
Abstract
Knee pain in older adults significantly reduces their physical function and quality of life. While lower-limb exercises are effective for treating this health issue, individuals’ access to supervised programs is often limited. To address this, our research team developed a machine learning-based lower-limb exercise system that offers video demonstrations of exercises, provides real-time movement feedback, and tracks performance and progress. Initial evaluation of the system revealed usability barriers. Consequently, we applied human factors principles to improve the system design and subsequently evaluated the usability and acceptance of the enhanced system. Ten adults (aged 60–73) with knee pain used the system to perform lower-limb exercises. Their opinions on usability and acceptance were gathered. We found that the enhanced system was perceived as both usable and acceptable. These findings underscore the necessity of integrating human factors principles into the design of such digital health applications, as this approach allows developers to create intuitive user interfaces that align with users’ preferences and expectations.
Introduction
Knee pain is a prevalent health problem among older adults worldwide. Physical exercise is a recommended non-pharmacological treatment (Porcheret et al., 2007). Challenges with access and cost of therapist-led exercise programs have led to the use of digital technologies for remote exercise training. However, many digital programs lack real-time supervision and progress tracking, which is crucial for effective knee health management.
Our research team developed a machine learning-based lower-limb exercise training system for older adults with knee pain (Chen et al., 2024; Chen & Or, 2021, 2023). The system offers video demonstrations of exercises, provides real-time posture analysis and feedback based on machine learning techniques, and tracks performance and progress. In a 3-week implementation study (Or et al., 2024), 60 participants used the system to perform lower-limb exercise training. During this period we identified usability issues through direct observation and participants’ responses. Usability issues can hinder user acceptance and potentially diminish a system’s benefits. It is essential to address these issues before promoting the