
Abstract
Background:
The best operative construct and technique for treatment of isolated syndesmotic injuries is highly debated. The purpose of this study was to determine whether the addition of anterior inferior tibiofibular ligament (AITFL) suture repair or suture tape (ST) augmentation provides any biomechanical advantage to the operative repair of an isolated syndesmotic injury.
Methods:
Twelve lower leg specimens underwent biomechanical testing in 6 states: (1) intact, (2) AITFL suture repair, (3) AITFL suture repair + transsyndesmotic suture button (SB), (4) AITFL suture repair + ST augmentation + SB, (5) AITFL suture repair + ST augmentation, and (6) complete syndesmotic injury. The ankle joint was subjected to 6 cycles of 5 Nm internal and external rotation torque under a constant axial load. The spatial relationship between the tibia, fibula, and talus was continuously recorded with a 5-camera motion capture system.
Results:
AITFL suture repair and AITFL suture repair + ST augmentation showed no statistically significant change in fibula kinematics compared to the intact state. Compared to native, AITFL suture repair + SB showed increased fibular external rotation (+2.32 degrees, P < .001), and decreased tibiofibular gap (overtightening) (–0.72 mm, P = .007). AITFL suture repair + ST augmentation + SB also showed increased fibular external rotation (+1.46 degrees, P = .013). Sagittal plane motion of the fibula was not significantly different between any states. None of the repairs restored intact state talus rotation; however, the repairs that used ST augmentation reduced the talus external rotation laxity compared to the complete syndesmotic injury.
Conclusion:
AITFL suture repair and AITFL ST augmentation best restored the rotational kinematics and stability of the fibula and ankle joint in an isolated syndesmotic injury model.
Clinical Relevance:
AITFL suture repair with or without ST augmentation may be a good operative addition or alternative to SB fixation for isolated syndesmotic disruptions.
Introduction
The syndesmotic ligament complex is a significant contributor to the dynamic stability of the ankle as it prevents diastasis of the tibia and fibula and external rotation of the fibula.1,7,37 Isolated syndesmotic injuries or high ankle sprains are increasing in prevalence and diagnosis because of enhanced awareness of syndesmotic injuries, better understanding of the clinical diagnosis, and improved imaging methods.5,31,32,34 Traditional management of isolated syndesmotic injuries involved a period of protected weightbearing in a cast or boot or transsyndesmotic screw fixation. 37 Newer technology has led to the development of syndesmotic fixation that aims to restore native ankle and distal tibiofibular joint motion and stability with a goal of returning athletes to sport more quickly.27,37 Indications for operative fixation of isolated syndesmotic injuries are evolving but are trending toward more aggressive treatment, especially in high-level athletes.1,2,13
Traditional operative repair of syndesmotic disruptions with cortical screw fixation has shown high rates of syndesmotic malreduction and screw breakage.9,24,25 More dynamic methods of fixation using suture button (SB) constructs have been developed to avoid the potential complications of transsyndesmotic screw fixation. 34 Clinical studies have shown better functional outcomes and lower rates of complication and malreduction with dynamic fixation compared with static screw fixation.11,20,22
Optimal operative fixation of syndesmotic injuries has been elusive in both clinical and biomechanical studies.6,11,18 Perfect anatomic reduction and restoration of physiologic motion at the syndesmosis is challenging to achieve, partly because of limitations in various fixation devices. Despite promising results with SB fixation, there are concerns about lack of stability with these constructs, specifically in rotational and sagittal plane motion. 6 Multiple biomechanical studies have suggested that direct reconstruction or repair of the anterior inferior tibiofibular ligament (AITFL) may provide extra stabilization to the syndesmosis and restore native anatomy more precisely.27,30,33,37 However, there is still no consensus on the optimal method of fixation. 34
The purpose of this study was to biomechanically compare operative constructs for repair of the ankle syndesmosis, and specifically to determine whether the addition of AITFL suture repair or ST augmentation would benefit the operative repair of an isolated syndesmotic injury. The 3 methods tested included direct suture repair of the AITFL with the addition of one of the following: (1) SB fixation, (2) suture tape (ST) augmentation, or (3) ST augmentation + SB fixation. It was hypothesized that tibiofibular and ankle joint kinematics would be significantly altered by the syndesmotic injury, that AITFL suture repair alone would be insufficient to fully restore native kinematics, and that the addition of suture tape would increase resistance to external rotation and restore native kinematics of the fibula and the ankle.
Materials and Methods
Specimen Preparation and Mounting
Twelve unpaired lower leg specimens (tibial plateau to toe-tip) with a mean age of 41 (range, 23-62) years and no history of foot or ankle injury, prior surgery, osteoporosis, or osteoarthritis were obtained for this study. The specimens were arthroscopically screened for syndesmotic pathologies by documenting inability to place a 3-mm probe into the syndesmosis, which has been shown to be highly predictive of no injury to the syndesmosis. 12 All skin, subcutaneous tissue, and muscle was removed proximal to the foot, and all structures of the proximal tibiofibular joint and medial and lateral ankle were left intact.
