
Abstract
It is the researcher's responsibility to provide accurate, complete, and unbiased verbal and written information yet, as this essay discusses, challenges to meaningful research consent abound in the communication between researcher and subject. This discussion of these challenges is far from exhaustive, but it will flag some of the potholes that researchers must anticipate on the sometimes rocky road to eliciting meaningful consent. These include, but are not limited to, inadequate scientific literacy, poorly written consent forms, and even the deployment of scientific terms and seductive acronyms like CURE and MIRACL. Studies with acronyms, for example, enroll five times as many patients as those without, are more likely to be published by prestigious journals, and have higher Jadad methodologic quality scores although they are no more likely to conclude with positive findings. Other barriers to researcher-subject communication include: widely differing beliefs and customs, semiotics, socioeconomic status, iatrophobia, and dramatically different histories of treatment in the medical-research arena.
The Code of Federal Regulations is unambiguous in regard to providing research subjects the information that provides the underpinning of informed consent: “The information that is given to the subject or the representative shall be in language understandable to the subject or the representative.” 1
This is a straightforward requirement, but not an easy one. To risk belaboring the obvious, it is also the dialogue, not the signed document alone, that provides the basis for informed consent. 2 It is the researcher's responsibility to provide accurate, complete, and unbiased verbal and written information yet, as this essay discusses, challenges to meaningful research consent abound in the communication between researcher and subject. This discussion of these challenges is far from exhaustive, but it will flag some of the potholes that researchers must anticipate on the sometimes rocky road to eliciting meaningful consent.
These hazards include unfamiliar scientific terms and connotations, divergent conceptions of medical history and science, the conscious and unconscious deploying of rosy adjectives with which scientists sometimes “sell” a study in lieu of describing it, semi-otics that magnify the therapeutic illusion, and legal maneuvers that bypass consent altogether. Even the deceptively optimistic acronyms by which many medications and clinical trials are known — LIVE, CURE or MIRACL, anyone? — present semantic pitfalls that undermine objectivity, impede communication, and distort the appropriateness of and expectations of medical research.
It is the researcher's duty to bridge the gap in order to effect informed consent, or indeed, any meaningful species of consent. The typical US researcher is fluent in English and hyper fluent in medical jargon; however, many agree that the average subject reads English at an eighth-grade level and is quite innocent of medical argot. 3
Researcher-subject perspectives on medical research are also likely to differ accordingly. The researcher and the subject often share a broad culture, as evinced by their common language, nationality, and geographical locus. But within this larger overarching culture, parties to this research dyad also tend to possess distinct cultural identities that differ widely in religious beliefs and customs, native tongue or patois, familiarity with scientific terms, ethnicity, socioeconomic status, and a dramatically different history of treatment in the medical-research arena.
Even subjects and researchers who share a mother tongue tend to speak different medical languages. For example, a 2000 study of rural African Americans found that “31% of subjects who answered “yes” to whether they had “sugar” at the screening had answered “no” to the survey question about diabetes. Subjects who believed they had “sugar” felt their condition was less serious and had higher glucose levels than those who said they had diabetes.” 4
Clinicians may unintentionally sow seeds of misunderstanding well before the informed-consent process begins. Especially when they are delivered by the patient's physician rather than a study researcher, the earliest discussions about the purpose of a trial, which predate the formal informed-consent process, may easily raise expectations or imply promises of treatment outcomes — promises that cannot be delivered in a research setting. When the personal physician tells her patient, “We have another option: a drug that I think can help you: come in and we'll discuss getting you into the trial,” the oft-blurred line between research and treatment may be hopelessly effaced as unrealistic expectations are conveyed.
Clinicians may unintentionally sow seeds of misunderstanding well before the informed-consent process begins. Especially when they are delivered by the patient's physician rather than a study researcher, the earliest discussions about the purpose of a trial, which predate the formal informed-consent process, may easily raise expectations or imply promises of treatment outcomes — promises that cannot be delivered in a research setting. When the personal physician tells her patient, “We have another option: a drug that I think can help you: come in and we'll discuss getting you into the trial,” the oft-blurred line between research and treatment may be hopelessly effaced as unrealistic expectations are conveyed.
Subject Literacy
The 1998 article “Patient Literacy, a Barrier to Quality of Care,” 5 established that adults tend to read three to five grades lower than the highest grade they finish, so that potential research subjects who are high-school graduates should be presented with consent forms written at about an eighth-grade reading level. 6 Subsequent studies have not materially challenged this finding. Yet other investigations consistently demonstrate that the language in such documents fails readability scores and is sometime so impenetrable that scientists themselves are unable to understand them.
In fact, Randy K. Otto and James Ogloff found that consent forms directed at adults contemplating medical research boast 16th-grade readability levels, 7 which would preclude the participation of anyone who is not a candidate for a master's degree or higher, given the finding that adults read as many as five grades below their highest completed grade. Moreover, the excessive length of many informed-consent forms militates against their being completely read and understood by potential subjects. 8
Not only are consent forms complex and lengthy, they are rife with medical jargon. Jargon is useful shorthand for research scientists that allows them to discuss complex topics elegantly and succinctly, but jargon does more than include scientists: it also excludes the lay public, the pool from which most subjects are drawn. In so doing, it operates against the ubiquitous goal of informing the subject before procuring his consent.
