
Abstract
Background:
Forefoot plantar ulcers in patients with diabetic neuropathy are considered to be primarily the result of increased shear forces applied over prominent plantar bony prominences. The purpose of this article is to describe a 2-stage treatment pathway utilizing an outpatient percutaneous tendon-Achilles lengthening (TAL) as the first stage procedure and subsequent proximal metatarsal osteotomy (MTO) as a second stage procedure for a persistent or recurrent ulcer.
Methods:
A consecutive 112 patients (146 feet), who presented to our Multidisciplinary Diabetic Foot Team clinics since February 2019 with plantar nonischemic forefoot ulcers were included in this study. Excluding the patients who died or were lost to follow-up, 96 feet were followed for a minimum 12 months (range 12-36 months). After TAL, patients were encouraged to walk in a walking cast for 6 weeks and were followed for a minimum 12 months. Patients with persistent or recurrent ulcers were investigated with magnetic resonance imaging scan, and based on intramedullary osteomyelitis and septic destruction of distal metatarsal, we describe a second-stage MTO with the 3 most common clinical presentations.
Results:
Of 96 feet, none had infection or wound-related problems following TAL. Complete transection of the tendon was noted in 4 patients (4%) and heel callosity in 1 patient. In 92 feet (96%), the ulcers healed within 10 weeks (±4 weeks) after TAL but, in 12 feet (10%), the ulcer failed to heal or recurred. At a minimum 12 months after the second-stage MTO, none in this subgroup had recurrence of ulcer or a transfer lesion.
Conclusion:
TAL followed with a walking cast as an outpatient procedure was effective in healing forefoot ulcers in 96% of feet. Comparable to the widely practiced hand surgery Wide Awake Local Anesthesia No Tourniquet (WALANT) procedure, our approach involved active control of the degree of ankle dorsiflexion by the patient, and the procedure was proven to be safe and well tolerated. When the second-stage MTO was required to offload the forefoot, in our small cohort, patients had ulcer-free outcome for a minimum 12 months.
Level of Evidence:
Level IV, retrospective case series.
Introduction
Forefoot ulcers in patients with diabetic neuropathy are a result of factors that increase forefoot plantar pressure.8,9,22,35,39,48 Pedo-barographic studies show twice the normal peak plantar pressures.6,8,9,24 Two mechanical factors contribute to this, progressive claw toe deformity secondary to plantarflexed metatarsal heads and, secondly, progressive hindfoot equinus from changes within the gastrocnemius- soleus-tendo-Achilles complex, both a result of motor neuropathy.23,30 Callosity under the metatarsal heads is the first sign of this, which progresses to ulceration from increased shear stress when walking on an insensate foot.4,19,30
A nonremovable total-contact cast (TCC) is considered a gold standard to offload the foot and shown to be effective for treating foot ulcers.2,20 However, as the deforming forces were not corrected, 4 the risk of ulcer recurrence was reported to be around 80% at 2 years 38 and 70% at 5 years, 3 with significant proportion seen within a month of stopping the TCC.4,10,20,38,45 When TCC was combined with TAL, the forefoot plantar pressures reduced by 27% 4 and the risk of reulceration to around 38% at 2 years.20,32,38 This recurrence could be due to persistent high forefoot plantar pressures from progressive plantarflexed metatarsal heads as the claw toe deformity worsens.17,30,33
The aim of this article is to describe a 2-stage treatment pathway for managing forefoot ulcers using an outpatient TAL as the first-stage procedure and subsequent metatarsal osteotomy (MTO) as a second-stage procedure for a persistent or a recurrent ulcer and, report our findings after a minimum follow-up of 12 months.
Materials and Methods
Hospital governance approval was obtained for the retrospective analysis of notes and radiographs and informed consent from patients were taken for the use of photographs relevant to this study. Consecutive cohort of 112 patients (146 feet), who presented to our Multidisciplinary Diabetic Foot Team clinics with forefoot ulceration or recurrent callosity and managed with the described 2-stage approach were included in the study. Excluding patients who died for medical reasons (8 feet) and lost to follow-up (3 feet), 96 feet were available for analysis at minimum 12 months (range 12-36 months), age range was 36-71 (mean 57) years, 71 males: 53 females; and 35 right: 61 left feet.
Two-Stage Procedure
First stage: Percutaneous outpatient TAL (HOKE technique)
After a successful pilot and approval from the local governance team, TAL has routinely been carried out in the outpatient clinics since February 2019 by 3 consultants (2 orthopaedic surgeons and a medical endocrinologist).14,40 Before this, the TAL was routinely carried out in the operating theatre by the orthopaedic surgeons (Figure 1).

Schematic diagram of Hoke hemisection.
