
Abstract
To assess the reliability and construct validity of the Personality Inventory for DSM-5 Brief Form (PID-5-BF) among adolescents, 877 Italian high school students were administered the PID-5-BF. Participants were administered also the Measure of Disordered Personality Functioning (MDPF) as a criterion measure. In the full sample, Cronbach’s alpha values for the PID-5-BF scales ranged from .59 (Detachment) to .77 (Psychoticism); in addition, all PID-5-BF scales showed mean interitem correlation values in the .22 to .40 range. Cronbach’s alpha values for the PID-5-BF total score was .83 (mean interitem r = .16). Although 2-month test–retest reliability could be assessed only in a small (n = 42) subsample of participants, all PID-5-BF scale scores showed adequate temporal stability, as indexed by intraclass r values ranging from .78 (Negative Affectivity) to .97 (Detachment), all ps <.001. Exploratory structural equation modeling analyses provided at least moderate support for the a priori model of PID-5-BF items. Multiple regression analyses showed that PID-5-BF scales predicted a nonnegligible amount of variance in MDPF Non-Cooperativeness, adjusted R2 = .17, p < .001, and Non-Coping scales, adjusted R2 = .32, p < .001. Similarly, the PID-5-BF total score was a significant predictor of both MDPF Non-Coping, and Non-Cooperativeness scales.
Keywords
To address various concerns with personality disorder (PD) categories in use since the third edition of Diagnostic and Statistical Manual of Mental Disorders (DSM-III; American Psychiatric Association, 1980)—for example, lack of empirically validated cutoffs, extensive comorbidity, and temporal instability (Widiger & Trull, 2007)—an Alternative Model of Personality Disorder (AMPD) was provided in DSM-5 Section III (American Psychiatric Association, 2013a), along with traditional PD symptom criteria listed in DSM-5 Section II (which reprints DSM-IV [American Psychiatric Association, 1994] Axis II PD symptom criteria). DSM-5’s AMPD requires evidence for impaired self- and interpersonal functions of personality (i.e., Criterion A) of at least moderate severity level for PD diagnosis. A core component (i.e., Criterion B) of the DSM-5 AMPD is an empirically based model of maladaptive personality traits (Krueger & Markon, 2014). In particular, the AMPD allows clinicians to assess five major domains of maladaptive personality—namely, Negative Affectivity (frequent and intense experiences of high levels of a wide range of negative emotions), Detachment (avoidance of socioemotional experience), Antagonism (behaviors that put the individual at odds with other people), Disinhibition (orientation toward immediate gratification and impulsive behavior), and Psychoticism (a wide range of culturally incongruent odd, eccentric, or unusual behaviors and cognition).
This model did not arise de novo; rather, it represents a synthesis of existing dimensional models of personality pathology, focused on maladaptive variants (e.g., Clark, 2007; Harkness, McNulty, & Ben-Porath, 1995; Trull & Durrett, 2005; Widiger & Simonsen, 2005). Although there is a consensus that extremity on personality traits is insufficient to identify personality disorder (e.g., Livesley & Jang, 2000; Wakefield, 2008), it should be observed that the PID-5 traits are maladaptive personality traits rather than normative personality traits. Indeed, they operationalize five specific maladaptive personality trait dimensions with a focus on the poles that are associated with traditionally-defined PDs (i.e., detachment, antagonism, disinhibition, negative affectivity, and psychoticism).
Although assessment of severity level of impairment in self and interpersonal function of personality cannot be derived simply by the assessment of the level of DSM-5 AMPD dysfunctional PD traits, it should be stressed that dysfunctional personality traits represent cognitive, behavioral and affective indicators of personality dysfunction; indeed, both moderate impairment or greater in personality (self/interpersonal) functioning, and one or more pathological personality traits are necessary to diagnose PD according to DSM-5 AMPD (Skodol, 2014). Although thorough assessment of both DSM-5 AMPD criteria is necessary to yield PD diagnoses, subjects may be screened for possible presence of PD psychopathology using either measures of impairment in self/interpersonal function or measures of pathological personality traits/domains. Indeed, specific impairment in self/interpersonal function may also involve pathological trait manifestations (e.g., grandiosity in DSM-5 AMPD criteria for Narcissistic PD is present among possible impairment in self function and among defining traits, along with Attention Seeking); similarly, several DSM-5 AMPD pathological traits and domains also involve impairment in interpersonal functioning (e.g., Hostility, Intimacy Avoidance, Callousness, Deceitfulness, Manipulativeness, Withdrawal, Suspiciousness, Irresponsibility, etc.) and/or self-function (e.g., Separation Insecurity, Submissiveness, Anhedonia, Depressivity, Grandiosity, Attention Seeking, etc.).
The Personality Inventory for DSM-5
Based on this model, Krueger, Derringer, Markon, Watson, and Skodol (2012) developed the Personality Inventory for DSM-5 (PID-5); the PID-5 is a 220-item self-report questionnaire with a 4-point response scale; it yields 25 primary scales that can be combined to also delineate 5 higher order scales (Negative Affectivity, Detachment, Antagonism, Disinhibition, and Psychoticism). Indeed, a burgeoning literature is yielding consistent evidence for the validity of the DSM-5 trait model as it is operationalized in the PID-5. A substantial body of literature suggest that the PID-5 can account for the reliable variance in DSM-IV personality disorders, as well as for specific clinical constructs beyond personality traits and personality disorders (e.g., dysfunctional beliefs; Krueger & Markon, 2014); moreover, the DSM-5 traits as they are operationalized in the PID-5 can be well understood as a maladaptive extension of the five-factor model of personality (Suzuki, Samuel, Pahlen, & Krueger, 2015). The PID-5 scales also proved useful in provide orienting dimensions for identifying the empirical structure of psychopathology (Wright & Simms, 2014). Data strongly support a hierarchical structure of PID-5 pathological traits ranging from a general personality pathology factor to a two-factor (i.e., internalizing pathological trait factor vs. externalizing pathological trait factor) and a three-factor (internalizing factor, externalizing factor, and detachment factor) down to a five-factor model of maladaptive personality domains (Wright et al., 2012). The PID-5 has been translated and validated in a number of languages, including Italian (Fossati, Krueger, Markon, Borroni, & Maffei, 2013).
In addition to the 220-item self-report version of PID-5, a number of alternative forms of the PID-5 have been developed in recent years; for instance, Markon, Quilty, Bagby, and Krueger (2013) developed and validated the informant-report form of the PID-5 (i.e., the PID-5-IRF). Recently, Maples and colleagues (2015), through the use of item response theory methods proposed a 100-item version of the PID-5 to score the DSM-5 domains and facets that resulted in nearly identical reliability and validity and similar nomological networks with the PID-5 (Maples et al., 2015).
The Personality Inventory for DSM-5 Brief Form
Interestingly, a very brief form of the PID-5 (PID-5-BF) has been made available to researchers and clinicians (American Psychiatric Association, 2013b). The PID-5-BF is not proposed as a fine-grained measure for assessing AMPD traits; rather, it was designed to screen for possible personality disorder by quantifying the overall elevation of scores across the five broad maladaptive trait dimensions listed in DSM-5 Criterion B. As a screening measure for personality pathology, the PID-5-BF has several potentially attractive features. The PID-5-BF is a 25-item self-rated measure for maladaptive personality trait assessment which can be administered to both adults and adolescents (namely, children aged 11-17 years). The PID-5-BF items come from the 220-item self-report PID-5. As in the PID-5, each PID-5-BF item is rated on a 4-point scale (American Psychiatric Association, 2013b).
