 Therefore, the purpose of this study is to describe the application of this technique for lesser TMT fusions using autologous bone dowel, CCDs, and BMAC. In addition, we provide data—primarily nonunion rates and time to postoperative union—from a cohort of patients who underwent surgery for lesser TMT arthritis.
Materials and Methods
Institutional review board oversight was used during the completion of this work (Oklahoma State University Center for Health Sciences IRB #2021061).
Indications
TMT joint degeneration can cause significant pain and functional impairment. This condition is typically managed in the initial stages with conservative measures such as rocker-bottom shoes, orthoses, and analgesics. Arthrodesis of the lesser TMT joints is indicated in the setting of joint arthritis, which has failed these conservative measures and is causing significant impairment to a patient’s activities of daily living.
Contraindications
Although many patients with severe lesser TMT joint arthritis are candidates for operative fusion, several contraindications exist. For instance, this technique may not be applicable in the instance of infections, severe bone loss, or poor bone quality.
Operative Technique
After transport to the operating room, the patient was positioned supine with a bump underneath the ipsilateral hip. A nonsterile tourniquet was placed around the thigh and the foot was sterilely prepped and draped. A standard 3- to 4-cm longitudinal incision was made directly over the second or third TMT joints. An alternative incision may also be made halfway between the second and third rays if both are to be fused and using the single-incision approach seen in Figure 1A.
The neurovascular bundle was then carefully dissected and the extensor hallucis brevis tendon was identified and retracted to gain access to the second or third TMT joint. Pertinent structures to be avoided include the extensor hallucis longus tendon, dorsalis pedis artery, and the medial branch of the superficial peroneal nerve (Figure 2A).
Any dorsal osteophytes were removed forming a continuous, flat surface from the cuneiform to the proximal metatarsal. The graft was then sized using an operative ruler to determine the largest-diameter graft that would remain within the cortex of the cuneiform and metatarsal base.
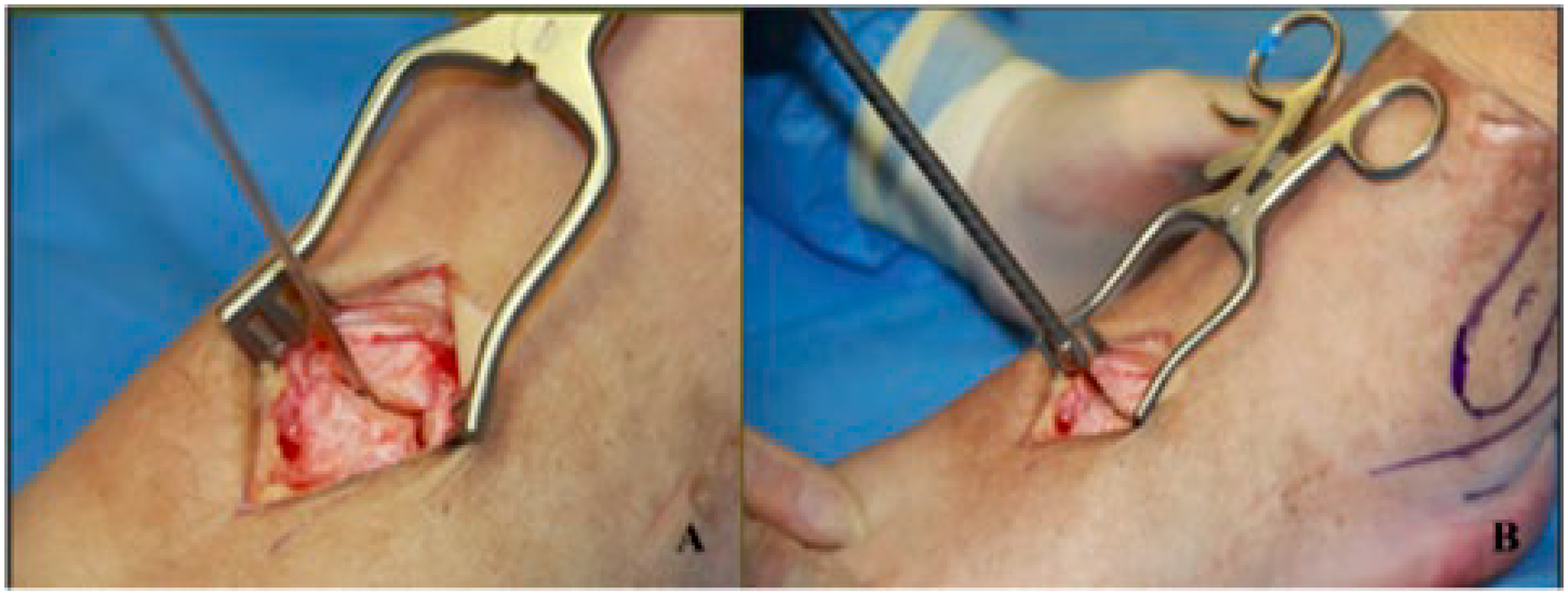
For calcaneal bone dowel graft harvest, an incision approximately 2 cm distal to the tip of the fibula over the calcaneal tuberosity was made and special care was taken not to injure the sural nerve—which runs approximately 1 cm distal to the tip of the fibula (Figure 1B.). Fluoroscopy may be used to aid in the placement of the graft harvester within the calcaneal tuberosity. The Arthrex OATS system (Arthrex) has either 6-, 8-, or 10-mm harvesters, with 8 mm size being most commonly used. The size of the graft is determined intraoperatively such that the bone dowel graft straddles the affected joint symmetrically. We advocate for the largest-diameter reamer that will fit within the joint but does not cross adjacent TMT joints.
