
Abstract
This article is about the recent and profound changes in the conceptualization of dementia, especially the turn towards prevention. The main argument is that more attention needs to be paid to “situated prevention” — the framing of internationally circulating data on the “new dementia” in different contexts. After introducing some of the more problematic issues related to the “new dementia,” a first comparison of major preventive clinical trials in Europe and in North America will be provided. The major insight stemming from situating the global message of preventing dementia is recognition of the responsibility researchers and policy makers bear with respect to the implicit and potential moral narratives in emerging scientific landscapes.
In the early 1980s, biographies and autobiographies from U.S. authors about living with dementia often depicted the dramatic search for a diagnosis, 1 at a period of time when Alzheimer's disease was only starting to become better known to the general population — even among some doctors. 2 During the 1990s — declared the “decade of the brain” by former president George Bush — this changed, and a greater awareness regarding the first signs of dementia resulted in much earlier diagnoses. In some contexts this resulted in what Adelman 3 called the “Alzheimerization of aging”: a concentration of resources going to research about Alzheimer's disease to the detriment of other aging-related issues. This was increasingly paired with a hyper-vigilance among aging individuals, leading to a general anxiety regarding signs of forgetfulness. 4 However, interventions generally only began when symptoms interfered with daily life, and the whole idea of prevention remained absent from public discourses on dementia, except for rather ambiguous ideas about “brain training” in the later years (e.g., learning languages and doing crossword puzzles).
What I want to call here the “new dementia” consists mainly of two recent and profound epistemological changes. 5 1. Current research agendas show a major effort to develop means for reliable, early, ideally pre-symptomatic detection (through biomarkers such as found in the cerebrospinal fluid and through brain scans) or of detecting very early symptoms, therefore placing a lot more importance on mild cognitive impairment (MCI) than in the past. 6 Some also argue that first noticeable changes should be called Mild Behavioral Impairment (MBI), 7 since slight behavioral alterations seem to precede cognitive impairment — both extremely imprecise signs of change observed usually in the elderly, though sometimes in younger individuals as well. The category “mild cognitive impairment” that has existed at least since the 1960s 8 refers to the observation that initial complaints of memory loss may or may not develop into a dementia. Now, however, MCI is becoming increasingly part of the general dementia syndrome, although this perception is contested and context-dependent on (see below).
2. The focus of this article will be on the second change, although it often cannot be separated from the first point. Until recently dementia was understood by the general public in many countries as a mixture of destiny and family history, 9 and the afore-mentioned recommendation of “brain training” almost the only preventive practice aging people and health professionals were aware of. 10 Now, however — and similar to arguments made regarding other syndromes (e.g., Parkinson's disease, schizophrenia) — researchers argue that interventions for Alzheimer's patients happen far too late, a point that is also commonly made in explaining the need for early detection. A common argument today and widely propagated by media internationally, is that “[o]nce someone has dementia there is already an advanced stage of brain degeneration. It takes an estimated 10 to 20 years for dementia to become obvious (…). But if we can identify people in this pre-symptomatic phase, (…) we may be able to treat them with drugs and recommend lifestyle changes that delay or even stop the disease's progression.” 11
In the following pages these recent changes will be briefly discussed, followed by the central argument of this article, namely that what I call “the new dementia,” and especially the aspect of prevention, needs to be “situated.” My claim is that paying more attention to a critical contextualization of prevention will lead to a more nuanced analysis of recent changes in dementia research and to a greater awareness of what is at stake for aging individuals.