To secure the foot, 2 threaded rods were inserted through a custom fixture into the calcaneus. Nuts and washers were used to rigidly fix the calcaneus to the rods, and 2 pins were inserted into the metatarsals to keep the anterior foot seated against the base of the fixture. The subtalar joint was stabilized by 2 screws placed from anterior to posterior through the talus into the calcaneus to isolate the motion to the ankle joint. The custom fixture was then aligned with the biaxial load frame (ElectroPuls E10000; Instron Systems) such that the center of the ankle joint was aligned with the axis of the biaxial load frame’s actuator. Extreme care was taken to align the axis of the Instron actuator with the natural axis of rotation of the joint to closely approximate natural joint rotation. Prior to clamping the foot fixture to the testing bed, the joint was aligned in 3 planes using a plumb bob in line with the axis of the actuator. The foot fixture was positioned such that the center of the joint was located directly along the axis of the actuator by aligning the most prominent point of the medial malleolus from the medial side, lateral malleolus from the lateral side, and the previously marked center of the exposed talus from the anterior side. The tibia was then fixed to the actuator of the biaxial load frame via 2 threaded rods placed anterior to posterior through the proximal tibia. This process is shown in Figure 1.
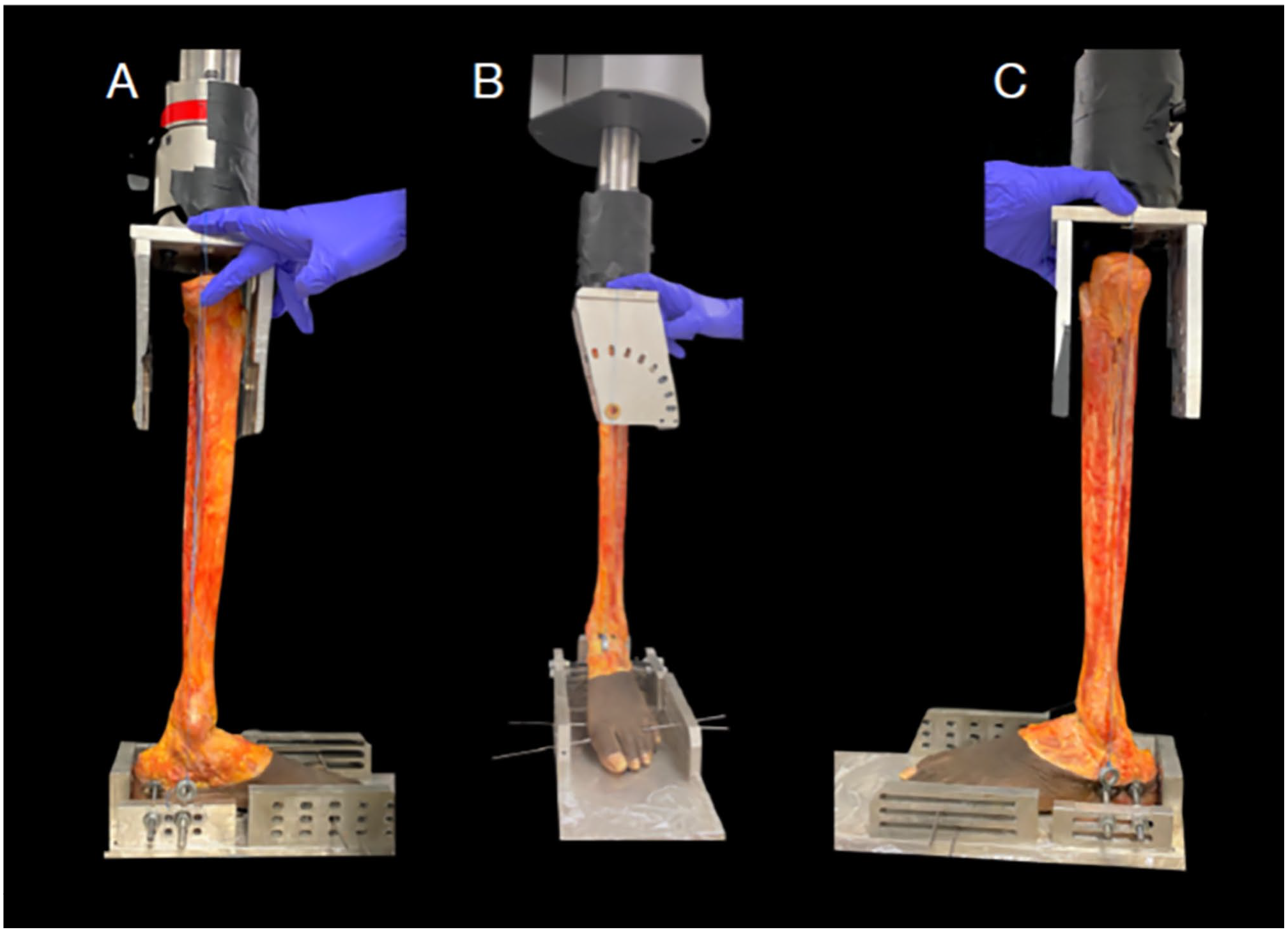
Plumb bob method of alignment of the custom foot fixture to the biaxial load frame actuator. (A) medial view; (B) anterior view; (C) lateral view.
Motion Capture and Anatomic Coordinate System
To track the motion of the tibia, fibula, and talus throughout the testing, a cluster of 4 reflective markers were securely drilled into each bone with a wood screw (Figure 2). Five Miqus motion capture cameras (Qualisys AB) were used to track the location of the markers throughout testing. A coordinate measuring machine (Romer Absolute Arm; Hexagon Metrology) was used to collect 11 points on each ankle: the medial malleolus, lateral malleolus, 4 points forming a ring around the proximal tibia, a point on the anterior foot directly between the second and third metatarsals, the most posterior point of the calcaneus, and 3 points on the plane of the floor. These points were used to establish tibial, fibular, and foot coordinate frames, as described in the SimVITRO software (SimVITRO). Further detailed explanation of the coordinate systems are available in supplemental images.
