
Abstract
While risk of harm is an important focus for whether clinical research on humans can and should proceed, there is uncertainty about what constitutes harm to a trial participant. In Phase I trials on healthy volunteers, the purpose of the research is to document and measure safety concerns associated with investigational drugs, and participants are financially compensated for their enrollment in these studies. In this article, we investigate how characterizations of harm are narrated by healthy volunteers in the context of the adverse events (AEs) they experience during clinical trials. Drawing upon qualitative research, we find that participants largely minimize, deny, or re-attribute the cause of these AEs. We illustrate how participants' interpretations of AEs may be shaped both by the clinical trial environment and their economic motivation to participate. While these narratives are emblematic of the larger ambiguity surrounding harm in the context of clinical trial participation, we argue that these interpretations also problematically maintain the narrative of the safety of clinical trials, the ethics of testing investigational drugs on healthy people, and the rigor of data collected in the specter of such ambiguity.
Introduction
As part of drug development, pharmaceutical companies conduct Phase I clinical trials on healthy volunteers to test the safety and tolerability of investigational drugs. U.S. federal regulations provide oversight to protect these research participants and to limit their exposure to potential harm (45 CFR 46; 21 CFR 50, 56), whether the risks are physical, legal, economic, or psychological. 1 The current regulatory structure and related ethical guidance are largely reactions to twentieth-century cases in which human subjects were harmed as a result of their undue exposure to physiologic risk without informed and voluntary consent to research. 2 Thus, through informed consent processes and institutional review board (IRB) oversight, regulatory guidance aims to protect human subjects and to reassure society that clinical trial participation is safe. 3
Despite this notorious history, knowledge about the risk of research-related harm — whether regarding its nature, probability, magnitude, or duration — continues to be delusive, and the research community operates on problematic assumptions about what informed subjects can voluntarily agree to undertake in order to answer important scientific questions. 4 For example, the regulatory definition of “minimal risk” frames research risks in relation to the risk of daily life (45 CRF 46:102(i)), assuming that the latter is a self-evident metric against which the former can be weighed. The burden to do so falls on IRBs tasked with appraising the risk of harm to participants and ensuring that consent materials convey proper warnings of this risk. 5 Yet, IRBs differ in their deliberations about degree of risk and its necessary mitigation. 6 As a result, while assessing the risk of harm to participants is clearly a critical part of the protection of human subjects, normative standards for doing so remain uncertain.
In Phase I trials in particular, risk of harm is directly related to the collection and reporting of data on adverse events (AEs). 7 While the phrase “adverse event” may connote something quite grave to an outsider, it, in fact, encompasses all physiological signs and symptoms or medical events experienced by participants during a clinical trial. The term intentionally leaves open the possibility that bodily changes experienced by participants could be explained by the investigational drug, a nocebo effect, or chance, among other plausible reasons. Causation is immaterial to the full accounting of AEs required of investigators.
Although documenting and measuring harm are the primary purposes of Phase I trials, the process is plagued with ambiguity and problems. Identifying a drug-related harm — as opposed to an AE — requires first recognizing a bodily change, either through physiological markers or participants' self-report. Then, only after the conclusion of the clinical trial, investigators and the pharmaceutical company sponsoring the trial adjudicate which AEs were likely caused by the investigational drug and can therefore be classified as “side effects.” The remainder of the bodily changes experienced by trial participants are discounted as unrelated to the drug. Discounting them often translates into their disappearance from the reported trial results, though not necessarily from the view of any participant. While there are cogent scientific reasons to disambiguate Phase I trial participants' signs, symptoms, and medical events from their causes in this way, 8 the retrospective sorting of AEs by presumed causation makes attribution of harm nearly impossible during the trials. Importantly, this leaves space for participants to develop their own narratives surrounding if and why they have experienced harm as a result of their participation.
Drawing upon qualitative research, we analyze how characterizations of harm are narrated by healthy volunteers themselves. By focusing on participants' stories of AEs that occur to them or others during clinical trials, we describe how they make sense of those experiences of potential harm. We find, with little exception, that participants minimize, deny, or re-attribute the cause of AEs. To explain this phenomenon, we illustrate how participants' interpretations of AEs may be shaped both by the clinical trial environment and their economic motivation to enroll.