The New Dementia
Starting more or less in 2007, 12 changes in the conceptualization of dementia have resulted in (a) an intense and contested search for predictive biomarkers in a pre-clinical phase — often targeting individuals in their 40s or even earlier; (b) the study of very first signs — the greater emphasis on Mild Cognitive Impairment already mentioned — and finally, (c) the insight that the prevention of dementia is possible. One reason for these conceptual changes springs from the need to explore new avenues of treatment after the continued failure of drug trials and the limited effect of currently existing specific medications for dementia. 13 A 2012 study by the Pharmaceutical Research and Manufacturers of America (PhRMA) showed that in the 13 previous years, 101 Alzheimer's drugs failed in testing and so would not reach the market. 14 As I have argued elsewhere, 15 early detection and preventive measures — a “critical turning point in the history of the field” 16 — were not only related to the growing insight that current specific dementia medications were inefficient (with sometimes severe side effects), but that, in effect, dementia, especially in very old age, is tied up with the overall breakdown of the aging organism, rather than a neatly isolated, specific disease. As Richards and Brayne had already argued in 2005, 17 “It is timely to interrogate the term Alzheimer's Disease. In older age groups, AD seems to be a diffuse clinical syndrome representing the gradual accumulation of multiple pathologies, arising from multiple interlocking risk factors over the life course. The term Alzheimer's syndrome seems more appropriate.” And Molin and Rockwood 18 in their critical discussion of an early detection of dementia point out that “biomarkers' ability to distinguish normal subjects from AD patients lessens with age. The typical pattern of AD-related (…) brain changes seen in the young old (…) appears to be less salient in very old patients (…), despite similar levels of cognitive impairment.” In other words, for older people it is the complexity and the accumulation of many coexisting conditions that seem to be strongly related to cognitive decline, something that is nearly impossible to cure or slow down with a single drug. It is among the affected younger old that the typical Alzheimer's pathology is more easily distinguishable from an aging process, something that would confirm Alois Alzheimer's description in 1907 of the early onset form of dementia as “peculiar” and different from the syndrome detected in older people — a point that has been debated ever since. 19
Further, earlier studies showing a high correlation between first signs and a concomitant dementia among patients recruited from clinical settings were relativized by more recent research in community settings, in which early signs of forgetfulness developed less often into a dementia. These insights serve to question the usefulness of the category “Mild Cognitive Impairment” understood as an early phase of Alzheimer's syndrome. Finally, clinical trials testing substances which are supposed to clear the brain's most prominent biomarker, ß amyloids, has not lead to any improvement of dementia, showing that looking only at ß amyloids will probably not lead to a cure, something that is now well known and accepted, including by the pharmaceutical industry. 20 Recent headlines concerning the Pharma company Pfizer announcing its desisting from research on dementia, is but one sign of the difficulty of targeting a complex condition like Alzheimer's disease (as well as other kinds of dementia), and especially the hope for a blockbuster drug.
Related to the idea of early detection and intervention is the growing awareness that prevention of dementia might be possible: One third of cases could be prevented, mostly through lifestyle interventions, suggests a recent Lancet commission,
21
though others are skeptical about making such direct links.
22
In other words, often-heard public health recommendations, easily merged with ideas regarding active and successful aging — for instance, avoiding sedentarism, smoking, and unhealthy food — are now also applicable to dementia: [L]arge cohort studies have implicated multiple health factors that may increase the risk for developing cognitive decline and dementia thought to be caused by AD. (…) In particular, vascular risk factors such as hypertension, hypercholesterolemia, and diabetes have been associated with an increased risk of dementia.
23
Cardiovascular risk factors have previously been linked to vascular dementia (due to mini strokes), although even in this case, until recently, prevention was not explicitly a major public health issue. Now, however, the once separate categories “vascular dementia” and “Alzheimer's disease” are increasingly perceived as merging with regard to aetiology and common risk factors. 24 The link between Alzheimer's disease and cardiovascular risk factors has been known at least since the beginning of the 1990s, but was widely ignored, largely because Tacrine, the first dementia-specific medication arrived on the market in 1993 25 and a blockbuster drug approach tended to be privileged over a more complex explanatory pathway.
The recent reconfiguration of the conception of dementia as preventable is gaining currency circulating internationally, and with it the recommendation to manage risk factors such as diabetes, depression, hypertension, smoking, poor diet, hearing loss in middle age, air pollution, as well as ongoing education and cognitive stimulation. However, prevention is not an unproblematic or straightforward concept, hence my claim that prevention needs to be contextualized — that more attention needs to be paid to “situated prevention.”
The recent reconfiguration of the conception of dementia as preventable is gaining currency circulating internationally, and with it the recommendation to manage risk factors such as diabetes, depression, hypertension, smoking, poor diet, hearing loss in middle age, air pollution, as well as ongoing education and cognitive stimulation. However, prevention is not an unproblematic or straightforward concept, hence my claim that prevention needs to be contextualized — that more attention needs to be paid to “situated prevention.”