The PID-5-BF assesses the 5 AMPD maladaptive trait dimensions of Negative Affectivity (NA), Detachment (De), Antagonism (A), Disinhibition (Di), and Psychoticism (Ps), with each domain scale consisting of 5 items; in addition, the PID-5-BF yields a score for the overall measure. The availability and routine use of a brief screen for personality pathology could potentially permit earlier detection of personality pathology in samples of community-dwelling adolescents (and hopefully also in clinically referred adolescents), perhaps prior to the development of more severe externalizing (e.g., drug abuse, deliberate self-harm, aggressive behavior, etc.) and internalizing (e.g., depression, anxiety symptoms, etc.) indicators. The availability of a brief and reliable screen for maladaptive personality domains would increase the likelihood that practitioners alerted to the possibility of personality pathology would pursue a more formal evaluation (Noblin, Venta, & Sharp, 2013; Patel, Sharp, & Fonagy, 2011).
It should be noted that the PID-5-BF does not aim to yield a measure of impairment in DSM-5 AMPD Criterion A core functions (i.e., self/interpersonal functions); rather it simply aims to screen for elevation in one or more of the maladaptive trait dimensions and to evaluate the overall profile elevation across the five maladaptive trait dimensions. Importantly, the presence of personality dysfunction as operationalized in Criterion A conveys information primarily regarding disorder severity, rather than personality “style,” which is reflected in traits (Morey et al., 2011; Pincus, 2011; Tyrer et al., 2011).
Recently, supporting earlier research (Ro & Clark, 2013), Zimmermann et al. (2015) showed that the empirical structure of the Criterion A subdomains is broadly in line with the theoretical model representing two highly correlated factors of self- and interpersonal functioning, and can be differentiated from Criterion B traits. Although there is some evidence that pathological personality traits may capture personality dysfunction (e.g., Few et al., 2013; Hill, Fudge, Harrington, Pickles, & Rutter, 2000), and Zimmermann et al.’s (2015) findings indicated that the distinction between Criteria A and B may not be as clear cut as the DSM-5 AMPD suggests, at the same time their results also do not indicate that Criterion A and B reference the same constructs. As such, the PID-5-BF total score is expected to be associated with measures of self and interpersonal dysfunction, but not to be entirely redundant with detailed assessments of functioning in these domains. In other words, the PID-5-BF total score should not be considered as a measure of DSM-5 AMPD Criterion A, but as an index reflecting the possible need for a thorough clinical assessment of severity of self and interpersonal impairments (as well as thorough assessment of the full DSM-5 maladaptive trait model) in selected individuals.
Although the PID-5-BF includes a total score intended to serve the two functions of screening for and summarizing overall profile elevation, its use might be taken to suggest the presence of an overall general personality pathology factor. The idea of such a factor is controversial, however, with some suggesting such factors reflect general psychopathology (e.g., Lahey et al., 2012), and others suggesting that they are source-specific artifacts or reflect response bias (e.g., Anusic, Schimmack, Pinkus, & Lockwood, 2009). Our purpose here is not to adopt a stance on these issues or to find support for the existence of a general personality pathology factor in a wider conceptual sense, but to evaluate the tenability and utility of the PID-5-BF total score from a psychometric perspective.
The Assessment of Maladaptive Personality Traits in Adolescence
The assessment of personality pathology in adolescence is important, since personality dysfunction is commonly misdiagnosed or missed completely in the adolescent population, in which clinically significant emotional dysregulation and externalizing behavior are sometimes missed because they are mistaken for developmentally appropriate behaviors (Sharp & Bleiberg, 2007). Although, a number of recently published reviews discuss developmental antecedents of personality pathology (for a review, see De Fruyt & De Clercq, 2014), and a recent study (De Clercq et al., 2014) showed that the PID-5 scales had generally acceptable-to-good internal consistencies in adolescence, more research is needed in evaluating maladaptive personality traits in adolescence.
Previous studies (e.g., Marsh, Nagengast, & Morin, 2013) examined the role of gender differences in Five Factor Model traits. For instance, Klimstra, Hale, Raaijmakers, Branje, and Meeus (2009) in a sample of Dutch adolescents, found that girls had consistently higher scores than boys for Neuroticism, Agreeableness, with tendencies toward higher scores for Openness and Extraversion. However, this appears to be the first study to examine the impact of gender on the PID-5-BF domain and total scores in adolescence.
The Present Study
The PID-5-BF is an easy to administer (and score), very short instrument specifically designed to screen for DSM-5 AMPD maladaptive personality trait dimensions which does not include any psychiatric symptom per se among its items. These features seem to indicate the PID-5-BF may be a viable tool for personality disorder screening among adolescents. Notwithstanding these promising features of the PID-5-BF as a screening instrument, to the authors’ knowledge no study has been carried out on the psychometric properties of the PID-5-BF up to now, particularly in adolescence. Moreover, no study addressed the issue of the reliability and validity of the PID-5-BF in different linguistic or cultural contexts. The availability of assessment instruments like the PID-5-BF, which have been validated in different countries as a reliable and valid measure of DSM-5 pathological traits, will help to address concerns that useful clinical information is not lost in the translation of PD diagnoses from a categorical framework to a dimensional framework.
Starting from these considerations, we aimed at providing initial data on the reliability and construct validity of the PID-5-BF. In order to obtain initial evidence of the ability of PID-5-BF scores to predict the level of personality dysfunction, participants were administered also the Measure of Disordered Personality Functioning (MDPF; Parker et al., 2004). In the absence of agreed-upon, easy-to-administer measures of DSM-5 AMPD Criterion A, the MDPF may be used as a “criterion A-like” measure of impairment in core personality functions (Ro & Clark, 2013). As noted earlier, some research suggests differentiation between dysfunction and traits (Zimmermann et al., 2015), and in the AMPD personality dysfunction is necessary for a PD diagnosis, as the simple presence of extreme traits does not necessarily indicate mental disorder (Livesley & Jang, 2005). Finally, in the present study, we examined the role of gender on the PID-5-BF domain and total scores.
Method
Participants
Participants were 1042 adolescents (52.9% female; mean age = 15.65 years, SD = 2.10) who were attending one public junior high school and six public high schools in Southern Italy, Central Italy, and Sardinia Island, Italy, respectively. Data were incomplete for 165 participants (15.8%) (questionnaires were considered incomplete if more than 10% of the items in any given scale were not answered) and these participants were excluded from the final sample. Participants with incomplete questionnaires did not differ from participants with complete questionnaires on gender, χ2(1) = 1.52, p > .20, φ = .04, region of Italy, χ2(2) = 0.22, p >.50, φ = .02, school that participants were attending, χ2(6) = 5.21, p > .10, Cramer’s V = .07; participants with incomplete questionnaires were significantly, albeit slightly younger (mean age = 15.18 years, SD = 2.16) than participants with complete questionnaires (mean age = 15.74 years, SD = 2.07), age, t(1040) = −3.19, p > .70, d = −0.20. The final sample was comprised of 877 adolescent students; 471 participants (53.7%) were female and 406 (46.3%) were male, with a mean age of 15.74 years (SD = 2.07). In order to participate in the present study, participants were required to speak Italian as their first language in order to avoid cultural and lexical bias in questionnaire responses.
After obtaining institutional review board approval from the university and the principals of the schools, researchers recruited adolescents from classrooms (data were collected in Autumn 2014–Spring 2015). Written informed parent consent and adolescent assent were obtained prior to study participation. Although socioeconomic status was not directly controlled for in this study, it should be emphasized that participants were selected from public high schools. Data from the National Institute of Statistics of Italy (ISTAT; retrieved from http://dati.istat.it/Index.aspx?DataSetCode=DCIS_SCUOLESECOND2) showed that 95.28% of the Italian students attended public high schools in 2013. In particular, ISTAT records (retrieved from http://www.istat.it/it/archivio/17290) showed that 93.1% of the Italian adolescents were high school students during 2012/2013 (the median percentage of the Italian who were high school students from 2007 to 2013 was 94.3%, with a mean value of 94.0%, SD = 0.79), thus suggesting that samples of adolescents attending public high schools may be representative of the Italian adolescent population.
