
Abstract
The objective of this study was to assess the beliefs of parents of youth soccer players about Chronic Traumatic Encephalopathy (CTE), concussion, and retirement from sport decisions and compare them to those of concussion-specialized clinicians. An electronic survey was completed by parents of youth club soccer players (n=247/1600, 15.4% response rate) and concussion-specialized clinicians (n=18/47, 38.3% response rate) located in a large U.S. urban center. Parents believed more strongly in the causal relationship between concussions and CTE, and between CTE and harm than did clinicians. Parents who themselves had participated in sport at a high level had more conservative beliefs than other parents about the number of concussions after which an athlete should retire from contact or collision sport. Results are discussed in the context of ethical risk communication between clinicians and parents. This includes the importance of communicating information about CTE to parents and youth athletes in an understandable way so that they can make informed choices about contact and collision sport participation. Further research is encouraged to evaluate approaches of communicating evidence about CTE to a diverse population of families of youth athletes.
Introduction
Chronic Traumatic Encephalopathy (CTE) has made its way into public discourse due to increasing media coverage, movies, and documentaries covering diagnoses of high profile athletes. 1 Such media coverage has contributed to a public dialogue about the risks and appropriate limits of contact sport participation. This type of narrative approach to health communication, with stories focused on the experience of a single individual, is often highly effective in shaping public opinion. 2 Readers or viewers tend to empathize with and generalize from the experience of the exemplar. 3 A consequence of this type of communication could be that parents of young athletes inaccurately perceive the extent to which the experience of a small subsample of deceased professional athletes, with years of head impacts and probable multiple concussions, is relevant to their child's sport participation. Understanding how parents view the causality and consequences of CTE can inform how health care providers approach communication about this topic.
Media interest and public concern notwithstanding, the evidence about the natural history of CTE is in fact relatively limited. Although all diagnosed CTE cases have been associated with a history of repeated brain trauma, Meehan and colleagues 4 note that in these cases “the reported degree of severity, frequency of blows to the head, and documentation of prior concussion is highly variable.” As yet there is no prospective data and all evidence has been collected in the form of pathologic case series of donated brains. This approach has substantial limitations including sampling bias, self-selection bias, and a limited ability to assess the presence of confounders, or person-specific modifiers. 5 The Institute of Medicine's report on Sports Concussions in Youth concluded that “whether repetitive head impacts and multiple concussions sustained in youth lead to long-term neurodegenerative diseases, such as CTE and Alzheimer's disease, remains unclear.” 6
Amid this uncertain causality, parents make (or depending on the child's age, contribute to) decisions about contact and collision sport participation. Decisions about ceasing participation in certain sports may be influenced by perceptions about the strength of evidence related to CTE. A consensus statement on the topic from the 4th International Conference on Concussion stated that “it is important to address the fears of parents/athletes from media pressure related to the possibility of CTE.” 7 Parents who more strongly believe in a causal link between concussions, CTE, and long-term harm may perceive a greater threat to continued sport participation after concussions, and thus have a lower threshold for ceasing participation. Consistent with Social Cognitive Theory, 8 these beliefs may be influenced by parents' own experiences with sport and concussions.
The overarching goal of this study was to understand more about the preconceived notions parents of youth soccer players have about CTE so as to help clinicians communicate effectively and ethically with them about this topic. Thus, the aims of this study were (1) to assess athletes' parents' beliefs about the strength of evidence related to CTE, (2) to assess athletes' parents' beliefs about the appropriate threshold for retiring an athlete from sport due to concussion, and (3) to examine the relationship between these two variables and explore differences by parent characteristics including their own sport and concussion history. As there is at present no clear scientific consensus related to CTE and concussion-related retirement decisions, we also surveyed a sample of concussion-specialized clinicians using the same questions to provide reference values to which parent beliefs could be compared.
The overarching goal of this study was to understand more about the preconceived notions parents of youth soccer players have about CTE so as to help clinicians communicate effectively and ethically with them about this topic. Thus, the aims of this study were (1) to assess athletes' parents' beliefs about the strength of evidence related to CTE, (2) to assess athletes' parents' beliefs about the appropriate threshold for retiring an athlete from sport due to concussion, and (3) to examine the relationship between these two variables and explore differences by parent characteristics including their own sport and concussion history.
Methods
Sample and Procedure
Sixteen hundred parents of club soccer players ages 8-18 years old in a league located in a large U.S. urban region were contacted by email and invited to complete an anonymous electronic survey using Qualtrics. Forty-seven concussion-specialty physicians, neuropsychologists, physician assistants (PA) and registered nurse practitioners (ARNP) at two medical institutions in the same region were invited by email to complete an anonymous electronic survey containing a subset of the questions administered to parents. Research activities were approved by the Seattle Children's Hospital Institutional Review Board.
Measures
demographic characteristics
Parents indicated their gender, age, and the highest level of education that they had attained, the highest level at which they previously competed in sport (none or pre-high school, high school, college, professional), and the number of concussions with which they had previously been diagnosed. Clinicians indicated their credentials (physician, neuropsychologist, PA, ARNP).
cte perceptions
Parents and clinicians answered five questions about the perceived strength of scientific evidence supporting causal claims about concussions, CTE, and long-term harm (e.g., concussions cause CTE; all items are listed in Table 3). Responses were on a 100 point scale, ranging from 0=no scientific evidence to support this claim to 100=scientific evidence fully supports this claim.
influences on retirement decisions
Parents and clinicians responded to seven prompts about reasons for ceasing participation in contact and collision sport (e.g., the level of sport at which the athlete is competing; all items are listed in Table 2). Participants were asked to indicate the extent to which they believed that these factors should influence the decision to stop playing a contact or collision sport, with response options of should not influence at all, should influence somewhat, and should influence strongly.
retirement threshold
Parents and clinicians reported the number of concussions after which they believed an athlete should cease participating in contact or collision sports.
