
Abstract
Background:
Patients with diabetes are at increased risk for postoperative complications after ankle arthrodesis (AA) and total ankle arthroplasty (TAA), yet few studies directly compare outcomes between these procedures in a matched diabetic cohort. This study evaluates outcomes of TAA vs AA in patients with diabetes with end-stage ankle arthritis.
Methods:
We performed a retrospective cohort study using the TriNetX Research Network. Adults undergoing primary TAA (Current Procedural Terminology [CPT] 27702) or ankle arthrodesis (CPT 27870 or 29899) between 2005 and 2025 were included. Diabetes was defined by hemoglobin A1c (HbA1c) ≥6.5% recorded at any point within 1 year prior to surgery. Propensity score matching (1:1) was performed using demographic and clinical covariates. Outcomes included 1-year infection and 1-, 3-, and 5-year structural complications and emergency department (ED) visits. ED visits captured all-cause encounters rather than ankle-specific presentations. The pre-specified primary endpoint was 1-year structural complication; secondary endpoints included infection at 1 year and ED visits and structural complications at 3 and 5 years, with FDR applied to secondary outcomes. Risk estimates, Kaplan-Meier analyses, and Benjamini-Hochberg false discovery rate (FDR) correction were applied.
Results:
After propensity score matching, 255 patients remained in each group. At 1 year, postoperative infection occurred in 5.5% of TAA patients and 9.4% of AA patients; this difference did not meet statistical significance after false discovery rate (FDR) adjustment. ED visits were more common in the AA cohort at 1, 3, and 5 years after FDR correction. Structural complications occurred more frequently in the AA cohort at 1 year (29.8% vs 15.3%; RR 0.51), 3 years (38.8% vs 20.0%; RR 0.52), and 5 years (39.6% vs 21.2%; RR 0.54), and these differences were statistically supported after FDR adjustment.
Conclusion:
In patients with a recorded HbA1c ≥6.5% at any point within the previous year undergoing surgery for end-stage ankle arthritis, TAA demonstrated non-inferior structural complication rates across 1-, 3-, and 5-year follow-up without evidence of increased early infection risk after FDR adjustment.
This is a visual representation of the abstract.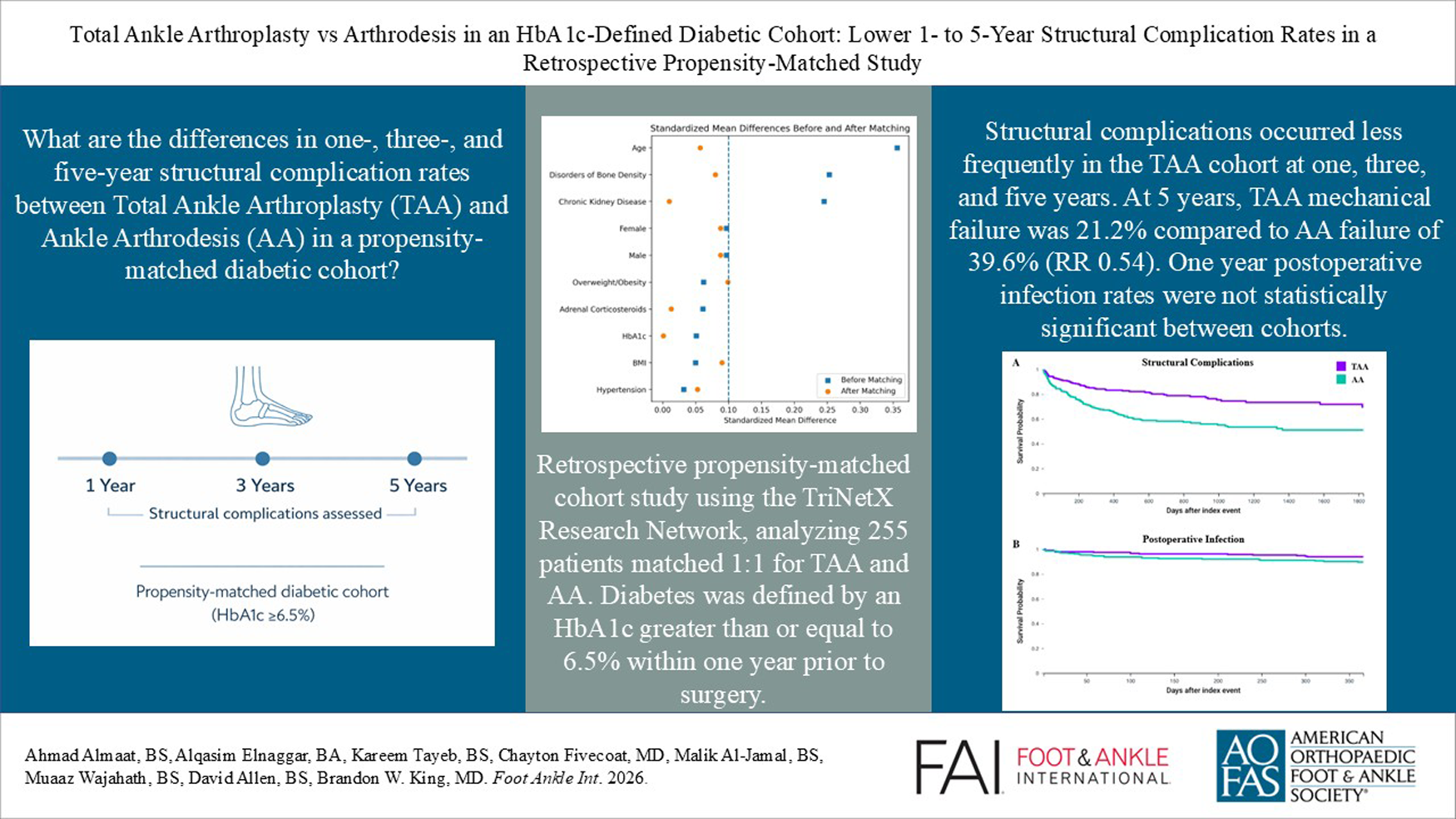
Introduction
End-stage ankle arthritis is a debilitating condition characterized by chronic pain, functional limitation, and reduced quality of life, with a burden comparable to that of end-stage hip arthritis. 1 Etiologies include post-traumatic degeneration, primary osteoarthritis, and inflammatory arthropathies. When nonoperative measures, such as bracing, physical therapy, analgesics, and injections, fail to provide relief, surgical intervention becomes necessary.2,3
Ankle arthrodesis (AA) has long served as a reliable operative option, offering predictable pain relief and durable outcomes, though at the cost of hindfoot and midfoot compensatory motion and a known risk of adjacent joint degeneration over time. In contrast, total ankle arthroplasty (TAA) has emerged as a viable motion-preserving alternative, with contemporary implants demonstrating encouraging survivorship and gait restoration.4 -6 Despite these advances, patients with diabetes remain underrepresented in TAA and AA outcome studies, even though diabetes mellitus is a well-established risk factor for impaired wound healing, infection, and mechanical complications. 7
Prior research suggests that diabetes increases complication rates for both AA and TAA, but findings are fragmented across heterogeneous populations. Large database studies and systematic reviews have noted elevated risks among patients with diabetes, yet few have directly compared TAA and AA within a single, matched diabetic cohort.7 -12 As a result, clinicians lack clear, high-quality evidence to guide procedure selection for this growing and high-risk patient population.
