
Abstract
Background:
First metatarsophalangeal (MTP) arthrodesis is a common surgical intervention for addressing MTP pain and deformity. Despite great interest on the topic of return to sport (RTS) after first MTP arthrodesis in the literature, no systematic review exists on this topic. The purpose of this systematic review is to investigate RTS after first MTP arthrodesis.
Methods:
This study is a systematic review using PubMed, Web of Science, CINAHL, and MEDLINE from database inception until May 10, 2023. Search algorithm used was (MTPJ OR MTP OR “hallux rigidus” OR cheilectomy OR metatarsal OR metatarsophalangeal) AND (arthrodesis OR fusion) AND sport. Inclusion criteria were surgical intervention of first MTP arthrodesis and outcomes related to sport.
Results:
Ten articles were included out of 249 articles initially retrieved. Patients (n = 450) had a frequency weighted mean (FWM) age of 58.6 ± 5.1 years with a FWM follow-up time of 32.1 ± 18.9 months. A total of 153 patients (reported in 34.0% of patients) had a FWM postoperative Foot and Ankle Ability Measure Sport score of 70.4 ± 21.8 at final follow-up. For sporting activities reported by multiple studies (running, yoga, golf, hiking, tennis, elliptical, and biking), about 9.8% to 28.1% of patients (n = 69 reports) stated that sporting activity difficulty decreased, 67.2% to 87.5% of patients (n = 340 reports) stated that sporting activity remained the same, and 1.8% to 8.5% of patients (n = 23 reports) stated that sporting activity difficulty increased after first MTP arthrodesis depending on the sporting activity. One article reported RTS time of 11.7 ± 5.1 weeks after first MTP arthrodesis (n = 39).
Conclusion:
RTS after first MTP arthrodesis is highly variable depending on patient and sport. Numerous different sporting activities have high rates of RTS after first MTP arthrodesis, with a majority of patients reporting similar or increased ability to perform sporting activities after surgery.
Keywords
Introduction
First metatarsophalangeal (MTP) arthrodesis is a common surgical intervention for addressing MTP joint pain from arthritis, deformity such as hallux varus or hallux valgus, and in the treatment of other degenerative processes relating to some neuromuscular or inflammatory conditions.6,7,9 Arthrodesis is often considered in late-stage hallux rigidus or following failure of joint-preserving/motion-preserving management strategies.1,4,6
First MTP arthrodesis has been shown to provide good to excellent results in the literature, with union rates typically reported between 90% and 100% with marked improvements in functional outcome measures.8,11-13,16-24,26-31 Nevertheless, hesitation commonly exists among both younger and older patients when considering MTP arthrodesis given a concern for possible hindrance of future athletic capabilities postoperatively. As a result, these patients often pursue ineffective conservative measures or a motion-preserving interventions, such as arthroplasty in an effort to avoid arthrodesis. 6 Several motion-preserving options for pathology of the first MTP have been shown to be associated with high complication rates. 25 Although return to sport (RTS) following first MTP arthrodesis has been investigated, the literature is relatively scant regarding consensus on postoperative athletic expectations. Importantly, as preoperative expectations among orthopaedic surgery has been found to portend postoperative outcomes, it is imperative to inform patients regarding their postoperative course as accurately as possible prior to surgery.3,23,24,28
To date, no systematic review has been performed on the RTS after MTP arthrodesis. The purpose of this systematic review is to explore both qualitative and quantitative measures for RTS after first MTP arthrodesis to improve patient education and expectation management.
Methodology
Study Setup
This study is a systematic review on the topic of return to sport (RTS) after MTP arthrodesis using PubMed, Web of Science, CINAHL, and MEDLINE from database inception until May 10, 2023. Search algorithm used in all databases was (MTPJ OR MTP OR “hallux rigidus” OR cheilectomy OR metatarsal OR metatarsophalangeal) AND (arthrodesis OR fusion) AND sport. This systematic review is in accordance with the most recent Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Inclusion and Exclusion Criteria
Inclusion criteria for this study were surgical intervention of first MTP arthrodesis, adult patients (older than 18 years), studies with level of evidence I to IV, full text, articles in English, and outcomes related to sport. Exclusion criteria were articles not in full text, abstracts only, non-English articles, no outcomes related to sport, pediatric patients (younger than 18 years), systematic reviews, meta-analyses, case reports, and surgical interventions other than first MTP arthrodesis.
