
Abstract
Several measures are available that assess inattention, hyperactivity/impulsivity, and executive functioning deficits. Treatments for adults with attention-deficit/hyperactivity disorder (ADHD) and skill-based academic interventions focus on improving compensatory strategies to ameliorate functional impairment; however, no measure exists that examines the compensatory behaviors adults utilize to compensate for the functional deficits associated with inattention and hyperactivity/impulsivity. The current study aimed to determine the psychometric properties of the Compensatory ADHD Behaviors Scale (CABS). Five-hundred participants (Mage = 36.83, SD = 11.57) completed measures of ADHD symptomatology, executive functioning, functional impairment, mood disorder symptoms, and the CABS. Analyses revealed that scales assessing both use and effectiveness of compensatory behaviors subscales had similar factor structures, reflecting present- and future-oriented behaviors. The present-, but not future-oriented, behaviors significantly related to ADHD symptomatology, executive dysfunction, and functional impairment; effectiveness of present-oriented compensatory behaviors demonstrated incremental validity in predicting impairment. Compensatory strategies may be a useful variable to measure when examining functional impairment associated with inattention and hyperactivity/impulsivity. The current study provides preliminary evidence of the ability of CABS to validly measure various strategies associated with (clinical and subclinical) ADHD symptomatology, executive functioning, and overall impairment.
Keywords
Children with attention-deficit/hyperactivity disorder (ADHD) continue to experience significant symptoms as adults (Barkley, Fischer, Smallish, & Fletcher, 2002; Rasmussen & Gillberg, 2000; Weiss & Hechtman, 1993). Although there is often some decline in inattention and hyperactivity/impulsivity symptoms over time, the functional impairment often remains into adulthood (Biederman, Mick, & Faraone, 2000; Rasmussen & Gillberg, 2000). ADHD symptoms are known to wax and wane throughout development (Hart et al. 1995; Larsson et al., 2011), with some evidence that they continue to vary into old age (Guldberg-Kjär, Sehlin, & Johansson, 2013). This heterogeneity likely contributes to the significant variation in the pattern and severity of the 18 symptoms (Nigg, Willcutt, Doyle, & Sonuga-Barke, 2005).
The heterogeneity in symptom distribution and severity led some researchers to suggest that ADHD symptoms operate across a spectrum (Barkley, 1998; Levy, Hay, McStephen, Wood, & Waldman, 1997; Tannock, 1999). Now, there is strong evidence that inattention and hyperactivity/impulsivity symptoms are a continuous trait, where ADHD is seen to be an extreme of this dimensional construct (Carragher et al., 2014; Marcus, Norris, & Coccaro, 2012). Studies utilizing various methodologies, as well as a number of important outcome variables, provide significant support for this notion. For instance, statistical modeling has repeatedly found that ADHD symptoms are on a severity continuum (Frazier, Youngstrom, & Naugle, 2007; Haslam et al., 2006; Jarrett, 2016; Lubke, Hudziak, Derks, van Bijsterveldt, & Boomsma, 2009). Moreover, a large, twin-study found that a diagnosis of ADHD is most accurately viewed as the measurable extreme of genetic and environmental factors working dimensionally throughout the ADHD symptom distribution (Larsson, Anckarsater, Råstam, Chang, & Lichtenstein, 2012). Personality research has also found differences between individuals with subthreshold ADHD and controls, providing further support for the dimensionality of ADHD (Faraone, Kunwar, Adamson, & Biederman, 2009). While disinhibition is theorized to be the core deficit in ADHD that subsequently disrupts other executive functioning processes (Barkley, 1997; see Lijffijt, Kenemans, Verbaten, & van Engeland, 2005, Cohen’s effect size, d = 0.58; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005, d = .4-.7, respectively), these deficits (measured through performance and self-report) are also associated with subclinical inattention and hyperactivity/impulsivity symptoms (Bidwell, Willcutt, DeFries, & Pennington, 2007; Brown & Casey, 2016; Faraone et al., 2006; Jarrett, 2016; Scahill et al., 1999).
Executive functioning deficits, and associated inattention and hyperactivity/impulsivity symptoms, negatively affect daily academic and social functioning (Faraone et al., 2006; Frazier et al., 2007; Hechtman et al., 2016; Overbey, Snell, & Callis, 2011). For instance, problems with time management, organization, and planning can represent inattention, distractibility, and impulsivity symptomatology. Difficulties managing time can facilitate procrastination, incomplete, and/or inaccurate work. As such, individuals with ADHD report greater psychological maladjustment, more driving risks (i.e., speeding tickets), more frequent changes in employment, multiple marriages, and a history of poor educational performance (Hechtman et al., 2016). These functional impairments are also associated with subthreshold inattention and hyperactivity/impulsivity symptoms in adults (Faraone et al., 2006; Frazier et al., 2007; Overbey et al., 2011).
Individuals with ADHD can engage in compensatory behaviors to ameliorate their impairment (Solanto, Marks, Mitchell, Wasserstein, Kofman, 2008). Given the impairment found in subclinical ADHD (Faraone et al., 2006; Frazier et al., 2007; Overbey et al., 2011), it follows that dimensional ADHD and executive functioning may also be related to use of compensatory behaviors. For instance, adults with clinical and subclinical ADHD may use to-do lists, calendars/planners, reminders, alarms, and various organizational systems as a means to decrease functional impairment (Solanto et al., 2008). Relatedly, they may complete tasks when they hear of them, organize items, and engage in checking behavior as to reduce forgetting, losing/misplacing items, and/or making careless mistakes. Both cognitive-behavioral therapy (CBT) for ADHD (Knouse, Teller, & Brooks, 2017) and organization, time management, and planning skills training teach nearly identical compensatory strategies (LaCount, Hartung, Shelton, & Stevens, 2015). Notably, there is now evidence that organization, time management, and planning improves inattention, hyperactivity/impulsivity, and academic impairment in college students with elevated ADHD symptoms (LaCount et al., 2015). Although impairment associated with clinical and subclinical ADHD can be improved through increasing compensatory behaviors, no scale exists to measure the use and effectiveness of compensatory behaviors that adults utilize in order to minimize the functional deficits associated with executive dysfunction, inattention, and hyperactivity/impulsivity.