Extant research on Phase I trial risks typically reports on AEs because they are readily available and quantifiable. This approach tends to ignore the ambiguity surrounding harm that is embedded in the trial process. Meta-analyses of Phase I healthy volunteer trials indicate they are relatively safe, but AEs are very common. 9 One such study found that 65% of participants had at least one per trial, with most of these AEs characterized as minor and temporary, such as headaches and gastrointestinal (GI) changes. 10 However, further gradation of AEs is often absent in these meta-analyses, thus leaving the magnitude (intensity) or duration of the headache or GI distress unmeasured in terms of its “daily life” comparator. Moreover, although it is rare, healthy volunteers have also died or suffered serious injuries as a result of their participation. 11 Thus, AEs exist along a spectrum that includes the ambiguous category of “everyday risks” described in the statutory minimal risk definition, an uncertain area of more severe experiences, and also catastrophic harms. Still, these published cases of AEs in Phase I trials provide little insight into how healthy volunteers themselves perceive the significance of these harms.
Most healthy volunteers enroll in Phase I trials despite the risk of harm in order to receive the financial compensation. 12 Because participants are normally required to consent to a confinement period in a residential research clinic for some portion of, if not the entire, clinical trial, 13 these studies typically pay $100-300 per day. 14 Indeed, some lengthy studies even offer several thousand dollars. 15 Because the level of compensation for Phase I trials is strikingly high compared to later-phase trials, scholars have voiced concern that it acts as an undue inducement that leads participants to accept risks they would otherwise say were unacceptable 16 as well as to encourage them to enroll serially in these trials. 17 With AEs as common occurrences in Phase I trials, however, it is important to examine how healthy volunteers might interpret the bodily changes they experience, particularly in terms of harm.
Drawing upon qualitative research, we analyze how characterizations of harm are narrated by healthy volunteers themselves. By focusing on participants' stories of AEs that occur to them or others during clinical trials, we describe how they make sense of those experiences of potential harm. We find, with little exception, that participants minimize, deny, or re-attribute the cause of AEs. To explain this phenomenon, we illustrate how participants' interpretations of AEs may be shaped both by the clinical trial environment and their economic motivation to enroll. While these narratives are emblematic of the larger ambiguity surrounding harm in the clinical trial process, we argue that these interpretations maintain the narrative of the safety of clinical trials and the ethics of testing investigational drugs on healthy people. Participants' denial of harm is not only a self-serving narrative that allows them to continue to enroll in clinical trials, but ultimately, it also buttresses the research enterprise by maintaining a pool of willing participants to enroll in Phase I trials.
Methods
This article draws upon interviews from a single-wave of data collection from a longitudinal study on healthy volunteers' experiences in Phase I trials, which has been described in more detail elsewhere. 18 The goal of the longitudinal study was to assess how healthy volunteers' perceptions of, decisions about, and behaviors surrounding clinical trial participation change over time. To this end, between May and December 2013, our research team recruited and enrolled English- and Spanish-speaking healthy volunteers from seven U.S. research clinics while they were participating in various Phase I trials. Our team was not affiliated with any of these clinics, each of which gave permission to recruit participants but otherwise had no involvement in the design or execution of our study. Following in-person recruitment and enrollment, subsequent study activities occurred remotely by telephone or online. Our study was reviewed and approved by the Biomedical Institutional Review Board at the University of North Carolina at Chapel Hill.
The data we use in this article come from semi-structured interviews that were conducted in 2014 with participants one year after their enrollment in our study. This included 131 participants, comprising 90% of those with whom we attempted follow-up. We chose these study data because this wave of interviews included the most relevant questions for our analysis. Specifically, participants were asked to reflect on their or others' experiences of AEs, their perception of the frequency of AEs in Phase I trials, and their beliefs about why these AEs occur. Each interview was conducted by phone, recorded with permission, then transcribed by an independent company. Transcripts were verified and corrected for accuracy by a member of the research team. Using Dedoose qualitative analysis software, two team members coded each transcript to ensure completeness of code applications. Data analyzed for this article include all transcript excerpts coded as “Adverse Events/Side Effects.” This code was applied when participants spoke about their or others' AE experiences, including any of their remarks on the subject that were not specifically prompted by our interview guide.
The demographic characteristics of our sample are detailed in Table 1. The majority of our participants were men (75.6%) and racial or ethnic minorities (65.6%), which is common of U.S. healthy volunteers more generally. 19 Participants were predominantly over 30 years of age (81%). Only roughly one-third (35.9%) of our sample were employed full-time. The remaining participants were employed part-time (16.8%), self-employed (25.2%), and unemployed or retired (22.1%). Most (84%) claimed an annual household income of less than $50,000, and few (4.6%) reported incomes exceeding $100,000 annually. In addition, our sample varied in terms of Phase I trial participation: 15.3% had participated in only one study, 19.8% had participated in 2 to 4 studies, 27.5% had participated in 5 to 10 studies, and 37.4% had participated in more than 10 studies. We use pseudonyms below to protect the confidentiality of our participants.
