
Abstract
Background:
Calcaneal tuberosity avulsion fractures are challenging to treat because of the poor bone stock and high risk of fixation failure secondary to the strong Achilles tendon pull. The purpose of this study is to compare the tensile force to failure of 2 different types of screw fixation construct in a cadaveric model of calcaneal tuberosity avulsion fracture.
Methods:
An oblique osteotomy was created in the calcanei of 7 matched pairs of cadaveric specimens to simulate a tuberosity avulsion fracture and one specimen from each pair randomized into one of the 2 groups for comparison. Two cancellous screws were inserted perpendicular to the fracture line at the posteromedial and posterolateral corners of the avulsed fragment for the 2-screw construct. For the second group, an additional stab incision was made at the midline of the Achilles insertional region for a screw placed between the initial 2 screws with a trajectory toward the calcaneocuboid joint in the 3-screw construct. These specimens were then mounted and loaded to failure.
Results:
The mean force to a predefined failure at 3.0-mm gap for the 3-screw construct was 468.7 ± 267.9 N vs 278.9 ± 164.0 N for the 2-screw construct (P < .001). The addition of a central nonparallel screw in the 3-screw construct significantly increased the force required for fracture gap displacement at all cut-off points (1.0-8.0 mm) when compared to the 2-screw construct (P < .001). Notably, the mean peak tensile force for the 3-screw construct was 499.4 ± 255.4 N occurred at the gap displacement of 4.1 mm for the 3-screw construct whereas the mean peak tensile force for the 2-screw construct was 315.9 ± 162.4 N displacing the gap at 4.3 mm.
Conclusion:
This study showed that an additional central nonparallel screw in the 3-screw construct provided significant mechanical superiority compared to a 2-screw construct.
Clinical Relevance:
The present study supported the use of augmented fixation with an additional central off-axis screw to reduce risk of fixation failure in calcaneal tuberosity avulsion fractures.
Introduction
Calcaneal tuberosity avulsion fractures are uncommon injuries that pose a high risk of skin compromise.3,4,5,11,12,16-18 The superiorly displaced tuberosity fragment often tents the skin overlying the posterior heel leading to ischemia and skin necrosis if not managed in an emergent manner.3,4,5,11,12,16-18 These types of avulsion fracture differed from the more common intra-articular calcaneal fracture because it occurs from the intense contractions of the gastrocnemius-soleus complex during forced dorsiflexion of the ankle with or without trauma.3,4,16 Risk factors for these avulsion fractures were reported to be intrinsic gastrocnemius tightness, diabetics, osteoporotic, and elderly patients.4,5,7,14,15,16-18,21,22 They are challenging to fix because of poor bone stock and an increased risk of fixation failure that is largely contributed by the strong avulsion force of the Achilles tendon.4,5,7,12,14,15,16-18,21,22
In terms of fixation, there is no consensus for the optimal construct with various types of fixation techniques being reported in multiple scattered case reports and small series looking at screw fixation techniques with or without augmentation with suture anchors, cerclage/tension band wiring, and plating to improve fixation strength.1,10,12,13,15,17,19,20,22 Although conventional fixation construct as recommended by OTA/AO utilizes 2 or 3 cortical lag screws inserted perpendicular to the fracture line with bicortical purchase after appropriate reduction, 3 screw fixation alone has been shown to be inadequate to resist the strong Achilles tendon pull in a cadaveric study. 16 Mitchell and colleagues 18 demonstrated 28.2% fracture displacement or implant failure from a cohort of 39 patients treated with screw fixation, whereas Gitajn et al 12 reported 38.5% fixation failure with cannulated lag screws in their review of 33 calcaneal avulsion fractures. In the only other cadaveric study, Khazen et al found that 2 × 4.0-mm lag screw fixation perpendicular to the fracture augmented by suture anchors placed in the distal fragment with grasping sutures in the Achilles tendon improved the force to failure for calcaneal tuberosity avulsion fractures when compared to screws alone by neutralizing the Achilles tendon pull and decreases the risk of posterior fracture gapping. 16 Although augmenting screw fixation with suture anchors improve the force to failure of the construct, the extensive exposure needed for suture anchor fixation cannot be recommended if the overlying soft tissue is damaged or compromised. 16
Therefore, the primary aim of this study is to compare the force to failure for 2 different types of screw fixation construct in a cadaveric model of calcaneal tuberosity avulsion fracture. By eliminating extensive dissection for augmented fixation with suture anchors, cerclage wiring or plates, these screw fixation constructs can be performed percutaneously to reduce the risks of soft tissue injury. We hypothesized that the 3-screw fixation construct with a central off-axis screw can neutralize the avulsion force of the Achilles tendon by providing a higher tensile force to failure compared to the conventional 2-screw fixation construct.
