
Abstract
The authors explored differences in posttraumatic stress disorder (PTSD) symptoms as a result of rating symptoms from two separate, differentially distressing traumatic events. In an initial sample of 400 nonclinical participants, the authors inquired through a web survey about previous psychological trauma, instructing participants to nominate their most distressing and second most distressing traumatic events experienced. Using the PTSD Checklist, participants rated their PTSD symptoms separately from these worst and second worst events. Using the four-factor emotional numbing PTSD model in confirmatory factor analysis, results demonstrated evidence supporting separation of PTSD symptom rating sets from two differentially distressing traumas—specifically, the worst and second worst events. Measurement invariance tests revealed that factor loadings did not vary between the worst and second worst event PTSD ratings; item thresholds (indexing symptom severity) differed. Results generally support the recommended PTSD assessment protocol instructing participants to rate PTSD symptoms from a single, worst index event.
Keywords
For victims of multiple traumatic events, it is typically recommended that posttraumatic stress disorder (PTSD) should be assessed in relation to one’s most distressing trauma. Few studies have empirically tested the validity of this approach to assessing PTSD. Furthermore, it is unknown whether PTSD symptom ratings from one’s most distressing traumatic event would be different from ratings from another distressing trauma.
For individuals who have experienced a single traumatic event (or traumatic event type), experts typically recommend that PTSD should be assessed specifically in relation to that trauma, using a psychometrically sound PTSD assessment instrument (reviewed in Elhai, Ford, & Naifeh, 2010; Wilson & Keane, 2004). Yet most victims of psychological trauma report having experienced more than one type of traumatic event (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995). The American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) requires that for a PTSD diagnosis, PTSD symptom criteria must be fully satisfied in response to a single, particular traumatic event; it is not permissible to assign a PTSD diagnosis based on only some symptoms met from one trauma, and other symptoms met from another trauma(s). Yet it is often not feasible to assess PTSD separately from each different traumatic event among individuals reporting multiple traumas.
Experts typically recommend that for victims of multiple traumatic events, a single, index traumatic event should be used from which to rate PTSD symptoms—specifically, one’s worst or most distressing traumatic event (e.g., Elhai, Ford, et al., 2010; Wilson & Keane, 2004). This so-called worst event method of assessing PTSD should ensure the greatest likelihood of endorsing relevant PTSD symptoms and fulfilling diagnostic criteria among those who truly qualify for the diagnosis. The utility of this method rarely has been empirically tested, and some investigators have questioned whether respondents can reliably distinguish PTSD symptom ratings from one trauma versus another trauma (e.g., Elhai, Ford, et al., 2010). Furthermore, despite expert recommendations, many researchers and clinicians do not use the worst event method in assessing PTSD. Rather, many professionals instead query PTSD symptoms without reference to any index trauma (Elhai, Ford, et al., 2010).
Recently, Naifeh and Elhai (2010) tested whether variations of specifying one’s worst traumatic event would result in differences in PTSD symptom severity from that event. Among traumatic events endorsed by subjects (meeting PTSD’s traumatic stressor criterion, A1), they altered whether subjects were instructed to nominate their (a) “most upsetting event”; (b) “currently most upsetting” event; or after providing a list of PTSD symptoms as a reference, (c) event that “currently causes you the most of these problems.” No significant differences in PTSD severity were evident across conditions, suggesting that each of these methods resulted in comparable PTSD estimates. Furthermore, Elhai et al. (2009) tested differences in PTSD’s factor structure based on whether trauma victims were instructed to rate PTSD symptoms from their worst trauma versus overall trauma history. The authors found little evidence for differences between groups across several factor structure parameters (including intercepts, indicative of item severity), suggesting that perhaps trauma victims have difficulty in separating PTSD symptom ratings from one trauma over others. On the other hand, more recently, Simpson, Comtois, Moore, and Kaysen (2011) found that the prevalence of PTSD increased substantially when patients were instructed to rate their PTSD symptoms from their overall trauma history instead of indexing a single traumatic incident.
These recent studies exploring the worst event method of PTSD assessment do not provide direct evidence of whether individuals’ PTSD symptom ratings from a worst trauma are different from their ratings of a different trauma that is distressing. This research question is important in understanding the extent to which individuals exposed to more than one traumatic event can reliably differentiate their ratings of PTSD symptoms from one trauma over another trauma.
In the present exploratory study, we tested this research question among a nonclinical sample of individuals reporting a trauma history. We investigated potential differences in PTSD symptom rating patterns from differentially distressing traumatic events using confirmatory factor analysis (CFA) in a within-subjects design. For instructive purposes, we next discuss the literature on the factor structure of PTSD.
DSM-IV PTSD criteria are organized around three symptom clusters: reexperiencing (PTSD Items B1-B5), effortful avoidance and emotional numbing (Items C1-C7), and hyperarousal (Items D1-D5). Yet little empirical support has been found for this PTSD model based on CFA studies (reviewed in Elhai & Palmieri, 2011; Yufik & Simms, 2010). Instead, two four-factor models have demonstrated the most empirical support in accounting for PTSD’s underlying structure, with little evidence supporting one-, two-, or three-factor models (reviewed in Elhai & Palmieri, 2011; see meta-analysis by Yufik & Simms, 2010).
