
Abstract
Protective and intrusive parenting behaviors consistently relate to children’s anxiety development. We present two studies describing the development of the Attitudes about Parenting Strategies for Anxiety (APSA) scale, which assesses parent distress about children’s displays of anxiety and shyness as well as parent attitudes about the effectiveness of protective and intrusive responses across several domains. Study 1 included 594 parents who completed the APSA and additional measures online and established the factor structure, internal reliability, and validity of the measure. We also performed a latent profile analysis of the attitude items to understand common patterns and their correlates. Study 2 comprised 108 mothers participating in a laboratory-based study and provided additional evidence for the factor structure, reliability, and validity, as well as 1-year stability. The APSA appears to be a reliable and valid measure that could have utility for understanding the determinants of parenting behaviors relevant to child anxiety development.
Of the multiple factors influencing the development and maintenance of child anxiety and related constructs (e.g., shyness, fearful/inhibited temperament), parental behaviors, especially controlling behaviors (e.g., overprotection, intrusiveness), have been found to be among its strongest predictors (Laurin, Joussemet, Tremblay, & Boivin, 2015). Multiple studies have found that mothers and fathers of anxious children are more likely to express protective or intrusive behaviors than parents of nonanxious children (Greco & Morris, 2002; Hudson & Rapee, 2001; Wood, 2006). These behaviors are also related to dimensional assessments of shyness and fearful temperament, developmental precursors of anxiety (Rapee & Coplan, 2010). It is not known whether meaningful individual differences exist in how effective parents view such behaviors to be for helping children cope in anxiety-producing situations, for children’s future coping, and for parents’ own coping in these situations. Parents’ attitudes about their own protective and intrusive behaviors are important because they may explain why parents engage in such behaviors (see Figure 1), despite previously demonstrated negative outcomes (Rapee & Coplan, 2010). Previous measures assess parental attitudes about children’s anxiety spectrum behaviors or other aspects of parenting, but no measure captures parents’ attitudes about their own protective or intrusive behaviors. In the current study, we developed and validated a new measure of parents’ attitudes about protective and intrusive behaviors with their children.
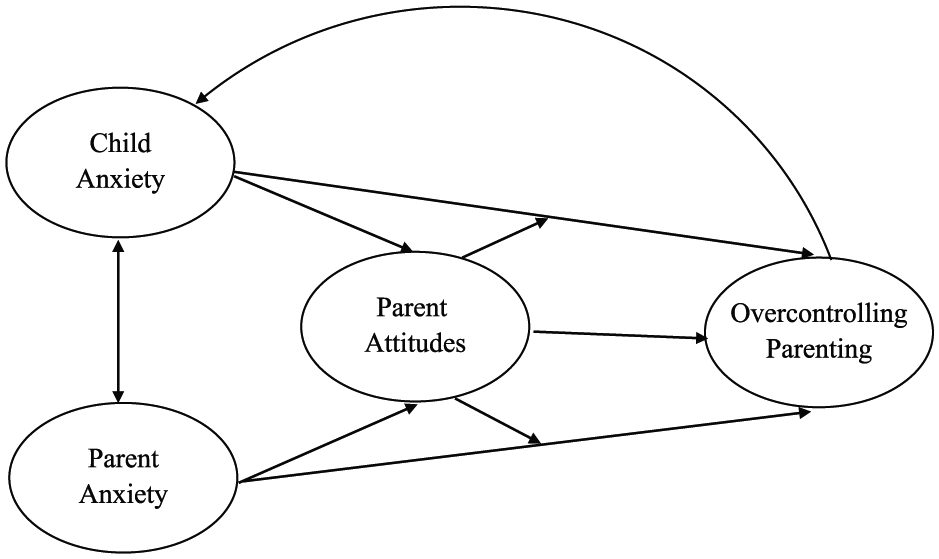
A conceptual model of relations among child anxiety, parent anxiety, and parent behavior, as well as how parent attitudes may assist in understanding these relations. Relations with parent attitudes require further investigation.
Parental Overcontrol and Child Anxiety
Protective and intrusive behaviors are considered types of parental control. Protective behaviors include removing or sheltering children from stressful situations, unnecessary or excessive comforting, and discouraging independence (Chorpita & Barlow, 1998; Kiel & Buss, 2010; Rubin, Burgess, & Hastings, 2002). Intrusive behaviors, on the other hand, include urging the child to interact with something feared, or overinvolvement in a challenging task for the child (Chorpita & Barlow, 1998; Kiel & Buss, 2010). Related to intrusive behavior is criticism of children’s withdrawal behavior, which may be a form of psychological control that limits children’s independent pursuit of goals (Barber & Harmon, 2002; McShane & Hastings, 2009).
Parental controlling behaviors are related to the development of child anxiety (Laurin et al., 2015; Wood, McLeod, Sigman, Hwang, & Chu, 2003). Although differing in the method, both types of control are characterized by a pattern of unnecessary or unwarranted regulation of a child’s activities. It should be noted that these behaviors represent more extreme versions of behaviors that, in lesser forms, may benefit anxiety-prone children. Being sensitive and responsive to child distress in moderation is linked to positive child outcomes, but too much responsiveness and comforting may be overprotective (Mount, Crockenberg, Bárrig Jó, & Wagar, 2010). Moderate encouragement of independence may decrease children’s anxiety, but forceful coercion to interact with novelty predicts increased anxiety (Kiel, Premo, & Buss, 2016). Theory and empirical evidence suggest that these behaviors interfere with a child’s ability to cope and develop mastery over stressful situations by taking away the child’s control over them (Chorpita & Barlow, 1998). This, in turn, encourages the child’s dependence on parents (Wood et al., 2003), reinforces that uncertain situations are threatening, and engenders the perception that stressful or anxiety-producing situations are out of their control (Chorpita & Barlow, 1998). Dependence, overinterpretation of threat, and feelings of lack of control are subsequently related to fear, shyness, and anxiety (Chorpita & Barlow, 1998; Fox, Henderson, Marshall, Nichols, & Ghera, 2005; McClure & Pine, 2006). Given the significance of these behaviors for the development of child anxiety spectrum outcomes, researchers have aimed to understand the factors that influence their engagement, finding evidence for parent anxiety, and children’s inhibited temperament, shyness, and anxiety (Figure 1; Chen et al., 1998; Clarke, Cooper, & Creswell, 2013; Cooklin, Giallo, D’Esposito, Crawford, & Nicholson, 2013; Kiel & Buss, 2010; Whaley, Pinto, & Sigman, 1999). Studies have also focused on parenting attitudes.
Parenting Attitudes
Parenting attitudes constitute parents’ affectively laden evaluations of their children’s behavior and development, including goals and attributions for, and emotional reactions to, children’s behavior (Mills & Rubin, 1993; Rubin & Mills, 1992). Although these have been referred to as “parenting beliefs,” their evaluative and affective nature, as well as their tendency to predispose parents toward behavior, are consistent with the definition of attitudes (Fishbein & Ajzen, 1975) and so will presently be referred to as such. Parenting attitudes can also include the evaluations parents have about their own parenting. Parenting attitudes are situation or context dependent (Coplan, Hastings, Lagacé-Séguin, & Moulton, 2002). In other words, different child-rearing situations, as well as different child behaviors, may elicit different parental attitudes.
Several measures of parents’ attitudes about child anxiety and parenting already exist. Measures assessing parenting attitudes about children’s behavior (including anxiety spectrum behavior) include the Child Behavior Vignettes (CBV; Coplan et al., 2002; Hastings & Grusec, 1998; Mills & Rubin, 1990), the Parent Beliefs Questionnaire on Anxiety in Children (Nauta, Bögels, & Siqueland, 2002), and the Parental Beliefs about Anxiety Questionnaire (Francis & Chorpita, 2010). Parenting attitudes about child anxiety and shyness derived from these measure have been highlighted as correlates of parent anxiety, child anxiety, parenting behavior, and socialization (Francis & Chorpita, 2011; Hastings & Rubin, 1999; Kiel & Buss, 2012; Rubin, Coplan, & Bowker, 2009). Parents of anxiety-prone children, in particular, have been shown to evaluate their children as more vulnerable and to more accurately, yet more anxiously, anticipate situations that elicit fear and anxiety than parents of less anxiety-prone children (Hastings & Rubin, 1999; Herren, In-Albon, & Schneider, 2013; Kiel & Buss, 2011). Mothers of inhibited children have also reported distress associated with their child’s shy and withdrawn behavior (Hastings & Rubin, 1999). Other measures of parents’ evaluations assess parenting competence, parental responsibility for the child, or parents’ attitudes about behaviors relevant to externalizing problems (Apetroaia, Hill, & Creswell, 2015; Laskey & Cartwright-Hatton, 2009). These types of parenting attitudes relate to parent anxiety, child anxiety, and maladaptive parenting behavior (Apetroaia et al., 2015; Laskey & Cartwright-Hatton, 2009). Although attitudes about child shyness/anxiety and parenting competence appear to be related to protective and intrusive parenting responses, no existing measures assess parents’ attitudes about these behaviors, specifically.
One aspect of previously studied parenting attitudes, parenting goals, may shed light on how parents assess the value of responding in particular ways. Parenting goals characterize what parents want to achieve in their interactions with their child (Coplan et al., 2002). For example, parent-centered goals focus on resolving the situation immediately, such as quickly terminating the child’s displays of shyness and anxiety. Relationship-centered (also, “child-centered”) goals focus on helping the child feel good about the parent–child relationship or to learn something from a situation. Thus, it may be inferred that, depending on the particular goal a parent has for a situation, she or he might engage in protective or intrusive behavior to stop the anxious behavior in that moment, or, alternatively, to help the child learn something for the future. Whether parents evaluate their overcontrolling behavior as having these functions has yet to be tested.
Furthermore, given that some parents report being distressed by their children’s withdrawn behavior, parents may engage in these different behaviors to help manage their own distress when children display anxiety. Parents of anxious children, compared with parents of nonanxious children, may have a lower tolerance for seeing their child in distress as a result of their own limited ability to cope with negative emotions (Tiwari et al., 2008). In one study, Turner, Beidel, Roberson-Nay, and Tervo (2003) found that anxious parents were no more likely than nonanxious parents to engage in intrusive behavior, but they did report more distress than nonanxious parents when their children participated in routine activities and play. In another study, anxious parents intruded only when their children were displaying negative emotions (Hudson, Comer, & Kendall, 2008). Cortisol reactivity and embarrassment about child shyness have been found to play a role in observed intrusive behavior (Kiel & Buss, 2013). Thus, it is possible that some parents engage in protection or intrusiveness to reduce their own distress. Unfortunately, we lack direct assessments of parents’ attitudes about this function of overcontrol.