Research has also found that individuals with subclinical ADHD show a similar treatment response (i.e., improved attention) to low-dose psychostimulants (Rapoport et al., 1980). Although popular, efficacious psychopharmacological treatments for ADHD (Elia, Borcherding, Rapoport, & Keysor, 1991; Michelson et al., 2003; Biederman, Spencer, & Wilens, 2004) have focused on symptom reduction only, with little attention paid to improvements in functional impairment. This led Solanto et al. (2008) to suggest that psychopharmacological treatment alone may not be sufficient to improve skill deficits that often facilitate functional impairment (e.g., time management, difficulties planning, disorganization, procrastination, incomplete or inaccurate work). Thus, psychosocial treatments have also been developed as a possible means to reduce functional impairment and symptom expression, with some success (Hesslinger et al., 2002; Knouse et al., 2017; Safren et al., 2005; Solanto et al., 2008; Solanto et al., 2010; Stevenson, Whitmont, Bornholt, Livesey, & Stevenson, 2002; Weinstein, 1994; Wilens et al., 1999).
There have been substantial gains in the development of effective psychosocial treatment for adults with ADHD (Knouse et al., 2017) and skill-based interventions for college students (LaCount et al., 2015). However, researchers, clinicians, and educators are forced to rely on measures of ADHD symptoms (e.g., Conners’ Adult ADHD Rating Scales; Conners, Erhardt, & Sparrow, 1999), executive functioning (e.g., Barkley Deficits in Executive Functioning Scale for Adults; Barkley, 2011), or functional impairment (e.g., Weiss Functional Impairment Rating Scales; Weiss, 2000) to assess treatment progress and outcome (Knouse et al., 2017). Relatedly, interventions targeting students’ occupational/academic skills (irrespective of ADHD symptomatology) do not have any standardized methods to assess the use of these skills. Although executive functioning self-report measures typically include items assessing difficulties with organizing/planning, time management, attention, impulsivity, behavioral inhibition, and emotion control/regulation, they do not assess whether an individual is utilizing compensatory strategies to help ameliorate functioning in these domains.
Despite evidence for the effectiveness of compensatory behaviors across the ADHD spectrum (LaCount et al., 2015; Safren et al., 2005; Solanto et al., 2008, 2010), the field does not currently have a way of measuring the use and effectiveness of compensatory strategies. With these goals in mind, the Compensatory ADHD Behaviors Scale (CABS) was designed to measure not only the use of compensatory behaviors (e.g., “I create lists to remind me of tasks I need to complete”) but also their effectiveness (e.g., “Using lists helps me complete the tasks I need to complete each day”). Hence, the CABS has the potential to assess whether the individual is reporting using the strategy and whether he/she is finding it helpful. The CABS has utility measuring treatment outcome/monitoring and functional impairment in adults undergoing CBT for ADHD and interventions targeting students’ organizational/academic skills. Additionally, it can serve subclinical ADHD populations who also have functional impairment and engage in inefficient compensatory strategies. Since the CABS was created to be diagnostically agnostic, the proposed measure has wide-ranging assessment implications, able to aid individuals with broad academic, occupational, and/or social impairment (e.g., LaCount et al., 2015), regardless of diagnosis or clinical significance.
Purpose and Hypotheses
The purpose of the current study is to report the development and initial validation of the CABS in a large, heterogeneous sample of adults. Given the ubiquity of the behaviors being measured, the CABS has utility beyond assessing ADHD treatment progress and outcome. Thus, the current study is the first step toward creating a measure with a wide range of uses, able to aid adults across the ADHD spectrum (i.e., clinical and nonclinical), college students, and the general population who experience occupational, family, and/or social functional impairment.
We first examine the factor structure and internal consistency of subscales derived from the CABS. To examine convergent and discriminant validity, we examine relationships of the CABS to ADHD symptoms and other clinical symptoms (i.e., depression, anxiety, obsessive-compulsive disorder [OCD]) with the hypothesis of stronger relationships between the CABS and ADHD symptoms. To further examine the validity of the CABS, we explored the relationship between CABS scores and self-reported executive functioning, where we hypothesize that the CABS and self-reported executive functioning are related but distinct. In addition, we posit that higher CABS scores would be associated with less functional impairment. We also examined the incremental validity of the CABS by examining whether compensatory behaviors significantly predict total functional impairment above and beyond that of ADHD symptomatology and executive dysfunction; we hypothesize that the CABS will explain variance in an individual’s functional impairment above and beyond that of ADHD symptomatology and executive dysfunction. We then examine the interaction between self-reported use and effectiveness of compensatory behaviors. Finally, we provide preliminary evidence of the CABS preliminary clinical utility by exploring group differences on CABS scores between individuals self-reporting a primary diagnosis of ADHD and those that did not.