Inclusion criteria were patients with persistent forefoot plantar callosities or ulcers and fixed tightness of calf muscle complex (negative Silfverskiold test and ankle equinus of <10-15 degrees). Exclusion criteria were patients with fixed ankle equinus of >20 degrees, ischemic toe ulcers, significant venous disease, or lymphedema; as plaster cast treatment was difficult in this group of patients. Patients with positive Silfverskiold test were treated with either stretches or serial castings and TAL planned if the callosity persisted or signs of worsening noted. 4 Patients with contralateral above- or below-knee amputation were cautioned about the risk of resultant weakness after TAL. 38 Patients with fixed tightness of >15 degrees had TAL in operating theatre with a combination of gastrocnemius-soleus lengthening ± TAL with controlled dorsiflexion of ankle just short of neutral position (<10 degrees).
Preprocedure assessment of patients by the Multidisciplinary Diabetic Foot Team is paramount for optimization of glycemic levels, cardiovascular and renal functions, lower limb perfusion, and more importantly, adjustments in the home microenvironment to allow weightbearing with crutches or other walking aids as assessed by the physiotherapy team. 29 Patients were provided with a printed advice sheet and formal written consent was obtained before scheduling the procedure.
Procedure
The procedure can either be performed with patient in supine position with the involved leg held in a gentle figure of 4-position or in a prone position. After antiseptic skin preparation, 1% lidocaine was injected over the area of intended skin incisions. With an assistant holding the ankle in gentle dorsiflexion, 2-hemisections of distal tendo-Achilles14,40 were made, first directed medially around 1 cm from its insertion, and the second directed laterally around 1.5 to 2 cm proximal to the first incision (Figure 2). No attempt was made to dorsiflex the ankle to avoid potential overlengthening or complete transection of the tendon. The authors are of the opinion that 2 hemisections for TAL are adequate for controlled lengthening of the tendon but, a third cut directed medially, 2 cm proximal to the second cut, is optional when patients have fixed ankle equinus of >20 degrees and access to theatre was limited, as was common during the pandemic. The skin incisions were covered with Steri-Strips and a simple dressing applied.

Photograph taken during the tendo-Achilles lengthening. With the assistant holding the foot in gentle dorsiflexion, 2-hemisections involving 50% of the tendon, the distal cut directed medially, and proximal cut laterally is made using a size 11 scalpel blade.
After TAL, patients were encouraged to actively dorsiflex the ankle, and a below-knee walking cast was applied in maximum dorsiflexion for a total duration of 6 weeks, with one change of cast at week 2; this allowed further ankle active dorsiflexion. Patients were encouraged to weightbear with or without crutches (Figure 3) and oral thromboprophylaxis was prescribed for the duration of plaster cast based on HAS-BLED risk assessment tool. 41

Weightbearing plaster cast ± crutches.
A weightbearing cast in neutral ankle position allows controlled lengthening of the tendon to the required length without the risk of overlengthening. Patients are counseled for plantar flexion weakness for up to 7 months postprocedure26,38 and hence referred to physiotherapy after 6 weeks of cast treatment. The postprocedure protocol after TAL is illustrated in Table 1.
Weightbearing Protocol After TAL.
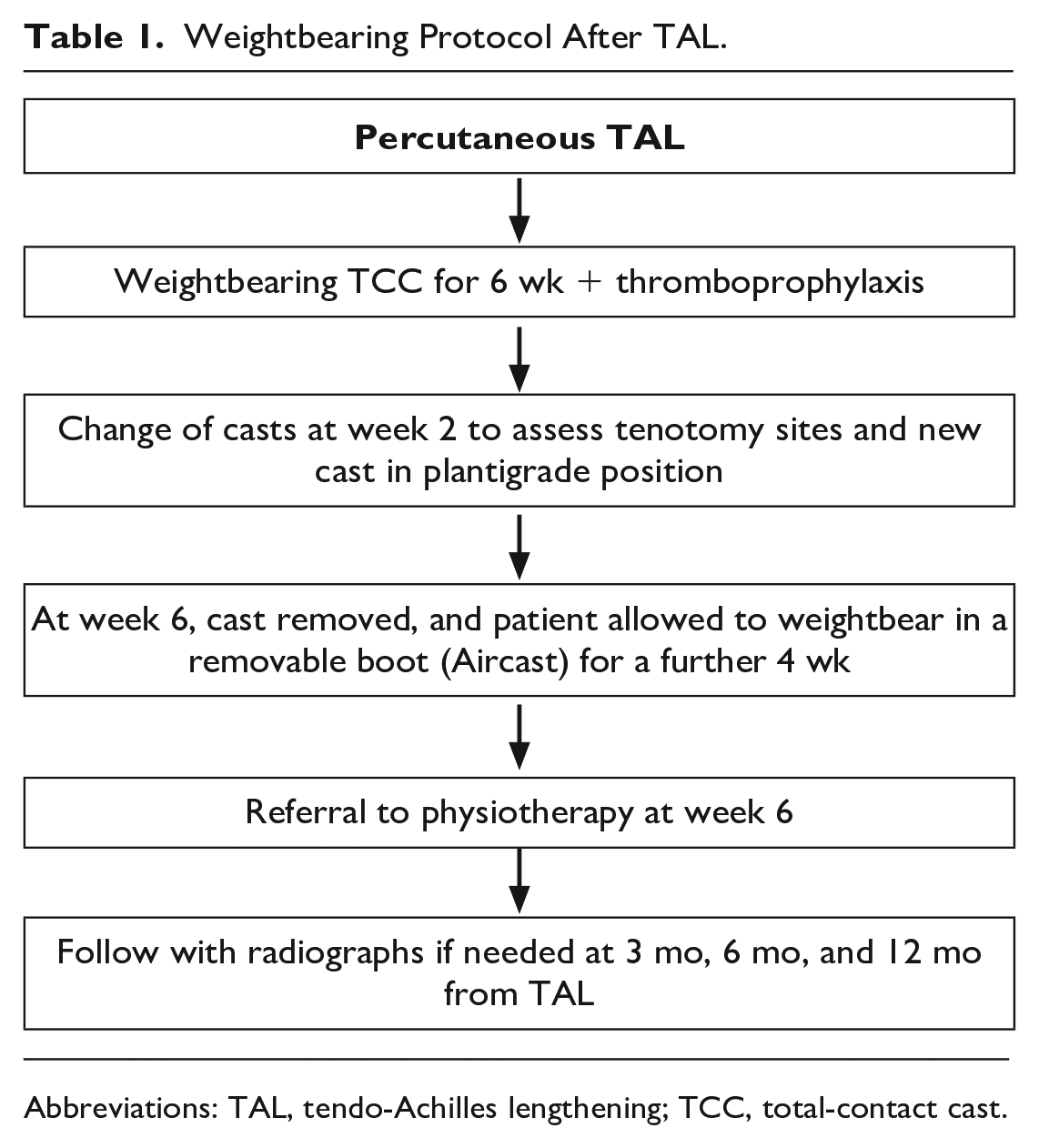
Abbreviations: TAL, tendo-Achilles lengthening; TCC, total-contact cast.
Patients are followed with radiographs (if indicated) at 3 months, 6 months, and at 12 months postprocedure.