wide adoption of a system in the community. Based on the authors’ prior research methodology (Chen et al., 2025; Liu et al., 2022, 2023; Or et al., 2014; Tao & Or, 2012), usability and acceptance evaluations were implemented in this study. Also, human factors principles were applied to enhance system design (Nielsen, 1994a, 1994b; Or & Chan, 2024; Or et al., 2022).
Therefore, this study aimed to (1) summarize the usability issues in our lower-limb exercise training system, then apply human factors principles to enhance its design; and (2) assess the usability and user acceptance of the enhanced system among aging individuals with knee pain. Based on the findings, we briefly compared the enhanced version of the system with the earlier version. We also discussed the study limitations and implications for future research.
Enhanced System Design
We implemented our system on a computer equipped with a camera and the necessary peripherals (e.g., monitor, mouse, keyboard). The lower-limb exercise training system guides users through video demonstrations. Throughout the exercise session, the camera captures the users’ exercise movements. These movements are analyzed by machine learning-based pose estimation techniques. The system provides real-time feedback to inform users about incorrect postures and movements. After the exercise session, users can check their exercise duration and performance in a training log. For further technical details, see our previous articles (Chen & Or, 2021; Or et al., 2024).
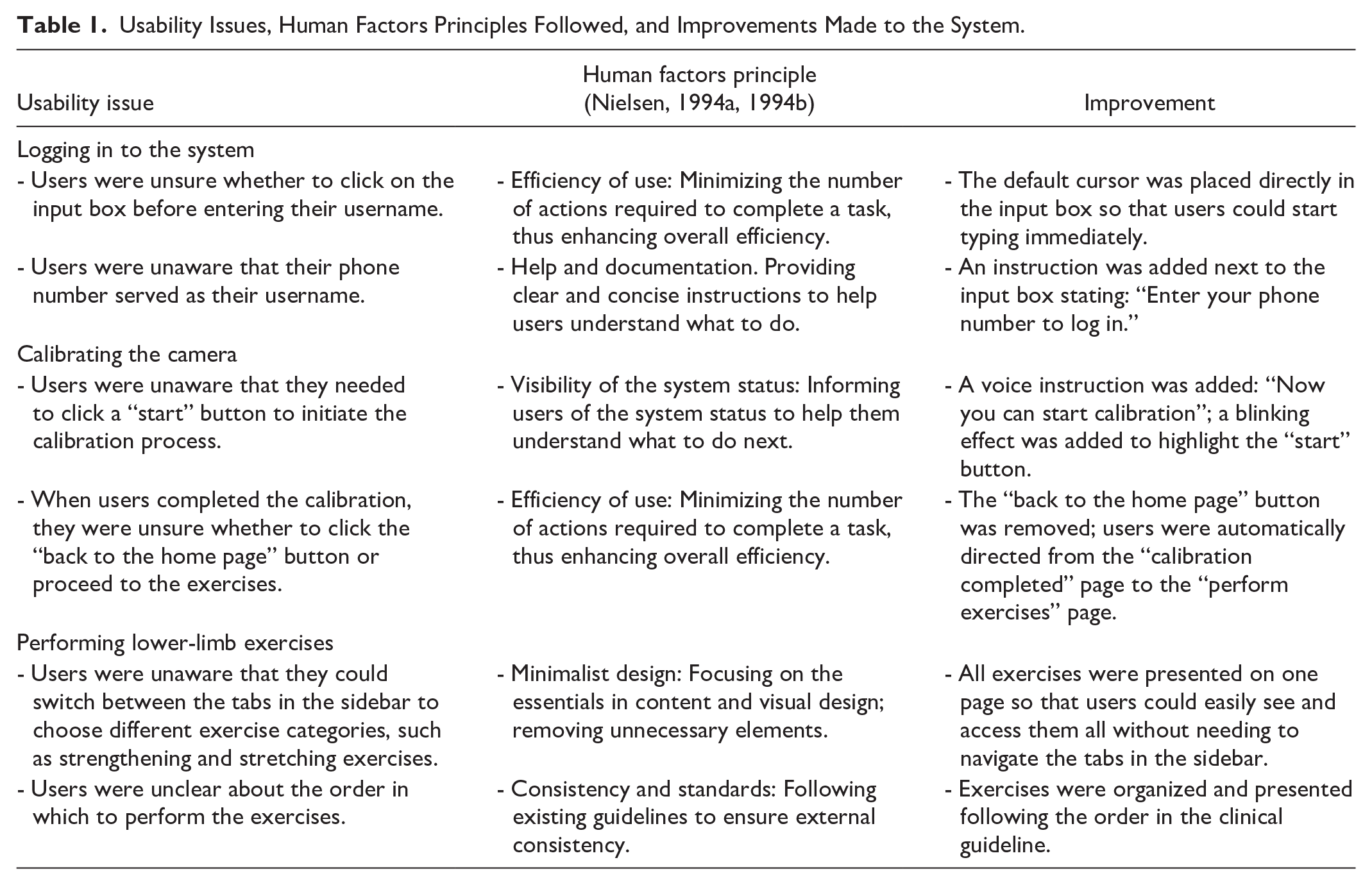
While implementing the preliminary version of the system (Or et al., 2024), we observed usability issues when the participants logged in to the system, calibrated the camera, and performed exercises. For each usability issue, we followed human factors principles (Nielsen, 1994a, 1994b) to improve the system design (Table 1). Figure 1 illustrates our enhanced system.
Usability Issues, Human Factors Principles Followed, and Improvements Made to the System.
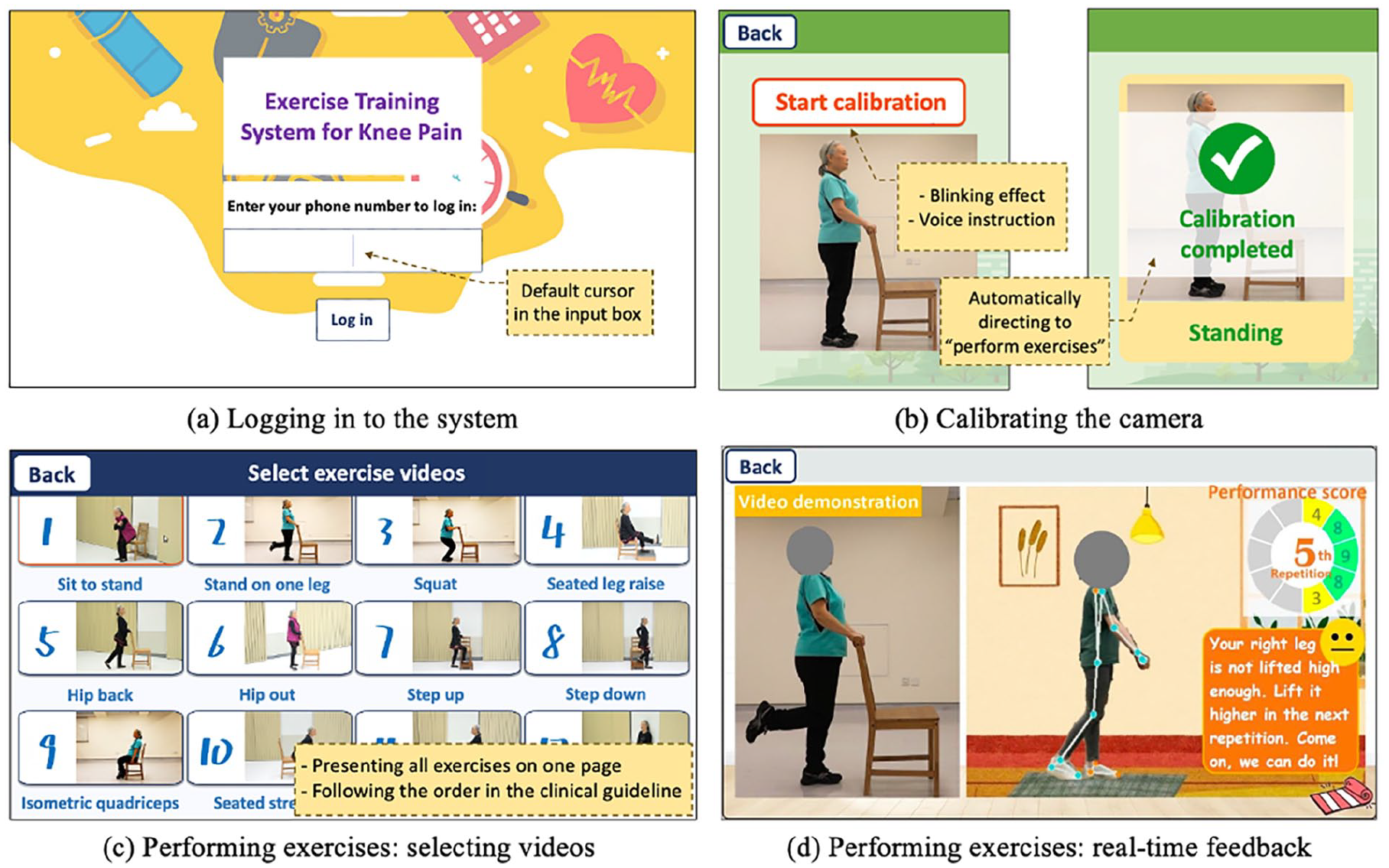
Demonstration of the enhanced system.
Methods
Study Design and Participants
