
Abstract
Background:
Success of valgus-type supramalleolar osteotomy (SMOT) depends on adequate correction of malalignment, which can be hard to achieve with current 2-dimensional (2D) planning and operative techniques. A personalized digital 3-dimensional (3D) workflow to virtually plan and perform a 2-step 3D-guided medial opening (MO) SMOT has the potential to improve precision of correction.
Methods:
Computed tomography (CT)–based Proplan medical 3D models were made to virtually plan the desired MO SMOT, and exported to 3-Matic medical to develop patient-specific 2-step cutting and wedge guides. Workflow accuracy was tested in this limited clinical pilot study (3 patients) by comparing the virtual planned position of the osteotomized distal tibial fragment with the 1-year post-MO SMOT configuration. Two millimeters or less translation deviation in every plane was defined as accurate.
Results:
Primary outcome analysis of the osteotomized distal tibial fragment deviation showed a median translation in all planes of 0.7 (range 0-8.2) mm (interquartile range 1.55) with an excellent interrater reliability of the measurements (intraclass correlation coefficient 0.998). There was a strong reduction in ankle pain as reflected by an increase of the AOFAS-AH score and decrease of NRS pain score with an unrestricted hindfoot motion 1 year after surgery.
Conclusion:
3D virtually planned bone cutting and wedge guides is a promising approach associated with minimal postoperative deviation from the desired correction in medial opening supramalleolar osteotomy.
Level of Evidence:
Level IV, case series.
Introduction
Joint-preserving procedures such as supramalleolar tibial osteotomy (SMOT) are broadly considered a valuable option in the treatment of asymmetric ankle osteoarthritis. 3 The main purpose of SMOT is to transfer the weightbearing line of the ankle by joint realignment. 4 Current 2D-based distal tibia correction techniques can result in great variation to the desired postoperative mechanical axis point in the ankle. 2 In recent years, the potential of converting to 3D measurements and prevent inaccuracies due to 2D projection errors and foot orientation variation has been presented. 6 Exact transfer of a 3D virtual operative plan to the operating room with 3D-printed patient-specific bone cutting guides may improve the precision of osteotomies. 10 The current study describes a newly developed digital 3D workflow to virtually plan and perform a patient-specific MO SMOT that guides the cut (step 1) and controls the correction (step 2) in all planes. Our hypothesis was that this 2-step type of MO SMOT provides an accurate method to achieve the desired spatial positions of the osteotomized distal tibia 1 year after surgery.
Materials and Methods
Three consecutive patients with symptomatic varus ankle OA eligible for SMOT were treated with a 3D planned and guided patient-specific MO SMOT in 2019 and reviewed retrospectively at 1-year follow-up. The study was approved by the Institutional Review Board of our hospital (MEC number 2021-026), and all patients gave their informed consent.
Operative Planning and Technique
The amount of angular correction in the frontal plane was determined using a baseline whole leg standing radiograph (WLR) and planned that the tibial axis is aligned with the center or slightly lateral to the center of the ankle joint. Using data of nonweightbearing SPECT-CT scan of the affected joint and contralateral tibia, 3D bone surface models of the distal tibia were segmented, and further processed for 3D planning of the MO SMOT with Proplan CMF 3.0 (Materialise, Leuven, Belgium). The osteotomy plane was aimed to end just above the syndesmosis, and the distal segment was virtually rotated around the lateral cortical hinge point toward the desired position. The virtual 3D models were exported to 3-Matic medical to design the actual 2-step patient-specific guides. The guides were 3D-printed from Polyamid-12 (PA-12) under the 13485 ISO certification and conform the EU-MDR requirements. At surgery, the saw-guide (step 1) was placed, under fluoroscopic guidance, in the preplanned position at the distal tibia, and fixated with 2.0-mm Kirschner wires (Figure 1A). Osteotomy was performed through the 1.27-mm cutting sleeve leaving the lateral distal tibia cortex intact to create a hinge. A medial opening wedge was created after removal of the saw-guide by using the same Kirschner wires as reference to put the wedge-guide (step 2) in place (Figure 1B). The design of the wedge-guide left sufficient space to put a case-specific manually bent LCP medial distal tibia plate of 3.5 mm (DePuy Synthes, Johnson & Johnson medical devices companies) in place to fixate the desired osteotomy position (Figure 1C). The opening wedge was filled with allograft bone chips (ETB-Bislife Multitissue Center). An oblique fibular osteotomy was performed and fixated with a nonlocking plate. After wound closure, a below-knee cast was administered for 2 weeks. Nonweightbearing ankle/hindfoot movements were allowed for another 4 weeks, after which full weightbearing was started.