Short Overview of Prevention as a Sociological Object
It is a commonplace and widely propagated notion these days that prevention should be seen as an investment in one's health, which at the same time lowers costs of health care systems increasingly solicited by the aging baby boomers. Social scientists have frequently criticized this kind of reasoning as neo-liberal and paternalistic, which has the effect of shifting blame for healthcare costs onto those who do not adhere to public health recommendations.
Much has been written about prevention by social scientists, so that here only a short overview of arguments will be provided. 26 Scholars have shown, for example, that preventive measures — those that are at the heart of public health campaigns — can be understood as a biomedicalization of the life course 27 with regard to a “new public health.” 28 Keywords in critical prevention discussions are, among others, healthism, the normalization of the body, responsibilization, and risk management. 29 Related to this is the important critique that neoliberal ideologies are transforming public responsibilities and structural factors into private concerns 30 or, as Mayes 31 recently observed regarding obesity, “a focus on the individual is ethically questionable, ineffective and ignores relevant research that suggests systemic factors, not individual choices, are behind the epidemic.” Aronowitz 32 further warns of the danger of conflation, when — as it well might well happen with “the new dementia” — being at risk is experienced as illness itself, leading to the possibility of years lived in anxiety, as well as stigma and unnecessary interventions.
I want to link the following reflections about the “new dementia” to existing discussions on prevention, lifestyle and public health 33 and, equally, to studies within the domain of a critical gerontology, especially to what Stephen Katz 34 has called “lifestyle in social context.” Recommendations in public health campaigns concerning both successful aging 35 and the prevention of dementia target individuals making responsible choices, which, as Katz writes, should take into account how “the recent individualistic story of lifestyle, the one that leads to improving or lengthening lifespan, […] positions lifestyle in the myriad of life chances, status hierarchies and social contexts.” 36
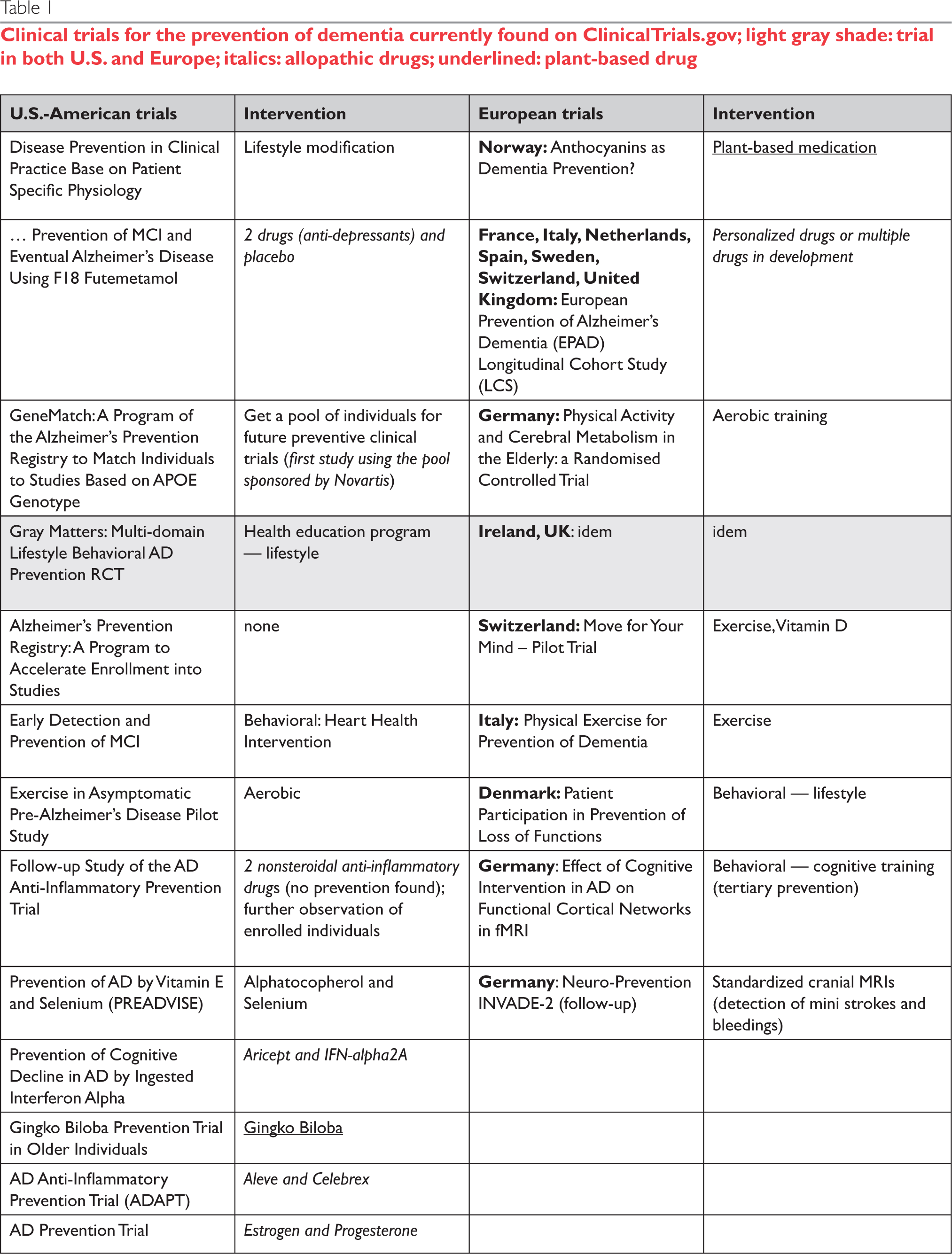
Clinical trials for the prevention of dementia currently found on ClinicalTrials.gov; light gray shade: trial in both U.S. and Europe; italics: allopathic drugs; underlined: plant-based drug
Situated Prevention
Situatedness emphasizes the context-dependency of a phenomenon — here, prevention. As defined by Chandler and Munday,
37
situatedness relates to [t]he dependence of meaning (and/or identity) on the specifics of particular sociohistorical, geographical, and cultural contexts, social and power relations, and philosophical and ideological frameworks, within which the multiple perspectives of social actors are dynamically constructed, negotiated, and contested.