Data Extraction
Data extraction was performed by multiple authors during the course of this study. Data collected include first author, year of publication, type of study (retrospective, prospective, randomized controlled trial), patient age, number of males/females, diagnosis at time of surgery, surgical intervention (variation of MTP arthrodesis or additional concurrent procedure), body mass index (BMI), comorbidities, RTS outcomes, complications, and follow-up time. For quality of return to sport (increased difficulty, decreased difficulty, or same difficulty), studies with similar sporting types were aggregated.
Bias and Quality Assessment
Observational studies were assessed via the Methodological Index of Non-Randomized Studies (MINORS) whereas randomized controlled trials (RCTs) were graded according to the Physiotherapy Evidence Database (PEDro) scale.
Statistical Analysis
This study used SPSS version 29.0 (IBM Corp, Armonk, NY) for statistical analysis. Frequency counts and descriptive data were used for patient demographics. Frequency-weighted means were used to compile data from individual articles.
Results
Initial Search Results
A total of 10 articles met the final inclusion criteria for this systematic review out of 249 articles found with the initial search criteria.1,2,4-7,9,10,14,15 The references were searched for the 10 included articles, but no additional articles were found that met inclusion criteria. See Figure 1 for the PRISMA diagram for visualization of the initial search, article screening, and final article selection. Nine of the included articles were observational studies, which were graded via the MINORS scale. Refer to Table 1 for the MINORS grading of the 9 observational studies. One study was a randomized controlled trial (RCT), which was graded via the Physiotherapy Evidence Database (PEDRO) scale. The article by Baumhauer et al 1 was an RCT that received a score of 6/10 points on the PEDRO scale. For Baumhauer et al 1 on the PEDRO scale, the article specified eligibility criteria, used random allocation, did not conceal allocation, used similar groups at baseline, did not perform subject anonymizing, did not perform clinician anonymizing, had less than a 15% dropout rate, did not use intention-to-treat analysis, did between-group statistical comparisons, and had point measures and variability data.
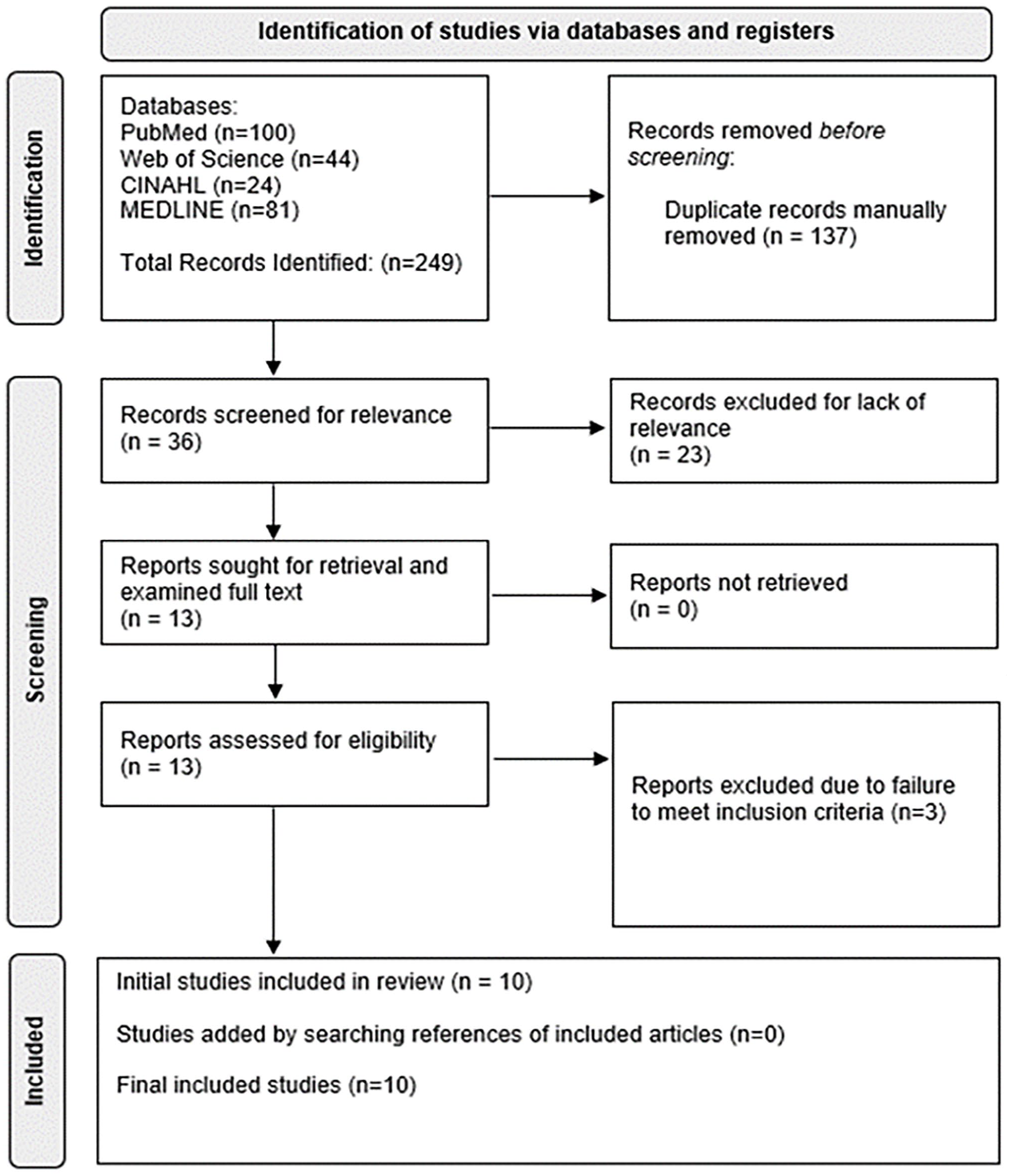
PRISMA diagram outlining the initial search, article screening, and final article selection for this systematic review.
Bias Grading for the 9 Observational Studies via the MINORS Scale Included in This Systematic Review. a
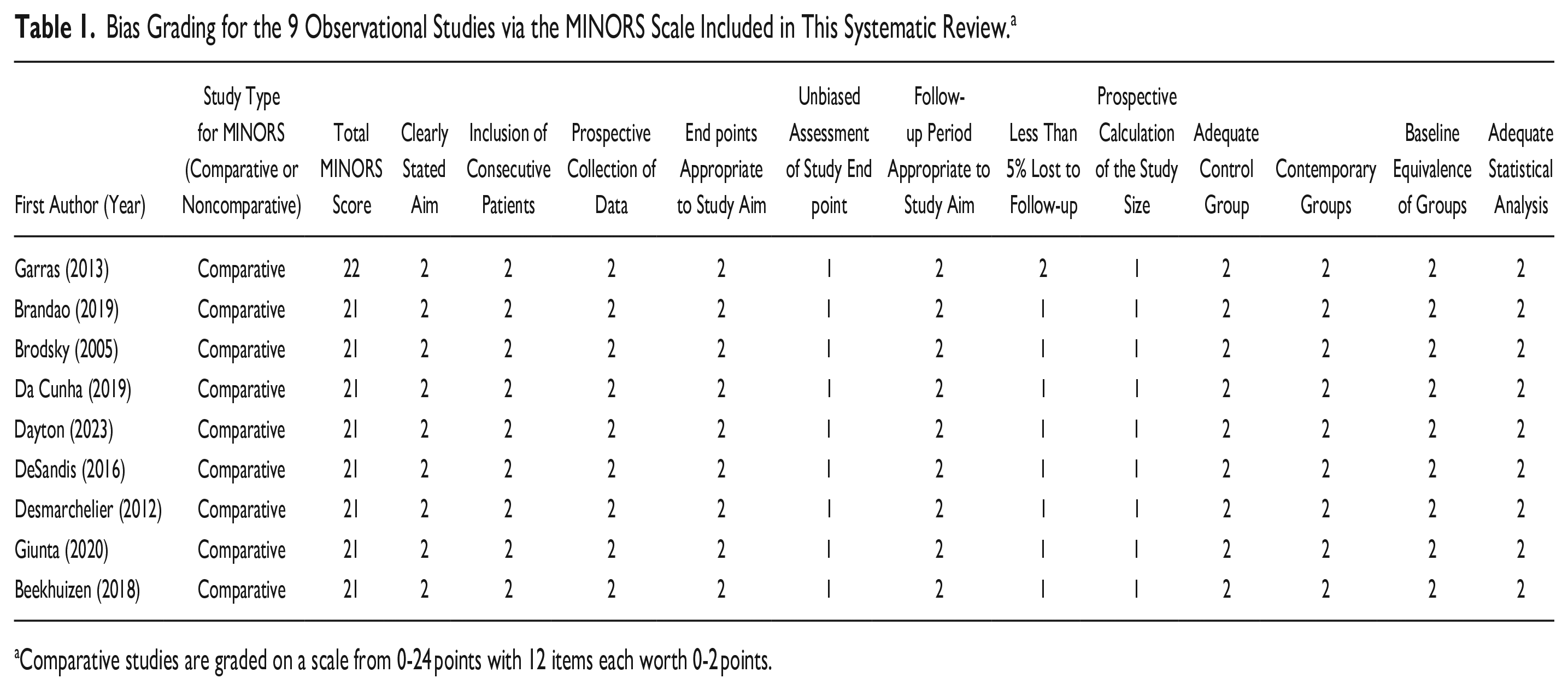
Comparative studies are graded on a scale from 0-24 points with 12 items each worth 0-2 points.
Patient Demographics
A total of 450 adult patients with a frequency-weighted mean age of 58.6 ± 5.1 years (n = 450 patients, 100.0%) with a frequency-weighted mean follow-up time of 32.1 ± 18.9 months (n = 450 patients, 100.0%). There were 347 patients (77.1% of patients) from studies that categorized