
Abstract
Background:
Cutaneous reflexes serve an integral role in maintaining efficient movement patterns and may be linked to sensory-perceptual deficits experienced by those with chronic ankle instability (CAI), namely, during the stance and transitional phases of the gait cycle. Abnormal reflex characteristics and perceptions of instability following unexpected perturbation have the potential to serve as potential patient-specific biomarkers for neuromuscular recovery following a lateral ankle sprain (LAS), however, these outcomes are scarcely explored.
Methods:
The purpose of this retrospective case control study (level III) was to observe lower limb cutaneous reflex patterns and variability as well as perceived instability following sural nerve stimulation in those with CAI. These outcomes were measured via electromyography of 6 lower limb muscles and self-reported perceived instability as participants received random, non-noxious stimulations while walking on a treadmill.
Results:
Those with CAI exhibited elevated peroneus longus facilitation and gastrocnemius reflex variability during midstance that were correlated with greater levels of perceived instability following sural stimulation.
Conclusion:
These findings indicate reflex alterations may contribute to perceived instability during functional activity, a hallmark symptom of CAI.
This is a visual representation of the abstract.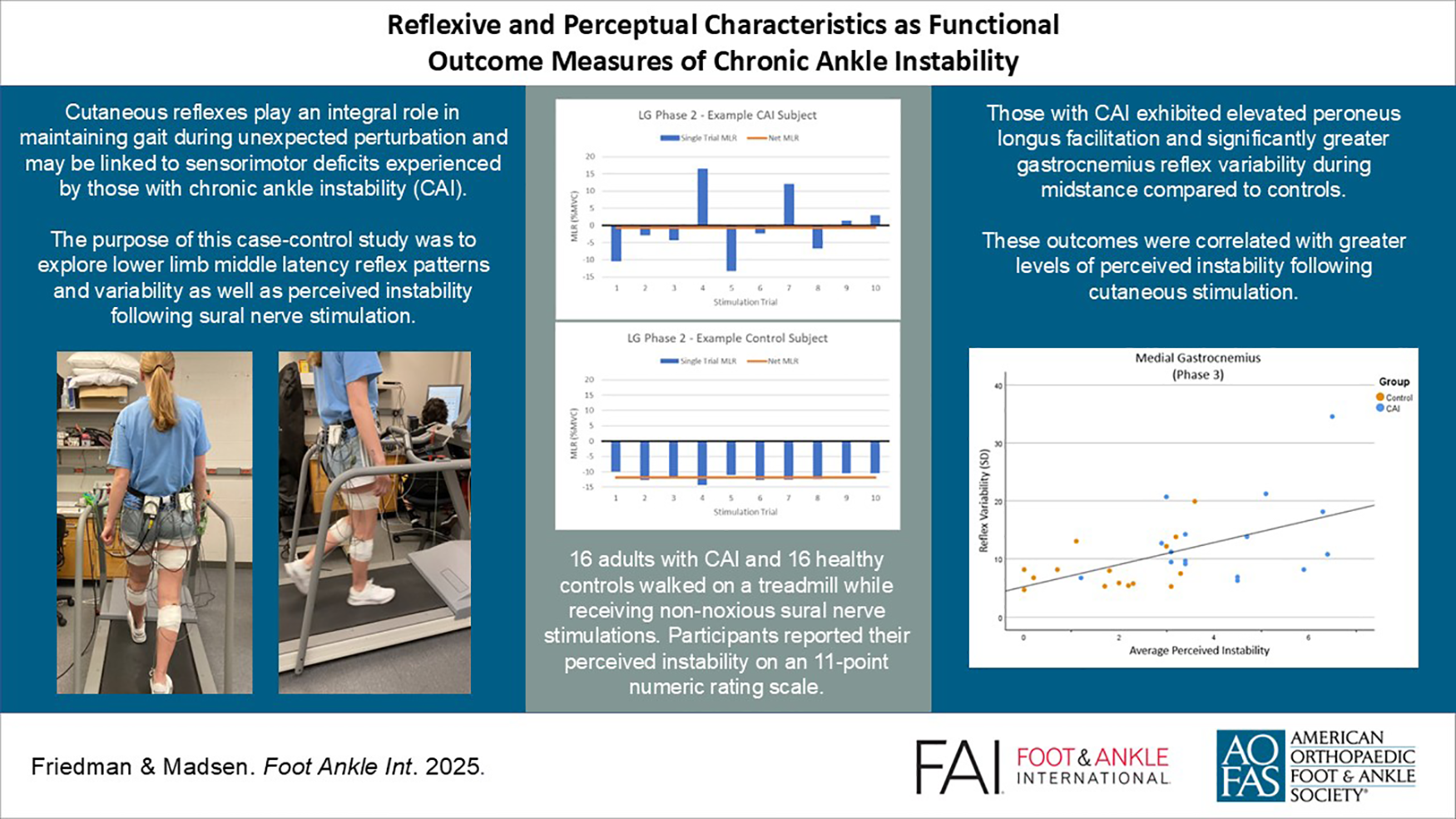
Introduction
With an incidence of more than 2 million in the United States annually, lateral ankle sprains (LAS) account for 15% of all athletic injuries, and approximately half of all LAS occurring among the general population. 16 Between 40% and 70% of individuals experiencing acute LAS will develop chronic deficits such as pain, perceptions of ankle weakness or giving way, limited range of motion, diminished sensorimotor function, and recurrent LAS, which comprise chronic ankle instability (CAI).15,16 Considered a multifaceted condition, CAI development arises from a variety of pathomechanical, sensorimotor, environmental, and personal factors, many of which have been thoroughly investigated over several decades.15,20 Recent CAI research has pivoted toward neuromuscular contributors to the condition, namely, lower limb cutaneous reflexes.2,15
Cutaneous reflexes modulate muscle activity at the spinal level to maintain postural stability and prevent injury when the skin is touched or stretched, such as when encountering an unexpected obstacle or walking on uneven surfaces.30,49 Recent literature has identified specific reflex patterns in those with CAI that affect dynamic joint stability mechanisms, contribute to perceptions of instability, and may play a role in reinjury risk.6-9,13,24 Alterations in spinal reflexes may also play an important role in subjective outcome measures such as perceived instability, self-reported function, and health-related quality of life. The unpredictable nature of perceived instability likely contributes to the fear of reinjury and subsequent reduced physical activity seen in individuals with CAI. 39 One study 43 found perceived instability reported via the Cumberland Ankle Instability Tool (CAIT) and Ankle Instability Instrument could predict 20% of the variance in soleus spinal reflex excitability as measured by Hoffmann reflex among those with CAI. The CAI participants in this study exhibited a disinhibition of the soleus, indicating an inability to appropriately modulate spinal reflexes during tasks that threaten postural stability. 43 Considering episodes of perceived instability are typically intermittent, alterations in motor output may contribute to the variability of subjective symptoms experienced by those with CAI during physical activity.