Methods
Specimen Preparation
Seven pairs of fresh frozen lower legs were thawed for 24 hours at room temperature prior to dissection. These specimens were obtained from local cadaveric donors and there were 4 males and 3 females with a median age of 74 years (range: 63-88 years). Causes of death were recorded for all specimens (3 died from ischemic heart disease; 2 died from cancer; 1 died from bleeding gastric ulcer; 1 died from bronchopneumonia). All specimens were free from deformities and gross abnormalities during visual inspection. Bone mineral densities (BMDs) of the calcaneus were measured using the dual energy X-ray absorptiometry scan (Hologic Inc., Bedford, MA, USA) for 1 specimen of each pair. BMD measured from the calcanei using dual energy X-ray absorptiometry scan showed a mean T score of -4.91 ± 2.0 (osteoporosis). Following that, 14 calcanei with attached Achilles tendons were carefully dissected from the specimens with extra attention to avoid disrupting the attachment of the Achilles tendon to the calcaneal tuberosity.
In order to achieve optimal results and mitigate inconsistency, an oblique osteotomy was marked following the landmark just posterior to the posterior calcaneal articular facet cartilage lip exiting 2.0 to 3.0 mm inferior to the Achilles tendon insertion to simulate a tuberosity avulsion fracture for all specimens similar to Khazen et al 16 (Figure 1). This osteotomy was performed for all 14 specimens by a single fellowship-trained orthopaedic surgeon using an oscillating saw based on the landmarks marked earlier for consistency and to minimize variability. The fractures were then anatomically reduced under direct visualization and held provisionally with a pointed reduction clamp to allow for compression of both fragments. In one randomly selected specimen of each pair, 2 fully threaded 4.0-mm