To address this gap, this study compares 1-, 3-, and 5-year outcomes of propensity-matched patients with diabetes undergoing TAA or AA for end-stage ankle arthritis. By examining a broad set of medical and structural complications in a strictly HbA1c-defined diabetic cohort, this work aims to provide meaningful insight into procedure-specific risks to inform surgical decision making.
Methods
We performed a retrospective cohort study using the TriNetX Research Network, which aggregates deidentified electronic health records from more than 100 health-care organizations. Adults aged 18 years or older who underwent total ankle arthroplasty (TAA: Current Procedural Terminology [CPT] 27702) or ankle arthrodesis (AA: CPT 27870 or 29899) between January 1, 2005, and January 1, 2025, were eligible. Diabetes mellitus was defined by documented HbA1c values of 6.5% or higher recorded in TriNetX and obtained within 1 year prior to surgery. The mean HbA1c was 7.1% in the TAA cohort and 7.3% in the AA cohort. No upper HbA1c limit was applied. Patients were required to have a diagnosis of primary or post-traumatic ankle osteoarthritis. Individuals with prior ankle arthroplasty codes and those with any diagnosis of Charcot neuroarthropathy were excluded from both cohorts.
To establish a stable analytic cohort, each patient was required to have at least 1 documented clinical encounter within 6 months following the index procedure, which was defined as the first qualifying surgical date. This 6-month encounter requirement was used only to confirm continued activity within the health system and did not determine follow-up duration for outcome analysis. Once the cohort was formed, TriNetX longitudinally identified all subsequent encounters and diagnosis codes for each patient. Outcomes at 1, 3, and 5 years were evaluated among all individuals with available data at those respective time points.
Outcome Definitions
All outcomes were identified exclusively using International Classification of Diseases, Tenth Revision (ICD-10) and CPT codes within the TriNetX network. Outcomes included infection following procedure at 1 year and emergency department (ED) visits and structural complication at 1, 3, and 5 years. ED utilization was identified using encounter codes that capture all-cause emergency visits within the TriNetX network, rather than ankle-specific or postoperative presentations. Given the medically complex nature of patients with diabetes, these encounters were reported to highlight general health care utilization patterns between these patient cohorts. Structural complication was evaluated as an exploratory composite outcome representing structural compromise that may require further evaluation or intervention. This composite included nonunion-related codes for AA and implant complication or loosening codes for TAA, as well as additional relevant structural complications such as fracture of the medial malleolus, idiopathic aseptic necrosis of the foot or talus, below-knee amputation, tibial or fibular osteotomy, combined tibia and fibula osteotomy, and subtalar arthrodesis. Long-term outcomes at 3 and 5 years included ED visits and structural complications.
Covariates and Matching
Demographic and clinical covariates, including age, sex, race, comorbidities such as chronic kidney disease, hypertension, obesity, disorders of bone density, corticosteroid exposure, body mass index values, and qualifying HbA1c values, were extracted. Ethnicity was not included as a matching covariate due to incomplete coding. Patients with Charcot neuroarthropathy were excluded from both cohorts. To reduce confounding, we performed 1-to-1 propensity score matching using these covariates (Table 1). TriNetX applies greedy nearest-neighbor matching with a fixed caliper of 0.1 on the logit of the propensity score. Covariate balance was assessed using standardized mean differences, with values less than 0.1 considered indicative of adequate balance. Balance was visualized using a Love plot (Figure 1).