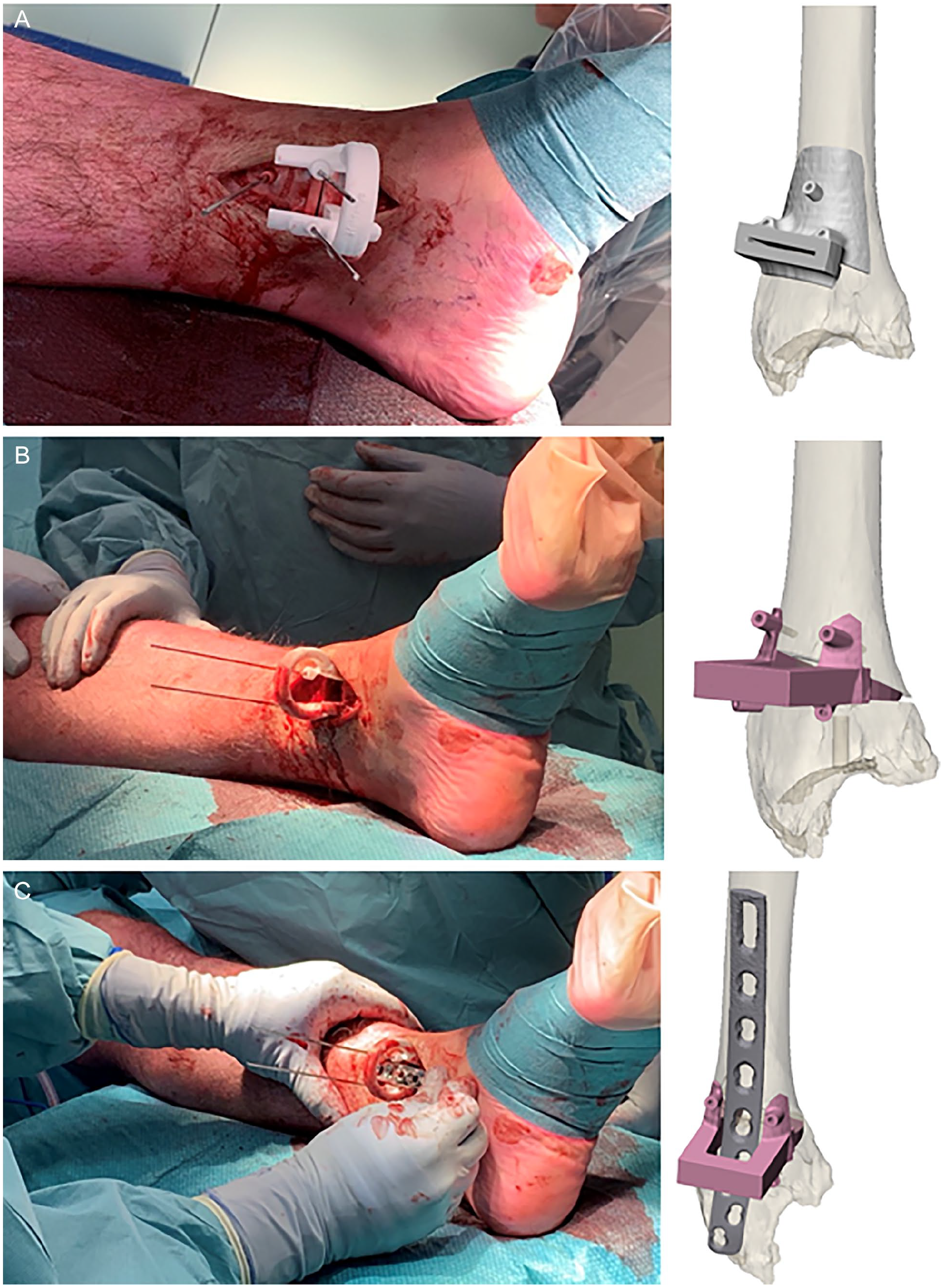
Operative procedure: 2-stage supramalleolar osteotomy saw (step 1) and wedge (step 2) guides. (A) Cutting sleeve guide (step 1) accurately placed and fixated with Kirschner wires. (B) Wedge guide (step 2) placed over 2 prior Kirschner wires. (C) Less invasive plate osteosynthesis insertion with wedge guide (step 2) in place.