Analysis
Descriptive statistics were calculated for all variables. Comparisons between parents and clinician responses for the number of concussions after which an athlete should retire, and for statements about CTE evidence, were made using two-group t-tests with unequal variance. Comparisons between parent and clinician beliefs about reasons for retirement were made using Pearson chi-squared tests of independence and Fisher's exact test. A measurement model was fit for the CTE variable to ensure good local fit before combining it into the larger structural equation models. Using the criteria specified by Hu & Bentler, 9 thresholds for a close model fit were set as CFI >0.95, TLI >0.95, RMSEA <0.05 and chi-squared p value >0.05. Four nested structural equation models were tested, with chi-square difference tests comparing the fit of model iterations. The base model examined the association between CTE beliefs and retirement threshold. Subsequent models added parent characteristics as predictors of CTE beliefs and retirement threshold. Direct, indirect, and total effects for the best fitting structural equation model were calculated. Maximum likelihood estimation was used to account for missing values in all models, meaning that estimates were unbiased under the assumption of missing at random. Missingness ranged from a low of 1.21% for reasons for retirement items to a high of 26.72% for CTE belief items. Analyses were conducted in Stata 13.1 (College Station, TX) and a threshold of p<0.05 was used as the criterion for statistical significance.
Results
Respondent Characteristics
247/1600 parents (15.4%) and 18/47 clinicians (38.3%) responded to the survey. On average, parents were 30 years old and highly educated, with over 95% having obtained at least an undergraduate degree. Around one-third had competed in organized collegiate sport. Additional sample characteristics are reported in Table 1.
Descriptive Characteristics of Sample of Parents of Competitive Youth Soccer Players and Clinicians Who Care for Concussed Youth Athletes
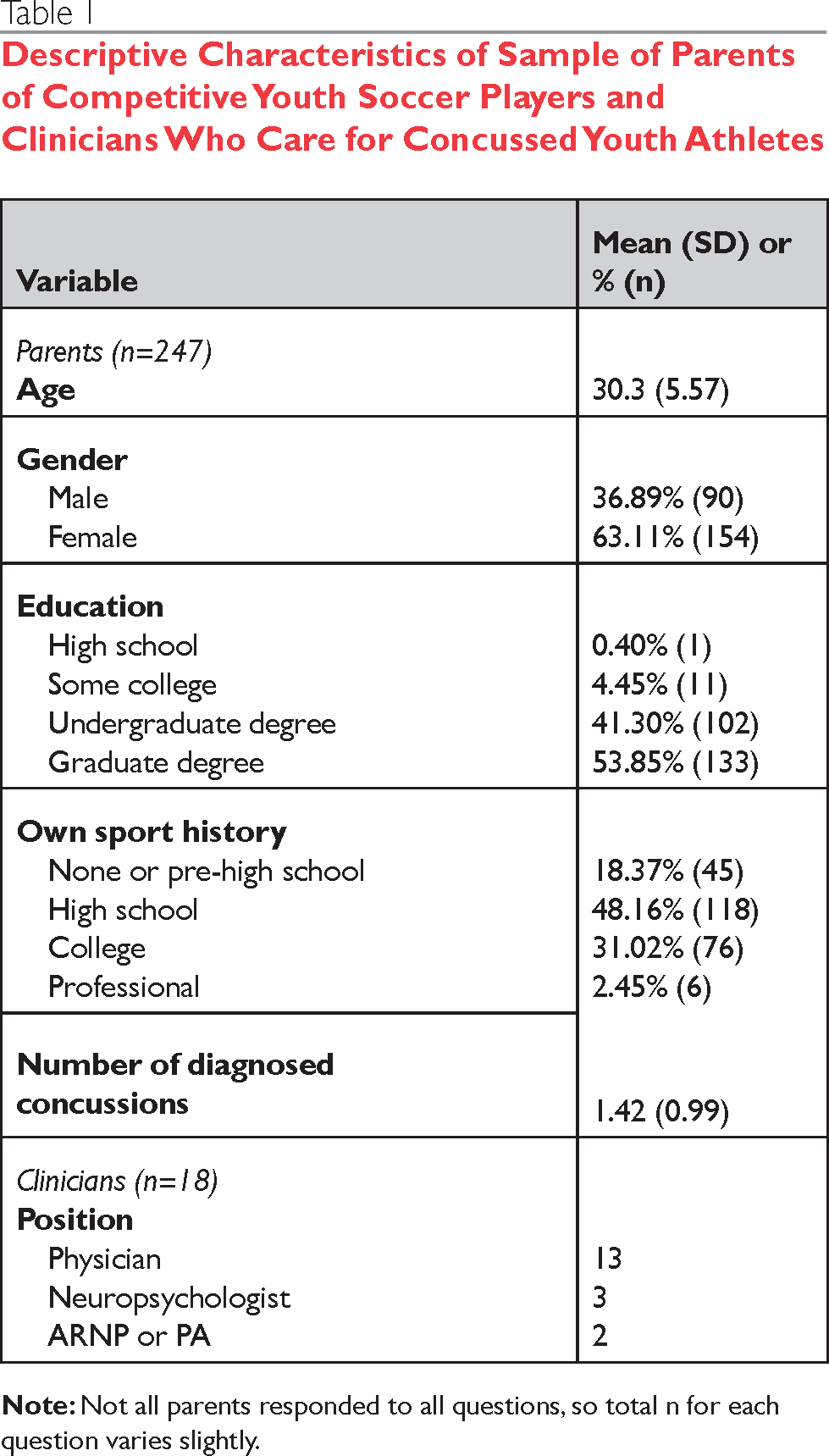
Not all parents responded to all questions, so total n for each question varies slightly.