By exploring their specific presentation during functional activity, these reflexive and perceptual outcomes have the potential to serve as markers of sensorimotor deficit among those with CAI and could be used to monitor neuromuscular recovery following injury. For example, one study 34 explored static balance and motoneuron pool excitability as potential biomarkers for sensorimotor function, finding these outcomes, in combination, could predict CAI status. To examine reflex characteristics and perceived instability in those with CAI, the purpose of this study was threefold. The first aim was to substantiate previous findings, specifically, that those with CAI exhibit unique reflex modulation patterns across the stance phase of gait compared with healthy controls. Because cutaneous reflex measurement during this functionally relevant task has the potential to serve as a marker of neuromuscular recovery, the second aim was to then identify which specific variables (reflex amplitudes and variability among specific lower limb musculature) contribute to abnormal reflex modulation. Finally, because perceived instability is a hallmark symptom of CAI and may be linked to reflexive outcomes, this study also sought to explore how perceived instability following sural nerve stimulation relates to specific cutaneous reflex characteristics exhibited by those with CAI.
Methods
This study was part of a larger experiment exploring reflexive and perceptual outcomes across two experimental sessions; therefore, the following methodologies only describe experimental procedures relevant to this study’s aims. A more detailed description of experimental methods for group assignment, electromyographical measurements, gait cycle timing, sural nerve stimulation parameters, and reflex data processing may be found in a separate article. 5
Participants
Thirty-two participants volunteered for the study (control: n = 16 [11 female, 5 male), 21.2 ± 4.72 years, 167 ± 8.31 cm. height, 65.8 ± 12.7 kg weight; CAI: n = 16 (10 female, 6 male), 21.1 ± 5.03 years, 171 ± 10.4 cm. height, 70.8 ± 14.7 kg weight). Referencing similar studies, the participant pool target was n = 29 as determined by a power analysis for a moderate effect size (r = 0.70, α = .05). All participants completed the CAIT and Identification of Functional Ankle Instability (IdFAI) questionnaires to determine group assignment, a method endorsed by the International Ankle Consortium. 10 Specifically, all subjects enrolled in the CAI group had a cumulative score of ≤27 on the CAIT and ≤11 on the IdFAI (Table 1). The most affected limb served as the test limb in CAI participants, which was matched based on limb dominance among control participants to ensure that the same number of dominant and nondominant limbs were evaluated in each group.
CAI Questionnaire Cut-off Scores and Average Group Scores.

Abbreviations: CAI, chronic ankle instability; CAIT, Cumberland Ankle Instability Tool; IdFAI, Identification of Functional Ankle Instability.
Protocol
Muscle activity of the tibialis anterior (TA), peroneus longus (PL), medial (MG) and lateral (LG) gastrocnemius, rectus femoris (RF), and biceps femoris (BF) were continuously measured via wired bipolar surface electrodes applied to the test limb (Delsys Inc, Natick, MA). A stimulating bar electrode (Ambu, Inc, Columbia, MD) affixed over the sural nerve of the test limb was used to administer random, non-noxious stimulations at the level of each participant’s radiating threshold multiplied by 2. This final stimulation intensity was ultimately reduced in most participants (n = 23) to ensure pain and withdrawal reflex were not produced during the walking task. All participants walked at 4 km/h on a treadmill for approximately 20 minutes while receiving sural stimulations across 5 equal phases of stance, heel strike (phase 1) to toe-off (phase 5) of the test limb. Stimulation trials were randomized to ensure 10 stimulations occurred at each of these phases, totaling 50 trials throughout the walking task. Additionally, participants reported their feelings of instability on a subjective scale of 0 (no instability) to 10 (severe instability) following each stimulation trial. Participants were instructed that a report of zero describes “no instability” and “normal gait,” whereas a report of 10 describes “feeling as if you may stumble or lose balance.”
Data Processing
All data processing was completed offline using AcqKnowledge 5.0 software. Following filtering and normalization procedures, 5 stimulated trials were reviewed for step timing consistency, and successful trials (10 for each phase) were ensemble averaged. Approximately 100 unstimulated gait cycles were also identified and ensemble averaged and subtracted from stimulated trials, resulting in a reflex waveform for each muscle at each phase. Middle-latency reflex (MLR) values were identified as the mean amplitude of the reflex waveform 80-120 ms after the first pulse in the stimulation train. MLR values for 6 muscles during each of the 5 gait phases were extracted for statistical analysis. Unstimulated amplitudes during this time window were also extracted for analysis of background muscle activity. Additionally, normalized stimulated waveforms were extracted for analysis of reflex variability, that is, the SD of the 10 trials at each phase for each muscle.