Recurrent Ulceration
Patients with recurrent callosity or ulceration, or where the ulcers failed to heal, were investigated with magnetic resonance imaging (MRI) scan to assess the anatomy of the metatarsal heads, intramedullary osteomyelitis, and potential bone loss due to infection. Surgical treatment in these patients (second of the 2-stage procedure) was planned based on extent of osteomyelitis and septic destruction of metatarsals (Figure 4).
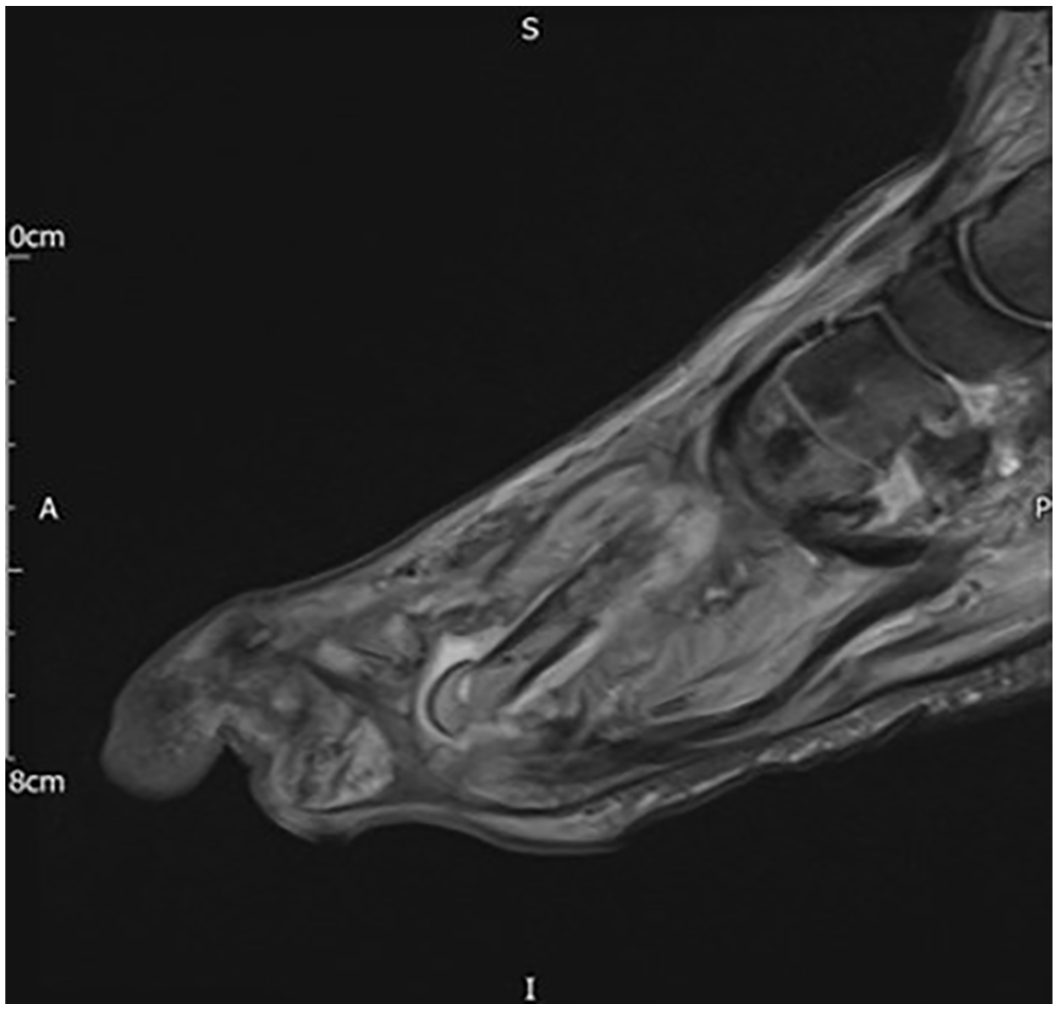
Sagittal magnetic resonance imaging scan of septic fracture of neck of metatarsal with intramedullary osteomyelitis and subluxed metatarsophalangeal joint with claw toe deformity.
Stage 2: Proximal Metatarsal Osteotomy
This procedure was carried out in theatre under anesthesia with the use of limb tourniquet. We describe this procedure in 3 commonly seen scenarios.
Scenario 1: Patients with no evidence of osteomyelitis and intact metatarsal head
Patients in this group present with a recurrent forefoot callosity and may have changes of progression to a hemorrhagic blister but with no break to the skin surface. Preoperative MRI scan is advised in patients with previous ulceration to assess residual intramedullary osteomyelitis.
With a short longitudinal incision, the proximal metatarsal shaft distal to the tarsometatarsal joint was exposed. A dorsiflexion ± shortening closing wedge osteotomy was carried out with an aim to reduce the MTPJ (Figure 5). The authors prefer to stabilize the osteotomy with a staple; this is to avoid transfer lesion to the subsequent metatarsals because of uncontrolled dorsiflexion. Patients were encouraged to weightbear in a flat postoperative shoe following surgery.
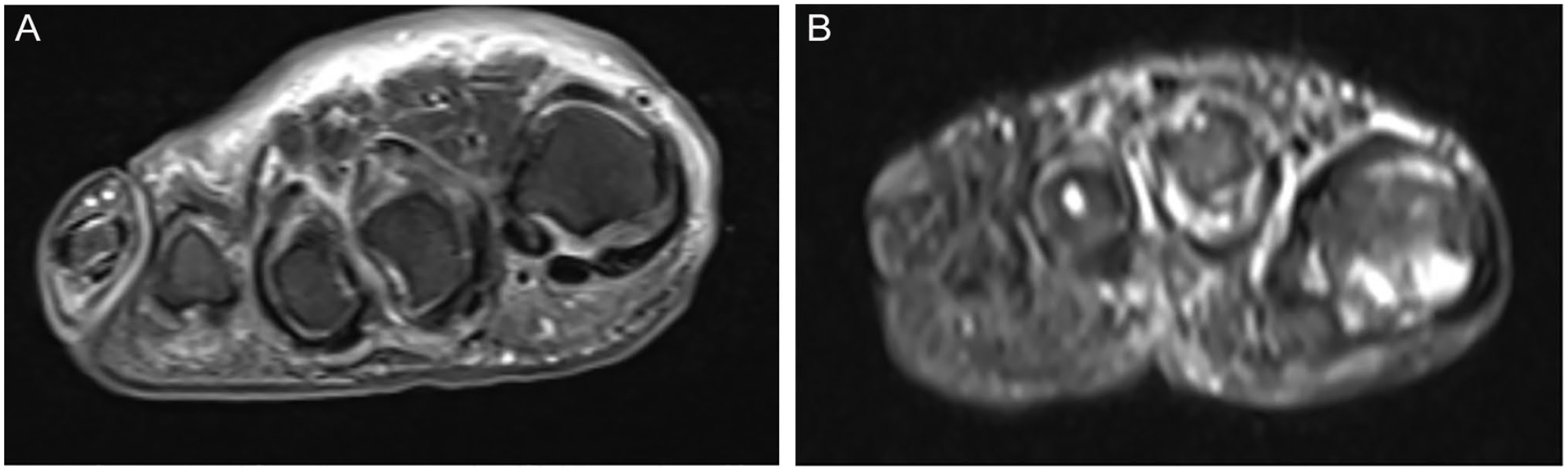
(A) Preoperative and (B) postoperative axial magnetic resonance imaging scan of forefoot with elevated second and third metatarsal heads after proximal metatarsal osteotomies.