Demographics of Study Participants (N = 131)
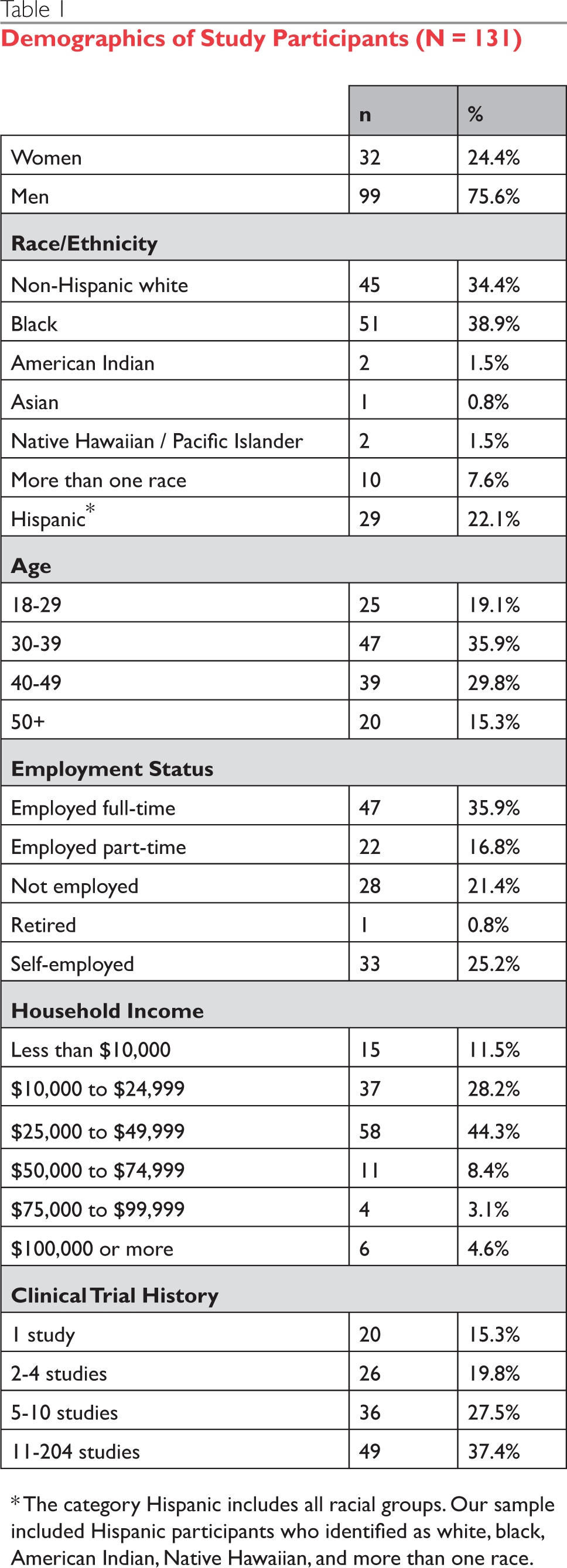
The category Hispanic includes all racial groups. Our sample included Hispanic participants who identified as white, black, American Indian, Native Hawaiian, and more than one race.
Healthy Volunteers' Interpretations of AEs
Given the high prevalence of adverse events in Phase I trials, 20 it should be no surprise that many participants in our study personally experienced or witnessed AEs over the course of enrolling in trials. In what follows, we refer to these bodily changes as AEs, even though participants themselves might use a variety of terms, such as side effects or symptoms, to describe their experience. Overall, our participants' exposure to AEs varied with their clinical trial history, including the number and type of trials in which they had enrolled. Regardless of the extent of their experiences with AEs, we found that they almost always minimized, denied, or re-attributed the cause of the AE, thereby rejecting any notion that a drug-related harm occurred. This was true both for AEs they personally experienced and those they observed in others. We demonstrate that participants' tendency to delink their experience of AEs from conceptualizations of harm results from the structure of Phase I trials and participants' economic need to enroll in clinical trials. As we will show, this narrative process can be seen in participants' portrayal of AEs (1) as insignificant discomforts, (2) as imagined or fabricated bodily changes, or (3) as distressing symptoms unconnected to the study drug. In addition, we present an example of one of the rare participants who perceived the AEs they had experienced as a form of drug-related harm. Together, these findings suggest that participants' constructions of Phase I trials as safe are critical for their ongoing involvement in the research enterprise.
AEs as Insignificant
Most participants referred to their experiences of having AEs during Phase I trials by framing them as insignificant or not concerning. Rather than perceiving any bodily changes as a sign of being harmed by the trial, they instead minimized these AEs by comparing them to other possible complications or problems that could have occurred and that they considered more harmful. While this view of AEs is experiential, we illustrate that it is also structural, particularly influenced by the informed consent process, the confinement period required for most studies, and the regular monitoring of healthy volunteers. Participants referred to each of these elements as they dismissed the possibility that their experience of an AE was evidence of being harmed in a study.