The principals of the school in Southern Italy agreed to participate in the test–retest study of the PID-5-BF. Among the 306 community-dwelling adolescents who attended school in the South of Italy and were included in the final sample, 42 (13.7%) participants agreed to participate in the 2-month test–retest reliability study of the PID-5-BF scale scores. In the test–retest subsample, 31 participants (73.8%) were female and 11 (26.2%) were male, with a mean age of 15.00 years (SD = 1.06). A significantly lower proportion of female adolescents (n = 440, 52.7%) was observed among adolescents in the final sample who did not participate in the test–retest study (N = 835) than among adolescents in the test–retest subsample, χ2(1) = 7.17, p < .01, φ = .09, although the effect size for this difference (i.e., φ coefficient value) was small by conventional standards (Cohen, 1988). On average, adolescents in the test–retest subsample were significantly, albeit slightly (Cohen, 1988), younger than adolescents who did not participate in the test-retest study (mean age = 15.78 years, SD = 2.11), separate variance t(59) = −4.36, p <.001, d = -0.36. Test–retest participants did not show any significant difference from the participants who did not take part in the test–retest study on the PID-5-BF total score at the baseline, t(875) = −0.50, p > .60, d = −0.03, and on any of the baseline PID-5-BF scale scores—minimum t(875) = 0.10, d = 0.01 (Negative Affectivity); maximum t(875) = 0.80, d = 0.05 (Detachment)—except for the Antagonism scale score, t(875) = −2.18, p < .05, d = −0.18, although the effect size for this difference (i.e., d coefficient value) was small by conventional standards (Cohen, 1988).
Measures
Cronbach’s alpha values for the PID-5-BF scales in the whole sample and in the subgroups based on participants’ gender are listed in Table 1.
Descriptive Statistics, Cronbach’s α Values and Mean Interitem Correlations, and Gender Comparisons for the Personality Inventory for DSM-5 Brief Form (N = 877).
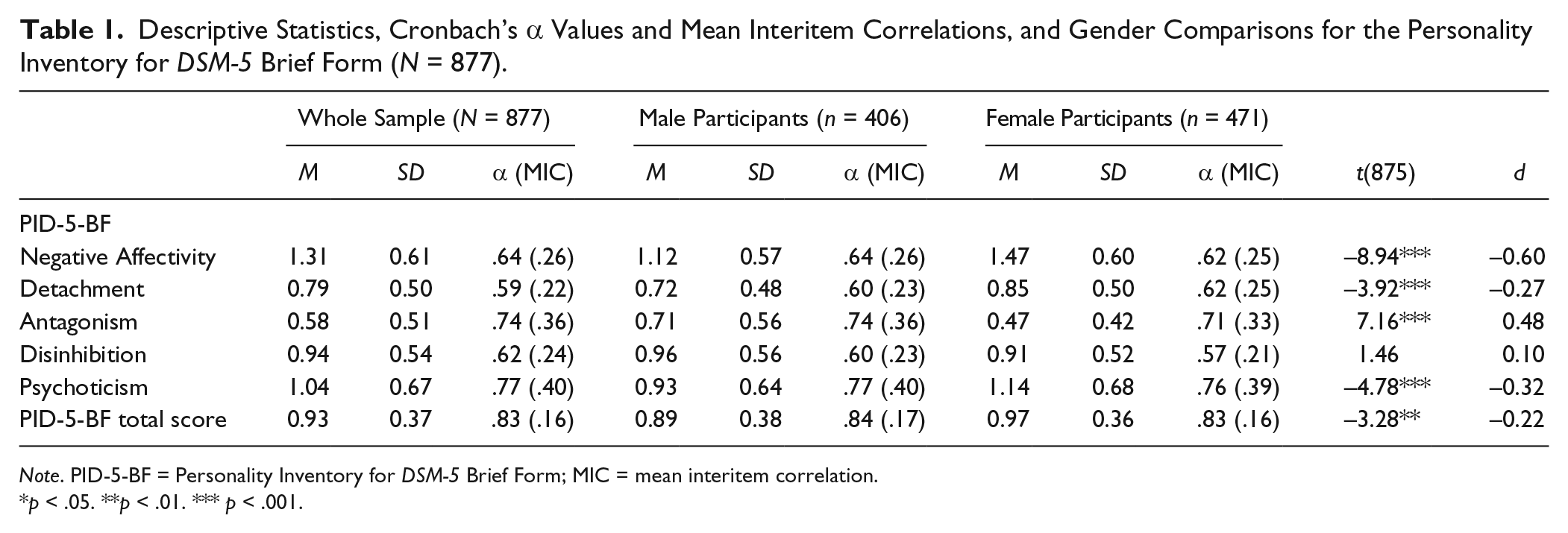
Note. PID-5-BF = Personality Inventory for DSM-5 Brief Form; MIC = mean interitem correlation.
p < .05. **p < .01. *** p < .001.
Personality Inventory for DSM-5 Brief Form
The PID-5-BF (American Psychiatric Association, 2013b) is a 25-item self-report questionnaire which was designed to assess the five AMPD trait dimensions of Negative Affectivity (NA), Detachment (De), Antagonism (An), Disinhibition (Di), and Psychoticism (Ps) in both adults and adolescents; each domain scale consisting of 5 items. Each PID-5-BF item is scored on only one PID-5-BF trait scale. The PID-5-BF items come from the 220-item self-report PID-5. As in the PID-5, each PID-5-BF item is rated on a 4-point scale (i.e., 0 = very false or often false; 1 = sometimes or somewhat false; 2 = sometimes or somewhat true; 3 = very true or often true). Different from other versions of the PID-5, the PID-5-BF yields a score for the overall measure (American Psychiatric Association, 2013b).
Measure of Disordered Personality Functioning
The Measure of Disordered Personality Functioning (MDPF; Parker et al., 2004) is a 20-item, Likert-type self-report questionnaire that has been explicitly designed to assess two broad dimensions of personality dysfunction, namely, Non-Coping and Non-Cooperativeness. The MDPF provides 10 items assessing the Non-Coping dimension, and 10 items assessing the Non-Cooperativeness dimension. Items are simply summed to yield each dimension total score; on each MDPF dimension, higher scores indicate higher levels of personality dysfunction. Each MDPF item is measured on a 4-point scale (i.e., 0 = definitely false; 1 = mostly false; 2 = mostly true; 3 = definitely true). Items are listed in the MDPF in random order; 13 MDPF items are scored in reversed order. The 20 items included in the MDPF came from an original pool of 141 items that were selected and reviewed by experienced clinicians to identify 17 constructs historically defining personality dysfunction (Parker et al., 2002). The final version of the MDPF was validated in both nonclinical samples and clinical samples (Parker et al., 2004) and is considered a reliable and valid self-report measure of personality dysfunction (Ro & Clark, 2013). Although the MDPF does not explicitly assess Criterion A of DSM-5 AMPD, it provides scores for two major dimensions of personality dysfunction, namely, Non-Coping and Non-Cooperativeness, which bear close resemblance to the DSM-5 Criterion A constructs of self-dysfunction and interpersonal dysfunction. Indeed, Criterion A from the DSM-5 AMPD defines the presence of a PD by the degree of disturbance in self- and interpersonal functioning; self-functioning involves identity and self-direction; interpersonal functioning involves empathy and intimacy (American Psychiatric Association, 2013a). For instance, some of the MDPF items might be considered akin to empathy (e.g. “I tend to be very understanding of other people’s feelings and problems”), whereas other MDPF items are more similar to self-direction construct (e.g. “I feel like I am going around in circles in life”). MDPF items may be easily administered to adolescent participants, with the possible exception of two Non-Cooperativeness items, “Even when I have to, I am unable to get along with family or people at work” and “People at work see me as cooperative and agreeable”. To increase the adequacy of these items for use of the MDPF with adolescents we rephrased them as follows: “Even when I have to, I am unable to get along with family or people at school” and “People at school see me as cooperative and agreeable.”