The claw deformity was corrected with proximal interphalangeal joint fusion stabilized with a percutaneous smooth wire (Figure 6).

Anteroposterior radiograph of the foot with proximal metatarsal osteotomies stabilized with staples and proximal interphalangeal joint fused with a 1.6 mm K-wire.
Scenario 2: Patients with osteomyelitis but intact metatarsal head
Patients in this group present with a plantar forefoot ulcer, intramedullary osteomyelitis, and intact metatarsal head and distal metatarsal on preoperative MRI scan.
The ulcer edges and the base were debrided, and communication to the MTPJ capsule, if present, was excised and the deep samples sent for microbiological assessment. This will guide postoperative systemic antibiotics.
The MTO was carried out as described in scenario 1. The intramedullary canal was curetted under fluoroscope, samples sent for microbiology, and the canal filled with local antibiotic eluting agents such as Cerament G. The osteotomy was stabilized with a smooth 1.6-mm K-wire (Figure 7) extending from the tip of the toe to the tarsometatarsal joint.

Intraoperative radiograph of foot after excision of infected metatarsal head, curettage of intramedullary canal, and injection of Cerament G. The metatarsal osteotomy and proximal interphalangeal joint fusion were stabilized with a single 1.6-mm K-wire.
Once the pressure of the metatarsal head was elevated, the ulcer edges often can be approximated primarily without tension; however, if the gap was significant, secondary wound closure methods such as split-skin or synthetic skin grafts can be considered—this was rare when only 1 ray was involved.
The claw toe deformity as above was corrected with a proximal interphalangeal joint fusion. The smooth wire used for metatarsal osteotomy can be extended distally to stabilize the proximal interphalangeal joint (Figure 7).
Scenario 3: Patients with osteomyelitis and septic destruction of distal metatarsal
Patients in this group present with chronic forefoot plantar ulcer, septic destruction of metatarsal head, and distal metatarsal with intramedullary osteomyelitis (Figure 4).
The ulcer edges were excised as above with obvious loose bony fragments. With an additional dorsal incision extending the length of metatarsal, the involved segment of metatarsal head, neck, and distal shaft were excised. The intramedullary canal was curetted and filled with Cerament G after deep samples for microbiology (Figure 7). Plantarflexed metatarsal was corrected with a short dorsal closing wedge osteotomy, and to maintain the soft tissue balance, the distal P1 and the metatarsal was stabilized with a smooth wire and the gap filled with Cerament G. The ulcer edges are managed as described in scenario 2.
In patients with intramedullary osteomyelitis where local Cerament G was injected (scenario 2 and 3), additional 2 weeks of oral broad-spectrum antibiotics were prescribed. This was to treat other possible foci of infection and were modified based on culture results, guided by weekly blood inflammatory markers and wound healing. The percutaneous wire, when used, was removed at week 6.
Additional lengthening of peroneal longus tendon for plantar first metatarsal ulcers and tibialis posterior tendon for plantar fifth metatarsal ulcer is recommended. 32
Results
In 92 feet (96%), the forefoot callosities and the ulcers healed after TAL within an average of 10 weeks (range 6-12 weeks). Complete transection of the tendon was noted in 4 patients and 1 patient developed callosity under the heel. This was due to attempted dorsiflexion following the TAL, which was reported as a standard practice in many centers.6,26,32,38 Owing to these early experiences, this part of the procedure was stopped and, consequently, none in the later cohort were noted to have these complications. Two of these patients with complete transection were managed nonoperatively, and 2 needed secondary repair. The patient with heel callosity was managed in a custom orthosis.
None of the patients developed wound-related problems at the tenotomy site or thromboembolism. On average, most patients had improved dorsiflexion of 10 degrees (0-15 degrees) following TAL.
Recurrence
The ulcer recurred or failed to heal in 10% (12 feet). Clinical assessment in these patients showed significant claw toe deformity with prominent plantar metatarsal head. The MRI scan showed a plantar plate tear resulting in MTPJ subluxation/dislocation and plantarflexed metatarsal head (Figure 8).