First, the emotional numbing model (King, Leskin, King, & Weathers, 1998) represents a revision of the DSM-IV PTSD model by splitting avoidance (PTSD Items C1-C2) and numbing (Items C3-C7) into separate factors (item mappings are displayed in Table 1). The numbing model is based on theory and empirical evidence supporting avoidance and numbing as two statistically separate constructs, differentially related to psychopathology and treatment outcome (reviewed in Asmundson, Stapleton, & Taylor, 2004). In addition, the dysphoria model (Simms, Watson, & Doebbeling, 2002) removes Items D1 to D3 and combines them with the numbing items to form a dysphoria factor, reflecting the notion that these items are less unique to PTSD but are common features of dysphoria and distress found in other anxiety and mood disorders (Watson, 2009). Both the numbing and dysphoria models are empirically supported in characterizing PTSD’s latent structure (reviewed in Elhai & Palmieri, 2011; Yufik & Simms, 2010). Several studies have found that the choice of PTSD assessment instrument (Elhai, Biehn, Naifeh, & Frueh, 2011; Palmieri, Weathers, Difede, & King, 2007) or specific PTSD assessment instructions (Elhai et al., 2009) affect which of these models fits best.
Item Mappings for the Three-Factor DSM-IV and Four-Factor Emotional Numbing PTSD Models
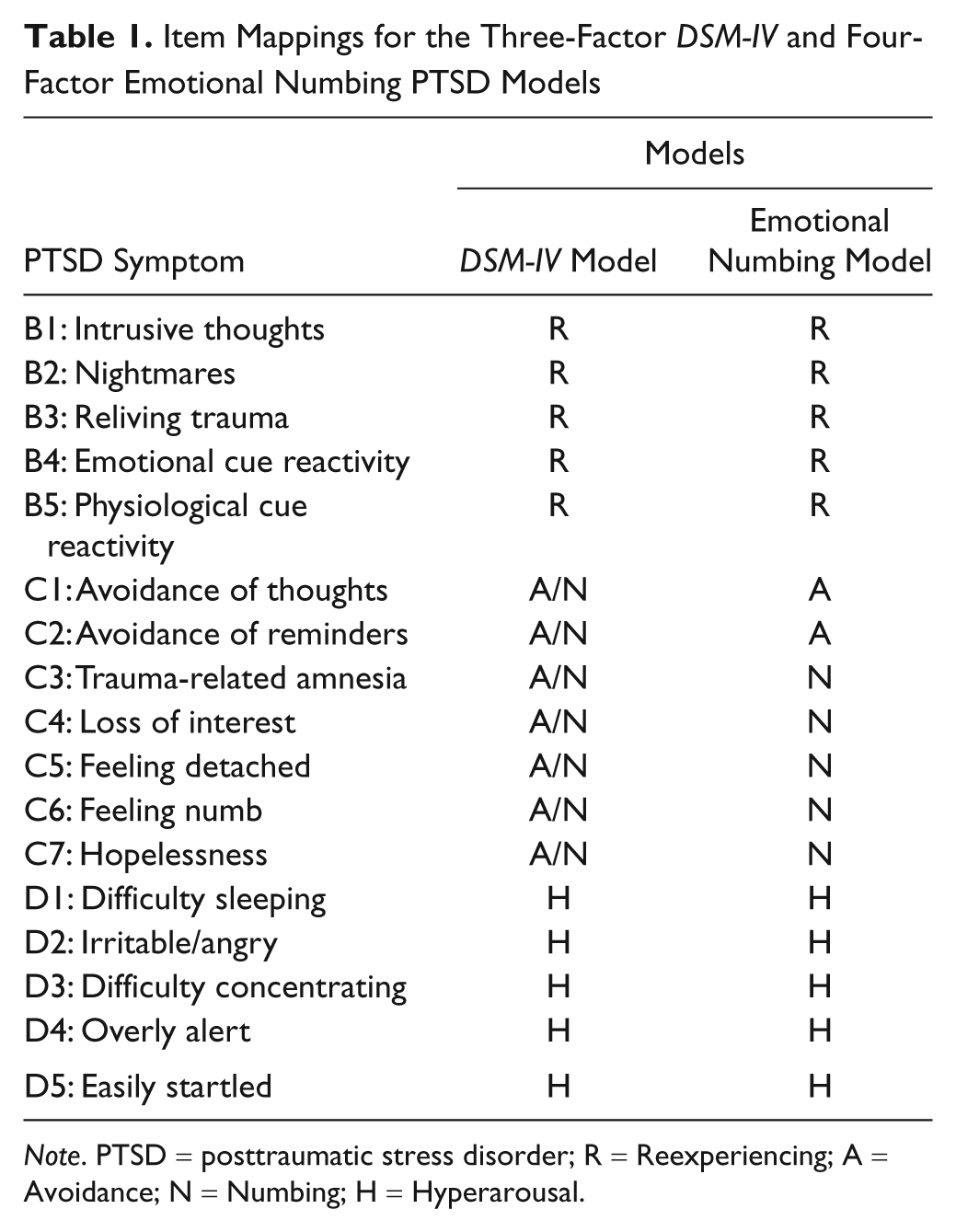
Note. PTSD = posttraumatic stress disorder; R = Reexperiencing; A = Avoidance; N = Numbing; H = Hyperarousal.
