
Abstract
The U.S. and Canadian health care systems are more similar than is commonly believed. This article debunks some of the powerful myths about these health care systems and opens up the discussion for greater policy learning from both sides of the border. Cross-border comparisons can yield a number of lessons from common policy challenges such as cost control, physician organization and payment, and the organization of health coverage and services for Native Americans and Indigenous Canadians.
So close yet so far. These words apply with great force to how healthcare in Canada is perceived in the United States (U.S.) and vice-versa. U.S. proponents of major health reform regularly use Canada as Exhibit A in arguments around greater government involvement and single-payer financing. In Canada, the U.S. is demonized or lauded depending on where observers sit on the potential of private financing and delivery to improve performance. Myths and misperceptions — sometimes willful — about each health-care system abound.
In this article, we briefly examine the more common myths and misperceptions of the U.S. and Canadian health systems. However, our ambition is to reach beyond myth busting in the second part where we will highlight some lesser known facts about each system to open the possibility of greater policy learning on both sides of the border.
Myths and Misperceptions
Our Two Systems are Completely Different
It is a common misconception that the U.S. and Canadian health care systems are different in every respect. There is of course one big difference. In the U.S., the public system of financing and regulation was designed to fill the gaps left by private health insurance. 1 In Canada, a mix of private insurance and government and charitable programming was replaced entirely by government-financed universal health coverage for hospital and primary care. 2 In reality, however, both health systems have much more in common than this difference suggests.
First, federalism is the political and constitutional foundation of both systems. As a consequence, it is essential to understand the relationship between the federal and state/provincial governments in the both countries. 3 Although Canada is a more politically decentralized federation than the U.S., key programs such as Medicaid in the U.S. and single-payer Medicare in Canada, are administered and delivered at the subnational level in both countries. 4 At the same time, in both countries, the federal government plays a key role in setting standards through national laws including requirements to receive federal grants. 5 These similarities mean that, when it comes to the federalist dimensions of health care, the two countries can be usefully compared.
Second, universal health coverage (UHC) in Canada has been narrowly drawn relative to most Western European and the U.S. Medicare systems. Restricted to hospital and medical care, UHC in Canada excludes outpatient prescription drug therapies, dental care, most vision care, and social care including long-term care and home care. These non-UHC services are funded by a combination of private health insurance and out-of-pocket payments supplemented by some public services, subsidies, or supplementary plans for seniors and the indigent. 6 Therefore, when it comes to prescription drugs, ancillary health services and social care, Canada is actually more similar to the U.S. than it is to any Western European country, particularly in the patchwork way that it extends coverage.
Third, the education, training and work environment of health professions in both countries bears far more similarities than differences. 7 The organization of post-secondary education and the curriculum for the health professions is almost identical on both sides of the border. Specialized training, especially in the medical profession, is virtually identical with many physicians from one country pursuing fellowship training in the other country before retuning home to practice. Self-regulation is the norm for the health professions in both countries. These similarities encourage what is already a porous border in terms of professional mobility and shared intellectual environment. As a result, Canada must maintain competitive professional remuneration compared to the U.S. or risk a significant southward loss of doctors, nurses, and other professionals. Where there are differences is in the amount of clinician time consumed by administration, with the U.S. having historically much higher amounts of administrative burden because of the number of payors and the complexity of the reimbursement process. 8
We Have the Best Healthcare in the World so Why Bother Comparing Ourselves to a Country Whose System is Clearly Inferior
Based on some recent reports in the media in both nations, it would seem that this is a common view among both Americans and Canadians although for different reasons. Many Americans think that the Canadians are being held hostage to long wait times for medical care while most Canadians think that Americans who do not have insurance or the money to pay out of pocket are blocked from treatment. Although there are significant wait times for elective procedures such as hip and knee replacements and delays to see physicians, urgent conditions such as heart attacks or cancer are treated immediately in Canada. And while Americans without sufficient means may be discouraged from obtaining basic medical care, Medicare-certified hospitals must provide urgent and emergency care to anyone who shows up. 9
Based on the Commonwealth Fund's international comparison of health systems, both systems perform poorly on a number of quality and access indicators compared to other high-income countries. 10 This is particularly disturbing given the amount of money spent on healthcare in both countries — a poor value for money proposition in both cases but especially in the United States. As a consequence, policymakers in both countries should be humble enough to seek policy lessons from wherever they are available including lessons from each other.