Beliefs about CTE
Parents rated the strength of scientific evidence related to CTE as significantly greater than did clinicians, with all effect sizes over Cohen's threshold for a large effect (Table 2). 10 The biggest differentials were for evidence about concussions causing CTE (parent mean=65.1, SD=30.3 vs. clinician mean=17.3, SD=15.2), and the possibility of developing CTE after sustaining only one concussion (parent mean=46.2, SD=27.0, clinician mean=6.5, SD=8.8).
Parent and Clinician Perceptions about the Strength of Scientific Evidence Supporting Claims about CTE
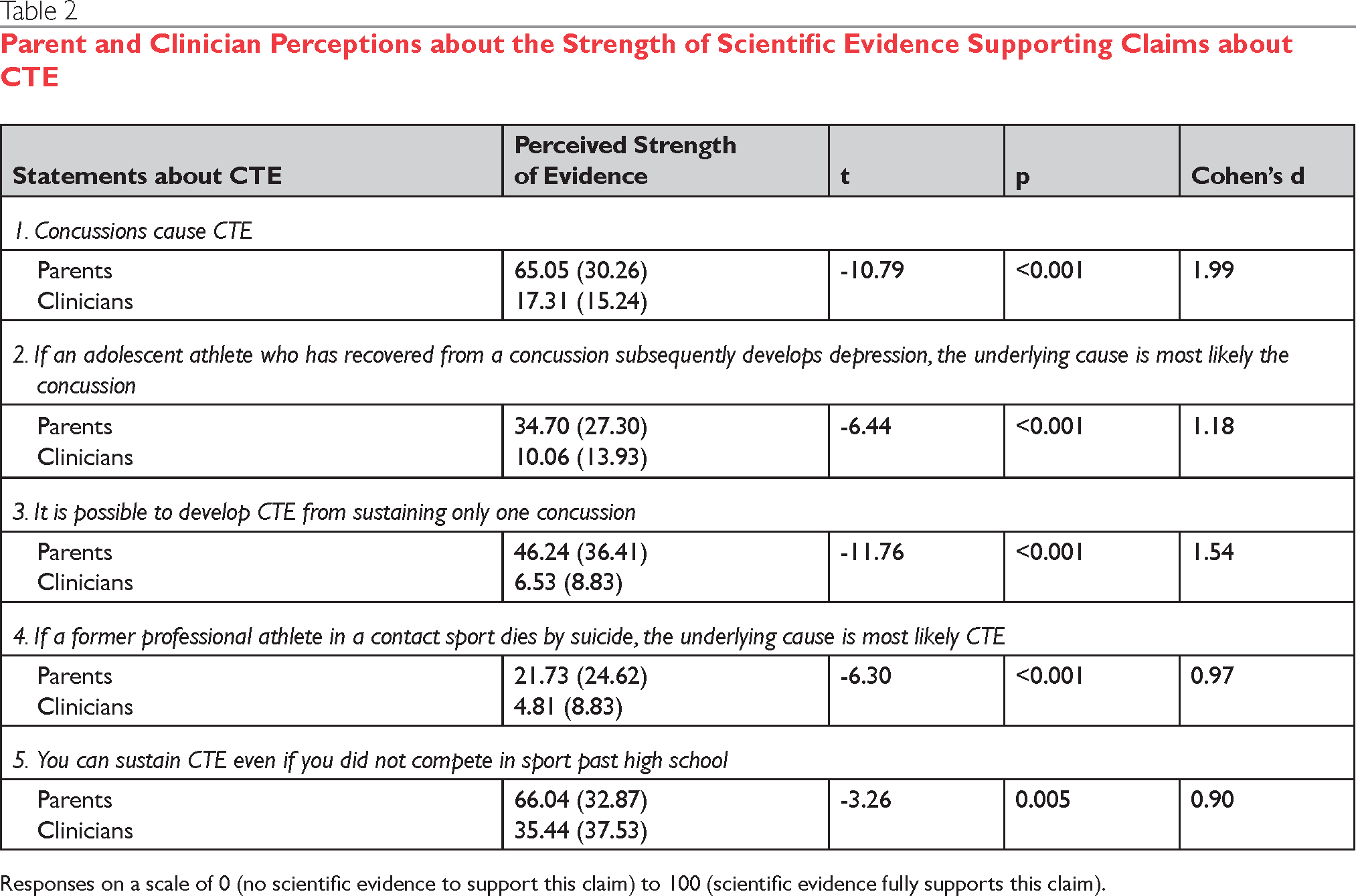
Responses on a scale of 0 (no scientific evidence to support this claim) to 100 (scientific evidence fully supports this claim).