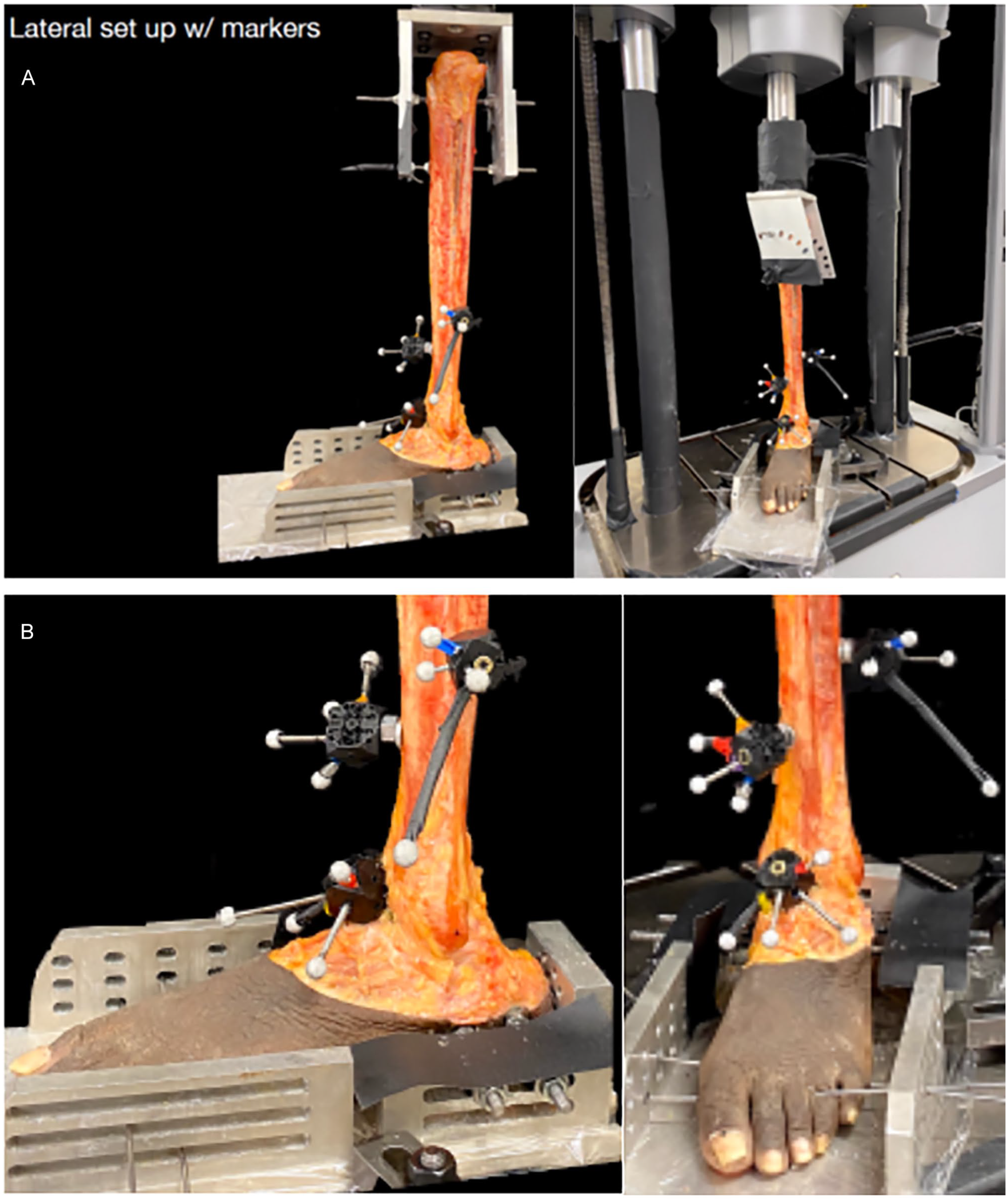
(A) Lower leg specimen secured in the dynamic, biaxial testing machine with tracking markers in place. (B) Magnified image of the specimen showing the location of the tracking markers in the tibia and talus.
Biomechanical Testing
Twelve specimens were tested in the following states: (1) intact, (2) AITFL suture repair, (3) AITFL suture repair + ST augmentation, (4) AITFL suture repair + ST augmentation + SB, (5) AITFL suture repair + SB, and (6) complete syndesmotic injury. The order of states 3 and 5 was randomized. Prior to testing, the neutral position of the joint was recorded in the intact state by applying a 750-N compressive load to the joint and setting the torque control to zero. A 750-N compressive load remained constant throughout testing. Two tests were run: 5-Nm internal rotation test and 5-Nm external rotation test. In both tests, the torque was ramped up to the target value over a period of 7 seconds and was then held constant for an additional 10 seconds. All data for each test are reported from the kinematics at the end of the 10-second hold. The joint was then returned to the previously recorded neutral position before the start of the next test. Each test was run 6 times in each state. The average joint kinematics was calculated for each test and the average of the 6 test repetitions was calculated for each state. The spatial relationship of the fibula and talus with respect to the tibia was evaluated for anterior translation, lateral translation, and rotation in both external rotation and internal rotation at 5 Nm of torque through the foot. A lower level of torque was chosen than previous studies in order to replicate physiologic motion of everyday activities instead of injury-level forces that have caused fracture and damage to specimens in previous studies. 37
Operative Techniques
After specimen preparation and testing of the intact state, a complete syndesmotic injury was created by sectioning the AITFL, interosseous tibiofibular ligament (ITFL), interosseous membrane 5 cm proximal to the ankle joint, and superficial and deep posterior inferior tibiofibular ligament (PITFL). The deltoid ligament and proximal tibiofibular joint were left intact. For all repair techniques, syndesmotic reduction was performed by manual compression across the tibiofibular joint, which has been shown to be more accurate than clamp placement with less risk of fibular malreduction and translation. 8 Direct repair of the AITFL was performed using 2 figure-of-8 stiches with no. 0 Vicryl Suture (Ethicon, Inc). The sutures were placed in line with the fibers of the AITFL and tied under maximum tension.