Method
Scale Development
The items included on the CABS were derived from ADHD treatment manuals, clinical observations, and scales measuring impairment associated with ADHD (e.g., Safren et al., 2005; Solanto et al., 2008, 2010). First, domains were created that those with ADHD report having difficulties with (i.e., planning, forgetting, organization, time-management). These domains were chosen because CBT for adult ADHD typically focuses on these domains when teaching compensatory strategies (Solanto et al., 2008). In addition, executive functioning scale items, which relate to compensatory strategies as opposed to emotion regulation, typically cluster around these domains (e.g., Barkley Deficits in Executive Functioning Scale; Barkley, 2011). Next, the CABS use subscale was created utilizing the aforementioned resources within the domains. Following, the CABS effectiveness items were created by changing the language of the use subscale to reflect whether the compensatory behaviors have been helpful to the respondent. The instructions ask the rater to first assess the use of the strategies and then to assess the effectiveness of the same strategies. Participants rate the use and effectiveness, respectively, of a particular behavior as either 0 (not at all), 1 (a little bit), 2 (sometimes), 3 (quite a bit), and 4 (often). Total scores for the use and effectiveness scales, respectively, are a sum of all items.
Procedures
Participants were recruited via Amazon’s Mechanical Turk (MTurk; www.mturk.com; for an introduction to using MTurk, see Mason & Suri, 2012). MTurk is a website used to recruit participants to complete tasks in exchange for a specified payment (i.e., $1.50 in the current study). MTurk has been shown to provide data that have sound psychometric properties (Paolacci & Chandler, 2014), and demographic surveys demonstrate that MTurk workers are very similar to the national populations from which they are drawn (Paolacci, Chandler, & Ipeirotis, 2010). In addition, MTurk has been used in prior clinical and measure development studies (Shapiro, Chandler, & Mueller, 2013), as well as to define national norms of a common clinical measure (i.e., inventory of depression and anxiety symptoms; Nelson, O’Hara, & Watson, 2018). Researchers have demonstrated that data obtained by MTurk workers are similar to data collected from college undergraduates or community samples derived from college towns in domains such as political orientation (Berinsky, Huber, & Lenz, 2012), personality characteristics (Buhrmester, Kwang, & Gosling, 2011), and basic biases in decision making (Paolacci et al., 2010). The study was advertised as open to individuals over the age of 18 years who were fluent in English. In addition, participants had to have a high reliability rating on MTurk (>95%), which is established through published feedback from other data collectors. Those who chose to participate were directed to the online battery (i.e., qualtrics.com), where they could answer questions regarding their demographic information, mental health status, daily functioning, and typical behaviors.
Participants
Five-hundred participants were recruited using MTurk. Each subject completed a 376-question battery, composed of previously established measures and the CABS. Eligible participants had to be at least 18 years of age or older, be native English speakers, be U.S. residents, and have a satisfactorily completed at least 95% of their previous MTurk assignments. Given the length of the survey, two validity check questions were also included in the survey, although these were not mentioned in the survey description (Hauser & Schwarz, 2016). For these validity items, participants were asked to select a particular response (i.e., please select option “only a little bit” for this question) imbedded within a questionnaire. The two validity checks were imbedded within measures that were approximately one-half and three-fourths into the battery. Of the 500 responses, 8 participants failed the first validity check, and 11 failed the second validity check, whereas 3 participants failed both validity checks. Therefore, 16 participants were excluded from all analyses given concerns regarding the validity of their responding. These 16 participants did not significantly differ from the larger sample on any demographic information (p’s > .05). The final sample included 484 participants.
Participants who completed the battery in its entirety were predominantly female (n = 279) and had an average age of 36.83 years (SD = 11.57). Approximately 78.6% of our sample (n = 383) were Caucasian, 8.8% (n = 43) were African American or Black, 1.4% (n = 7) were American Indian or Alaska Native, and 4.5% (n = 22) were identified as other. Additionally, most participants identified as non-Hispanic or Latino 87.9% (n = 428). There was a diverse representation of educational backgrounds within this sample, with the majority of individuals reported having a 4-year college degree 38.8% (n = 189), followed by some college 13.4% (n = 27.5), a high school diploma 11.3% (n = 55), 2-year college degree 11.3% (n = 55), a master’s-level degree 7.6% (n = 37), and a doctorate-level degree 3.3% (n = 16). Last, 26.1% (n = 137) reported a current primary mental health diagnoses, and 34.3% (n = 167) reported being previously diagnosed. These disorders included a depressive disorder 19.3% (n = 94), anxiety disorder 20.9% (n = 102), attention-deficit disorder (ADD)/ADHD 6% (n = 31), OCD 3.9% (n = 19), a traumatic brain injury 1.4% (n = 2), or some other disorder (e.g., bipolar, posttraumatic stress disorder [PTSD], schizophrenia, etc.).
A number of participants endorsed more than one current mental health diagnosis (n = 72). Specifically, 13.4% self-reported comorbid depression and anxiety (n = 38); 1.0% reported comorbid depression, anxiety, and OCD (n = 5); 0.8% reported comorbid anxiety and ADHD (n = 4); 0.8% reported comorbid depression, anxiety, and PTSD (n = 4); 0.6% reported comorbid depression and ADHD (n = 3); 0.6% reported comorbid anxiety and OCD; and 0.6% reported comorbid anxiety, depression, and ADHD. All other comorbid diagnoses (n = 10) occurred in less than 0.5% of the sample. See Table 1.
Participant Demographic Information.