One aspect of Donna Haraway's well-known reflections on situated knowledge 38 is especially relevant to this article, namely her claim that situatedness does not mean relativism, but responsibility regarding multiple existing kinds of knowledge. In other words, it makes a difference which of the many existing or possible (moral) narratives are being privileged when talking about the prevention of dementia.
Situatedness can be studied on different levels. In this article, an analysis comparing major prevention initiatives in North America (especially in the U.S.) and in Northern Europe will be emphasized. There are differences that can be observed between nations or, more precisely, between different epistemic cultures 39 — that is, “glocal” scientific models and traditions and their translations into concrete recommendations and ways of living. The following differences, detected when comparing North-American and European preventive initiatives might initiate a discussion about how the conceptualization of prevention and its concomitant recommendations can have an impact on the way individuals age.
Methods Overview
Relying on the author's earlier studies on epistemological changes in dementia research, the general context of this article has been conceptualized. 40 Recent national and transnational major research initiatives (clinical trials) in Europe and North America targeting prevention of dementia (studies that were often conceived in combination with an early detection) were then listed, and the general objectives of these initiatives studied. The main source was the site ClincalTrials.gov (n=22 relevant trials in North America and Europe) and related sites that provided additional information regarding the listed trials. The websites of different Alzheimer Societies/Associations — arguably the most influential sources for those worrying about dementia — were studied in order to see which prevention trials were discussed on those sites, as well as explicit recommendations posted for their readers (the U.S. Alzheimer's Association, Alzheimer Society Canada, and Alzheimer Europe and its sub-sections). Although Alzheimer's Society and Associations were more often a direct source of information in the U.S. when compared with Europe, 41 other informational material in Europe (newspaper articles, community groups, etc.) rely on them in order to inform their readers and members.
A summative content analysis 42 provides a first reflection on the discovered differences and their possible impact on older individuals and societies at large, although further (ideally longitudinal) studies are needed in order to determine how explicit and implicit recommendations from those prevention studies are being concretely incorporated into people's everyday lives and transformed into health and social policies in different countries.