patients as male or female, with 111 male patients (32.0% of patients) and 236 female patients (68.0%). All included patients (n = 450 patients) underwent first MTP arthrodesis with or without additional forefoot procedures for MTP pathology such as hallux rigidus or hallux valgus. Table 2 outlines further demographic information in the included patients in this systematic review such as number of patients, average age, female and male count, diagnosis, surgery type, body mass index, comorbidities, and follow-up time.
Information From the 12 Included Articles in This Systematic Review. a
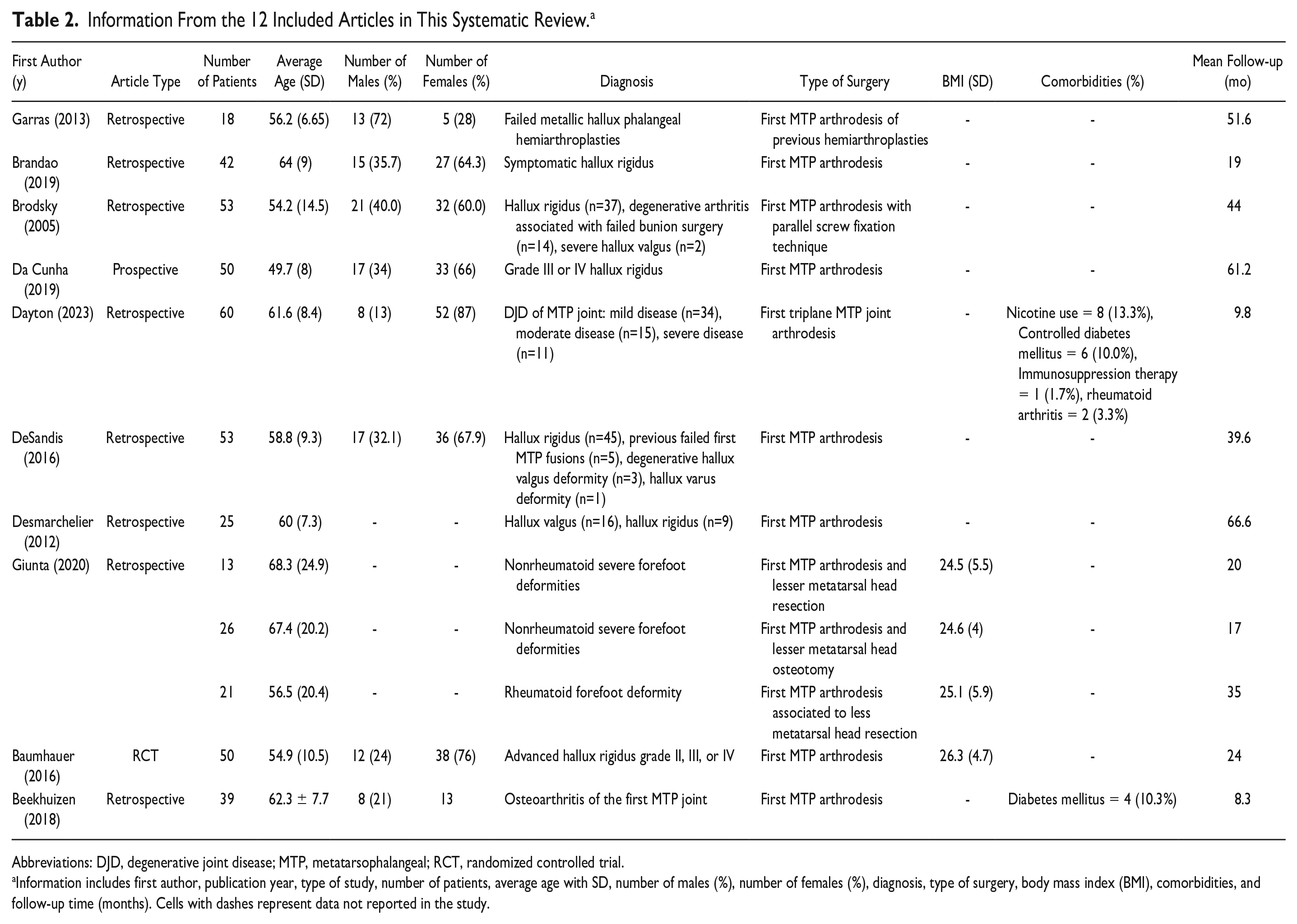
Abbreviations: DJD, degenerative joint disease; MTP, metatarsophalangeal; RCT, randomized controlled trial.
Information includes first author, publication year, type of study, number of patients, average age with SD, number of males (%), number of females (%), diagnosis, type of surgery, body mass index (BMI), comorbidities, and follow-up time (months). Cells with dashes represent data not reported in the study.
Included Sport Activities
Sporting activities included in this systematic review include jogging, running, use of a treadmill, yoga, golf, hiking, tennis, use of an elliptical, and biking. Sports not mentioned in the articles of this systematic review included surfing, skateboarding, lacrosse, and rugby among others.
Return to Sport Outcomes