Patient Profile Before and After Propensity Score Matching.
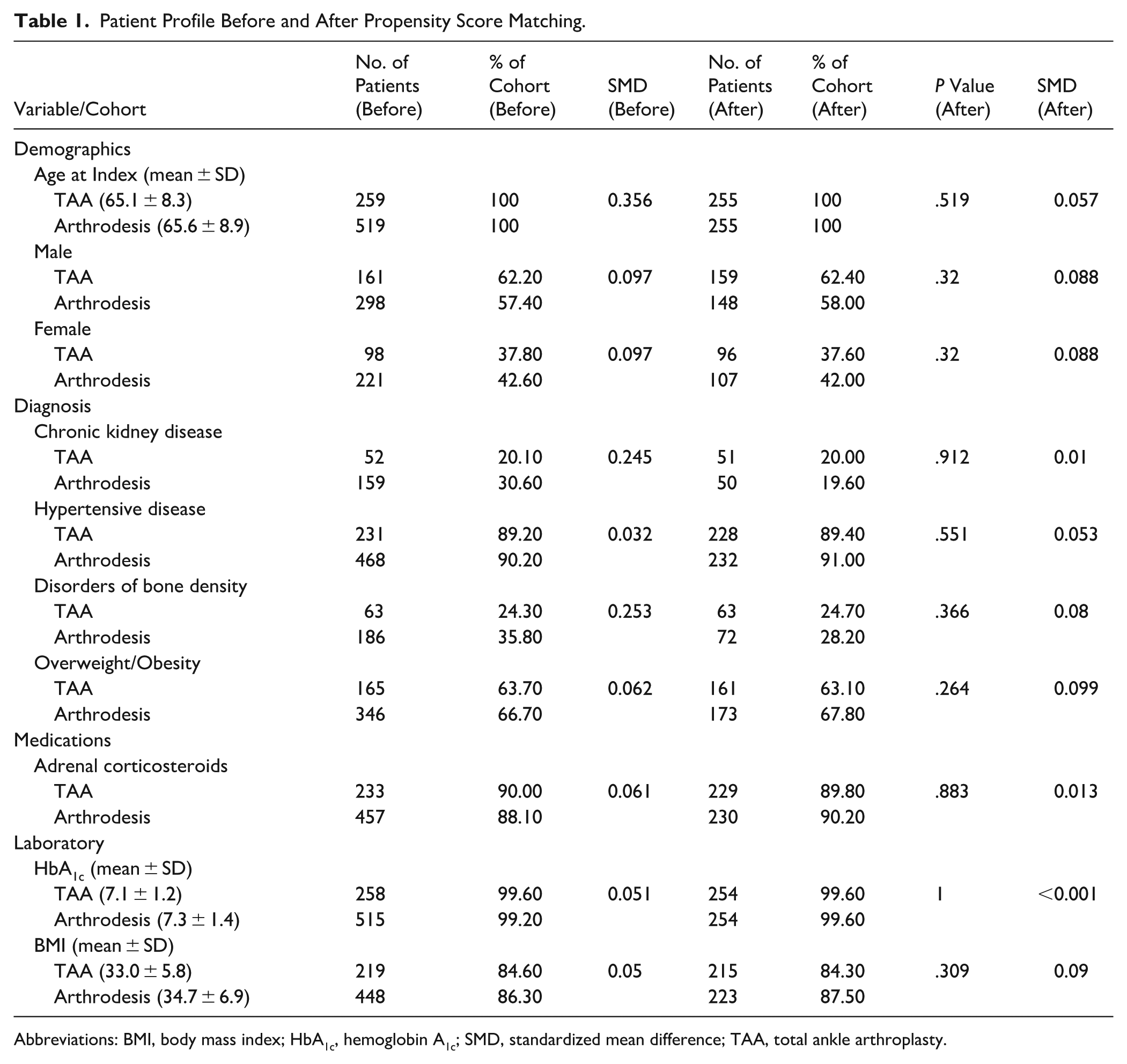
Abbreviations: BMI, body mass index; HbA1c, hemoglobin A1c; SMD, standardized mean difference; TAA, total ankle arthroplasty.
