
Abstract
Research increasingly indicates that prototypical trajectories of resilience, recovery, delayed, and chronic distress characterize reactions to acute adversity. However, trajectory research has been limited by the practical and methodological difficulties of obtaining pre-event and longitudinal data. In two studies, we employed a novel method in which trained interviewers provided a graphical depiction of prototypical stress trajectories to participants and asked them to select the one that best described their experience. In Study 1, self-identified trajectories from 21 high-exposure survivors of the September 11th World Trade Center attacks distinguished variation in posttraumatic stress disorder and depression symptoms at 7 and 18 months, and were consistent with trajectories based on longitudinal outcomes and friend/relative ratings. In Study 2, we examined self-identified trajectories from 115 bereaved spouses at 1.5 to 3 years. Persons who identified a resilient trajectory, compared with recovery and chronic distress trajectories, had fewer interviewer-rated symptoms of grief, depression, and posttraumatic stress disorder were rated as functioning more effectively by friends, reported higher life satisfaction, and had fewer somatic complaints. The present results provide initial evidence for the construct validity of a cross-sectional and less demanding method for identifying acute stress trajectories.
How do people respond to acute stress? This question has critical implications for how we study, assess, and treat exposed persons. Historically, it has been assumed that people’s reactions follow a roughly normal distribution: The modal response is moderate distress and difficulty meeting everyday obligations, while resilient and elevated stress reactions fall on the opposing tails of the distribution. Although this conceptualization has intuitive appeal, a growing body of evidence has called it into question (Bonanno, Westphal, & Mancini, 2011). Instead, it appears that the way people respond to acute stress is not captured by a single homogeneous distribution (Bonanno & Mancini, 2012). Indeed, when we examine the full range of responses to acute stress, we find a surprising degree of variation and heterogeneity.
Empirical studies increasingly indicate that this variation conforms to four prototypical patterns or trajectories: Stable and resilient functioning, elevated and chronic distress, gradual recovery, and delayed reactions (Bonanno, 2004). These prototypical trajectories have been observed following bereavement (Bonanno et al., 2002; Mancini, Bonanno, & Clark, 2011; Ott, Lueger, Kelber, & Prigerson, 2007), breast cancer surgery (Deshields, Tibbs, Fan, & Taylor, 2006; Lam et al., 2010), the World Trade Center (WTC) attacks (Bonanno, Rennicke, & Dekel, 2005), traumatic injury (deRoon-Cassini, Mancini, Rusch, & Bonanno, 2010), spinal injury (Bonanno, Kennedy, Galatzer-Levy, Lude, & Elfström, 2012), natural disaster (Norris, Tracy, & Galea, 2009), and combat deployment (Bonanno, Mancini, et al., 2012).
Despite empirical support for these trajectories, research on trajectories is still limited. One reason for the relatively sparse literature is the practical and methodological difficulties of obtaining preevent and longitudinal data. In the present study, we addressed this issue by testing an interactive retrospective method for identifying trajectories of adjustment following acute stress, one that can be used in research and clinical settings relatively easily and at a single point in time. Trained interviewers provided an oral description of the prototypical trajectories and gave participants a graphical depiction of them (Figure 1). Participants were asked to select the trajectory that best described their experience of adjustment over time. If persons exposed to acute stress can accurately report their own trajectories retrospectively, then cross-sectional designs could apply this method in cases where longitudinal research is not possible.
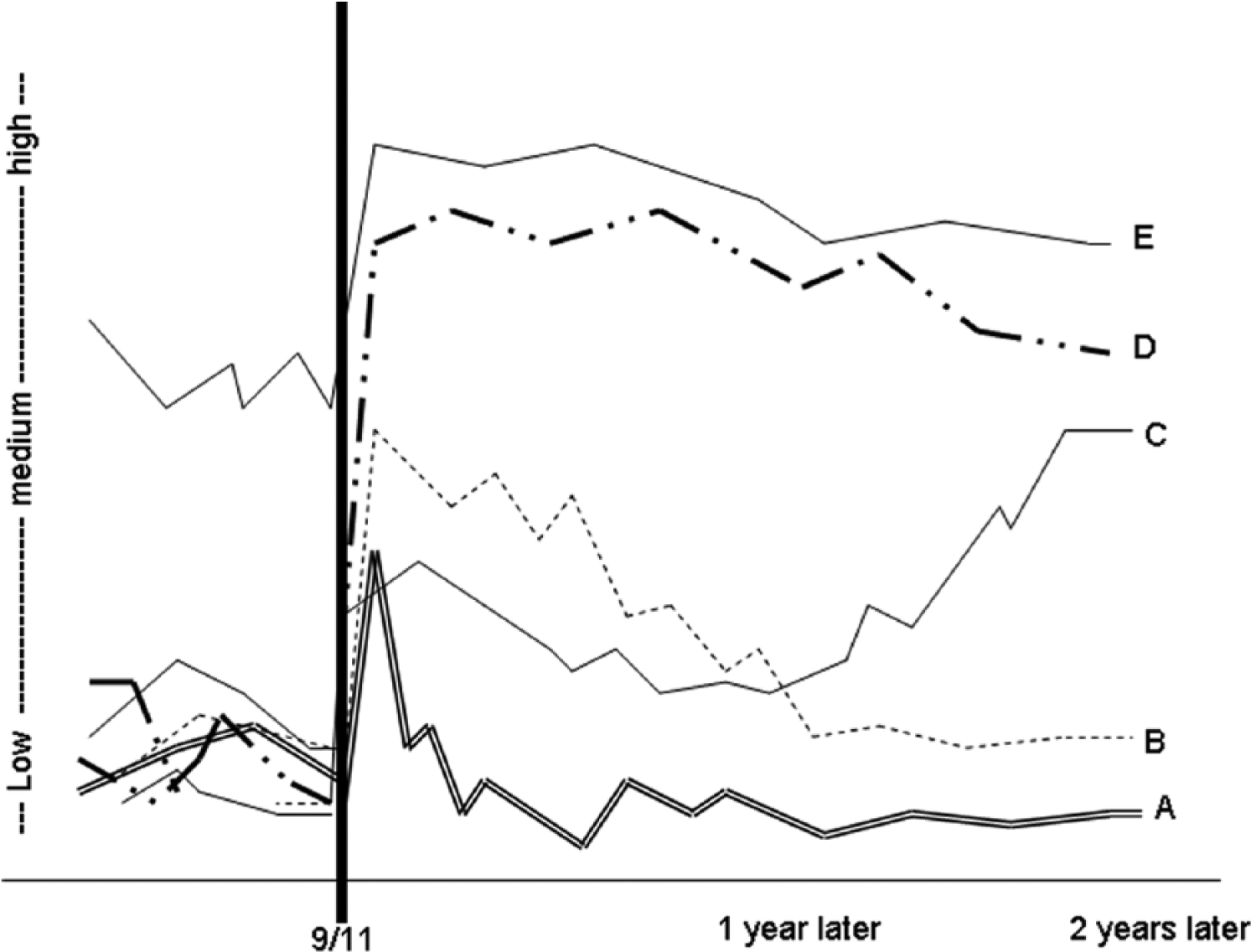
Depiction of prototypical trajectories provided to 9/11 participants.