Potential Policy Lessons from Little Known Facts
Myth-busting alone cannot tell us the potential policy lessons from each country. For this, we have to explore other aspects of each country's health system including some facts that are less obvious. This next section presents a few of the more promising areas that should be explored by policy decision makers.
Cost Control Within a Federalist Context
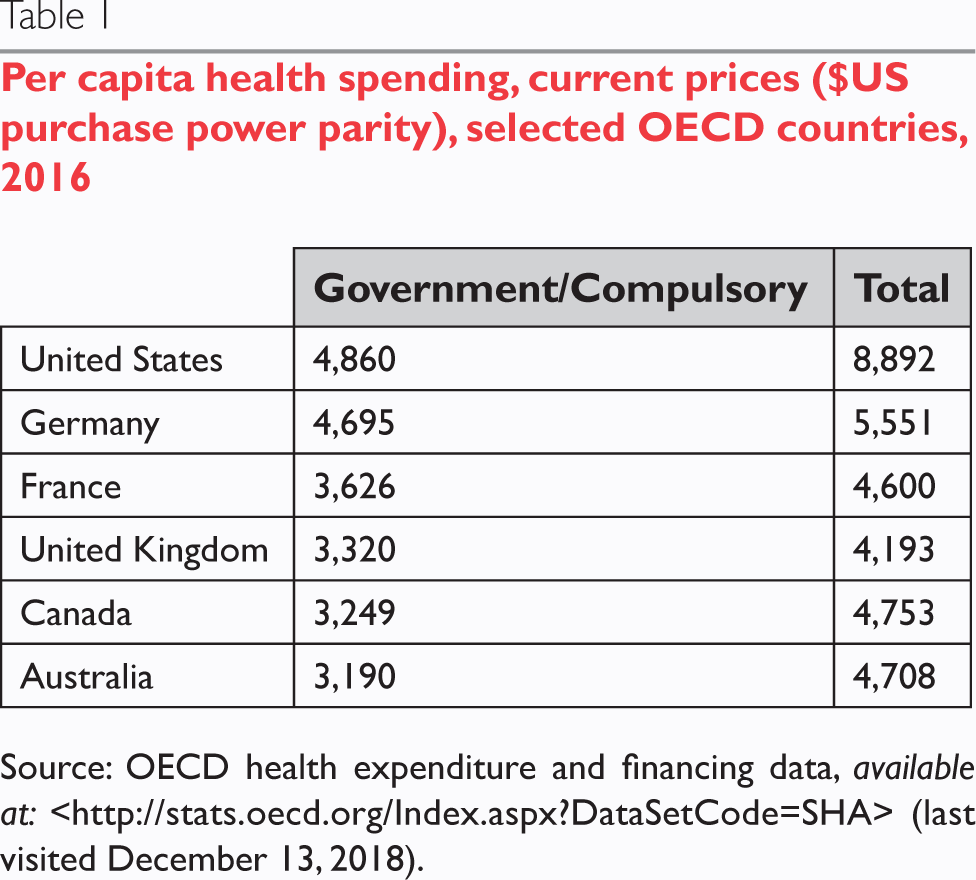
As shown in Table 1, the U.S. spends a great deal of public funds on healthcare through government programs such as Medicaid and Medicare. However, it is dollars spent on private insurance and healthcare in the U.S. that boost the country's total spending well above that of other OECD countries. As a result, the average American spends almost twice as much on healthcare as the average Canadian. This raises the question of whether policy makers in the U.S. can obtain some policy lessons on cost control from Canada and vice-versa for policy makers in Canada (at least in terms of what not to do).
Per capita health spending, current prices ($US purchase power parity), selected OECD countries, 2016
Governments in both countries have different experiences with the use of spending caps to control spending. In the 1990s, the U.S. federal government increased state power over their respective Medicaid programs to cap spending. 11 More recently, efforts to repeal and replace the Affordable Care Act have included proposals on per capita caps. 12 In Canada in the early to mid-1990s, a number of provincial governments used spending caps to reduce spending on physician care 13 and more broadly on health system spending. Recently, the provincial government of Ontario tried to re-introduce a physician spending cap that was strongly (and successfully) opposed by the Ontario Medical Association. It would be useful for policy makers in both countries to have a body of research comparing the design, effectiveness, and sustainability of this blunt policy instrument.
