
Abstract
Background:
The posterolateral approach to the ankle allows for reduction and fixation of the posterior and lateral malleoli through the same surgical incision. This can be accomplished via 1 or 2 surgical “windows.” The purpose of this study is to compare outcomes including wound complications following direct fixation of unstable rotational ankle fracture through the posterolateral approach using either 1 or 2 surgical windows.
Methods:
One hundred sixty-four patients with bi- or trimalleolar ankle fractures treated using the single-window posterolateral approach (between the peroneal tendons and the flexor hallucis longus [FHL]) or the 2-window technique (between the peroneal tendons and the FHL for posterior malleolus fixation; lateral to the peroneal tendons for fibula fixation) were reviewed for demographics, radiographic details, and clinical outcomes. We were able to review these 164 at the 3-month follow-up and a subset of 104 at a minimum of 12-month follow-up.
Results:
One hundred eight ankles had the single-window approach; 56 had the 2-window approach. These 2 cohorts did not differ in demographic or injury characteristics. Ankles in the 2-window group experienced a greater number of early (3 months postsurgery) wound complications (32% vs 12%, P < .01). Two-window patients had more wound complications among ankles treated later than 1 week after injury (44% vs 16%, P < .01). There was no difference in surgical site infection, with low rates in both cohorts. Single-window patients had greater plantarflexion (35 ± 10 vs 30 ± 11 degrees, P = .025) and dorsiflexion after 12 months (21 ± 10 vs 16 ± 11 degrees, P = .021). We did not find a significant difference in nerve complications for these 2 cohorts.
Conclusion:
In our study, we found the single-window posterolateral approach to be associated with fewer wound complications and better postoperative range of ankle motion when compared to the 2-window approach.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Ankle fractures are among the most common fractures treated by orthopaedic surgeons.6,13 Those involving the posterior malleolus comprise between 7% and 44% of all ankle fractures. 12 With isolated posterior malleolus fractures constituting just 0.5% to 1% of these injuries, posterior malleolus fractures are most frequently seen along with lateral and/or medial malleolus ankle fractures. 3
Indications for posterior malleolus fracture fixation remain controversial. Historically, posterior malleolus fractures were only indicated for direct repair when the fragment constituted at least 25% to 30% of the tibia’s articular surface from a lateral view X-ray or CT scan.5,8,17 However, more recent studies have demonstrated that fixation of smaller posterior malleolus fractures creates a more stable construct and may restore the syndesmosis.9,12,14 It has been our practice to fix most posterior malleolus fractures when surgically feasible, especially when associated with dislocations.
As noted by Talbot et al, 19 the posterolateral approach has many advantages. It gives surgeons a more direct approach to inspection and fixation of the posterior malleolus for impaction and comminution. Furthermore, with patients placed in the prone position, surgeons do not have to fight gravity, making fracture-dislocations easier to treat.19,21 The posterolateral approach also places the incision over soft tissue rather than bone, providing protection in case of wound breakdown. One of the greatest advantages of the posterolateral approach is allowing surgeons to reduce the lateral malleolus and the posterior malleolus through the same incision.
There are 2 variations to the posterolateral approach. The first is the single-window approach (Figure 1). Here, both the lateral and posterior malleoli are reduced and fixed through the same interval between the peroneal tendons and the flexor hallucis longus (FHL). The second method is the 2-window approach, where the surgeon views and reduces the posterior malleolus in an interval between the peroneal tendons and the FHL and uses a second interval lateral to the peroneal tendons for lateral malleolus fixation (Figure 2). A benefit of the 2-window approach is it allows the option of direct lateral fibula plating if needed. The approach used is based on either surgeon preference or fracture configuration requiring either a posterior or lateral fibula plate. To our knowledge and literature search, there are no reports that compare these 2 methods.
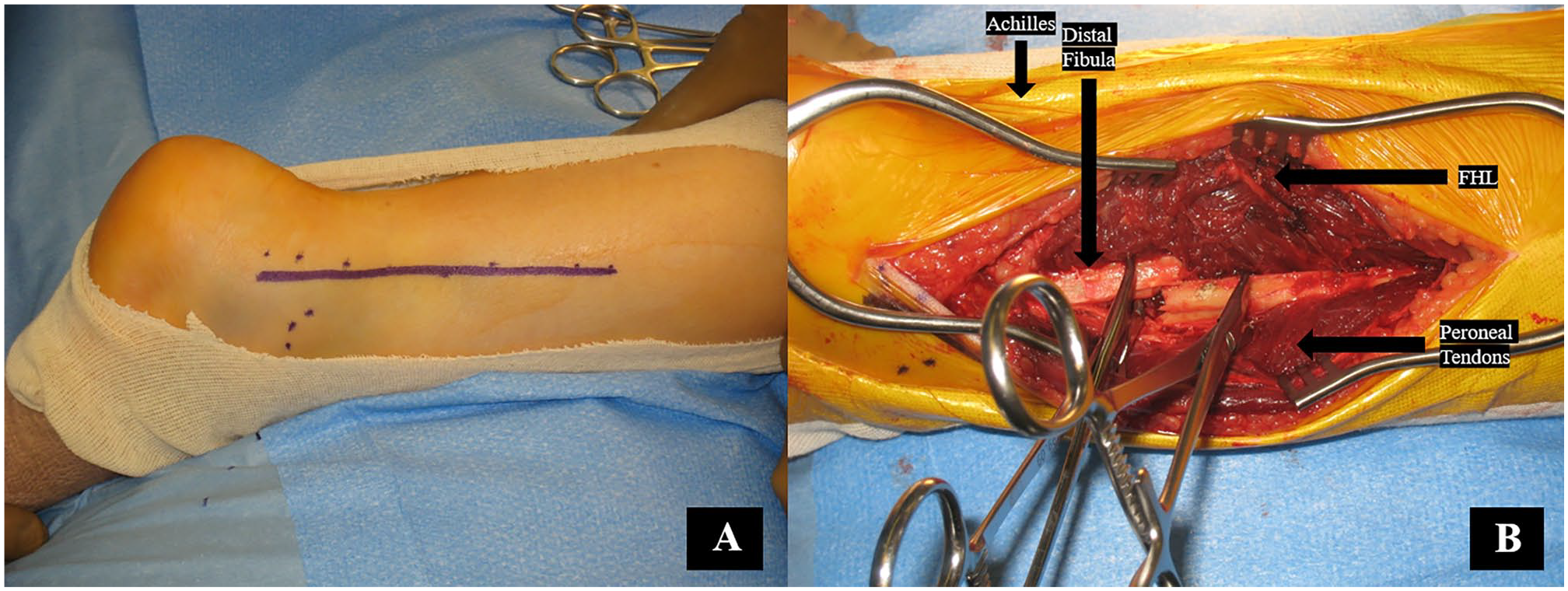
The single-window approach. (A) Patient positioned prone with incision marked between the Achilles and fibula. (B) Single-window interval between peroneal tendons and flexor hallucis longus.