Consistent with previous studies on adult participants (e.g., Ro & Clark, 2013), in our adolescent sample the MDPF Non-Coping (M = 10.25, SD = 5.19, Cronbach’s α = .79, mean interitem correlation [MIC] = .28) and Non-Cooperativeness (M = 8.33, SD = 4.10, Cronbach’s α = .74, MIC = .22) scales showed adequate internal consistency reliability in the whole sample, as well in the male subgroup (Cronbach’s α = .78 for the MDPF Non-Coping scale, and Cronbach’s α = .74 for the MDPF Non-Cooperativeness scale) and in the female subgroup (Cronbach’s α = .79 for the MDPF Non-Coping scale, and Cronbach’s α = .72 for the MDPF Non-Cooperativeness scale). Marginally, according to Fisher’s z test, no significant difference in MIC values for MDPF Non-Coping scale (MIC female = .26, MIC male = .28, z = −0.32, p > .50) and Non-Cooperativeness scale (MIC female = .22, MIC male = .20, z = 0.31, p > .50) scores was observed between male participants and female participant. In the present study, female participants (M = 11.00, SD = 5.24) scored higher than male participants (M = 9.36, SD = 4.99) on the MDPF Non-Coping scale, t(875) = 4.57, p < .001, d = 0.31, whereas male participants (M = 9.19, SD = 4.16) scored higher than female participants (M = 7.60, SD = 3.80) on the MDPF Non-Cooperativeness scale, t(875) = 5.65, p <.001, d = 0.38. Finally, according to previous findings (Parker et al., 2004; Ro & Clark, 2009), in our adolescent sample, the MDPF Non-Coping and Non-Cooperativeness scales were moderately intercorrelated (r = .32, p < .001).
Measure Translation Process
Participants were administered the PID-5-BF and the MDPF in their Italian translation. The Italian translation of the PID-5-BF was derived from the Italian translation of the 220-item PID-5. The procedure of the translation PID-5 was detailed elsewhere (Fossati et al., 2013); equivalence with the original meaning of the items was the guiding principle in the translation process (Denissen, Geenen, van Aken, Gosling, & Potter, 2008). First, the PID-5 was independently translated into Italian by one of the authors (A.F.), and by two other clinical psychologists who were fluent in English. After reaching a consensus, we had an English mother-tongue professional translator translate the Italian version back into English, and this English back-translation (Cha, Kim, & Erlen, 2007; Geisinger, 1994; van De Vijver & Hambleton, 1996) was sent to the authors of the PID-5. If the latest version differed from the English original, the translators came to an agreement on the definitive Italian translation. A similar procedure was followed for translating the MDPF into Italian.
Procedures
Participants received the Italian translations of the instruments. The questionnaires were administered in random order and anonymously during class time in school by psychology students when teachers were not present in the classrooms. In order to be selected for the test–retest subsample, participants were assigned by their respective teachers an alphanumerical code based on their student identification number; teachers were blind to adolescent students’ questionnaire scores, and graduate psychology students who administered and scored the questionnaires were blind to participants’ identities.
Data Analyses
Cronbach’s alpha coefficient and mean interitem correlation (MIC) were used to assess the internal consistency of the scales; considering that the PID-5-BF items were measured on a four-point ordinal scale and showed a significant multivariate kurtosis, z = 37.67, p < .001, polychoric correlations coefficients were computed among the PID-5-BF items. PID-5-BF item analyses were carried out according to a multitrait paradigm (Nunnally & Bernstein, 1994), which involved the computation of two distinct item-total correlation coefficients for each PID-5-BF item. PID-5-BF item convergent validity was assessed through computation of item–total correlations corrected for item–total overlap (rit) between each item and the total score of the scale to which the item was assigned. PID-5-BF item discriminant validity was evaluated by correlating each PID-5-BF item with the total score for the remaining four scales to which the item was not assigned. Multitrait analysis determines the extent to which items correlate more strongly with their own domain than with other domains in the scale. Differences in excess of twice the typical error of the correlation coefficient—that is,
Intraclass r for absolute agreement based on random effects one-way analysis of variance (ANOVA) were used to evaluate the 2-month test–retest reliability of PID-5-BF scores.
In the present study, we relied on a two-stage approach to the assessment of the factor structure of the PID-5-BF. First, we performed a dimensionality analysis of the PID-5-BF item polychoric correlation matrix using differing criteria in order to determine the number of factors underlying the PID-5-BF item correlation matrix. Then, we performed exploratory structural equation model (ESEM) analysis. 1 Indeed, in recent literature, ESEM (Asparouhov & Muthén, 2009) has been suggested as a promising tool in personality research, blending elements of confirmatory factor analysis with those from exploratory factor analysis (Hopwood & Donnellan, 2010; Marsh, Morin, Parker, & Kaur, 2014). Rather than optimizing factor rotation to the characteristics of the sample at hand, we used the a priori binary (i.e., 1s and 0s) matrix of assignment of PID-5-BF items to scales for oblique target rotation. Indeed, the use of target rotation formalizes the view of ESEM as a primarily confirmatory approach, as it allows the analyst much more a priori control on the expected factor structure (Marsh et al., 2014). In line with previous studies of the PID-5 structure (e.g., De Clercq et al., 2014), we used an oblique rotation allowing the factors to be correlated. The replicability of the factor structure across subsamples based on participants’ gender was also assessed.
Differing criteria, consisting of Hull’s method (Lorenzo-Seva, Timmerman, & Kiers, 2011; Wilderjans, Ceulemans, & Meers, 2013) and parallel analysis (Buja & Eyuboglu, 1992) were used for determining the number of factors to be retained.
The logic behind Hull’s method is identifying a model that optimally balances model goodness of fit/misfit and model complexity (Wilderjans et al., 2013); recent Monte Carlo data have shown the Hull method to be superior to other methods in identifying the optimal number of factors (Lorenzo-Seva et al., 2011). In the present study, the Hull method was based on root mean square error of approximation (RMSEA). Parallel analysis contrasts each eigenvalue of the real-data correlation matrix with the corresponding average eigenvalue obtained from a large number (say, ≥1,000) random correlation matrices. Following Buja and Eyuboglu’s (1992) suggestions, parallel analysis was based on 1,000 independent polychoric correlation matrices that were obtained by random permutations of the original data. Monte Carlo studies showed parallel analysis to be one of two methods most efficient for recovering the correct number of factors (Zwick & Velicer, 1986).
Weighted least square means and variance adjusted (WLSMV) algorithm was used in ESEM analysis. Oblique target rotation was used to rotate the ESEM factors. In order to assess model fit, we calculated RMSEA, Tucker–Lewis index (TLI), and comparative fit index (CFI) in addition to goodness-of-fit chi-square test. Consistent with Hu and Bentler’s (1999) indications, we used the following cutoff values to evaluate the model fit: a TLI/CFI of .90 and higher, and an RMSEA of .08 and lower are indications of an adequate fit, while a TLI/CFI of .95 and higher and an RMSEA of .05 and lower are indications of a good fit (but see Marsh, Kit-Tai, & Zhonglin, 2004 for a comment on these commonly applied cut-off values for assessing model fit). To assess if a total score for the PID-5-BF items could be structurally tenable, we also assessed a WLSMV ESEM bifactor model with a general factor which all PID-5-BF items were expected to load on, and five specific orthogonal factors; bi-geomin orthogonal rotation was used to obtain interpretable factors in bifactor analyses.