Outcome measures reported in several of the included articles in this systematic review included the Foot and Ankle Ability Measure (FAAM) Sport and the Foot and Ankle Outcome Score (FAOS) Sports. Other measures included return to sport time (weeks), sport involvement (type of sport), rate of RTS, and change in sport activity after surgery (better, same, or worse). For FAAM Sport, 153 patients (34.0% of patients) had a frequency-weighted mean postoperative FAAM Sport score of 70.4 ± 21.8 at final follow-up. DeSandis et al 9 reported that patients undergoing MTP arthrodesis had an average preoperative FAOS Sports score of 50.4 (n = 42 feet) with a significant improvement for average postoperative FAOS Sports score of 75.3 (n = 52 feet) (P < .001). Brandao et al 4 studied 42 patients who underwent MTP arthrodesis and reported that the mean postoperative FAAM Sports score was 80.9% ± 21.9%. Beekhuizen et al 2 reported an RTS time of 11.7 ± 5.1 weeks in 39 patients after first MTP arthrodesis. DeSandis et al 9 reported that the greatest functional improvement noted in patients after first MTP arthrodesis was the ability to perform in-line athletic activities, such as walking, jogging, running, and treadmill activities. In that study, 24% of patients reported improvement in jogging activities and 23% of patients reported improvement in running. 9 For sporting activities reported by multiple studies such as running, yoga, golf, hiking, tennis, elliptical, and biking, about 9.8% to 28.1% of patients (n = 69 reports) stated that sporting activity got easier, 67.2% to 87.5% of patients (n = 340 reports) stated that sporting activity remained the same difficulty level, and 