The Current Studies
Previous literature has established relations among protective and intrusive parenting behaviors and child anxiety, and measures exist to assess parental attitudes about youth’s anxious symptoms. Importantly, however, there is no measure to assess parents’ attitudes about their own protective and intrusive parenting behaviors. Thus, the goal of the current study was to develop a new measure. This measure, the Attitudes about Parenting Strategies for Anxiety (APSA) scale, was developed to assess parents’ distress in relation to child anxiety as well as their attitudes about protective and intrusive behaviors. Given that measures already exist for assessing parent attitudes about the acceptability of children’s shy/anxious behavior (Coplan et al., 2002; Francis & Chorpita, 2010; Hastings & Grusec, 1998; Nauta et al., 2002), we focused on parenting behaviors. In Study 1, we used a large online sample to investigate the factor structure, internal consistency, and validity of the APSA. Person-centered approaches can complement variable-centered techniques by identifying heterogeneous patterns of attitudes that characterize individuals. Therefore, Study 1 also included a latent profile analysis of APSA items. In Study 2, the measure was completed by a sample of mothers engaged in a larger laboratory-based study, and additional factor analysis and analyses for reliability and validity were performed.
For Study 1, we hypothesized that the APSA would yield separate factors for protective and intrusive behaviors and that resulting scales would demonstrate adequate internal consistency. Furthermore, we hypothesized that more anxious parents and parents who perceive their children to experience higher anxiety symptoms would report more distress when asked to imagine their children showing shyness and anxiety in the vignettes. We also hypothesized that more positive attitudes about the effectiveness of protective and intrusive behaviors in the moment, for children’s future behavior, and for the parents themselves would relate to higher parent anxiety, higher child anxiety, more negative parenting attitudes about child shyness and anxiety, and higher engagement in protective and intrusive behaviors. Finally, we hypothesized that the latent profile analysis would reveal heterogeneous groups based on attitude items, but given no prior person-centered analyses of parenting attitudes in the literature, we did not have specific hypotheses about how items would determine groups, or how groups would differ on measure of parent or child anxiety, parenting goals, or perceived parenting behaviors.
Study 1
Method
Participants
Participants were recruited from Amazon’s Mechanical Turk (MTurk), a recruitment website that allows potential participants to select and engage in online surveys. MTurk is quickly gaining usage for psychological research. Internal consistency and test–retest reliability of data collected through this site has been found to be comparable to traditional methods of data collection (Buhrmester, Kwang, & Gosling, 2011). Specifically relevant to the current study is the precedent for the ability to collect high-quality data (e.g., validated by consistency checks, psychometrically sound, correlations in expected directions, and more inclusive of fathers) from parents (Schleider & Weisz, 2015). Inclusion criteria included being 18 years of age, a U.S. citizen, and having at least one child between 1 and 12 years of age. Exclusion criteria included endorsement of more than one item on the Jackson Infrequency Scale (see below, n = 122), the target child being reported to have a chronic illness or developmental disability that may affect typical development (n = 30), or having already taken the survey (n = 1). Participants were also excluded if they did not fill out the child’s birthdate or indicated that the child was older than 12 (n = 25), or provided inconsistent responses about the child’s age or birthdate (n = 81), about which respondents were asked several times throughout the survey. This ensured that the parent responded about the same child and provided more confidence that a true parent was responding. All participants, including those whose data were excluded, were compensated for their time at a rate commensurate with those typical of MTurk surveys ($3.00 for 40 minutes). In all, 853 participants responded to the survey, and, based on the exclusion criteria stated above, 594 (70%) were included in the current study. This is consistent with previous MTurk studies excluding up to 37% of participants based on various criteria (Chandler, Mueller, & Paolacci, 2014).
The 594 final participants included 357 (61%) mothers and 233 (39%) fathers; 4 participants (0.7%) did not indicate their genders. All participants were from unique families. On average, parents were 33.54 years of age (SD = 7.81; range = 18.77-66.57 years). Participants reported their racial identity to be European American (n = 447; 75%), African American (n = 43; 7%), Asian American (n = 32; 5%), Native American (n = 4; 0.7%), biracial (n = 33; 6%), or “Other” (n = 3; 0.5%). The racial makeup of participants in this sample closely mirrored that of the U.S. population, as of the 2010 Census, with 72.4% European American, 12.6% African American, 4.8% Asian American, 0.9% Native American, and 2.3% identifying with two or more races (U.S. Census Bureau, 2010). Twenty-nine participants (5%) identified themselves as Hispanic, Latino, or Chicano. In the 2010 Census, 16.3% of the population identified themselves as Hispanic, Latino, or Chicano (U.S. Census Bureau, 2010). Most parents (94%) reported that they were the biological parents of the child about which they completed the survey. Parents reported gross annual family income as falling into the following categories: less than $15,000 (n = 36; 6%), $15,000 to $29,000 (n = 107; 19%), $30,000 to $44,000 (n = 115; 20%), $45,000 to $59,000 (n = 106; 18%), $60,000 to $74,000 (n = 69; 12%), $75,000 to $89,000 (n = 58; 10%), $90,000 or higher (n = 86; 15%). Individuals in the United States reported gross annual family income as falling into the following categories in 2015: less than $15,000 (11.6%), $15,000 to $34,000 (20.5%), $35,000 to $49,000 (12.7%), $50,000 to $74,000 (16.7%), $75,000 to $99,000 (12.1%), $100,000 or higher (26.4%; U.S. Census Bureau, 2016). Children (49% female) were in one of three age groups, specified for the purposes of administering the age-appropriate measure of child anxiety: 1 to 3 years (n = 227, 38%; M = 2.29 years, SD = 0.92 years), 4 to 8 years (n = 205, 35%; M = 5.71 years, SD = 1.11 years), or older than 8 years (n = 162, 27%; M = 10.53 years, SD = 1.78 years). Roughly half of children had other siblings (32% had one sibling, 13% had two, 4% had three, 2% had four or more, and 49% were only children). Parents with only one child were heavily represented in the 1 to 3 years (52%) compared with the 4 to 8 years (30%) and older than 8 years (18%) age group.
Procedure
All procedures were approved by the university’s institutional review board. Potential participants saw a brief description of the study on the MTurk website. If they selected it, participants were taken to a website with the survey, the first screen of which was an informed consent form. Participants were informed that data would be collected anonymously. After providing informed consent, participants completed a battery of questionnaires, only some of which were included in the current study. Participants were instructed to answer questions about the same child throughout the survey. On completing the measures, participants saw a debriefing screen, were thanked for their time, and were provided a completion code to receive financial compensation through the MTurk site. On average, participants completed the survey in 34.79 minutes (SD = 17.43 minutes).
Measures
Parent Attitudes About Protective and Intrusive Parenting Behaviors
The APSA is a new measure that assesses parents’ attitudes about protective and intrusive responses to child anxiety-spectrum behavior. The measure (see the appendix) presents three vignettes about situations that might induce anxiety, shyness, or inhibition in children (i.e., interacting with a clown at a birthday party, speaking to an unfamiliar adult, feeding small animals at a petting zoo) that are similar to tasks used in studies assessing fearful/inhibited temperament (Buss, 2011; Buss & Goldsmith, 2000; Calkins & Fox, 1992). Parents first rated how distressed they would feel to see their child react to the situation in a shy or anxious manner on a 1 (none/not at all) to 5 (extremely) scale. Parents were then instructed to imagine engaging in a protective response (e.g., telling the child they do not have to engage) and then responded to several items on the same scale about their attitudes about the protective response (“attitude items,” see Table 1). Finally, parents were instructed to imagine engaging in an intrusive response (e.g., forcing the child to engage) and responded to the same attitude items.
Descriptive Statistics and Factor Loadings for Attitude Items on the Attitudes About Parenting Strategies for Anxiety Scale.
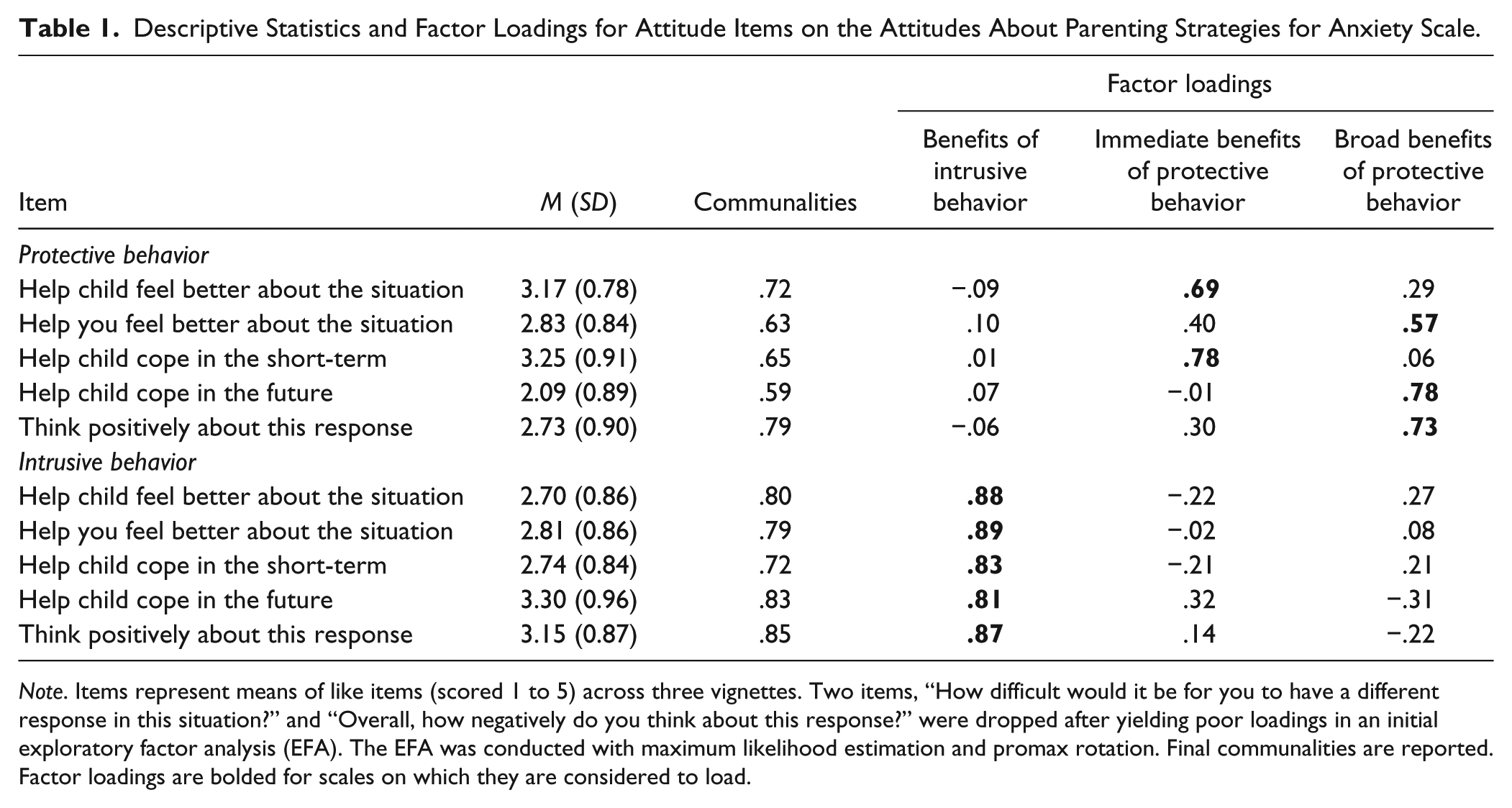
Note. Items represent means of like items (scored 1 to 5) across three vignettes. Two items, “How difficult would it be for you to have a different response in this situation?” and “Overall, how negatively do you think about this response?” were dropped after yielding poor loadings in an initial exploratory factor analysis (EFA). The EFA was conducted with maximum likelihood estimation and promax rotation. Final communalities are reported. Factor loadings are bolded for scales on which they are considered to load.