The meta-analysis by Yufik and Simms (2010) demonstrated a slight advantage for the dysphoria model in the PTSD CFA literature, albeit based on the small proportion of PTSD CFA studies included in the meta-analysis (N = 40), because only 10% of covariance matrices requested from the authors were obtained and used in the meta-analysis. In the present article, we focus on the emotional numbing model because of its longevity since, unlike the dysphoria model, the numbing model aligns closely with the proposed DSM-5 PTSD symptom model conceptualization (American Psychiatric Association. DSM-5 Development, 2010).
We tested whether PTSD’s factor structure parameters differed based on rating PTSD symptoms from one’s worst traumatic event type in comparison to their second worst traumatic event type (a traumatic event that is presumably nearly as distressing). For example, we wanted to learn whether factor loadings from one’s worst trauma would be equivalent or different than those from one’s second worst trauma; equivalency would indicate that the items hang together within factors in similar and stable ways across traumas, whereas differences would not indicate this. We hypothesized based on preliminary evidence from Elhai et al. (2009) that PTSD factor structure parameters overall would not differ significantly between ratings from one’s worst versus second worst traumatic event. That is, we surmised that the factor structure of PTSD would be fairly stable across symptom ratings from two different traumatic events. This research has implications in understanding the stability of the PTSD construct by examining differences in how PTSD is rated from different traumatic events.
Method
Participants
A nonclinical sample of undergraduates from a medium-sized Ohio public university’s psychology research pool volunteered between spring 2010 and spring 2011 using internal, university web-based recruitment. Potential participants were presented a web-based consent statement describing the study as involving “stressful events and emotional functioning,” with class research/extra credit offered, but no monetary compensation. Initially, 1,709 individuals signed up for the study, but only 1,645 provided any responses to the traumatic event queries. Among the 1,645 subjects, 928 (56%) endorsed at least one traumatic event, of which 863 nominated a worst (or only) traumatic event. Among participants nominating a worst/only trauma, only 407 both endorsed multiple traumas and also nominated a second worst trauma (required for our within-subject analyses).
We compared subjects with multiple prior traumas (n = 407) with subjects reporting only one trauma (n = 456) on demographic characteristics. Compared with participants with one trauma, those with multiple traumas were older, F(1, 859) = 5.55, p = .02, partial η2 = .01, and more represented by women, χ2(1, n = 862) = 7.47, p = .01, phi = .09 (albeit with small effect sizes).
Among those subjects nominating a second worst trauma, one subject did not continue the survey after nomination of this trauma (leaving 406 subjects). We excluded six subjects from the subsample of 406 because they missed more than 11 (35% of) PTSD items in total from the two sets of 17 items; thus, the final effective sample size was 400.
Among the effective sample of 400 subjects, 26% (n = 105) were men and 74% (n = 295) were women. The average age was 20.27 years (SD = 5.05), and average years of schooling was 12.94 (SD = 2.37). Racial background (not mutually exclusive) was predominantly Caucasian (74%, n = 294) and African American (25%, n = 99), with some Asian (4%, n = 15) and Native American (4%, n = 15) representation; Hispanic ethnicity was identified by 7% of subjects (n = 26).
Procedure and Instruments
We inquired about demographics such as gender and age. Subsequently, we used the Stressful Life Events Screening Questionnaire (Goodman, Corcoran, Turner, Yuan, & Green, 1998) to measure self-reported lifetime psychological trauma exposure using 11 PTSD criterion A1 traumatic stressors and a 12th A1 item assessing “other” serious injury/life danger. Adequate validity and reliability have been found for this instrument (Goodman et al., 1998). We inquired about participants’ most distressing and second most distressing traumatic event types, with follow-up questions regarding characteristics of those events, including perceived distress currently caused by the particular trauma (1 = “no distress” to 10 = “extreme distress”).
We used the PTSD Checklist-Specific Stressor Version (PCL; Weathers, Litz, Herman, Huska, & Keane, 1993), assessing DSM-IV PTSD symptoms over the past month using a Likert-type scale (1 = not at all to 5 = extremely). It has adequate reliability (coefficient α = .95 in ratings from both the worst and second worst event in this study, separately) and validity across samples (reviewed in McDonald & Calhoun, 2010; Wilkins, Lang, & Norman, 2011), including with samples of college students (Ruggiero, Del Ben, Scotti, & Rabalais, 2003).
We used conditional branch/skip logic that automatically routed subjects through the survey based on their particular responses. Specifically, participants endorsing only one criterion A1 trauma were routed to rate PTSD symptoms from that trauma. Participants endorsing more than one criterion A1 traumatic event type were instructed to nominate their most distressing and second most distressing traumas, subsequently routed to rate PTSD symptoms specifically in relation to those two traumas separately (randomized in a counterbalanced order, to account for order effects). Participants who did not endorse any traumatic events were administered a separate protocol unrelated to this study. After survey completion, participants were presented with contact information for the principal investigator and treatment resources.