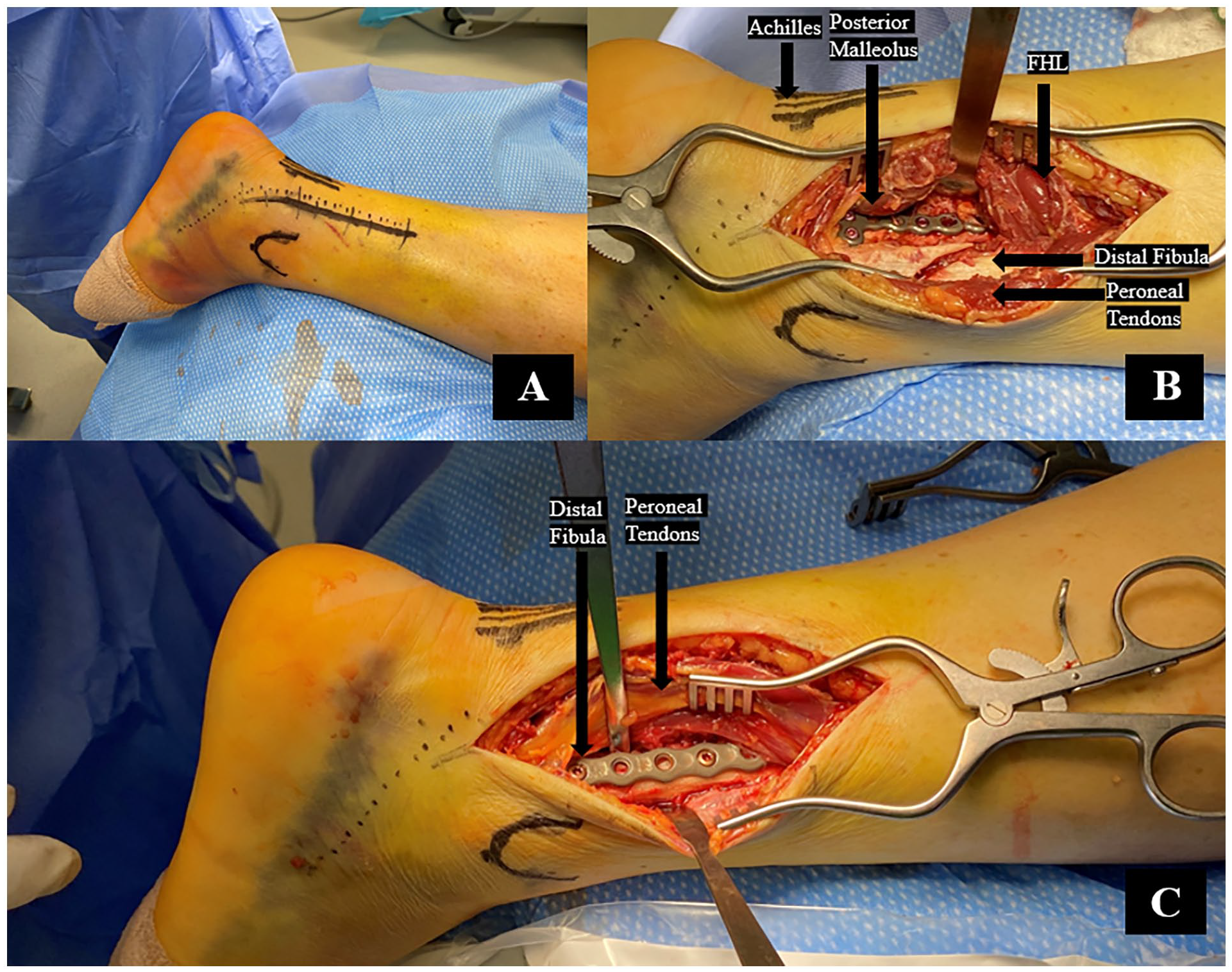
The 2-window approach. (A) Patient positioned prone with incision marked between Achilles and Fibula. (B) Medial window. (C) Lateral window.
The aim of this study is to compare the incidence of wound complications and clinical outcomes between the single- and 2-window approaches in patients with ankle fractures involving the posterior and lateral malleoli that underwent fixation using the posterolateral approach. We hypothesize that the 2-window approach will be noninferior in outcome measures and wound complications.
Materials and Methods
An IRB-approved database of surgically treated ankle fractures was queried for this study. Between May 2013 and April 2021, a total of 173 patients with rotational ankle fractures involving the distal fibula and the posterior malleolus requiring open reduction and internal fixation via the posterolateral approach were identified and retrospectively studied (Figure 3A and B, Figure 4A and B). Unstable ankle fractures were operated upon (eg, bimalleolar or trimalleolar fracturs with posterior malleolus fracture). Three fellowship-trained orthopaedic trauma surgeons performed all surgeries on these patients. Preoperative radiographs and CT scans were assessed using PACS (Siemens; Erlanger, Germany) by the surgeon to determine the percentage of articular surface of the tibia in the ankle joint separated as part of the posterior malleolus fragment.