Outcome Measurements
Primary outcome was the translation deviation between the preoperative virtual planned and 1-year postoperative position of the osteotomized distal tibial fragment measured with 3D CT imaging (Figure 2). Secondary outcome measurements were 3D CT–measured rotation deviation of the osteotomized distal tibial fragment, the American Orthopaedic Foot & Ankle Society-ankle and hindfoot (AOFAS-AH) score, and pain on an 11-point numeric rating scale (NRS) at baseline and after 1 year postoperatively.
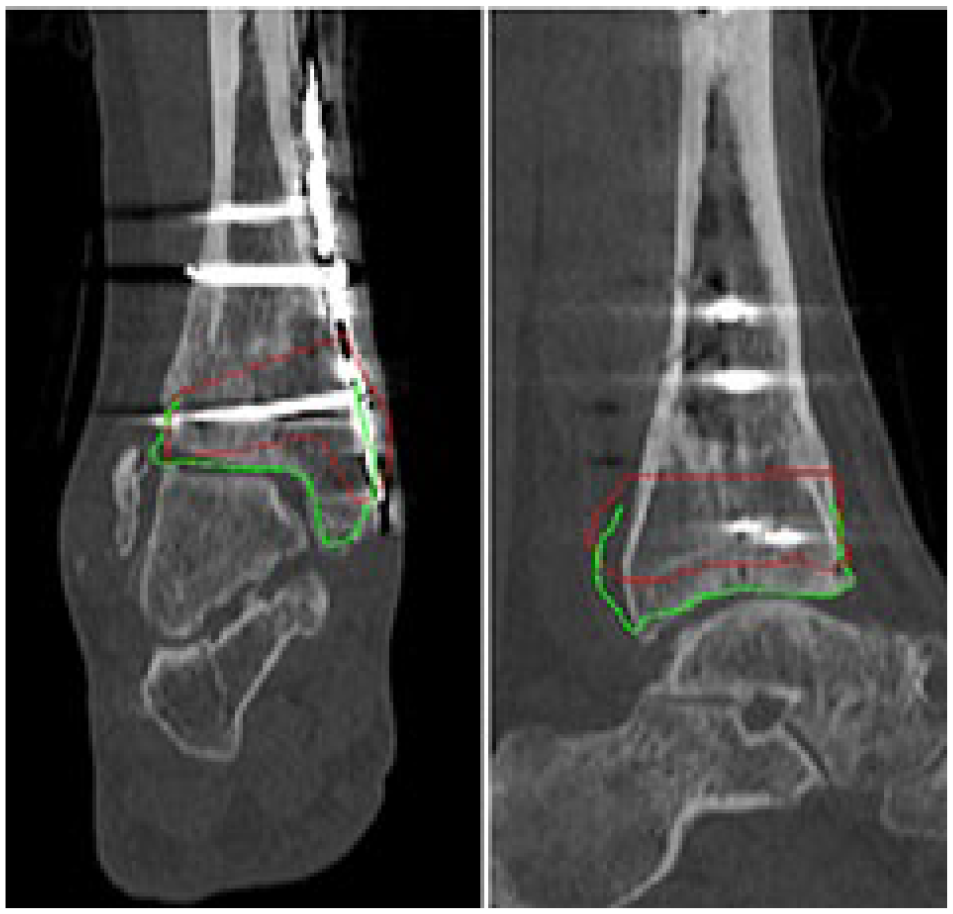
Proplan medical 3D model in frontal and sagittal directions with overlay projected of the preoperative situation (red) and achieved correction (green). [See online article for color figure.]