cancellous screws (Synthes GmbH, Oberdorf, Switzerland) were inserted perpendicular to the fracture line at the posteromedial and posterolateral corners of the posterior superior calcaneal process which is part of the avulsed fragment to achieve bicortical purchase (Figure 2) in compression held by the pointed reduction clamp. These screws were inserted in slight divergent manner guided by an image intensifier to ensure homogeneity.

Illustration of the osteotomy line starting from just posterior to the posterior calcaneal articular facet cartilage lip exiting 2.0 to 3.0 mm inferior to the Achilles tendon insertion to simulate a tuberosity avulsion fracture according to Khazen et al. 16
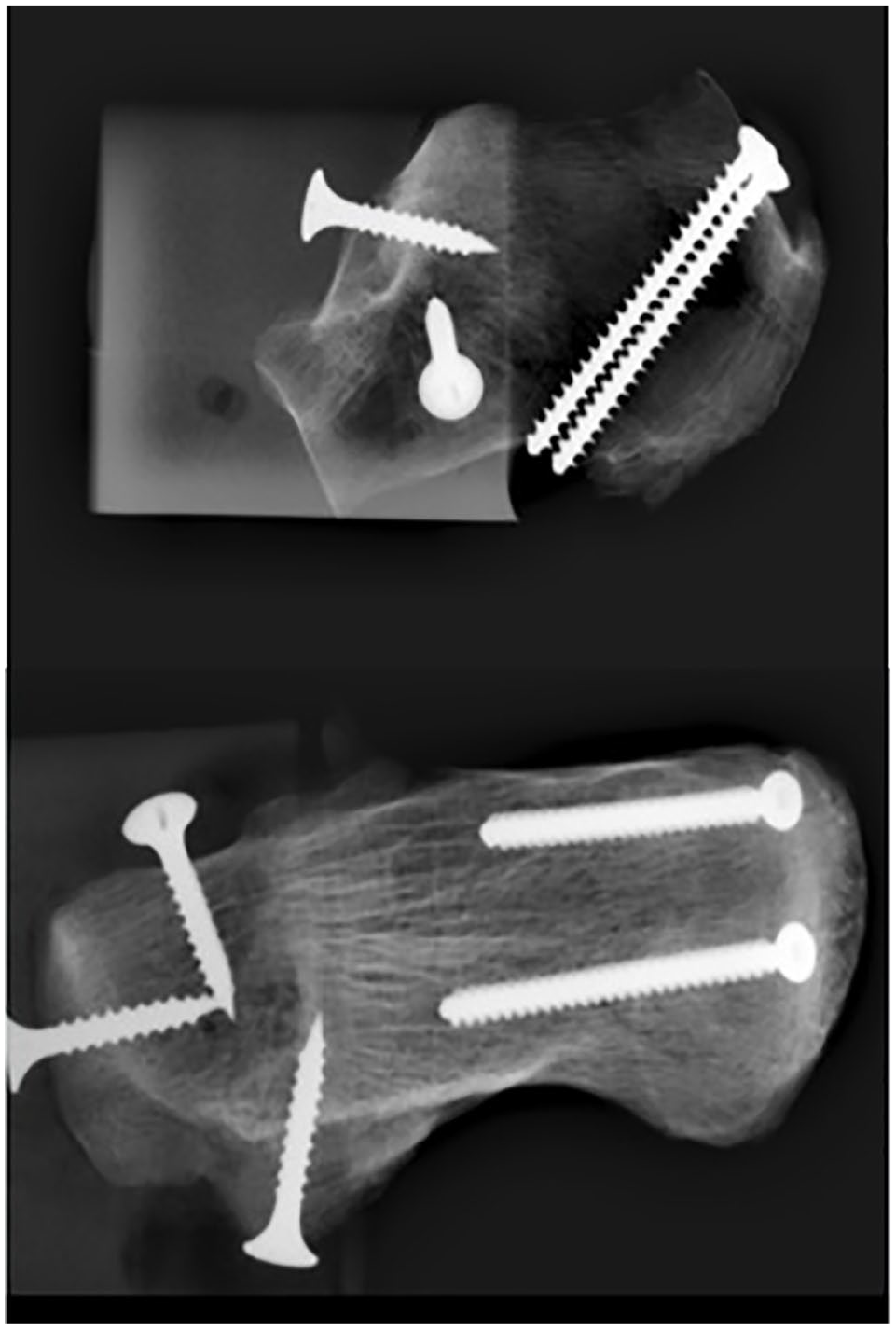
Radiographs of the 2-screw construct in lateral and axial view demonstrating the trajectory of short bicortical screws across the simulated fracture site with presence of the drywall screws into the anterior process of the calcaneus to reinforce potting fixture.
In the remaining specimen of each pair, the specimens were prepared as described above with the 2-screw fixation. However, a small stab incision was made at the midline of the Achilles insertional region. Using clinical palpation of calcaneocuboid joint and image intensifier guidance, an additional fully threaded 4.0-mm cancellous screw was inserted between the initial 2 screws with a trajectory toward the calcaneocuboid joint with an aim to neutralize the Achilles tendon pull (Figure 3).
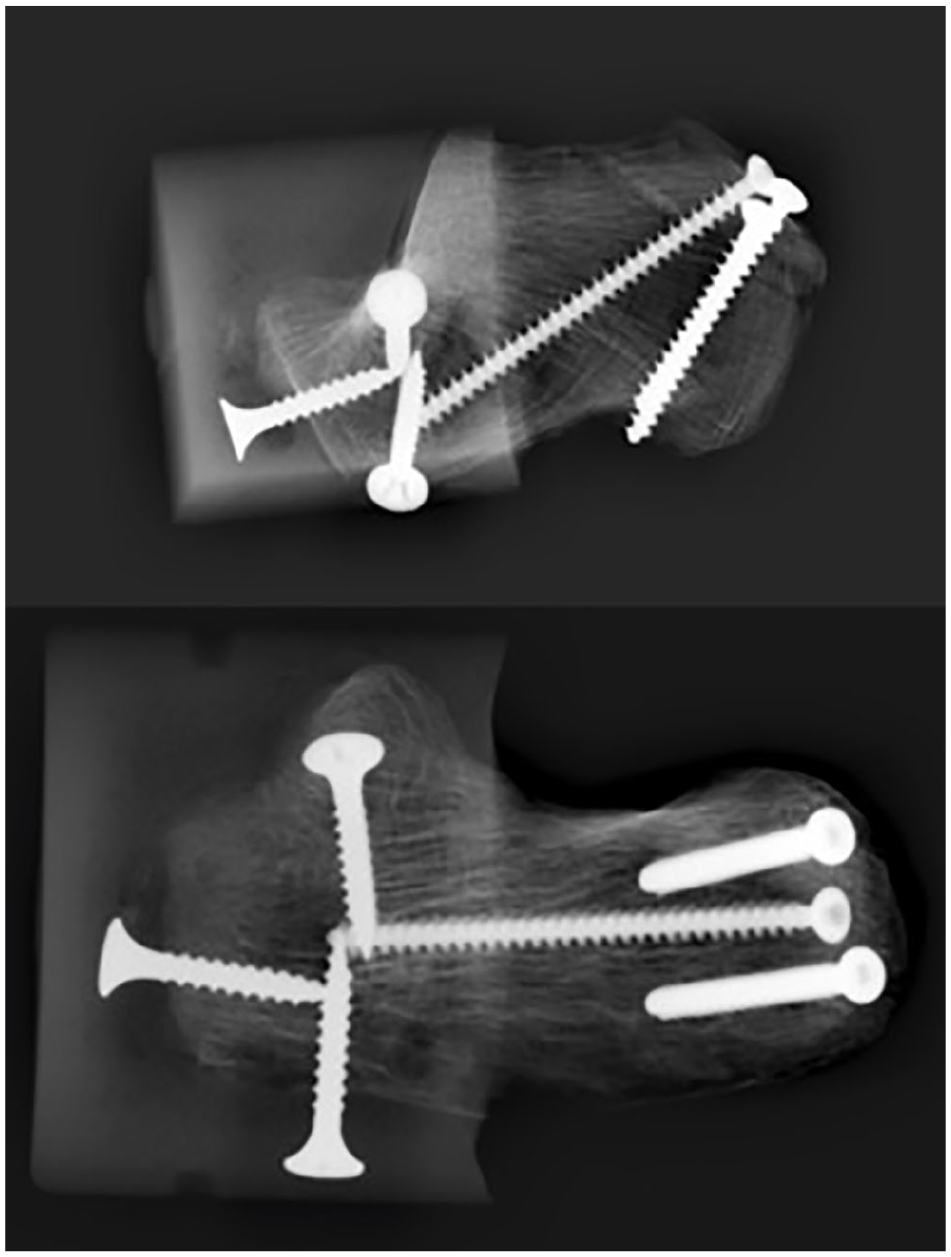
Radiographs of the 3-screw construct in lateral and axial view demonstrating the trajectory of central nonparallel screw toward the calcaneocuboid joint together with the 2 bicortical screws across the simulated fracture site with presence of the drywall screws into the anterior process of the calcaneus to reinforce potting fixture.