Suture tape augmentation of the AITFL was performed using an InternalBrace (Arthrex, Inc) per the manufacturer’s technique guide. First, the fibular tunnel was made with a 2.7-mm drill starting at Wagstaffe’s tubercle and angled approximately 30 degrees plantar, remaining parallel to the long axis of the fibula. The drill tunnel was tapped followed by insertion of a 3.5-mm SwiveLock (Arthrex, Inc) anchor loaded with collagen-coated FiberTape (Arthrex, Inc). At Chaput tubercle within the AITFL footprint, a 3.4-mm drill was aimed slightly cephalad away from the tibiotalar joint and then tapped. A 4.75-mm SwiveLock was loaded with the ST, tensioned appropriately, and then inserted into the tibial tunnel so that the ST was lying parallel to the AITFL fibers.
A TightRope XP (Arthrex) was used for SB fixation in accordance with the manufacturer’s technique guide. All 4 cortices from the fibula through the tibia were drilled using a 3.7-mm drill bit, 1.5 cm proximal to the ankle joint and aimed approximately 30 degrees anterior to the coronal plane. The SB was passed through the drill hole, deployed with confirmation that the oblong button was flipped and seated flush against the medial tibia. It was then tightened by pulling on the sutures sequentially until both buttons were flush against bone. All repairs were performed by one of 2 orthopaedic surgeons (MJ and IS) during their foot and ankle fellowship.
Statistical Analysis
Random intercepts linear mixed effects (LME) models were used to compare experimental conditions for each of the 4 measurements during simulated internal rotation and external rotation tests. For each LME model, 6 possible covariance structures were considered to reflect the repeated measures experimental design (zero within-group covariance, autoregressive, compound symmetry, exponential, spherical, and unstructured). The covariance structure resulting in the smallest Bayesian information criterion (BIC), while also producing acceptable residual diagnostics, was chosen as the final mode. 3 Estimated marginal means were reported and Tukey method was used to make all pairwise comparisons among the states. Residual diagnostics were inspected to ensure model fit and that assumptions were met. Tukey adjusted P values less than .05 were considered statistically significant. The statistical software R, version 4.0.0, was used for all plots and analyses (R Core Team; with additional packages nlme and emmeans; Pinheiro and Bates, Lenth). 3
Results
Fibular Lateral Translation
With an external rotation torque of 5 Nm through the foot, none of the repair states or the injury state were significantly different from the intact state in fibular lateral translation relative to the tibia.
With an internal rotation torque, only the AITFL suture repair + SB state was significantly different from the intact state showing more medial translation, or overtightening, compared to the intact (mean −0.72 mm, P = .007). AITFL suture repair + ST augmentation had significantly less medial translation compared to the states with an SB (AITFL suture repair + SB: mean −0.93 mm, P < .001; AITLF suture repair + ST + SB: mean −0.77 mm, P < .001) (Figure 3).
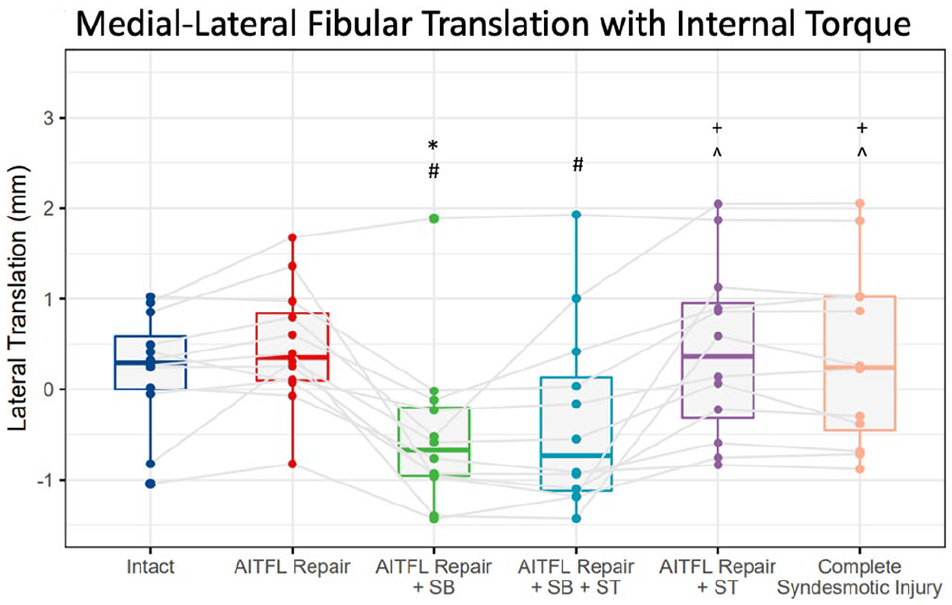
Box plot graph demonstrating fibular medial-lateral translation in millimeters relative to the tibia during the internal rotation test. Dots represent individual specimen observations. Thick horizontal lines represent group medians, whereas the top and bottom of the boxes represent the 25th and 75th percentiles, respectively. *Significant difference compared to intact state. #Significant difference compared to AITFL suture repair state. +Significant difference compared to AITFL suture repair + SB state. ^Significant difference compared to AITFL suture repair + SB + ST state. AITFL, anterior inferior tibiofibular ligament; SB, suture button; ST, suture tape.