Analysis
The effective sample had a subset of respondents missing fewer than four PCL items each (mostly one to two items each). Missing data were missing completely at random (MCAR), Little’s MCAR test, χ2(1,109, N = 400) = 1179.14, p = .07; thus, patterns of PTSD ratings were not associated with missingness. CFA analyses were conducted using Mplus 6.1 software (Muthén & Muthén, 2010a). We used a pairwise present approach to use all available data by estimating missing parameters based on available values within pairs of responses. CFA analyses were specified based on King et al.’s (1998) four-factor emotional numbing model.
Responses to PTSD items that queried the worst and second worst traumas, separately, did not evidence significant nonnormality; no univariate skewness values were greater than 2.0, and the largest kurtosis value was 2.33. Initially, CFA using maximum likelihood estimation resulted in a very poor fit when modeling the worst and second worst PTSD ratings sets using the four-factor emotional numbing model: comparative fit index (CFI) = .77, Tucker–Lewis index (TLI) = .75, root mean square error of approximation (RMSEA) = .11. Elhai and Palmieri (2011), in their review of the PTSD factor structure literature, discussed that poor fit for otherwise robust PTSD factor models tends to occur when treating items that have five or fewer response options as continuously scaled items. In fact, methodological research demonstrates that instruments with five or fewer response options are better conceptualized as ordinal variables and should be treated as such (Flora & Curran, 2004; Wirth & Edwards, 2007), especially with a nonclinical sample evidencing floor effects. Therefore, in CFA, we treated PCL items as ordinal rather than continuous variables; as a result, we used polychoric (rather than Pearson) covariances, probit (rather than linear) regression coefficients, and robust weighted least squares estimation with a mean- and variance-adjusted chi-square (WLSMV). As discussed below, treating PCL items as ordinal data substantially improved fit, as expected. Goodness-of-fit indices are reported, including CFI, TLI, and RMSEA. Models that fit very well (or adequately) are indicated by CFI and TLI ≥.95 (.90-.94) and RMSEA < .06 (to .08; Hu & Bentler, 1999).
We conducted a chi-square difference test assessing invariance between two models: (a) the four-factor emotional numbing model, with the 17 worst event PTSD and 17 second worst event PTSD items specified to load on their four respective intercorrelated PTSD factors and (b) a similar model but with eight intercorrelated factors, separating the PTSD factors into four worst event and four second worst event factors based on the emotional numbing model. This difference test essentially evaluated whether the PTSD ratings from the worst versus second worst event were represented by distinct constructs (i.e., measured by different factors); a correction factor was used by implementing the Mplus DIFFTEST function, given that the WLSMV-generated chi square is not normally distributed on a chi-square distribution (Muthén & Muthén, 2010b). We next conducted measurement invariance testing using parameter equality constraints with the emotional numbing model (implementing four factors), testing invariance/noninvariance across the worst event and second worst event PTSD ratings on factor loadings and observed variable thresholds, following established procedures (e.g., Meredith & Teresi, 2006). Invariance testing was conducted to test which parameter estimates (if any) may differ between the two sets of PTSD ratings: factor loadings, representing the importance of specific PTSD items within a factor; and thresholds, representing the likelihood of endorsing more severe item response options.
Normally in CFA, residual error covariances are fixed to zero. Conversely, there are design-driven situations in which it is reasonable, and even preferred, to estimate residual error covariances. Cole, Ciesla, and Steiger (2007) argued for estimating error covariances among subsets of items sharing the same methodology where other item subsets have different methodologies. In the present study, all residual covariances between symptom items (e.g., between DSM-IV PTSD’s B1 and B2) were fixed to zero. However, the worst event and second worst event PTSD responses within a symptom (e.g., B1 from the worst event and B1 from the second worst event) share substantial residual variance, since an item’s worst and second worst event PTSD responses are based on the same PTSD symptom. Therefore, all analyses estimated residual covariances for the worst and second worst event PTSD rating pairs, for a total of 17 estimated residual error covariances.
In the invariance testing, Model A included all 34 items (17 worst event PTSD ratings and 17 second worst event PTSD ratings), specified to load on their respective four PTSD factors from the emotional numbing model. Thus, a given PTSD symptom’s worst and second worst event ratings were allowed to freely vary from each other. Subsequent models tested progressively more conservative restrictions, constraining particular parameter estimates to be equal across the rating sets within a worst event/second worst event PTSD item pair and tested against the prior step’s model. Model B constrained factor loadings as equal across the symptom sets within a pair (testing metric or pattern invariance); this step assisted in evaluating whether the meaning of the PTSD factor constructs were consistent across the worst event/second worst event ratings. Model C additionally constrained observed variable thresholds to be equal (testing strong or scalar factorial invariance); this step was meant to inform whether the worst event and second worst event PTSD ratings were of comparable severity.