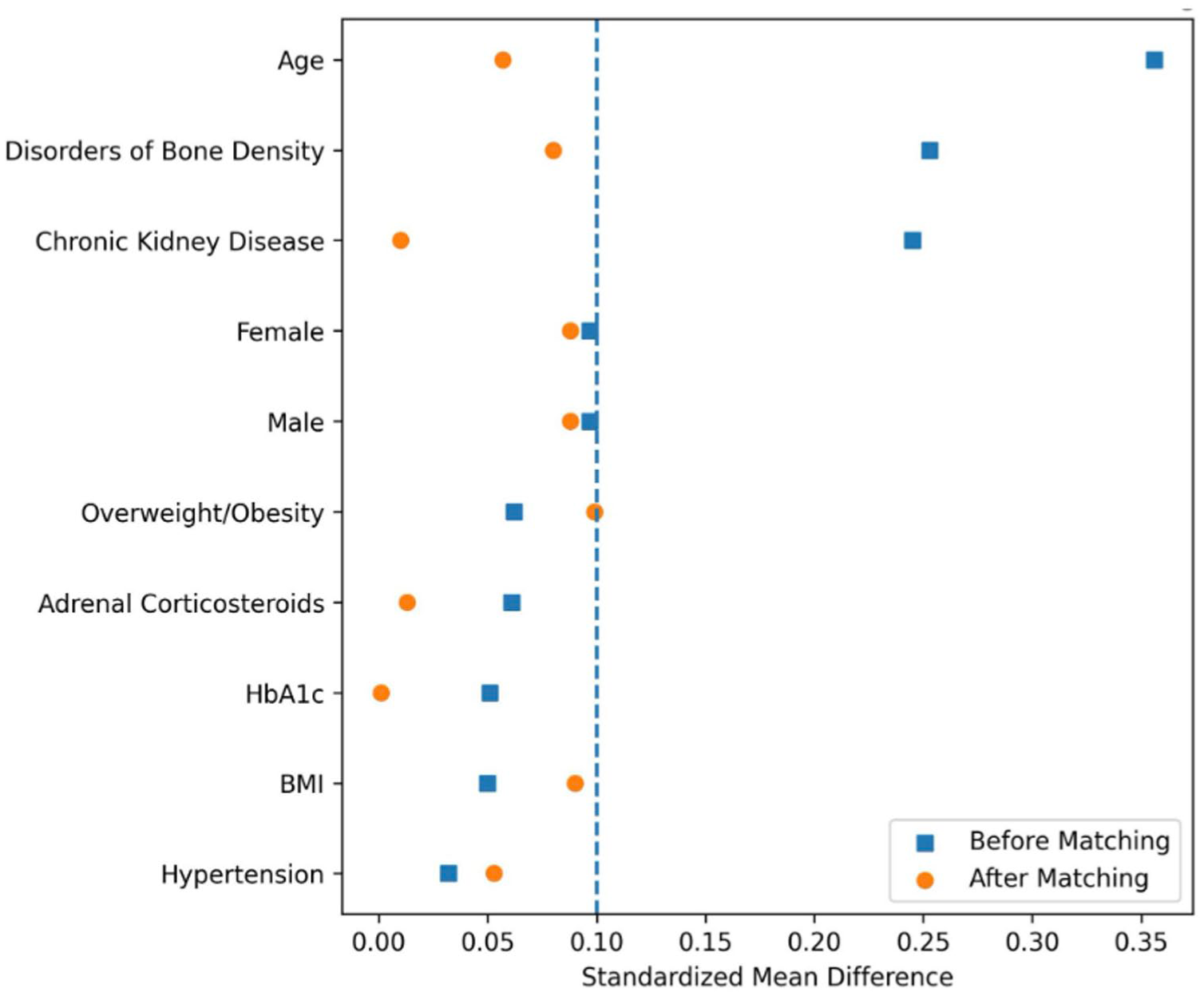
Love plot showing standardized mean differences (SMDs) before and after propensity score matching.
Statistical Analysis
Risk estimates, including risk differences, risk ratios, and 95% CIs, were calculated, and statistical significance was defined as a 2-sided P value less than .05 (Table 2). Kaplan-Meier survival analyses with hazard ratios and absolute event-free survival probabilities were generated for structural complication and infection outcomes (Figure 2, Table 3). Structural complication at 1 year was prespecified as the primary endpoint. Secondary endpoints included infection at 1 year and ED visits at all time points. False discovery rate (FDR) correction was applied to secondary outcomes within each respective time frame using the Benjamini-Hochberg procedure, with Q values less than 0.05 considered statistically supported (after correction). All diagnostic and procedural codes used in this study are listed in Supplementary Table 1.