Current Investigation
In the present research, we tested this possibility in two studies. In both studies, we examined whether the self-identified trajectories were concordant with other data sources and methods (Campbell & Fiske, 1959), including interviewer-rated measures, self-report, and friends’ ratings. We expected that the self-identified trajectory would be consistent with longitudinal assessments of trajectory pattern, other indices of functioning, and friends’ reports. We used two samples to address these issues: A longitudinal assessment of high-exposure survivors of the WTC attacks and a cross-sectional assessment of bereaved spouses at 1.5 to 3 years after the loss.
Study 1
In Study 1, we examined a unique sample of people who were in or near the WTC towers at the time of the September 11th attack. Participants completed a battery of questionnaires and were interviewed at approximately 7 and 18 months post–September 11th. As part of this battery at 18 months, trained interviewers asked participants to identify their likely trajectory of adjustment based on the prototypical patterns of resilience, recovery, delayed or chronic distress. In addition, participants reported their depression and posttraumatic stress disorder (PTSD) symptom scores at 7 and 18 months, allowing us to assign participants to one of the four trajectories of adjustment on the basis of those scores (Bonanno et al., 2005). Using these data, we compared the self-identified trajectory with continuous (symptom scores) and categorical (trajectory pattern) outcomes. To provide additional validation for the self-identified adjustment trajectories, we independently asked participants’ friends and/or relatives at 28 months post–September 11th to assign the participants to one of the four trajectories. We expected that the self-identified trajectory method would be concordant with (a) continuous assessments of depression and PTSD symptoms, (b) categorical adjustment trajectories assigned on the basis of depression and PTSD symptom scores, and (c) friend/relative ratings of adjustment trajectory.
Method
Participants and Procedure
Seventy-nine people responded to recruitment notices disseminated through companies that had been located in the WTC, flyers posted south of 14th Street in Manhattan, and public service announcements. Sixty-five people (83%) agreed to participate and returned the questionnaire materials. Participants completed the first wave of assessments at approximately 7 months post–September 11th. Each participant completed a questionnaire packet at home, an interview in our offices that included an assessment of PTSD and depression symptoms, and distributed anonymous rating forms to three close friends or relatives. At 18 months after September 11th, these procedures were repeated. In addition, a subset of the sample was (n = 21) was asked to provide ratings of their trajectory of adjustment (self-identified trajectory). At 28 months post–September 11th, we obtained an additional set of friend and relative ratings, including a friend’s rating of the adjustment trajectory of the participant. These self-identified trajectories have not been previously analyzed. Participants who provided trajectory ratings did not differ on demographic factors or on levels of distress from those who did not. (For a detailed description of participant characteristics, see Bonanno et al., 2005).
Measures
Self-Reported Distress Trajectory
Trained doctoral students provided an oral description of the trajectories to participants and then a graphical depiction and written description of each of the prototypical outcome trajectories (see Figure 1), which included resilience, chronic distress, recovery, and delayed symptoms (Bonanno, 2004), as well as a fifth trajectory indicative of continuous distress that began before September 11th. Participants were asked to select the trajectory that best resembled their experience following September 11th. Of the 21 participants with trajectory data, 9 identified themselves as resilient (43%), six identified as recovered (29%), three identified as delayed (14%), and three identified as chronic distress (14%). No participant endorsed the continuous distress trajectory.
Posttraumatic Stress and Depression
We assessed posttraumatic stress symptoms using the PTSD Symptom Scale, Self-Report Version (Foa, Riggs, Dancu, & Rothbaum, 1993), a 17-item self-report measure based on the DSM-III Diagnostic and statistical manual of mental disorders (3rd ed., rev.; American Psychiatric Association, 1987). Internal consistency was .91. Depressive symptoms were assessed using the Center for Epidemiologic Studies Depression Scale, Brief Version (Kohout, Berkman, Evans, & Cornoni-Huntley, 1993). Internal consistency was .79.
Friend and Relative Ratings
At 7 and 18 months post–September 11th, participants were provided with three packets containing consent materials and ratings forms and asked to distribute these materials to three close friends or relatives whom they felt knew them well and with whom they had relatively consistent contact. Friends and relatives returned these ratings directly to us using stamped, preaddressed envelopes. At 28-months post–September 11th, we asked friends and relatives to assign an outcome trajectory to the participant based on written and graphic depictions of the four prototypical outcome trajectories (resilience, recovery, delayed symptoms, and chronic symptoms) as well as a fifth trajectory indicative of chronic symptoms beginning prior to September 11th. Friends and relatives were asked to select the trajectory that most closely matched the participant’s. In the present study, we report data for 18 participants who had friends or relatives identify the outcome trajectory of participants.