Statistical Analyses
Background Muscle Activity
As a protective mechanism to appropriately match the task, reflex amplitudes are enhanced with increases in background muscle activity, a result of increasing excitation of the motoneuron pool.25,36 Because motor units are recruited in order of their force-producing capability, larger motor units would be the first to be influenced by afferent input as they are closer to their recruitment thresholds during physical activity while smaller motor units are already discharging.14,32,36 Therefore, it is important to determine if the background electromyographic (EMG) pattern was significantly different between groups in any muscle throughout the gait cycle, which may have affected subsequent reflex ampltudes.25,37 To compare background muscle activity throughout testing between the 2 groups, 6 separate 2-way mixed-factor analyses of variance (one for each muscle) were run with 1 between-subjects factor at 2 levels (CAI and control groups) and 1 within-subjects factor at 5 levels (phase of gait). Interactions and group main effects of these analyses were used to identify specific differences that were further analyzed via Pearson correlations to determine whether reflex amplitudes were associated with background EMG.
Aims 1 and 2: Cutaneous Reflexes
To explore reflex patterns throughout gait (aim one), one-sample t tests for each muscle were used to identify significant reflex amplitudes from zero during each phase within each group. This analysis is commonly used among cutaneous reflex literature to reveal specific reflex patterns throughout the gait cycle.24,46 To further explore group differences in reflex amplitude and reflex variability (aim 2), independent t tests were run for specific muscles of interest as revealed by one-sample t tests from aim 1 analyses. Average reflex amplitudes and SD of the 10 normalized stimulated trials were used for aim 2 analyses.
Aim 3: Perceived Instability
A one-way analysis of variance with 1 between-subjects factor at 2 levels was run for each phase of stance to compare perceived instability between groups. Pearson correlations were run to examine the relationship between perceived instability and reflex characteristics, both average reflex amplitude and reflex variability. These were determined by group differences revealed by aim 2 analyses. All statistical analyses were conducted using IBM SPSS version 29.0.1 (IBM Corporation, Armonk, NY) with significance set a priori at P ≤.05.
Results
Box and whisker plots were used to identify extreme outliers, which were subsequently explored to determine whether the EMG values accurately represented muscle activity collected throughout the testing session. One participant (n = 1, female) from the control group was removed from the sample as they exhibited clearly abnormal reflex amplitudes throughout several phases of the gait cycle, likely due to equipment error, which affected control group analyses. All other outliers were inspected and confirmed to represent accurate reflex and background muscle activity. This left 31 participants for the final analyses (demographic information reflects final sample).
Background Muscle Activity
Two-way mixed factor analyses of variance revealed a significant phase-by-group interaction for the PL only (F1.99,57.6 = 4.55, P = .015, partial ƞ2 = 0.136). Because Mauchly’s test indicated that the assumption of sphericity had been violated, χ2(9) = 63.3 (P < .001), results were adjusted with a Greenhouse-Geisser correction. Simple main effects revealed the control group exhibited significantly greater PL background activity during phase 4 compared with the CAI group (CAI = 57.8% ± 14.9%, control = 71.49% ± 14.6%, P = .016). Pearson correlations during phase 4 indicated no significant relationship was present between background PL activity and PL reflex amplitudes, r(29) = .164 (P = .379). No group main effects were identified for any muscle, but significant phase main effects were identified for all muscles (P < .001), indicating background EMG amplitudes varied throughout the gait cycle in accordance with the demands of the walking task.
Aim 1: Cutaneous Reflex Pattern Exploration
In the TA, one-sample t tests revealed that both groups exhibited significant facilitation during phases 4 and 5; however, the CAI group exhibited significant facilitation during phase 3 (T15 = 2.31, P = .035, 95% CI 0.522, 12.9) whereas controls did not (T14 = 2.31, P = .144, 95% CI −1.16, 5.83). Significant PL facilitation was exhibited by both groups throughout stance except during phase 3, where the control group did not exhibit a significant PL reflex (T14 = 1.79, P = .095, 95% CI −4.31, 48.2). The control and CAI groups exhibited similar reflex patterns in the MG, namely, significant inhibition at phases 2-4 and facilitation at phase 5. Significant LG inhibition during phases 3 and 4 and significant LG facilitation at phase 5 were identified for both groups. The control group also exhibited significant LG inhibition at phase 2 (T14 = −2.90, P = .012, 95% CI −8.84, −1.33), whereas the CAI group did not (T15 = .122, P = .905, 95% CI −6.50, 7.28). Additionally, neither group exhibited a significant MG or LG reflex at phase 1. Both groups exhibited statistically significant facilitation of the RF and BF throughout stance. Peak RF facilitation occurred at phase 3 for both groups (CAI: 66.7% Control: 83.7%), whereas peak BF facilitation occurred at phase 1 among the CAI group (19.3%) and at phases 1 (17.1%) and 5 (17.7%) among controls. Reflex patterns for all 6 muscles measured in this study are represented in Figure 1.