One-, 3-, and 5-Year Postoperative Medical and Structural Complications. a
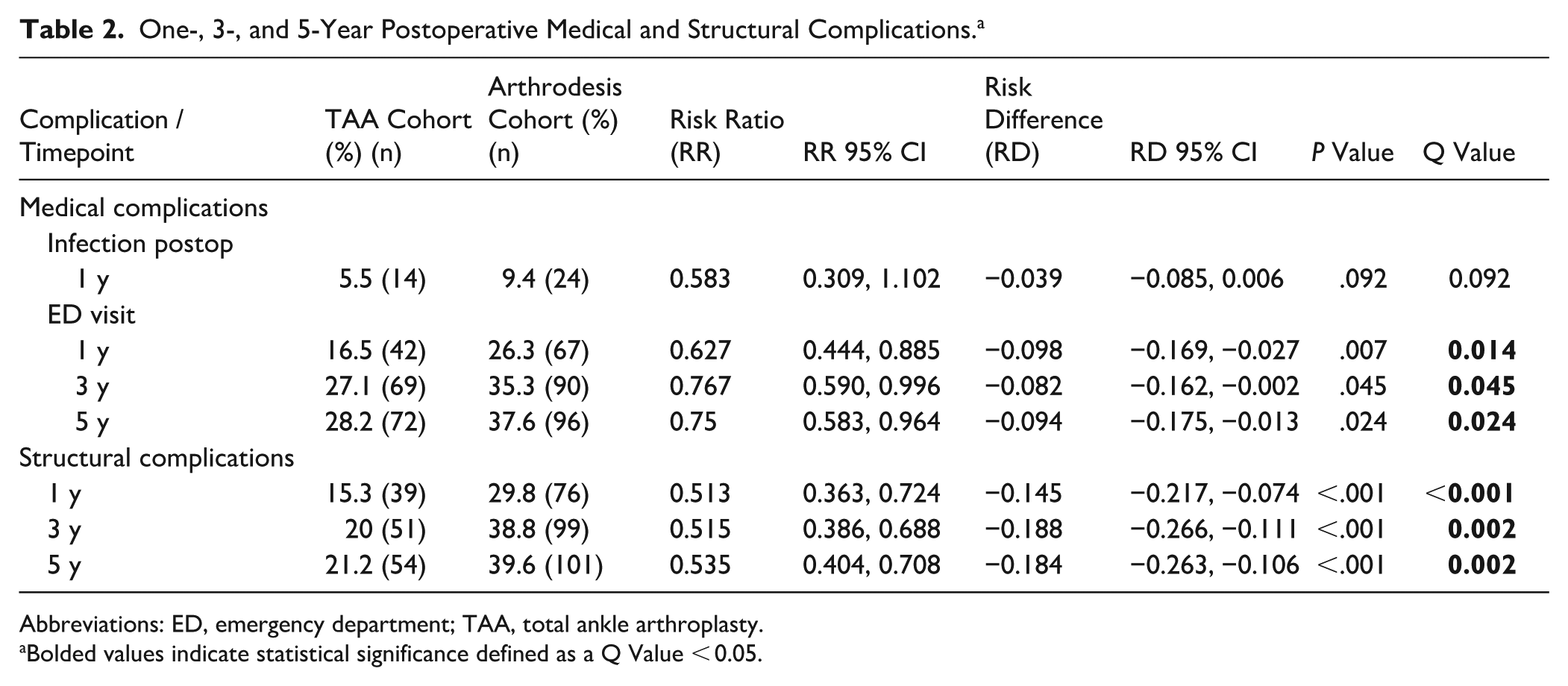
Abbreviations: ED, emergency department; TAA, total ankle arthroplasty.
Bolded values indicate statistical significance defined as a Q Value < 0.05.
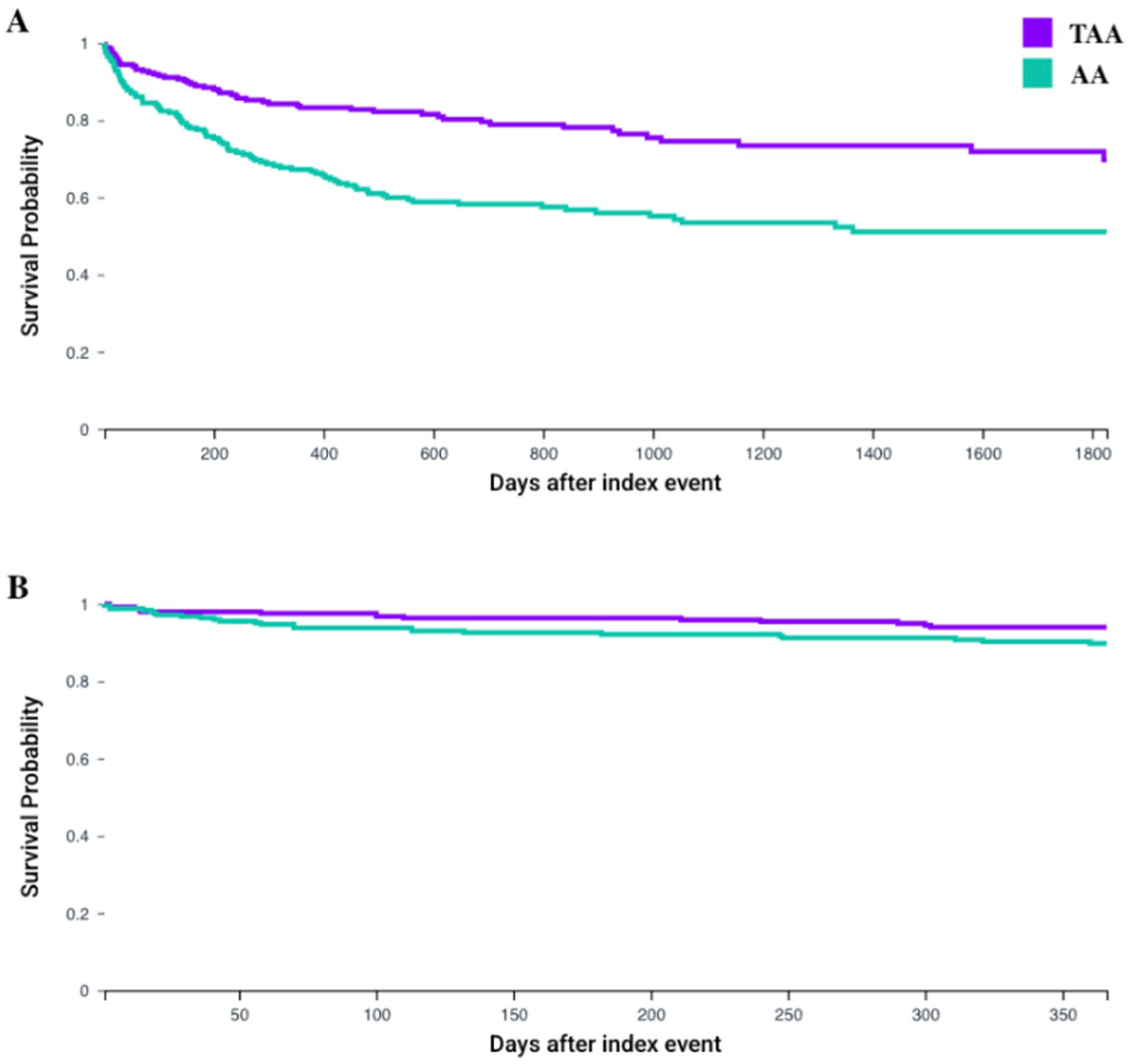
Kaplan-Meier curves comparing (A) mechanical failure-free survival through 5 years and (B) infection-free survival through 1 year between total ankle arthroplasty (TAA) and ankle arthrodesis (AA) cohorts. Absolute event-free survival probabilities at 1, 3, and 5 years are reported in Table 3.