Using a mallet, the donor harvester was driven into the calcaneus until the harvester abuts the far cortex of the calcaneus. The harvester was then removed and the bone dowel was subsequently cleaned of all soft tissues (Figure 3). Of note, if fusion of more than 1 joint is desired, the bone dowel may be cut into 2 pieces using a sharp operative blade. Otherwise, the bone dowel graft may be left intact if fusing a single joint. Next, the autograft was placed in BMAC harvested from the ipsilateral iliac crest. The bone dowel graft is soaked in the BMAC solution for approximately 5 minutes. After the bone dowel has been inserted, the remaining BMAC solution is used to bathe the affected joint.
To place the graft and hardware, a guide wire was centered between the cuneiform and metatarsal base (Figure 4A). This step can be accomplished with a driver attachment and power, but often can be done without power. We recommend confirming the position of the wire using fluoroscopy to ensure placement within the joint center and the correct metatarsal ray. The OATS system reamer and harvester sizes are determined by centering the drill over the middle of the affected joint, such that one-half of the bone dowel graft comes from each side of the joint. The reamer and harvester are the same size and both are provided in the same OATS system.
Once the position was confirmed, the cannulated reamer was advanced over the wire and reamed to the plantar surface of the TMT joint (Figure 4B). Excess debris and cartilage should be removed (Figure 2B). Of note, the joint can be distracted using traction and plantarflexion on the affected ray during bone dowel insertion. A tamp may be used to assist with bone dowel insertion (Figure 2C). Care should be taken to not break or smash the bone dowel while inserting within the trephinate.
Once the bone dowel is flush or near flush with the dorsal cortex of the TMT joint, a Nitinol staple was measured. The staple should span a minimum of 4 mm on either side of the bone dowel. For example, if an 8 mm diameter bone dowel is used, a minimum 16-mm-wide staple should be used.
Once the appropriate-sized staple was determined, the staple was placed longitudinally using the staple’s insertion guide, drill holes, tamp, and mallet (Figure 2D). The skin incision was closed in the appropriate fashion. Figure 5 demonstrates adequate placement of the bone dowel with ideal placement of the staple tyne symmetrically placed over the affected TMT joints.