Parent Anxiety
Parents completed the Depression Anxiety Stress Scales (DASS; Lovibond & Lovibond, 1995), which is a reliable and valid measure (Crawford & Henry, 2003) that asks respondents to indicate how much statements about core symptoms of depression, anxiety, and stress apply to them on a 0 (did not apply to me at all) to 3 (applied to me very much, or most of the time) scale. The current study utilizes the Anxiety subscale (7 items, α = .86; e.g., “I felt I was close to panic”). Following previously established scoring procedures (Lovibond & Lovibond, 1995), the sum of items was computed and then multiplied by two to create the final variable of parental anxiety.
Parent Attitudes About Child Shyness
The CBV (Coplan et al., 2002; Hastings & Rubin, 1999) is a reliable and valid vignette-based measure of parents’ goals, attributions, and emotions in relation to child behavior. The current study used the Shyness vignette, which provides a scenario of the parent dropping her or his child off at school and seeing the child act shy around peers. Parents reported on their parent-centered goals (2 items; e.g., “I would want my child to behave properly, right away”) and their relationship-centered goals (3 items; e.g., “I would want my child to know that I love him or her”) on a 1 (not at all important) to 5 (very important) scale. We found a strong correlation between the two parent-centered goals (r = .77, p < .001) and adequate internal consistency for the relationship-centered goals (α = .70). Means of items were computed to create the goal scales. Parents also rated the extent to which they feel angry, embarrassed, and happy (1 item each) on a 1 (not at all) to 5 (very strongly) scale. The fact that these are one-item measures and therefore cannot yield internal reliability information warrants some caution in interpreting relevant results.
Parent Behavior
The Child-Rearing Practices Report (CRPR; Block, 1965) was originally developed as a Q-sort to assess parents’ attitudes and behaviors regarding child rearing. It has since been adapted and validated as a questionnaire, in which items are answered on a scale from 1 (strongly disagree) to 6 (strongly agree) and make up 21 scales (e.g., Hastings & Rubin, 1999; Volbrecht & Goldsmith, 2010). The current study used the Encouraging Independence (7 items α = .67; e.g., “I try to let my child make many decisions for him or herself”) and Protection (4 items, α = .56; e.g., “I prefer that my child not try things if there is a chance she or he might fail”) scales. Although internal consistencies of these scales were low, this is consistent with previous studies and has been explained by the original measure being developed as a Q-sort because this methodologically uses items that, in a forced-ranking paradigm, should have low correlations with one another (Hastings & Rubin, 1999). The final variables of Encouraging Independence and Protection were derived by calculating means of relevant items.
Child Anxiety
Parents completed items from one of three measures, depending on the child’s age. For children 1 to 3 years, parents completed items from the Infant–Toddler Social Emotional Assessment–Revised (ITSEA; Carter & Briggs-Gowan, 2000) which reliably measures typical and atypical behaviors in young children (Carter, Briggs-Gowan, Jones, & Little, 2003). The current study used the Separation Distress (6 items, α = .77; e.g., “Cries or hangs onto you when you try to leave”), General Anxiety (10 items, α = .76; e.g., “Seems nervous, tense, or fearful”), and Inhibition to Novelty (5 items, α = .87; e.g., “Is shy with new children”) subscales. Means of relevant items were computed to derive scale scores. These scales were intercorrelated (rs = .36-.43, ps < .001) and so were averaged to provide the anxiety measure for the youngest group.
For children between the ages of 4 and 7 years, parents completed the Health Behavior Questionnaire (HBQ; Ablow et al., 1999), a multidimensional measure of children’s functioning, which has been found to provide a valid assessment of mental health difficulties. The current study used the Separation Anxiety (10 items, α = .80; e.g., “Worries about being separated from loved ones”), Overanxious (12 items; α = .75; e.g., “Worries about doing better at things”), and Social Inhibition (3 items, α = .72; e.g., “Shy with other children”) subscales. The mean of relevant items was taken to derive scale scores. These scales were interrelated (rs = .36-.61, ps < .001), so their average comprised the final variable of child anxiety for the 4- to 7-year-old age group.
For children between the ages of 8 and 12 years, parents completed the Revised Children’s Anxiety and Depression Scale–Parent Version (RCADS; Chorpita, Yim, Moffitt, Umemoto, & Francis, 2000), which is a reliable and valid measure for evaluating depressive and anxious symptomatology in middle childhood. The RCADS requires parents to respond about the frequency of symptoms on a 0 (never) to 3 (always) scale across 47 items. The current study utilized the Separation Anxiety (7 items; α = .80; e.g., “My child worries about being away from me”), Generalized Anxiety (6 items, α = .86; e.g., “My child worries about things), and Social Phobia (9 items α = .86; e.g., “My child feels afraid that he or she will make a fool of him or herself in front of people”) scales. The mean of respective items comprised each scale. Scales were found to be interrelated (rs = .48-.65, ps < .001), so they were averaged to yield the final measure of child anxiety for children in the 8- to 12-year age range.
Screening for Invalid Responses
Parents completed the Infrequency Scale of the Personality Research Form (Jackson, 1984), which contains 12 true/false items that should be endorsed in the same way by the vast majority of the population (e.g., “On some occasions I have noticed that some people are better dressed than myself”). Answering more than one of these statements in the unexpected direction suggests an invalid response style, or that a “bot” is completing it. We used this criterion to exclude participants from analyses.
Analysis Plan
We first investigated the psychometric properties of the APSA by testing its factor structure and internal consistency of resulting scales. We performed descriptive statistics on the items and scales, testing potential differences based on parent and child gender. We tested correlations between these scales and other measures to provide initial information about the validity of the measure. Finally, we performed a latent profile analysis of the scales to take a person-centered approach to understanding patterns of attitudes about parental overcontrol.
Results
We examined descriptive statistics for each of the attitude items. Means and standard deviations are presented in Table 1. Scores of all items ranged the entirety of possible values (minimum = 1.00, maximum = 5.00) and demonstrated reasonable adherence to a normal distribution (skew and kurtosis < |1.00|).
Exploratory and Confirmatory Factor Analyses
We randomly split the sample in half, performing exploratory factor analysis (EFA) on the first half and confirmatory factor analysis (CFA) on the second half. APSA items evaluating parents’ attitudes about protective and intrusive responses were subjected to an EFA using maximum likelihood estimation and promax rotation to assess the underlying factor structure. All participants had complete data for the APSA. The Kaiser–Meyer–Olkin measure of sampling adequacy (.81) and Bartlett’s test of sphericity, χ2(45) = 2131.09, p < .001, supported the EFA. The ocular scree test, Horn’s parallel analysis, and eigenvalues were used to determine the number of factors to retain. All methods suggested the retention of three factors. Item were considered to reside on a factor if pattern coefficients loaded >.32, and we planned to drop items loading >.50 on two factors (Tabachnick & Fidell, 2001). Of note, no items were dropped by this criterion.
See Table 1 for item communalities and factor loadings. All items about attitudes about intrusive behavior loaded on one factor, which we named, “Perceived Benefits of Intrusive Behavior.” The attitude items for protective behavior were split between two factors, which we named, “Perceived Immediate Benefits of Protective Behavior” and “Perceived Broad Benefits of Protective Behavior.” The item addressing how much protective behavior would help the parent feel better loaded >.32 on both the perceived Immediate Benefits and Perceived Broad Benefits scales, which makes some sense because it is both concerned with the present moment and a factor outside of the child’s well-being. For the ease of creating scales, we chose to consider this item on the Perceived Broad Benefits scale, where it had a substantially higher loading, rather than including it in both scales.
CFA was performed using Mplus Version 7. We specified the factor structure suggested by the EFA and allowed the item assessing the parent feeling better from protective behavior to cross-load. The initial model demonstrated poor to mediocre fit, comparative fit index (CFI) = .87, Tucker–Lewis index (TLI) = .82, standardized root mean square residual (SRMR) = .07, root mean square error of approximation (RMSEA) = .16, χ2(31) = 275.40, p < .001. Modification indices suggested several changes to the model. A few suggested changes involved allowing residuals of various items within a factor to correlate. Given the similarity of these items, it seemed reasonable that leftover variance would also be related, so we made this change. Another suggested change was allowing the residuals for the “Help my child cope in the short-term” item on the Perceived Benefits of Intrusive Behavior and Perceived Broad Benefits of Protective Behavior to correlate. We might expect parents to answer the same item similarly for the different types of behaviors, so we adhered to this suggestion. Although we acknowledge that modification indices should be used with caution and that we did not have a prior hypothesis about correlated residuals, we felt they would be valuable in understanding the measure in these initial analyses. After these modifications, the CFI (.95), TLI (.92), and SRMR (.06) converged to suggest adequate fit. The chi-square remained significant, χ2(27) = 122.35, p < .001, and RMSEA (.11) was outside the bounds of adequate fit. Therefore, fit indices were inconsistent in the evaluation of the model.