Many participants compared their AEs to more significant outcomes that could have occurred, often basing their comparison on the risk information communicated during the informed consent process. Consent forms, of course, describe “any reasonably foreseeable risks or discomforts” that may occur as a result of participation (21 CFR 50.25(a)(2)). Study risks typically vary in severity, with consent forms listing minimal to serious problems that could develop during a clinical trial. This structure of conveying the possibility of harm becomes a touchstone for participants to minimize their AEs. For example, when responding to a question about her personal experiences with AEs, Alison, a white woman who joined a clinical trial to help raise funds for her college tuition, said,
Well, I only did the one [study], and I really didn't-, I didn't have much of side effects. I ran a fever like once or twice maybe, but I didn't have any of the extreme side effects that were possible, and so that made me feel more comfortable too, because I went through it so smoothly.
Despite experiencing fevers during the trial, Alison felt reassured about her participation because she contrasted these to the side effects the consent form categorized as more harmful. In a similar vein, Justin, a white man who used clinical trials as a needed supplement to the income he got from his part-time job, reflected on the AEs he had experienced:
I've never been like, “Oh, my gosh. What's this?” … They [the AEs] would just seem like, you know, they've been explained beforehand that they could happen, and they happened. I was like, “Okay, I have one.” It was pretty well explained what to expect, so it wasn't anything alarming.
Alison's and Justin's viewpoints indicate that although reading the broad range of potential side effects could cause participants to worry more about participation risks, it may also result in them feeling safer when actually experiencing what were considered relatively minor AEs about which they have been warned.
Beyond comparing their AEs to potential side effects enumerated in the consent forms, some participants framed their own bodily changes as insignifi-cant compared to more alarming AEs experienced by fellow participants. The confinement during Phase I trials creates a structure in which healthy volunteers might witness AEs that occur to other participants in their study or different trials being conducted concurrently. Elena, an unemployed Hispanic woman, described a study in which she experienced flashes in her vision, which she referred to as “lightning.” Even so, she brushed off the AE by comparing herself to other participants: “I think I've done good, compared to-, I've seen people constantly vomiting or with diarrhea or [saying], ‘Oh my goodness, I just want to sleep.’ And yeah, you see a lot of things.” Whether Elena's symptom was truly less concerning than others' is debatable, but she positioned it as less harmful than vomiting or diarrhea on the spectrum of potential AEs. This type of comparison is possible only by having the opportunity to observe others' AEs during confinement.
Participants also downplayed the significance of harm by appealing to the attentiveness of researchers in ensuring participants' safety. Rachel, an unemployed black woman, said:
But as you get going to the studies, you see how educated everyone is about the study, as far as the staff, how professional they are, how they monitor everything, so then that makes you more comfortable knowing that they do know what they're doing. … I've only had one [AE] experience, and that was like a really bad headache … and basically they monitored me, took my blood pressure every so often, put me in a quiet, dark room … and they checked on me.
In addition to the care participants receive during a trial, the research staff evaluate participants to confirm that all AEs have resolved before they are discharged from the study. This check on healthy volunteers' return to overall good health after each trial provided many participants with assurance that AEs were neither significant nor harmful. Paolo, an unemployed Hispanic serial participant, held this view even though a recent trial in which he had to take naltrexone, an opiate antagonist, made his “mind split in two,” a feeling he described as “very, very, very, very uncomfortable.” Dismissing the possibility of being harmed, Paolo asserted,
Like, nothing happens to us, and we're still healthy [after doing studies]. These [participants] are guys that still go running; they look healthy… I mean, we wouldn't be getting inside [the studies] if our cholesterol wasn't in good level, if our blood cells-. Our white blood cells, red blood cells, everything has to be within a certain shape because we're not doing a sick volunteer [study], we're doing a healthy volunteer [study], so obviously if we're in there, our bodies are still good.
This minimization of harm is strongly tied to serial clinical trial participation. Paolo relied fully on compensation from trials to earn his income, so he was likely to screen for a new clinical trial in fairly short order after finishing one. The fact that he had been participating in studies for over a decade and completed an estimated 26 trials was due to the financial compensation, but it also became the basis for his belief that he had not been harmed. Thus, his definition of harm rested on his own continued ability to qualify as a healthy volunteer, which he could do despite the AEs he had during his trial history.