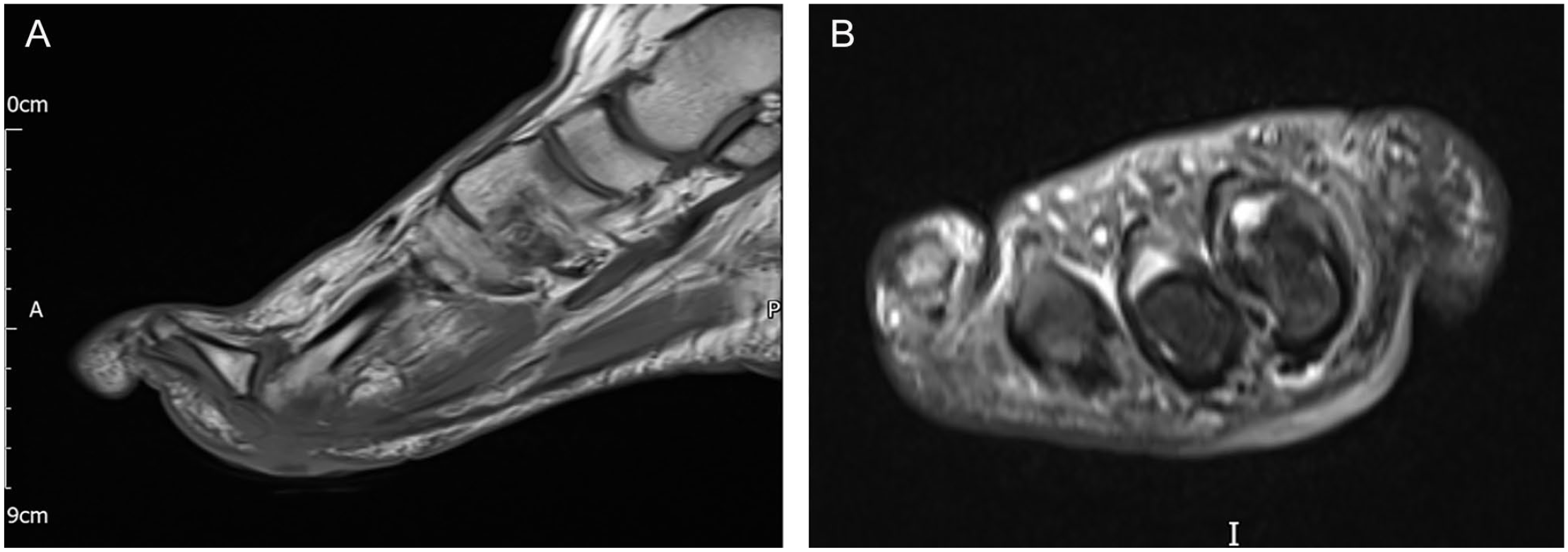
(A) Sagittal and (B) axial magnetic resonance imaging scans of forefoot, showing plantarflexed metatarsal with subluxed metatarsophalangeal joint and claw toe deformity.
These patients underwent the second-stage MTO based on the above-described scenarios and were followed clinically and radiologically for recurrence. In this subgroup, the ulcers healed primarily in 10 feet with no further recurrence, and secondary skin closure methods such as synthetic skin graft was used in 1 foot, and in 1 foot delayed wound dehiscence was noted that healed with regular dressings.
Discussion
Forefoot ulcers are a precursor to osteomyelitis, and when left untreated are a major cause for amputation and poor quality of life.4,16 The 5-year mortality after a below-knee amputation is reported to be >80%4,47; hence, timely identification and treatment of modifiable risk factors can save limbs, improve quality of life, and preserve independence.4,12,16
TCC is considered a gold standard2,34,49 to offload the foot but as the dynamic and static deforming forces remain untreated, the risk of ulcer recurrence is >60% at 5 years, with most recurrences seen within the first month of stopping the cast treatment.4,6,33,39,42 This led to infer that the TCC alone cannot be considered a gold standard for diabetic foot ulcer without adjuvant surgical offloading procedures. 32
A minimum 10 degrees of ankle dorsiflexion is essential for normal gait, and factors that reduce this range increases the forefoot plantar pressures. 24 The common reasons are from motor neuropathy-induced progressive hindfoot equinus from contracture of the gastrocnemius-soleus muscle complex and increased glycosylation of the type 1 collagen fibers of the tendo-Achilles.11,23 This can be flexible to start with (Silfverskiold test positive 44 ), and becomes fixed and static as the disease progresses (Silfverskiold test negative). The callosities under the plantar forefoot are a sign of this transformation. Frykberg et al 21 reported higher prevalence of ankle equinus in patients with diabetes; however, in practice, most patients with forefoot callosity or ulcerations have fixed tightness—recognition of this is clinical, and often missed.