Many researchers turn to tools to ensure the readability of their documents, but a Southern Illinois University assessment of randomly selected consent forms discovered that when these forms were analyzed in accordance with the Flesch Reading Ease, Flesch-Kincaid Grade Level, Coleman-Liau Grade Level, and the Bormuth Grade Level, each exceeded the (approximately eighth-grade) reading level of the general population. 9
Researchers also turn to readability formulae that ease readability assessments by automating the features of document analysis, not always realizing that an overreliance on such formulae, which assess the number of words per sentence, the number of syllables per word, and that rely upon word-difficulty lists, is an error. Unfamiliar short terms and words, such as “os,” or “b.i.d.” can be as just as difficult to understand as longer ones, with the added difficulty of providing fewer recognizable clues from Latin or Greek root words. Moreover, although some such formulae are very easy to use, they have limitations: The Fry Readability Graph is accurate to 12th grade level, but the Flesch Readability Formula, for example, is reliable only up to the seventh-grade level — below the recommended eighth-grade level for consent forms. 10
Semantic Masks and Semiotics
Some other intelligibility failings are due to technical terminology, like randomization, that diverges from common and colloquial definitions. Drug nomenclature adds to the confusion: only 53 percent of people in a New Jersey IRB survey recognized acetaminophen as the active ingredient in Tylenol and other common OTC painkillers. 11 Scarcely 15 years after the banning of the infamous German teratogen Thalidomide from the market, tests of it and its analogues under unfamiliar names such as Synovir and lenalidomide shrouded the drug's identity in clinical studies against myeloma and leprosy in Europe and the developing world. 12 It has not helped that until 1979, West African promotional materials still described thalidomide as “completely harmless,” adding to the iatrogenic confusion.
Not all communication hurdles are verbal. The very act of signing a consent form sometimes causes participants to believe that they have signed away or waived their rights and so have no recourse if they are misled or harmed by the research study. 13 A dramatic instance of this phenomenon was recounted in the volume Acres of Skin: Human Experiments at Holmesburg Prison, 14 a chronicle of Albert Kligman's research at Philadelphia's Holmesburg Prison Complex from 1951 through 1974. Many prisoners stated they were harmed by experiments that seemed to violate basic ethical strictures, but explained their slowness or failure to seek legal redress after their release to their belief that they had signed waivers that prevented them from pursuing justice; they did not know that they cannot legally sign away their rights to seek justice in such an instance.
It is possible that the inmates did sign waivers, but given the general low level of literacy in the population, it is also possible that they mistook consent forms for waivers. Researchers can avoid such misunderstandings by offering verbal as well as written reassurance that subjects have not waived the right to complain and can seek recourse in such cases. 15
There seem many other workable avenues for addressing these sorts of informed-consent barriers, such as simplifying the forms' language and providing supplemental brochures and handouts. Simply asking the subject to “repeat back” what he had been told about the study to the researcher, who gives corrective feedback until the subject's comprehension seems complete, has worked well. In a research study, this step added only 3 minutes to the conventional process. 16
Trials of electronic informed consent, in which subjects completed digital rather than paper documents within a program that gave information as it was requested, resulted in a greater understanding of the study than the use of conventional paper documentation. 17 Another trial of women suggested that watching videotaped educational tools helped to score 56 percent higher on knowledge assessments than women who saw no such video in addition to conventional informed consent procedures. 18
Not only scientific terminology but modern research practices have caused inevitable confusion that precludes voluntary and meaningful and consent.
Consent Optional
In the research arena, the naming problem even impinges upon the acronyms by which clinical trials are known because they can undermine objectivity about the appropriateness of and expectations from the research. One example is the manner in which researchers refer to the 1996 amendment to the Code of Federal Regulations 21 50.24, which allows testing under an exception to informed consent under certain conditions. Persons who urgently need care and are unable to give consent, often because they are unconscious from trauma, can be enrolled in studies without any attempt to garner consent from them, their loved ones, or their legal representatives. Within this essay I often refer to such studies as “no-consent” or “non-consensual” trials, because dispensing with informed consent is the salient feature of such studies for the laypersons who comprise the subject pool.
Although ethicists and researchers coolly write of the rationale for and efficiency of such studies, its potential subjects, relatively few of whom are aware that legal waivers to research consent exist, share a different perspective. Many have read or heard widely of the troubling abrogation of informed consent in the US Public Health Service-conducted Tuskegee syphilis study, of the appropriation of cells from an unwitting Henrietta Lacks over the strident objections of her husband, of the highly publicized research deaths of subjects like Ellen Roche at Johns Hopkins, as well as of Jesse Gelsinger and Nicole Wan at the universities of Pennsylvania and Rochester (New York), respectively. From the perspective of many research subjects, informed consent is less a malleable abstraction to be debated than an essential layer of protection.