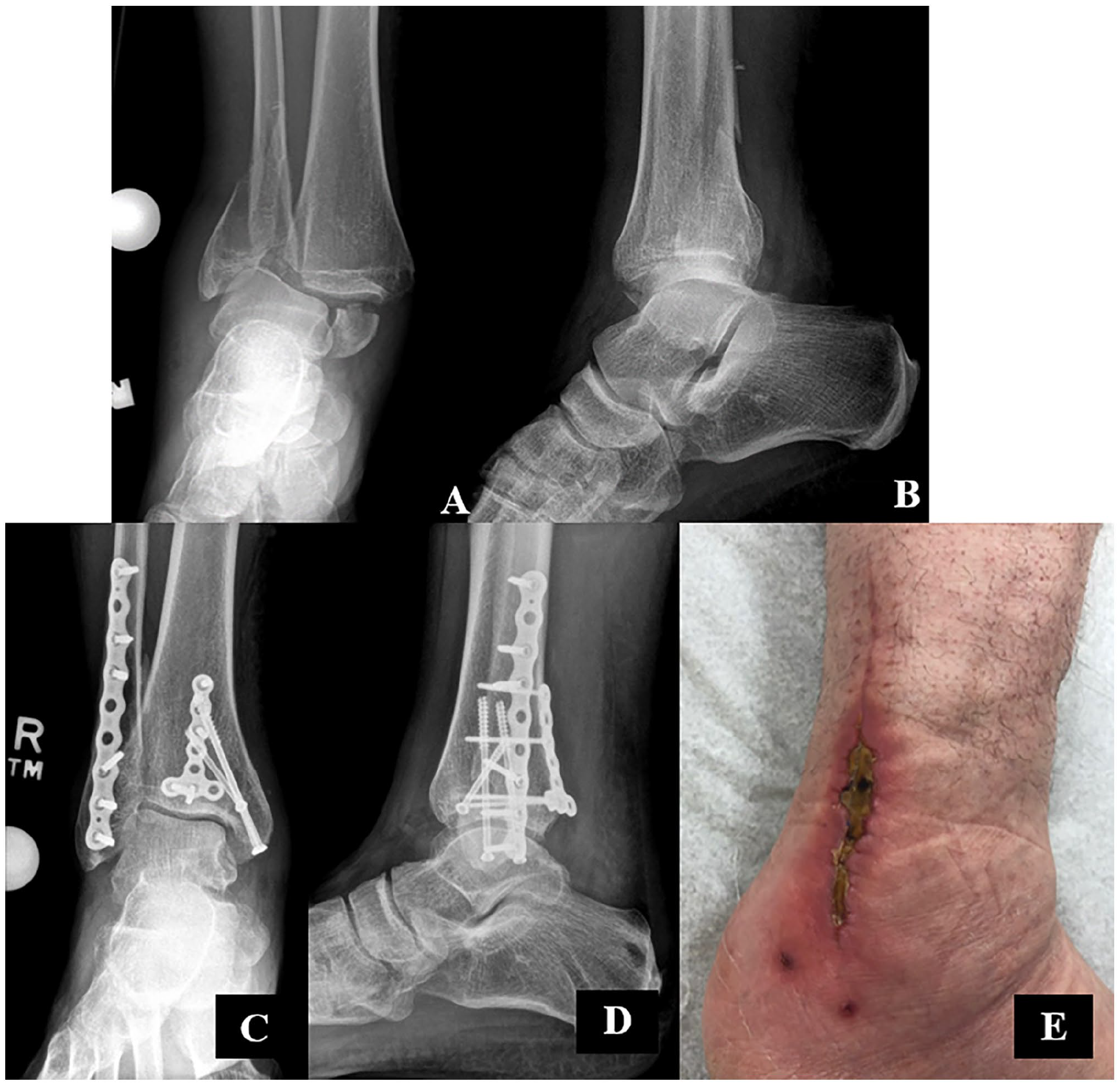
Trimalleolar ankle fracture-dislocation before treatment through the 2-window approach. (A) Anteroposterior view of fracture-dislocation before reduction. (B) Lateral view of fracture-dislocation before reduction. Outcomes of trimalleolar ankle fracture open reduction and internal fixation through 2 windows. (C) Anteroposterior view of healed ankle fracture-dislocation. (D) Lateral view of healed fracture-dislocation. (E) Wound dehiscence following 2-window approach.
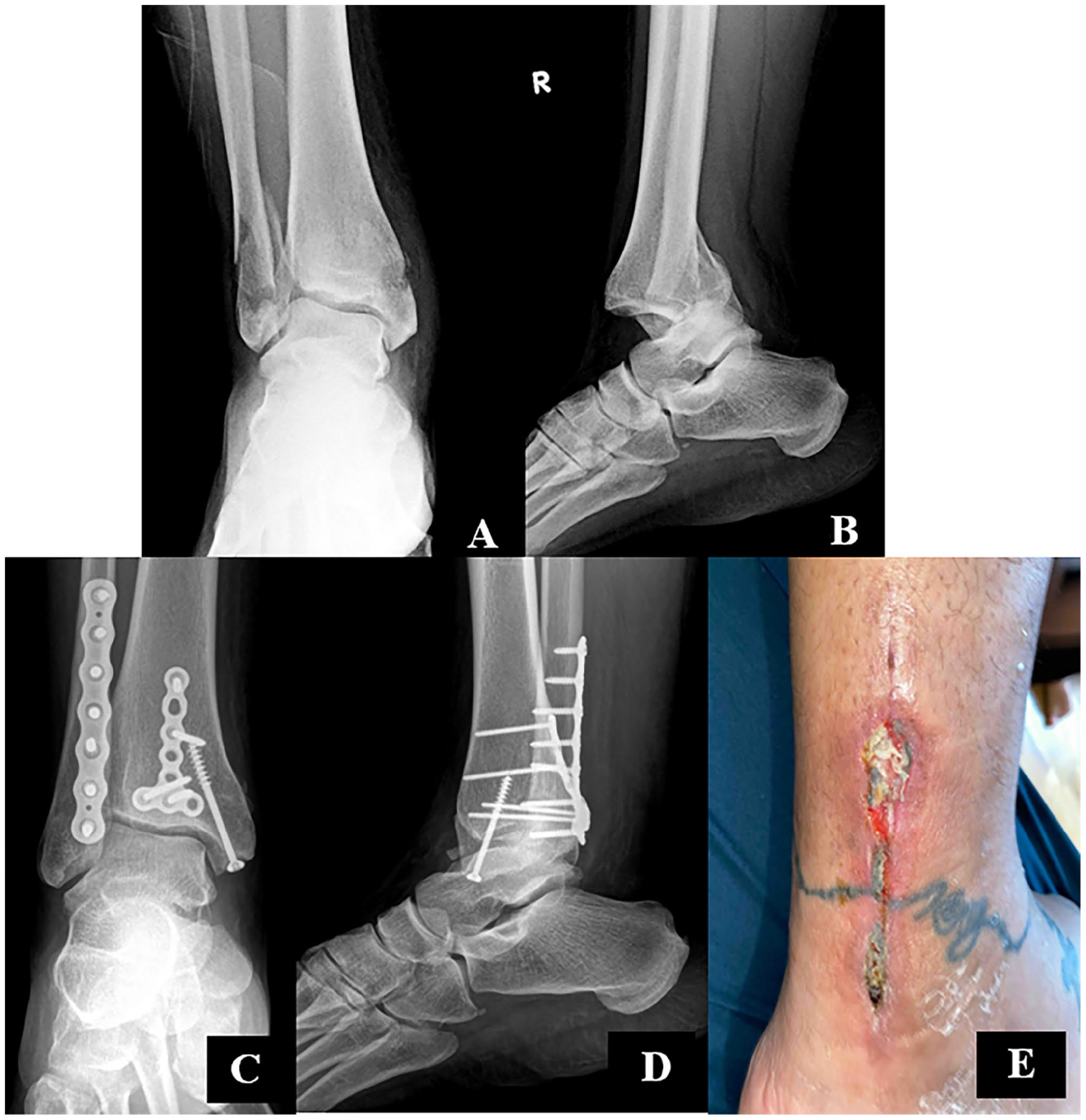
Trimalleolar ankle fracture-dislocation before treatment through the single-window approach. (A) Anteroposterior view of fracture-dislocation before reduction. (B) Lateral view of fracture-dislocation before reduction. Outcomes after open reduction and internal fixation via the single-window approach. (C) Anteroposterior view of healed fracture-dislocation. (D) Lateral view of healed fracture-dislocation. (E) Wound necrosis following single-window treatment.