Results
To assess the relationship of self-reported trajectories and other trajectory methods, we first assigned participants to high versus low symptom categories based on the depression cutoff scores for the Center for Epidemiologic Studies Depression Scale, Brief Version and the 7-month sample mean for PTSD symptoms (for which there is no established cutoff). Based on these designations at 7- and 18-months, participants were assigned to one of the four prototypical trajectories. (These procedures are described in detail in Bonanno et al., 2005.) Of the 21 participants who provided self-reported trajectories, eight participants (48%) were assigned to the resilient trajectory, six participants (29%) to the recovery trajectory, one participant to the delayed trajectory (5%), and six (29%) to the chronic distress trajectory. These designations were assigned blind to the self-identified trajectory.
Self-Identified Trajectories and Continuous Distress Measures at 7 and 18 Months
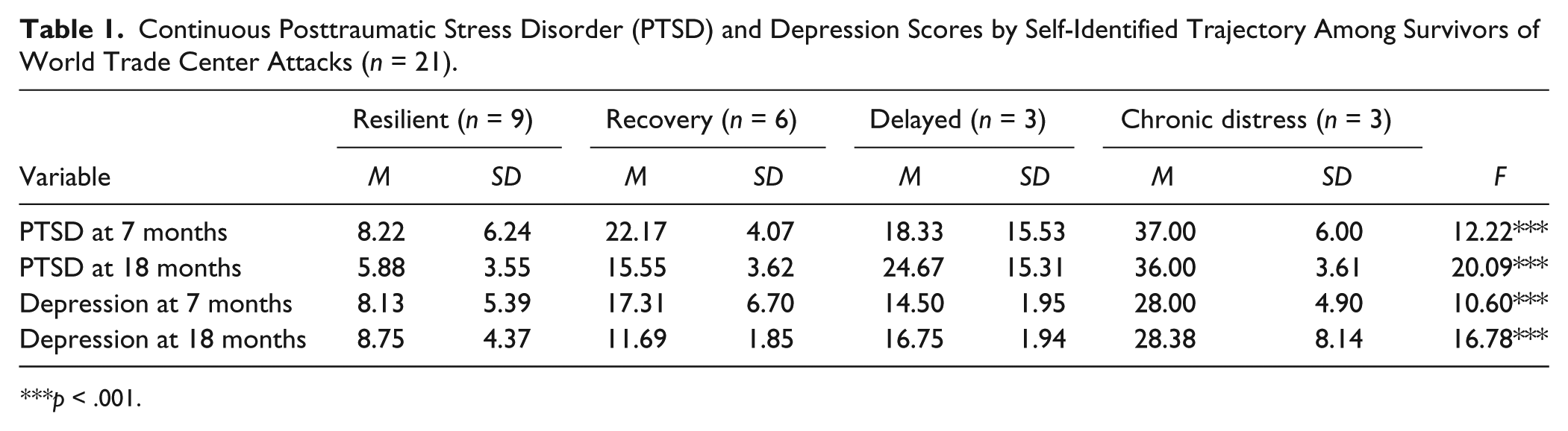
We first examined whether the self-reported trajectories distinguished variation in continuous scores for depression and PTSD at 7 and 18 months. To achieve this aim, we computed a mean value for depression and PTSD at 7 months and 18 months (see Table 1). We then conducted a series of one-way analyses of variances comparing mean values for PTSD and depression scores at 7 and 18 months for each of the trajectory groupings. We focused on the omnibus test because pairwise comparisons, given the small sample, would be difficult to draw conclusions from. Despite the small sample, trajectory grouping accounted for significant variation in all four omnibus tests (ps < .001), distinguishing PTSD and depression scores at both 7 and 18 months.
Continuous Posttraumatic Stress Disorder (PTSD) and Depression Scores by Self-Identified Trajectory Among Survivors of World Trade Center Attacks (n = 21).
p < .001.
Self-Identified Trajectories and Categorical Outcome Trajectories
We next compared self-identified trajectories at 18 months with categorical longitudinal trajectories assigned on the basis of PTSD and depression symptoms (see Table 2). We used chi-square analyses to compare the probability that the self-identified trajectory and the longitudinal trajectory were consistent. This analysis revealed a significant, nonrandom distribution across the four outcome patterns, χ2(9, N = 21) = 26.06, p = .002. Follow-up analyses of individual cells compared the frequency probability for each cell relative to chance using Haberman’s (1978) standardized, adjusted residuals statistic (HAR). Across 71.1% of the sample, the self-reported trajectory was concordant with the longitudinal outcome trajectory. One-third of the sample (33.3%) was resilient according to the self-rated and longitudinal trajectory measures, a percentage well in excess of chance probability, HAR = 3.2, p < .001. We found that 19% of the total were classified as recovery, HAR = 2.4, p = .02, on both measures; 4.8% were classified as delayed, HAR = 2.3, p = .02, on both measures; and 14.3% being classified as chronic distress, HAR = 3.0, p < .01, on both measures. These results confirmed that participants’ rating of their trajectory is concordant with the assignment of trajectory based on longitudinal outcome measures.
Agreement Between Self-Identified and Longitudinal Trajectories Among Survivors of World Trade Center Attacks.