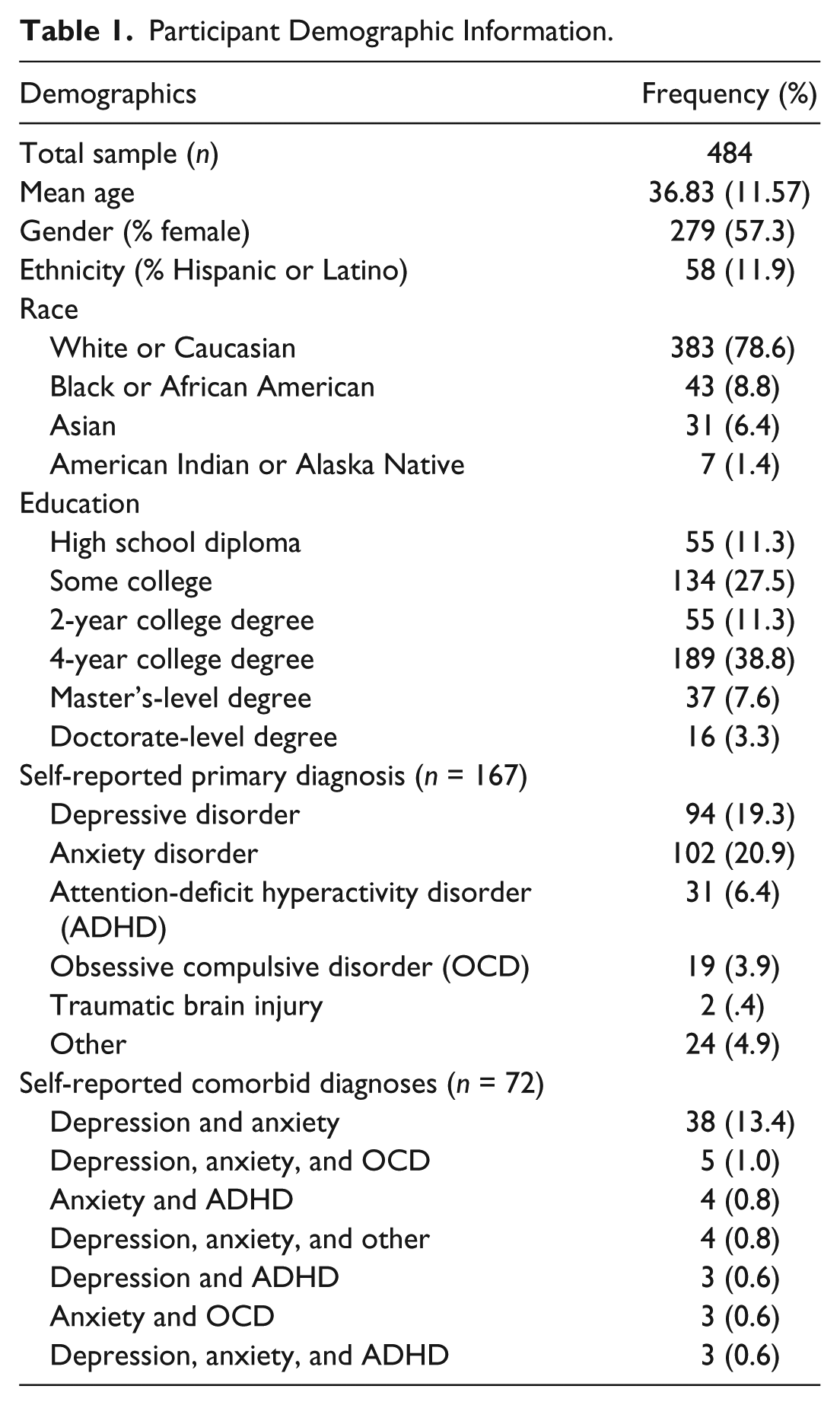
Within the sample of 484 participants, 31 adults reported having a diagnosis of ADHD (or ADD). ADD was included as some adults may not be familiar with changes in terminology. Of this subsample, 51.6% reported having only ADHD, whereas 48.4% reported ADHD and a comorbid diagnosis or comorbid diagnoses. Four participants reported comorbid ADHD and an anxiety disorder; three reported comorbid ADHD and a depressive disorder; three reported comorbid ADHD, anxiety, and depressive disorder; and three reported comorbid ADHD and OCD. The remaining two adults reported having comorbid anxiety, depression, ADHD, and OCD. The number of individuals who reported having a diagnosis of ADHD was 6.4%, which mirrors epidemiological studies of adult ADHD (i.e., 4% and 5% of the adult population; Faraone, Sergeant, Gillberg, Biederman, 2003; Kessler et al., 2006; Murphy & Barkley, 1996; Torralva, Gleichgerrcht, Lischinsky, Roca, & Manes, 2013; Wender, Wolf, Wasserstein, 2001).
Measures
Adult ADHD Self-Report Scale (ASRS)
The ASRS is an 18-item measure developed by the World Health Organization Composite International Diagnostic Interview (Kessler & Ustun, 2004). This measure contains questions that are consistent with DSM-IV criteria for ADHD and demonstrates a high internal consistency and concurrent validity (Adler, Spencer, & Faraone, 2006). This measure is typically divided into two parts. The first six items are commonly used as a screener for ADHD and demonstrates good consistency with clinical diagnoses, with an area of .90 under the receiver operating characteristic curve (Kessler et al., 2005). The remaining 12 items are often used to inquire about additional ADHD symptoms. Typically, each question contains shaded boxes, which are used to demonstrate symptom severity. However, for the purposes of our study, these boxes were removed in order to avoid any potential responses bias. The current study utilized the ASRS total score (α = .84).
Current Behaviors Scale (CBS)
The CBS (Barkley, 1997) is a 99-item measure used to assess executive functioning–related behaviors. Scores from this measure can be subdivided into six separate executive functioning categories: behavioral inhibition, sense of time, verbal working memory, emotion regulation, self-motivation, and planning. This measure has demonstrated good face validity for identifying executive functioning deficits within adult ADHD samples (Biederman et al., 2006). Coefficient alpha for subscales on the CBS ranged from .82 to .90, and the subscales were significantly associated with one another (r range = .48 to .52). The current study utilized the CBS total score.