Prevention Studies in Europe and in North America
Studying recent European and U.S. clinical trial initiatives found on the site ClinicalTrials.gov, it appears at first sight that the objectives and study designs of preventive interventions are similar: Recommendations of lifestyle changes and pharmaceutical interventions can be found on both continents. However, in Europe, only the EPEAD study is testing allopathic drug interventions. “As yet, there is no preventative or curative treatment for Alzheimer's disease,” one reads on the Alzheimer Europe website, while a major initiative funded by them — The European Collaboration on Dementia — targets lifestyle changes as the future treatment options.
On both continents early detection and early intervention is recommended. After a survey conducted in 2011 by the Harvard School of Public Health and Alzheimer Europe in the U.S. and four European countries, a “great public desire to seek early diagnosis of Alzheimer's” emerged. 43 This result indicates that the recent turn towards a “new dementia” has reached, at least partly, the general public on both continents. Financed by Bayer Pharmaceuticals, this survey was conceived in order to see whether individuals in those five countries were interested in early testing (67% were interested). This high degree of interest needs to be seen in conjunction with high expectations regarding currently available medications as effective in slowing down the progression of AD, especially in Poland (63%) and the U.S. (47%), while the other European countries score lower in this regard.
Both the U.S. and E.U. Alzheimer Societies describe currently available medications as having only a temporary effect for some patients, and make clear that some risk factors (age, gender, genetics) cannot be changed, but suggest there are modifiable risk factors that have an influence on the epidemiology (and epigenetics) of dementia. On the U.S. website, hope exists that in the future, drugs will be developed that address the complexity of the dementia syndrome: “many of the new drugs in development aim to modify the disease process itself, by impacting one or more of the many wide-ranging brain changes that Alzheimer's causes. (…) Many researchers believe successful treatment will eventually involve a ‘cocktail’ of medications aimed at several targets, similar to current state-ofthe-art treatments for many cancers and AIDS.” 44 Although lifestyle factors are mentioned, prevention trials are clearly described as Pharma-based interventions, and larger trials are then listed, which cannot be found on the ClinicalTrials.gov website, but that have been strongly mediatized in the last years.
When looking at those larger, transnational and relatively well mediatized clinical trials, differences between Europe and the U.S. become more clear-cut.
Discussion
All in all, a tendency exists in which prevention in the North American context — though this may be less accentuated in Canada
45
— is described as primarily emphasizing drug interventions, while in Europe lifestyle changes are more in the foreground. As an example: The participants [from the U.S.] receive solanezumab, an antibody-based drug that aims to reduce brain amyloid-beta, which recently failed to improve mild Alzheimer's dementia. Despite the failure, researchers speculate the drug may be effective in preventing dementia in people who have amyloid-beta aggregates in the brain.
46
The PREVENT study, based in the U.K., is an example of how the same problem (early detection and prevention) is described as being achieved primarily through lifestyle-related changes: Recent research suggests changes in the brain may precede symptoms of Alzheimer's disease by many years. (…) Our research (…) focuses on people in middle age to identify biological and psychological factors which may increase the risk of dementia in later life. Once we have identified which factors are changing we would like to select those people at high risk and intervene in this process. These interventions might be lifestyle changes or measures to affect the risk of an individual developing dementia.
47
The North American dementia models rely more often on brain-based biomarkers compared to European studies, while the latter seem to privilege the heart-head connection (“what is good for your heart is good for your brain”) as the central model framing preventive interventions, although, as Anstey and Peters 48 argue, the heart-head connection is often communicated in an oversimplified way and, therefore, is sometimes as reductionist as some proposed drug interventions. 49 Also the use of medications in the first case is based on a logic of biomarkers generally found in tissues and body fluids made visible (regarding different kinds of biomarkers), while in the European context medications are being used primarily in order to improve concomitant health conditions (diabetes, hypertension, etc.) conceived as risk factors — two different kinds or levels of biomarkers and medication use. 50
This difference is especially relevant today, a time in which health and illness are increasingly being conceived using a future-oriented process Metzler calls “biomarkerization.” 51 One of the consequences of this process is the blurring of previously existing boundaries between health and illness, and more inclusive thinking regarding presymptomatic individuals who easily become presymptomatic patients. And although brain-based biomarkers are often indeterminate — as is the case with those linked to Alzheimer's disease — their central feature, that of being a sign and therefore suggesting concreteness and certainty, can transform a single person, or even whole groups, into individuals who are apparently at greater risk of contracting or already having the disease. As Baker 52 convincingly showed, the great interest in research on biomarkers is directly linked to the desire for more cost-effective and quicker drug development — see, for example, the current large patient register initiatives for prevention trials.