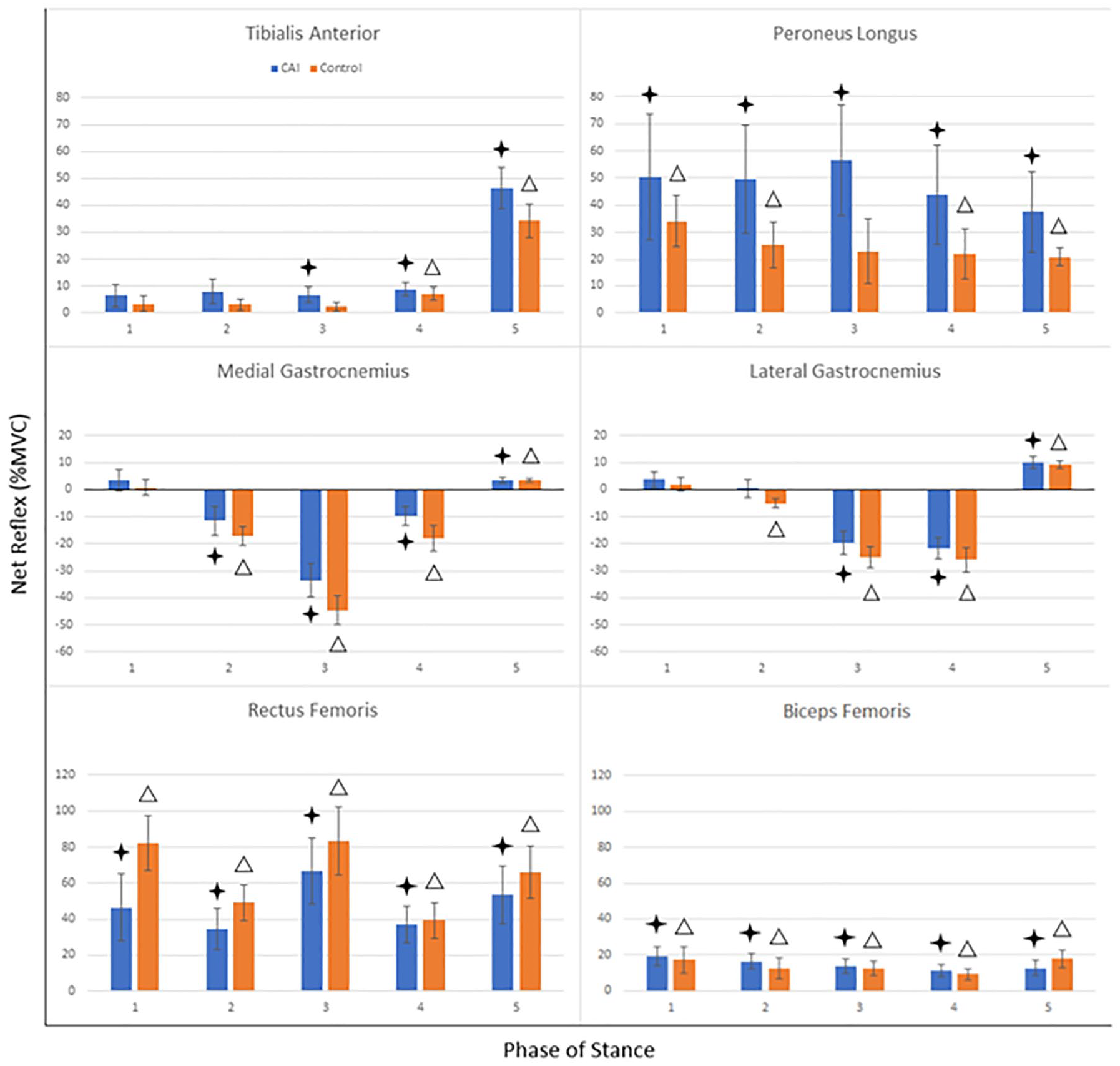
Cutaneous reflex patterns across stance for all muscles. Net reflexes with standard error bars: significant reflexes (P ≤ .05) based on one-sample t tests are indicated by a star for the CAI group, and a Δ for the control group.
Aim 2: Unique CAI Reflex Characteristics
Aim 1 analyses revealed that reflex patterns among the CAI group differed from controls for the TA, PL, and LG; therefore, these muscles were evaluated further to identify whether group differences in reflex amplitudes or variability contributed to these patterns. Considering the abnormal reflexive activity previously reported in the triceps surae,4,6,24 the MG was also included in aim 2 and 3 analyses.
The CAI group exhibited significantly greater LG variability at phase 2 compared with controls (T29 = 2.04, P = .025, Cohen d = .735) ranging from −15.6% to 35.8%. The CAI group also exhibited significantly greater MG reflex variability during phases 2 (T29 = 2.98, P = .006, Cohen d = 1.07), and 3 (T29 = 2.16, P = .039, Cohen d = .777). Illustration of LG findings within single subjects may be found in Figure 2. No group differences in reflex variability were identified for the TA or PL throughout stance. Although facilitation of the PL was visually greater among the CAI group throughout stance, independent t tests revealed no significant differences in reflex amplitudes between groups. Similarly, no significant group differences in reflex amplitude were identified for the TA, LG, or MG throughout stance.