The Obsessive-Compulsive Inventory–Short Version (OCI-R)
A brief version of the Obsessive-Compulsive Inventory, the OCI-R is used to assess symptom severity within those diagnosed with OCD. The OCI-R in current study had good internal consistency (α = .81). The 18 items within this measure demonstrate good internal consistency for five of the six subscales, including washing, checking, ordering, obsessing, and hoarding, and an adequate reliability for mental neutralizing (Huppert et al., 2007). The OCI-R also exhibits good test–retest reliability among a variety of clinical samples (i.e., OCD, generalized social phobia (social anxiety disorder), and PTSD) and good convergent validity with the OCI (Foa et al., 2002). Moreover, this measure is an effective tool for discriminating between patients and nonpatients with OCD, as well as for discerning between patients with OCD and those with other anxiety disorders (Foa et al., 2002).
Patient-Reported Outcomes Measurement Information System (PROMIS)-Anxiety and Depression-Short Forms
The PROMIS is a publically available set of measures used to better assess patient-reported outcomes (Cella et al., 2010). Constructing the PROMIS was a collaborative effort by the National Institutes of Health Roadmap for Medical Research Initiative. For the purposes of this study, we used short forms from two mental health subtests in order to assess symptoms of depression and anxiety. The items related to depression inquire about negative mood, decrease in positive affect, information-processing deficits, self-criticism, and negative social cognition, whereas items related to anxiety focus on fear, worry, hyperarousal, and somatic symptoms related to arousal. These measures have demonstrated good reliability and construct validity with the original instruments (Cella et al., 2010). In the current study, the PROMIS-anxiety and PROMIS-depression had acceptable internal consistency (α = .80, .87, respectively).
Weiss Functional Impairment Rating Scales (WFIRS)
The WFIRS (Weiss, 2000) is a measure used to identify and evaluate emotional and behavioral impairment among individuals with ADHD (Gibbins & Weiss, 2007). This 70-item questionnaire identifies seven individual domains of functioning: family relations, work adjustment, school performance, life skills, self-concept, social functioning, and risk-taking behaviors. This measure demonstrates robust psychometric properties, in relation to internal consistency and convergent validity. Additionally, the WFIRS exhibits discriminant validity between individuals with and without an ADHD diagnosis (Canu et al., 2016). Coefficient alpha for subscales on the WFIRS ranged from .90 to .97, and the subscales were significantly associated with one another (r range = .61 to .72). The current study utilized the WFIRS total score.
Statistical Analyses
Data from all participants that demonstrated valid responding (i.e., N = 484; see participants section of the methods for more information) were included in all analyses. Statistical software Mplus was used to compute the factor structure, and SPSS were used for all other data analyses.
Factor Analysis
Exploratory factor analysis (EFA) was used as a statistical data reduction technique to determine the underlying constructs that the CABS measures. We expected that the resulting factors would correlate and chose to utilize an oblique (Geomin) rotation. Parallel analysis (Horn, 1965) was used to determine the maximum number of factors to extract. This method compares obtained eigenvalues of a sample with those generated from random data sets, thereby providing the largest number of factors that should be considered (Humphreys & Montanelli, 1975).
Internal Consistency
We calculated internal consistency using Cronbach’s alpha (α) based on the average correlation of items within a scale and total number of items (Cronbach, 1951). Although suggested values for adequacy vary in the literature, and are dependent on expected characteristics of the measure, one often-used minimum value of internal consistency is .65 (Zhang, Faries, Vowles, & Michelson, 2005).
Normality
The distribution of scores on the CABS within a population plays a role in a measure’s discriminatory power. Scores on the CABS should approximately reflect a normal distribution, as indicated by skewness and kurtosis values. The spread of scores should be on a continuum, where few individuals score at the highest (i.e., ceiling) or lowest (i.e., floor) end of the distribution.
Associations With ADHD Symptoms, Executive Functioning, and Impairment
The relationship among compensatory behaviors related to ADHD, ADHD symptomatology, executive functioning, and functional impairment was determined by calculating Pearson’s correlation coefficients between the CABS subscales, ASRS total score, CBS total score, and WFIRS total score. These analyses were chosen to demonstrate the CABS concurrent validity.
Associations With OCD, Anxiety, and Depressive Symptoms
Pearson’s correlation coefficients among the CABS subscales and OCI-R, PROMIS-depression, and PROMIS-anxiety were calculated to determine whether compensatory behaviors relate to disorders that are commonly comorbid with ADHD. These analyses were chosen to demonstrate the CABS discriminant validity. Follow-up partial correlations were calculated to examine the aforementioned relationships while ADHD symptomatology is held constant.
Incremental Validity
Incremental validity was determined by examining whether compensatory behaviors significantly predict total functional impairment above and beyond that of ADHD symptomatology (i.e., total scores on the ASRS) and executive dysfunction (i.e., total scores on the CBS). These analyses were conducted to provide evidence of the CABS incremental validity. Following, we provide evidence for the validity of both sections of the CABS (i.e., use and effectiveness) by predicting functional impairment through the interaction between the use and effectiveness sections for the present- and future-oriented subscales, respectively.
Preliminary Clinical Utility
Preliminary evidence for the CABS clinical utility was examined by first confirming adults reporting a diagnosis of ADHD reported significant differences on ADHD symptomatology (i.e., total scores on the ASRS), executive dysfunction (i.e., total scores on the CBS), and total impairment (i.e., total score on thee WFIRS); second, we explored whether this subsample significantly differs from the larger sample in their reporting on the CABS. Finally, we examined whether the use and effectiveness of compensatory behaviors (respectively) interact with executive dysfunction, to predict self-reported impairment (i.e., total score on the WFIRS) in adults self-reporting a diagnosis of ADHD.
Results
Item Analyses
No direct-keyed items had overly high endorsement (i.e., mean greater than 4), nor did any items display excessively low endorsement (i.e., mean less than 2). Two items had a high correlation (r = .75); however, the items were retained for factor analysis, as they may not load on the same scale for either the use or effectiveness domains (Gerbing & Anderson, 1988). No other item correlations exceeded .60. Therefore, all items were retained from the preliminary item pool prior to factor analysis.