However, researchers' writings describe noncon-sensual studies differently, as “emergency research” as they aver that medical urgency excuses dispensing with consent in life-or-death situations, although they must conflate research with urgent care in order to do so. This emphasis on “emergency” nomenclature deflects attention from lack of consent and simultaneously stresses a rationale for such studies — an emergent situation in which the subject is unconscious or incapacitated to give consent, yet in which something novel must be urgently be done to save him — and to study how better to deal with such emergencies. Substituting “emergency” for “noncon-sensual” deftly sidesteps the fact that this is research, not treatment, for which no consent or refusal is sought and for which most subjects have no way to refuse participation.
Even intramedical discussions debating the merits of this consent issue sometimes do so obliquely, as “50.24 studies” or even more opaquely, by using the acronym EFIC, which stands for “exception from informed consent.” Among medical professionals, EFIC is an instantly recognizable umbrella term for research under 50.24, but this term would mystify laypersons.
It is far from the only troubling acronym labeling contemporary medical research studies.
Acronym Required
Such shorthand terms for medical studies were once the exception, except for cardiology research, which has long embraced them. But over the past two decades, medical researchers have become hotly enamored of acronyms, which the Oxford English Dictionary defines as “[a]n abbreviation formed from the initial letters of other words and pronounced as a word.” It is taken from the Greek akron ‘end, tip’ and onuma ‘name.’ Unlike mere initialisms, which consist of the phrase or title's initial letters that are pronounced separately (e.g., FDA, MRI) acronyms are pronounceable words.
Moreover, fudging is common, and acronyms are often constructed by selecting letters other than the initial ones, and even by slipping in letters that do not appear in the title. However they are generated, some of these nicknames that researchers give their studies, such as CURE (Clopidogrel In Unstable Angina To Prevent Recurrent Events Trial Investigators) 19 or HOPE (Heart Outcomes Prevention Evaluation) raise concerns — and expectations.
Acronyms, once rare, have now grown so numerous that today, one can hardly recall a word that has not been pressed into service — or invented. Acronym trials are now the norm, and are especially popular in research funded by pharmaceutical companies. But, what is the attraction?
Acronyms are designed to persuade subjects, other scientists, or both, depending upon the intent of the study, of the study's virtues. It is easy to grasp the attraction of a study nicknamed CURE, 20 HOPE, 21 or ALIVE, 22 which introduces the research with a positive connotation. In what psychologists call “automatic attitude activation,” the mind evaluates and attaches positive or negative values to the stimuli evoked even before being conscious of the reaction.” 23 In short, the positive emotion evoked by the chip-per acronym eclipses the very logical thought upon which informed consent, or any consent, should be predicated.
Researchers know too much science to be so easily swayed, one would think, and they develop habits of intellectual rigor that inoculate them against the worst deceptions. For example, although it allows him to hope that the tested preparation will be effective, the requirement of equipoise dictates that a researcher's professional stance must be a genuine uncertainty about the outcome of the trial. But the subject need operate under no such compunction or mindset and, unfortunately, these acronyms make implicit promises to her with no proof that the study can deliver.
Despite this, authors and their funders have embraced acronyms in hopes that their semantic felicities will enhance perception of their studies' quality 24 and will serve as a mnemonic aid, helping others to remember their research, and so distinguishing their study from the common herd. Successful acronyms do this so well that they can consign the labels and titles they replace to oblivion. We're all familiar with radar, lasers, and scuba gear, but who remembers radio detecting and ranging, light amplification by stimulated emission of radiation, or self-contained underwater breathing apparatus? 25 All this retention and positive attention, authors reason, can elevate their studies' citation rates.
Yet all is not relentless optimism when it comes to research acronyms: scientists are also fond of classical allusions that clothe a trial in an aura of borrowed wisdom and gravitas. Beginning in 1986 a related group of ISIS trials took the name of the Egyptian goddess of health. ATHENA, PALLAS, PLATO, SOCRATES, and of course, OSIRIS 26 were not far behind, lending a patina of wisdom to the studies, as does the EINSTEIN trial. 27 Investigators hope that this whiff of erudition will also pay off in impressed subjects, increased impact and citations. And indeed, studies with acronyms do enjoy greater prominence than so-called “anonymous” studies without them.
The Cochrane Heart Group scrutinized 173 randomized studies published before 2003 and found that three prestigious journals — Circulation, the Lancet, and the New England Journal of Medicine — published 61 percent of the acronym studies. Studies with an acronym had higher Jadad methodologic quality scores 28 and were able to enroll five times as many patients as those without — although they were no more likely than others to emerge with positive results. Thus, acronyms have repeatedly been shown to deliver, boosting not only scientists' ability to remember the research, but also to remember it positively and on the whole, acronym studies do enjoy higher citation rates.