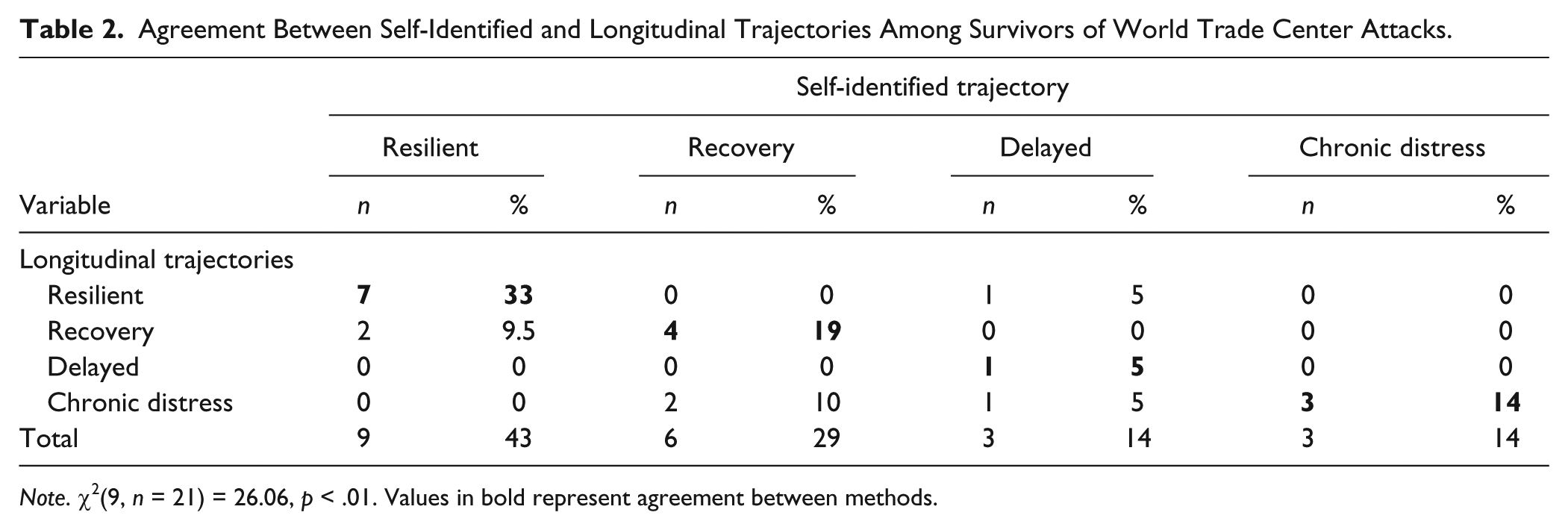
Note. χ2(9, n = 21) = 26.06, p < .01. Values in bold represent agreement between methods.
Self-Identified Trajectories and Friend/Relative Ratings
Finally, as shown in Table 3, we examined the relation of self-reported trajectory to friend and relative assignments of trajectory. We had at least one friend rating for 18 participants, and two trajectory ratings for 11 participants. We expected that a similar convergence of the two measures would be observed in chi-square analyses. We compared the self-reported trajectory with a single randomly selected friend. The analysis revealed a significant, nonrandom distribution across the four outcome patterns, χ2(9, n = 18) = 19.64, p = .02. Using HAR to assess frequency probability, we found that 66.7% of the sample showed concordance for the two measures, with 38.9% being identified as resilient on both the self-rated and friend/relative-rated trajectory, HAR = 3.3, p < .001; 16.7% being classified as recovery, HAR = 1.9, p = .057, on both measures; and 11.1% being classified as chronic distress, HAR = 2.5, p < .012, on both measures.
Agreement Between Self-Identified and Friend-Rated Trajectories Among Survivors of World Trade Center Attacks.
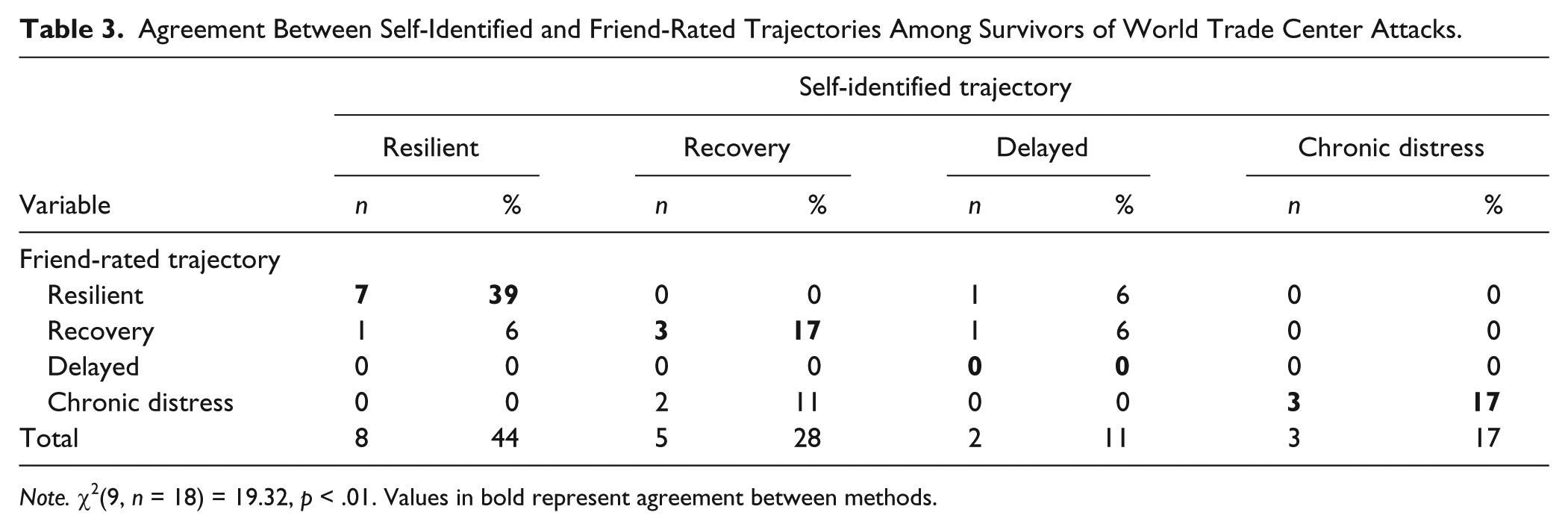
Note. χ2(9, n = 18) = 19.32, p < .01. Values in bold represent agreement between methods.
Discussion
The results of Study 1 provided initial evidence that the self-identified trajectory method has convergent validity among a sample of high exposure survivors of the WTC attacks. Self-identified trajectories significantly distinguished variation in PTSD and depression symptoms at both 7 and 18 months, were consistent with categorical outcome trajectories determined on the basis of PTSD and depression symptoms, and showed significant relations to friend/relative ratings of trajectory pattern.
Although these results support the trajectory method, there were some key limitations. A principal limitation was the small sample. Thus, it is unclear how generalizable our findings are and whether they are robust. An additional issue is that the sample was exposed to an exceptionally acute stressor, the WTC attacks. Although this suggests that the method can be used for persons exposed to extreme events, it is unclear that similar findings would obtain following a more normative stressor. In addition, because this study was longitudinal and produced relatively prototypical patterns of outcome, it is possible that trajectory assignments may have been informed by population norms. In other words, participants and friend/relative raters may have believed, on the basis of cultural assumptions, that they should have experienced a particular trajectory of response (e.g., chronic distress). A more rigorous test would therefore be to apply the method when specific trajectories are deliberately oversampled.