Material Setup and Testing
The anterior process of the calcaneus was potted into a customized base fixture using polymethyl methacrylate dental cement (Meliodent; Kulzer GmbH, Hanau, Germany) reinforced with drywall screws (25.0 × 3.5 mm; Phillips Flathead Screw) into the anterior process. Radiographs were taken at this stage to confirm placement of screws and potting position (Figures 2 and 3). This base fixture was custom-made to position the calcaneus at a 30° angle to replicate an early heel rise posture, whereas the direction of Achilles pull was made vertical to the floor based on previous studies (Figure 4). 6 The proximal ends of the tendon were prepared by removing any attached muscle fibers and clamped 10-12 cm proximal to the insertion at the calcaneus using custom-made clamp with sinusoidal grips with reference to Beitzel et al. 6 This custom-made clamp with sinusoidal grips were made up of 3 tampered square waves with an amplitude of 2 mm and wavelength of 15 mm. The male and female part of the grips are tightened together by 4 threaded bolts to provide tight grip to the proximal ends of the tendon. The base and top fixtures were then attached to an MTS 858 Mini Bionix testing machine (Materials Testing System, Eden Prairie, MN) with its default load cell (10 kN with a 1% minimum accuracy as calibrated by manufacturer).
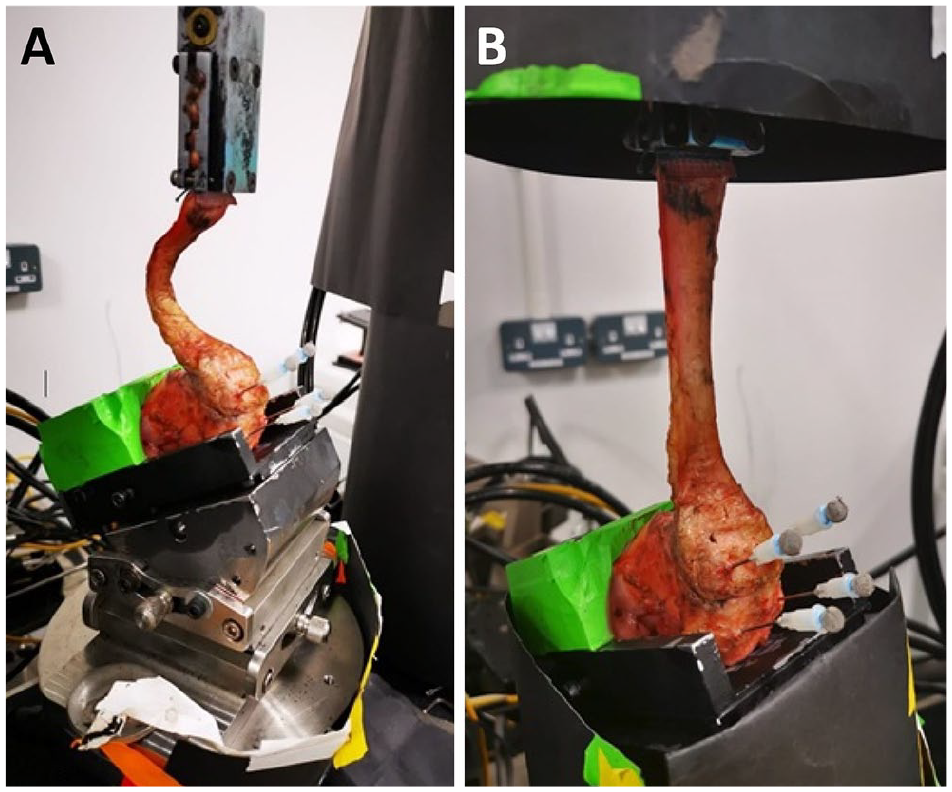
Image of the experimental setup depicting the base fixture that was custom-made to position the calcaneus at 30° angle to replicate an early heel rise posture while the direction of Achilles pull was made perpendicular to the floor based on previous study by Beitzel et al. 6 The tendon (A) prior to tensioning and (4B) after tensioning. Positions of the reflective markers for the Vicon Motion Analysis System are also illustrated here in both panels A and B.