Finally, also within this half of the sample, we conducted a multigroup SEM analysis to test if the factor structure of the newly created scale differed between mothers (n = 181) and fathers (n = 112; four participants did not provide data on gender and were therefore removed from the data for this analysis). To test for weak factorial invariance, or whether factor loadings could be considered equal across mothers and fathers, a model with loadings constrained across gender was compared with a model with loadings allowed to be freely estimated. The model with parameters allowed to be free fit the data adequately according to some indicators (CFI = .94, SRMR = .07), although the chi-square value was significant, χ2(63) = 184.71, p < .001, and the RMSEA (.12, 90% confidence interval [CI; .10, .13]) fell outside the bounds of acceptable. The model in which factor loadings were constrained fit similarly to the free model, χ2(74) = 199.13, p < .001, RMSEA = .10, 90% CI [.09, .13], CFI = .94, SRMR = .08. Importantly, testing the chi-square difference between the two models indicated that the constrained model did not fit significantly worse than the free model, Δχ2(11) = 14.41, p = .21. This suggests that the structure of the APSA fits similarly across mothers and fathers. Notably, all factor loadings were of similar magnitude across mothers and fathers and each loaded significantly on their respective factors.
Reliability
We evaluated internal consistency of the scales using the full data set. The three distress items, which were not included in the EFA, demonstrated adequate internal consistency (α = .73). Coefficient alphas for items within each of the three scales suggested by EFA also yielded adequate internal consistency (Perceived Benefits of Intrusive Behavior: .92, Perceived Immediate Benefits of Protective Behavior: .81, Perceived Broad Benefits of Protective: .83). Final scales were computed by averaging item scores within scales.
Descriptive Statistics and Missing Data
Prior to testing relations between the APSA scales and other measures, we computed descriptive statistics for the primary measures (Table 2). All variables showed reasonable adherence to normality (skew < |3.00|). We evaluated whether the APSA scales differed according to parent or child gender, or the interaction between the two, using a 2 (parent gender) × 2 (child gender) multivariate analysis of variance. The multivariate test was only significant for parent gender, F(4, 582) = 2.42, p = .048, η p 2 = .016. Parent gender related to Distress, F(1, 585) = 8.83, p = .003, η p 2 = .015, with mothers reporting higher distress (M = 2.17, SD = 0.85) than fathers (M = 1.98, SD = 0.70; Cohen’s d = 0.24). Parent gender did not relate to any of the attitude scales.
Descriptive Statistics and Bivariate Correlations for Study 1 Primary Variables.
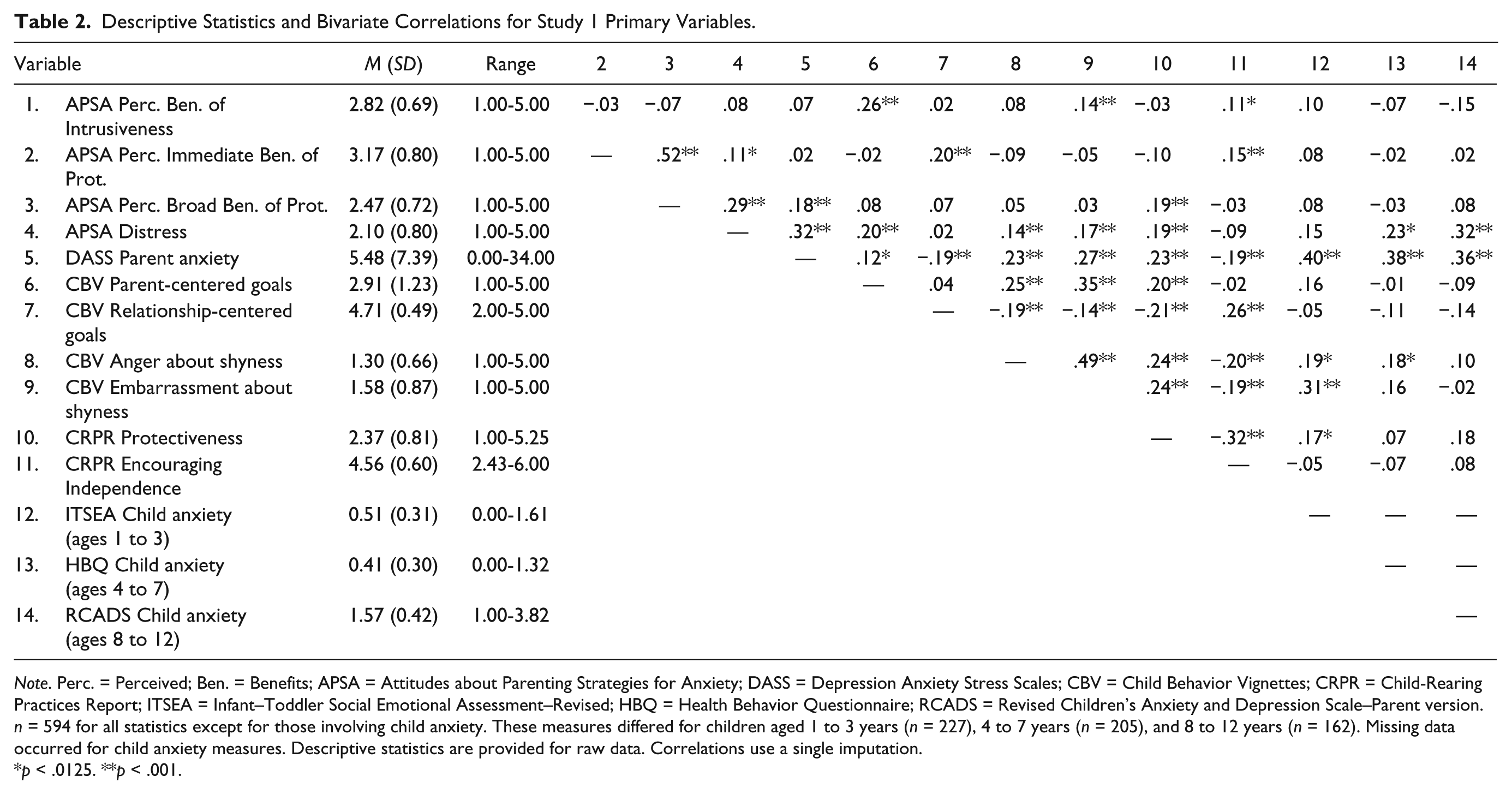
Note. Perc. = Perceived; Ben. = Benefits; APSA = Attitudes about Parenting Strategies for Anxiety; DASS = Depression Anxiety Stress Scales; CBV = Child Behavior Vignettes; CRPR = Child-Rearing Practices Report; ITSEA = Infant–Toddler Social Emotional Assessment–Revised; HBQ = Health Behavior Questionnaire; RCADS = Revised Children’s Anxiety and Depression Scale–Parent version. n = 594 for all statistics except for those involving child anxiety. These measures differed for children aged 1 to 3 years (n = 227), 4 to 7 years (n = 205), and 8 to 12 years (n = 162). Missing data occurred for child anxiety measures. Descriptive statistics are provided for raw data. Correlations use a single imputation.
p < .0125. **p < .001.
We also investigated the nature and extent of missing data within the final sample of 594 participants. Importantly, no participants were missing data on the APSA, and almost all other primary measures had complete data. As exceptions, 13 participants were missing the ITSEA (for children 1-3 years), 2 were missing the HBQ (for children 4-7 years), and 2 were missing the RCADS (for children 8-12 years). In many cases, missingness occurred because the parent completed the anxiety measure for the wrong age group. Overall, this represented 2.86% of cases and 0.24% of observations among primary variables. Participants missing the age-appropriate child anxiety measure did not differ from participants with complete data on other primary variables (including the APSA scales) or demographic variables (all ts < 1.94 or χ2 < 0.44, all ps > .05). Little’s Missing Completely at Random (MCAR) tests were not significant (χ2s = 53.79, 99.81, 83.95 for the youngest, middle, and oldest age groups, respectively, all ps > .05), suggesting data did not deviate from the MCAR pattern of missingness. Given the small number of missing values and the pattern of missingness, we followed contemporary recommendations (Widaman, 2006) and performed a single imputation to derive missing values for child anxiety. Thus, all subsequent analyses use the full data set or full age-appropriate subsample.
Validity
We examined convergent validity for the distress scale through correlations with other measures examining parent distress about child shyness, and construct validity by examining correlations with concomitants of parent distress (e.g., attitudes about child shyness, parenting behavior, child anxiety). Because no existing measure, to our knowledge, assesses parental attitudes about protective and intrusive behavior, we focused on establishing construct validity for the attitude scales with other aspects of parenting and the development of child anxiety. To this end, we investigated relations between the APSA distress and attitude scales, on the one hand, and parental anxiety, parenting goals for and emotional reactions to child shyness, parenting behavior, and child anxiety, on the other. Correlations are presented in Table 2. Given the large number of correlations and the large sample size, we applied a Bonferroni correction consistent with having four families (one for each of the APSA scales) of correlations. Thus, correlations were considered significant at p values less than .0125.
In support of convergent validity of the distress scale, parents who scored higher on the APSA distress scale also scored higher on anger and embarrassment in response to the CBV shyness vignette. In support of construct validity, parents who reported being distressed by their child’s shyness on the APSA also reported more parent-centered goals for a shyness situation and more protective behavior. Parents who perceived their 4- to 7-year-old or 8- to 12-year-old children as more anxious reported higher distress.
In support of construct validity for the attitude scales, a number of relations emerged. Consistent with the hypothesis that parents with higher reactivity to child anxiety-spectrum behavior view overcontrolling parenting more positively, parents who reported more embarrassment in response to shyness on the CBV reported higher Perceived Benefits of Intrusive Behavior. Parents reporting higher Perceived Benefits of Intrusive Behavior reported more encouragement of independence on the CRPR.
Interestingly, differential relations emerged for Perceived Immediate Benefits versus Perceived Broad Benefits of Protective Behavior. Parents reporting higher Perceived Immediate Benefits, but not Perceived Broad Benefits, of Protective Behavior also reported higher relationship-centered goals and encouragement of independence. However, Perceived Immediate Benefits did not relate to protective behavior. Although both Perceived Immediate and Perceived Broad Benefits of Protective Behavior related to Distress in response to their children’s shyness, this relation was stronger for Perceived Broad Benefits (Steiger’s Z = 4.61, p < .001). Parents reporting higher levels of Perceived Broad Benefits, but not Perceived Immediate Benefits, of Protective Behavior reported higher anxiety and engaging in more protective behavior.