1.8% to 8.5% of patients (n = 23 reports) stated that sporting activity got harder after first MTP arthrodesis depending on the sporting activity.6,9 Information regarding breakdowns by difficulty level in specific sporting activities are illustrated in Table 3. DeSandis et al 9 also reported that postoperative limitations, as well as overall procedure satisfaction, was similar irrespective of patient age. Despite limitations, Dayton et al 7 reported that 97% of patients (58 of 60 patients) were satisfied with RTS after first MTP arthrodesis. Similarly, although 32% of patients in another study (n = 16 patients) described increased difficulty with RTS, all of these patients reported satisfaction with their first MTP arthrodesis procedure in terms of RTS. 6 From a total cohort of 50 patients, 96% of patients (48 of 50 patients) were satisfied with their first MTP arthrodesis procedure in terms of RTS. 6
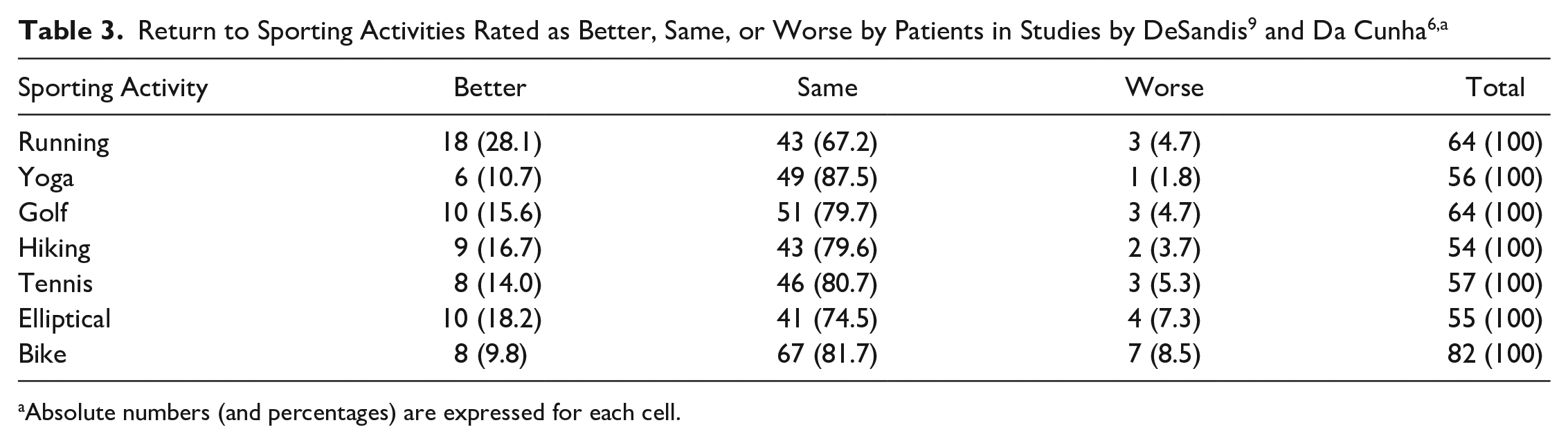
Absolute numbers (and percentages) are expressed for each cell.
Complications
Seven of the 10 included articles in this systematic review reported complications associated with MTP arthrodesis, which plays a role in RTS.1,2,4,9,10,14,15 There were 3 cases of superficial wound infection, 5 cases of hardware removal, 1 case of stress fracture, 4 cases of persistent pain after surgery, 16 cases of revision surgery, and 9 serious adverse events. For more detail on the complications associated with MTP arthrodesis in studies that reported RTS outcomes, refer to Table 4 below.