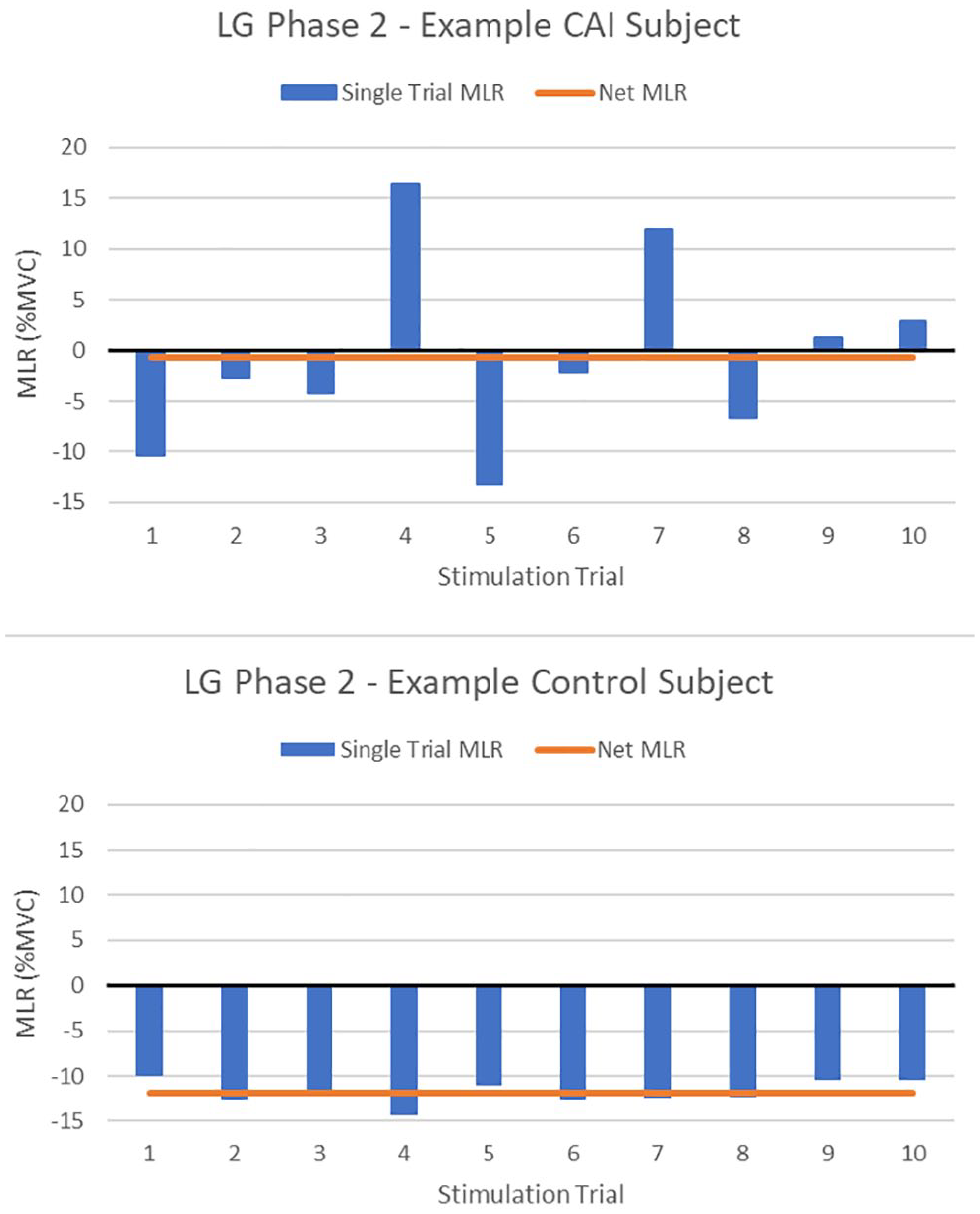
Example subject single trial reflexes and net reflexes. Phase 2 (early stance) LG middle-latency reflexes (MLR) extracted 80-120 ms after each sural nerve stimulation (10 per phase) denoted in blue. The CAI subject exhibits relatively high reflex variability (SD = 9.24%) whereas the control subject exhibits low variability (SD = 1.37%). The orange line denotes resultant net LG reflexes for each subject at this phase. [See online article for color figure.]
Aim 3: Perceived Instability
Overall, participants with CAI reported significantly greater levels of instability following sural nerve stimulation throughout the stance phase of gait (P < .001 for all phases, CAI = 4.63 ± 1.91, control = 2.23 ± 1.73). Pearson correlations revealed a significant positive relationship between PL reflex amplitude at phase 3 and perceived instability following sural nerve stimulation, r(29) = .407 (P = .023). Perceived instability was also significantly correlated with LG reflex variability at phase 2, r(29) = .403 (P = .025) (see Figure 3), and MG reflex variability at phases 2, r(29) = .454 (P = .010), and 3, r(29) = .537 (P = .002) (see Figure 4). Perceived instability was not correlated with TA reflex amplitude or variability during any phase of stance.
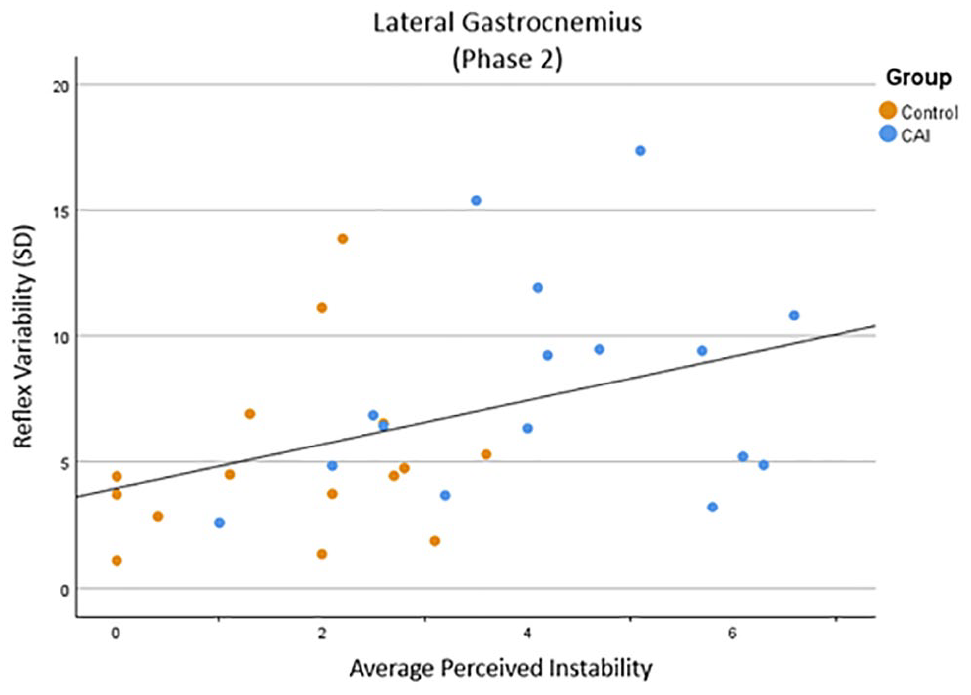
Scatterplot with line of best fit illustrating positive linear relationship between average perceived instability and LG reflex variability at phase 2.