Latent Profile Analysis
Latent profile analyses were conducted using Mplus 7 to understand patterns of parental beliefs about protective and intrusive parenting behaviors. Rather than the broader belief scales, the model included the 10 individual items (5 for intrusiveness, 5 for protection) to test whether patterns unique from the factor structure emerged. We compared LPA models based on sample-size adjusted Bayesian information criterion (BIC), the Vuong–Lo-Mendell–Rubin likelihood ratio test, and the parametric bootstrapped likelihood ratio test, as these indices have been shown to most accurately identify correct mixture models in simulation studies (Nylund, Asparouhov, & Muthén, 2007). We fit models with successively more profiles, examining them for a decrease in adjusted BIC (smaller values indicate better fit) and significant likelihood ratio tests (indicating the present model fits better than a model with one fewer profile). We also examined entropy, which indicates certainty in classifying individuals into profiles (values closer to 1 are better). We compared models with up to six profiles (Table 3), as more profiles would be difficult to interpret. Considering all criteria, the model with four profiles represented the best fit. Although adjusted BIC and entropy increased across all six models, the model with four profiles was the last to yield significant results for both the Vuong–Lo–Mendell–Rubin and parametric bootstrapped likelihood ratio tests. This model yielded high probability for class membership (rs = .90-.96, mean r = .93). Participants were assigned profile membership based on the highest posterior probability. The first profile (“moderately low perceived benefits,” n = 239) included parents reporting relatively low (although never the lowest) values across protective and intrusive items. The second profile (“intrusiveness-specific perceived benefits,” n = 132) had the lowest scores on the protective items and the highest scores on intrusive items. The third profile (“protection-specific perceived benefits,” n = 67) represented parents with the highest scores on the protective items and the lowest scores on the intrusive items. Finally, the fourth class (“moderately high perceived benefits,” n = 156) included parents who endorsed relatively high (but never the highest) scores on items about both protective and intrusive parenting behaviors. Figure 2 displays the patterns of means across the APSA attitude scales for the four profiles.
Model Fit for Study 1 Profile Solutions.
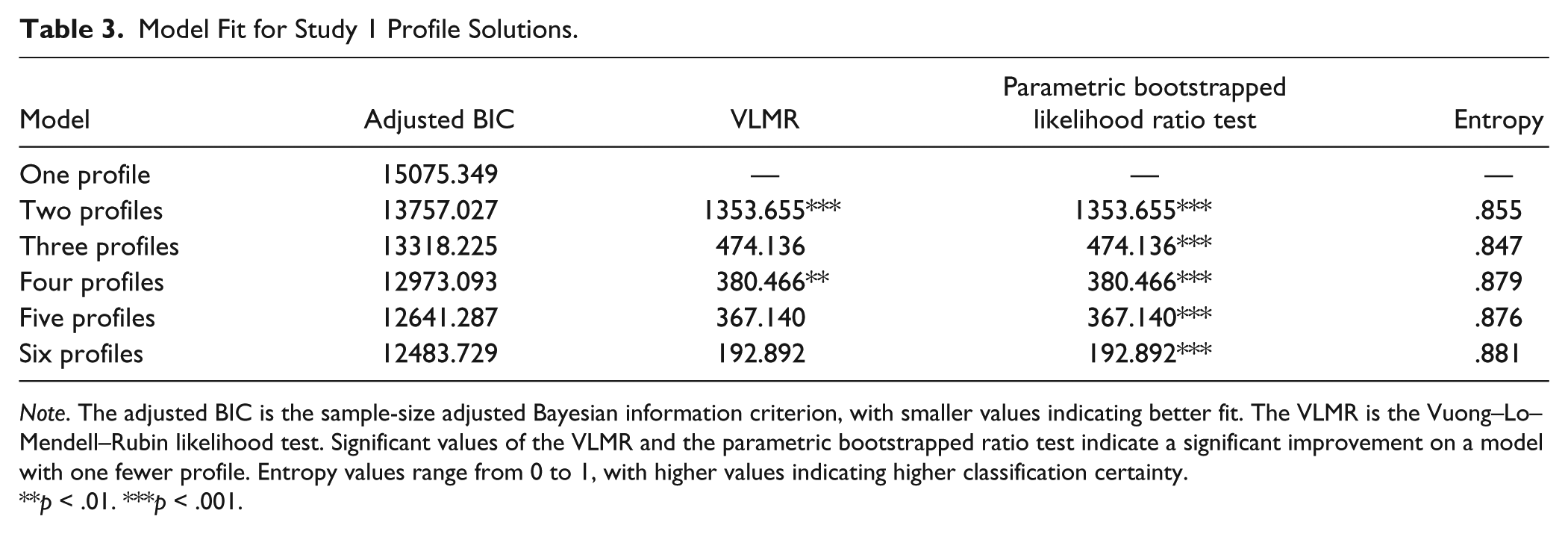
Note. The adjusted BIC is the sample-size adjusted Bayesian information criterion, with smaller values indicating better fit. The VLMR is the Vuong–Lo–Mendell–Rubin likelihood test. Significant values of the VLMR and the parametric bootstrapped ratio test indicate a significant improvement on a model with one fewer profile. Entropy values range from 0 to 1, with higher values indicating higher classification certainty.
p < .01. ***p < .001.
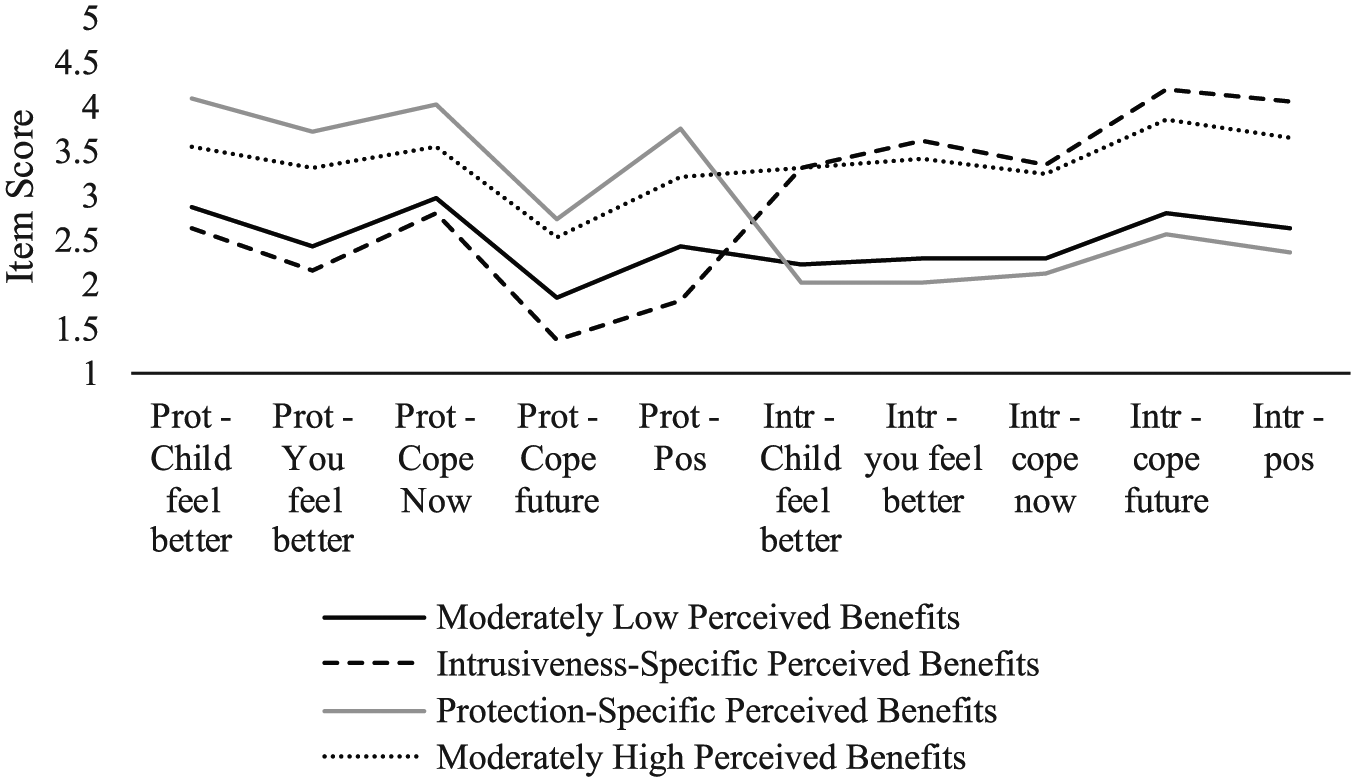
Results of latent profile analysis of attitude items.
We next used one-way analyses of variance (ANOVAs) to examine whether parents differed on APSA distress, parental anxiety, parenting goals for and emotional reactions to child shyness, parenting behavior, and child anxiety based on profile membership (Table 4). Levene’s homogeneity of variances tests were significant for all variables except for parent-centered goals, protection, encouragement of independence, and child anxiety for 1-, 3-, and 4- to 7-year olds. For variables with heterogeneous variance, we examined Welch and Brown–Forsythe tests. Most results did not differ from the original ANOVAs in significance; the few exceptions are noted below. Significant omnibus tests were followed up with Tukey’s wholly significant difference tests for post hoc pairwise comparisons.
Comparisons of Means Among Profiles of Parenting Attitudes.