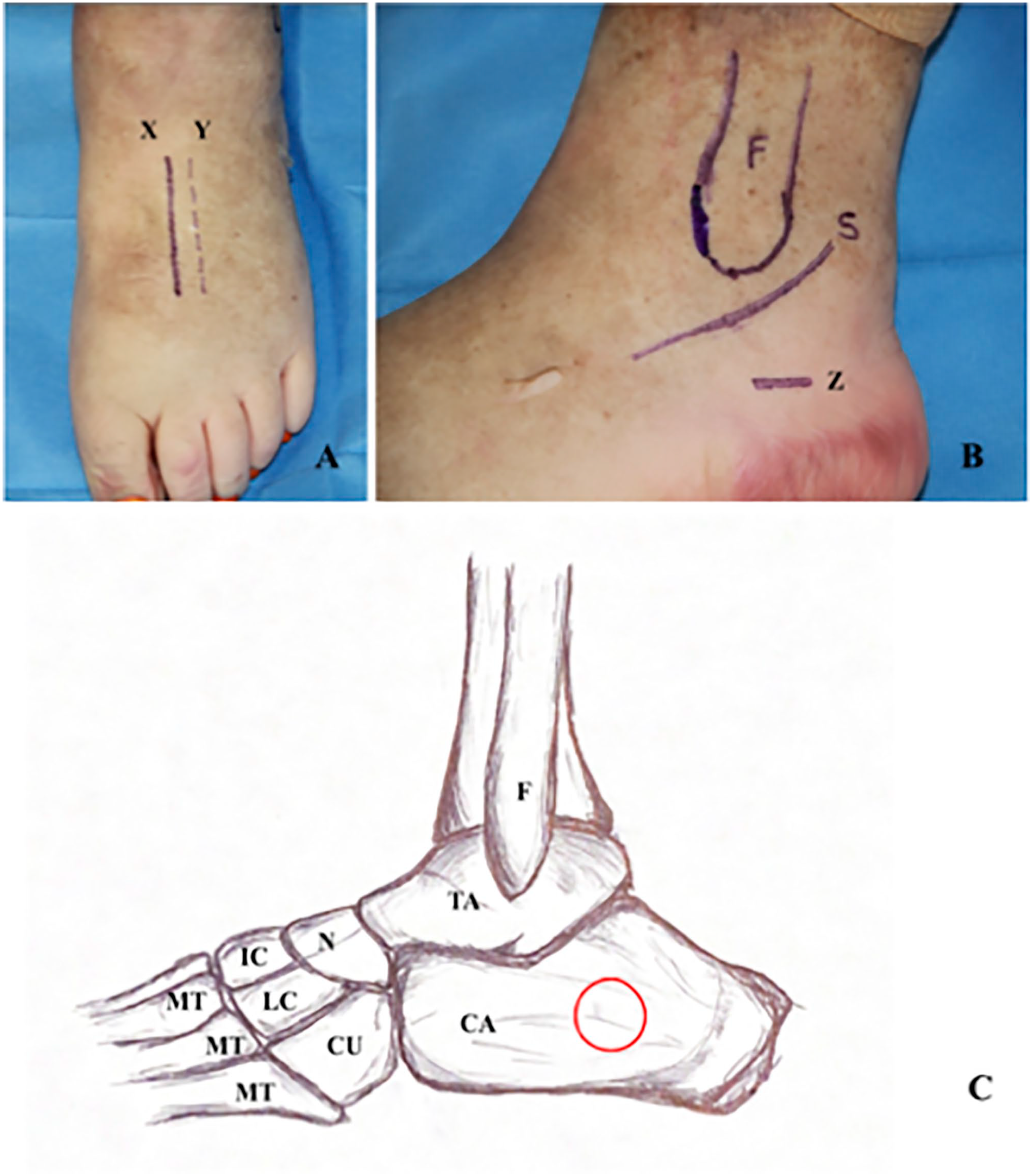
(A) Solid line represents the dorsal incision used to access the second TMT joint. Dotted line represents an accessory incision used to access the second and third TMT joints. (B) Solid line (Z) represents incision for calcaneal bone graft harvest taking care not to damage the sural nerve (S). (C) Diagrammatic illustration of lateral view of calcaneal bone dowel-graft harvest site, as indicated by the circle. Abbreviations: CA, calcaneus; CU, cuboid; F, fibula; IC, intermediate cuneiform; LC, lateral cuneiform; MT, metatarsal; N, navicular; S, sural nerve; TA, talus; TMT, tarsometatarsal.