Exclusion criteria included the use of the patients <18 years old, the lateral approach, incomplete radiographic imaging, pilon fractures, and lack of adequate clinical follow-up. Nine patients with less than 3-month minimum postoperative clinical follow-up were entirely excluded from this study, leaving 164 patients to be considered for an analysis of the incidence of early wound complications (Figure 5). Of these, 108 were treated with the posterolateral approach through a single window and 56 were treated through 2 windows.
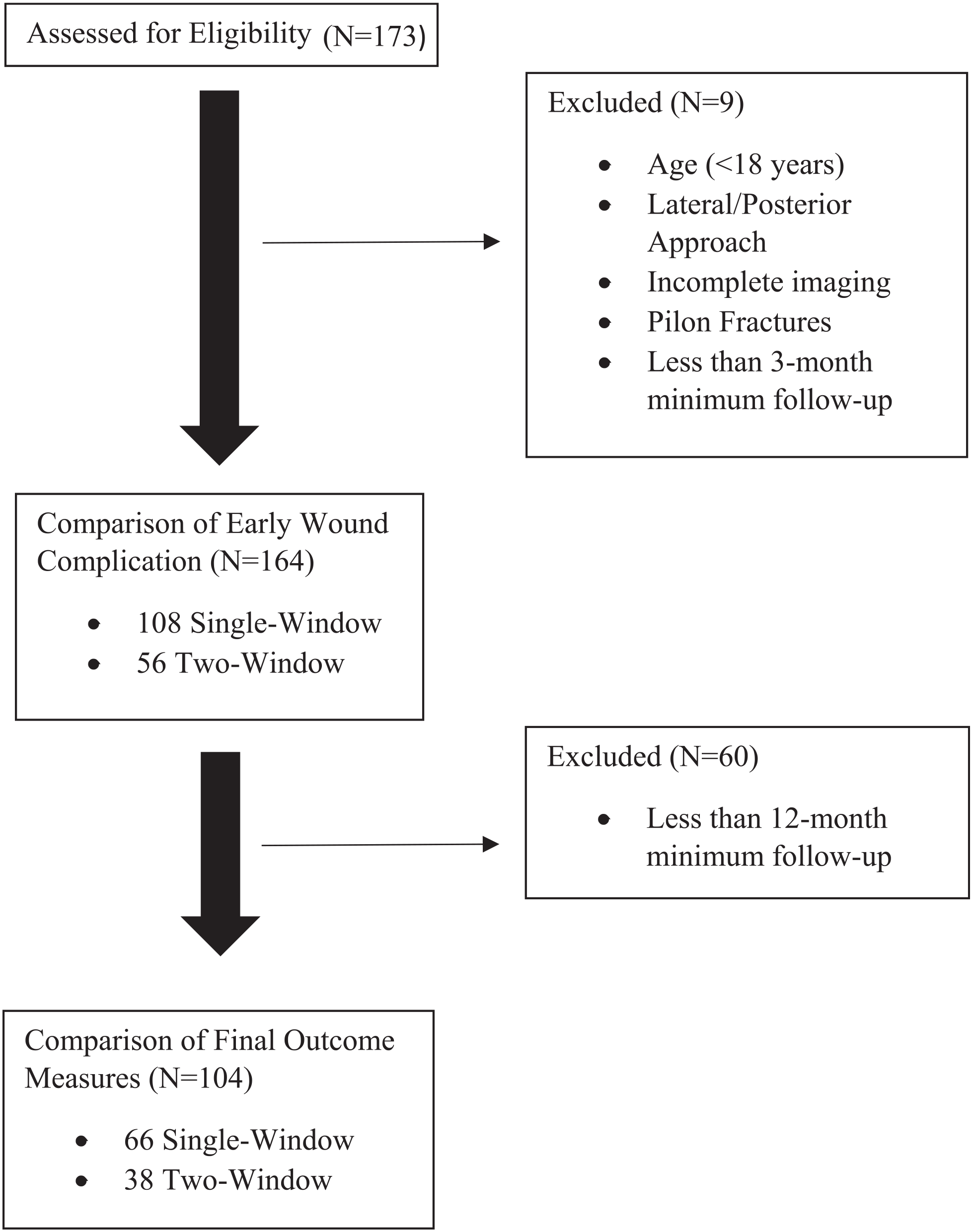
Flow chart diagram describing the primary comparison cohorts in this study.
Only patients with 12-month minimum follow-up were considered for final outcome measures. Of the 164 patients included in the analysis of early wound complications, 60 patients did not return for an in-person office visit at least 12 months after surgery, leaving 104 patients to be assessed for final outcomes. Of these patients, 66 were treated through the single-window approach and 38 were treated through 2 windows (Figure 5).
Demographics and Fracture Characteristics
Demographics of the single-window and 2-window cohorts are shown in Table 1. No differences in age, body mass index (BMI), Charlson Comorbidity Index, operative measures, sex, injury energy, syndesmotic fixations, fracture dislocations, or trimalleolar fractures were observed (Table 1). Injury energy was defined according to the ATLS guidelines where high-energy mechanisms include falls from at least 3 m, motor vehicle accidents, and high-velocity impacts. 2 Patients in both groups had their posterior malleolus fracture directly repaired regardless of its size.