In the present study, we used multiple-group WLSMV ESEM in order to test the replicability of the five-factor structure of the PID-5-BF items across subgroups based on participants’ gender. In particular, we tested the following invariance models: (a) a configural invariance model with invariant factor loading pattern and (b) a scalar invariance model with invariant factor loadings and thresholds. The DIFFTEST procedure was used to evaluate the presence of significant differences in goodness-of-fit function between nested models (Muthén & Muthén, 1998-2012). WLSMV ESEM analyses were carried out using MPlus 7.3 (Muthén & Muthén, 1998-2012).
Finally, multiple regression analyses were performed in order to evaluate multivariate models in which the PID-5-BF scores predicted the MDPF Non-Coping and Non-Cooperativeness scale scores, respectively. Bivariate correlations with Bonferroni-corrected (i.e., p < .005) between PID-5-BF domain scales and MDPF dimensions were used in order to select the initial set of predictors in multiple regression analyses; the remaining PID-5-BF scales were entered in Step 2 of the hierarchical regression model in order to evaluate their possible significant role as predictors in the multivariate space. Change in adjusted R2 value was used as effect size measure; the variance inflation factor (VIF) was computed in order to assess collinearity (Cohen, Cohen, West, & Aiken, 2003). In all analyses, the invariance of findings across subgroups based on gender was formally assessed. The Hayes and Matthes (2009) procedure was used to detect significant interactions between participants’ gender and each PID-5-BF scales in predicting MDPF scale scores, holding the other PID-5-BF scales constant; predictors and moderators were mean centered before multiplication (Hayes, Glynn, & Huge, 2011).
Results
PID-5-BF Scale Descriptive and Reliability Analysis Results
Descriptive statistics, Cronbach’s alpha and average MIC values, and gender comparisons for the PID-5-BF scales are listed in Table 1. According to Fisher’s z test, no significant difference in MIC values for PID-5-BF scale and total scores was observed between male participants and female participants, minimum z value = −0.24 (Detachment), maximum z value = 0.57 (Antagonism), all ps > .50.
Although our adolescents participants scored on average on the PID-5-BF scales in the 0.60 to 1.30 range, suggesting that all PID-5-BF domains were usually very/often false or sometimes/somewhat false for community-dwelling adolescents, repeated-measures multivariate analysis of variance (MANOVA) showed that in the whole sample the five PID-5-BF domains scales did not yield equal average scores, Pillai’s V = .52, p < .001; paired-sample t tests with Bonferroni-corrected nominal significance level showed that adolescent participants scored significantly higher on Negative Affectivity than on all the other PID-5-BF scales, whereas they scored significantly lower on Antagonism than on all the remaining PID-5-BF scales. In our adolescent sample, the average score on the PID-5-BF Psychoticism domain scale was significantly lower than the average score on the PID-5-BF Negative Affectivity domain scale, but it was significantly higher than the average scores on all the other PID-5-BF domain scales. This pattern was somewhat reproduced across male and female subgroups, although a significant gender-by-PID-5-BF scale interaction was observed in repeated-measures MANOVA, Pillai’s V = .18, p < .001.
With the partial exception of PID-5-BF Psychoticism domain scale, r = −.09, p < .05, participants’ age correlated trivially and nonsignificantly with all PID-5-BF scale score, with r values ranging from −.04 (Disinhibition) to .06 (Negative Affectivity), all ps > .05.
On average, the five PID-5-BF scale scores were moderately intercorrelated, median r value = .28, SD = .10, minimum r value (Antagonism and Negative Affectivity) = .13, maximum r value (Negative Affectivity and Psychoticism) = .44, all ps < .001; correlation corrected for part–whole overlap between PID-5-BF domain scale scores and PID-5-BF total score were .42 for Negative Affectivity, .43 for Detachment, .31 for Antagonism, .37 for Disinhibition, and .55 for Psychoticism. This pattern of correlations among the PID-5-BF domain scales was consistently replicated across male subgroup, median r value = .31, SD = .09, minimum r value = .15, maximum r value = .44, all ps < .001, and female subgroup, median r value = .28, SD = .08, minimum r value = .19, maximum r value = .40, all ps < .001.
Two-month test–retest reliability of the PID-5-BF scale and total scores was assessed in a subsample of 42 adolescents. In the test–retest subsample, the PID-5-BF Negative Affectivity domain score at the baseline did not differ significantly from PID-5-BF Negative Affectivity domain score at retest, t(876) = −0.08, p > .10, d = −0.00; rather, the intraclass correlation coefficient for absolute agreement based on random effect one-way ANOVA (ρ1,1) was highly significant, ρ1,1 = .78, p < .001. Similar results were observed when we compared the PID-5-BF Detachment domain score at the baseline and the PID-5-BF Detachment domain score at retest, t(876) = −1.31, p > .10, d = −0.04, ρ1,1 = .92, p < .001. Similarly, neither the PID-5-BF Antagonism domain score at the baseline differ significantly from PID-5-BF Antagonism domain score at retest, t(876) = 0.00, p > .10, d = 0.00, ρ1,1 = .97, p < .001, nor the PID-5-BF Disinhibition domain score at the baseline differ significantly from PID-5-BF Disinhibition domain score at retest, t(876) = −1.23, p > .10, d = −0.04, ρ1,1 = .96, p < .001. When we considered the PID-5-BF Psychoticism domain score at the baseline, it did not differ significantly from PID-5-BF Psychoticism domain score at retest, t(876) = −0.26, p > .10, d = −0.01, ρ1,1 = .92, p < .001. Finally, among the 42 adolescents who agreed to participate in the 2-month test–retest study, no significant difference was observed between the mean PID-5-BF total score at the baseline, and the mean PID-5-BF total scores at follow-up, t(876) = −1.05, p > .10, d = −0.04, ρ1,1 = .95, p < .001.
PID-5-BF item analysis results are summarized in Table 2. Considering that a large number of correlation coefficients (n = 125) were computed, the nominal significance level (i.e., p <.05) was corrected according to the Bonferroni procedure and set at p < .0004; r coefficients equal to or greater than .12 were significant at p < .0004. In this study, PID-5-BF item convergent validity was assessed through rit coefficients. PID-5-BF item discriminant validity was evaluated by correlating each PID-5-BF item with the total score for the remaining four scales to which the item was not assigned. Differences between convergent validity coefficients and discriminant validity coefficients in excess of twice the typical error of the correlation coefficient indicate the strength of the association (e.g., Virtues-Ortega et al., 2010); in the present study the critical value for a relevant difference was .07. For instance, the item-total correlation for item 8 is .40, therefore any discriminant validity coefficients greater than .33 would reflect poor discriminant validity.
Personality Inventory for DSM-5 Brief Form (PID-5-BF) Item Analyses: Descriptive Statistics, Item–Total Correlations Corrected for Item–Total Overlap, and Correlations Between Each PID-5-BF Item With the Total Score for the Scales to Which It Was not Assigned (N = 877).
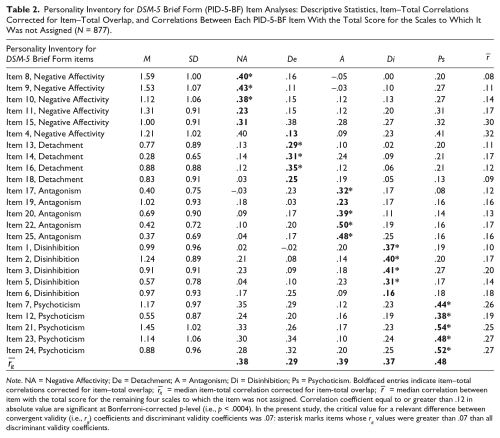
Note. NA = Negative Affectivity; De = Detachment; A = Antagonism; Di = Disinhibition; Ps = Psychoticism. Boldfaced entries indicate item–total correlations corrected for item–total overlap;
As it can be seen in Table 2, rit coefficients for the PID-5-BF scales were significant and usually of moderate size, with the exception of small rit values that were observed for PID-5-BF Item 4 (“I often feel like nothing I do really matters,” Detachment) and Item 6 (“I’m not good at planning ahead,” Disinhibition). Only 25 discriminant validity coefficients did not reach statistical significance (i.e., they were smaller than .12 in absolute value). A total of 19 (76.0%) PID-5-BF items showed discriminant validity with the other four scales. By contrast, Item 4, Item 6, Item 11 (“I get stuck on one way of doing things, even when it’s clear it won’t work,” Negative Affectivity), and Item 15 (“I get irritated easily by all sorts of things,” Negative Affectivity) showed rit values that were markedly (i.e., at least .07) lower than one or more discriminant validity coefficients.