Tests of statistical significance between models were assessed with chi-square difference tests, comparing a given CFA model assuming equal parameter estimates (e.g., factor loadings) against a model allowing those estimates to vary across a given symptom’s worst versus second worst event PTSD ratings; a correction factor was used for the nonnormally distributed WLSMV-generated chi-square value. A significant difference between a model with a parameter constrained (e.g., factor loadings) and a model without the parameter constrained would indicate that the two sets of PTSD ratings are not invariant on that parameter (and thus are different). Because the invariance testing involved factor loadings, we estimated all loadings in our models (rather than the traditional fixing of a factor’s unstandardized loading to 1), assigning factor metrics by fixing their variances to 1; factor means were fixed to zero.
Results
The most prevalent traumatic events endorsed were losing a close associate to an accident, homicide or suicide (56%, n = 223), physical abuse by a non-caregiver (46%, n = 181), being in a life-threatening accident (38%, n = 149), and witnessing a trauma involving death or serious injury (33%, n = 132). The most prevalent events nominated as the worst trauma included the unexpected death of a close associate (31%, n = 124), being in a life-threatening accident (10%, n = 38), forcible rape (8%, n = 33), and physical abuse by a caregiver (8%, n = 32). The most prevalent events nominated as the second to worst trauma were the unexpected death of a close associate (20%, n = 80), being in a life-threatening accident (17%, n = 66), and physical abuse by a non-caregiver (10%, n = 39).
Perceived amount of distress currently caused by the worst event averaged 6.28 (SD = 2.89), compared with that of the second worst event, which averaged 5.19 (SD = 2.95), F(1, 326) = 64.26, p < .001 (partial η2 = .17). Perceived distress scores had a possible range from 1 (No distress) to 10 (Extreme distress). Summed PTSD scores from the worst trauma ranged from 17 to 85 (M = 36.44, SD = 16.05), compared with that from the second worst trauma ranging from 17 to 81 (M = 32.71, SD = 15.30), F(1, 399) = 52.96, p < .001 (partial η2 = .12). We also estimated the prevalence of “possible PTSD” (albeit based solely on self-report rating), using a total PCL cutoff score of 44 or higher (Ruggiero et al., 2003). Using this cutoff score, among the 400 respondents with a history of trauma exposure (an “at risk” population for PTSD), 123 respondents (30.8%) would meet possible PTSD criteria based on the worst event ratings, and 94 (23.5%) would meet possible criteria based on the second worst event ratings.
Because women are twice as likely as men to develop PTSD after trauma exposure (Tolin & Foa, 2006), we assessed the relationship between gender with both summed PTSD scores and possible PTSD prevalence. Women (M = 38.52, SD = 16.26) scored higher than men (M = 30.62, SD = 13.95) on summed worst event PTSD scores, F(1, 398) = 19.64, p < .001 (partial η2 = .05). Women (M = 34.42, SD = 15.76) also scored higher than men (M = 27.89, SD = 12.80) on summed second worst event PTSD scores, F(1, 398) = 14.58, p < .001 (partial η2 = .04). Women were more likely than men to be classified with “possible PTSD” based on the worst traumatic event, χ2(1, N = 400) = 10.70, p = .001 (phi = .16), and second worst traumatic event, χ2(1, N = 400) = 5.41, p = .02 (phi = .12).
First, we present CFA model results for the worst event and second worst event models separately. The four-factor PTSD model based on the 17 worst event ratings yielded adequate model fit, χ2(113, N = 400) = 449.16, p < .001, CFI = .97, TLI = .97, RMSEA = .09 (90% CI = .08, .10). Additionally, the four-factor PTSD model based on the 17 second worst event ratings yielded adequate model fit, χ2(113, N = 400) = 392.97, p < .001, CFI = .98, TLI = .98, RMSEA = .08 (90% CI = .07, .09). Factor intercorrelations are displayed in Table 2, and standardized factor loadings are presented in Table 3.
Standardized Factor Intercorrelations and Confidence Intervals for the Worst Event and Second Worst Event PTSD Ratings
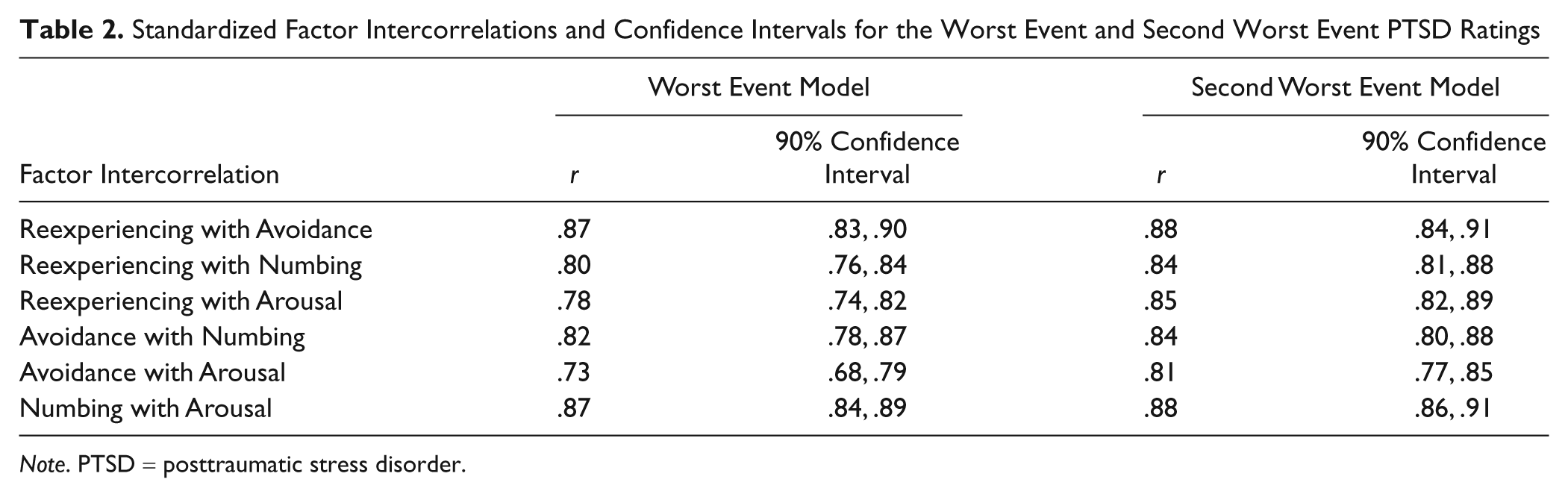
Note. PTSD = posttraumatic stress disorder.