Demographic, Injury, and Operative Information of all Patients Included in This Study. a
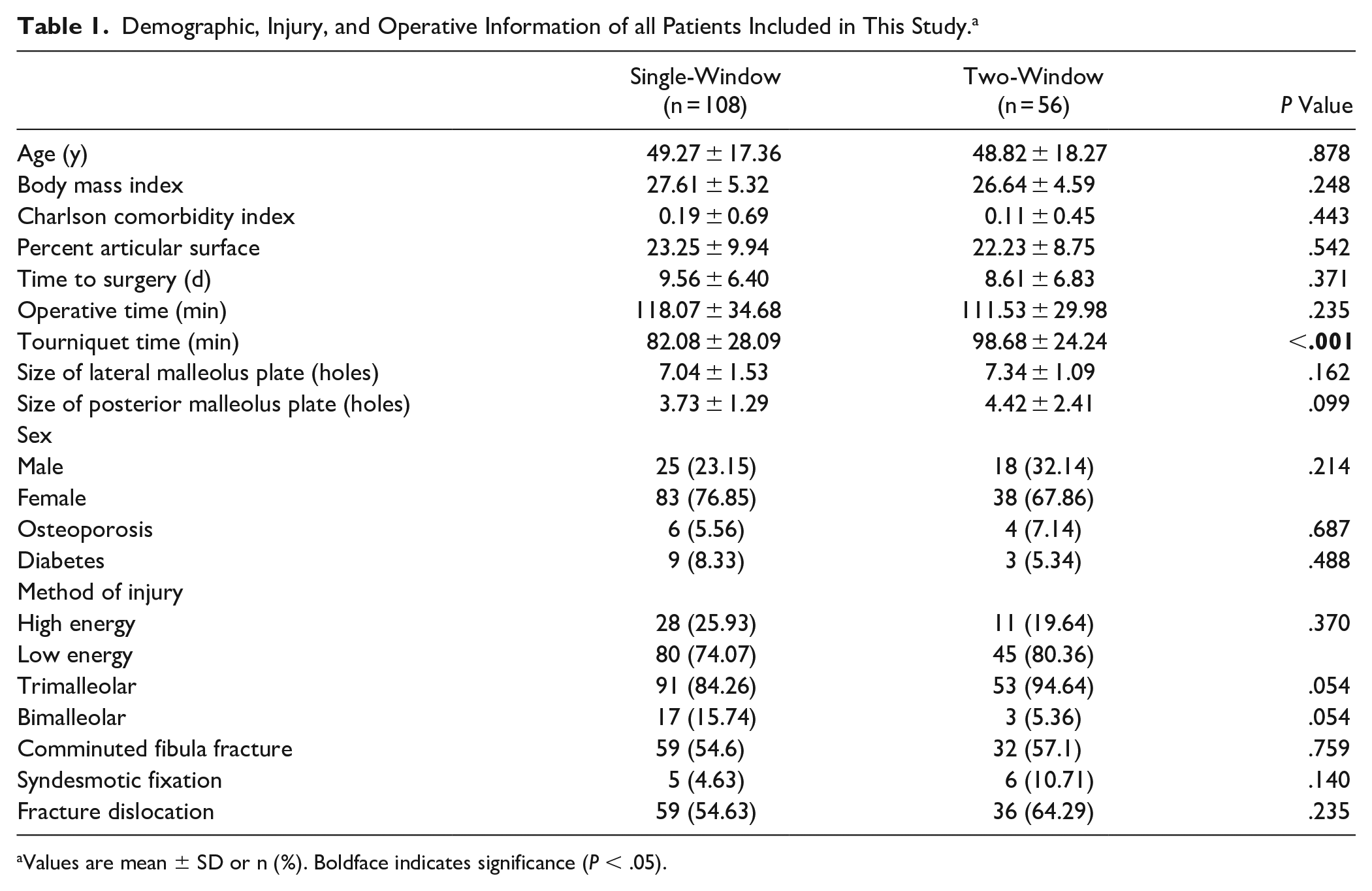
Values are mean ± SD or n (%). Boldface indicates significance (P < .05).
Surgical Techniques
Patients in both groups underwent surgery under regional block anesthesia. Patients were placed in the prone position and a tourniquet was used in all cases. In both approaches, the skin incision was made midway between the Achilles tendon and the fibula (Figures 1A and 2A). In the single-window group, a single interval between the FHL and peroneal tendons was developed (Figure 1B). In the 2-window approach, a second interval was developed, through the same incision, lateral to the peroneal tendons to access the lateral malleolus (Figure 2C). The fixation was similar in both groups, with the posterior malleolus fixed first with 2.7-mm T-plate and then the fibula using a one-third tubular plate (Stryker; Kalamazoo) (Figure 3C and D, Figure 4B and D). Surgical approach was selected based on surgeon preference.
Both groups had similar postoperative protocol, with splint removal at 2 weeks for suture removal along with placement in a CAM boot, and range of motion exercises allowed out of the boot. Patients were allowed to bear weight at 2 or 6 weeks at discretion of the surgeon. All patients were seen at 6, 12, 24, and 52 weeks for follow-up. Those with wound complications were seen more frequently as needed for wound checks (Figures 3E and 4E).
Clinical and Radiographic Assessment
All patient demographic and operative information including age, sex, Charlson Comorbidity Index, diabetes, BMI, length of hospital stay, fracture comminution, and fragment size were reviewed from electronic medical records. Plate size was assessed as the number of screw holes in the lateral malleolus plate and number of screw holes in the posterior malleolus plate. Outcomes in this study including active range of ankle motion, general and early wound complications, need for painful implant removal, sensory nerve complications, peroneal tendonitis, and fracture healing were evaluated at in-person office visits by the operating surgeon and reviewed from electronic medical records. Ankle range of motion was assessed using a goniometer at each follow-up visit.
Early wound complications were defined as dehiscence, drainage from incision, delayed wound healing, infection, and wound edge necrosis within 3 months after operation (Figures 3E and 4E). Operative site infections were defined as deep according to the Centers for Disease Control and Prevention guidelines. 11 Wounds taking longer than 6 weeks to close were classified as delayed. Sensory nerve complications were defined as peroneal or sural nerve numbness or paresthesia at final visit.
Statistical Analysis
Patient and operative information and outcome measures were analyzed using IBM Statistical Package for Social Sciences, version 25. Means of scale variables including age, percentage articular surface, BMI, ankle range of motion, and length of surgery were compared using independent samples t tests and Man-Whitney U tests where appropriate. Categorical variables including method of injury, sex, various complication types, and rate of implant removal were tested for significance using Pearson chi-squared tests. Logistic regression was performed using wound complication as the dependent variable.