Ten individuals with knee pain tested our enhanced system during a 45-minute session of lower-limb exercise training in our study laboratory. After a brief introduction to the system’s features, the participants were asked to explore the system independently and freely. During this period, no detailed instructions were provided. The participants (i) were aged 55 years or over, (ii) self-reported experiencing knee pain for at least one month during the previous 12 months, (iii) were able to speak and read Chinese, and (iv) were able to provide written informed consent. Exclusion criteria included having inflammatory arthritis, having a knee injury within the previous 6 months, having a history of knee replacement surgery, waiting for knee surgery, having physical therapy for knee problems within the previous 3 months, and being unable to participate in exercise training due to physical impairment or medical comorbidities. To ensure unbiased evaluation, we selected different participants from those who participated in our previous studies.
Outcomes
We assessed the usability and user acceptance of the enhanced system using questionnaires. We assessed usability using the 10-item System Usability Scale (SUS) (Brooke, 1996). The participants rated each item on a 5-point Likert scale, from 1 (strongly disagree) to 5 (strongly agree). The raw scores were converted to a standardized SUS score (possible range: 0 to 100), with higher scores indicating better usability. We assessed user acceptance across four dimensions adapted from previous studies (Chen et al., 2022; Davis, 1989; Or & Karsh, 2006; Xie & Or, 2020). These dimensions were: perceived usefulness (four items), perceived ease of use (four items), attitude toward the system (three items), and behavioral intention to use the system (two items). The participants rated each item on a seven-point Likert scale, ranging from 1 (very strongly disagree) to 7 (very strongly agree), with higher scores indicating better acceptance.
Procedures
Eligible participants visited our laboratory, where a research assistant introduced the study details, obtained written informed consent, and collected demographic and clinical information using a questionnaire. The participants then used the enhanced system to perform lower-limb exercises for 45 minutes. Afterward, they completed a questionnaire to indicate their opinions on the system’s usability and acceptance for managing knee pain. Each participant received a HK$150 incentive after the experiment.