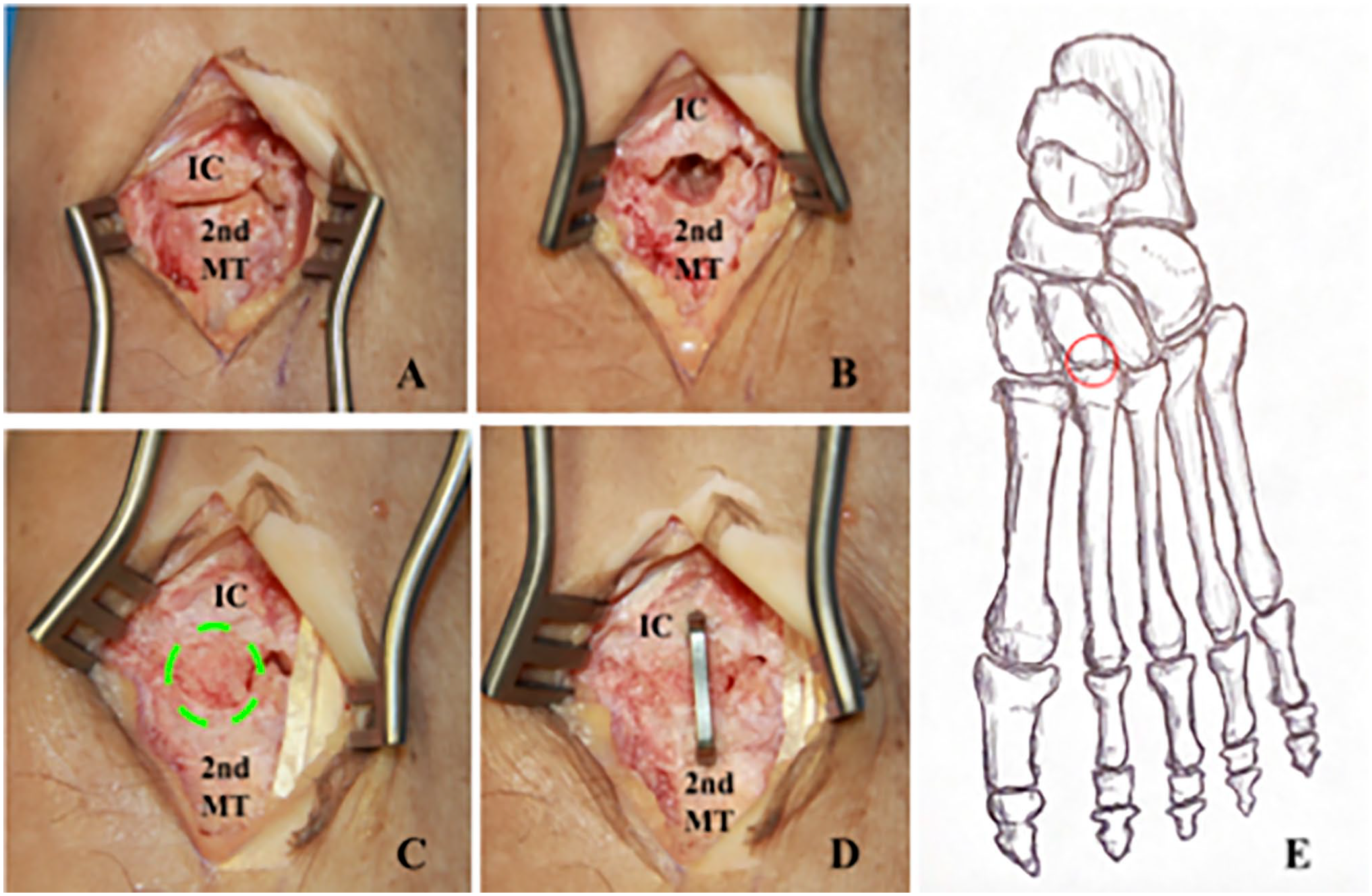
(A) Exposed second tarsometatarsal joint with dorsal osteophytes removed. (B) Trephinated joint status post reaming. (C) Trephinated joint with bone dowel in place (as indicated by green dashed circle) of void created during the reaming step. (D) Final placement with compression staple bisecting bone dowel and spanning articulation between the base of the second metatarsal and the intermediate cuneiform. (E) Diagrammatic illustration of anterior-posterior view of the dorsum of the foot showing the dowel-graft placement between the articulation of the second metatarsal base and the intermediate cuneiform, as indicated by the circle. Abbreviations: 2nd MT, second metatarsal; IC, intermediate cuneiform [See online article for color figure.].

Calcaneal bone dowel autograft.