Study 2
In Study 2, we sought to address these limitations by applying the same method to a larger sample of persons and to a stressor that is more normative, the loss of a spouse. We used the same interactive self-identified trajectory method among a larger sample of bereaved spouses at 1.5 to 3 years after the loss. A key feature of this study is that the sample was recruited specifically to include a greater proportion of chronic dysfunction and a lesser proportion of resilient outcomes.
Our analyses had two primary aims. First, we wanted to provide additional convergent evidence for the construct validity of the self-identified trajectory method. To achieve this end, we compared the self-reported trajectory patterns with friend/relative ratings of trajectory. As in Study 1, we expected these ratings to be concordant with the self-identified trajectory. We sought to further validate the self-identified trajectory by comparing it with other indices of functioning, including interviewer ratings of global functioning, depression, grief, and PTSD symptoms, as well as self-reported somatic symptoms and life satisfaction. We expected the resilient group to show a clear pattern of adaptive functioning in relation to the recovery and prolonged groups. We further expected the recovery group to show intermediate levels of functioning compared with the resilient and the prolonged grief groups.
To address our hypotheses, we used the trajectory patterns as the independent variable in between group analyses, followed by pairwise comparisons to identify differences among bereavement trajectories. To ensure a comparison with persons with normative levels of functioning, a final critical element of our approach was comparisons with a married control group. We note that married controls are rare in bereavement research but address crucial alternate hypotheses. Specifically, the married controls allowed us to distinguish mild symptom elevations among the resilient bereaved, which are normative, from symptoms that occur in response to bereavement. They also allowed us to evaluate correlates of each trajectory pattern with reference to a normative sample.
Method
Sample and Procedure
Bereaved spouses and nonbereaved married control participants younger than 65 years in the New York metropolitan area were recruited by distributing flyers, posting advertisements in local newspapers and online, and sending letters to recently bereaved persons listed in public obituaries and to individuals likely to have contact with bereaved persons (for example, leaders of bereavement support groups at community organizations and local hospitals). We specifically recruited grievers with significant levels of distress in our postings and advertisements. Participants received $200 for completing two 2-hour sessions, involving the completion of questionnaires, interviews, and experimental tasks. One hundred and sixteen bereaved and 74 married participants eventually enrolled in the study, which was approved by the institutional review board at Teachers College, Columbia University. Enrolled participants completed a questionnaire, a structured clinical interview, a semistructured narrative interview, and experimental tasks. In addition, participants were asked to provide forms to friends or relatives that requested information about the participants’ level of functioning and grief. Seventy-one participants had friend/relative ratings. Participants whose friends provided trajectory ratings did not differ on demographic factors or on levels of distress from participants whose friends did not provide ratings (ps < .21). The present study analyzed self-report, interview, and friend/relative data (for a more detailed account of the sample, see Gupta & Bonanno, 2011; Mancini & Bonanno, 2012).
Measures
Self-Reported Bereavement Trajectory
We used the same method as in Study 1. Unlike Study 1, however, we did not include a delayed distress trajectory in the graphical depiction, because of the absence of empirical support for delayed grief (Bonanno & Field, 2001). Of the 116 participants, 33 identified themselves as resilient (28%), 40 identified as recovered (35%), 31 identified as prolonged grievers (27%), and 12 identified as continuous distress (10%). Because only 12 participants endorsed the pre–post continuous distress trajectory, which did not afford sufficient statistical power to make meaningful comparisons in analyses of continuous variables, we omitted those participants from those analyses.
Functioning
Using criteria from the DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision; American Psychiatric Association, 2000) on Axis I disorders (Spitzer, Williams, Gibbon, & First, 1990), trained clinical interviewers administered a questionnaire to measure symptoms of posttraumatic stress disorder and major depressive disorder. We used symptoms derived from Horowitz, Siegel, Holen, and Bonanno (1997) to measure grief. These included strong yearning; preoccupation with the loss; recurrent regrets or self-blame; recurrent regrets or blame regarding others; difficulty accepting the loss; sense of emptiness; sense that life is meaningless; difficulty developing new relationships. As part of the structured interview, trained interviewers also assigned a score on a 0 to 100 scale to assess global functioning based on criteria detailed in the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, fourth edition; American Psychiatric Association, 1994). Interviewers were 9 doctoral candidates in clinical psychology. To increase reliability for symptom interviews and global functioning, each interviewer coded videotapes of five interviews (κ =. 92) and rated additional videotaped interviews for global functioning (intraclass correlation = .88). Somatic complaints were measured using an 18-item checklist format (Marmot et al., 1991). Representative items include “cough” and “toothache.” For this study, α = .83.
Interviewer Ratings
Interviewers rated participants’ degree of suffering on a 7-point scale, where 1 = not at all and 7 = severely, and how much they liked the participant, where 1 = much less than others and 7 = much more than others.
Friend and Relative Ratings
Participants were provided packets containing consent materials and ratings forms and asked to distribute these materials to three close friends or relatives whom they felt knew them well and with whom they had relatively consistent contact. These materials asked friends and relatives to rate the participant on two scales: Participant’s adjustment prior to the loss was compared with “most other people” using a 7-point scale (1 = much worse than most people; 7 = much better than most people) for five dimensions (mental health, physical health, quality of social interactions, ability to accomplish goals, and coping ability; .81). Change in participant’s current level of adjustment (at 7 and 18 months) was rated “in comparison with his or her usual level” using a 7-point scale (1 = much worse than usual; 7 = much better than usual) for the same five dimensions. We averaged the two scales into a single index of adjustment. In addition, as in Study 1, we asked friends and relatives to assign an outcome trajectory to the participant based on written and graphic depictions of the four prototypical outcome trajectories (resilience, recovery, prolonged grief, and continuous distress). Seventy participants had at least one friend/relative rating, and 56 participants had two ratings.