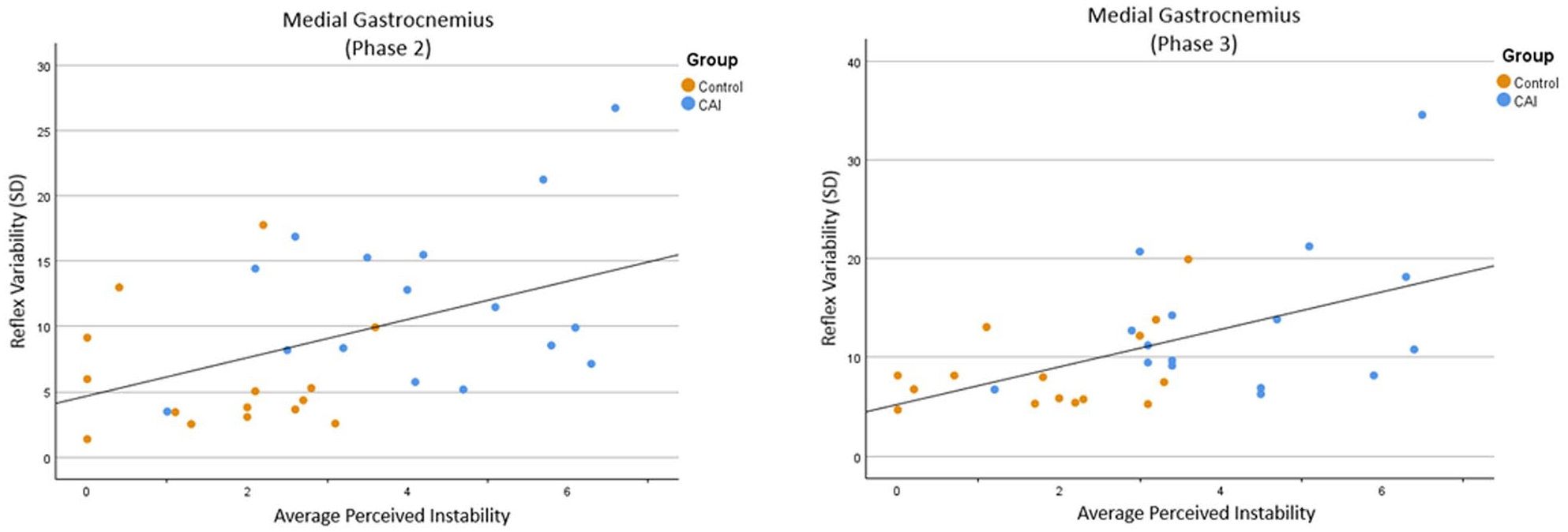
Two scatterplots with line of best fit illustrating positive linear relationship between average perceived instability and MG reflex variability. The left scatterplot depicts phase 2 correlations whereas the rightm scatterplot depicts phase 3 correlations.
Discussion
Cutaneous Reflex Patterns
The cutaneous reflex patterns observed in this study were generally well-aligned with previous literature examining reflexes of healthy individuals and those with CAI. During late stance, facilitation of the TA is typically observed as a mechanism to dorsiflex the foot up and away from a perceived obstacle while transitioning into swing.3,23,24,45,46 This facilitation was observed during late stance (phase 4) and the stance to swing transition (phase 5) in both groups; however, the CAI group also exhibited TA facilitation during midstance (phase 3). This may act to provide additional stability at the ankle during maximal, single-limb weightbearing, stability which is enhanced by the pronounced PL facilitation observed during the same phase among those with CAI (see Figure 1). Coactivation of the TA and PL during this time would increase sagittal and frontal plane joint stiffness, counteracting an inversion sprain mechanism.11,22,29 PL facilitation was observed throughout the other phases of stance in both groups, and although this reflex was more pronounced in the CAI group, no significant group differences were identified, likely because of marked variability in average PL reflex amplitudes across the sample.
Inhibition of the gastrocnemius muscles during midstance and facilitation during the transition to swing is well evidenced among healthy individuals.23,24,46 This pattern was observed in both control and CAI groups, as MG inhibition was exhibited during phases 2-4 which then became facilitatory during phase 5. This pattern was also exhibited by both groups in the LG; however, the CAI group exhibited delayed inhibition, reaching statistical significance at phases 3 and 4 only. Inhibition during stance acts as an unloading mechanism in preparation for efficient transition to the contralateral limb should postural control become compromised.24,46 Therefore, delayed gastrocnemius inhibition may leave an individual inadequately prepared should sudden perturbation threaten stability during single-leg stance. This substantiates findings from a 2019 study 24 that observed delayed inhibition of the MG and LG until phase 3 in the MG and phase 4 in the LG, suggesting those with CAI exhibit difficulty in appropriately modulating motor responses throughout the stance phase.
Continuous RF and BF facilitation throughout stance in response to cutaneous stimulation as observed in this study also aligns with previous literature.41,44,48 This facilitation would provide functional bracing at the knee when experiencing an unexpected obstacle while in single-leg stance. 48 One notable difference in this study was the ratio of facilitation of the BF and RF at the transition to swing. Previous studies41,44,48 indicate facilitatory activity of knee flexors should surpass that of the knee extensors to allow for withdrawal of the limb away from a perceived obstacle; however, both groups exhibited remarkably greater RF facilitation (control: 66.0% ± 14.7%, CAI: 53.5% ± 15.9%) compared with the BF (control: 17.7% ± 5.05%, CAI: 12.6% ± 4.42%) at phase 5. Considering the RF is also a hip flexor, the pronounced facilitation observed during the terminal stance may indicate this withdrawal mechanism occurred further up the kinetic chain.