Fibular Anterior Translation
With an external rotation torque through the foot, the complete syndesmotic injury state showed no difference from the native state but was significantly more posteriorly translated compared to all repair states (AITFL suture repair: +0.61 mm, P = .035; AITFL Suture repair + SB: +0.88 mm, P = .007; AITFL suture repair + ST: +1.11 mm, P < .0001; AITFL repair + SB + ST: +1.37 mm, P < .0001). However, none of the repair states were significantly different from the intact state, as shown in Figure 4.
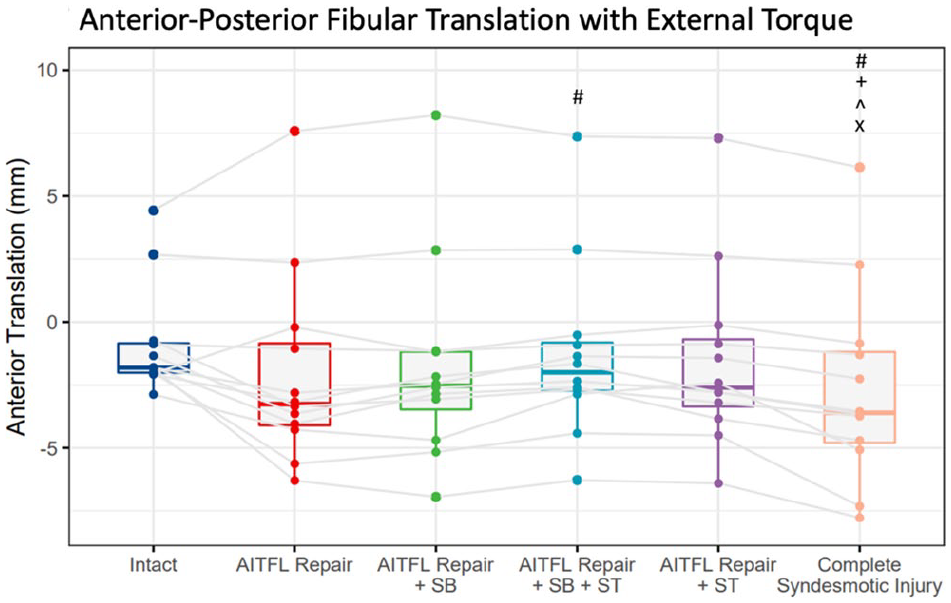
Box plot graph demonstrating fibular anterior-posterior translation in millimeters relative to the tibia during the external rotation test. #Significant difference compared to AITFL suture repair state. +Significant difference compared to AITFL suture repair + SB state. ^Significant difference compared to AITFL suture repair + SB + ST state. xSignificant difference compared to AITFL suture repair + ST state. AITFL, anterior inferior tibiofibular ligament; SB, suture button; ST, suture tape.
With an internal rotation torque, none of the states were significantly different in anterior translation of the fibula compared to the intact state.
Fibular Rotation
With an external rotation torque through the foot, the fibula externally rotated significantly more relative to the tibia in the complete syndesmotic injury state compared to the intact state (mean 1.57 degrees, P = .006) and in the constructs with an SB (AITFL suture repair + SB: mean 2.32 degrees, P < .001; AITFL suture repair + ST augmentation + SB: mean 1.46 degrees, P = .013) (Figure 5).
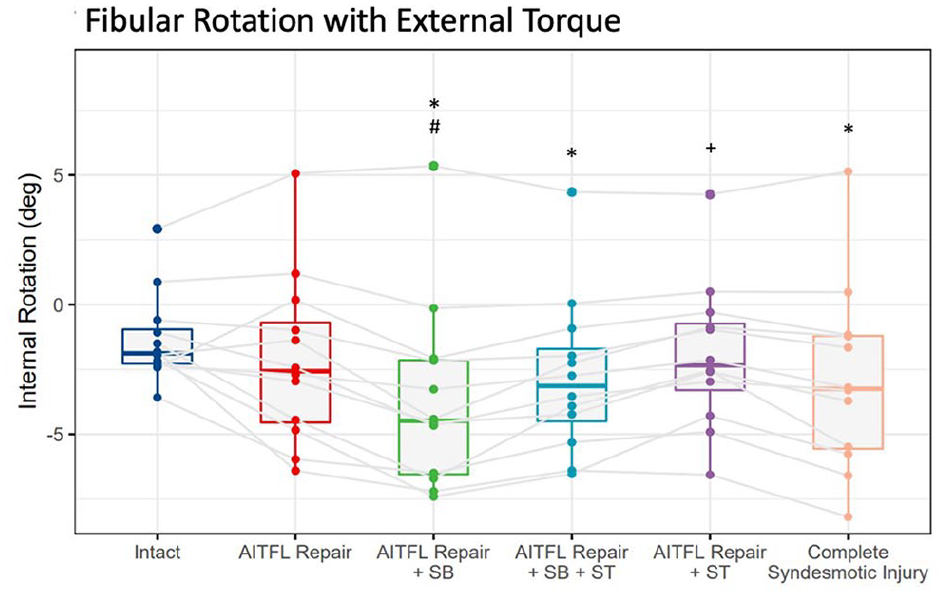
Box plot graph demonstrating fibular rotation in degrees relative to the tibia during the external rotation test. *Significant difference compared to intact state. #Significant difference compared to AITFL suture repair state. +Significant difference compared to AITFL suture repair + SB state. AITFL, anterior inferior tibiofibular ligament; SB, suture button.