Results
To further establish the convergent validity of the method, we first compared the self-rated trajectory with friends/relative rating of trajectory using chi-square analyses. We used trajectory designation as the independent variable in a series of one-way analyses of variance. Omnibus differences were followed up by pairwise comparisons using the Student-Newman Kuels test. For categorical predictors, we used chi-square tests to examine group differences and Haberman’s standardized adjusted residual statistic for pairwise differences. Means and standard deviations for all variables by group are summarized in Table 5.
Self-Identified Trajectory and Friend/Relative Ratings
Consistent with Study 1, we compared the self-reported trajectory with a single friend rating (randomly selected when there was more than one rating). For this analysis, we included the continuous distress trajectory, because removing it would have reduced the sample and arbitrarily excluded some friend ratings. As shown in Table 4, the analysis revealed a significant, nonrandom distribution across the four outcome patterns, χ2(9, N = 71) = 17.18, p = .05. Using HAR to assess frequency probability, we found that 48.5% of the sample showed concordance for the two measures, with 22.9% being identified as resilient on both the self-rated and friend/relative-rated trajectory, HAR = 3.2, p < .001; 12.9% being classified as recovery, HAR = 2.1, p = .04, on both measures; and 10% being classified as chronic distress, HAR = 1.8, p = .07, on both measures. None of the participants who reported the continuous distress trajectory were identified as continuous distress by their friends.
Agreement Between Self-Identified and Friend-Rated Trajectories Among Bereaved Participants.
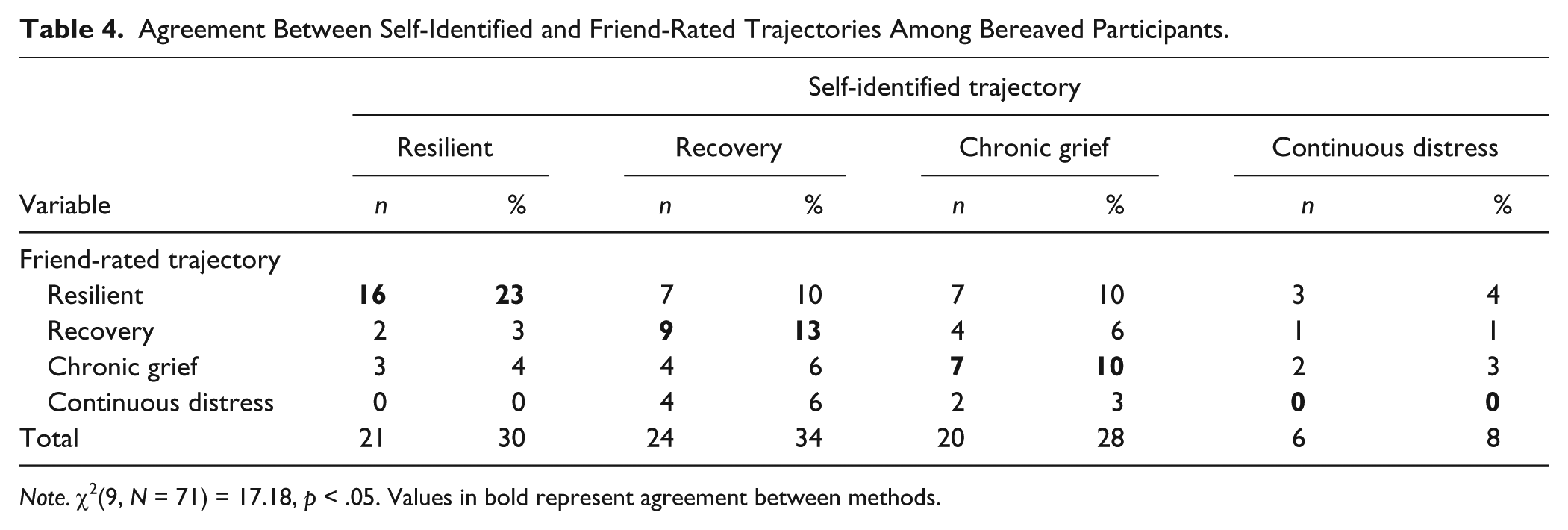
Note. χ2(9, N = 71) = 17.18, p < .05. Values in bold represent agreement between methods.
Correlates of Simple Agreement
We next examined whether simple agreement between self-identified and friend/relative trajectory (coded as 1 = agreement, 0 = nonagreement) was correlated with specific trajectory patterns, demographics, or levels of distress using chi-square analyses and independent sample t tests. First, we found that simple agreement between participant and friend/relative did show variation across the four trajectories χ2(3, N = 71) = 13.95, p < .01. Follow-up analyses showed that the resilient trajectory was significantly more likely to show simple agreement, HAR = 3.3, p < .01, whereas the continuous distress trajectory was inversely associated with simple agreement HAR = −2.4, p < .01. Second, participant demographics (age, gender, education, family income; ps < .12) showed no relation to agreement. Third, there was a marginal tendency, t = 1.90, p < .07, for participants who disagreed with their friend/relative to report more grief (M = 2.55, SD = 2.11) than those who agreed (M = 1.55, SD = 2.33). A similar marginal tendency emerged for PTSD symptoms, t = 1.70, p < .10, among participants who disagreed (M = 4.34, SD = 3.47) than agreed (M = 2.93, SD = 3.46).
Trajectory Comparisons
To further address convergent validity of the self-identified trajectory method, we next compared it with interviewer-rated depression, PTSD, and grief symptoms, and GAF (Global Assessment of Functioning) scores, and with self-reported somatic symptoms and life satisfaction (see Table 5). We expected that persons who identified themselves as resilient would show a pattern of adaptive functioning across various indices. Resilient persons had significantly fewer PTSD and depression symptoms, higher GAF scores, higher life satisfaction, and fewer somatic complaints than the prolonged grief group. Consistent with the idea that the recovery trajectory represents an intermediate level of functioning, individuals who reported the recovery pattern had significantly fewer PTSD and depression symptoms, higher life satisfaction, and higher GAF scores when compared with the prolonged grief group. As expected, no differences emerged between resilient and married persons. However, substantial differences emerged between prolonged grievers and married persons, with prolonged grievers showing less adaptive functioning.