Standardized Factor Loadings for the Worst Event and Second Worst Event PTSD Ratings
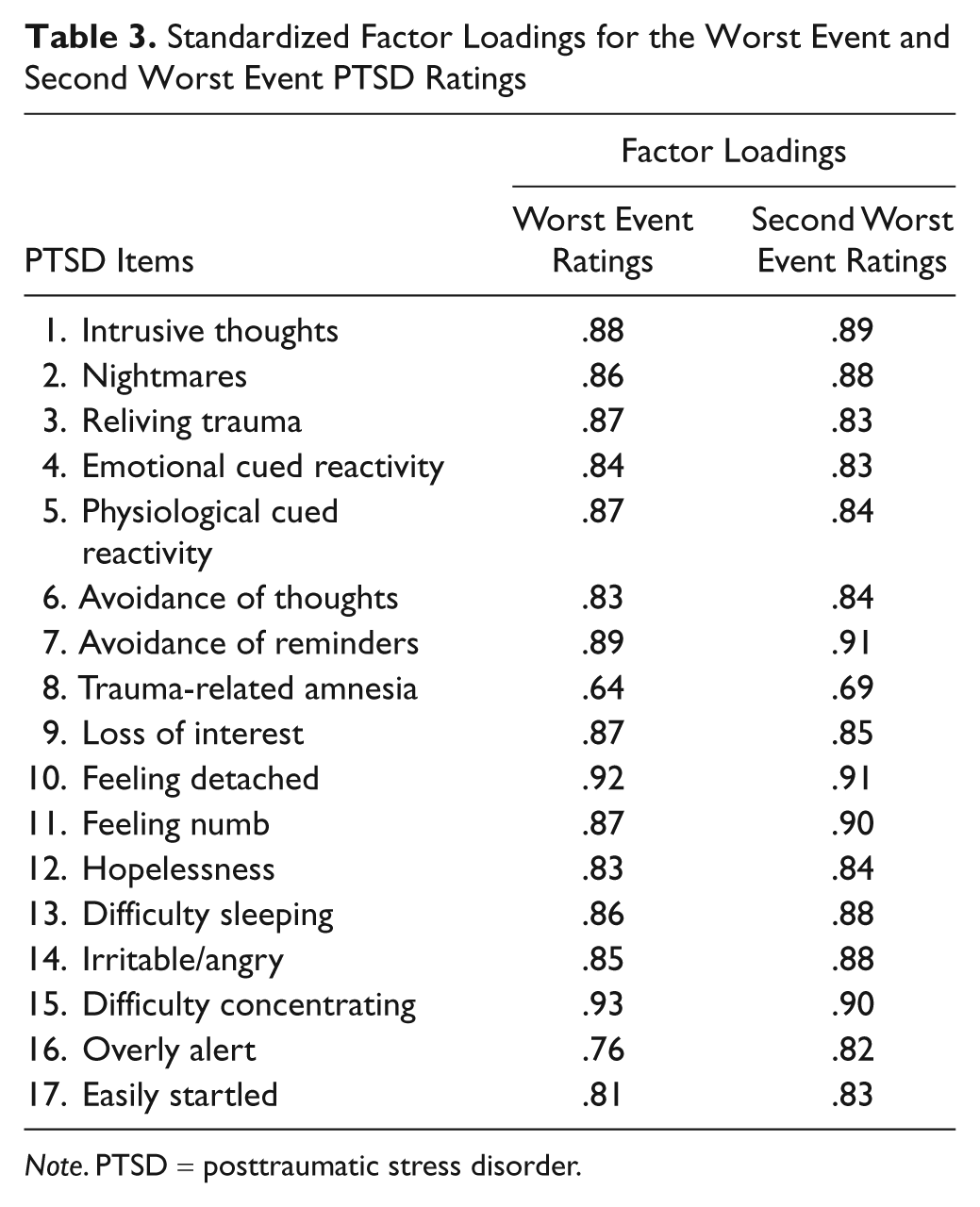
Note. PTSD = posttraumatic stress disorder.