Other times participant viewed AEs as insignifi-cant because their bodily changes were not altogether unpleasant. This was the case in one clinical trial for AJ, a black man who participated in studies full-time. Brushing off his experiences when asked about AEs, AJ instead described them in a positive light when narrating the vivid dreams he had experienced:
It was crazy because … the dreams felt like, as if you're awake right now and walking around and stuff like that. It felt like that, like I was awake and then I couldn't decipher what was, if I was up [and awake], and I'm like, “Whoa, this is kind of weird.” It was, it was crazy … I was like, “Wow.” I couldn't wait to go to sleep. [laughs]
By viewing these dreams as an enjoyable experience, AJ not only discounted the potential harm associated with that symptom, but he also recast it as a benefit of participating in that particular trial. Other participants might not have gone quite as far as AJ, but they too saw particular AEs as anything but harmful. For instance, Oscar, a Hispanic participant, laughed about how a clinical trial gave him a “subtle sense of euphoria” that transformed him for several hours from his usual grouchy, “goblin” disposition to feeling happy. A friend even commented to Oscar that he had not “said anything remotely sarcastic with a cynical undertone” during their entire conversation following the dose of the study drug. With these AEs in particular, it is understandable why AJ and Oscar might not perceive any harm having occurred to them from the trials.
AEs as Imagined or Fabricated
In participants' discussions of having evaded harm in Phase I trials is evidence that some AEs were experienced but not acknowledged as real. In these instances, participants doubted the authenticity of the bodily change, believing instead that the symptoms might be imagined, psychosomatic, or even complete fabrications invented by other participants. Supporting participants' skepticism of any bodily changes is the lack of feedback about AEs from research staff, who neither confirm nor deny the legitimacy of participants' reports of symptoms. As this section reveals, participants' interpretation of AEs as specious illustrates the degree of ambiguity surrounding the possibility that harm might have occurred during a clinical trial.
When participants were uncertain about the credibility of their own assessments of bodily changes, some believed that an AE was simply imagined. For example, Lindsay, a white woman struggling to make ends meet despite her full-time job in a fast-food restaurant, disputed her own experience of AEs when asked how common it was for her to have side effects during studies:
Common. Mostly just nausea or being light-headed or, yeah. And I think it's because I over-think it and just like waiting for the effects to happen, and then I'm just like, “Oh, I think this is an effect. Something is happening to me.”
Rather than assuming her symptoms were real, Lindsay instead questioned them, framing them as figments of her imagination that resulted from her expectation that she would experience them. The confinement structure of the trial seemed to add to Lindsay's impression. Because she had to stay in the clinic, she was much more conscious of the fact that she had taken an investigational drug — and thus entered a state of waiting for effects — than if she were outside of the clinic going about her more typical routine.
Bruce, a white self-employed man who had a long history of participating in biomedical and other research studies, took a step further the view that AEs are spurious. His theory imputed that AEs are largely psychosomatic, which means that they are real experiences generated not by the study but the participant's mind. Harnessing this conceptualization of AEs to his advantage, Bruce declared,
I always envision myself as getting the placebo; therefore, I never suffer the side effects that other people have, all of these tragic things. And usually they're the ones that are on the placebo, so I don't get it, but whatever. [chuckles] I mean, it's all psychosomatic.
The notion that feelings of discomfort are imagined or self-induced often cannot be confirmed or contradicted by objective measures. Many AEs do not have physiological markers, so there is no test that can determine if they are imagined or real. Moreover, if AEs are truly psychosomatic, then medical instruments or procedures can register the AE, such as a thermometer confirming a fever, but the cause of the sign or symptom remains ambiguous.
Researchers explicitly recognize that AEs can be psychosomatic. As a result, most clinics prohibit healthy volunteers from sharing information about AEs with each other. The reason for this is that the knowledge that one participant has an AE can “infect” the others, creating a contagion of psychosomatic headaches, fevers, and so on. In spite of this, the confinement structure of Phase I trials encourages participants to disregard this rule because of the social interactions that naturally occur when individuals share a relatively small space for days or weeks on end.
However, what researchers do not account for is that healthy volunteers might be skeptical about other participants' accounts of AEs. This is part of a broader narrative of participants doubting the validity of others' experiences even when stories of AEs are shared directly with them. They might discredit the teller or assume the AE is fabricated. Discrediting often involves participants perceiving the person with the AE as ignoble, often coming from a different race and/or class background and an untrustworthy reporter as a result. For example, Harry, a college-educated multiracial man with full-time employment, recalled how after an outpatient study visit, he had shared the elevator with another participant. The man, whom Harry described as old and disheveled, told Harry that he felt sick and had been in pain throughout the trial. Reflecting on this interaction, Harry dismissed the man's story:
I don't know if I believe if he really was [sick] ‘cause no one else seemed like that guy. I didn't see anybody else like that, and he just seemed kinda like a hobo off the street, didn't know what was going on. I don't even know why he was talking to me.