To measure the displacement of the osteotomy line, microminiature differential variable reluctance transducer (M-DVRT) (MicroStrain Inc, Burlington, Vermont) was compared with Vicon Motion Analysis System (Vicon–Oxford Metrics, Oxford, UK) in a controlled testing environment prior to actual experiment to mitigate any potential bias from internal measurement errors. In our preliminary analysis, the Vicon motion analysis system was preferred for 4 reasons: (1) The M-DVRT maximum stroke length is 4.0 mm and any gap displacement beyond 4.0 mm will not be registered rendering load to failure not possible in our analysis; (2) a lower calculated relative error (~3%) as compared to the M-DVRT system (~5%) with respect to the MTS displacement, (3) 3D kinematics measurement is possible, and (3) it is easy to set up. In addition, the Vicon motion analysis system had been considered as a valid and reliable measurement practice in other studies.8,23 Two reflective markers were placed superior and inferior respectively to the posterior fracture site, 5.0 mm medially and laterally off the midline (Figure 4).
The Achilles tendon of each specimen was pretensioned with 10 N, then ramp loaded using an axial tensile force applied to the Achilles tendon at a rate of 25 mm/min until failure. 16 To allow comparison to the previous study by Khazen et al, 16 we defined failure as a simulated fracture gapping of 3.0 mm, screw pullout, screw breakage, or tendon rupture. The proximal-distal displacement of the simulated fracture line was measured using the Vicon Motion Analysis System while the tensile force was measured using the load cell of the MTS machine.
Although Khazen and colleagues selected 3.0 mm as the force-to-failure cutoff for the simulated fracture gap, there was no biomechanical study that determined the point of failure in terms of the size of the gap at the fracture site. 16 Therefore, we address this by identifying the magnitude of the fracture gap created by peak force to failure. As a result, we did not end the study when the simulated fracture gap displaced at 3.0 mm but continued escalating the tensile force applied to the Achilles tendon to maintain the rate of 25 mm/min until the gap size increases to 10.0 mm, or if the construct fails because of the other reasons stated above. The matched force-displacement graph was plotted to determine the force when the gap was 3.0 mm and the peak tensile force.
Statistical Analysis
Using data from Khazen et al’s study (mean load to failure for lag screws alone of 251.3 N and SD of 33.6 N), 16 a power analysis was performed a priori, assuming an alpha value of 0.05 and a power of 0.80, 14 specimens with 7 in each group will be needed to demonstrate a 20% difference in load to failure. Results generated from the study were then compared using the paired t test to determine any statistically significant differences in load to failure, with P ≤.05 considered significant. Data analysis was performed using SPSS (version 16, SPSS Inc, Chicago, IL).
Results
Force to Failure
The addition of a central off-axis screw in the 3-screw construct significantly increased the force required for measured fracture gap displacement at all cutoff points (1.0-8.0 mm) when compared to the 2-screw construct (P < .001) with a percentage difference of at least 38.6% (Table 1). When we compare to the previous study by Khazen et al, 16 the mean force to failure (defined as a 3.0-mm gap) for the 3-screw construct was 468.7 ± 267.9 N, whereas the mean force to failure was 278.9 ± 164.0 N for the 2-screw construct with a statistically significant difference of 189.8 N (40.5%) (P < .001).
Force Required to Displace the Fracture Gap at Each 1.0-mm Cutoff Point Between the 3-Screw vs 2-Screw Construct.