(A) Intraoperative image demonstrating guidewire placement centered between the intermediate cuneiform and second metatarsal base. (B) Intraoperative image demonstrating the cannulated reamer after advancement over the guidewire down to the dorsal surface of the tarsometatarsal (TMT) joint.

Anterior posterior radiograph demonstrating postoperative fusion of the second and third TMT joints using the nitinol compression staple and bone dowel graft. Radiograph demonstrates adequate placement of the bone dowel with ideal placement of the staple tyne symmetrically placed over the affected TMT joints. TMT, tarsometatarsal.
Postoperative Protocol
Postoperatively, patients were placed in a stirrup plaster splint and scheduled for their first postoperative follow-up visit 7 days after surgery. Patients were instructed to remain completely nonweightbearing on the operative extremity. At the first postoperative visit, patients were transitioned to a short leg cast and instructed to remain nonweightbearing. Patients remained nonweightbearing for an additional 4 weeks, after which the short leg cast was removed and the patient was transitioned to a walking boot and allowed to progressively weightbear on the operative extremity while wearing the boot. Ankle range of motion and strengthening exercises were encouraged.
Clinical Data
Retrospective chart review was performed on patients treated with arthrodesis for lesser TMT fusion from January 2015 to January 2020. Data from 10 patients undergoing the novel technique—the Nitinol staple, BMAC, and calcaneal bone dowel—were included. Each patient underwent radiographic review by at least 2 authors (J.C.T and J.S.)