Harry discounted the man's experiences of a potential AE by contrasting him with the other participants in the study who did not exhibit the same symptoms and by challenging the man's right even to interact with him. In the process, Harry did not have to acknowledge that the study in which they were both enrolled could be harmful.
Discrediting the narratives of other participants might also be tied to the public perception of healthy volunteers as financially desperate people willing to tell outright lies to participate in clinical trials. Rather than considering their own motives for enrolling in trials to refute this view, many participants continued to believe that others are fundamentally dishonest. When it comes to AEs specifically, many participants claimed that others' purported symptoms were mere fabrications intended to deceive the research staff. This speculation stemmed from some clinics' policies to compensate healthy volunteers for the entire clinical trial when they are withdrawn or the entire study is halted due to safety concerns. 21 In this context, our participants suggested that others might exaggerate symptoms as a strategy to the leave the study early with their full payment. Travis, a black man with more than two decades of trial participation, explained,
Some people, they're like, “Oh my god! I have these headaches!” And the first thing I think of is, you know, in those cases, like, “Are these people just trying to kind of weasel out [of the study]?” Because they know that there's a policy in place where, you know, if you can't participate or they drop you for any reason, then you get full compensation if it's, you know, an AE from the drug. I think sometimes people just play that out, see how that goes just to kind of, you know, say, “Hey, listen, I don't want to be here for a whole month if I don't have to or whatever.”
Discrediting the narratives of other participants might also be tied to the public perception of healthy volunteers as financially desperate people willing to tell outright lies to participate in clinical trials. Rather than considering their own motives for enrolling in trials to refute this view, many participants continued to believe that others are fundamentally dishonest.
Travis' view of others' AEs is particularly striking because any bodily changes that would result in a participant's removal from a study could generally be considered serious harms. Yet, because of the prohibition on sharing information about AEs, researchers rarely communicate any information about other participants, which creates fertile ground for participants to deny that any harm has occurred. By instead positioning others' AEs as fabrications, participants maintained their own sense of the overall safety of Phase I trials, justifying their decision to continue to enroll, perhaps as in Travis' case for decades.
AEs as Distressing but Not Caused by the Study Drug
While AEs were routinely dismissed as insignificant or imaginary, there were times in which participants did acknowledge that their or others' bodily changes were real and painful. Yet, they often chose to explain these AEs as caused by some factor other than the study drug. They instead attributed AEs to the clinic environment, the restrictions associated with the clinical trial, or other participants' deceptive practices — such as lying about their medical histories or past trial participation — that made them more vulnerable to AEs. As this section illustrates, these interpretations of distressing AEs similarly function as a mechanism for participants to avoid altering their perceptions of the safety of Phase I trials.
Because of the required study confinement period, participants often perceived AEs as caused by the artificial environment to which they were subjected. For example, rather than experiencing a side effect of the study drug, they might argue that fatigue or somnolence was due to their inactivity, boredom, or change in sleeping arrangements. Similarly, the study diet provided an alternative explanation for gastrointestinal changes, even when those symptoms were common among participants. Reflecting on the only clinical trial she had done, Jennifer, an unemployed white woman, expressed ambivalence about the cause of a distressing AE she had experienced: “I don't know if that [back pain] was because of the [study] medication or if it was because the hospital beds were terrible.” Because only one other person in her study had a similar AE, Jennifer added, “It's kind of debatable as to whether or not it had anything to do with the medication itself.”
In some instances, there is indeed a lot of ambiguity surrounding the cause of AEs. The nearly universal prohibition on caffeine during Phase I trials is an example of a study restriction that certainly can cause participants to experience withdrawal headaches when they are used to regular caffeine consumption. At the same time, however, headaches are regularly listed as a potential risk of the study drug. Recognizing this ambiguity becomes a way for participants to explain away drug-related harm. When asked about AEs, Steve, a white full-time study participant, responded:
It's pretty rare [for me to experience AEs], really. I get headaches in almost every study, but that tends to be more from caffeine withdrawal. And so I can't know for certain that it's from the drug, even though almost every informed consent [form] will list headaches as a potential side effect. I doubt that's why I'm getting the headaches. It's most likely the caffeine withdrawal.
Most notable about Steve's dismissal of the study drug causing his headaches is his explicit acknowledgment of the consent form detailing headaches as a potential risk of participation. As someone who relied on clinical trials for his entire income, it perhaps behooved Steve to blame the study restrictions instead of the investigational drugs for these painful AEs.