On average, PID-5-BF items showed moderate and significant item-total correlations corrected for item–total overlap with the PID-5-BF total score, median rit = .31, SD = .10, minimum rit value (Item 18) = .18, maximum rit value (Item 24) = .49, all ps < .001; rit values equal to or greater than .30 were observed for 14 (56.0%) PID-5-BF items.
PID-5-BF ESEM Analysis Results
Dimensionality analyses consistently suggested that polychoric correlations that were observed among the PID-5-BF items might be explained by five factors. The Hull method based on minimizing RMSEA value (i.e., the ratio of the goodness-of-fit measure to the number of estimated parameters) peaked at 1.20 for a three-factor model, 1.28 for a four-factor model, 1.89 for a five-factor model, and 0.00 for a six-factor model; according to the Hull method, a five-factor model of the PID-5-BF items would provide the best balance between goodness-of-fit and model complexity. When the first five factors were extracted from the polychoric correlation matrix of the PID-5-BF items using ULS EFA, the corresponding RMSEA value was .069. Parallel analysis yielded similar findings. The first six eigenvalues of the PID-5-BF items were 5.18, 2.64, 2.01, 1.41, 1.25, and 1.17, respectively; the first six average eigenvalues that were computed from 1,000 random polychoric correlation matrices that were obtained by random permutations of the original data were 1.41, 1.35, 1.30, 1.26, 1.22, and 1.19, respectively. According to parallel analysis results, only the first five eigenvalues of the PID-5-BF item polychoric correlation matrix exceeded the expected values of the corresponding random eigenvalues. Parallel analysis results also supported the hypothesis that five factors may adequately explain the polychoric correlations that were observed among the PID-5-BF items.
When we extracted the first five principal components from the PID-5-BF polychoric correlation matrix, with the partial exception of Item 18 (standardized loading = .28) and Item 8 (standardized loading = .27), all other PID-5-BF item showed substantial (i.e., >.30) loadings on the first unrotated principal component, median standardized loading value = .43, SD = .10, minimum standardized loading value = .31 (Item 13), maximum standardized loading value = .63 (Item 24). This finding was consistent with the presence of latent dimension common to all PID-5-BF items along with group factors (Nunnally & Bernstein, 1994).
WLSMV ESEM results suggested adequate fit for a five-factor model of PID-5-BF items, WLSMV χ2(185) = 419.13, p < .001, RMSEA = .041, 95% confidence interval for RMSEA = [0.036, 0.046], TLI = .92, CFI = .95. Most PID-5-BF items showed a substantial degree of factor complexity, showing significant factor loadings on two or more WLSMV ESEM factors.
As it can be observed in Table 3, with the exception of PID-5-BF item 11, all PID-5-BF items showed significant, positive factor loadings on the factors which were assigned to according to the PID-5-BF a priori model of item assignment to scales. However, several PID-5-BF items did not show their largest positive loading on their corresponding expected factors; for instance, PID-5-BF Item 4, which was expected to index the Detachment domain showed its largest positive loading on the Negative Affectivity factor. Similarly, PID-5-BF Item 5 (Disinhibition), Item 6 (Disinhibition), Item 11 (Negative Affectivity), Item 15 (Negative Affectivity), Item 19 (Antagonism), and even Item 22 (Antagonism) did not show their largest positive loading on their corresponding expected factors. All factor correlations were in the small-to-moderate range, indicating that the WLSMV ESEM factors represented non-isomorphic (e.g., separate) latent dimensions underlying the observed polychoric correlations of the PID-5-BF items.
Personality Inventory for DSM-5 Brief Form: Exploratory Structural Equation Model Standardized Factor Loadings and Factor Correlations (N = 877).
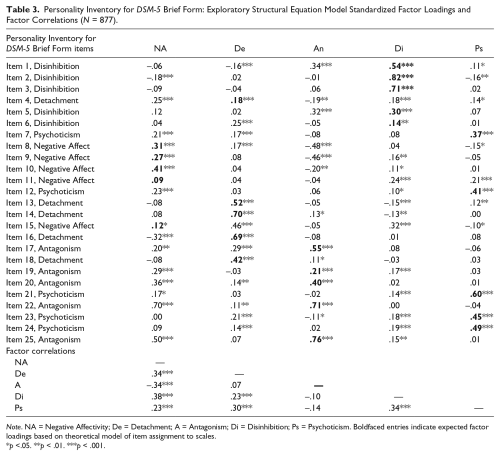
Note. NA = Negative Affectivity; De = Detachment; A = Antagonism; Di = Disinhibition; Ps = Psychoticism. Boldfaced entries indicate expected factor loadings based on theoretical model of item assignment to scales.
p <.05. **p < .01. ***p < .001.
To test the factor structure invariance of PID-5-BF items across subgroups based on participants’ gender, we performed multi-group WLSMV ESEM analyses. First, we fitted a model in which the pattern of factor loadings was constrained to be invariant across groups (i.e., “configural” invariance model). This model showed adequate values of fit indices, WLSMV χ2(370) = 616.88, p < .001, TLI = .916, CFI = .948, RMSEA = .039, test of close fit for RMSEA (i.e., RMSEA ≤. 05) p > .90, supporting the hypothesis of “configural” invariance. Then, we tested a “scalar” invariance model to test the hypothesis of “strong factorial invariance,” that is, a model with invariant factor loadings and thresholds across subgroups based on participant’s gender. We observed adequate values of fit statistics even for the most restrictive model, WLSMV χ2(55) = 790.15, p < .001, TLI = .933, CFI = .942, RMSEA = .035, test of close fit for RMSEA (i.e., RMSEA ≤ .05) p > .90, even though constraining thresholds across groups significantly worsened the fit of the invariant model, DIFFTEST χ2(145) = 233.81, p < .001. Then, we could accept the hypothesis of “configural” invariance of the PID-5-BF factor structure across groups based on participants’ gender.
WLSMV ESEM bifactor analysis results suggested adequate fit for a model assuming a general factor and five specific factors (as suggested by the current published scoring guidelines) underlying the polychoric correlation matrix of the PID-5-BF items, WLSMV χ2(165) = 350.15, p < .001, RMSEA = .036, 95% confidence interval for RMSEA = [0.031, 0.041], TLI = .94, CFI = .97; with the possible exception of item 18 (standardized factor loading = .17), all PID-5-BF items showed positive, moderate loadings on the PID-5-BF general factor, median factor loading value = .40, SD = .12.
Relationships Between the PID-5-BF Domain and Total Scores and the MDPF
The PID-5-BF total score correlated significantly with both MDPF Non-Coping, r = .53, p < .001, and Non-Cooperativeness scale scores, r = .26, p < .001. All PID-5-BF domain scales showed significant, positive correlations with MDPF Non-Coping scales, with r values ranging from .11 (An) to .45 (NA), median r = .37, SD = .14, all ps < .005. With the exception of PID-5-BF NA scale, r = −.03, p > .30, all the remaining PID-5-BF showed significant bivariate correlations with MDPF Non-Cooperativeness scale, as it was indicated by r coefficient values ranging from .13 (Ps) to .32 (An), median r = .24, SD = .08, all ps <.001.