Kaplan-Meier Analysis for 1-, 3-, and 5-Year Postoperative Medical and Mechanical Complications.
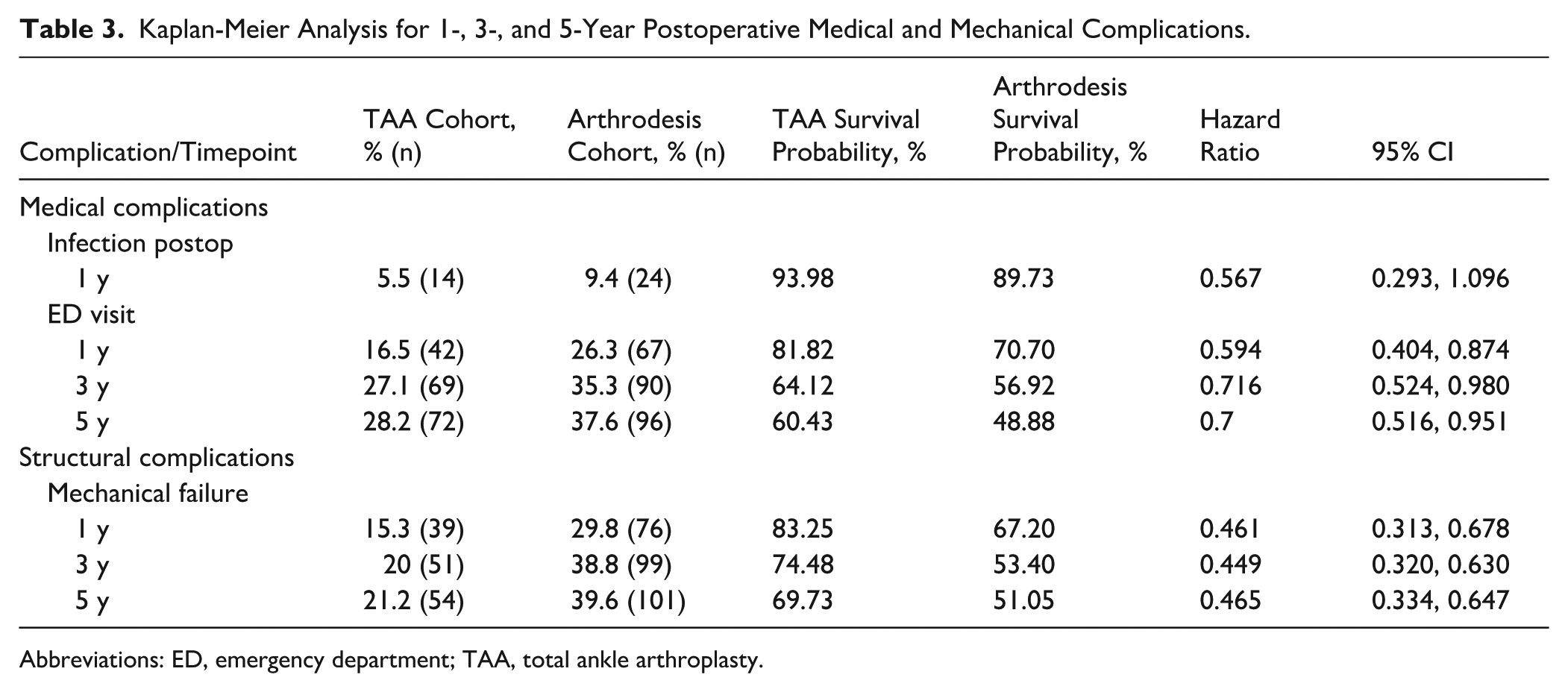
Abbreviations: ED, emergency department; TAA, total ankle arthroplasty.