In addition to attributing their own AEs to non-drug-related factors, participants interpreted AEs experienced by other participants this way. In these cases, they were able to invent possibilities for why one participant might have experienced a more severe outcome than others. However, when they did so, they often assumed these other participants had lied in order to qualify for the trial, broke the clinic rules, or failed to observe restrictions during the study itself. As with the discounting of other participants' AEs we described above, this perspective casts other participants as dishonest and deceptive. Plus, it engages in a blame-the-victim narrative that dismisses the possibility that the participant her- or himself might also be at risk when witnessing or hearing secondhand about serious AEs. The following excerpt from Everett, an unemployed black man who had participated in trials regularly for the past 6 years, demonstrates that this narrative can be maintained even in cases of witnessing frightening AEs:
This one guy, he stopped breathing. I remember it was down in [clinic] last year. They did a code blue on this guy. He stopped breathing, and [they] took him downstairs to the emergency room … Maybe he took some [illicit] drugs, or maybe he lied when he came in, and he was taking other things and wasn't supposed to. There's a lot of people [who] do that when they doing studies. They go take supplemental things, you know, as a upper to get ‘em ready for the next study. Some people go study hopping, and they do too many at one time. You know what I mean? So, if you do that, do too many at one time, you don't know what's gonna happen. Your body's not gonna be ready for it.
In this example, it is notable that Everett tried to explain the distressing AE he witnessed by offering multiple explanations for the event without ever speculating that it could be a direct result of the study drug itself. Implicit in Everett's account is his knowledge that trials have measures in place to maintain a controlled environment, permitting conjecture that breaches in these standards are responsible for AEs. This type of speculation can prevent participants from fearing the study drugs themselves, believing that following the rules alleviates the risk of harm. This perception can also attenuate feelings of concern for other participants, viewing them as responsible for, and possibly deserving of, any harm that occurs due to their deceptive practices.
Secondhand stories about harmful AEs were all the more likely to contain narratives of blameworthy individuals who lied to get into studies or who cheated thereafter. These stories could then also serve as cautionary tales to remind participants to follow trial protocols, especially when the financial compensation could prompt healthy volunteers to bend the rules as a means to maximize their earnings. 22 Perhaps most indicative of participants' desire to maintain the reality that AEs can be explained by participant wrongdoings, rather than unfortunate drug reactions, was their retelling of Phase I tragedies about which they had heard from news sources. We have already noted that participants do not receive much information about AEs during trials from the research staff, but news reports, in contrast, often contain details about what might have caused AEs when participants are injured or have died. Referencing the infamous immunotherapy study that took place on healthy volunteers in London in 2006, Tammy, a self-employed white woman who used studies to help cover her bills, reported,
You know, the one [study] that really sticks in my mind was hearing about these people in England that had done a study and they all swole up and died, and the reason—they, they figured out—was because they'd gone straight from one study to another and they had drugs in their system [from the prior study] that interacted badly with the new drug they were given. And I think actually in Europe they [now] make you wait two months between studies because of that horrible thing that happened.
Tammy's retelling of the first-in-human trial for theralizumab contains several factual errors. Specifically, none of the healthy volunteers died, but they did experience life-threatening cytokine storm reactions that resulted in multiple organ failure and some were left with permanent body disfigurements. 23 Additionally, post-trial investigations of the tragedy confirmed that the AEs were an unforeseen drug reaction that had not been predicted in prior nonhuman animal testing, 24 not that the participants had done anything themselves to provoke the AEs. Despite the news reports, Tammy distorted the case by linking the AEs to participant misconduct. This misrepresentation of the trial, as with all instances of participants blaming other healthy volunteers who experienced AEs, dismisses the risks of Phase I trials and helps participants to avoid questioning the safety of testing investigational drugs.
The Exception to the Rule: An AE Viewed as a Study-Related Harm
As we have now illustrated, many of our participants experienced or witnessed symptoms that involved some level of discomfort during their Phase I trial participation. Yet, it was very uncommon for them to identify these AEs as significant and caused by the study drug itself. When participants did describe their AEs in terms that conveyed that the bodily changes were actually drug-related harms, the following exception to the rule brings into focus why the majority of participants might prefer their different interpretations.
Because study enrollment is voluntary, understanding an AE as related to the trial requires participants to acknowledge that they knowingly exposed themselves to harm. This comes across in the case of Timothy, a white participant who described himself as financially stable and reported a yearly household income over $100,000. Timothy suffered an alarming AE in his first and only Phase I trial. Enrolled as a healthy volunteer in an outpatient study of an investigational drug for diabetes, he lost a significant amount of weight and was ultimately taken to a hospital's emergency department after passing out at work. In spite of the fact that he was informed about the risks prior to enrolling, he decided to participate in the study because he did not expect to be harmed, recalling, “[I] figured my body would handle whatever was put in me.” Timothy had no doubts that his AE was caused by the study drug, and even a year following the incident and his return to full health, he continued to regret his decision to enroll: “Yeah, it really made me sick, and… had I known those side effects would have happened [to me], I would not have done the study.” Without hesitation, he added, “I'm really not inclined to do any more.” Timothy was explicit in linking his decision not to enroll in future studies to the harm he experienced, but he further justified his position by rejecting the importance of the economic benefit he could receive from trial participation: “The other thing was it was kind of some supplemental income, and that's not necessary at this point.”