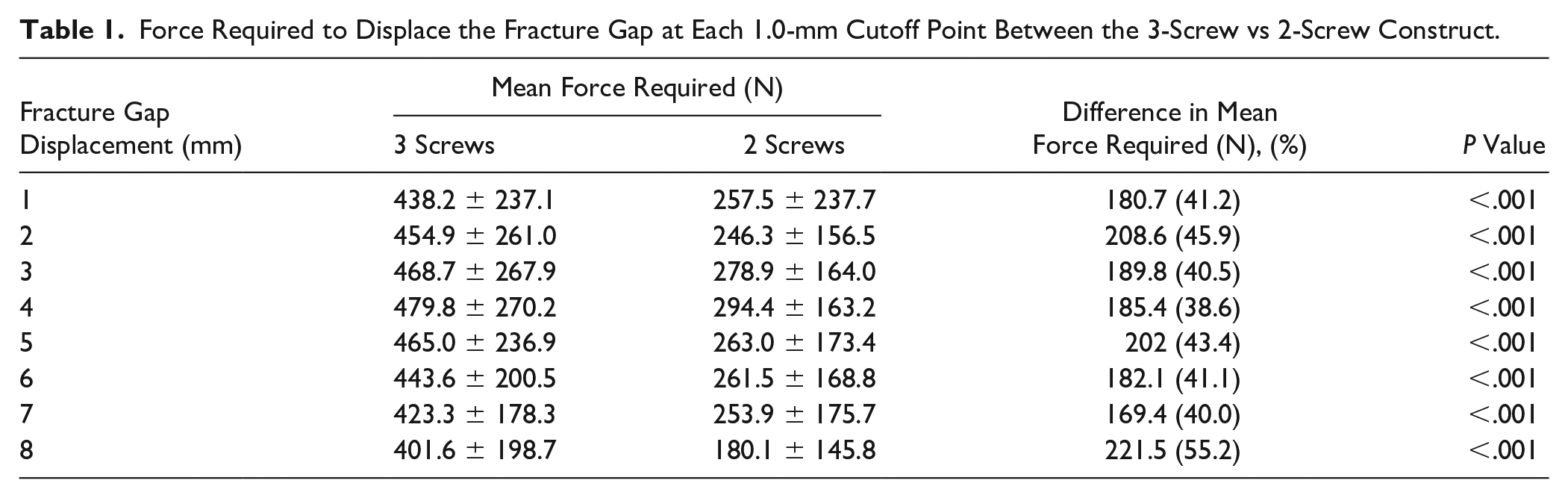
Notably, the mean peak tensile force for the 3-screw construct was 499.4 ± 255.4 N occurred at the gap displacement of 4.1 mm for the 3-screw construct whereas the mean peak tensile force for the 2-screw construct was 315.9 ± 162.4 N displacing the gap at 4.3 mm.
Force-Displacement Graph
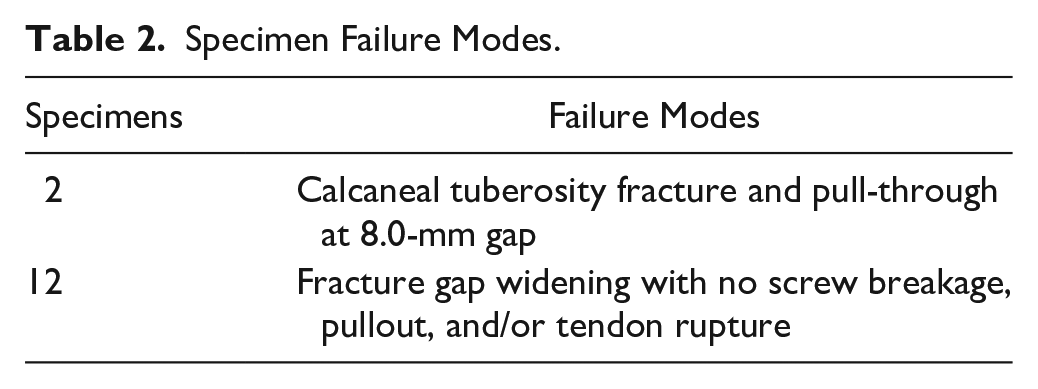
The force-displacement curve for both constructs illustrate an upward slope for the force require to displace the fracture gap up to a 4.0 mm gap where it began a downward slope. The average force required to displace the fracture gap gets progressively less once the gap was > 4.0 mm (Figure 5). The gap displacement measurement was stopped at 8.0 mm instead of the initially planned 10.0 mm in view of 2 specimens from the 2-screw construct failed because of calcaneal tuberosity fracture and pull-through. The remaining specimens from both the 2-screw and 3-screw constructs failed by fracture gap widening with no screw breakage, pullout, and/or tendon rupture (Table 2).