Results
The 2 cohorts did not differ significantly in demographic characteristics (Table 1). There was no difference between single- and 2-window fractures in plate size, comminuted lateral malleolus fractures, need for syndesmotic fixation, or fracture-dislocation (Table 1). The posterior malleolus fragment size, measured as percentage of the articular surface, was similar in both groups with involvement of composed 23.3% ± 9.9% of the articular surface in the single-window group and 22.2% ± 8.7% in the 2-window group (Table 1). In regard to surgical characteristics, the single-window approach was not different from the 2-window approach in time to surgery and length of surgery, but had shorter tourniquet time (82.1 ± 28.1 vs 98.7 ± 24.2 minutes, P < .001) (Table 1).
A higher proportion of patients treated through the 2-window approach had early wound complications compared to the single-window approach (32.1% vs 12.0%, P < .01) (Table 2). Among the 108 patients treated through 1 window, 13 (12.0%) had wound issues. Seven (6%) had persistent drainage from the incision an average of 28 days after surgery, 3 (3%) had dehiscence, 2 (2%) had delayed healing, and 4 (4%) had wound-edge necrosis (Table 2). Among the 56 two-window patients, 18 patients (32.1%) had a wound issue. Eight (16%) had persistent drainage from the incision after an average of 30 days, 10 (18%) had wound dehiscence, 3 (5%) had delayed healing, and 1 (2%) had a deep infection requiring surgical irrigation, debridement, and implant removal (Table 2).
Incidence of Wound Complication Within 3 Months of Surgery When Ankle Fractures Were Treated Through the Single- and 2-Window Posterolateral Approaches.
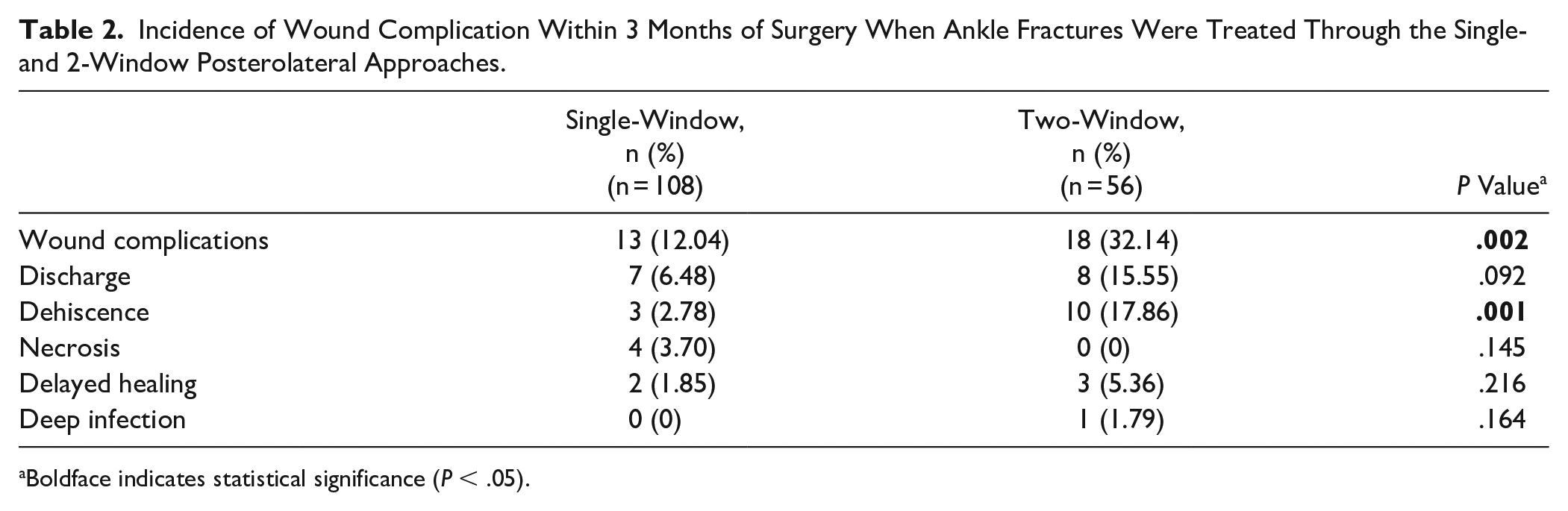
Boldface indicates statistical significance (P < .05).
No difference in early wound complication was observed between patients with fracture-dislocation relative to no dislocation (23.2% vs 13.0%, P = .102). Among patients with fracture-dislocation, single-window patients had a lower incidence of wound complications (15.3% vs 36.1%, P = .019). Medial malleolus fixation had no impact on lateral wound complication; however, both the length of surgery (123.5 ± 31.8 vs 89.1 ± 22.6 minutes, P < .001) and tourniquet time (92.9 ± 27.5 vs 70.6 ± 22.0 minutes, P < .001) were significantly longer in patients requiring medial malleolus fixation. Patients treated more than 7 days from their injury had higher incidence of wound complication (24.7% vs 12.7%, P = .049). Among these patients, those treated through 2-windows had more wound issues (44.4% vs 15.5%, P < .01). No difference was seen in wound complication among patients treated within 1 week of their injury (8.0% vs 20.7%, P = .102). When comparing patients who had wound complications with those who did not, there was no difference in operative time (118.2 ± 33.0 vs 115.3 ± 33.4 minutes, P = .667) or time to surgery (10.8 ± 9.03 vs 8.9 ± 5.8 days, P = .129). However, wound complication patients had longer tourniquet times (85.4 ± 26.4 vs 97.9 ± 32.2 minutes, P = .025). Logistic regression demonstrated that surgical windows and BMI independently predicted wound complications (OR = 4.149, 95% CI = 1.642-10.53, P = .003) and BMI (OR = 1.104, 95% CI = 1.010-1.207, P = .029) (Table 3).