Factor Analysis
Factor analysis of data resulted in a two-factor solution for both the use of ADHD compensatory behaviors and their effectiveness, confirming that the scale can accurately assess ADHD compensatory behavior use and effectiveness in a parallel manner. The first three eigenvalues in the solution for the use of ADHD compensatory behaviors were 5.92, 1.74, and 1.22. The first three eigenvalues in the parallel analysis were 1.31, 1.24, and 1.19, suggesting that we could extract two factors for the CABS scale assessing the use of ADHD compensatory behaviors. One item (i.e., “Creating budgets helps me manage my money/bank accounts”) was eliminated due to low loading (i.e., <.40); the item “I create lists to remind myself to tasks I need to complete” was eliminated due to high interitem correlation; two items were removed due to cross-loading (i.e., loadings greater than .40 on one factor and greater than .30 on the other factor). Therefore, the final CABS use and effectiveness sections contained 11 and 13 items, respectively.
The first factor, which relates to the use of ADHD compensatory behaviors that are present-oriented, includes five items (e.g., “I often complete tasks as soon as possible so that I do not forget to do them” and “I keep things organized so I do not forget where I placed them”). The first three eigenvalues in the solution for the effectiveness of ADHD compensatory behaviors were 6.43, 1.61, and 1.11. The first three eigenvalues in the parallel analysis were 1.31, 1.24, and 1.19, suggesting that we could extract two factors for the CABS scale assessing the effectiveness of ADHD compensatory behaviors used. This scale’s factor structure directly parallels the use of ADHD compensatory behaviors section, where the first factor contains six items that are present-oriented (e.g., “Completing tasks as soon as possible helps me avoid forgetting to do them later” and “Keeping things organized helps me avoid forgetting where I place them”), and seven items that reflect future-oriented compensatory ADHD behaviors (e.g., “I create lists to remind myself to tasks I need to complete” and “Checking things helps me avoid making mistakes”). Tables 2 and 3 provide the items in each subscale, for each section (i.e., use and effectiveness), and the factor loadings from the analyses.
Rotated Factor Loadings of the Use of ADHD Compensatory Behaviors Scale.
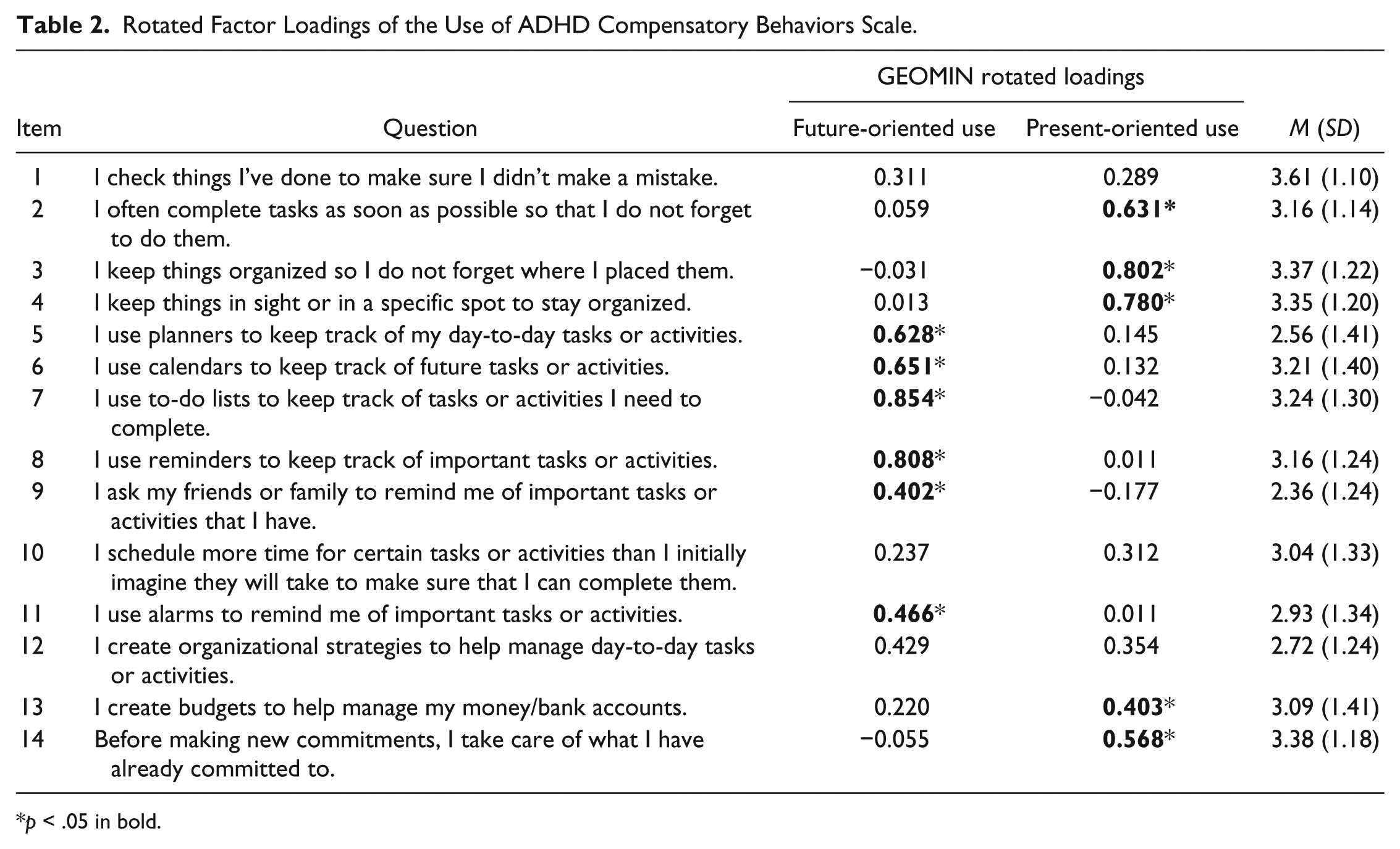
p < .05 in bold.