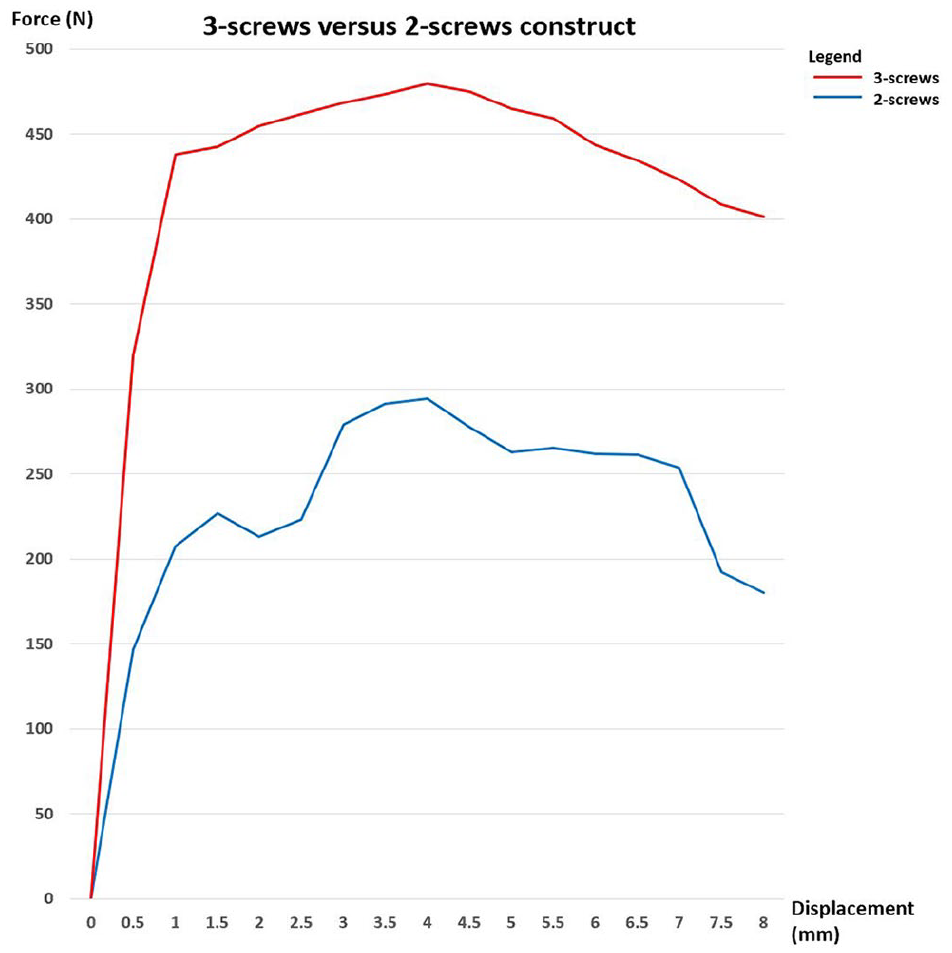
Force-displacement curve for the 2- and 3-screw constructs demonstrating the force required to displace a fracture gap followed by the progressively lower force needed to displace the gap after 4.0 mm.
Specimen Failure Modes.
Discussion
The results of this biomechanical study proved our hypothesis that an additional central nonparallel screw in the 3-screw construct provided statistically significant biomechanical superiority with nearly twice the load force necessary before failure as compared with a 2-screw construct. Impressively, the mean force needed to displace the fracture gap after failure continued to demonstrate superiority in the 3-screw construct up to an 8.0-mm gap with statistical significance. Correspondingly, Akizuki and colleagues reported that patients ambulating in an ankle immobilizer in neutral dorsiflexion will continue to experience Achilles forces of up to 369 N. 2 Therefore, these findings support the use of a central nonparallel screw in the 3-screw construct directed toward the calcaneocuboid joint to prevent early failure by neutralizing the Achilles tendon pull.
In the only other biomechanical study on calcaneal tuberosity avulsion fractures, Khazen et al found that 2 suture anchors augmentation of the conventional 2 lag screws fixation provided statistically significant force to failure (defined as a 3.0-mm gap) at 441.6 ± 39.9 N vs screws alone at 251.3 ± 33.6 N (P = .002). 16 Owing to the lack of biomechanical studies on calcaneal tuberosity avulsion fractures, we draw comparisons from almost similar biomechanical studies evaluating Achilles tendon insertional tendinopathy repair strength with suture anchors. Beitzel et al 6 compared 18 cadaveric specimens and reported that the load to failure for the knotted double-row repair was greater at 354.7 ± 106.2 N, whereas the single-row repair specimens failed at 197.8 ± 39.5 N. On the other hand, Cox et al 9 demonstrated in their study of 10 cadaveric specimens comparing knotted vs knotless double-row repair failed at 317.8 ± 93.6 N for the knotted group compared with 196.1 ± 12.9 N for the knotless group. Our results echo similarities in terms of improved construct fixation strength with just an additional central nonparallel screw in the 3-screw construct. We also postulate that this long central nonparallel screw in the 3-screw construct that is inserted more horizontally with an extended length into the thicker portion of the body of calcaneus provided better bony purchase and resisted displacement through a long lever arm when compared to the short bicortical screws placed perpendicular to the fracture line in which the holding forces are their threads only.