Results
One-Year Outcomes
After propensity-score matching, 255 patients remained in each cohort (Table 1). At 1 year, postoperative infection occurred in 5.5% of TAA patients and 9.4% of AA patients (RR 0.58, 95% CI 0.31-1.10; P = .092; Q = .092). Kaplan-Meier analysis demonstrated higher infection-free survival following TAA compared with AA (93.98% vs 89.73%), although the difference did not meet statistical significance after FDR adjustment (Figure 2, Table 3). ED utilization was more frequent in the AA cohort at 1 year (26.3% vs 16.5%; RR 0.63, 95% CI 0.44-0.89; Q = .014).
Structural complications occurred in 15.3% of TAA patients and 29.8% of AA patients at 1 year (RR 0.51, 95% CI 0.36-0.72; P < 0.001; Q < 0.001). Kaplan-Meier estimates showed higher structural complication–free survival in the TAA cohort (83.25% vs 67.20%), with a significantly lower hazard of structural complication compared with AA (HR 0.46, 95% CI 0.31-0.68) (Figure 2, Tables 2 and 3).
Three-Year Outcomes
By 3 years, ED visits occurred in 27.1% of TAA patients and 35.3% of AA patients (RR 0.77, 95% CI 0.59-1.00; P = .045; Q = .045). Kaplan-Meier analysis demonstrated higher ED visit-free survival in the TAA cohort compared with AA (64.12% vs 56.92%), with a lower hazard of ED visits following TAA (HR 0.72, 95% CI 0.52-0.98) (Tables 2 and 3).
Structural complications occurred in 20.0% of TAA patients and 38.8% of AA patients at 3 years (RR 0.52, 95% CI 0.39-0.69; P < 0.001; Q = .002). Structural complication-free survival was higher following TAA compared with AA (74.48% vs 53.40%), and the hazard of structural complication was significantly lower in the TAA cohort (HR 0.45, 95% CI 0.32-0.63) (Figure 2, Tables 2 and 3).
Five-Year Outcomes
By 5 years, ED utilization occurred in 28.2% of TAA patients and 37.6% of AA patients (RR 0.75, 95% CI 0.58-0.96; P = .024; Q = .024). Kaplan-Meier analysis demonstrated higher ED visit-free survival following TAA compared with AA (60.43% vs 48.88%), with a lower hazard of ED utilization in the TAA cohort (HR 0.70, 95% CI 0.52-0.95) (Tables 2 and 3).
Structural complications occurred in 21.2% of TAA patients and 39.6% of AA patients at 5 years (RR 0.54, 95% CI 0.40-0.71; P < 0.001; Q = .002). Structural complication-free survival remained higher in the TAA cohort compared with AA (69.73% vs 51.05%), and the hazard of structural complication was significantly lower following TAA (HR 0.47, 95% CI 0.33-0.65) (Figure 2, Tables 2 and 3).
Primary Endpoint and False Discovery Rate Correction
The primary endpoint, 1-year structural complication, was significantly lower following TAA, a finding supported by Kaplan-Meier survival analysis demonstrating a reduced hazard of structural complication (HR 0.46, 95% CI 0.31-0.68). After Benjamini-Hochberg false discovery rate correction, structural complication remained statistically significant at 1, 3, and 5 years (all Q < 0.01). ED utilization also remained significantly lower in the TAA cohort at 1, 3, and 5 years after correction, whereas 1-year postoperative infection did not remain statistically significant following FDR adjustment (Table 2).
Discussion
In this propensity-matched cohort of 510 patients with diabetes undergoing surgical treatment for end-stage ankle arthritis, several key findings emerged. First, AA was associated with higher rates of structural complications at 1, 3, and 5 years compared with TAA. These differences persisted after FDR adjustment and were consistent across absolute event rates and survival analyses. Second, although postoperative infection at 1 year was numerically higher in the AA cohort, this difference did not meet statistical significance after adjustment. Third, ED utilization was more frequent after AA at 1, 3, and 5 years and remained lower after TAA when considering all-cause ED encounters. Collectively, these findings suggest that TAA may offer non-inferior structural durability in patients with diabetes without evidence of increased early infectious complications.
The higher composite structural complication rate observed after AA is supported by the clinical plausibility of the outcome definition and by the biological demands of the procedure in patients with diabetes. The composite was structured to capture meaningful structural compromise across both procedures, incorporating nonunion-related diagnoses for AA and implant-related or loosening diagnoses for TAA, as well as shared complications such as medial malleolar fracture, osteonecrosis of the foot or talus, subtalar arthrodesis, tibial or fibular osteotomy, combined tibia and fibula osteotomy, and below-knee amputation. These events represent clinically relevant situations in which the operated ankle required further evaluation or intervention because of compromised structural integrity. AA depends on achieving successful bony fusion, and patients with diabetes are at increased risk for delayed union or nonunion, which directly contributes to several components of this composite.9,13 -15 In contrast, TAA can suffer implant-related complications that also contribute to several components of this composite. Within this context, TAA demonstrated lower structural complication rates at every time point.