Statistical Analysis
Descriptive statistics were used to present the data per casus. The intraclass correlation coefficient was calculated as a measure of conformity between 2 observers for the 3D positional and angular measurements separately. A 2-way random intraclass correlation coefficient model on absolute agreement was used. Statistical data analysis was carried out with IBM SPSS Statistics for Windows (version 25.0; IBM Corp).
Results
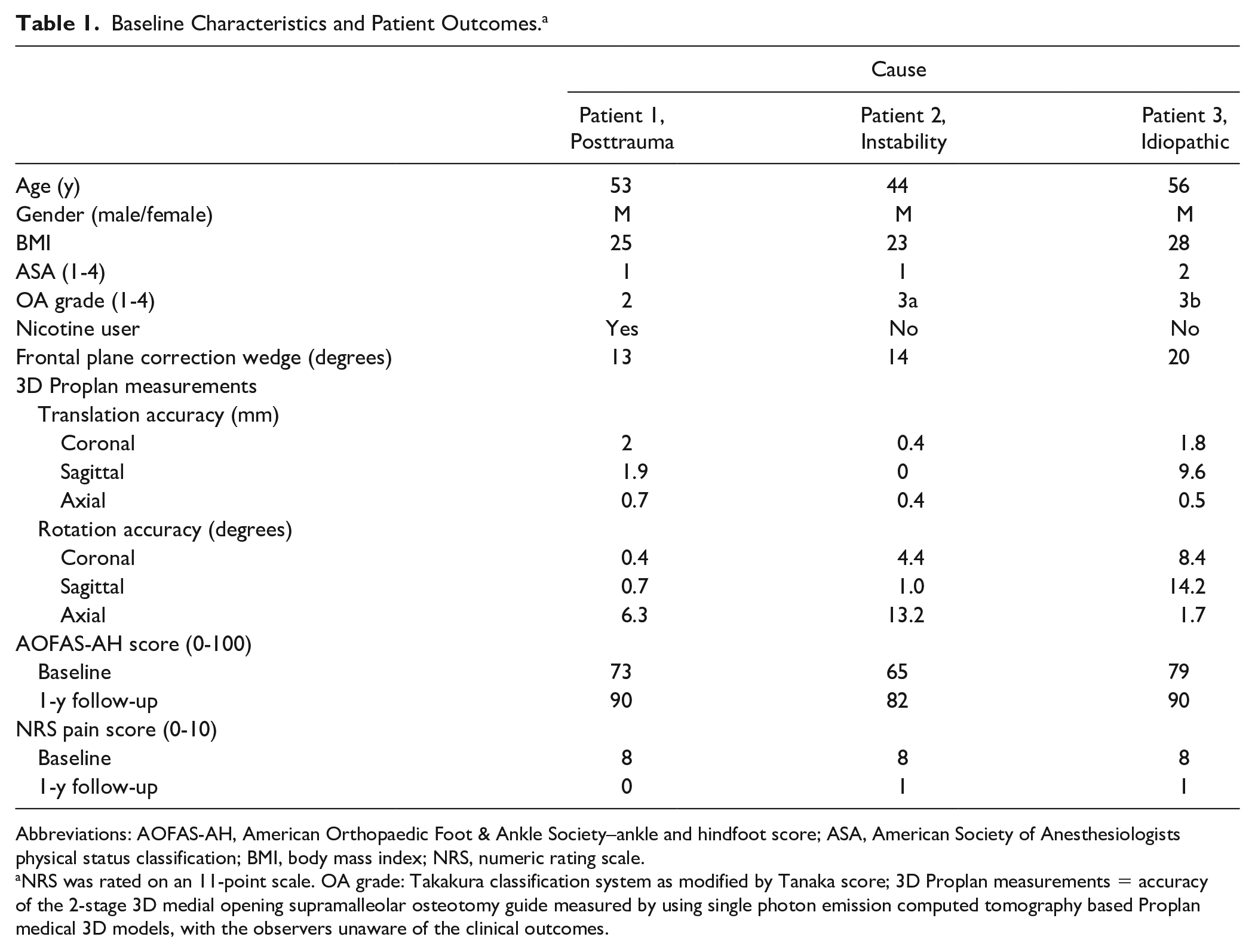
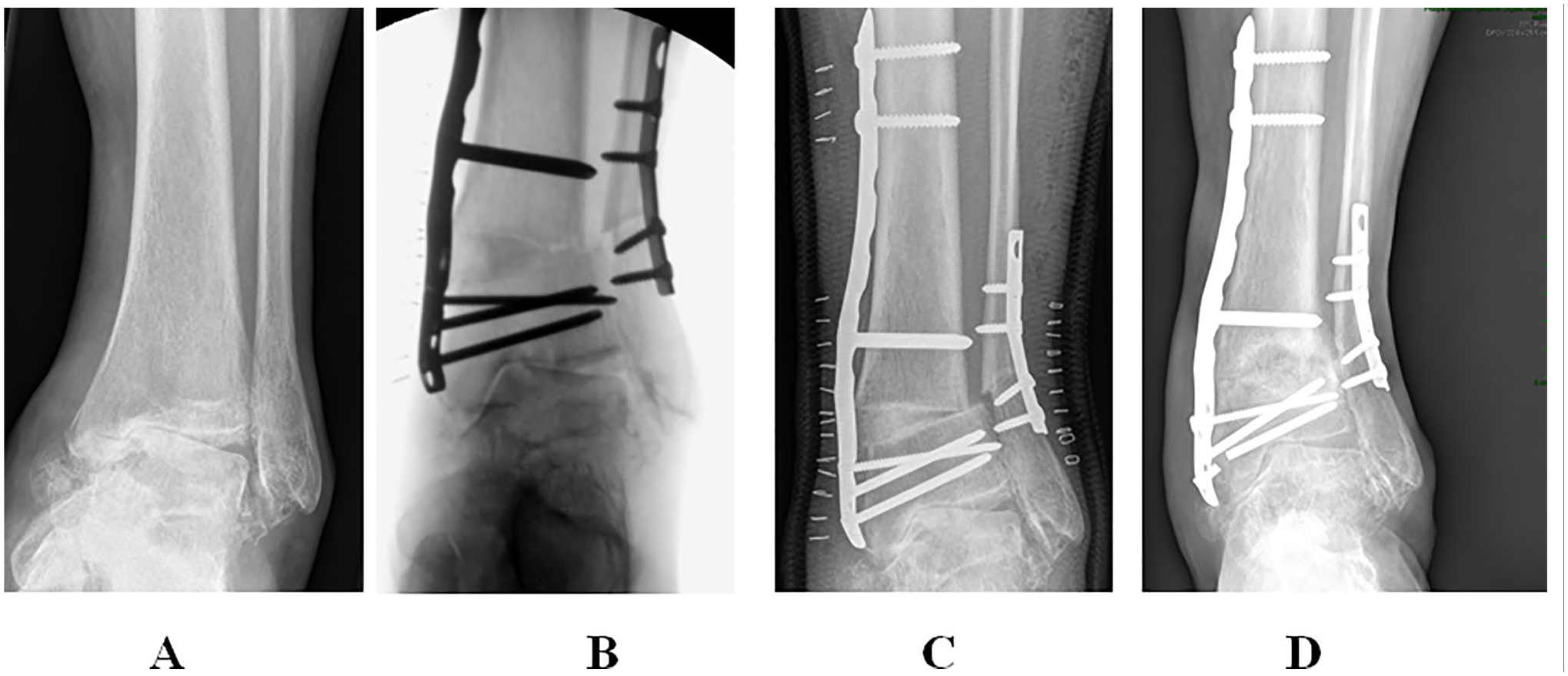
The baseline characteristics and outcomes are summarized in Table 1. Lateral cortex disruption occurred in all patients during surgery. There were no neurovascular or wound healing complications. The 3D primary outcome analysis showed a median translation in all planes of 0.7 (range 0-8.2) mm (interquartile range: 1.55). The median deviation from the planned rotation of the distal fragment in all axes was 4.4 (range 0.4-14.2) degrees (interquartile range: 10.1) at 1-year follow-up. An excellent intraclass correlation coefficient for translation of 0.998 (0.990-0.999) and for rotation 0.991 (0.847-0.998) was found between the 2 observers. AOFAS-AH score increased 11 or 17 points with no hindfoot motion restriction for the 3 ankles 1 year postoperatively. Ankle pain was strongly reduced with 7 or 8 points’ decrease of the NRS pain score. Patient 1 and 3 developed radiologic delayed union with screw breakage at 1 year (example shown in Figure 3). The patients were willing to undergo SMOT if that decision could be made again.