Demographic, Functioning, and Other Variables by Self-Identified Trajectory and Married Control.
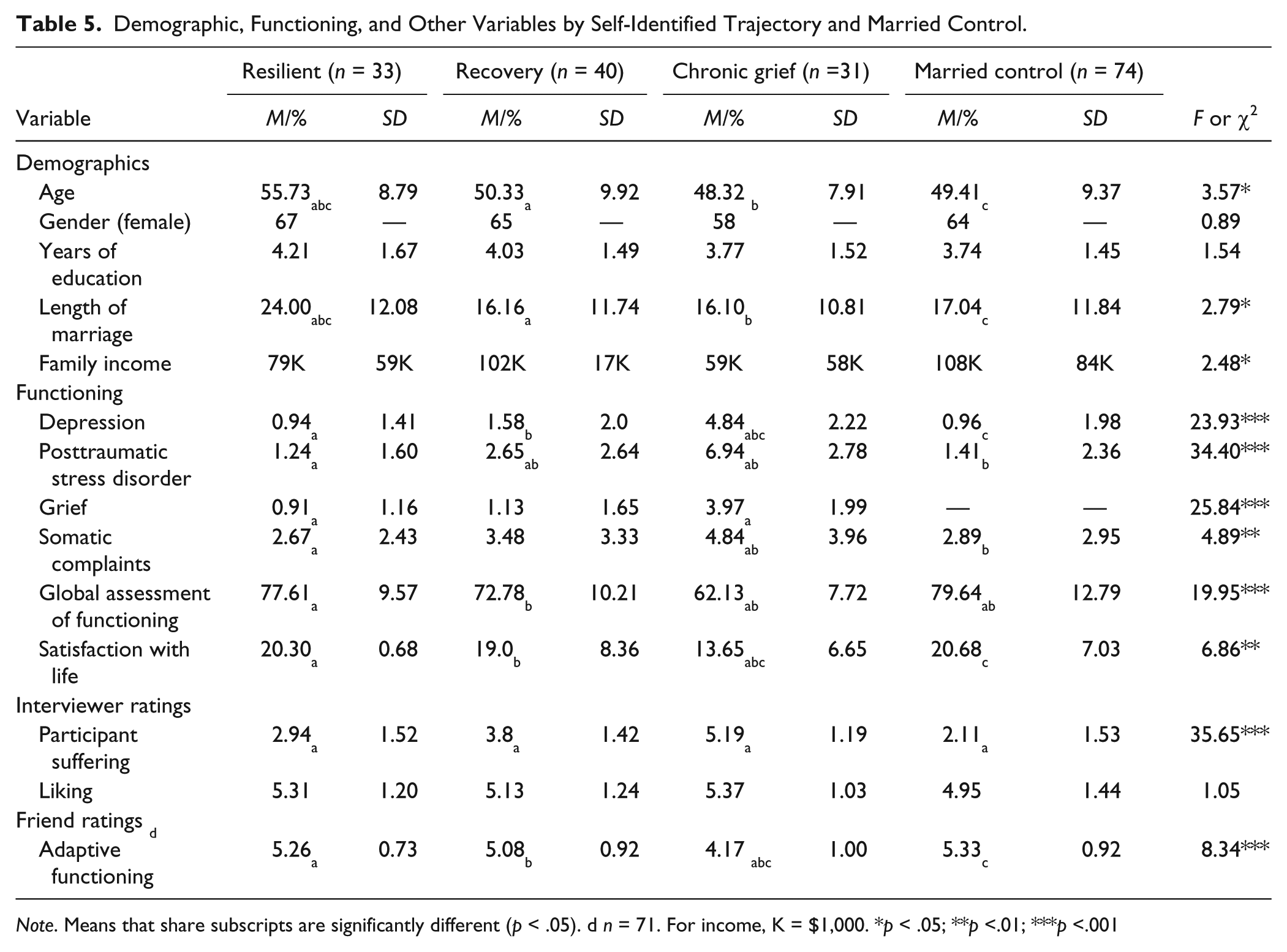
Note. Means that share subscripts are significantly different (p < .05). d n = 71. For income, K = $1,000. *p < .05; **p <.01; ***p <.001
Discussion
These results provided additional support for the retrospective trajectory method: The trajectory the participant identified was consistent, in terms of the degree of impairment and level of functioning, with interviewer-rated symptoms of depression, PTSD, grief, and overall functioning, and with self-reported somatic symptoms and life satisfaction. Consistent with Study 1, the self-identified trajectory also accorded with friend/relative ratings of trajectory, although the level of agreement was modest; resilience was more likely to show agreement between informants; and higher levels of distress were marginally associated with disagreement between informants. Nevertheless, it is worth emphasizing that these findings obtained in a sample of persons who experienced a normative stressor, the loss of a spouse, and who were recruited according to their level of distress. These factors provide additional support for the validity and generalizability of the self-report trajectory method.
General Discussion
A growing literature has examined prototypical trajectories of adjustment following interpersonal loss and other acute stressors (Bonanno, 2004; deRoon-Cassini et al., 2010; Deshields et al., 2006; Hobfoll et al., 2009; Mancini et al., 2011). However, the arduousness of collecting longitudinal data has limited our capacity to understand these trajectories. Indeed, we have only preliminary indications of what factors distinguish persons who experience one trajectory over another. In the present research, we provided evidence for the validity of an alternate self-report method for identifying longitudinal trajectories. This method can be used at a single point in time and has applications for research and for clinical assessment.