With an internal rotation torque, only the states with an SB were significantly different from the intact states (AITFL suture repair + SB: mean 1.58 degrees, P < .001; AITFL repair + ST augmentation + SB: mean 1.42 degrees, P < .001), showing more external rotation of the fibula (Figure 6).
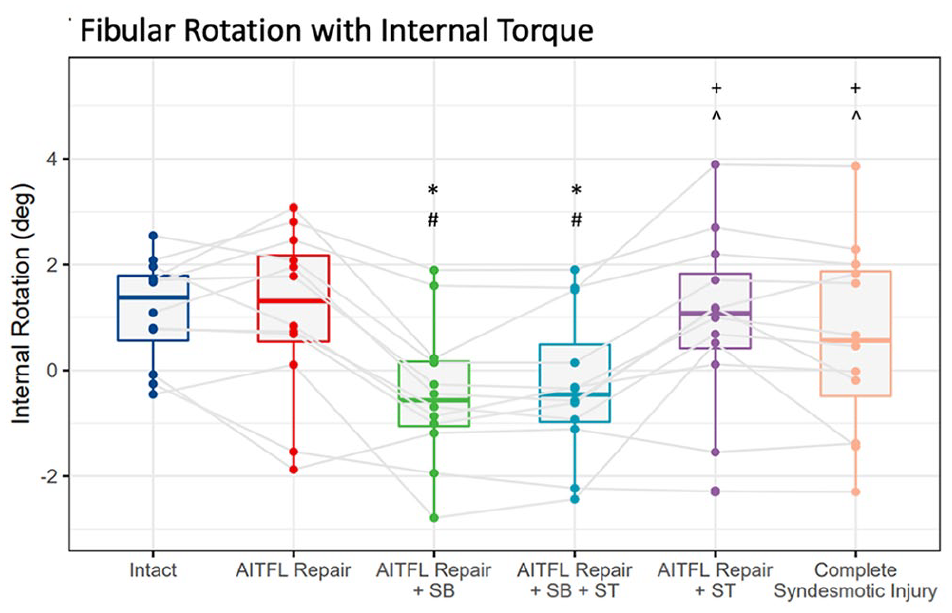
Box plot graph demonstrating fibular rotation in degrees relative to the tibia during the internal rotation test. *Significant difference compared to intact state. #Significant difference compared to AITFL suture repair state. +Significant difference compared to AITFL suture repair + SB state. ^Significant difference compared AITFL suture repair + SB + ST state. AITFL, anterior inferior tibiofibular ligament; SB, suture button; ST, suture tape.
Talus Rotation
With an external rotation torque through the foot, none of the tested repairs restored the talus rotation back to the intact state, all showing significantly more external rotation of the talus relative to the tibia (Figure 7). However, the repair states that used ST significantly reduced external rotation of the talus compared with the injury state (AITFL suture repair + ST: mean −1.28 degrees, P < .001; AITFL suture repair + SB + ST: mean −1.36 degrees, P = .008). The repairs that did not use ST were not significantly different from the complete syndesmotic injury state in talus external rotation.
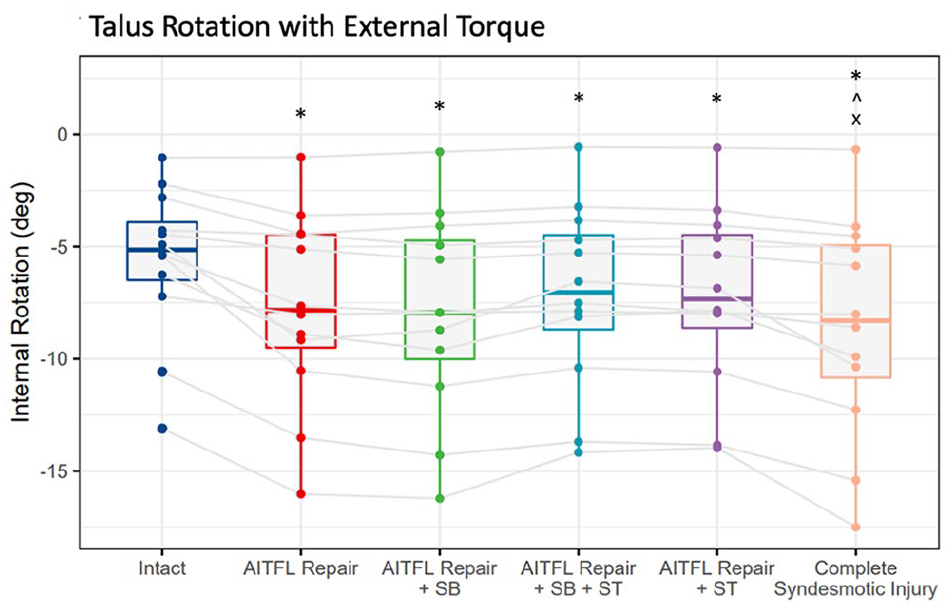
Box plot graph demonstrating talus rotation in degrees relative to the tibia during the external rotation test. *Significant difference compared to intact state. ^Significant difference compared to AITFL suture repair + SB + ST state. xSignificant difference compared to AITFL suture repair + ST state. AITFL, anterior inferior tibiofibular ligament; SB, suture button; ST, suture tape.