Unique CAI Reflex Characteristics
Although the CAI group exhibited some reflex patterns which varied from those of controls, there were no significant differences in reflex amplitudes between groups at any phase of stance. Considering average reflex amplitudes for each participant were derived from the mean of 10 individual stimulation trials, these pattern alterations may be attributed to another source, reflex variability. For example, the CAI group exhibited a net LG reflex amplitude of 0.039% during phase 2; however, LG amplitudes ranged from −15.6% (inhibition) to 35.8% (facilitation) among CAI participants, suggesting not all participants exhibited absent LG reflexes during this phase. Similarly, at an individual level, rather than exhibiting no motor response to stimulation during all 10 trials, CAI participants often exhibited facilitation during some stimulation trials, and inhibition during others, meaning a participant’s net reflex may not accurately reflect their motor response to every perturbation at that phase (see Figure 2).
The CAI group exhibited significantly greater LG reflex variability during early stance (phase 2) compared with controls, which likely contributed to the absent LG inhibition observed in the CAI group during this phase. MG reflex variability was also significantly greater among the CAI group in early and midstance (phases 2 and 3), although this did not translate to differences in reflex patterns between groups as both exhibited significant net MG inhibition. Considering the protective role cutaneous reflexes serve during gait, irregularity in motor response to an unexpected perturbation may leave an individual at greater risk for loss of balance or subsequent injury.
Perceived Instability
Variability in reflexive activity may also account for the elevated levels of perceived instability seen among those with CAI (see Figure 5). When evaluating perceived instability reports among our sample, greater LG and MG variability during midstance were significantly correlated with higher levels of perceived instability following sural nerve stimulation (see Figures 3 and 4, respectively). This aligns with a recent study from our laboratory that found PL and LG reflex variability could predict perceived instability during perturbated gait. 6 Specifically, greater levels of PL ad LG variability predicted greater perceptions of instability following sural nerve stimulation in participants with and without CAI, indicating inconsistencies in motor output following lateral perturbation may be responsible for feelings of giving way at the ankle. 6 Other studies have also identified relationships between reduced spinal excitability and self-reported function via the Foot and Ankle Ability Measure and the CAIT, indicating reflexive alterations may play a role in general perceptions of instability during physical activity.12,43 Considering feelings of instability are intermittent among those with CAI, varying in severity and frequency across different activities, greater variability in lower limb reflexes would indicate some instances of inadequate motor output in response to an unexpected perturbation. Irregular spinal reflex modulation may then be consciously perceived as novel or uncontrolled and could explain the unpredictable nature of perceived instability.
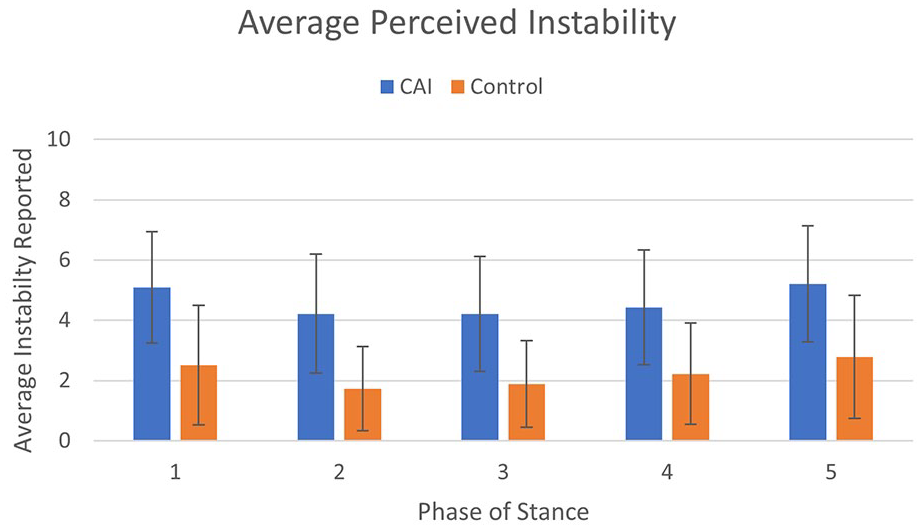
Average perceived instability reported by each group during the first 5 phases of the gait cycle (stance). Error bars represent SD of instability reports.
Greater levels of perceived instability were also correlated with increased PL reflex amplitudes at midstance (phase 3). The CAI group exhibited peak facilitation at this phase although no significant reflex was observed among controls, indicating this facilitation may be amplified beyond what is necessary for dynamic stabilization of the ankle. In a study 33 exploring cutaneous reflexes while standing, those with CAI exhibited hyperreactivity following noxious sural stimulation, exhibiting an exaggerated unloading response that the authors concluded may play a role in the feelings of instability this population frequently experiences. The pronounced PL facilitation seen among the CAI group during midstance is a similar dramatization of the protective response to prevent injury following stimulation, which may explain the positive relationship observed between perceptions of instability and PL reflex amplitude.
Clinical Implications
Every CAI subject enrolled in the present study met or exceeded questionnaire thresholds (see Table 1); thus, we can be assured that our sample falls within the heterogeneous condition of CAI, and our results can be accurately compared to any other study implementing these same stringent guidelines. The role of cutaneous reflexes in maintaining postural control and preventing injury during gait is well established.30,49 Additionally, perceptions of instability contribute to the fear of reinjury, reduced physical activity and diminished health-related quality of life seen in individuals with CAI.18,19,39 Therefore, the unique reflex characteristics and associated perceived instability identified in this study may be clinically relevant biomarkers following LAS. Because these outcomes exhibit plasticity, clinicians may observe modification of reflexive and perceptual measures over time.7,21,31,47 The unique reflex characteristics observed among those with CAI in this study may be measured both post-injury and throughout rehabilitation to monitor for normalization of reflexive activity or reduction of perceived instability following sural stimulation as markers of neuromuscular recovery. For example, LG reflex variability is correlated with perceived instability following stimulation, as a patient with recurrent LAS undergoes rehabilitation, LG reflexive activity and patient-reported instability may be monitored during midstance to serve as a clinical measure of improved neuromuscular control (ie, improved consistency of reflexive output). Although capturing accurate EMG data in a controlled clinical environment requires additional equipment and training, surface electrodes are noninvasive and the assessment can become time efficient if the outcomes of interest are narrowed to those presented in this study.