However, the differences detected between European and North American prevention studies are not as clear-cut as they might seem at first sight. First, many of the trials based in Europe also include samples from North America, and vice-versa (e.g., the EMERGE study is also taking place in several European countries). Furthermore, major joint initiatives, dominated by the pharmaceutical industry, have been sharing forces in order to reduce the costs of clinical trials, speed up the time of recruitment, and standardize procedures across sites, making it difficult to separate results of these studies from commercial interests. 53 As an example, the U.K.-based Dementia Discovery Fund (see http://www.theddfund.com/) works with researchers from around the world and is clearly drug-focused: “Our goal is to invest over $200m over fifteen years to support the creation of novel disease-modifying drugs for dementia,” it reads on their website, of an initiative that is sponsored by “[t]he Department of Health, the charity Alzheimer's Research UK and (…) six pharmaceutical firms [that] have raised $100m (£65m) to invest in early-stage, novel treatments for (…) dementia (…) [T]he company is joined by the US drugmakers Johnson & Johnson, Biogen, Eli Lilly and Pfizer, and Japan's Takeda.” 54
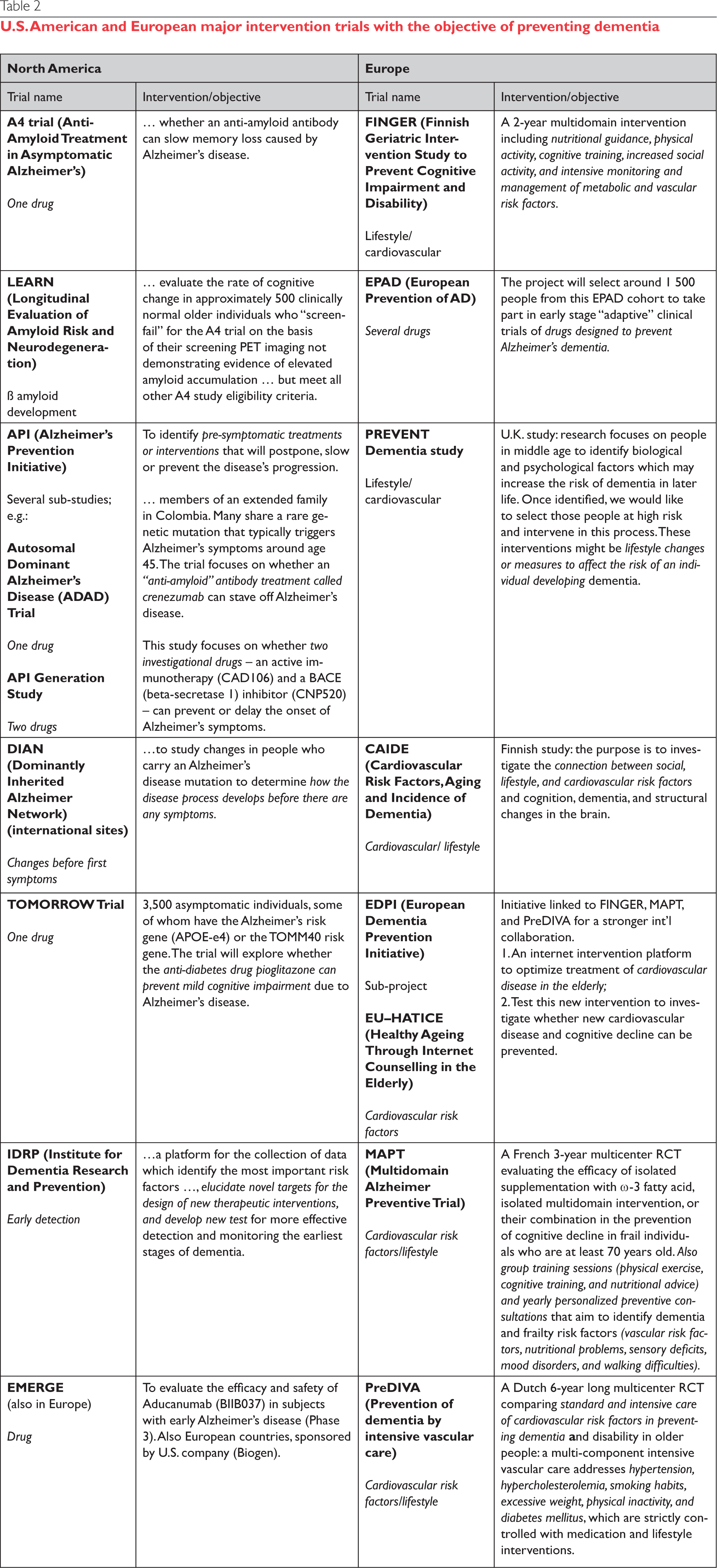
The international, U.S.-based Global Alzheimer Platform 55 has a similar objective: “the GAP Foundation is joining together leading academic researchers, pharmaceutical companies, nonprofit organizations and foundations, and governments around the world to reduce the time, cost and risk of Alzheimer's clinical trials, in order to speed innovative medicines to those with or at risk of Alzheimer's disease.” This initiative is associated with the European EDPI study (see table 2).
U.S. American and European major intervention trials with the objective of preventing dementia