Retirement Decisions
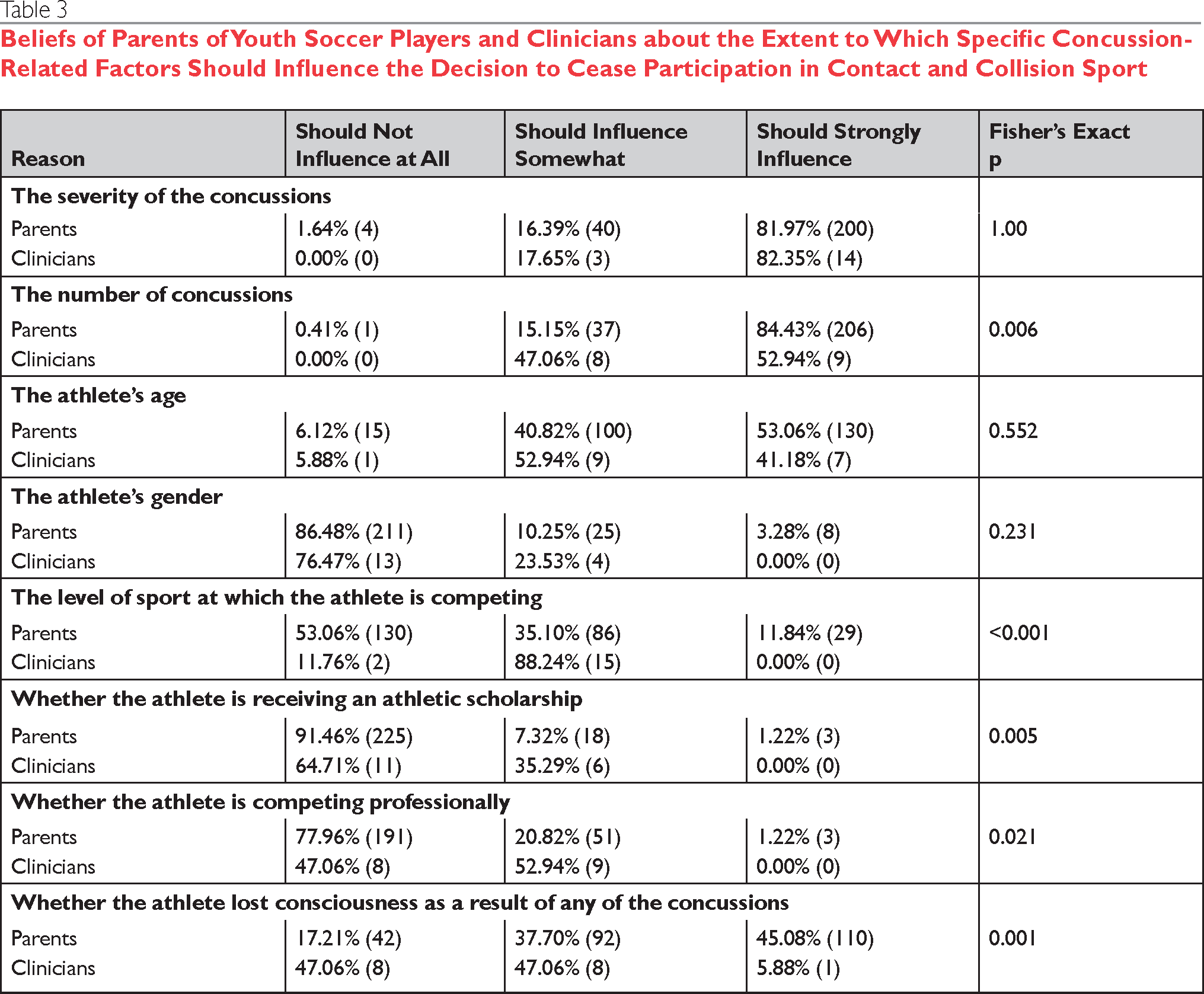
The majority of parents (84%) believed that the number of concussions sustained should very strongly influence retirement decisions, while only about half of clinicians (53%) felt the same (see Table 3). Clinicians tended to weight other factors more heavily than did parents. The majority of clinicians believed that level of sport and whether an athlete was receiving an athletic scholarship should somewhat influence retirement decisions, and more clinicians than parents held these beliefs. There were no statistically significant differences between parents and clinicians in beliefs about how strongly gender, age, and concussion severity should influence retirement decisions; nearly all in both groups felt that the severity of concussions sustained was highly relevant.
Beliefs of Parents of Youth Soccer Players and Clinicians about the Extent to Which Specific Concussion-Related Factors Should Influence the Decision to Cease Participation in Contact and Collision Sport
Retirement Threshold
On average, the mean number of concussions after which parents thought that someone should cease participating in contact or collision sport was 3.7 (SD=2.3), and the average number endorsed by clinicians was 4.6 (SD=2.1). This difference was not statistically significant (p=0.398).
Association between Beliefs about CTE and Retirement Threshold
Structural equation modeling was used to model the association between CTE beliefs and retirement threshold. The initial CTE beliefs measurement model with no covariances between items did not fit the data well, so we examined modification indices and added a correlation between the two items relating to depression and suicide, based on theoretic reason to believe that errors could be correlated. This model was a good fit for the data. Fit statistics and the p value for difference tests comparing these two nested measurement models are presented in Appendix B. Pairwise correlations between all model components are provided in Appendix A. After specifying the CTE beliefs measurement model, we examined a bivariate model (Figure 1) testing whether CTE beliefs predicted retirement threshold. Fit of the model was good (see Appendix B). CTE beliefs were not a statistically significant predictor of retirement threshold; standardized path coefficients are presented in Figure 1. We added parent characteristics (gender, sport history, and concussion history) as additional predictors of both CTE beliefs and retirement threshold in a stepwise process. The final model including all three parent characteristics, with covariance between the three characteristics, was the best fit to the data of the three models including parent characteristics. Standardized path coefficients for this model are presented in Figure 2 and direct and indirect effects in Table 4. There was a statistically significant direct and total effects on retirement threshold by parent sport history (ß=-0.17, p=0.010), with parents who had themselves played sport at a higher level endorsing a lower retirement threshold. There was a statistically significant total effect on retirement threshold by gender (ß=-0.16, p=0.019) with female parents more likely to select a lower number than male parents.