So. it is not surprising that acronym studies have burgeoned, increasing tenfold over 6 years from 1996 until 2002. Today, most studies are referred to by acronyms. 29 James P. Orlowski, M.D., and James A. Christensen, acknowledge the power of acronyms to sway scientists and subjects, and they are concerned enough to castigate many as “coercive.” In a report for Chest they determined that 155 (6.5 percent) of the 2383 clinical-trial acronyms they evaluated were coercive and they summarize: “A distraught or frightened patient with a life-threatening illness who is offered a research study with an acronym of CURE, HOPE, HELP, IMPROVED, LIFE, RESCUE, MIRACL(sic), SAVED, or ALIVE is possibly being coerced by the acronym. Institutional review boards and the medical research community would not tolerate a CRT entitled, ‘A Surefire Cure for Cancer,’ they write. “They should be no more tolerant of a CRT with an acronym listed above.” 30
Many ethicists would quibble with the label “coercive,” which typically is reserved for more extreme volitional pressures. Yet one needn't hold a gun to the head of a seriously ill and frightened subject with diminishing options who is looking into the abyss in order to achieve a coercive level of influence. An expert need merely suggest, even implicitly, that the CURE trial is all that stands between him and the end. The suggestion of an actual “cure” may remain subliminal: it need not be uttered, but it is there in the trial's name, and perhaps looms large in his decision, triggering “emotions, memories, or hopes that might subliminally sway a potential research subject to participate in a research trial.” 31
FDA regulations don't directly address acronyms, but the agency is alive to the risk of such undue influence on patients and subjects. Their draft regulatory guidance on informed consent 32 states that “overly optimistic representations of the clinical investigation may be misleading and may violate FDA regulations that prohibit promotion of investigational drugs and devices.” 33
Moreover, the FDA does seek to rein in the optimism of, for example, medication brand names that impart misleading linguistic cues born of marketing psychology and scientific testing. In addition to guarding against drug names that look or sound similar enough to trigger one in four US medication errors when one is mistaken for another, 34 the FDA's Division of Drug Marketing, Advertising and Communications rejects suggestive brand names that imply a benefit the medication does not impart, that downplay its risks, or that suggest a drug works for conditions for which it is not approved. 35 It is true, however, that some names seem to slip through the cracks: Concerta for ADHD sounds like “concentrate,” and Relenza to offer “relief from influenza.” 36
Even so, the FDA rejects two of every five suggested brand names. The agency also contributes to the phenomenon of increasingly strange-sounding and unpronounceable brand names by insisting upon names that are clearly distinguishable from each other, which has become nearly impossible because of the plethora of drug names already circulating. In addition, the FDA militates against intelligibility by banning “overly fanciful” names — No “Cancer-Be-Gone” or “HepC Helper” — and this encourages drug makers to pursue Latinate or chemically referential rather than easily recognizable and accessible drug names. Many unpronounceable drug names feature X's and Z's because these letters were once rare and helped the medications to stand out.
The consultants who devise new brand names, like the researchers who devise catchy acronyms, seek standouts that differ from other names and that doctors will remember, sometimes sending coded allusions to prescribing physicians; Liptor for example, lowers lipids. Sometimes brand names send a message to the patients as well, like Tamiflu, whose name suggests that it may “tame the flu.” But the more usual long, technical-sounding, tongue-twisters of today can provoke alienation and even fear in some patients and subjects, 37 a problem of which the pharmaceutical companies seem insufficiently aware.
Although acronym-named studies are no more likely than other studies to result in positive conclusions, the pharmaceutical industry is four times as likely to be fund them and the studies are eight times as likely to be authored by an industry employee than other studies. 38
In fact, pharmaceutical funders are so enamored of acronyms that researchers are running out of new ones, which drives a serious duplication problem. For example, in 2015, Tsung O. Cheng listed 40 distinct studies using the acronym HEART, and ClinicalTrials.gov displays 47 SMART, 16 HOPE, and six CURE studies. This embarrassment of riches means that a PubMed search for one of these acronyms can easily result in the scientific equivalent of the phone book, counteracting the original purpose of helping the study stand out in a field of similar research, and making research into individual studies a Sisyphean task.
Cheng further writes that the industry's appetite for acronyms now leads it to paper over original study titles with an acronym — after the fact. A completed trial of amiodarone, for example was retroactively dubbed the Amiodarone Resuscitation of REfractory Sustained ventricular Tachyarrhythmias (ARREST) trial, at the insistence of pharmaceutical sponsors — although the acronym was never mentioned in the original article. Cheng also recounts how some investigators first produce an acronym, then flesh out a title to support it. 39
If the subject lives in the sort of area where public-health agencies stand accused of colluding with landlords who illegally rent lead-imbued homes to families with small children and where public-health leaders have orchestrated the spread of “treated” human waste on residents' front lawns, he may well view research — and its descriptive language — more warily than the researcher, who lives in a community where such hazards and indignities are unknown.
Speaking in Tongues
What about researcher literacy? Much attention is paid, and rightly so, to the challenges presented by low scientific literacy within the subject pool. But literacy failings dog well-educated researchers as well as subjects, and these also contribute to readability issues.
In The Elements of Style, William Strunk, Jr., advised, “Do not be tempted by a twenty-dollar word when there is a ten-center handy, ready and able,” 40 but few academics seem to listen. Informed consent forms, like other works generated within academia, sometime fail to define terms that are common to scientists but not to lay readers, a disaster for communication.