It might be though that the international initiatives (here: those targeting European and U.S. publics) influence or even render irrelevant the differences detected between the American and European prevention studies. Molin and Rockwood 56 believe that the turn toward integrating pre-clinical phases into the dementia syndrome itself will continue to be more important in North American, with the result that these differences will persist. European researchers also are more sceptical of the concept of Mild Cognitive Impairment than their American counterparts, 57 which means that some forgetfulness is treated as a normal part of aging and so, is less likely to be pathologized.
A significant factor explaining these differences is the media, an important vehicle of knowledge transmission. In the U.S., historically the media has become more closely related to interest groups and is less controlled by the state than in Europe. 58 Additionally, and related to the previous point, pharmaceutical products may be advertised in the U.S., but generally not in Europe, which suggests that it is easier for U.S. companies to transmit desired messages — and the underlying scientific models — to clients, prescribing doctors, and policy makers as compared to Europe. 59 Furthermore, as Hunt, Kreiner and Brody 60 showed for the U.S., national guidelines that instruct and guide the majority of prescribing clinicians are often heavily influenced by the pharmaceutical industry, in many cases resulting in “polypharmacy”: the prescription of more drugs to moderate the effects of already-prescribed medications.
Although the differences between European and American media and Pharma practices are not new — and, in fact, well-known ideas — the point here is that facts regarding the “new dementia” are generally being propagated as if they were universal facts and situational differences are rarely taken into account.
For instance, since most dementia risk factors are correlated with socioeconomic status, management of them is dependent on access, for those at risk, to certain resources, so the prevention of dementia becomes in part a political discussion about living conditions in different societies. Or, as Strighini et al. 61 recently recommended in a Lancet article, “socioeconomic adversity should be included as a modifiable risk factor in local and global health strategies, policies, and health-risk surveillance.”