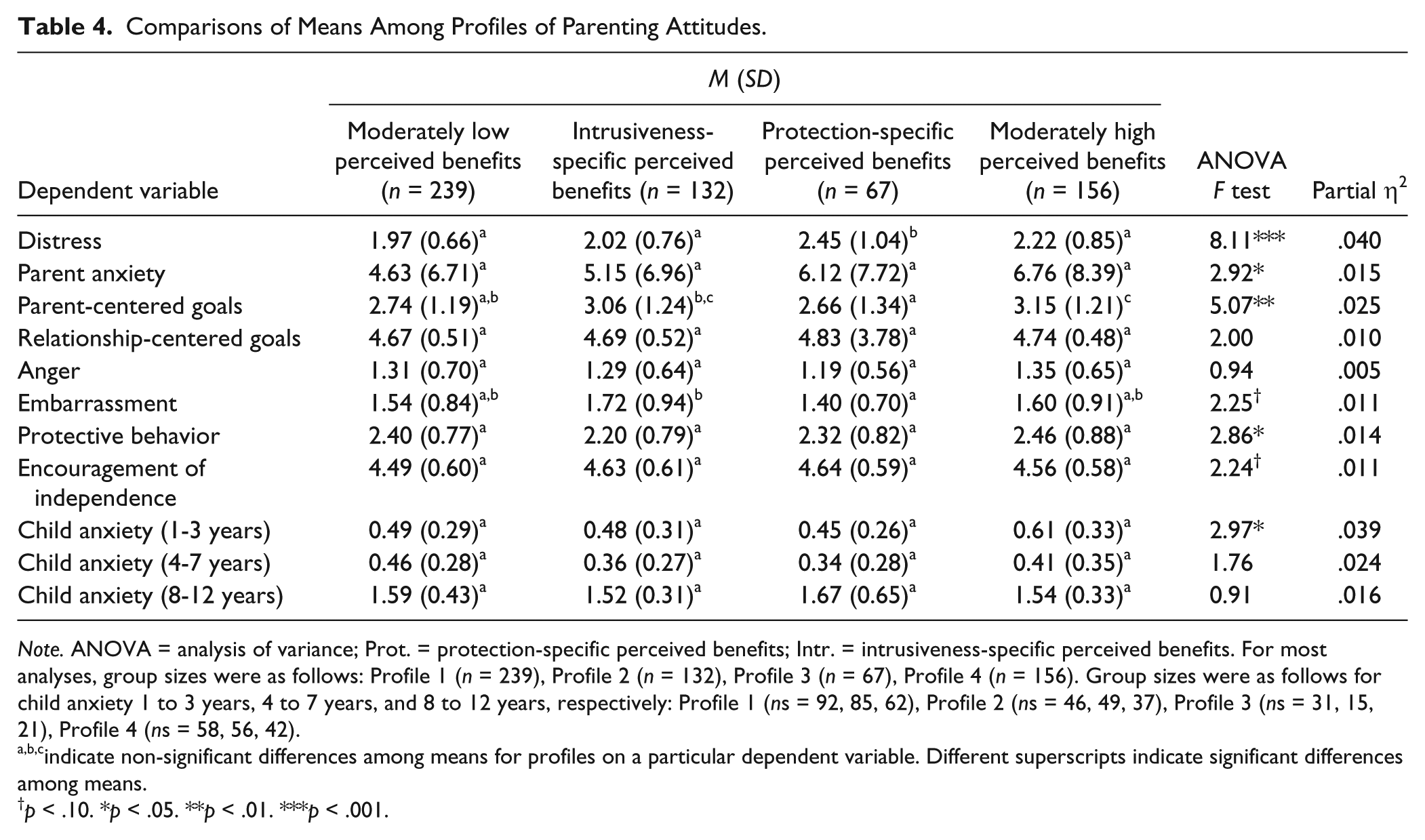
Note. ANOVA = analysis of variance; Prot. = protection-specific perceived benefits; Intr. = intrusiveness-specific perceived benefits. For most analyses, group sizes were as follows: Profile 1 (n = 239), Profile 2 (n = 132), Profile 3 (n = 67), Profile 4 (n = 156). Group sizes were as follows for child anxiety 1 to 3 years, 4 to 7 years, and 8 to 12 years, respectively: Profile 1 (ns = 92, 85, 62), Profile 2 (ns = 46, 49, 37), Profile 3 (ns = 31, 15, 21), Profile 4 (ns = 58, 56, 42).
indicate non-significant differences among means for profiles on a particular dependent variable. Different superscripts indicate significant differences among means.
p < .10. *p < .05. **p < .01. ***p < .001.
The omnibus test for APSA distress was significant, and pairwise comparisons revealed that the “protection-specific perceived benefits” group scored significantly higher on distress than the other three groups, which did not differ from one another. Thus, parents who were more distressed about their child’s shyness felt uniquely positive about protective parenting behavior. The omnibus test for parent anxiety was significant, but no significant pairwise comparisons emerged. A significant omnibus test emerged for parent-centered goals. Pairwise comparisons for parent-centered goals revealed that the “moderately high perceived benefits” group had higher parent-centered goals than the “moderately low perceived benefits” group and the “protection-specific perceived benefits” group, but scored similarly to the “intrusiveness-specific perceived benefits” group. The “intrusiveness-specific perceived benefits” group scored similarly to the “moderately low perceived benefits” group but was higher than the “protection-specific perceived benefits” groups. Thus, endorsing positive attitudes about intrusive behavior appeared to be the driving factor in group differences in parent-centered goals. The omnibus test for relationship-centered goals was not significant for the original ANOVA, but the Welch test was significant, F(3, 246.09) = 2.74, p = .044. Post hoc comparisons revealed no significant differences among profiles. Omnibus tests for angry and embarrassed reactions to shyness did not reach significance. A significant omnibus test emerged for protective parenting behavior, but not encouragement of independence; however, no pairwise comparisons of protective behavior reached significance. The only significant omnibus test for child anxiety was in the 1- to 3-year age range. Parents in the “moderately high perceived benefits” group endorsed higher child anxiety than the “protection-specific perceived benefits” group. Note, however, that the omnibus test fell to marginal significance for both the Welch, F(3, 96.18) = 2.31, p = .081, and Brown–Forsythe, F(3, 181.80) = 2.58, p = .055, tests. In summary, parents solely endorsing positive attitudes about protective responses reported more distress about their children’s shy behaviors, and parents who reported positive attitudes about both protective and intrusive behaviors endorsed higher parent-centered goals and perceived their 1- to 3-year-old children to be higher in anxiety. Parents reporting positive attitudes about intrusive behaviors, whether or not they felt positively about protective parenting, reported higher parent-centered goals than if they reported less positive attitudes about intrusive behaviors.
Discussion
Study 1 examined the structure, reliability, and initial validity of the APSA. EFA suggested that attitude items fell into one of three scales: Perceived Benefits of Intrusive Behavior, Perceived Immediate Benefits of Protective Behavior, and Perceived Broad Benefits of Protective Behavior, each of which were found to have “good” to “excellent” internal reliability. Person-centered analyses suggested that patterns of high versus low levels of positive attitudes about intrusive and protective behaviors related meaningfully to parental and child characteristics, as well as self-reported parenting behaviors. Although the factor analysis suggested that attitudes about protective behavior should be subdivided into the immediate and broad benefits, the person-centered analysis suggested that protective items hung together in the various profiles.
Bivariate correlations provided initial validity information about the measure. Specifically, parents reporting distress in response to child anxiety-spectrum behavior on the APSA also reported greater anxiety, generally, as well as specific negative emotions (anger, embarrassment) in response to child shyness on another measure. Greater distress on the APSA also related to parent-centered goals and more protective behavior, consistent with previous research showing that parents with higher levels of traits related to distress (e.g., anxiety, negative emotionality) had similar goals and behaviors (Apetroaia et al., 2015). Parents’ own distress may prevent them from focusing on anything more than resolving the immediate situation, consistent with goals that focus on the child’s immediate compliance and behaving to minimize distress by taking over the child’s emotion regulation.
Importantly, we found relations between parents’ attitudes about protective and intrusive behaviors and the extent to which they reported engaging in these behaviors. Viewing intrusive behavior more positively related to more encouragement of independence. Although intrusiveness and encouragement of independence are not the same construct, they are similar in encouraging approach-oriented behavior. For protective behavior, relations between positive attitudes and reports of engagement in protective behavior differed based on whether parents focused on the immediate situation or more broadly. Results indicated that parents may perceive immediate benefits of protective behavior but do not act on these perceptions in the service of maintaining a positive relationship and encouraging independence. Perceiving more broad benefits of protective behavior related to higher reports of engagement in protective behavior. Thinking about the child’s future development as well as the parent’s own reaction to child anxiety may be particularly important in determining when protective behavior occurs. The fact that distress in relation to child anxiety was also more highly related to broad than immediate benefits of protective behavior is consistent with previous conceptualizations of protective or withdrawal-based responses as being motivated by the parent’s own subjective experience of seeing their children display anxious behavior (Tiwari et al., 2008).
Study 1 had several limitations. The alpha values of the parenting behavior scales were similar to those found in previous studies and understandable given that the measure was originally developed as a Q-sort (Hastings & Rubin, 1999). Low reliability would nevertheless attenuate associations with other variables and may also indicate that the CRPR did not adequately measure the parenting behaviors of interest. We used one-item measures for parental emotional reactions to child shyness, for which reliability could not be assessed. We cannot verify the identities of MTurk participants, and it is unclear whether social desirability would influence parent report on parenting, such that parents report different behaviors than they actually enact. Furthermore, we were unable to provide estimates of test–retest reliability or stability of the APSA scales. Study 1 was also limited by its focus on a broad measure of parental anxiety that assessed primarily physiological reactions. It is possible that different types of anxiety, such as worry and social anxiety, could have unique relations to distress and parenting attitudes about overcontrol. Therefore, Study 2 examined the APSA in a laboratory-based study of mothers and children that addressed these concerns. We hypothesized that the APSA would show similar psychometric properties (internal consistency, factor structure, convergent validity) as in Study 1 as well as moderate stability. We further hypothesized that attitudes about parenting behaviors would show stronger relations to worry and social anxiety than with physiological symptoms of anxiety given the shared cognitive nature of these constructs.
Study 2
Method
Participants
This sample comprised 120 mother–toddler dyads participating in a laboratory-based longitudinal study of temperament and parenting. Participants were recruited by mail based on birth announcements published in local newspapers, in person at meetings of the Women, Infants, and Children program, and from flyers hung in pediatricians’ offices, child care centers, and other local establishments. The current study focuses on the 108 participants (90%) who completed the APSA. Dyads were invited to come to the laboratory when toddlers were approximately 24 to 30 months old (Time 1: M = 26.84 months, SD = 2.10 months). Mothers were 19.67 to 45.11 years old (M = 32.55, SD = 5.53). Mothers reported themselves and their children, respectively, to be European American (88.0%, 82.4%), Black/African American (1.9%, 1.9%), Asian or Pacific Islander (3.7%, 1.9%), Native American (0.9%, 0%), multiracial (0%, 9%) or “Other” (0.9%, 1.9%). Two mothers (1.9%) and three children (2.8%) were reported to be Hispanic or Latina/o. Five mothers (4.6%) did not report on race/ethnicity for themselves or their children. Most children (78.7%) resided with both biological parents, 13.9% lived only with their mothers, and 3% lived with adoptive parents. A subsample of mothers (n = 98, 91%) were invited to participate in a 1-year follow-up assessment when children were approximately 36 to 42 months old (Time 2) based on the child aging into this age range. Of this subset, 63 (64%) participated and completed the Time 2 APSA.