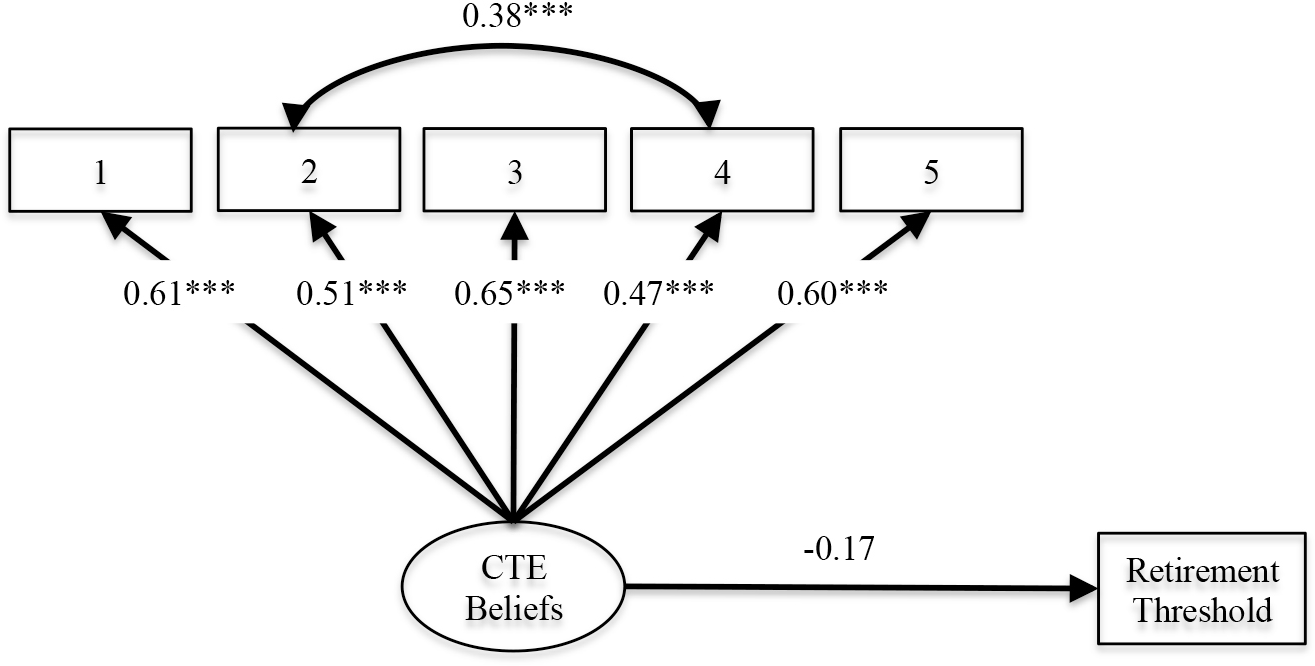
Path Analysis for the Relationship between Beliefs about Chronic Traumatic Encephalopathy, and the Number of Concussions after Which Contact Sport Participation Should Be Ceased (n=241). ***p<0.001
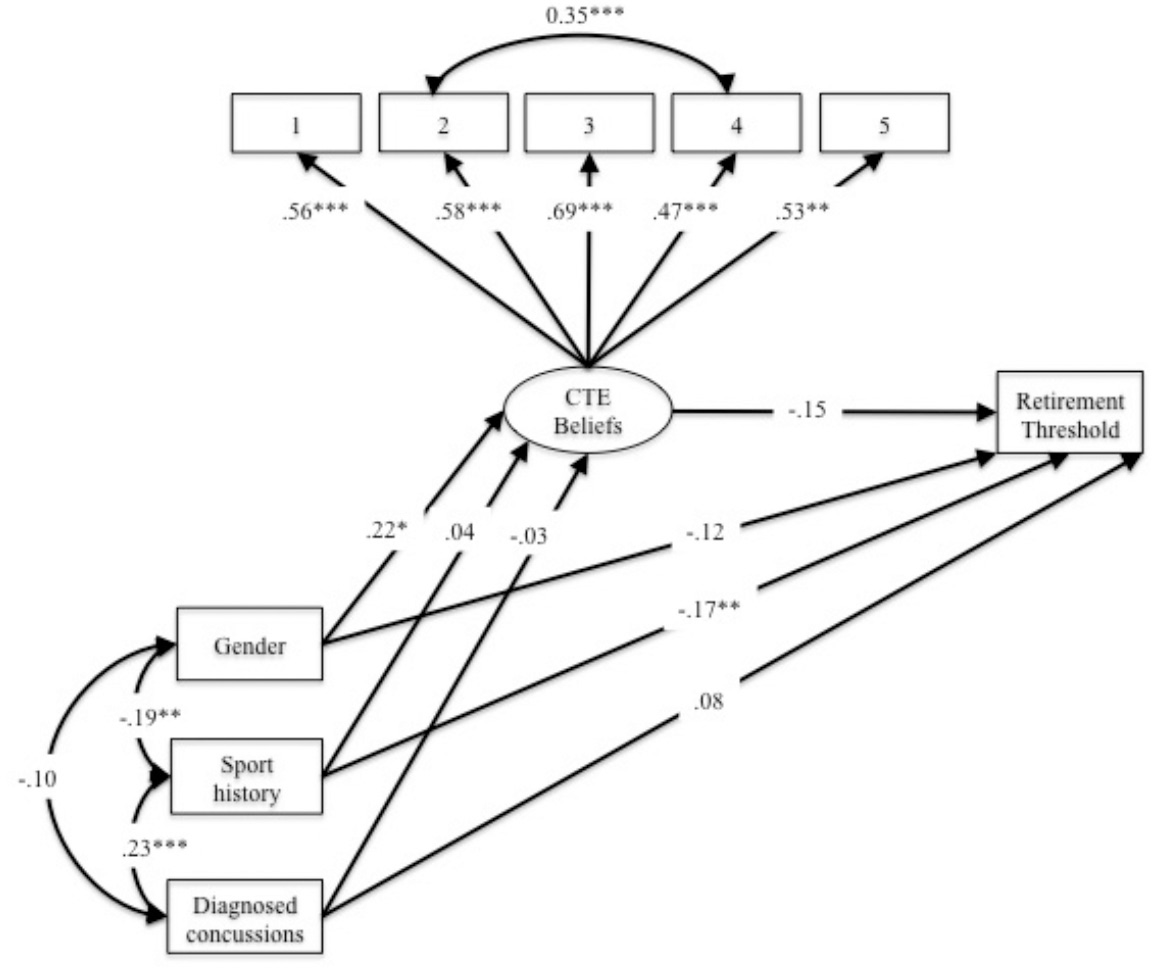
Path Analysis for the Relationship between Parent Characteristics, Beliefs about Chronic Traumatic Encephalopathy, and the Number of Concussions after Which Contact Sport Participation Should Be Ceased (n=241) **p<0.01, ***p<0.001
Direct and Indirect Effects in Final Model Predicting Number of Concussions after Which Contact or Collision Sport Participation Should Be Ceased in a Sample of Parents of Youth Soccer Players (n=241)
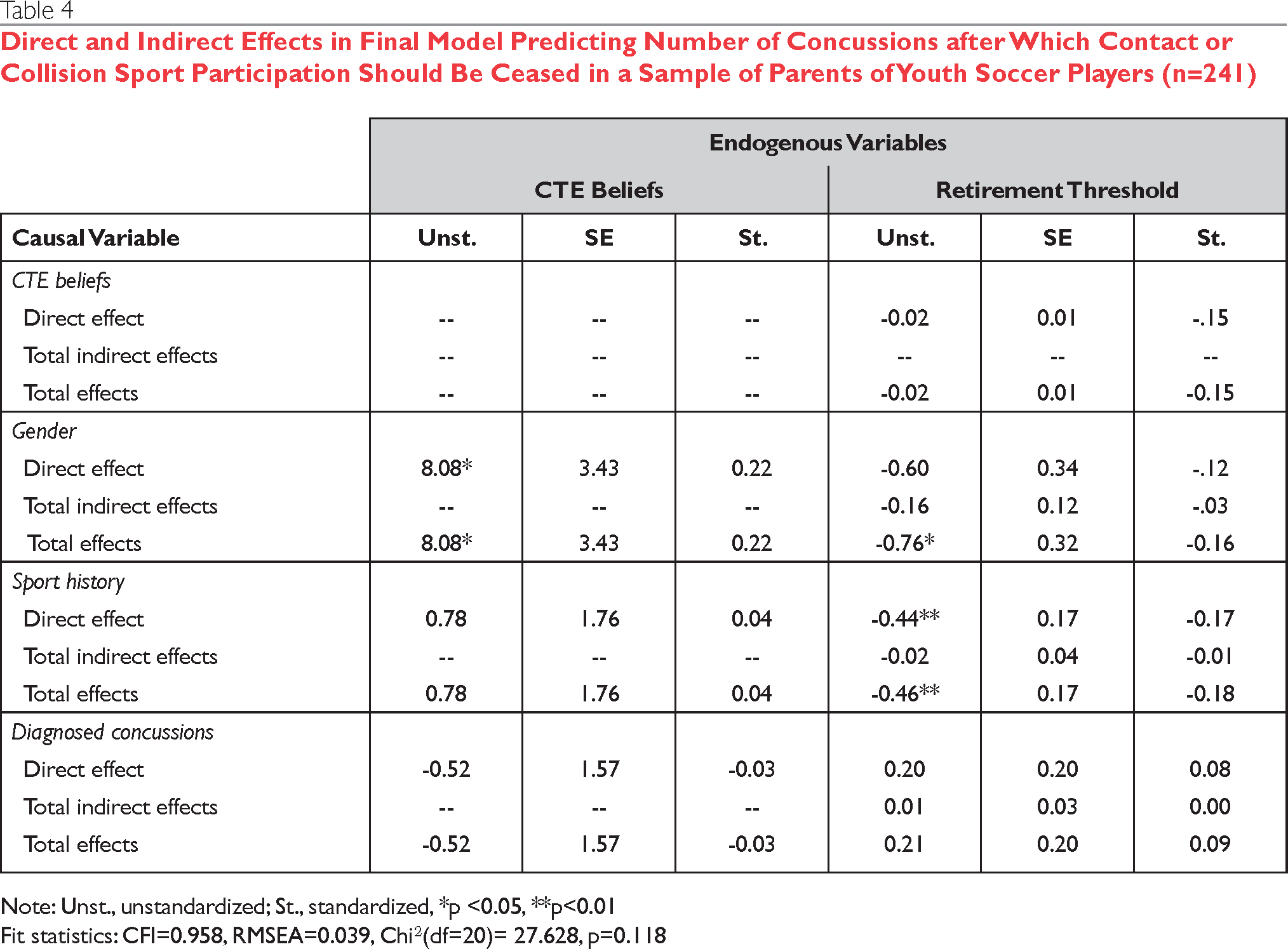
Note: Unst., unstandardized; St., standardized
p <0.05
p<0.01
Fit statistics: CFI=0.958, RMSEA=0.039, Chi2(df=20)= 27.628, p=0.118
Discussion
This study found that clinicians tended to be less confident than parents that there was strong existing evidence about the causes and consequences of CTE. This is not surprising given the different channels through which knowledge transfer to both groups occurs and the different skill sets that each group has for interpreting and contextualizing media coverage of scientific studies and news reports about professional athletes diagnosed with CTE. There were also significant differences between parents and clinicians in beliefs about factors that should influence decisions on retirement from contact sports. Parents were significantly more likely than clinicians to believe that number of concussions should strongly influence retirement decisions. This difference is understandable as number of concussions is a heuristic for decision making that is accessible to parents. It is also possible that clinicians are more aware that self-reported number of concussions may be an imprecise estimate, given endemic under-reporting. 11
These findings of differences between parents and clinicians can help inform approaches to appropriate and ethical communication about the topic. Kirschen and colleagues 12 state that “physicians have a duty to inform [patients] (in understandable language) about the evidence for potential short- and long-term neurocognitive and neurobehavioral risks associated with single and multiple concussions as well as common clinical concussion manifestations.” The fact that many parents appear to make causal attributions about concussions and CTE that are not substantiated by the current body of evidence provides an opportunity for clinicians to accurately translate existing knowledge for families to help facilitate their informed decision making.