With an internal rotation torque, only the injury state was significantly different from the intact state showing significantly more internal rotation of the talus (mean 0.52 degrees, P = .035). All the tested repairs restored the talus internal rotation back to the intact state.
Discussion
The most important finding of this study was that in an isolated syndesmotic injury model, AITFL suture repair and AITFL augmentation with ST most accurately restored stability and the 3-dimensional anatomic relationships of the tibia, fibula, and talus under simulated physiologic or stress loading conditions. ST augmentation may add additional constraint to talus rotational laxity. It also confirms the tendency of SB fixation to overtighten or over-reduce the syndesmosis and produce a small but significant degree of external rotation of the fibula, as seen in previous reports.29,32
The current study was designed to evaluate isolated syndesmotic injuries under simulated physiologic or stress loads and not higher torques used in prior studies, which could explain the lack of posterior fibular translation in this study. Additionally, the subtalar joint was fused in this study in order to isolate the tibiotalar joint, which also could have contributed to the lack of fibular posterior translation. Previous studies have shown increased posterior translation of the fibula with SB constructs compared to screw constructs, 6 and excessive sagittal plane motion has remained a primary concern with the use of SB in syndesmosis repair.17,21,26,33,34 This study demonstrates a lack of excessive sagittal plane motion under simulated physiologic, lower torque conditions in an isolated syndesmotic injury model.
In agreement with previous literature, this study showed that SB constructs can overtighten or overreduce the syndesmosis. 29 The AITFL suture repair + SB construct was the only state with significantly different coronal plane motion compared to the intact state, showing more medial fibular translation. It is important to keep in mind that testing is performed at time zero, and it is thought that SB constructs loosen over time.17,18,28 A retrospective review of 56 patients who underwent syndesmotic repair with an SB construct showed an average of 1.1-mm increase in distance between the buttons at final follow-up. 28 The mean amount of medial translation of AITFL suture repair + SB fixation was 0.72 mm in our study. Another important finding was that AITFL suture repair + ST augmentation did not cause significant overcompression of the syndesmosis, and the fibula was stable in the coronal plane under physiologic loads.
A similar cadaveric study published by Wood et al 37 evaluated the kinematics of the fibula and tibia after a syndesmotic injury under an external rotation stress with repairs using 1 SB, 2 divergent SBs, and both with the addition of AITFL suture anchor augment. They found that the addition of ST augmentation to SB fixation provided more fibular external rotation constraint than an SB fixation alone, but none of the repair states restored the external rotation of the fibula back to the uninjured state. In the current study, AITFL suture repair + ST augmentation + SB fixation also showed less external rotation of the fibula than the SB alone, but this difference was not significant. However, AITFL suture repair and AITFL suture repair + ST augmentation both restored fibular rotation back to the intact state. In the study by Wood et al, 37 double the amount of torque was used in testing, manual as opposed to robotic rotation was performed, the ankle was held in 10 degrees of dorsiflexion as opposed to neutral, and the PITFL and ITFL were left intact whereas they were transected in the current study. These design differences could help explain the difference in findings between the 2 studies. The information from both studies suggests that SB fixation alone allows excessive external rotation of the fibula and that anatomic suture repair or ST augmentation of the AITFL reduces or prevents excess rotation of the fibula.
The AITFL has been shown to be the most commonly disrupted ligament in a syndesmosis injury.7,23,37 Restoring anatomy should in theory restore native motion and stability so it is not surprising that direct repair or reinforcement of the AITFL can provide intact state kinematics. Multiple studies have provided evidence supporting anatomic repair or fixation of the AITFL.15,27,35 Shoji et al 30 evaluated the fibular rotational angle during ankle dorsiflexion, inversion, and external rotation forces and found that ST augmentation alone and in combination with SB fixation reproduced intact fibular rotation better than screw fixation or SB fixation alone, although the PITFL was left intact with their study. Teramoto et al 33 found that anatomic SB fixation, directed from the posterior cortex of the fibula to the anterolateral edge of the tibia (in line with the AITFL), provided the most physiologic stabilization of the fibula and syndesmosis compared to screw fixation, single-SB, and double-SB constructs with standard placement.
Additionally, the kinematics of the tibiotalar joint were better restored with repairs that utilized ST augmentation compared to AITFL suture repair alone or AITLF suture repair + SB fixation. Even though none of the repair states restored talus rotation back to the intact state, the repairs that used ST augmentation reduced the talus external rotation laxity compared to the complete syndesmotic injury. This could be explained by mortise stability or increased external rotation constraint from the fibula with the ST augmentation. In agreement with our study, Goetz et al 10 also found that SB fixation allowed significantly increased talar rotation whereas both screw fixation and anatomic AITFL and deltoid ligament repair using suture tape was able to decrease the talar rotation. The current study did not include a deltoid ligament repair but found the same talar constraint, which suggests AITFL repair is also important in restoring rotational motion of the talus. Similarly, Liu et al 22 showed excessive talus rotation after inferior tibiofibular syndesmosis injury, which was decreased but overconstrained with screw fixation.