In rationalizing why he had put himself in harm's way through study participation, Timothy excused his initial decision to enroll in a clinical trial by claiming ignorance about the potential to personally suffer any negative consequences. 25 After his experience of a frightening AE, this excuse could only remain plausible as long as he did not participate in additional studies. Fortunately for Timothy, his financial stability further enabled him to stop participating in studies and might help to explain why he, unlike so many other participants, acknowledged his AE as harmful and believed it was caused by the trial. This point of view departs radically from that of many of the participants who denied that AEs were forms of harms. The difference between these two perspectives illustrates how harm is ultimately a fuzzy construction that relies heavily on individuals' interpretations, which in turn may be shaped by their trial experience and reliance on trial income.
Conclusion
By exploring participants' narratives of their AE experiences in Phase I trials, we demonstrate the ambiguity that surrounds research harms in this context. There are no clear-cut definitions that map harm onto objective bodily changes or experiences healthy volunteers might have over the course of their participation. Instead, the structure of these clinical trials provides participants with the opportunity to interpret their own and others' AEs as related to the study drug or, instead, to other factors. As we have illustrated, participants' discussions of AEs downplay the possibility and magnitude of experienced harm by portraying bodily changes as insignificant, imagined, fabricated, or unrelated to the study drug. They do this by comparing relatively minor AEs to the greater risks outlined in informed consent forms, by blaming the confinement period for their discomfort, and by assuming that other participants are dishonest. These interpretations function to minimize, deny, or re-attribute the cause of AEs in order to avoid perceiving them as instances of harm. Our findings underscore the importance of acknowledging how the research environment assists in shaping and maintaining ambiguity about the potential risks of harm in clinical trial participation.
By dissociating the experience of AEs from harm, healthy volunteers avoid needing to reevaluate the possible risks of trial participation. This might be in their financial interest if they wish to continue enrolling in trials, but it poses ethical dilemmas for researchers and for research oversight bodies charged with risk mitigation and management of research-related harms. First, it raises questions about the ability of the informed consent process to communicate effectively about risk when actual participants engage in a process of denying how those risks translate into bodily harms. Second, by perceiving AEs as insignificant or imagined, participants might be disinclined to report bodily changes to research staff, which would undermine a critical function of Phase I trials. 26 Put another way, flawed accountings of harm potentially jeopardize both the protection of research participants and the trustworthiness of trial results.
Additionally, in demonstrating that participants typically do not recognize AEs as indicative of safety concerns, it casts in a new light the lack of information provided to healthy volunteers about trial results. While there might be clear scientific value in collecting data on all AEs without attributing causation during the clinical trial itself, it is more difficult to justify why participants remain ignorant about which AEs are later identified as drug side effects. Return of results has become a larger ethical conundrum in research, 27 but this information could be especially meaningful in Phase I trials. Because healthy volunteers often enroll serially in these trials, learning how their AEs were later classified could benefit the informed consent process for their future trial participation. Although AEs in one trial should not be extrapolated to the next, participants might be more sensitized to study risks by ascertaining that previous bodily changes they or others experienced were indeed drug effects. If results were shared in this way, participants might also be more apt to interpret future AEs as potential harms and in turn reevaluate the safety of participation in general. While this might make it more difficult for researchers to enroll healthy volunteers in Phase I trials, it would provide more meaningful informed consent in the context of serial participation.
Without such a change to more rigorously inform healthy volunteers about the likelihood of suffering drug-related harm, participants' interpretations of their AEs problematically contribute to a wider narrative downplaying Phase I trial risks. Evinced in recent commentaries that laud the safety of healthy volunteer trials, 28 the bodily changes that participants routinely experience are rarely reflected upon as harms. Without such a framing, the appropriateness of using healthy volunteers as opposed to affected patients in Phase I trials is rarely challenged. 29 Subsequently, the pharmaceutical industry is advantaged by the broad support of these trials by regulatory bodies and many bioethicists as well as the pool of serial participants eager to enroll in their next study. Although not all harms are equally concerning, critical assessments of Phase I trials must not fall into the trap of minimizing, denying, or re-attributing the harms that routinely occur.
Footnotes
Dr. Fisher reports grants from National Institutes of Health during the conduct of the study.