TAL has shown to reduce the plantar forefoot pressures by 27% and ulcer healing in >96% of patients.6,36-38 However, the plantar pressures return to preprocedure levels within 7 months of TAL 38 and the risk of ulcer recurrence can be as high as 38% at 2 years.4,6,24,38 This may be due to recurrence of progressive hindfoot equinus but most commonly from progressive claw toe deformity and gradual subluxation of the MTPJ. This is secondary to wasting of the intrinsic muscles of the foot and consequent hypertrophy of the plantar fascia.5,30 The forefoot plantar pressures increase exponentially with the tear in the plantar plate plunging the metatarsal head plantarly.13,24 Additional tightness of peroneal longus and tibialis posterior muscle/ tendon complex result in ulcers under the first metatarsal head and fifth metatarsal head respectively. 32 This is evident clinically as a callosity that progresses if these dynamic and static factors were uncorrected such as the treatment in the TCC. 32
Heel Ulcers After TAL
Overlengthening of the tendon, heel ulcers, and loss of plantar flexion strength are the major risks associated with TAL. 6 Complete transection of the tendon is another known but avoidable complication after TAL. These are due to forceful dorsiflexion of the ankle >15 degrees after TAL. 27 The degree of dorsiflexion after TAL is not easily controlled and can result in 34% increase in heel plantar pressures, cause of heel ulcers.25,38 Selective gastrocnemius recession without lengthening of the soleus avoids this overlengthening; however, this is indicated in mild to moderate ankle equinus (Silfverskiold test positive). 25 Patients with forefoot callosity or ulceration are commonly negative for the Silfverskiold test; hence, distal TAL is effective.25,36,38 A controlled lengthening of <10 degrees of ankle dorsiflexion is recommended, 38 but this is difficult to estimate in practice. In our practice, no attempt was made to push the ankle in dorsiflexion, and similar to a WALANT procedure, we encourage patients to actively dorsiflex the ankle, and a walking cast is applied in the position achieved, and changed at week 2, where patients can further dorsiflex with an aim to achieve a neutral plantigrade position. We feel this avoids the risks of overlengthening of the tendon, and change to this practice resulted in no further transection of tendon or heel callosity/ulcers at the latest follow-up of >12 months. A walking cast soon after the procedure helps to auto-lengthen the tendon to the required length.
MTO for Recurrence
The described surgical options for chronic or recurrent forefoot ulcers are either transmetatarsal amputation,15,27,28 excision of involved metatarsal head, 5 a 2-stage debridement and delayed wound closure, 31 distal metatarsal metaphyseal osteotomy, 1 and the described proximal metatarsal osteotomy. 18 Excision of the involved metatarsal head is effective and best reserved for infective destruction. This helps the ulcer to heal in 93% of patients within 3 months5,43; however, it has a risk of transfer lesion with ulceration at the next metatarsal heads (Figure 9A). 17 The distal metatarsal metaphyseal osteotomy is ideal in scenario 1 but will have limited access to curette the intramedullary canal for osteomyelitis.1,7,46 The described MTO is reported to heal ulcers in 95% of patients within an average of 40 days,18,32 and our experience mirrors this with no recurrence or transfer lesions at the 12-month follow-up (Figure 9B and C). However, our numbers were small to have a definitive conclusion, and a larger follow-up of these patients are planned.