Unfortunately, the conventions of academic scientific writing sometimes encourage pretentious, unnecessarily complex wording and unwieldy sentence construction. Sadly, this is often the hallmark of what is considered compelling academic prose. Writing that favors the passive voice, excessive qualification, and needlessly Byzantine sentence structure impresses colleagues even as it produces turgid prose that obscures rather than elucidates meaning, especially for readers at that prescribed eighth-grade level. 41
Not only words, but also extraverbal signifiers and semiotics convey information about human medical experimentation. As mentioned above, people who share language and a larger cultural and geographical identity sometimes are divided by cultural identities that differ widely — religious beliefs and customs, native tongue, ethnicity, socioeconomic status, and history, especially history within the US medical culture. Just a peek into Baltimore's history of medical abuses illustrates this point.
These include the 1886 documented “burking” (a murder carried out to sell a body to anatomists) of Emily Brown, 42 a white resident of the “colored section” in Baltimore, 43 the notorious rape of Henrietta Lacks' cells, 44 the death of Ellen Roche in a Johns Hopkins asthma study, 45 and a 2000 Maryland court ruling that compared the Kennedy Krieger Institute's (KKI) role in a lead-poisoning study of black children to the Tuskegee syphilis study. 46 Baltimore is ranked the sixth poorest city in America, 47 but if the researcher lives in affluent Towson and the subject in impecunious Sandtown, 48 they do not share a socioeconomic group, a divergence that is significant not only for health status, but also for research practice.
If the subject lives in the sort of area where public-health agencies stand accused of colluding with landlords who illegally rent lead-imbued homes to families with small children and where public health leaders have orchestrated the spread of “treated” human waste on residents' front lawns, he may well view research — and its descriptive language — more warily than the researcher, who lives in a community where such hazards and indignities are unknown.
In consequence, words pertaining to medical research and the systems they encapsulate may be viewed very differently by researchers and subjects. The disparate medical experiences of researchers and subjects can effectuate a higher index of suspicion in the latter and additional effort to understand this as something other than “paranoia” must take place in order to convey information. Unfortunately, the glossary of medical research reflects a privileged perspective and elides the ulterior enrollment, grant-seeking, and professional-advancement goals of researchers even as their statements are accepted as the default, “value-free,” lingo of the objective scientist. Donna Haraway captures this common linguistic assumption in her essay “Situated Knowledges: The Science Question in Feminism and the Privilege of Partial Perspective.”
Scientists tell parables about objectivity and scientific method to students in the first years of their initiation…[Their] gaze claims the power to see and not be seen, to represent while escaping representation. This gaze signifies the unmarked positions of Man and White, one of the many nasty tones of the word “objectivity.”
49
In the medical-research arena, discussions of “mythology,” “illogic,” “distrust,” “fear,” and even “paranoia” are culturally loaded and tend to focus upon the reticence and supposed psychological anomalies of subjects, while maintaining silence about the mythologies, bias, and illogic that may fuel the designs of “objective” researchers, or even about the illogical or mythical nature of the research questions that are posed. For example, supposed distrust, fear or even “paranoia” of medical research among African Americans is frequently laid by researchers to one signal event, the Tuskegee syphilis study, even though one can do so only by ignoring centuries of documented abusive research studies conducted with black Americans. 50 The large body of studies seeking how to determine how this one event created a blanket rejection of medical research assumes this causal connection without evidence and so constitutes an example of mythology on the part of scientists, a mythology that is not subjected to the stricter scrutiny of African American fears.
When researchers do acknowledge troubling lapses or breaches of research ethics or performance during communication with subjects, these breaches are often qualified as “past abuses” with no evidence offered that these and similar errors are confined to the past.
One corrective would be to substitute fact for mythology by acknowledging this occult history and by using the neutral term “iatrophobia,” from the Greek iatros and phobia and meaning “a fear of healers”: This term avoids the unsubstantiated judgment inherent in “paranoia.”
When researchers do acknowledge troubling lapses or breaches of research ethics or performance during communication with subjects, these breaches are often qualified as “past abuses” with no evidence offered that these and similar errors are confined to the past. Just as the tendency to ascribe fears to single event tacitly judges subjects by implying that their broad aversion to research studies is an overreaction to a single event, so the unsubstantiated location of such abuses “in the past” implies that today, a subject's concerns are groundless.
Blood Rites
Unfortunately, there are plenty of contemporary examples of research abuse and miscommunication as exemplified by the PolyHeme study, conducted between 2005 and 2007 at 26 sites in the US and Canada. It well illustrates the communication gap between researchers and subjects, because a plethora of communications errors, including misused terms, operated to deceive subjects about the nature of the research. However, these errors did not prevent informed consent, because there was never a provision for giving consent, informed or otherwise, in the experiment. That experiment was designed to test the biological PolyHeme, a hemoglobin-based oxygen carrier (HBOC) blood substitute that was the only patented product of Northfield Laboratories. Northfield anticipated a $6 billion dollar market for artificial blood should it win approval. Following a disastrous hospital study that ended in high rates of heart problems and death, PolyHeme was tested in clinical trials without informed consent, in fact, without obtaining any species of consent whatever from subjects.
Any trauma victim who lived in one of the Poly-Heme test cities could be unwittingly enrolled in the study and given either the experimental substance or the standard of care. Here's how: When the ambulance raced to the scene of a trauma such as a car accident or gunshot wound, the EMTs paused before beginning treatment to open a manila envelope with a computer readout that told them which modality to give the victim: PolyHeme or the standard of care.