Logistic Regression on Early Wound Complication. a
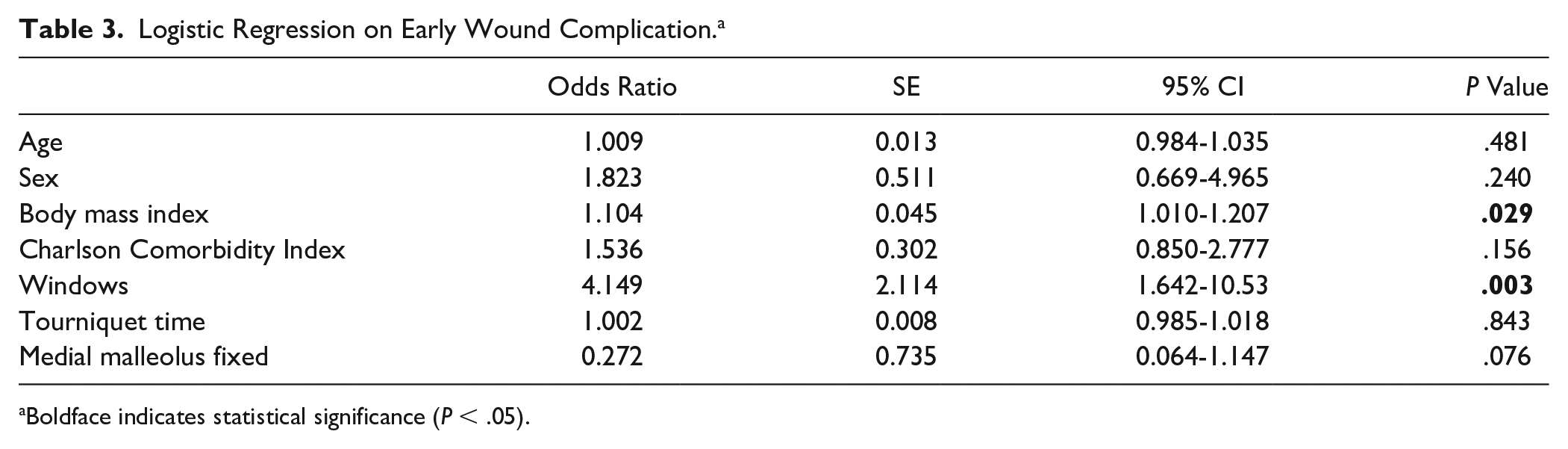
Boldface indicates statistical significance (P < .05).
When comparing the single-window and 2-window cohorts at their most recent visit among 104 patients with minimum follow-up of 12 months (mean 19.4 ± 10.6 months), single-window patients had significantly greater plantarflexion (35.0 ± 10.1 vs 29.7 ± 11.3 degrees, P = .025) and dorsiflexion (21.2 ± 9.7 vs 15.9 ± 10.9 degrees, P = .021) relative to the 2-window group (Table 4). There was no difference in time to final follow-up between the single- and 2-window groups among patients with 12-month minimum follow-up (Table 4). No difference was observed in implant removal rate or rate of nonunions (Table 4). No loss of reduction was observed in any case.
Final Outcomes and Complications When Treated Through the Single- or 2-Window Approaches Among Patients With Minimum 12-Month Follow-up.
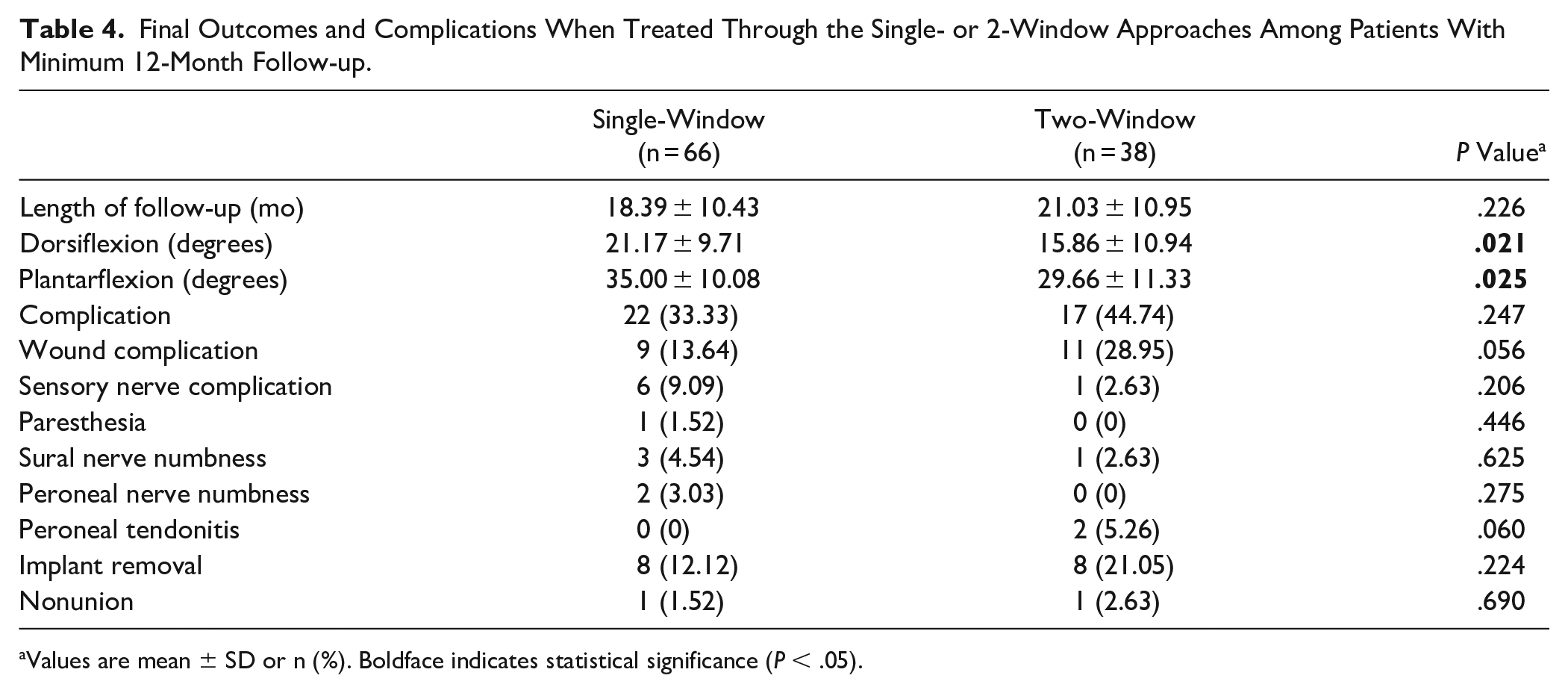
Values are mean ± SD or n (%). Boldface indicates statistical significance (P < .05).
Despite a higher incidence of wound complications in the 2-window cohort at the 3-month time point, no difference between the single- and 2-window approaches was observed in general complications or wound complications at any other time point among patients with 12-month follow-up (Table 4). Incidence of sensory nerve complications, including paresthesia and numbness, were not significantly different between the 2 groups though more were observed in the single-window group (9.1% vs 2.63%, P = .206) (Table 4).