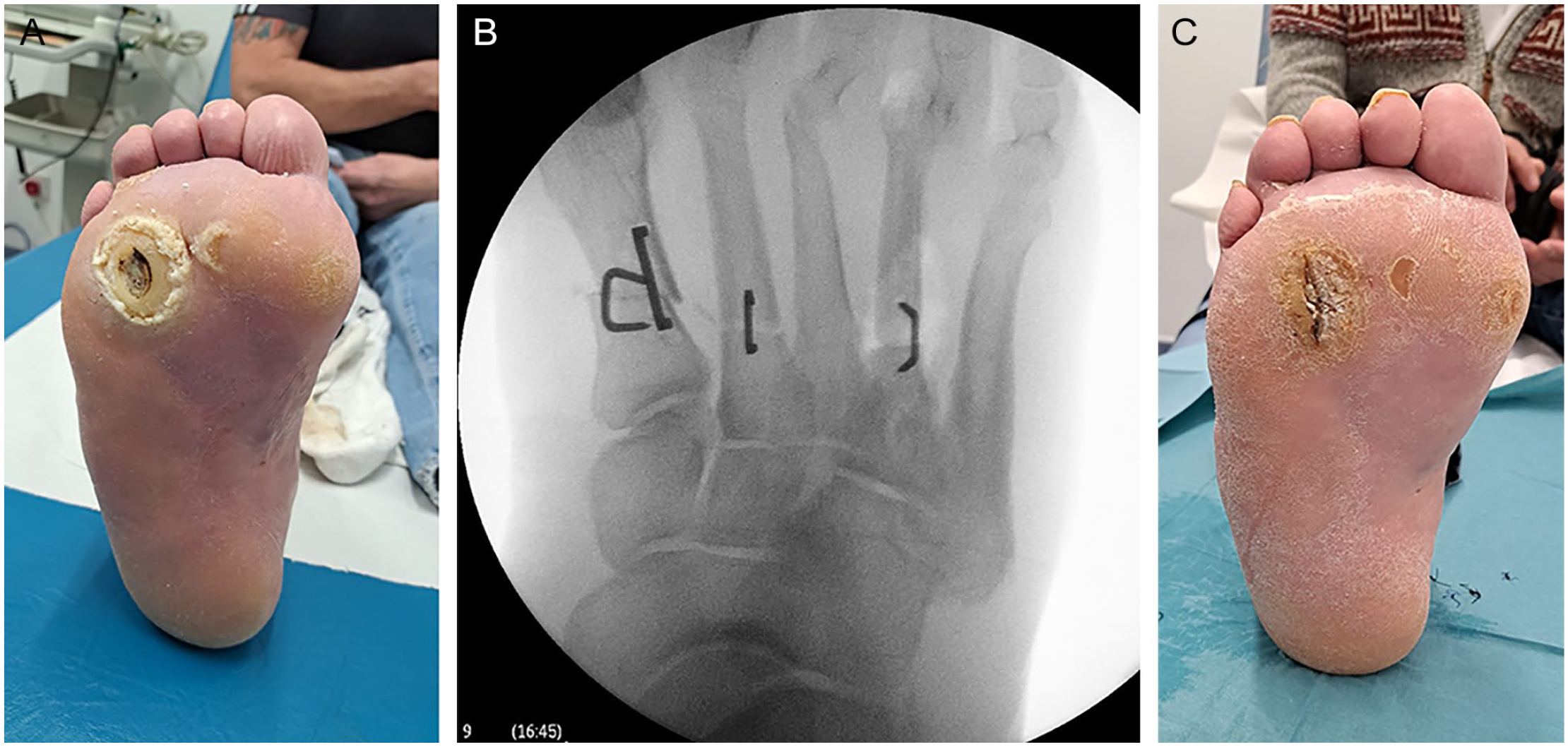
(A) Clinical photographs of foot with transfer lesion under the fourth metatarsal head following previous third metatarsal head excision. (B) Intraoperative radiograph of dorsiflexion osteotomy in the patient (scenario 2). (C) Clinical photograph 3 weeks after metatarsal osteotomy of the patient with adequate healing of ulcer.
Limitations of the Study
This is a retrospective noncomparative study with medium-term follow-up. Armstrong et al 4 considered the diabetic healed ulcers to be in remission; hence, a long-term follow-up for up to 5 years is recommended to reliably judge the effectiveness of these 2-stage procedures. Although the number of patients who underwent TAL and followed for 12 months were adequate, this study lacked a direct comparative group. To avoid this, we compared the results after TAL with the outcomes of historic patients who presented to our Multidisciplinary Diabetic Foot Team clinics with forefoot ulcers. As the groups were heterogenous, direct comparison of the results was not possible, but ulcer recurrence was noted to be significantly lower after TAL, as was noted by Holstein et al 27 and Lin et al. 36 As the MTO was reserved for patients with recurrent or persistent ulcers, only 10% (12 feet) of the cohort needed this and hence a very small number of patients in each of the 3 scenarios described.
Conclusion
The described 2-stage pathway with percutaneous TAL in the outpatient clinic as the first stage, which by itself helped the forefoot ulcers to heal in 96% of patients, and a second-stage MTO based on the 3 scenarios described helped the ulcers heal in 100% of our patients with no reported recurrence at the 12-month follow-up. Similar to a WALANT procedure, TAL in the outpatient clinic is safe, effective, and well tolerated by the patients. It also reduces the need for the procedure in an operating room, thereby reducing the cost to the health care system.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231191132 – Supplemental material for A 2-Stage Approach in Managing Diabetic Forefoot Ulcers
Supplemental material, sj-pdf-1-fai-10.1177_10711007231191132 for A 2-Stage Approach in Managing Diabetic Forefoot Ulcers by Madhu Tiruveedhula, Anna Graham, Ankur Thapar, Shiva Dindyal and Michael Mulcahy in Foot & Ankle International
Footnotes
Ethical Approval
Hospital governance approval was obtained for the retrospective analysis of notes and radiographs and informed consent from patients was taken for the use of photographs relevant for this study. Formal ethical approval was not sought for the present study as this included a retrospective review of notes and radiographs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.