A CFA for the four-factor PTSD model of 17 worst event and 17 second worst event PTSD items yielded adequate model fit, χ2(504, N = 400) = 1933.45, p < .001, CFI = .94, TLI = .94, RMSEA = .08 (90% CI = .08, .09). The eight-factor variation, separating the worst and second worst event PTSD ratings into different PTSD factors, resulted in excellent model fit, χ2(482, N = 400) = 1089.60, p < .001, CFI = .98, TLI = .97, RMSEA = .06 (90% CI = .05, .06). The eight-factor model fit the data significantly better than the four-factor model,
Measurement invariance analyses (using the four-factor model) formally tested differences between the worst and second worst event PTSD rating sets on the structural parameters. Based on difference tests (see the All Factors column in Table 4), analyses revealed that factor loadings were not significantly different between the worst and second worst event PTSD ratings (Models A vs. B). On the other hand, thresholds (Models B vs. C) were significantly different across symptom rating sets and higher for the worst event PTSD ratings. Chi-square difference tests are reported in Table 4 instead of changes in goodness-of-fit indices, because using the WLSMV estimator does not allow for accurate, direct comparison of such goodness-of-fit indices because of the adjusted chi-square values generated in using WLSMV estimation (Cheung & Rensvold, 2002; Sass, 2011).
Comparisons of Worst Event and Second Worst Event PTSD Ratings Using Equality Constraints in Measurement Invariance Procedures
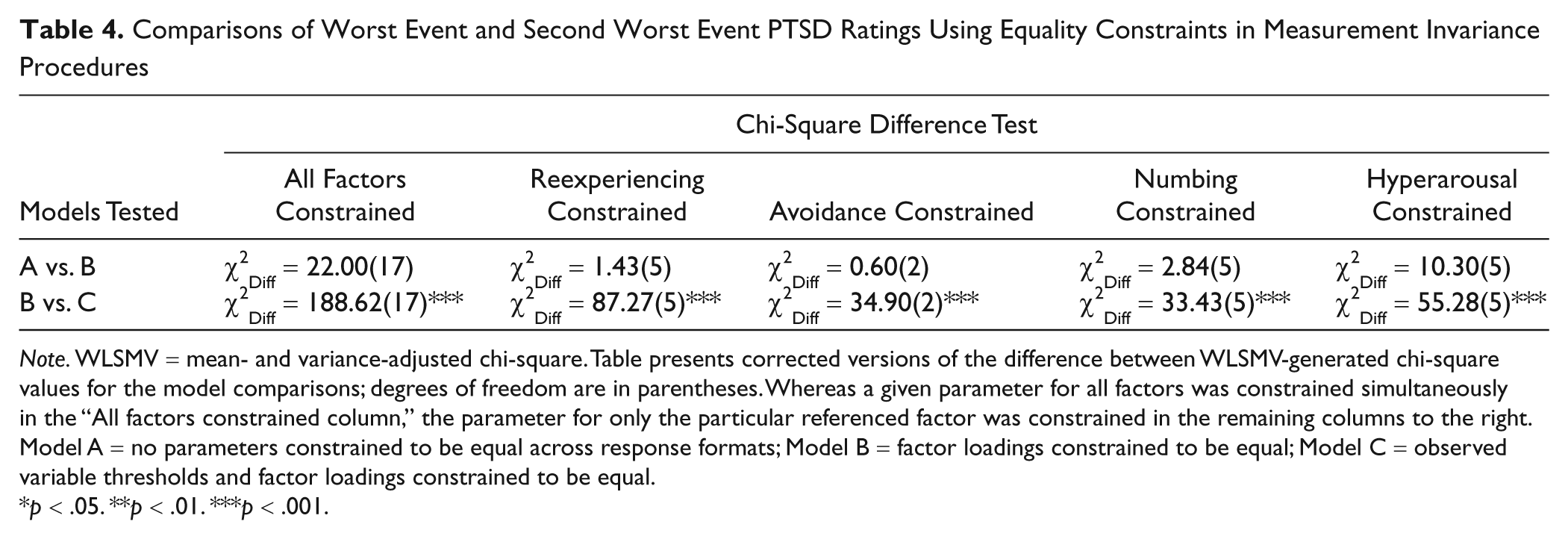
Note. WLSMV = mean- and variance-adjusted chi-square. Table presents corrected versions of the difference between WLSMV-generated chi-square values for the model comparisons; degrees of freedom are in parentheses. Whereas a given parameter for all factors was constrained simultaneously in the “All factors constrained column,” the parameter for only the particular referenced factor was constrained in the remaining columns to the right. Model A = no parameters constrained to be equal across response formats; Model B = factor loadings constrained to be equal; Model C = observed variable thresholds and factor loadings constrained to be equal.
p < .05. **p < .01. ***p < .001.