Calcaneal tuberosity avulsion fractures have a high risk of soft tissue compromise and a high risk of fixation failure.4,5,7,12,14,15,16-18,21,22 Up to 45% of patients presented with soft tissue complications such as skin tenting and blistering in a recent review from a multicenter study with high complication rates. 18 Early reduction and fixation to prevent secondary soft tissue complications from the persistent pressure and skin tenting by the avulsed fragment is vital especially with the use of minimally invasive or percutaneous techniques to prevent further insult to the compromised soft tissue envelope.2-7,9,10,15 Multiple case reports on augmented fixation with additional suture anchors, cerclage wiring, suture button, and even plating would require extensive soft tissue dissection to allow these supplemental fixations to hold.3,4,16 As there is little data and no consensus regarding the ideal fixation construct with a need to protect the already-compromised soft tissue envelope at the posterior heel, this 3-screw construct utilizing a long central nonparallel screw directed at the anterior process of the calcaneum could provide the additional fixation strength and at the same time protect the soft tissue envelope with its percutaneous nature of insertion. However, as a cadaveric study, the clinical implication of this additional stab incision for the central nonparallel screw on the soft tissue envelope is unknown because soft tissue complications are high in various clinical reports. This vital point was also corroborated by Khazen et al 16 in their conclusion that the extensive exposure necessary with use of suture anchors and other implants can provide better visualization and anatomic reduction with good fixation strength, but it cannot be recommended if the overlying skin is at risk. Although Khazen and colleagues 16 defined a 3.0-mm gap opening at the simulated fracture as failure, there was no literature to support a 3.0-mm gap as fixation failure. Therefore, we sought to understand what should be considered as the threshold for fracture gaping to be considered as fixation failure. Interestingly, the force-displacement curve showed that once the fracture gap was displaced >4.0 mm, progressively lower force is needed to produce further displacement of the fracture gap. The force-displacement curve showed a downward trend for any gap 4.1 mm or more for both the 2- and 3-screw construct up to an 8.0 mm gap. If translated to clinical setting, we propose that surgeons may want to consider refixation of the calcaneal tuberosity avulsed fragment if it was noted to displace >4.0 mm acutely postoperatively to prevent further displacement as the average force needed for further displacement is significantly lower.
This study is limited as with other cadaveric studies because the study was performed immediately after simulated fracture without considering fracture healing and the effect of immobilization. However, this reflects the time of failure in real clinical scenario as most fracture fixation failures occur quite early before healing has occurred.3,5 In addition, the use of cadaveric specimens may also lead to variations in tissue morphology and the BMD scores for the specimens were all osteoporotic in nature. Because of that, we randomized one of each pair of calcanei to receive either the 2- or 3-screw construct in order to control for variations in patient demographics. Although the BMD scores were in osteoporotic range, it suited the demographic of patients at high risk for calcaneal tuberosity avulsion fractures as reported by many previous authors.2,3,11-15 A larger screw could also be used as the central nonparallel screw for the 3-screw construct but decision was made to use a similar sized 4.0-mm screw because of its smaller size to prevent fragmentation of the avulsed bone and ease of insertion via a small stab incision to mitigate further soft tissue insult in a clinical setting. Finally, the application of this finding to clinical setting may be limited by the biomechanical setup as it was difficult to re-create accurate physiological loads although the intention to evaluate biomechanical stability of the fixation construct was achieved.
Conclusion
This study showed that an additional central nonparallel screw in the 3-screw construct directed toward the calcaneocuboid joint provided statistically significant biomechanical superiority with nearly twice the load necessary before failure as compared with a 2-screw construct for fixation of calcaneal tuberosity avulsion fracture.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007221130007 – Supplemental material for Biomechanical Comparison of a Novel 3-Screw Fixation vs Conventional 2-Screw Fixation of Calcaneal Tuberosity Avulsion Fractures
Supplemental material, sj-pdf-1-fai-10.1177_10711007221130007 for Biomechanical Comparison of a Novel 3-Screw Fixation vs Conventional 2-Screw Fixation of Calcaneal Tuberosity Avulsion Fractures by Choon Chiet Hong, Jun-Hao Tan, Amit Kumarsing Ramruttun and Christopher Jon Pearce in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors report all support for the present manuscript (eg, funding, provision of study materials, medical writing, article processing charges, etc) from National University Hospital’s Orthopaedic Pitch For Fund, Grant amount: SGD$10,000; the authors received the Department of Orthopaedic Surgery, National University Hospital’s Orthopaedic Pitch For Fund grant of SGD$10,000 in 2020 mainly for the cost of the bone mineral density scan (for cadaveric specimens), biomechanical laboratory usage (dissection, potting, biomechanical equipment [MTS Bionix and Vicon Motion Analysis System], purchasing of screws and raw materials as well as use of X-ray machine for radiographs) and finally the disposal cost.
Ethical approval
Ethical approval for this study was obtained from National Healthcare Group (NHG) Research Online Administration & Management (ROAM): Approval ID: 2019/00992.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.