Procedure
After expressing interest in participating, mothers scheduled a 3-hour laboratory visit. Laboratory staff mailed mothers a consent form and questionnaires (including the APSA, DASS, and ITSEA) to be completed prior to the visit. Mothers completed other questionnaires (including additional maternal anxiety measures) prior to leaving the laboratory.
Measures
In addition to the APSA (internal consistency provided in the Results), mothers filled out some of the same measures as in Study 1, including the DASS to measure maternal anxiety (α = .86) and the ITSEA to measure child anxiety (α = .78). Additional measures are listed below.
Maternal Anxiety
Mothers completed the Penn State Worry Questionnaire (PSWQ; Meyer, Miller, Metzger, & Borkovec, 1990). The PSWQ asks respondents to rate various aspects of worry and its uncontrollability (e.g., “My worries overwhelm me”) on a 1 (not at all typical of me) to 5 (very typical of me) scale. Items are reverse-scored as necessary and then summed to create a total score, which had excellent internal consistency in the current study (α = .94).
Mothers also completed the Social Interaction Anxiety Scale (Mattick & Clarke, 1989), which has been shown to be reliable and valid in assessing anxiety experienced during interactions with others (Brown et al., 1997). It comprises 20 items assessing difficulties with social interactions (e.g., “I become tense if I have to talk about myself or my feelings”) on a 1 (not at all characteristic or true of me) to 4 (extremely characteristic or true of me) scale. We summed item scores (reversed if necessary) for a total score of social anxiety (α = .94).
Maternal Parenting Behavior
Mothers completed the New Friends Vignettes (McShane & Hastings, 2009), a 36-item measure of parenting responses to children’s shy behavior. In each of two vignettes, mothers were asked to imagine their child acting shy when interacting with unfamiliar children and then to rate the likelihood as 0 (no), 1 (maybe), or 2 (yes) that they would engage in particular behaviors. The Overprotection scale comprises 12 items describing responses that encourage withdrawal by distracting the child with comfort or directly suggesting avoidance of the situation (e.g., “I would say, ‘Do you want to go home and play with Mommy?’”). The Critical Control scale comprises 12 items involving verbal criticism of the shy behavior or intrusive movement of the child into the situation (e.g., “I would move my son/daughter so he or she was standing in front of me”). The current study found adequate internal consistency for both the Overprotection (α = .79) and Critical Control (α = .69) scales.
Analysis Plan
Prior to primary analyses, we confirmed the factor structure of the APSA, computed descriptive statistics, examined gender differences, and described and handled missing data. We then calculated the internal consistency of the APSA scales and used partial correlations (controlling for variables related to missingness) to examine the stability of the scales from age 2 to age 3. Bivariate correlations addressed the construct validity of the scales in relation to concurrent measures of maternal anxiety, parenting behavior, and child anxiety.
Results
Factor Structure
We conducted a CFA for the factor structure established in Study 1 using maximum likelihood estimation in Mplus Version 7. We did not include the post hoc modifications from Study 1. An initial model yielded mixed evidence across fit indices, with the SRMR (.05) suggesting close fit, CFI (.94) and TLI (.92) suggesting acceptable fit, and the RMSEA (.11) and significant chi-square, χ2(32) = 76.40, p < .001, suggesting poor fit. Two modification indices suggested allowing correlations between the residuals of the “Help my child feel better” item for Intrusiveness and the “Help my child cope in the future” item for Protectiveness, as well as between the items of “Help my child cope now” and “Help my child feel better for Intrusiveness.” These modifications seemed reasonable given that items in each respective pair were similarly assessing perceptions of children’s coping. After modeling these correlations, the chi-square remained significant, χ2(30) = 52.33, p = .007, but the majority of indices suggested at least adequate fit (SRMR = .05, CFI = .97, TLI = .96, RMSEA = .08).
Descriptive Statistics
Descriptive statistics can be found in Table 5. Most variables reasonably adhered to a normal distribution (skew < |3.00|), but DASS anxiety showed positive skew (skew = 3.42). We added a constant and submitted it to a square root transformation, which reduced skew to normal limits (skew = 2.02). No differences emerged in the APSA scales based on child gender (all ts < 1.00, all ps > .30).
Study 2 Descriptive Statistics and Bivariate Correlations Among Primary Variables.
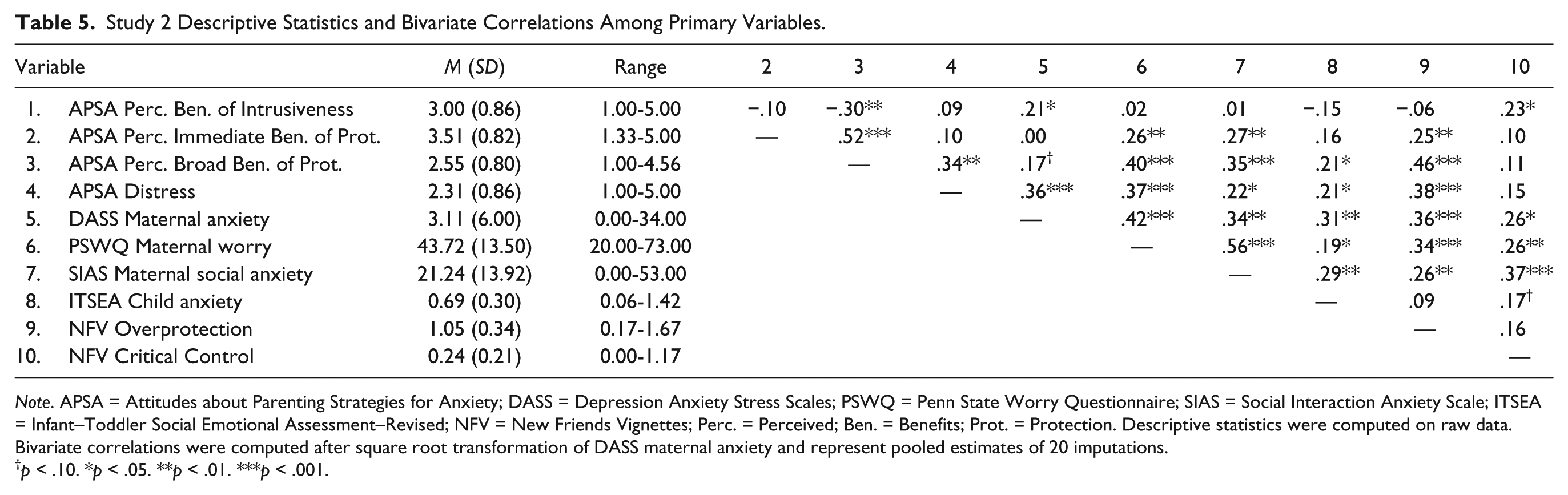
Note. APSA = Attitudes about Parenting Strategies for Anxiety; DASS = Depression Anxiety Stress Scales; PSWQ = Penn State Worry Questionnaire; SIAS = Social Interaction Anxiety Scale; ITSEA = Infant–Toddler Social Emotional Assessment–Revised; NFV = New Friends Vignettes; Perc. = Perceived; Ben. = Benefits; Prot. = Protection. Descriptive statistics were computed on raw data. Bivariate correlations were computed after square root transformation of DASS maternal anxiety and represent pooled estimates of 20 imputations.
p < .10. *p < .05. **p < .01. ***p < .001.
Missing Data
Missing values occurred across several of the age 2 questionnaires, including the anxiety variables (n = 2) and the parenting variables (n = 4). Overall, six participants had at least one missing value at Time 1. Furthermore, 45 mothers did not complete the APSA at Time 2 (some of whom were not invited to), and one additional mother missed enough Distress items that this scale could not be calculated. Overall, 12.90% of values were missing.
A significant Little’s MCAR test, χ2(129) = 164.59, p = .029, suggested that data could not be considered MCAR. Participants with versus without missing Time 1 data reported lower socioeconomic status (a composite of maternal education and household income; t(7.12) = 3.49, p = .010; Cohen’s d = 1.09. Mothers missing Time 2 data reported higher anxiety both on the DASS, t(47.09) = 2.26, p = .029; Cohen’s d = 0.48, and PSWQ at Time 1, t(104) = 2.53, p = .013; Cohen’s d = 0.50. Given relations of missingness to observed variables and our ability to include these variables in the imputation of missing values and relevant analyses, remaining variance in the occurrence of missing values most likely adheres to a missing at random pattern (Enders, 2010). We used multiple imputation to handle missing values. Twenty imputations were run using all primary variables and sociodemographic variables (maternal age, socioeconomic status) in the algorithm. We report pooled estimates of statistics (weighted by standard errors in aggregation).
Internal Consistency and Stability
To assess reliability of the APSA, we examined internal consistency and 1-year stability. Cronbach’s alphas indicated that all scales of the APSA at age 2 demonstrated good internal consistency. The Distress scale had an alpha of .81. Alpha values were good for Perceived Immediate Benefits of Protective Behavior (α = .82) and Perceived Broad Benefits of Protective Behavior (α = .85). In addition, the internal consistency for Perceived Benefits of Intrusive Behavior was excellent (α = .94). Similar values were found 1 year later at age 3: Distress (α = .78), Perceived Immediate Benefits of Protective Behavior (α = .83), Perceived Broad Benefits of Protective Behavior (α = .85), Perceived Benefits of Intrusive Behavior (α = .94).
Partial correlations 1 between Time 1 and Time 2 APSA scales (controlling for anxiety variables related to missing Time 2 measures) revealed moderate 1-year stability for Distress (r = .32, p < .01), Perceived Immediate Benefits of Protective Behavior (r = .46, p < .001), Perceived Broad Benefits of Protective Behavior (r = .42, p < .001), and Perceived Benefits of Intrusive Behavior (r = .47, p < .001). Paired-samples t tests revealed that mean scores of the attitude scales did not change across time (ts < 1.30, ps > .20). Distress showed a decrease from age 2 to age 3 (t = −2.48, p = .017; Cohen’s d [estimated from original data] = −0.53).