Baseline Characteristics and Patient Outcomes. a
Abbreviations: AOFAS-AH, American Orthopaedic Foot & Ankle Society–ankle and hindfoot score; ASA, American Society of Anesthesiologists physical status classification; BMI, body mass index; NRS, numeric rating scale.
NRS was rated on an 11-point scale. OA grade: Takakura classification system as modified by Tanaka score; 3D Proplan measurements = accuracy of the 2-stage 3D medial opening supramalleolar osteotomy guide measured by using single photon emission computed tomography based Proplan medical 3D models, with the observers unaware of the clinical outcomes.
Ankle radiograph anteroposterior views (patient 3): (A) preoperative; (B) intraoperative; (C) 1-day postoperative; and (D) 1-year postoperative.
Discussion
This study reports a novel personalized workflow for 3D virtual operative planning and a 2-step guided SMOT. Accuracy of comparable 3D operative planning and guide surgery in the reconstruction of maxillofacial defects revealed a median difference of fibula and implant placement of 0.3 and 2.2 mm, respectively. 7 We considered 2 mm or less deviation from the preoperative 3D operative plan to be accurate. Our results showed high accuracy with a median translation deviation of 0.7 mm. Less than 2 mm deviation of the distal tibial fragment occurred in all planes but one. Only in patient 3 with the largest correction wedge (20 degrees), a deviation in the sagittal plane of more than 2 mm occurred. The large wedge size with a fibular osteotomy may have stretched the limits of stability to be counteracted by the designed 3D osteotomy guides or perhaps the manually bent off-the-shelf plate was not accurate enough. 3D-printed patient-specific plates that contour the postoperative situation more precise may act as a superior reduction tool.
The present study is a retrospective pilot study with its limitations, and a direct postoperative CT scan was not part of standard patient care in our hospital. We cannot be sure if the correction achieved at 1 year matches the correction immediately after surgery.
There is no preferred supramalleolar osteotomy technique in correcting varus ankle OA. 8 We chose a medial opening wedge osteotomy that allowed for optimal access and anatomic fitting of the 3D-printed saw and correction wedge guides. Delayed union with breakage of screws in patients 1 and 3 was seen despite the use of standard allogenous bone grafting. Patient 1 was a tobacco user, and smoking has been identified as a major predictive risk factor for delayed or nonunion. Patient 3 needed a large opening wedge, which may have caused prolonged union.
To our knowledge, this is the first study to measure rotation of the distal tibia segment after MO SMOT. We found a median deviation of rotation of 4 (range between 0.4 and 14.2) degrees of the planned rotation in all directions 1 year postoperatively. Change in lower limb rotation can alter ankle loading, and consequently may lead to cartilage damage. 9 After 1 year, we noticed no clinical consequences. It can be argued that breakage of the lateral hinge point, which occurred in all cases, induces rotational instability. 4 We aimed our osteotomy site to end just proximal of the syndesmotic ligament, which consequently preserves a less stable fulcrum. 5 Superior 2D radiologic results have been shown for a distal syndesmotic osteotomy. 1 Our 3D-guided technique allows for a distal plane of osteotomy as well that may reduce the risk of malrotation.
Conclusion
3D-guided supramalleolar osteotomy shows promising results with minimal postoperative deviation from the desired correction after 1 year.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007221082643 – Supplemental material for Two-Step 3D-Guided Supramalleolar Osteotomy to Treat Varus Ankle osteoarthritis
Supplemental material, sj-pdf-1-fai-10.1177_10711007221082643 for Two-Step 3D-Guided Supramalleolar Osteotomy to Treat Varus Ankle osteoarthritis by Tom van Raaij, Hylke van der Wel, Mark Beldman, Astrid de Vries, PhD and Joep Kraeima in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
A supplemental video for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.