As a consequence of the debate over the future of the Affordable Care Act, there have been a number of proposals for the increasing use of largely unconditional block grants. This is a policy area from which U.S. decision makers might learn a great deal from Canada's forty-year experience with block grants. Although the Canada Health Transfer is conditional on provincial governments meeting five criteria in the Canada Health Act, these criteria are extremely light in their conditionality while monitoring and enforcement has been minimal. However, unlike Medicaid block grants in the U.S. which disconnect funding from both the number of beneficiaries and the cost of care, the Canada Health Transfer per capita formula — the main block transfer for health care — is based on the number of beneficiaries (i.e. all residents) even if it does not take into consideration other factors.
In both the U.S. and Canada, the argument for greater decentralization is to allow state and provincial government to tailor better their respective health programs to meet their specific needs. However, this benefit may be offset by the impact of growing regional disparities in both coverage and care. A rigorously designed study that researches this tradeoff in both countries could be of great benefit.
Physician Organization and Payment as Part of Health Reform
While the U.S. has led the way with new methods of compensating physicians, reimbursing hospitals, and encouraging integration through bundled or population-based payments, Canada has experimented in much more limited ways with narrow pay-for-performance schemes for physicians and global budgets for hospitals. In both countries the results of these different courses have been mixed. 15 The evidence on payfor-performance for physicians, almost anywhere in the world has been limited. However, new U.S. models of risk-based reimbursement for ACOs may offer better opportunities, even if recent reviews have shown limited impact. In what may be the most competitive market for healthcare in the world, the U.S. has relatively high levels of hospital and physician resources. In contrast, Canada has relatively low competition and overall resource levels but it has been able to control expenditure growth.
Given the greater range of experimentation with physician organization and payment in the U.S. relative to Canada (and most OECD countries), there is much to be learned from the U.S. experience on the Canadian side of the border. In particular, risk-based payments to ACOs should be of much greater interest to Canadians. In contrast, the large amount of time spent by U.S. physicians in interacting with multiple health plans and insurers compared to Canadian physicians interacting with a single payer suggests another avenue for learning.
Organizing Health Services for Native Americans and Indigenous Canadians
Native Americans and Indigenous Canadians have poorer health status and outcomes relative to the majority of their fellow citizens. This is a consequence of numerous factors including a colonial legacy that simultaneously required cultural and linguistic assimilation with physical segregation. From the beginning, health services for “Indians” were managed by the federal governments in both countries. With the introduction of UHC in Canada, provincial governments became responsible for providing medically necessary hospital and physician services to Indigenous Canadians although all other health services remained the responsibility of the federal government. 15 In the United States, however, health care by and large remains segregated for members of federally recognized tribes falling under the federal jurisdiction of the Indian Health Service. 16
In this commentary, we have put forward the case that there are many potential health policy lessons to be gained from comparing the United States to Canada, and Canada to the United States. In particular, in the areas of cost control, physician organization and payment, and the organization of health coverage and services for Native Americans and Indigenous Canadians, there is great potential for cross-border learning for scholars and decision-makers in each country. To facilitate this research, however, it is necessary to debunk two of the most powerful myths that have prevented rigorous and sustained comparative research in the past — the myth that health systems in the United States and Canada are so different that they cannot be usefully compared, and the myth that the other country's health system is so flawed that there is nothing on offer in terms of policy lessons.
Although public spending on Native American and Indigenous Canadian health services has increased faster than general public health spending in recent decades, this has not narrowed the health disparity gap. At the same time, there have been organizational innovations in both countries that have produced positive outcomes. In Alaska, for example, the Southcentral Foundation which serves approximately 60,000 Native Americans in south-central Alaska — “the Nuka System of Care” 17 — could be compared and contrasted with the nurse-led community health center model in the Northwest Territories and Nunavut. 18
Conclusion
In this commentary, we have put forward the case that there are many potential health policy lessons to be gained from comparing the United States to Canada, and Canada to the United States. In particular, in the areas of cost control, physician organization and payment, and the organization of health coverage and services for Native Americans and Indigenous Canadians, there is great potential for cross-border learning for scholars and decision-makers in each country. To facilitate this research, however, it is necessary to debunk two of the most powerful myths that have prevented rigorous and sustained comparative research in the past — the myth that health systems in the United States and Canada are so different that they cannot be usefully compared, and the myth that the other country's health system is so flawed that there is nothing on offer in terms of policy lessons.
Footnotes
Note
Hon. Cafaro reports other from Ohio Senate, outside the submitted work; and she was an elected official at the state level in Ohio from 2007 to 2016 and worked on health policy matters. The author notes her role as an elected official in no way has influenced anything she has worked on, but Hon. Cafaro feels it is important to be transparent and err on the side of caution. The other authors have no conflicts to disclose.