Rotated Factor Loadings of the Effectiveness of ADHD Compensatory Behaviors Scale.
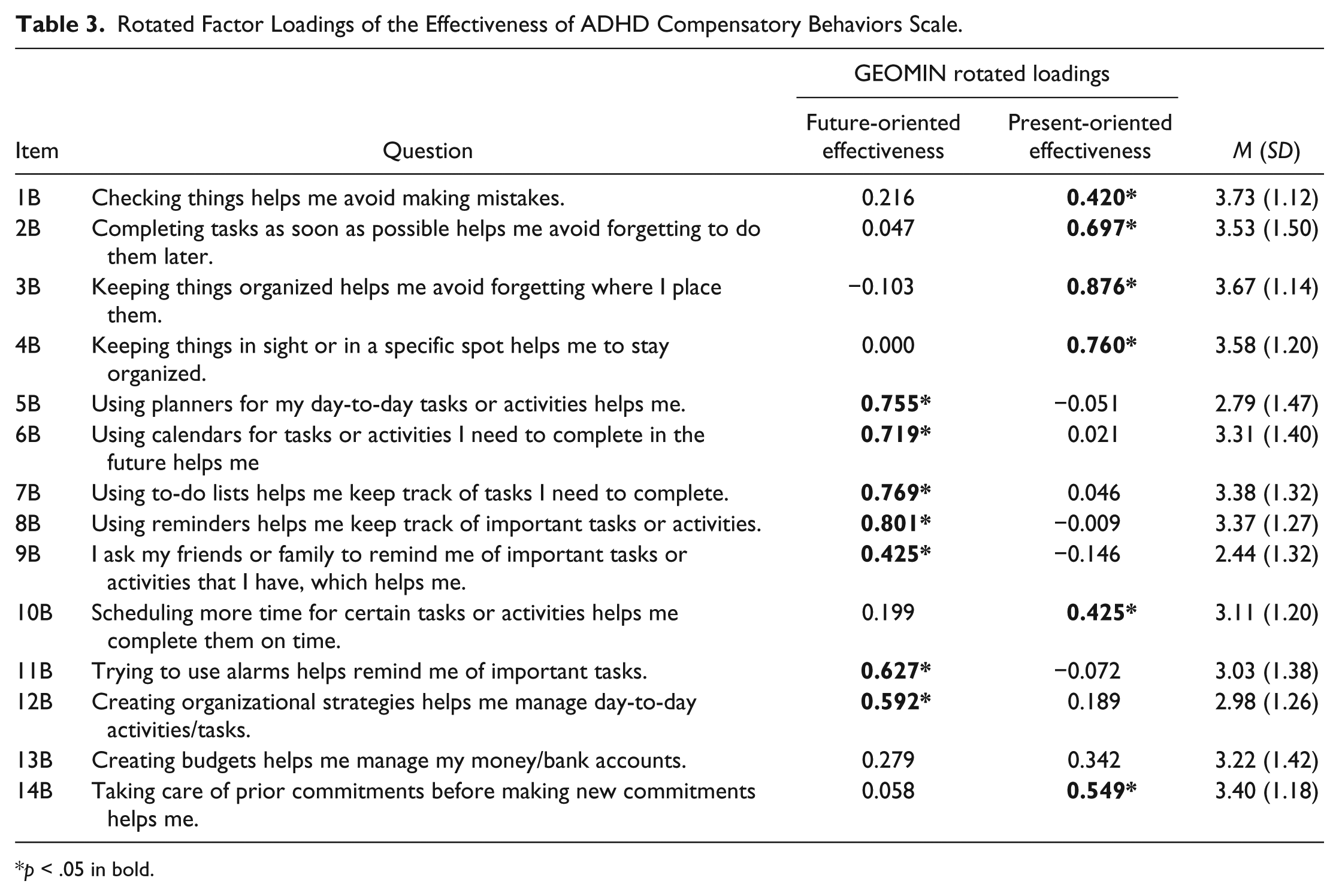
p < .05 in bold.
Internal Consistency
Using the factor structure previously described, the Cronbach’s α of the use of present-oriented compensatory ADHD behaviors was .81, whereas the use of future-oriented compensatory ADHD behaviors was .84. In terms of the effectiveness of present- and future-oriented compensatory ADHD behaviors, the Cronbach’s α was .84 and .87, respectively.
Normality
The distribution of scores across the CABS sections (i.e., use and effectives) and subscales determined through the EFA were examined. We inspected skewness and kurtosis values as well as scores that fell in the 1st percentile and 99th percentile for each subscale. The CABS use present-oriented (G = −.6, SD = .10), use future-oriented (G = −02, SD = .11), effectiveness presented-oriented (G = −.36, SD = .10), and effectiveness future-oriented (G = −.08, SD = .11) demonstrated skewness values well within the acceptable range. Similarly, the kurtosis values of the CABS use present-oriented (g2 = −.57, SD = .10), use future-oriented (g2 = −.66, SD = .11), effectiveness presented-oriented (g2 = −.11, SD = .10), and effectiveness future-oriented (g2 = −.67, SD = .11) also provided evidence of normal distribution of the CABS. Furthermore, the scores at the 1st, 50th, and 99th percentile demonstrated similar distributions across subscales, with a mean score of 6.5 (1st percentile), 20.25 (50th percentile), and 32 (99th percentile).