Statistical Analysis
Descriptive statistics were calculated for the sample characteristics, and for the usability and user acceptance scores of the enhanced system.
Results
Sample Characteristics
The participants comprised seven females and three males, aged 60 to 73 years (mean = 66.1 years, standard deviation [SD] = 4.1). Nine participants reported experiencing knee pain for at least three months within the previous 12 months. Knee pain intensity over the previous 12 months, measured on an 11-point scale (0 = no pain, 10 = worst possible pain), had a mean score of 4.9 (SD = 1.9) across all participants.
Usability of the Enhanced System
The enhanced system achieved a mean SUS score of 78.5 out of 100 (SD = 7.19, 95% confidence interval [CI]: [73.4, 83.6], range: 70 to 90, median = 76.3). All of the participants’ SUS scores exceeded 68, indicating above-average usability (Brooke, 2013). According to adjective ratings by Bangor et al. (2009), the mean SUS score of 78.5 fell between “Good” (score: 71.4) and “Excellent” (score: 85.5). Notably, all but one participant scored above the “Good” threshold.
User Acceptance of the Enhanced System
The participants expressed positive opinions across all of the four acceptance aspects (Table 2).
Descriptive Statistics of User Acceptance.

Discussion
This study demonstrated the positive impact of applying human factors principles to the design of human–computer systems, exemplified by a machine learning-based lower-limb exercise training system. Aging individuals with knee pain perceived the enhanced system to be both usable and acceptable.
Before this study, we developed and implemented a preliminary version of the system (Or et al., 2024), and assessed its usability and acceptance using the same questionnaire as was used in this study. Compared with the preliminary version, the enhanced system used in this study achieved higher mean scores for both usability and perceived ease of use. These improvements can be attributed to design modifications that addressed specific usability issues, particularly the clarity of instructions and ease of navigation. For instance, clear instructions helped the participants understand the system status and how to interact with its features effectively. Additionally, the use of blinking effects made the buttons visually distinct, enabling the participants to focus on the essential elements and use the system as intended. Moreover, reducing unnecessary clicks simplified system operation. This was particularly beneficial for users with limited computer skills or those unfamiliar with the system.
However, the mean scores for other aspects of user acceptance (perceived usefulness, attitude, and behavioral intention) did not surpass those of the preliminary version of the system. One potential explanation for this is the ceiling effect, as these aspects had already achieved high scores (over 5.6 out of 7 points), leaving limited scope for further improvement. Another contributing factor could be that the design enhancements focused on addressing usability issues to improve ease of use, with less attention on other aspects of user acceptance. Future improvements should expand the design focus to create a system that is not only easy to use but also highly useful, fosters positive attitudes, and encourages a strong intention to use it.
This study has several limitations. First, the sample size was relatively small, which limits the generalizability of the findings regarding the system’s usability and user acceptance. Future studies should include larger samples to confirm these results. Second, we did not conduct direct pre–post comparisons of usability and user acceptance between the different versions of the system as different participant cohorts were involved in the earlier and later studies.
Our study has implications that suggest directions for future research. First, whereas we assessed system usability using subjective measures, future research could benefit from incorporating objective measures. Examples of objective measures include eye-tracking data or task completion time for deeper insights into the identification of usability issues than this study (Wang & Or, 2020). Second, as perceptions may change, a longitudinal study is needed to evaluate whether the system’s usability and acceptance persist over time. Third, beyond usability and user acceptance, future research should explore the health benefits of the enhanced system.
Conclusions
This study assessed the usability of the enhanced design of a machine learning-based lower-limb exercise training system and proposed design enhancements. End users expressed positive feedback on the usability and acceptance of the enhanced system. These findings underscore the importance of applying human factors principles to improve system design. If users perceive the system developed in this study as easy to use, they may be more willing to engage in exercise training that benefits their knee health. The implications of this work extend beyond individual exercise programs. A human-centered approach throughout the design, development, implementation, and improvement enables the creation of systems that meet the needs of end users. Future research should apply human factors principles to promote the development of usable and accessible healthcare innovations for vulnerable populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partly supported by a General Research Fund grant from the Hong Kong Research Grants Council (Project No. 17200323).