Another possible indication for AITFL repair or augmentation is an abnormal morphology to the incisura, which would create an inherently unstable distal tibiofibular joint and a predisposition to malreduction. 36 A prospective study using bilateral CT scans of patients who underwent SB syndesmotic fixation found that patients with a shallow incisura had significantly more anterior fibular translation compared to the contralateral limb and that patients with a deep incisura had significant posterior and rotational malreduction compared to the contralateral side. 4 Direct anatomic repair of the AITFL may be a good alternative in patients with abnormal anatomy at the syndesmosis and would be an excellent topic for further research.
This study adds to the growing body of literature supporting the use of direct syndesmosis ligament repair, 16 specifically for additional rotational constraint. AITFL augmentation may be a good operative alternative for isolated syndesmotic injuries without significant fibular displacement, injuries that primarily involve damage to the AITFL, abnormal syndesmotic anatomy, or in revision settings. A recent clinical study by Kim et al 16 showed excellent clinical results and early return to play for athletes treated for isolated unstable syndesmotic injuries without fibula fractures using suture anchor fixation of the AITFL. Further clinical trials are needed to determine the role for ST augmentation of the AITFL in syndesmotic injuries.
The authors acknowledge the limitations of the present study. This biomechanical cadaveric analysis is performed at time zero, which does not account for the effects of biological healing or postoperative rehabilitation protocols. The operative constructs can fatigue or stretch with repeated testing as well. Additionally, all soft tissue and muscle was removed except for ligamentous structures in order to perform precise repairs and sectioning of the syndesmotic complex which may not accurately represent in vivo settings. Fusing the subtalar joint in order to isolate the tibiotalar joint could alter the talar measurements.
Furthermore, this study only evaluated isolated complete syndesmotic injuries and did not consider other injury patterns that often coexist such as deltoid ligament injuries and fractures. The possible effects of dorsiflexion and plantarflexion at the ankle were not evaluated in the current study, although previous studies have shown that reduction of the syndesmosis when fixed with an SB construct was not dependent on ankle position. 19 No comparison was made with screw fixation or double-SB constructs. It is important to note that the clinical significance of small amounts of rotational malalignment or translation are unknown; however, biomechanical studies have shown increased and abnormal tibiotalar contact pressures with small degrees of increased fibular movement after syndesmosis injuries. 14 Lastly, the clinical implications of a cadaveric biomechanical study under simulated conditions are unknown, and clinical trials are necessary to make any definitive conclusions.
Conclusion
Overall, the data from this cadaveric model study shows that under simulated physiologic loads in an isolated complete syndesmotic injury model, AITFL suture repair and AITFL augmentation with suture tape most accurately restored stability and the 3-dimensional anatomic relationships of the tibia, fibula, and talus. Augmentation with suture tape provides additional external rotation constraint for the talus compared to suture repair alone or SB fixation. In this setting, SB fixation was found to slightly overcompress and externally rotate the fibula.
Supplemental Material
sj-docx-3-fai-10.1177_10711007221082933 – Supplemental material for Anterior Inferior Tibiofibular Ligament Suture Tape Augmentation for Isolated Syndesmotic Injuries
Supplemental material, sj-docx-3-fai-10.1177_10711007221082933 for Anterior Inferior Tibiofibular Ligament Suture Tape Augmentation for Isolated Syndesmotic Injuries by Marissa D. Jamieson, Ingrid Kvello Stake, Alex W. Brady, Justin Brown, Kira K. Tanghe, Brenton W. Douglass and Thomas O. Clanton in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_10711007221082933 – Supplemental material for Anterior Inferior Tibiofibular Ligament Suture Tape Augmentation for Isolated Syndesmotic Injuries
Supplemental material, sj-pdf-1-fai-10.1177_10711007221082933 for Anterior Inferior Tibiofibular Ligament Suture Tape Augmentation for Isolated Syndesmotic Injuries by Marissa D. Jamieson, Ingrid Kvello Stake, Alex W. Brady, Justin Brown, Kira K. Tanghe, Brenton W. Douglass and Thomas O. Clanton in Foot & Ankle International
Supplemental Material
sj-pdf-2-fai-10.1177_10711007221082933 – Supplemental material for Anterior Inferior Tibiofibular Ligament Suture Tape Augmentation for Isolated Syndesmotic Injuries
Supplemental material, sj-pdf-2-fai-10.1177_10711007221082933 for Anterior Inferior Tibiofibular Ligament Suture Tape Augmentation for Isolated Syndesmotic Injuries by Marissa D. Jamieson, Ingrid Kvello Stake, Alex W. Brady, Justin Brown, Kira K. Tanghe, Brenton W. Douglass and Thomas O. Clanton in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Marissa D. Jamieson, MD, received monetary and product support for this investigator-initiated study from Arthrex and funds/reimbursement by the University of Colorado Department of Orthopedic Surgery.
Ingrid Kvello Stake, MD, position at the Steadman Philippon Research Institute was partially supported by Arthrex, Inc. Alex W. Brady, MS, received monetary and product support for this investigator-initiated study from Arthex, Inc. Thomas O. Clanton, MD, reports support from Arthrex, Inc, which provided product to the author’s research institute to use for the study; receives royalties or licenses from Arthrex, Inc, and Stryker, Inc, for products unrelated to this research project; consulting fees from Arthrex, Inc, Synthes, Inc, and Wright Medical, Inc; receives consultant payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from BICMD, Arthrex, Inc, Stryker, Inc, and Wright Medical; and received materials for biomechanical research projects from Arthrex, Inc. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.