—none of whom were the primary surgeon—to determine time to radiographic union. Disagreements were subject to review by a third author (B.H.) and settled by consensus agreement. Radiographic healing was assessed using standard anteroposterior, lateral, and oblique views of the operative foot and defined as bridging bone across a minimum of 3 cortices. Nonunion was determined if the above criteria were not met by the last follow-up (minimum 6 months postoperatively). Time to fusion was calculated as the time between the day of surgery and the first instance of radiographic union as defined above.
Of the 10 patients included in our sample, 21 joints were fused using the novel technique described above. Eleven joints (of 21; 52.3%) resulted from degenerative arthritis whereas the remaining 10 joints (of 21; 47.6%) resulted from posttraumatic changes (Table 1). The average age of patients included was 50.9 years (SD 9.6). Average time to fusion among all lesser TMT joints was 56.2 days (SD 13.9) following surgery. All lesser TMT joints included in our sample went on to radiographic fusion by 6 months after surgery (Table 2).
Patient Demographic Data (N = 10). a
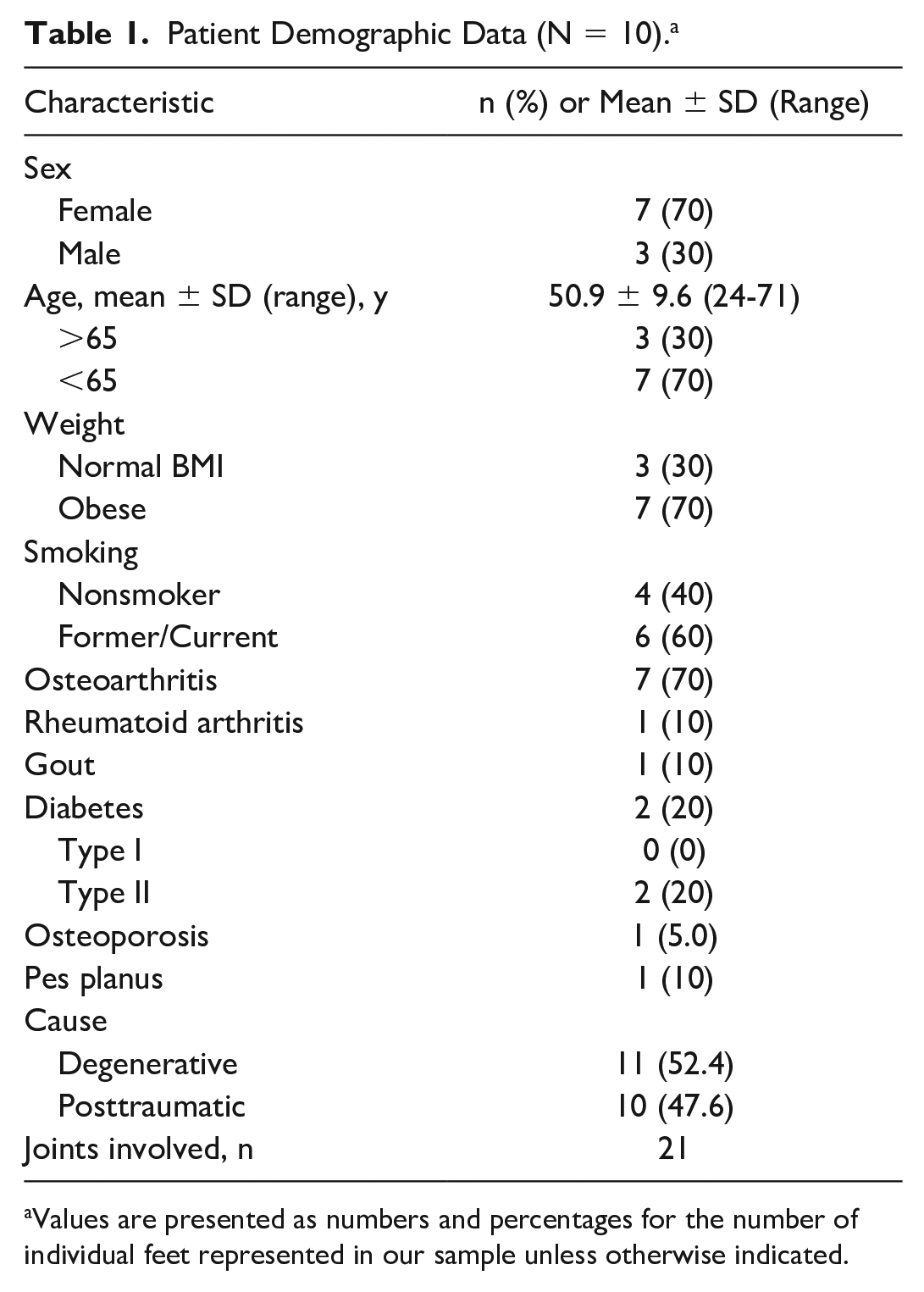
Values are presented as numbers and percentages for the number of individual feet represented in our sample unless otherwise indicated.
Patient Outcome Data Following Lesser TMT Fusion With Nitinol Staple, BMAC, and Calcaneal Bone Dowel.
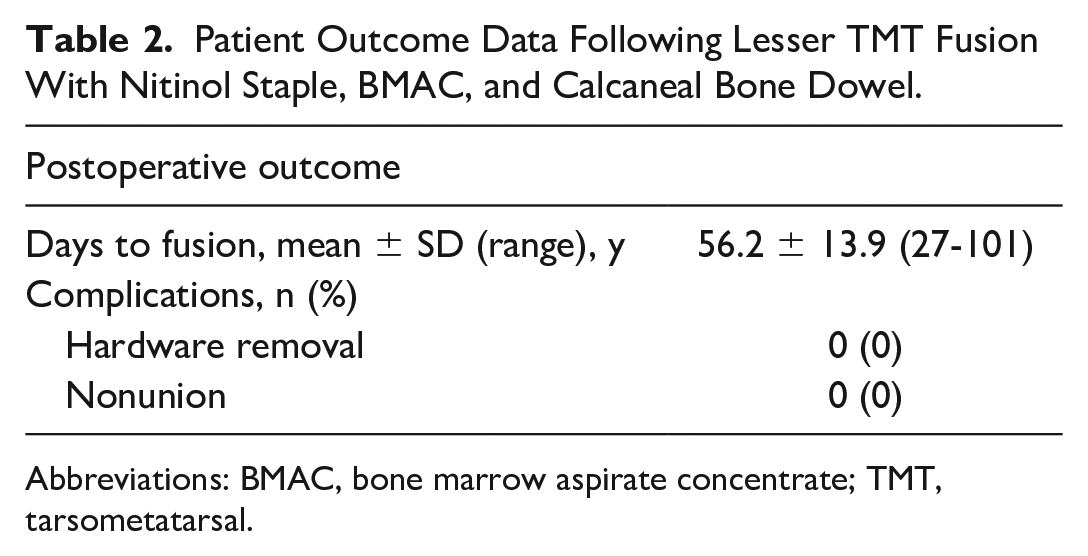
Abbreviations: BMAC, bone marrow aspirate concentrate; TMT, tarsometatarsal.