Discussion
We found a higher rate of early wound complications in ankle fractures undergoing repair via a posterolateral approach within 3 months postoperatively using the 2-window approach compared to the single-window approach as well as a diminished range of ankle motion 1 year after surgery. However, no difference in wound complications was observed among patients with minimum 1-year follow-up. Among these patients, the ability to achieve anatomic reduction, healing, and ambulation were similar. Little et al 16 also studied complications through the posterolateral approach, but their study was limited to the single-window method. They found a similar rate of wound complication in their cohort of 12.5% to our 12.0% result. However, they observed a higher rate of deep infection of 2.7% compared to our finding of 0% among single-window patients. A recent study by Tavares et al also explored wound complications among posterior malleolus fractures surgically treated in the posterolateral approach through a single window. 7 Their wound complication rate of 44.2% is higher than our findings and that of Little et al.7,16 In surgically treated geriatric ankle fractures, Aigner et al 1 had wound complications in just 9.7% of cases, making our 12.0% finding relatively high despite being younger with an average age of 49.3 years.
To our knowledge, wound complications in the 2-window posterolateral approach has not been described before in the English literature. The proportion of patients with wound issues treated through 2 windows in this study was far greater than the rate reported for single-window treatment in this study as well as the rates reported by Little et al 16 and Aigner et al. 1 This suggests that any benefits of the 2-window approach may come at a cost of increased soft tissue injury, resulting in a higher rate of wound complications. The 2-window approach requires retraction of the peroneal tendons in both directions to visualize the posterior and lateral malleoli. This soft tissue mobilization/retraction may potentially be responsible for higher wound complications seen in the 2-window cohort. Still, the high rate found by Tavares implies that the single-window approach is also susceptible to similar issues. 7
Of note, fracture-dislocations of the ankle did not have a significantly higher soft tissue complication rate, and, unexpectedly, waiting more than 7 days for surgery was associated with a higher wound complication rate. The observed higher incidence of wound issues among patients with a fracture-dislocation treated later than 7 days compared to those treated within a week when swelling is higher is contrary to expectations. However, a case study and review by Schepers et al 18 also found higher incidence of wound complications outside 1 week when compared to less than a week for operative ankle fracture treatment. We agree with their conclusion that these ankle fractures may be treated earlier depending on the condition of the soft tissues. It may be that operating later requires more soft tissue dissection/stripping for fracture reduction, however, the reason for lower wound complications, when operating earlier, remains unclear. Still, although this statistical analysis does control for dislocation, it does not fully control for soft tissue injury severity, which may also be contributing to wound complications.
Other factors that may influence wound complications were found not to have any difference between the single- and 2-window cohorts. No appreciable difference was seen in operative time, time to surgery, or fracture-dislocation. Lee et al 15 also did not find any correlation between surgical time and wound complication. However, tourniquet time was significantly longer in the 2-window group and was also found to be longer in patients with wound complications compared to those without. Differences in tourniquet use for medial malleolus fixation and wound closure (release tourniquet before or after closure of wounds) between surgeons was responsible for this difference. A study by Wiewiorski 20 demonstrated that such prolonged use of a tourniquet increases risk for wound complications. This leads us to believe that, in addition to soft tissue injury, longer tourniquet time may also be a factor contributing to the significant wound complication result. Still, even when controlling for tourniquet time and demographic factors, a significant relationship for wound complication with windows was found without an association with tourniquet time. Interestingly, this analysis also demonstrated a relationship between BMI and wound complication, which aligns with the current literature as shown by Bell et al. 4 Although tourniquet time was likely a factor, our analysis demonstrates that the choice of window technique for posterolateral approach was the driving factor.
Among patients with 12-month in-person follow-up, no difference in complications was observed. The 60 patients with 3-month follow-up who did not return for 1-year follow-up had a high rate of wound complication in the 2-window cohort, resulting in a loss of significance for this metric in the 12-month minimum follow-up analysis. Patients unhappy with early wound complications may have chosen to complete their follow-up at another health system of which there are many options in our large urban setting. A statistically insignificant, but relevant, result is more frequent sensory nerve issues in the single-window approach. Six such complications (9.4%) were observed in the single-window group with just 1 (2.32%) seen in the 2-window group. It appears that the 2-window approach may be an effective strategy for sural nerve protection. Heyes et al 10 completed a systematic review of studies using the posterolateral approach looking at several factors including nerve complications. They discovered numbness in 4.5% of patients treated through the single-window approach, which is similar to the rate seen in our 2-window cohort demonstrating that sensory nerve issues may not necessarily be correlated with the approach.
The single-window patients had significantly greater plantarflexion and dorsiflexion relative to the 2-window group. The slightly higher proportion of trimalleolar ankle fractures in the 2-window group may have contributed to the greater loss range of motion outcome. This result also may have been influenced by the higher incidence of wound complication seen in the 2-window group. However, although statistically significant, we acknowledge that a 5-degree difference in range of motion may not have any functional significance.
This study had several limitations. As a retrospective study, it comes with inherent selection bias. Among the 173 patients reviewed, 164 had 3-month follow-up and 60 patients did not have minimum 1-year outcomes. Furthermore, all outcomes and complications were dependent on the quality of documentation by the operating surgeons in follow-up visit notes. Limiting final outcomes to patients with 12-month minimum follow-up also limited the size of the cohorts. Long-term outcomes such as rate of implant removal and reoperation may therefore not be fully representative. There were 3 surgeons involved in this study, and differences in experience, preparation, or techniques between surgeons may have confounded the findings of this study. Although we may have missed late soft tissue complications, we felt the 3-month window was appropriate for identifying early soft tissue complications, which was the purpose of this study. Similarly, no analysis was done comparing each of the 3 surgeons to each other, as we did not think this was appropriate for this manuscript and the numbers will preclude any meaningful statistical comparison.
In conclusion, the 2-window posterolateral approach in our study was associated with greater incidence of early wound complications compared with the single-window approach, regardless of dislocation status. The single-window approach was associated with better postoperative range of ankle motion at an average on 1.5 years postoperation. Our findings indicate that the single-window posterolateral approach for fixation of unstable rotational ankle fractures may reduce risk of early wound complications without sacrificing early clinical outcomes.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231156163 – Supplemental material for The 2-Window Posterolateral vs Single-Window Approach for Ankle Fracture Fixation
Supplemental material, sj-pdf-1-fai-10.1177_10711007231156163 for The 2-Window Posterolateral vs Single-Window Approach for Ankle Fracture Fixation by Christopher G. Herbosa, Philipp Leucht, Kenneth A. Egol and Nirmal C. Tejwani in Foot & Ankle International
Footnotes
Ethical Approval
This study (i17-00419) was approved by the NYU School of Medicine Office of Science and Research Institutional Review Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.