In support of the validity of the method, we found that self-reported trajectories were concordant with alternate methods among high exposure survivors of the September 11th terrorist attacks and bereaved spouses. Longitudinal outcome trajectories of WTC survivors, determined on the basis of PTSD and depression symptoms, were strikingly similar to participant’s self-identified trajectory. Continuous assessments of PTSD and depression symptoms among WTC survivors also showed significant variation according to the self-identified trajectory, as did continuous assessments of grief-related distress (PTSD, grief, and depression) among bereaved spouses. Finally, friend/relative ratings of WTC survivors’ trajectory of adjustment were concordant with the participant’s self-identified trajectory, and similar results emerged when we compared the self-identified trajectory of bereaved spouses with friend/relative ratings. We emphasize that these findings involved various methods, including an interactive task (self-identified trajectory), self-report (indices of functioning), and interviewer ratings (symptomatology and global functioning), which removes common method variance as an explanation for these effects (Campbell & Fiske, 1959).
Our results comport with and extend prior research in several key respects. For example, we found clear support for resilient bereaved persons’ psychological health and adaptive functioning. Across multiple variables and outcomes, the resilient group showed superior functioning to the other trajectory groups. Resilient persons had fewer depression, grief, and PTSD symptoms, as well as fewer somatic complaints, than the prolonged grief group.
Further comparisons between the trajectory groups and the married controls supported the self-identified trajectory approach. Resilient persons did not differ from married controls on any aspect of adaptive functioning, indicating a normative profile of genuine psychological health that is not merely better than that of other bereaved persons. By contrast, prolonged grievers differed substantially from married controls on every measured aspect of functioning, showing elevated depression, PTSD, and somatic symptoms, and reduced life satisfaction and global functioning, as well as lower friend/relative ratings on adaptive functioning. Consistent with the potential for long-term residual effects of spousal loss, recovered persons showed some differences from the married control group, including significantly more PTSD symptoms and lower global functioning but on the whole showed a profile of relative psychological health.
Although these results supported the self-identified trajectory method, there were some anomalous findings, particularly with respect to friend/relative ratings of trajectory. Whereas agreement was relatively high among the 9/11 sample (66.7%), it was more modest among the bereaved sample (48.5%), though still substantially better than chance. The reasons for these differences are likely complex. One possible explanation is that 9/11 was an event of such magnitude and afflicted this high exposure sample in such a significant way that friends and relatives were more attentive to the participants’ reaction to it. By contrast, grief following loss, a more private experience, may not have prompted the same degree of scrutiny by friends, and may as well be more difficult for friends to detect. According to the self-other knowledge asymmetry model (Vazire, 2010), characteristics that are low in observability (such as neuroticism) are less likely to be accurately perceived by others, whereas characteristics that are high in evaluativeness (such as intelligence) may be more accurately perceived by others than by the self. By this logic, the affected individual would be the best judge of their adjustment, because internal distress is low in observability, and the concordance of self-ratings for high distress trajectories (chronic distress and recovery) with those of others should be relatively modest. Consistent with this perspective, the highest degree of agreement between self and friend/relative ratings was for the resilient trajectory, which is likely higher in observability because it implies behavioral correlates (such as seeing friends, engaging in activities).
Alternatively, correspondence with the self-identified trajectories may have been higher in the 9/11 sample because that sample had been assessed longitudinally. By contrast, the bereaved sample was assessed only once, at a single time point. The act of participating in repeated assessment interviews may have helped our 9/11 participants recall or construct a more meaningful and more accurate understanding of their level of adjustment over time.
Even in the context of these anomalous findings, the current results offered, on the whole, consistent support for the construct validity of the self-identified trajectory method. Persons who identified themselves as resilient were rated as suffering less by interviewers, and had fewer symptoms and higher adaptive functioning than the prolonged or recovered groups. The recovery group evidenced relatively few differences from the other groups, but those differences suggested an intermediate level of functioning, as would be expected. By contrast, the prolonged grief showed lower levels of adaptive functioning than both the resilient and recovery groups and substantially less than married controls.
The results suggest that this approach may have utility in both clinical and research settings. Therapists could use the self-identified trajectory in assessment and treatment planning, helping to determine the underlying source of the client’s distress or even whether treatment is warranted at all. It is now widely thought that people who demonstrate a resilient or even a normative grief reaction (i.e., recovery) should not receive grief-focused therapeutic approaches (Lilienfeld, 2007), and there is strong evidence that grief therapy is ineffective in the absence of significant grief-related distress (Currier, Neimeyer, & Berman, 2008). Moreover, early interventions for trauma have had a poor track record, at least in part, according to theorists (Litz, Gray, Bryant, & Adler, 2002), because people are being targeted for intervention when they may require no treatment at all. Researchers could also employ the retrospective method in situations where longitudinal data collection is not possible. The current method takes about 5 minutes to complete, provides a quick summary of the client’s longitudinal adaptation, and has direct relevance for intervention. 1
This study has a number of limitations. We established trajectories using an interactive task in which participants identified their own probable trajectory pattern. Thus, it is possible that participants’ current level of functioning may have influenced their assessment of the appropriate trajectory. That is, retrospective memory biases could have played a role in their identification of the trajectory. An additional limitation is that although the strongest test of our hypothesis—comparing the self-identified trajectory with actual longitudinal assessment—was affirmative, these data were based on a very small sample of 21 participants. Thus, additional research employing the method with a larger sample is a clear priority. We also did not assess additional stressful events that might have occurred between the stressor event and our assessment. It is possible that other stressors influenced the participants’ rating of their trajectory. A final limitation is that, because the trajectories were self-selected, we could not match participants on demographic variables, including age, gender, and income. However, we note that these differences were also a focus of investigation, and revealed findings consistent with prior research (for example, the association of older age with the resilient trajectory).
The current findings offer preliminary support for an alternative method to collecting longitudinal data following acute stress. The present method may also have potential use for clinical assessment. This method can potentially be readily adopted by researchers and clinicians alike with modest training and few resources. In addition to providing initial evidence for the validity of the assessment method, we would add that the present results add to a growing body of literature that resilient bereaved persons are psychologically healthy and show no enduring effects of the loss. By contrast, prolonged grievers showed substantial effects of the loss, even after 1.5 to 3 years. These results underscore that prolonged grief is a debilitating syndrome that is appropriate for clinical intervention (Mancini, Griffin, & Bonanno, 2012).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The research reported in this article was supported by a National Institutes of Health grant (RO1 MH703595) to George A Bonanno.