However, the absence of clear medical consensus about when athletes should retire from sport post-concussion means that the nature of clinician-patient communication about the topic is more complex than solely knowledge translation. Rational appraisals of risk may be relative to other opportunities and threats in the athlete's environment, and the value that families assign to achievement in sport relative to other domains. Such decisions can be viewed as “preference sensitive.” 13 Communication by clinicians in such situations thus requires respecting the autonomy of families to make decisions consistent with their own preferences. 14 However, this presumes that parents are making rational decisions focused on the long-term best interests of their child. In this study, a subset of parents (11.8%) believed that the level of sport at which the athlete was competing should strongly influence retirement decisions. It is possible that the beliefs of this subset of parents about the importance of athletic achievement reflect what these parents think is truly in the best interest of their child. It is also possible that these parents do not have full information about the probability and benefits of athletic success, or are inappropriately weighting short-term athletic outcomes relative to longer-term health threats. Consistent with this explanation, parents who themselves had participated in organized sport at a higher level of competition tended to have a lower retirement threshold as compared to parents who had competed at lower levels of organized sport. This finding was independent of the parent's own history of diagnosed concussions, and was not related to their gender or beliefs about CTE. It is possible that parents who played sport at a higher level may have had more opportunities to experience consequences of their own sport-related injuries, and/or to observe injuries among teammates. Alternatively, these parents may have had a greater understanding of the rarity of being able to play high-level sport in college or professionally, and thus less likely to believe the risk/reward of continuing to play with multiple concus sions was reasonable.
In cases where parent decision-making may not be solely focused on the child's long-term wellbeing, Kierschen and colleagues 15 suggest that “a physician's commitment to beneficence and duty to protect his or her patient from harm may occasionally supersede patient autonomy from an ethical perspective.” In practice, this may mean that in cases where families appear focused on short-term athletic benefits of continued play, the clinician should more strongly recommend an athlete cease contact sport participation. This is consistent with other literature suggesting that clinicians should take a conservative and individualized approach post-concussion sport retirement decisions. 16 It may also mean providing families with information about the likelihood of obtaining an athletic scholarship or competing in professional sport, as this may help facilitate more fully informed expected value calculations. Additionally, recent advances in patient-centered medicine propose that healthcare providers can support patients in making optimal preference sensitive decisions by helping them clarify their values and goals. 17 Research and program development work is needed to create tools to support clinicians in this value and goal clarification process relative to sport retirement post-concussion. Evaluation of such patient-centered communication tools should assess the extent to which their use results in earlier or later sport retirement, as well as how they impact athlete satisfaction with the retirement decision.
A final important consideration for clinicians thinking about how to ethically communicate information about CTE to families is that this information must be delivered in a way that families can comprehend. Love and Solomon 18 have written a primer to support non-specialist clinicians in communicating with families about CTE. Additional work is needed to determine whether this type of primer meets the learning needs of clinicians and whether it results in appropriate knowledge translation to families. Athletes and their families may have widely varying health literacy and numeracy, and different approaches to communication may be necessary depending on where they are on these spectrums. 19 Ensuring that materials are developed to support communication with all athletes and their families is critical for equitable ethical communication.
Limitations
A primary limitation of the present study is that the provider reference values are based on a small sample of concussion-specialized clinicians affiliated with one institution. It is likely that there is clustering in beliefs about CTE by institution, as a result of self-selection or hiring practices of like-minded practitioners. Further, it is possible that there is variability in responses across different types of clinicians. Additional work is needed to expand this study to obtain clinician reference values in a large and nationally representative data set, and to include a range of providers, both specialist and non-specialist, in the sample to determine whether there are differences between clinician types.
The generalizability of the parent data may also be limited as the present sample of parents was highly educated, with the majority having at least an undergraduate degree. We also only surveyed parents of soccer players. Parents whose children play sports that by their nature engender a greater level of physical contact and risk, such as football and hockey, might have a different understanding and appreciation of sport risk. Additionally, our response rate was low, and there may have been self-selection by parents on the basis of their knowledge or beliefs about concussions. Further work in a diverse sample of parents to build a more complex model of risk perceptions related to concussion and safety-related decision-making is warranted.
The missing data for questions about CTE beliefs among one-quarter of parents is another limitation of this study. It is our assumption that parents who had not heard of CTE or who had limited knowledge about CTE elected to not respond to these questions. As a result, the values for these variables may not be generalizable to the extent that they reflect the beliefs of parents who may be more health literate in general or more informed and interested in the health consequences of contact sport.
Conclusions
The present findings suggest that parents believe more strongly in the causal relationship between concussions and CTE, and between CTE and harm than do clinicians. Providers should be aware of the importance of staying abreast of the evolving science about harm from concussions, and of communicating this information to parents and youth athletes in an understandable way so that they can make informed choices about sport participation. Further research is encouraged to develop and evaluate effective methods of communicating evidence about CTE to a diverse population of families of youth athletes.
Footnotes
The authors have no conflict of interest to declare.