Discussion
The technique first described by Johnson and Johnson 5 using a calcaneal dowel plug and trephined joint resection of the TMT joint provides surgeons with another option for patients with lesser TMT joint arthritis. Drawing on information presented through previous studies, the senior surgeon has adapted the technique previously discussed to highlight the strengths of various arthrodesis techniques while using local autologous bone graft, trephined joint surface, BMAC, and CCDs to create a reproducible, simple technique for lesser TMT arthrodesis. Here, we discuss advantages of this technique and offer rationale for its use in the management of lesser TMT arthritis.
First, the technique takes advantage of autologous bone dowels that provide a scaffolding for fusion. Originally described by Cloward in 1961 for spinal fusion, the benefits of the bone dowel are multifactorial. 3 Multiple studies have demonstrated that the use of autologous bone graft significantly decreased nonunion rates in foot and ankle literature.2,5 Additionally, the bone dowel helps maintain length across the joint space, thereby preventing shortening of the rays, altering the foot biomechanics, and limiting the risk of transfer metatarsalgia. 8 In addition, the use of calcaneus bone graft has been shown to lower donor site morbidity in previous studies. 8 Results from our study, which had no donor site complications at the time of the most recent follow-up, further supports the use of calcaneus bone grafts for lesser TMT arthrodesis. Other sites such as the iliac crest or proximal tibia may be reasonable alternatives. The autologous bone dowel was also bathed in BMAC before insertion into the trephinate resection. A number of studies have identified BMAC as an aid in fracture healing and reduced nonunion rates. 4 The BMAC provides additional local osteoinductive properties directly to the bone dowel and fusion site.
Second, trephination of the subchondral joint space ensures an effective and efficient denudation of cartilage across affected joints. Several cadaveric studies using a curettage technique with midfoot fusions have demonstrated preserved calcified cartilage layers. 8 This remaining calcified cartilage layer has been theorized to hinder fusion consolidation. An effective trephinate ensures that this cartilage layer is removed in a timely manner using the cutting reamer compared to the manual curettage technique. The trephine also creates an inherent stability in multiple planes by producing a lock-and-key design.
Third, the adaptation of a CCD across the newly implemented bone plug provides an increased level of stability to the fusion site. Various techniques have been described and studied to aid in arthrodesis consolidation. Most commonly, the use of compression plating attached dorsally has been employed but others have described the use of lag screws, Kirschner wires, plates, and staples fashioned out of Kirschner wires. 6 Although these constructs have provided varying results with certain studies obtaining a 92% union rate, many constructs result in a nonunion rate of 3% to 11%.2,6 In a biomechanical study comparing nitinol staples to claw plating and cross screws, Aiyer et al 1 demonstrated a significant increase in contact force and area across the arthrodesis site with the use of nitinol staples. Another added benefit—likely attributable to the slender nature of the staple—is the reduced soft tissue burden compared to a prominent dorsal plate, which has demonstrated a 9% complication rate of screw irritation or breakage in previous studies. 6 The main disadvantage to this technique is the requirement of specialized instruments. A theoretical disadvantage can be that the compression staple may cause slight dorsiflexion of the affected rays; however, clinically we have not found this to be of concern.
Conclusion
The use of autologous bone dowel, CCD, and BMAC provides an encouraging union rate following lesser TMT joint arthrodesis. Further studies are required to evaluate the efficacy of this novel technique and better ascertain independent risk factors for nonunion of lesser TMT joints.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007221081878 – Supplemental material for Lesser Tarsal Metatarsal Joint Fusion Using Nitinol Staples, Bone Marrow Aspirate Concentrate, and a Calcaneal Bone Dowel: A Technical Note
Supplemental material, sj-pdf-1-fai-10.1177_10711007221081878 for Lesser Tarsal Metatarsal Joint Fusion Using Nitinol Staples, Bone Marrow Aspirate Concentrate, and a Calcaneal Bone Dowel: A Technical Note by Jay C. Thompson, Jared Scott, Mark Johnson, Byron Detweiler, J. Michael Anderson and Bryan Hawkins in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.