Considering the wide range of symptoms exhibited by those with CAI, it is likely not all patients would exhibit reflexive alterations identified in this study. This may be observed in Figures 3 and 4 where some CAI participants exhibit relatively low gastrocnemius reflex variability and perceived instability, aligning more with the control group. However, those demonstrating unique reflex patterns would benefit from monitoring and targeting these deficits just as clinicians may target deficient dynamic balance with specific interventions.26,27 Patient-specific rehabilitation focusing on the reflexive and perceptual outcomes explored in this study may involve traditional mobility, strength, and proprioceptive exercises with monitoring of reflexive markers, such as gastrocnemius variability during gait. Clinicians may also monitor reports of perceived instability in both controlled settings (cutaneous stimulation during gait) and during uncontrolled dynamic activity to observe how rehabilitation alters this patient-reported outcome measure. A recent study 7 observing PL cutaneous reflexes while seated found that MLRs typically recover within approximately 3 months after an initial LAS without participation in a clinical rehabilitation program. However, those with recurrent LAS exhibited reflexive alterations that persisted beyond 3 months post-injury, indicating these individuals may benefit from more targeted therapies.
In exploring motor neuron pool excitability in CAI participants, McVey et al 28 highlighted the need for establishing specific techniques to address arthrogenic muscle inhibition following recurrent LAS, as a strategy to reduce the incidence of the condition. Several more recent studies have explored such techniques to target the complex sensorimotor control systems to which cutaneous reflexes contribute.1,35,40,42 Some of these interventions include whole body vibration therapy, stochastic resonance stimulation, and visual biofeedback. One study 35 targeting cutaneous reflexes, specifically, found subthreshold mechanical stimulation modified TA and soleus reflex modulation, improving postural control mechanisms while standing with a forward lean. During gait, outcomes explored in the present study, such as excessive gastrocnemius reflex variability, have the potential to be similarly addressed though targeted therapies.
Limitations
Considering the multifaceted nature of CAI, participants in the CAI group are likely to present with heterogeneous symptoms and injury history. To account for this possibility, this study employed International Ankle Consortium recommendations 10 so that all participants in the CAI group met at least minimum diagnostic criteria derived from both the IdFAI and the CAIT. This ensured all participants sustained at least 1 LAS and were actively experiencing feelings of instability during physical activity. The inherent subjectivity of the perceived instability reporting scale should also be noted as a potential limitation of this study. Perceived instability is considered a highly subjective and complex outcome measure. To illustrate this, a 2022 study 38 exploring perceived instability used elements of 5 separate questionnaires to assess perceived instability and its relationship to other outcomes such as pain, ankle function, and fear-avoidance behaviors. Although only 2 other studies5,6 to date have used a numeric rating scale (NRS) to measure perceived instability following cutaneous stimulation, it should be noted that the 11-point (or 0-10) NRS is considered a reliable and valid tool for measuring pain levels in both clinical and human research settings. 17 To ensure all participants reported as accurately as possible, the same script was used during warm-up and again prior to testing to explain the instability scale. Additionally, it should be noted that discussion regarding the functional purpose of cutaneous reflexes during stance is informed by previous literature and based on interpretation of observed muscle activity alone, as joint kinematics were not measured in this study.
Although this study used rigorous statistical methods, the number of comparisons across muscles and gait phases increases the potential for Type I error. Given the exploratory nature of this analysis, findings should be interpreted with appropriate caution, and future studies with larger sample sizes and targeted hypotheses are warranted to confirm these results. All stimulation intensities were determined using the same procedures for each patient based on radiating threshold and lack of withdrawal reflex / pain. The inherent variability of the stimulation intensity across patients ensures consistency in patient perception of and physical response to this stimulation. Although this study identified specific cutaneous reflex characteristics that could serve as clinically relevant, potential biomarkers of neuromuscular function, it is important to explore these measures over time to determine the rate at which they change across LAS recovery or rehabilitation. Future studies should explore whether these results can be replicated across multiple testing sessions, as was initiated in a recent study from our laboratory, 5 to identify the efficacy of these reflexive and perceptual outcome measures in a longitudinal exploration. Future studies should also examine the effects of direct sensory interventions such as stochastic resonance or whole-body vibration on these outcome measures to better understand how clinicians may modify reflexive characteristics and perceived instability in those with CAI.
Conclusion
Cutaneous reflex patterns observed in this study are generally well aligned with those of previous literature exploring healthy and CAI populations. Although not statistically different from controls, the significant PL facilitation exhibited by the CAI group may indicate an exaggerated stabilization response in those with previous LAS. Reflex variability may play an important role in the altered gastrocnemius reflexes seen in the CAI group during midstance. Perceived instability following sural nerve stimulation provides insight into the consistency of dynamic stability responses during perturbated gait. Cutaneous reflexes and perceived instability following sural nerve stimulation may serve as potential biomarkers for neuromuscular recovery across LAS rehabilitation.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007251338279 – Supplemental material for Reflexive and Perceptual Characteristics as Functional Outcome Measures of Chronic Ankle Instability
Supplemental material, sj-pdf-1-fai-10.1177_10711007251338279 for Reflexive and Perceptual Characteristics as Functional Outcome Measures of Chronic Ankle Instability by Annalee M. H. Friedman and Leif P. Madsen in Foot & Ankle International
Footnotes
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Indiana University–Bloomington (protocol code 20192; approved 08/28/2023).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.