Complications Associated With the Included Patients for This Systematic Review. a
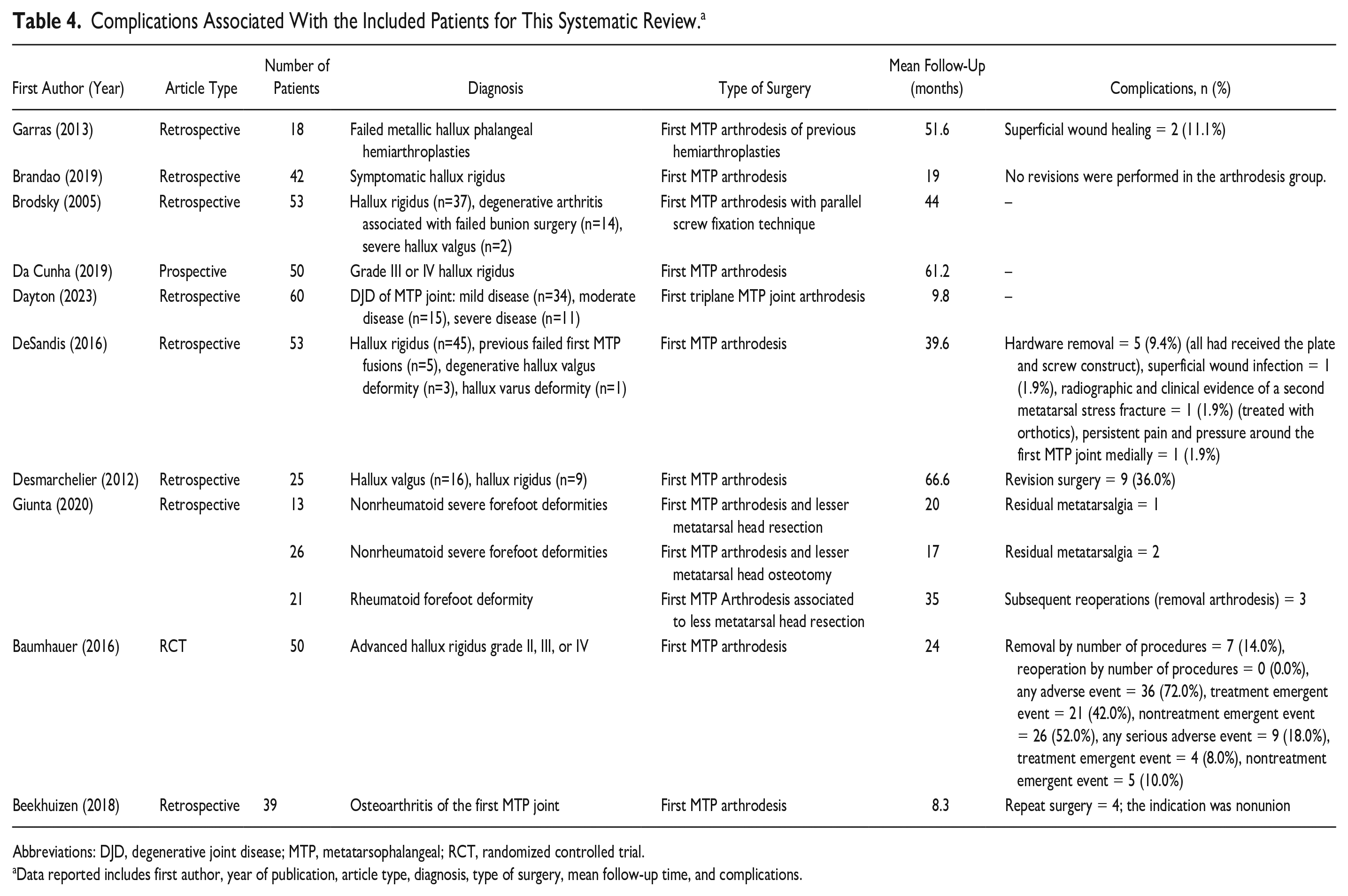
Abbreviations: DJD, degenerative joint disease; MTP, metatarsophalangeal; RCT, randomized controlled trial.
Data reported includes first author, year of publication, article type, diagnosis, type of surgery, mean follow-up time, and complications.