Someone who lived in a study city and did not want to participate had to contact the company to receive a bright blue plastic bracelet that read, “I decline the PolyHeme study,” then wear that bracelet at all times, every day.
Of course, the catch was that you had to know that the study was taking place, and then discover whence to obtain the bracelet. Most residents knew neither. In fact, bracelets were not always available. In Seattle, a different no-consent study ran out of bracelets after publicity caused alarmed urbanites to flood researchers with so many requests that they ran out of bracelets — for a year. This left no way to opt out, and they were not alone: people visiting or driving through study areas could not opt out if they suffered a qualifying injury in the wrong part of town.
These studies differ from presumed consent, in which a subject is “presumed” to consent in that the according to CFR 21 50. 24, the subject's right to consent is waived altogether without reservation, and no assumption, however tenuous, is made that he would acquiesce. 51
I have referred to these as “no-consent” studies because this failure to elicit consent is the salient feature that the average layperson (and potential subject) would find of greatest interest and concern. But this is not the way the medical community and literature refers to Northfield's PolyHeme study, the later Resuscitation Outcomes Consortium (ROC) study nor the myriad of similar studies that dispensed with consent under CFR 21 50.24. Instead, they employ the abovementioned acronym EFIC or simply refer to them as “emergency research,” studies. These lexical semantics simultaneously provide a rationale for the study — to learn how better to treat emergencies — and neatly sidestep the fact that no consent is sought and most subjects have no viable way to refuse participation.
Verbal Chameleons
Other word choices by Northfield and its researchers offered similar semantic sleights of hand. Early in the study, the company announced that it was offering “community consent” in lieu of informed consent. 52 This species of “consent” consisted of meetings notifying anyone who attended about the study. The study design was presented as a fait accompli, and no consent was elicited. Clearly these meetings met no objective definition of “consent,” and some years later, the language was changed to “community notification,” also a misleading term because the meetings were relatively sparsely attended.
The content of the standardized Powerpoint slides used to explain the study during these meetings as well as public statements from researchers reveal other consistent and telling distortions of language, including a number of frequently misused terms. PolyHeme is referred to as a “treatment” which encourages what the late Jay Katz called the “therapeutic illusion,” by encouraging the research subjects to think of themselves as “patients” and this leads the lay audience to suppose that PolyHeme's efficacy and safety have been demonstrated: they had not.
Shortly after the adoption of CFR 21 50.24, Katz wrote, …one of my most fundamental objections to the regulation is this: that in its emphasis on therapeutic benefits, the FDA obscures the fact that some of the permissible research activities either hold out no promise for therapeutic benefit or are so vaguely defined that potential therapeutic benefit can be inferred when research is the predominant intent. Research is not treatment, and whenever clear distinctions are not made between the two, the waiver of informed consent becomes problematic because some human subjects are being recruited to serve the ends of others.
53
Another community meeting slide insists that Polyheme is safe with “no known problems” — despite the injuries and deaths that marked the earlier hospital study and a long history of similar heart and excess-mortality problems in many earlier HBOC studies, which is documented in a 2008 JAMA article. 54
Most critically, these semantic lapses expose a crucial, but often overlooked distinction between patients and research subjects. That is, another misleading semantic lapse is that subjects are often referred to as “patients,” which implies a therapeutic relationship between the subject and the researchers that does not exist. Neither do the rights that accrue to a patient, such as the right to expect the best possible individualized treatment: yet subjects do not always understand this, as the Katz pointed out. 55 The perception of the physician as healer focused on the need of the patient before him is at odds with the physician's role as a researcher, and many subjects don't make this mental leap to understand that the wholly protective relationship is denied to the subject. In fact, the engineered confusion of “subject” and “patient” in the PolyHeme study backfired when the Duke University IRB temporarily suspended its arm of the study after it discovered that the PolyHeme study violated North Carolina's Patient's Bill of Rights. The study later proceeded, after receiving a waiver.
A similarly troubling description of an experimental reference to “safe” comes to mind. Kennedy Krieger Institute promised to help parents find “lead-safe housing” for their lead-poisoned children and enrolled them in a contested study. Yet researchers knew that the housing in question was imbued with lead that poisoned some of these children. No definition of “lead-safe” was given in the consent form, and a reasonable layperson would infer that such housing did not pose a lead threat to his child.