Another point to consider is that in some regions of the world (generally, parts of richer nations) dementia prevalence and incidence rates are declining, for instance in the U.S., 62 Holland, 63 Sweden, 64 and England. 65 These findings are creating some optimism — and the sense we might move “from muddled diagnosis to treatable mechanisms.” 66 But they also show that preventive interventions are tightly linked to sociopolitical factors: The longitudinal multi-domain Dutch PreDiva study (“Prevention of dementia by intensive vascular care”), aimed at reducing cardiovascular risk factors through nurse-led interventions targeting individualized lifestyle changes and drug treatments for hypertension and diabetes, arrived at no signifi-cant result. Researchers think that this is due to the fact that in Holland people are already quite well taken care of, through good quality health care, with regard to the most important risk factors, and they suspect a major impact of the studied interventions would have been noticeable in contexts with a less efficient health care system. The study nevertheless showed some effect for people who had untreated hypertension at baseline. 67
Researchers publishing in the two British journals The Lancet and BMJ that were involved in the “statin war” — also relevant to dementia research because of a possible preventive effect of statins on cardiovascular health — debated the usefulness of aggressive prescription of statins in the U.S. against its lower rate of prescription in Europe (where it tends to be combined with a greater emphasis on the “Mediterranean diet”). This is another example of a debate that shows that differences must not be merely acknowledged, but that, ideally, the origins of such differences, and their impacts on people's lives, need to be understood. 68
Conclusion
Major scientific insights generally circulate internationally and key findings are taken to be universally valid. When comparing conceptions of the “new dementia” and actual preventive dementia trials in North America with those in Europe, the core arguments are the same: current interventions happen too late, and preventable risk factors play a role in the aetiology of the “new dementia” (although this might only hold true for a mixed dementia and not necessarily the “pure” form of Alzheimer's disease 69 ). However, the translation of those core arguments into established facts happens in different ways, and this situatedness needs to be acknowledged in order to see that public health recommendations not only often ignore those factors that are linked to socio-political and economic issues, but also that they differ between sites. In sum, the central questions are whether different prescriptions will also have different impacts on the epidemiology of dementia and on what Nikolas Rose 70 called “somatic individuals” — the ever-increasing links being established between someone's biology and his or her conduct.
Future studies, including social science research, will need to pay attention to whether over time Americans begin to get a different message than Europeans about approaches to preventing Alzheimer's, how the “new dementia,” including the reading of biomarkers, will influence local health policies, and whether any of this will have specific impacts on aging individuals' attitudes toward themselves and others. Although it is not clear how exactly risk for dementia should be managed, what is apparent is that individualized attitudes are not enough: many commonly recommended changes evoke state responsibilities (providing good education, better food for all, cleaner air etc.), while others are individual choices, modified by lifestyle changes or by drugs 71 (for an extensive discussion see note 71), although this simple division between the state and the individual's responsibility obscures many complicating factors. It remains problematic that much of what constitutes “lifestyle” is usually considered an individual choice, ignoring the role society plays in providing conditions for choice (e.g., parks in neighborhoods, good schooling).
Future studies, including social science research, will need to pay attention to whether over time Americans begin to get a different message than Europeans about approaches to preventing Alzheimer's, how the “new dementia,” including the reading of biomarkers, will influence local health policies, and whether any of this will have specific impacts on aging individuals' attitudes toward themselves and others. Although it is not clear how exactly risk for dementia should be managed, what is apparent is that individualized attitudes are not enough.
It is important to disentangle the many co-existing narratives and see which are being privileged by whom, how early detection and prevention are being framed, whose interests the newer models serve, and what early detection means within a therapeutic landscape of uncertainty (e.g., until now biomarkers were not considered specific to dementia, and overlap with normal aging and other pathologies). The analytical category of “situated prevention” proposed here might contribute to a greater awareness regarding the framing of different factors involved in the “new dementia,” since risk factors come to life within moral narratives.
Footnotes
The author has no conflicts to disclose.
Acknowledgments
I am most grateful to the Social Sciences and Humanities Research Council (SSHRC) for funding my current research. A preliminary version of this article was discussed at the Brocher Foundation workshop, “The Redefinition of Alzheimer's Disease and its Social and Ethical Consequences”, organized by Richard Milne, Shirlene Badger and Jason Karlawish, April 14-15, 2016, in Geneva, Switzerland. Other parts of this text were presented at the Trent University meeting “Critical Intersections: Mild Cognitive Impairment, Aging and Dementia in Theory and Practice”, organized by Stephen Katz, May 7-8, 2015, and recently at the 2017 Canadian Anthropology Society (CASCA) conference, during the session “Movement of Medical Knowledge and Practice: Crossing Borders and Constructing Boundaries in a Global World,” organized by Loes Knaapen and Hanna Kienzler.