Discussion
The purpose of this systematic review was to examine participation levels and RTS in specific sport and physical activities in adult patients following first MTP joint arthrodesis. The vast majority of patients receiving MTP arthrodesis (>90% of patients) who participated in sport activity prior to surgery resumed their activities with a trend toward increased sport activity following first MTP arthrodesis, regardless of construct.6,7,9 Although the literature supports this trend in sport activities such as running, yoga, golf, hiking, tennis, elliptical, biking, and other similar sports, we suggest that several sports not mentioned in this systematic review may be particularly prone to functional disturbance caused by first MTP arthrodesis and require further research. Sporting activities such as surfing, skateboarding, and others may be difficult to resume because of the required dorsiflexed first MTP position of a participant’s foot to complete reasonably well. Therefore, it is plausible that patients may resume those sports with caution or with planned alterations to their footing, perhaps with the guidance/coaching of a physical therapist.
The literature is sparce with respect to return to specific sporting events following first MTP fusion. Perhaps the most robust study by Brodsky et al 5 reports on the activities of daily living and recreational sporting activities resumed following parallel screw fixation technique in 53 patients with a mean age of 54.2 (range, 21-79) years at a mean follow-up of nearly 4 years. The authors administered a questionnaire that queried walking, stair climbing, and return to work and specific recreational/sporting activities, including but limited to jogging, golfing, hiking, and tennis. The authors found that 75% returned to jogging, 80% returned to golf, 92% returned to hiking, and 75% returned to tennis. Although this study fits the general trend, we see in assessing all of the available literature and should be used to help counsel patients on postoperative expectations for resumption of sport, it lacks a temporal assessment of when patients can expect return to sport postoperatively. In their level IV, retrospective case series, Da Cunha et al 6 characterize RTS and physical activity following first MTP fusion specifically in younger patients, between ages 18 and 55 years, further provide meaningful generalizable data. Using a sports-specific, patient-administered questionnaire and FAOS, they report that approximately 45% of patients return to physical activities in less than 6 months, ~20% between 6 and 9 months, ~ 20% between 10 and 12 months, ~10% between 13 and 18 months, and approximately 5% between 19 and 24 months. 6 They report that patients reached their maximal participation levels in approximately 90% of physical activities, which was achieved in 26.1% of physical activities in less than 6 months. Importantly, they report that for none of their patients, any physical activity participated in preoperatively was discontinued postoperatively. 6
There are several limitations that limit the results and conclusions of this study. First, this systematic review consists mostly of observational studies, with only 1 randomized controlled trial, limiting the conclusions that can be drawn due to biases and confounding factors. This systematic review also consists of numerous articles that report RTS outcomes differently, which greatly limits the synthesis of the available data. The variability in sporting activities and methods of measuring RTS, along with the inability to determine the influence of confounding factors, limit the strength of the conclusions from this study. Nevertheless, this study represents the most comprehensive manuscript to date on the topic of RTS after first MTP arthrodesis and can serve both as a starting foundation for patient education and as an impetus for future research. Additional research should focus on prospective controlled trials, preferably randomized, with similar surgical approaches and reporting structures for RTS to allow for greater data synthesis and meta-analyses in the future. More research can build on the framework of this systematic review to improve patient counseling and education on RTS after first MTP arthrodesis.
Conclusion
RTS after first MTP arthrodesis is highly variable between patients and sport type. However, patients generally report a high degree of satisfaction with RTS after first MTP arthrodesis, with a majority of patients having similar or increased ability to RTS after surgery. Although numerous sporting activities have been examined in this systematic review, the impact of first MTP arthrodesis on other sporting activities is unknown at this time. This study represents the first systematic review in the literature to date on the topic of RTS after first MTP arthrodesis, providing a foundation for patient education as well as future high-level research.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231198817 – Supplemental material for Return to Sport After First Metatarsophalangeal Arthrodesis: A Systematic Review
Supplemental material, sj-pdf-1-fai-10.1177_10711007231198817 for Return to Sport After First Metatarsophalangeal Arthrodesis: A Systematic Review by Anthony N. Baumann, Kempland C. Walley, Nazanin Kermanshahi, Albert T. Anastasio, James R. Holmes, David M. Walton and Paul G. Talusan in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.