Next, we were interested in assessing whether a unique pattern of differences between the worst and second worst event PTSD rating sets was evident for specific PTSD factors, tested one at a time. We reconducted measurement invariance analyses for four sets of models, each implementing equality constraints across the worst and second worst event PTSD ratings (i.e., for loadings and thresholds) for only one of PTSD’s four factors at a time (reexperiencing, avoidance, numbing, and arousal). Table 4 indicates that these results map onto the results tested for all PTSD items overall.
Finally, we recomputed our CFA analyses, but without allowing any residual covariances for the 17 worst and second worst event PTSD item rating pairs; thus, we fixed all residual error covariances to zero. Because the worst and second worst ratings within a symptom pair are based on the same symptom, we expected to find worsened fit in these revised analyses; in fact, in our previous work, we found substantially reduced fit when not allowing residual covariances between different types of ratings (frequency vs. intensity) that were based on the same PTSD symptom (Elhai, Palmieri, Biehn, Frueh, & Magruder, 2010). Contrary to expectations, in the revised set of analyses, extremely similar fit indices were revealed, with discrepancies from the original analyses ranging only from .001 to .005 units in model parameters. Additionally, our eight-factor model was not computable because of a nonpositive definite covariance matrix. (These results are available on request from the first author.)
Discussion
Overall, we found that the worst and second worst event PTSD ratings were best modeled by separating them into distinct factors. This distinction appeared not to be influenced by factor loadings but rather by variable thresholds which index item severity.
We found that factor loadings were equivalent across the worst and second worst event PTSD ratings. Thus, the composition of factors based on individual PTSD items was essentially the same across the two PTSD symptom sets; PTSD’s nightmares symptom, for example, is equally important to the reexperiencing factor in one symptom set as in the other. The implication of this finding is that across two different self-defined traumatic events based on severity, PTSD symptom endorsements hung together in similar and predictable ways, a finding that we would expect if the PTSD construct is robust and stable across differentially severe traumas. This finding maps onto results from Yufik and Simms’s (2010) meta-analysis that demonstrated no appreciable differences in PTSD’s factor structure as a result of trauma type examined.
Despite consistency across symptom sets in factor loadings, item thresholds were different. Thus, participants appeared to discriminate item severity endorsements based on which particular traumatic event they rated their symptoms against. Elhai et al. (2009) demonstrated that item severity (based on intercepts, which are used for continuous rather than ordinal variables) was equivalent between subjects rating PTSD symptoms in relation to their worst trauma versus their trauma history as a whole. As such, we expected that this finding would generalize to the present study by demonstrating equivalent thresholds across PTSD symptom rating sets, but this was not the case. However, unlike in the authors’ previous study, which compared PTSD symptom ratings between a worst trauma versus global trauma history, in the present study we compared ratings between participants’ worst versus second worst traumas. Perhaps in Elhai et al.’s prior study, participants rating PTSD symptoms from their trauma history as whole were defining their overall trauma history by using their worst trauma as the prototype, resulting in little discrimination in symptom severity between ratings from the worst trauma versus overall trauma history. In the present study, however, providing separate traumas from which to rate PTSD symptoms appeared to result in discrimination in PTSD ratings across those traumas.
Therefore, based on our results, it appears that the worst event PTSD assessment method may function in holding the same pattern of item endorsements (in terms of how symptoms hang together and in the importance of specific symptoms to a certain factor) across the specific index event selected, but results in divergent levels of item severity across selected events. Despite Elhai, Ford, et al.’s (2010) skepticism that perhaps respondents are not able to distinguish their PTSD symptom ratings from one traumatic event over another, at least with regard to item severity the present study demonstrates that respondents may in fact be able to engage in such discrimination. Furthermore, based on our findings, we would argue that the worst event method is a more accurate method for assessing PTSD than globally querying PTSD symptoms without reference to an index trauma.
Several limitations are inherent in the present study. First, we used a self-report measure of PTSD, and thus we lacked a precise clinical interview that could be used to clarify responses and probe for further detail. Second, we used a nonclinical sample of college students, and thus generalizability to the general population or to clinical samples is unknown. In fact, given the nonclinical sample, we had a floor effect on PTSD items, such that the sample’s pattern of responding was consistent with mild to no PTSD as a whole. Additionally, we only tested our research question by examining the difference in PTSD symptom ratings between two traumas causing significantly different distress levels. In fact, it is possible that our instructions to nominate a worst and second worst event may have created demand characteristics such that subjects felt inclined by virtue of the study paradigm alone to respond more severely to the worst event PTSD items. Perhaps instructing participants to rate PTSD symptoms from various traumatic events, only later asking them to rank those events in terms of how distressing they are, could have bypassed this artifact; overcoming this artifact as such could be explored in future research. Finally, there is no way to rule out the possibility that perhaps the change in symptom rating levels between administrations was due to repeated assessment rather than based on the experimental manipulation of worst event/second worst event symptom rating.
Despite the limitations, the present study provides preliminary support for the ability of nonclinical participants to distinguish PTSD ratings separately from traumas that are self-rated as reflecting different distress levels and provides early support for the worst event method as a means of assessing PTSD. Results demonstrate that the underlying structure of PTSD may be consistent across ratings of differentially distressing traumas, but that as expected the severity of endorsements differs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.