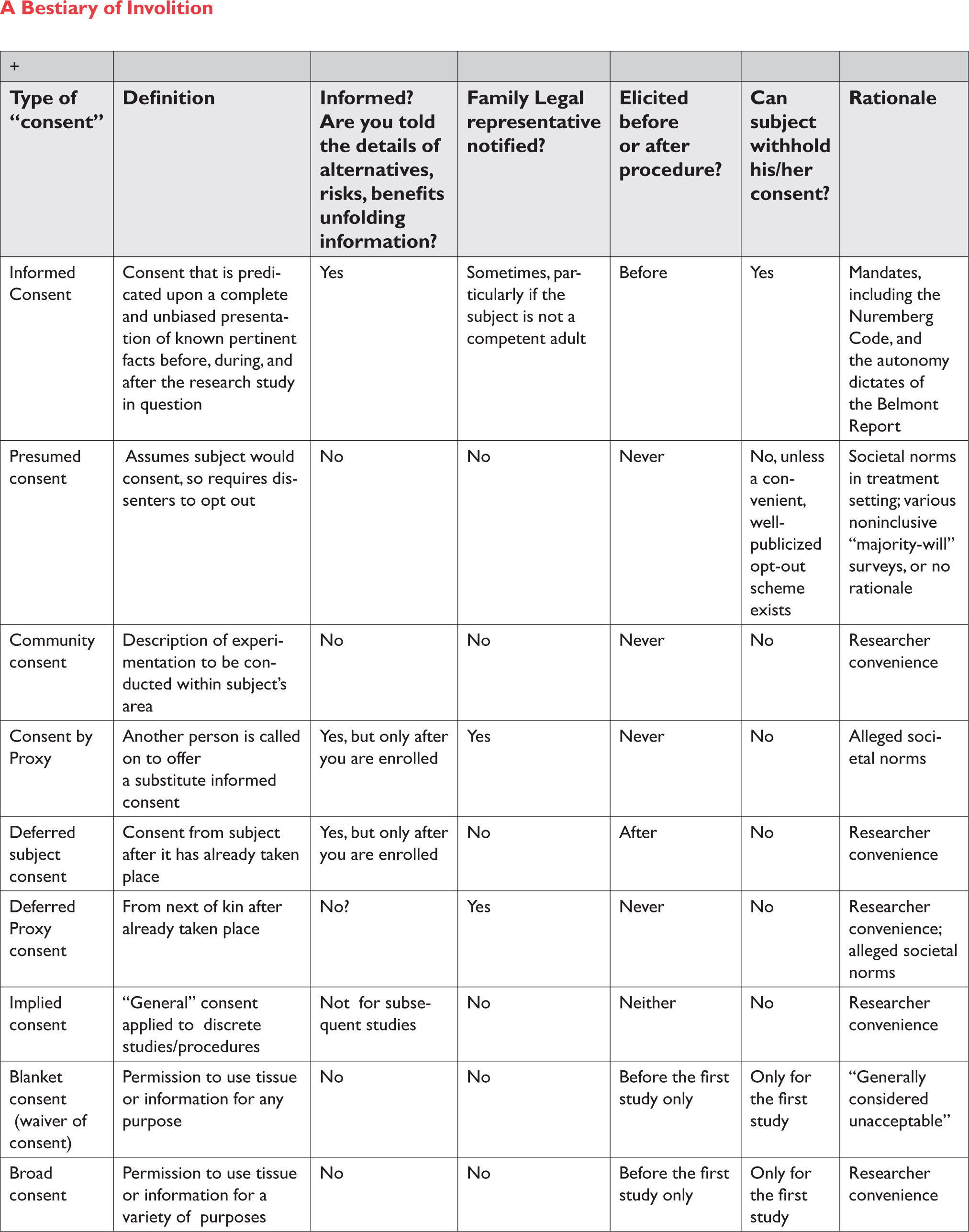
Other problematic words that arise during the consent process are noted in a 1995 article entitled “Who Understands? A Survey of 25 Words or Phrases Commonly Used in Proposed Clinical Research Consent Forms.” 56 But with apologies to James Kunen, 57 I can think of no greater example of the power of an adjective to modify a noun than the use of the word “presumed” before the word “consent” — unless of course, one considers the other unusual species of “consent” that have been used by researchers, but which would surely mystify subjects. The accompanying chart “A Bestiary of Involition” lists some examples.
Semiotics and the Therapeutic Illusion
Nonverbal signs and their interpretations reinforce the “therapeutic illusion” of clinical care that Katz decried in 1996. In the perception of subjects, traditional images and accouterments of the healer convey personalized care. The setting of a hospital or clinic, a white coat, clipboard stethoscope, thermometer, sphygmomanometer, and the taking of a medical history are closely associated with the image of a healer caring for his patient, as is the act of taking vital signs and drawing blood as well as other familiar aspects of the medical gaze. Throughout the subject's life, these have been encountered in healing sessions and these signs militate against the researcher's very different role as guardian of the study's ends and scientific protocol, which can be at odds with the optimal welfare of any individual subject.
Even the blue and green plastic bracelets dispensed to people who wished to avoid participation in the nonconsensual PolyHeme and ROC studies recall the plastic bracelets affixed to patients in hospitals as a sign they are under the hospitals' and doctors' care. People also associate modern ambulances with the rapid deployment of expert personalized medical response closely tailored to the patients' individual condition, whether giving fluids or performing CPR in response to immediate needs. Sirens, flashing lights, and speed signify responsive, highly individualized care. But in nonconsensual studies like that of Poly-Heme, the ambulance becomes a mobile laboratory where attendants' response is dictated by a computer printout that they are required to consult and act upon in accordance to the randomized study protocol, not in response to the patient's signs, symptoms, or immediate needs. In such an ambulance setting, where every sign points to personalized emergent clinical care, the failure to inform a subject that he is indeed a subject, not a patient, seems especially egregious.