The present analysis, which identified diabetes using HbA1c values of 6.5% or higher obtained at any point within the year prior to surgery, did not demonstrate a statistically significant difference in 1-year infection after false discovery rate correction; however, the higher numerical infection rate observed in the arthrodesis cohort is consistent with prior literature comparing infection risks between arthrodesis and arthroplasty. 16 The mean HbA1c values in our cohort (7.1% for TAA and 7.3% for AA) reflect laboratory values documented within the year prior to surgery and were used solely to identify diabetic status for study inclusion. Importantly, these values do not necessarily represent perioperative glycemic control. Therefore, although our findings do not suggest increased early infection risk with TAA within this HbA1c range and may suggest structural non-inferiority, they should be interpreted with caution and not be generalized to patients with substantially higher or uncontrolled glycemic levels perioperatively, who remain at elevated risk in prior literature.17 -19
From a clinical standpoint, these results challenge the historical tendency to favor AA in patients with diabetes out of concern for wound complications or infection following arthroplasty. Rather than demonstrating a safety advantage for AA, our data show that TAA was associated with non-inferior structural complication rates across all time points, with infection outcomes statistically comparable after false discovery correction. Motion preservation with TAA may also support more physiologic gait patterns, although the current study did not include functional or patient-reported outcomes. By helping maintain ankle motion and the ability to engage in physical activity, TAA may also support certain diabetes management goals outlined by the American Diabetes Association, including improving insulin sensitivity and reducing cardiovascular risk. 20 Conversely, salvage of a failed TAA through conversion to fusion, particularly when bone-block arthrodesis is required, carries substantial risk in patients with diabetes and remains an important factor influencing surgeon decision making despite the structural advantages observed with primary TAA.21,22 These observations support an individualized approach to procedure selection in patients with diabetes, taking into account expected structural durability, comorbidity optimization, and patient-specific functional priorities.
This study has several limitations. Its retrospective design and reliance on administrative coding introduce the possibility of misclassification, underreporting, and limited granularity regarding the severity or symptomatic relevance of complications. All outcomes were identified through ICD and CPT codes, without radiographic verification of nonunion, implant loosening, or deformity progression. Although propensity score matching improved covariate balance, residual confounding from unmeasured variables such as implant type, operative burden, prior infection history, or surgeon experience is possible. Diabetes was also defined strictly by a recorded HbA1c value ≥6.5% at any point within the prior year, which excludes diabetic patients with lower HbA1c values throughout that window who were medically managed, potentially limiting generalizability to all diabetic populations. Finally, ED visits represent all-cause encounters rather than ankle-specific presentations; these data should be interpreted as markers of overall health care utilization in patients with diabetes. While these findings suggest that TAA may be structurally non-inferior compared to AA in patients with diabetes, the results should be interpreted only as hypothesis-generating. Prospective studies with standardized radiographic assessment, functional outcome measures, and extended follow-up are needed to validate these observations and guide optimal surgical decision making in this high-risk population.
Conclusion
In this propensity-matched analysis of patients with diabetes undergoing surgery for end-stage ankle arthritis, total ankle arthroplasty was associated with consistently lower rates of structural complications at 1, 3, and 5 years compared with ankle arthrodesis. One-year infection rates were statistically comparable after false discovery rate correction. ED utilization was more frequent after arthrodesis when considering all-cause ED encounters. These findings suggest that total ankle arthroplasty may be structurally non-inferior compared to ankle arthrodesis for patients with diabetes without evidence of increased short-term infectious risk. As these findings are primarily hypothesis generating and should be interpreted with caution, prospective studies with radiographic assessment, detailed functional outcomes, and extended follow-up are warranted to validate these results and guide optimal surgical decision making in this high-risk population.
Supplemental Material
sj-docx-2-fai-10.1177_10711007261419131 – Supplemental material for Total Ankle Arthroplasty vs Arthrodesis in an HbA1c-Defined Diabetic Cohort: Lower 1- to 5-Year Structural Complication Rates in a Retrospective Propensity-Matched Study
Supplemental material, sj-docx-2-fai-10.1177_10711007261419131 for Total Ankle Arthroplasty vs Arthrodesis in an HbA1c-Defined Diabetic Cohort: Lower 1- to 5-Year Structural Complication Rates in a Retrospective Propensity-Matched Study by Ahmad Almaat, Alqasim Elnaggar, Kareem Tayeb, Chayton Fivecoat, Malik Al-Jamal, Muaaz Wajahath, David Allen and Brandon W. King in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_10711007261419131 – Supplemental material for Total Ankle Arthroplasty vs Arthrodesis in an HbA1c-Defined Diabetic Cohort: Lower 1- to 5-Year Structural Complication Rates in a Retrospective Propensity-Matched Study
Supplemental material, sj-pdf-1-fai-10.1177_10711007261419131 for Total Ankle Arthroplasty vs Arthrodesis in an HbA1c-Defined Diabetic Cohort: Lower 1- to 5-Year Structural Complication Rates in a Retrospective Propensity-Matched Study by Ahmad Almaat, Alqasim Elnaggar, Kareem Tayeb, Chayton Fivecoat, Malik Al-Jamal, Muaaz Wajahath, David Allen and Brandon W. King in Foot & Ankle International
Footnotes
Ethical Considerations
The authors take responsibility for every aspect of the work, ensuring its accuracy and integrity. This study used deidentified data from the TriNetX database and was exempt from Institutional Review Board approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Brandon W. King, MD, reports general disclosures of Stryker Consultant since March 1, 2025, not directly related to this manuscript. Disclosure forms for all authors are available online.
Data Availability Statement
Data were obtained from the TriNetX Research Network, which provides deidentified patient information under licensing agreements and is not publicly available.
Supplemental Material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.