Appendix
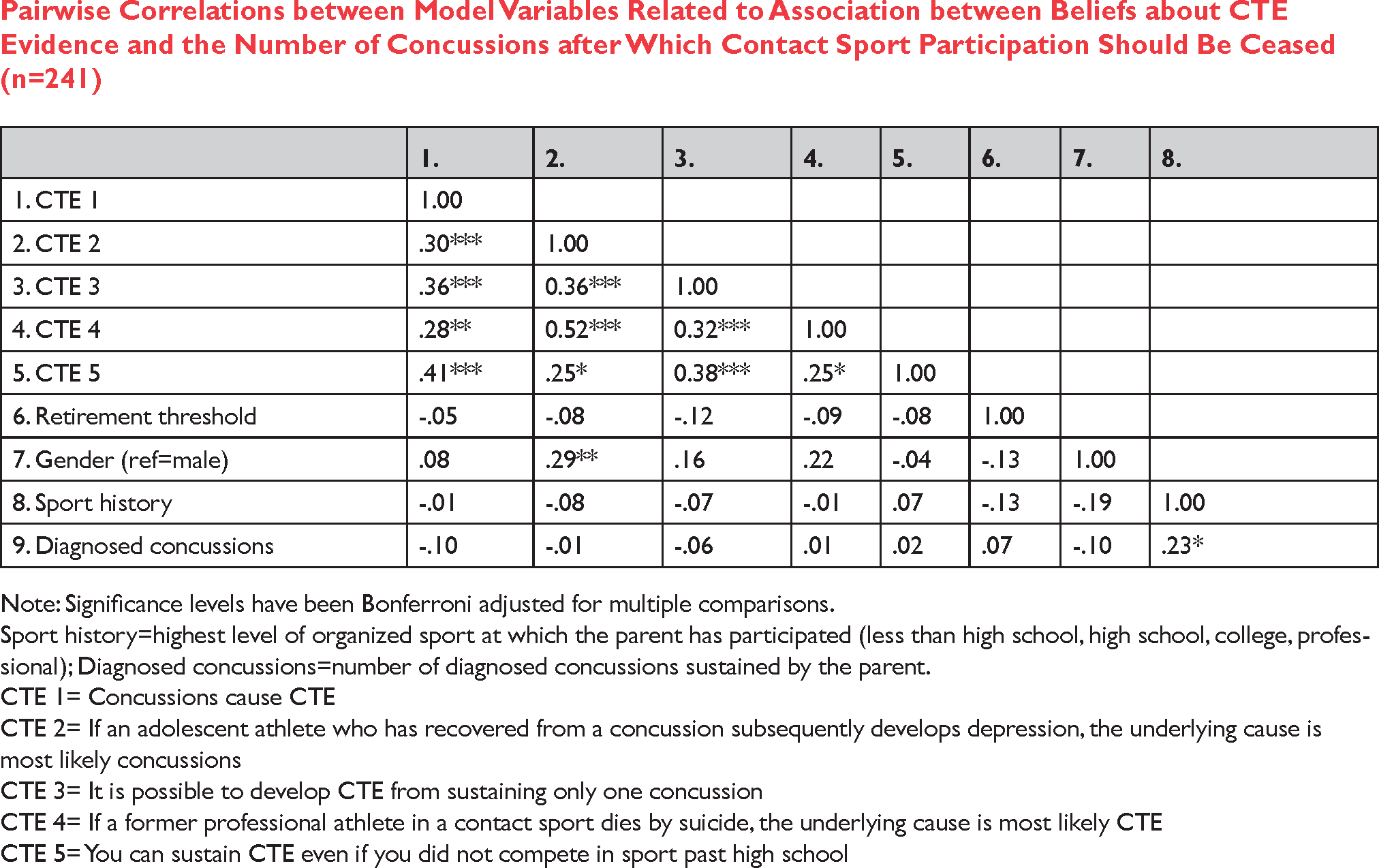
Pairwise Correlations between Model Variables Related to Association between Beliefs about CTE Evidence and the Number of Concussions after Which Contact Sport Participation Should Be Ceased (n=241)
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | |
|---|---|---|---|---|---|---|---|---|
| 1. CTE 1 | 1.00 | |||||||
| 2. CTE 2 | .30*** | 1.00 | ||||||
| 3. CTE 3 | .36*** | 0.36*** | 1.00 | |||||
| 4. CTE 4 | .28** | 0.52*** | 0.32*** | 1.00 | ||||
| 5. CTE 5 | .41*** | .25* | 0.38*** | .25* | 1.00 | |||
| 6. Retirement threshold | -.05 | -.08 | -.12 | -.09 | -.08 | 1.00 | ||
| 7. Gender (ref=male) | .08 | .29** | .16 | .22 | -.04 | -.13 | 1.00 | |
| 8. Sport history | -.01 | -.08 | -.07 | -.01 | .07 | -.13 | -.19 | 1.00 |
| 9. Diagnosed concussions | -.10 | -.01 | -.06 | .01 | .02 | .07 | -.10 | .23* |
Note: Significance levels have been Bonferroni adjusted for multiple comparisons.
Sport history=highest level of organized sport at which the parent has participated (less than high school, high school, college, professional); Diagnosed concussions=number of diagnosed concussions sustained by the parent.
CTE 1= Concussions cause CTE
CTE 2= If an adolescent athlete who has recovered from a concussion subsequently develops depression, the underlying cause is most likely concussions
CTE 3= It is possible to develop CTE from sustaining only one concussion
CTE 4= If a former professional athlete in a contact sport dies by suicide, the underlying cause is most likely CTE
CTE 5= You can sustain CTE even if you did not compete in sport past high school
Appendix
Fit Statistics for Parent Responses (n=241)

| Model | Df | Chi2 | p | CFI | TLI | RMSEA | Diff test p |
|---|---|---|---|---|---|---|---|
|
|
|||||||
| CTE evidence | |||||||
| Base model | 5 | 21.02 | 0.001 | 0.901 | 0.802 | 0.125 | |
| Depression and suicide 1 | 4 | 2.80 | 0.592 | 1.00 | 1.02 | 0.000 | <0.001 |
|
|
|||||||
| Model 1 2 | 8 | 3.19 | 0.922 | 1.00 | 1.06 | 0.000 | |
| Model 2 3 | 12 | 21.81 | 0.040 | 0.946 | 0.906 | 0.058 | |
| Model 3 4 | 16 | 24.706 | 0.075 | 0.953 | 0.921 | 0.047 | <0.001 |
| Model 4 5 | 20 | 27.628 | 0.118 | 0.958 | 0.931 | 0.039 | <0.001 |
“Depression and suicide” adds a correlation between depression and suicide items to base model.
Model 1 is the association between CTE evidence and number of concussions at which participation in contact and collision sports should be ceased (retirement threshold).
Model 2 adds to Model 1 gender as a predictor of CTE evidence and quit number.
Model 3 adds to Model 2 own sport history (highest level of sport in which the responding parent participated) as a predictor of CTE evidence and quit number.
Model 4 adds to Model 3 number of diagnosed concussions as a predictor of CTE evidence and quit number.