Newspeak: Purging “Experimentation”
During a university lecture about my book, Medical Apartheid: The Dark History of Experimentation on Black Americans from Colonial Times to the Present, an auditor criticized my use of the term “medical experiments” as “inflammatory.” I was a bit surprised, given that I had limned the etymology of “experiment,” including the definition given by Claude Bernard, author of An Introduction to the Study of Experimental Medicine, who wrote, “Experiment is fundamentally only induced observation.” But I also remembered enough high-school Latin to shed some light on the discomfort. Periculum, “danger,” is an inherent part of “experiment” — the word and the thing. To experiment is to risk success or failure and when human lives and health hang in the balance, the stakes are high indeed.
It is true that terms such as “medical study” have come to be preferred, and for understandable reason: they now seem more benign. But these terms are not more accurate when the researcher manipulates variables and observes the effects on the bodies and minds of human subjects. Human medical experimentation is an accepted umbrella term for many of the more popular variants, so why does it provoke such wide discomfort? After all, from the inception of modern ethical research assessments, “experimentation” was the default general term, wielded by investigators as well as by their critics. The first reference to human medical investigations, in the Nuremberg Code's first tenet, uses “experiment” twice when it reads in part “…before the acceptance of an affirmative decision by the experimental subject, there should be made known to him the nature, duration, and purpose of the experiment.” 58
The early authoritative classics of the field, from Henry K. Beecher's 1959 Experimentation in Man and his advisor Maurice Pappworth's 1967 Human Guinea Pigs Here and Now: Experimentation on Man use the verboten word. The title of Jay Katz’ seminal Experimentation with Human Beings: The Authority of the Investigator, Subject, Professions, and State in the Human Experimentation Process, like the Nuremberg Code, uses it twice.
Neither do respected works by research insiders shy from the term, such as Who Goes First? The Story of Self-Experimentation in Medicine, by Lawrence K. Altman, or The Human Radiation Experiments by the Advisory Committee on Human Radiation Experiments. As recently as 2015, Oxford Brookes professor Paul Weindling published his Victims and Survivors of Nazi Human Experiments: Science and Suffering in the Holocaust.
A Bestiary of Involition
But by the time I began a public health fellowship in 1992, the word “experimentation” was beginning to mutate. In fact, the fate of the word “mutation” itself provides a good parallel for the trajectory of “experiment” in the human-research context.
This essay seeks to show that words are powerful and that word choices can limit our ability to carry out the communication mandates upon which consent rests.
English evolves, and words, like living things, survive by changing in response to the pressure of experiences. The word “mutation” from the Latin verb mutare, to change, originally referred to tissue or genetic changes induced by radiation in a neutral or even benign manner, as when tumors shrunk after exposure: “mutation” was devoid of dread. By 1911, however, more than fifty cases of X-ray-induced cancer had been reported in researchers who worked with radioactive substances, followed by the ugly deaths of the young “radium girls who painted dials luminous watch dials with radium-226 and mesothorium. After World War II, the carnage in the wake of the Hiroshima and Nagasaki bombings joined the cancers induced in X-ray epilation clinics where physicians did a brisk business in removing coarse dark facial and arm hair of Eastern European immigrants and bleaching the skins of African Americans — all of whom were rewarded with burns and cancers instead of “whiteness”. Such reports helped transform the public image of radiation and American scientists as willing to exploit radiation's power for twisted curiosity or wealth. 59 The word “mutation” now fills Americans with dread.
Similarly, researchers now dislike “experiment” and not only because it reminds subjects of the dramatic domestic abuses of such as that of African Americans and prisoners, and abroad, of Jews and others under National Socialism. “Experiment” also reminds us of the danger, or periculum, inherent in even well-designed, ethically conducted research. Research subjects wish to avoid “experiment” for the same reason. As Carl Elliott points out in his perceptive essay, “Whatever Happened to Human Experimentation?” in a 1995 Advisory Committee on Human Radiation Experiments survey, 60 patients ranked the phrase “medical study” as the most benign, and “medical experiment” as so hazardous that some would risk joining one only if they were terminally ill.” Elliott clarifies that “[n]ot all research studies are experiments. Nor are they all clinical trials. Chart reviews, surveys, ethnographies, epidemiological studies, and many other kinds of medical research could hardly be described as ‘experiments,’ insofar as ‘experiments’ suggests scientific testing conducted under controlled conditions.” 61
Many studies and enterprises are perfectly described as human medical experimentation, but censorship reigns: The term has been, Elliott writes, “purged,” and the resulting newspeak, like so many other problematic linguistic choices discussed in this essay, serves to reinforce the therapeutic illusion by masking the hazards of human studies. Elliott cogently points out that ethicists, who one might expect to decry the bowdlerization, do not and this may be because so many ethicists receive checks and academic appointments from and sit on the boards of the research institutions that they ostensibly monitor, so that their interests are closely aligned with the institutions that shy from the word.
Conclusion
This essay seeks to show that words are powerful and that word choices can limit our ability to carry out the communication mandates upon which consent rests. In Nineteen Eighty-Four, Orwell warns us, “The purpose of Newspeak was not only to provide a medium of expression for the world-view and mental habits proper to the devotees of Ingsoc, but to make all other modes of thought impossible.” 62