Validity
We examined construct validity of the distress and attitude scales. We computed correlations between the APSA scales, on the one hand, and measures of maternal anxiety, parenting behavior, and child anxiety, on the other (Table 5). In support of the construct validity of the Distress scale, mothers reporting higher distress reported higher anxiety, worry, and social anxiety, and they perceived their children as more anxious. In support of the construct validity of the Perceived Immediate and Broad Benefits of Protective Behavior scales, mothers reporting higher scores on each also reported more worry and social anxiety. These correlations did not differ between the two scales (Steiger’s Zs < 1.60, ps > .10). Mothers endorsing higher levels of Perceived Broad Benefits of Protective Behavior also reported their children to display more anxiety. Both Perceived Immediate and Broad Benefits of Protective Behavior also related to overprotection. In this case, the correlation for Broad Benefits was significantly higher than that for Perceived Immediate Benefits (Steiger’s Z = 2.40, p = .016). Mothers reporting higher Perceived Benefits of Intrusive Behavior reported higher anxiety on the DASS but not more worry or social anxiety, and they reported more critical control.
Discussion
Study 2 extended the examination of reliability and validity of the APSA in a laboratory-based sample of mothers and toddlers. We found similar internal consistency for the distress and attitude scales, both at age 2 and at age 3. Furthermore, scale scores were relatively stable across the toddler period, with correlations in the medium to large range according to Cohen’s (1988) guidelines on effect sizes, and t tests suggesting no significant change over time except for a decrease in distress. Moderate stability may suggest that attitudes about anxiety-relevant parenting behaviors are trait-like. However, moderate correlations also suggest meaningful unique (unshared) variance across time, which future studies may attempt to understand. For instance, toddler temperament and parenting characteristics may interact with initial beliefs to predict change in attitudes over time in a transactional fashion (Hastings & Rubin, 1999).
Several aspects of validation were replicated between the two studies. For example, maternal anxiety related to the distress scale. More positive attitudes about protective behavior related to mothers’ self-reported protective/overprotective behaviors, and this correlation was again higher for Perceived Broad than Perceived Immediate Benefits. Thus, protective parenting may be uniquely related to cognitions pertaining to broader issues, such as the child’s development and mothers’ own distress, rather than what is happening in the moment. A finding unique to Study 2 that supports this notion is that maternal perceptions of child anxiety were related to both the Distress and the Perceived Broad Benefits of Protective Behavior scales. Mothers who perceive their children to be more anxious may be more distressed by displays of anxiety and shyness and then engage in protective behavior to benefit their children in the future and decrease their own anxiety. Future studies that can measure these constructs in longitudinal assessments may be able to delineate temporal and mechanistic relations among them.
This study expanded on the validation of the APSA by examining a wider range of maternal anxiety scales. Maternal anxiety is sometimes, but not always linked to child anxiety, and this may be because maternal anxiety is indirectly, rather than directly, linked to child anxiety through parenting behaviors (Murray et al., 2012; Shamir-Essakow, Ungerer, & Rapee, 2005; Turner et al., 2003; Whaley et al., 1999). Study 2 contributes to this literature by providing evidence for the association between maternal anxiety and attitudes about these parenting behaviors. Having more positive attitudes about intrusive behavior related to the self-report measure of anxiety that focused more on physiological symptoms. This is consistent with a previous study demonstrating that cortisol reactivity was an important determinant of intrusive parenting (Kiel & Buss, 2013). Worry and social anxiety, on the other hand, related to more positive attitudes about protective behavior. Perhaps the more cognitive aspects of these types of anxiety play a larger role in motivating mothers toward protective parenting.
Study 2 also had limitations. Only mothers participated in this study, so we could not test whether mothers and fathers differed in the APSA scales, or whether correlations between APSA scales and other measures differed between mothers and fathers, to compare with Study 1. The sample was relatively homogenous in terms of racial and ethnic identity of participants. It also relied on parent-report measures; observation of parenting behavior would best address the potential role of social desirability in survey responses.
General Discussion
The extant literature has provided evidence that protective and intrusive parenting behaviors relate to child anxiety development, warranting the investigation of motivations for these behaviors. Although parenting attitudes have previously been assessed in relation to child anxiety spectrum behaviors and other aspects of parenting (e.g., competence, broadly), no measure previously existed for evaluating parents’ attitudes about protective and intrusive behaviors. This is particularly needed to contribute to the etiological understanding of anxiety and assist with parent-focused intervention efforts. Across two studies, we provided evidence for the factor structure, reliability, and validity of a new measure, APSA. This survey measures parents’ distress in relation to their children’s displays of anxiety-spectrum behavior and parents’ attitudes about the immediate benefits of protective behavior (e.g., for helping children cope), broad benefits of protective behavior (e.g., for future situations and parents’ own potential distress), and benefits of intrusive behavior.
Across both studies, the APSA scales demonstrated adequate internal consistency. In Study 2, we found moderate stability across 1 year. To further knowledge about the reliability of the APSA, it will be important for future studies to assess short-term test–retest reliability.
Our results expand the literature on parenting attitudes about child anxiety and parenting (e.g., Chen et al., 1998; Clarke et al., 2013; Cooklin et al., 2013) to suggest that more anxious parents, particularly those endorsing worry and social anxiety, may view protective behaviors more positively. Furthermore, these positive attitudes seem to be somewhat more specific to the broad benefits of protective behavior, including being effective in alleviating parents’ own distress and being an effective long-term strategy. The relation between parental anxiety and protective behavior is typically small to moderate in strength (van der Bruggen, Stams, & Bögels, 2008), suggesting that not all anxious parents are overprotective, and that overprotection may also be displayed by nonanxious parents. Perhaps more versus less anxious parents engage in protective behavior for different reasons, with more anxious parents engaging in protection to help themselves cope, and less anxious parents focusing on other situational factors or attitudes about child development. This may be essential knowledge for tailoring intervention strategies for anxious parents when engaged in treatment for their anxious children. If therapists merely tell parents to change their protective behavior, without addressing the fact that parents use these behavior to manage their own distress or have attitudes about their children’s future development, parents may feel uncomfortable and lack confidence to reduce protective behavior.
Parents who perceived higher benefits of intrusive parenting reported more physiological anxiety, embarrassment about and parent-centered goals for children’s shyness, encouragement of independence, and critical control of their children during expressions of shyness. Thus, parents who believe intrusive behaviors are generally effective for their children’s anxiety may be more negatively reactive to these displays and more likely to prioritize critical and approach-oriented solutions to getting their children to behave properly. This is consistent with previous findings of cortisol and subjective reactivity being related to observed intrusive behavior (Kiel & Buss, 2013). Future studies may expand on this work to understand how other physiological aspects of reactivity relate to these attitudes and subsequent intrusive behavior.
Across both studies, we found some evidence for specificity of attitudes about protective or intrusive behavior in relation to that particular behavior. Parents who perceived protective behavior to be more beneficial engaged in more protective behavior. Parents who believed intrusive behavior to be more beneficial engaged in more intrusive behavior or critical control. Cross-relations were generally not found. This seems to indicate that these attitudes have unique implications for parenting behavior and do not merely reflect opposite ends of a continuum.
Future directions may include more nuanced examinations of how attitudes about protective and intrusive behaviors predict the development of parenting and subsequent child anxiety-spectrum outcomes in longitudinal models that account for child-directed effects on parents. For example, attitudes about overcontrol may mediate or moderate relations between child and parent anxiety, on the one hand, and parent behavior, on the other (Figure 1). For example, parents’ perceptions of children’s early fearfulness may predict change in parent distress and attitudes about these parenting behaviors, and distress and attitudes may subsequently predict parenting behaviors. These attitudes may be addressed as targets for intervention. In particular, it seems that reducing perceived benefits of protective behavior in managing parents’ own distress, perhaps by providing other sources of coping, as well as providing psychoeducation to reduce perceived benefits for children’s future behavior and overall positive evaluation, could aid in reducing parent behaviors that might exacerbate child anxiety. Tracking change in these perceptions after interventions for child anxiety without addressing parent behaviors could also speak to child-directed effects. Experimental designs manipulating the level of anxiety the child putatively displays in the vignettes could also provide insight into the nature of these attitudes. Furthermore, there may be bidirectional effects between child shyness/anxiety and attitude about parenting that cascade over time to influence parenting behaviors. Using these types of sophisticated developmental models would be consistent with transactional models that provide a more contextualized understanding of behaviors that emerge within the parent–child relationship (Sameroff, 2009). Additional validation work may provide insight into whether all three vignettes are equally valid in assessing parenting attitudes. Finally, studying parents’ attitudes about parenting any child, not just their own children, might assist in gauging population-level perceptions of overprotection and intrusiveness.
Results should be considered in light of several limitations. Both samples offered only limited diversity in the racial/ethnic identities of parents. Given that parenting beliefs and the use and consequences of specific parenting behaviors differ across socioeconomic and cultural groups (Belsky & Jaffee, 2006; Chen et al., 1998; Hill & Bush, 2001), attitudes about these protective and intrusive behaviors may differ as well. It is possible that some parents interpret the vignette situations differently, and we were unable to account for these individual differences. Furthermore, only one of the two studies included fathers, who remain understudied in the parenting literature, and this study did not include parents from the same family. Being able to examine the attitudes of multiple caregivers (whether they be mothers, fathers, grandparents, etc.) representing a wider range of family compositions (e.g., opposite-sex and same-sex partners) would not only help clarify whether this measure is relevant to other parent systems but also indicate the impact of attitudes on parenting when they converge or diverge within a household. We also acknowledge that the APSA does not comprehensively assess motivations behind these parenting behaviors. It may be beneficial in the future to add items assessing social acceptability and expectations for children’s social interaction. Finally, expanding validation of the APSA to observed parenting behavior will be important. Social desirability may play a role in how parents report their own behavior, although previous studies have found convergence between parents’ self-reported and observed overcontrol (McShane & Hastings, 2009).
In sum, the APSA appears to offer a reliable and valid measure of parents’ attitudes about protective and intrusive behaviors, which are some of the most robust environmental predictors of child anxiety. Examining parents’ motivations for their responses to child anxiety-spectrum behaviors may contribute to understanding the development of these child outcomes and point to targets for parent-based intervention.
Footnotes
Appendix
Acknowledgements
We express our appreciation to Julie E. Premo and staff of the Behavior, Emotions, and Relationships Lab at Miami University for assistance with data collection, and to the families who participated in this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project from which these data were derived was supported, in part, by a grant from the National Institute of Child Health and Human Development (R15 HD076158-01) and funds from the Miami University College of Arts and Science, both to Elizabeth J. Kiel. During this project, Aaron M. Luebbe was supported by the Robert J. and Nancy H. Blayney Professorship. Portions of these results were reported at the 2015 meeting of the Association for Behavioral and Cognitive Therapies in Chicago, IL.