Multiple regression analysis results in the whole sample and broken down by participants’ gender are summarized in Table 4. The hypothesis of slope parallelism (i.e., equality of regression coefficients) in subgroups based on participants’ gender was tested using moderated regression analysis. Although PID-5-BF NA scale did not show a significant bivariate correlation with MDPF Non-Cooperativeness scale, in multiple regression analyses it added a significant contribution in predicting MDPF Non-Cooperativeness scores when it was entered in Step 2 of a hierarchical multiple regression model. VIF values did not suggest any collinearity problem for the PID-5-BF scales. As a whole, the PID-5-BF scales and total scores predicted a significant and nonnegligible amount of variance in the MDPF scales, particularly in the Non-Coping scale. As it can be observed in Table 4, moderated regression analyses showed that the majority of regression coefficients linking each PID-5-BF scale to each MDPF dependent variables did not significantly differ in male participants and in female participants. Indeed, significant interaction effects (i.e., significant differences in β coefficient values) were observed only for PID-5-BF Antagonism scale as predictor of MDPF Non-Cooperativeness scale, gender-by-Antagonism scale interaction b coefficient = 1.09, SE = 0.54, p < .05, and for the PID-5-BF total score as predictor of the MDPF Non-Coping scale, gender-by-PID-5-BF total score interaction b coefficient = 2.46, SE = 0.84, p < .01.
Personality Inventory for DSM-5 Brief Form Scales and Total Scores as Predictors of Measure of Disordered Personality Functioning Scales: Multiple Regression Analysis Results in the Whole Sample and Broken Down by Participants’ Gender (N = 877).
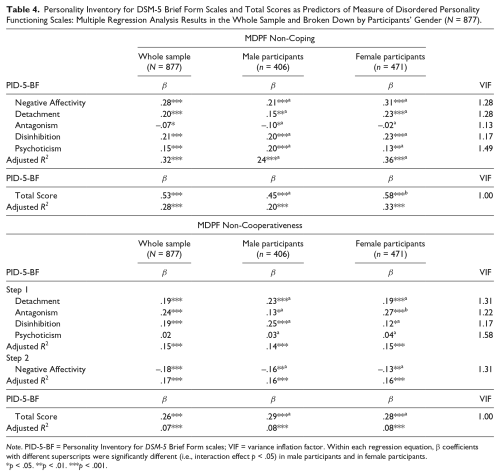
Note. PID-5-BF = Personality Inventory for DSM-5 Brief Form scales; VIF = variance inflation factor. Within each regression equation, β coefficients with different superscripts were significantly different (i.e., interaction effect p < .05) in male participants and in female participants.
p < .05. **p < .01. ***p < .001.
Discussion
To our knowledge, this study represents the first attempt at providing data on the psychometric properties of the PID-5-BF, particularly in a sample of community-dwelling adolescents. Our findings extended the results of previous studies on the applicability of the PID-5 in adolescence (De Clercq et al., 2014), supporting the hypothesis that also the PID-5-BF may represent a reliable measure of the DSM-5 AMPD maladaptive domains. Confirming and extending previous studies on the crosscultural applicability of the PID-5 (e.g., Bastiaens et al., 2015) our results suggested that the 25-item version of the PID-5 (i.e., the PID-5-BF) could prove useful in capturing personality pathology, at least in its Italian translation.
Our study yielded mixed results concerning the reliability of the PID-5-BF scales and total score. On one hand, MIC values were adequate according to conventional standards (Clark & Watson, 1995) for all PID-5-BF scales, as well as for PID-5-BF total score. On the other hand, Cronbach’s alpha values were at best modest for PID-5-BF Detachment, Negative Affectivity, and Disinhibition scales; Cronbach’s alpha values greater than .70 were observed only for PID-5-BF Antagonism and Psychoticism scales, and for the PID-5-BF total score. However, it should be observed that Cronbach’s alpha is an ambiguous indicator of internal consistency because it is a function of the number of test items and the MIC (Clark & Watson, 1995; Cortina, 1993; Cronbach, 1951). Whereas the degree of interitem correlation is a direct indicator of internal consistency, the number of items is not relevant (Clark & Watson, 1995). Accordingly, in our study we observed adequate internal consistency for all PID-5-BF scales, at least as it is measured by the MIC, which is considered a straightforward measure of internal consistency (Clark & Watson, 1995).
Despite the evidence of a significant effect of participants’ gender on the PID-5-BF scale scores in our sample, fairly similar Cronbach’s alpha values were observed in male participants and in female participants; this finding suggests that the PID-5-BF scales may require different norms for male adolescents and female adolescents while maintaining the same internal consistency properties, at least in a sample of Italian community-dwelling adolescents. Moreover, the significant gender differences in PID-5-BF domain average scores for Negative affectivity, Detachment, Antagonism, and Psychoticism may be particularly important for the early identification and prevention of PDs in adolescence. Indeed, identifying specific gender differences in maladaptive personality domains may be particularly important in order to prevent the clinical and social burden that are frequently associated with personality disorders diagnosis in adults (e.g., Michonski, Sharp, Steinberg, & Zanarini, 2013). For instance, adolescent girls appear to be at particularly high risk for Borderline Personality Disorder features and their detrimental consequences, and negative emotionality (i.e., high Negative Affectivity) and poor impulse control (i.e., high Disinhibition) are widely recognized in virtually all etiological theories as early markers or precursors of Borderline Personality Disorder (see, e.g., Stepp et al., 2014).
At first glance, our findings seem to suggest that PID-5-BF scale may be too short (they list only five items) to yield adequate Cronbach’s alpha coefficient values, with the possible exception of Antagonism and Psychoticism scales. However, the results of PID-5-BF item analyses in our sample seem to suggest a different possible scenario. With the exception of PID-5-BF Psychoticism scale, all other scales showed one (i.e., 20.0%) or two (i.e., 40.0%) of the items with poor convergent (i.e., item–total correlation corrected for item–total overlap) and/or discriminant validity. The problem was particularly significant for PID-5-BF Item 4 (“I often feel like nothing I do really matters,” Detachment) and Item 6 (“I’m not good at planning ahead,” Disinhibition). This finding suggests that the internal consistency of the PID-5-BF scales could be improved by selecting the five best performing PID-5 items for each domain using item response theory, without necessarily increasing scale length. It should be observed that this strategy has been recently used by Maples and colleagues (2015) in developing a 100-item version of the PID-5 which yields scores both for DSM-5 AMPD traits and DSM-5 AMPD domains. Moreover, a high MIC/alpha for the PID-5-BF scales might be undesirable because it could indicate an overrepresentation of one particular PID-5 trait of a domain rather than a representative sampling consistent with the goal of content validity.
In our study, we were able to evaluate the two-month test-retest reliability of the PID-5-BF scores only in a small subsample of adolescents who volunteered to participate in the longitudinal part of the study; moreover, this subsample was too small to allow for testing gender effects on test–retest reliability coefficients. Even keeping these limitations in mind, we would like to stress that intraclass r coefficient values suggested adequate consistency over 2 months of the scores for all PID-5-BF scales, as well as for the PID-5-BF total score. As a whole, our data suggest that the PID-5-BF total score is provided with adequate internal consistency reliability and 2-month test–retest reliability as a measure of overall personality pathology. Despite mixed findings concerning Cronbach’s alpha values, MIC values and 2-month test–retest reliability results that were observed in our study suggest that PID-5-BF scales may yield reliable scores purportedly measuring the corresponding DSM-5 domains.
In our study, we observed moderate factor intercorrelations (median r = .24) among the PID-5-BF scales. Our findings seem to suggest that the 25-item version of the PID-5 (i.e., the PID-5-BF) scale scores assess distinguishable constructs (i.e., Negative Affectivity, Detachment, Antagonism, Disinhibition, Psychoticism). Although moderate factor intercorrelation values that were observed in our study hint at adequate discriminant validity of the PID-5-BF trait scales, it should be observed that they were somewhat smaller than previously reported correlations among domains based on 220-item version and 100-item version of the PID-5 (e.g., Maples et al., 2015). We feel that these differences may stem from a number of factors, such as sampling differences, participants’ age, number of PID-5 items per factor, and method of factor rotation. Future research may clarify which of these potential explanations is most plausible.
Overall, our ESEM findings seem to support the factor structure validity of the PID-5-BF, at least in our adolescent sample, and seem to further stress the potential usefulness of refining the PID-5-BF selecting the five best performing PID-5 items for each domain through IRT. Indeed, this approach may allow for a more in-depth examination of the properties of PID-5-BF items and their relations with latent traits.
ESEM solutions are also valuable in the study of personality (Booth & Hughes, 2014) because they allow advanced analyses, such as investigating measurement invariance (Marsh et al., 2010; Marsh et al., 2014). When we tested multiple groups, the WLSMV ESEM factor structure of the PID-5-BF items that was observed in our male subsample could not be considered exactly equal (within sampling error) to the PID-5-BF items factor structure that was observed in our female subsample in terms of absolute fit. However, our findings seemed to indicate that the PID-5-BF item factor structure that was observed in our male adolescent subgroup closely matched the PID-5-BF factor structure that was observed in our female adolescent subgroup, although the differences between corresponding sets of factor loadings may not be exactly zero in the population. Finally, the PID-5-BF includes a total score intended to summarize the overall profile elevation (American Psychiatric Association, 2013b). Consistent with item analysis finding and principal component analysis results, ESEM bi-factor analysis data seemed to yield structural support to the use of a general score for the PID-5-BF items, at least in a sample of Italian community-dwelling adolescents.
External validity data for the PID-5-BF were somewhat limited, but in our opinion still interesting. Indeed, in our study we relied on the MDPF as a measure of level of personality dysfunction (Ro & Clark, 2009). The MDPF is a personality functioning measure that was developed for use in the context of personality disorder and personality traits (Ro & Clark, 2009); limitations in coping and cooperativeness formed the higher order constructs defining personality dysfunction (Parker et al., 2004).
Although the term personality functioning is not isomorphic with personality traits, measures of personality functioning (e.g., the MDPF), and measures of personality traits have common elements (Clark & Ro, 2014; Ro & Clark, 2009). Consistent with our hypotheses, regression analysis showed that the overall elevation of PID-5-BF profile (i.e. the PID-5-BF total score) was a positive, significant, and moderately strong predictor of the two MDPF scale scores, at least in our adolescent sample. In particular, the PID-5-BF total score predicted a moderate and non-trivial amount of variance in the MDPF Non-Coping scale score, and a less albeit significant amount of variance in the Non-Cooperativeness scale.
Confirming and extending Zimmermann et al.’s (2015) findings, our data suggested that self-dysfunction, as it was operationalized in the MDPF Non-Coping scale, was most consistently associated with self-report measures of maladaptive personality traits (i.e., PID-5-BF trait scores), at least in a group of Italian community-dwelling adolescents. Indeed, the PID-5-BF trait scales predicted a moderate amount of variance in the MDPF Non-Coping scale score, a measure which bear close resemblance to the DSM-5 Criterion A constructs of self-dysfunction. Specifically, in our study frequent and intense experiences of high levels of negative emotions (i.e. Negative Affectivity), an orientation toward immediate gratification without regard for past learning (or consideration of future consequences; i.e. Disinhibition), avoidance of socioemotional experience, and a tendency toward exhibiting culturally incongruent or unusual behaviors and cognition (i.e. Psychoticism) were the main predictor of MDPF Non-Coping scale, in both male and female adolescents.
In agreement with our hypotheses, behaviors that put the individual in disagreement with other people (i.e. high Antagonism) and orientation toward immediate gratification (i.e. high Disinhibition) significantly predicted the MDPF Non-Cooperativess scale score, a measure which was selected because of its close resemblance to the DSM-5 Criterion A construct of interpersonal dysfunction. Moreover, high Detachment scale scores (i.e., avoidance of socioemotional experience), and low Negative Affectivity (i.e., frequent and intense experiences of high levels of negative emotions) scale score, significantly predicted a failure to cooperate, at least as it is measured by the MDPF Non-Cooperativess scale (Parker et al., 2004).
Although additional studies would be needed before accepting our findings, our results seem to suggest that the PID-5-BF scales assess maladaptive personality trait dimensions that are related to the subjects’ level of personality dysfunction, at least as measured by the MDPF scales. Our findings appear to empirically support the hypothesis that DSM-5 AMPD Criterion A constructs of self-dysfunction and interpersonal dysfunction, at least as they are measured by the MDPF scales, and DSM-5 AMPD Criterion B maladaptive personality traits, at least as measured by the PID-5-BF, are not isomorphic, and seemed to stress the importance of considering both DSM-5 AMPD Criterion A and Criterion B in the assessment of personality pathology. Thus, although the PID-5-BF represents a short measure of the broad DSM-5 AMPD maladaptive personality trait dimensions, our data suggest that it may represent a useful tool for screening for personality pathology among community-dwelling adolescents, particularly when used in conjunction with a “DSM-5 Criterion A–like” measure of level of personality dysfunction such as the MDPF.
In summary, our findings suggest that the PID-5-BF has several advantages since it proved to be an easy-to-administer screening instrument for pathological personality domains. Moreover, the PID-5-BF total score might represent a tenable variable; indeed, its reliability coefficient value was adequate, at least in our adolescent sample and it was consistently associated with self-reports of levels of impairments in self function and interpersonal function, at least as they were operationalized in MDPF Non-Coping and Non-Cooperativeness scales, respectively. For clinical decision-making it should be emphasized that scores on the PID-5-BF total score may be easily converted to dichotomous evaluations (e.g., “possible maladaptive domain functioning” vs. “no maladaptive domain functioning”), and it may help in understanding why the overall score is elevated, at a greater level of detail.
Despite positive findings, there are several limitations that should be acknowledged. Although the current study included a moderately large number of participants (N = 877), it was based on community-dwelling adolescents; our sample represented a convenient study group rather than a sample representative of the Italian population. Moreover, all participants in our study were community-dwelling adolescents; thus, our findings should not be extended to adolescents from clinical or forensic setting. In our study, participants were adolescent volunteers who received no incentive for taking part in the research; extant research indicates that differences exist in the motivation between paid and nonpaid research participants (Gerstein, Wilkeson, & Anderson, 2004). However, research data offer conflicting findings as to using incentives for participants (particularly economic incentives) lead to improved commitment or to biased findings (e.g., Grady, 2005). Interestingly, Russell, Moralejo, and Burgess (2000) reported that most unpaid volunteers disagreed with paying research participants; the themes arising from their comments are similar to those that have been raised by ethicists and suggest that recognizing the time and effort of participants should receive greater emphasis than presently occurs.
We used a single measure for each construct, which limits the generalizability of our results to other measures. We administered only the MDPF scale as a measure of impairment included in Criterion A; although the MDPF was used to assess personality functioning in previous studies (e.g. Clark & Ro, 2014), our findings should not be extended to other Criterion A measures, particularly to the Level of Personality Functioning Scale (Bender, Morey, & Skodol, 2011). In our regression analyses we relied on self-report measures to assess both predictive variables (i.e., the PID-5-BF domain scales and total score) and criterion variables (i.e., MDPF scales). Indeed, this may have led to a spurious increase of the associations between the PID-5-BF trait and total scores and the external measure because of shared method variance.
As a whole, these limitations stress the need for further replications and extensions before accepting our results. Even keeping the limitations of our study in mind, we feel that our findings may prove useful in providing the first evidence of the reliability of the PID-5-BF as a brief screen for personality pathology in community-dwelling adolescents, at least in its Italian translation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.