Convergent Validity: Associations With ADHD Symptoms and Executive Functioning
To explore the relationship among CABS subscales, ADHD symptoms, and executive functioning, Pearson’s correlation coefficients among the CABS subscales, ASRS total score, and CBS total score were calculated (see Table 4). Utilizing the aforementioned factor structure, the CABS present-oriented use subscale demonstrated significant negative correlations with the ASRS total score (r = −.25, p < .001) and CBS total score (r = −.30, p < .001). Similarly, The CABS present-oriented effectiveness subscale demonstrated significant negative correlations with the ASRS total score (r = −.09, p < .05) and CBS total score (r = −.18, p < .01); greater ADHD symptoms and executive dysfunction were associated with less use and effectiveness of presented-oriented compensatory strategies. The CABS future-oriented use and effectiveness subscales were not significantly related to the ASRS total score (r = .08, p > .05; r = .06, p > .05, respectively) or the CBS total score (r = .04, p > .05; r = .03, p > .05, respectively).
Pearson’s Correlation Table.
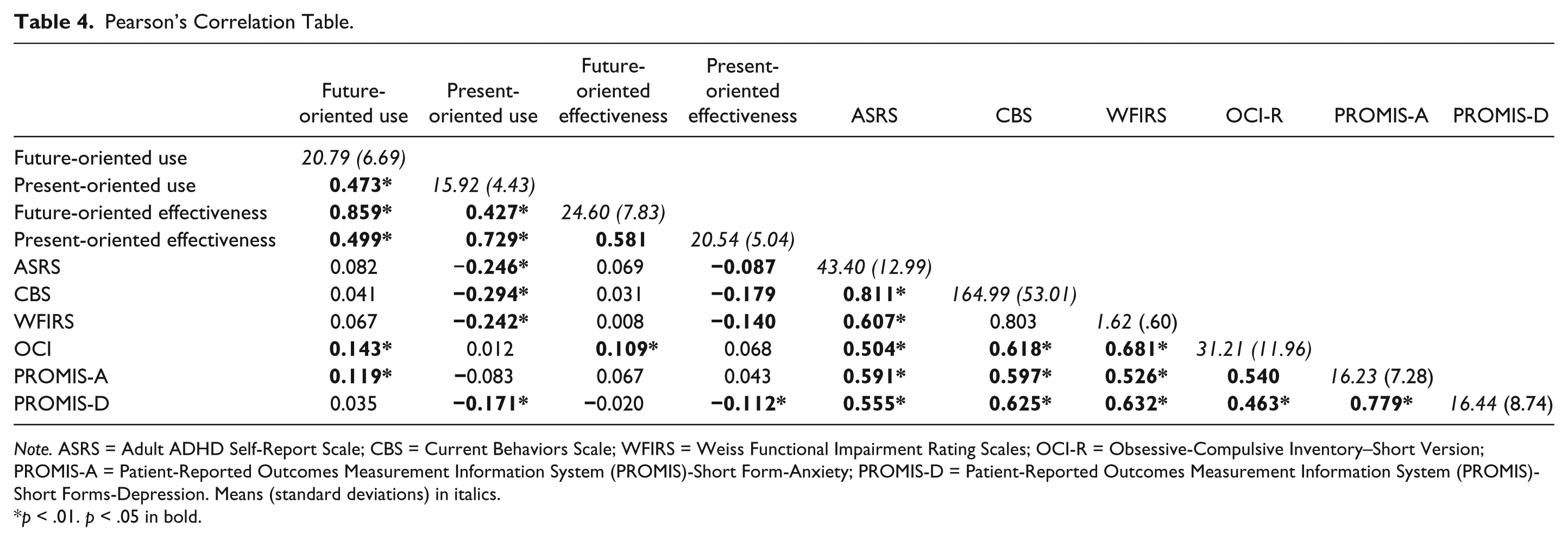
Note. ASRS = Adult ADHD Self-Report Scale; CBS = Current Behaviors Scale; WFIRS = Weiss Functional Impairment Rating Scales; OCI-R = Obsessive-Compulsive Inventory–Short Version; PROMIS-A = Patient-Reported Outcomes Measurement Information System (PROMIS)-Short Form-Anxiety; PROMIS-D = Patient-Reported Outcomes Measurement Information System (PROMIS)-Short Forms-Depression. Means (standard deviations) in italics.
p < .01. p < .05 in bold.
Convergent Validity: Associations With Impairment
To explore the relationship among CABS subscales and impairment, Pearson’s correlation coefficients among the CABS subscales and WFIRS total score were calculated (see Table 4). The CABS present-oriented use subscale demonstrated a significant correlation with the WFIRS total score (r = −.24, p < .001). The CABS present-oriented effectiveness subscale also significantly correlated with the WFIRS total score (r = −.14, p < .01). Greater functional impairment was associated with less use and effectiveness of presented-oriented compensatory strategies. The CABS future-oriented use and effectiveness subscales were not significantly related to the WFIRS total score (r = .06, p > .05; r = .01, p > .05). Overall, greater functional impairment was associated with less use and effectiveness of presented-oriented compensatory strategies.
Discriminant Validity: Associations With OCD, Anxiety, and Depressive Symptoms
We also examined Pearson’s correlation coefficients of the CABS and OCI-R, PROMIS-depression, and PROMIS-anxiety. The CABS present-oriented use and effectiveness subscales were not significantly related to the OCI-R or the PROMIS-anxiety total score but did significantly correlate with the PROMIS-depression total score (r = −.17, p < .05; r = −.11, p < .05, respectively); demonstrating more depressive symptomatology was associated with less use and effectiveness of presented-oriented compensatory strategies.
In contrast, the CABS future-oriented use subscale was significantly related to the OCI-R and PROMIS-anxiety total score (r = .14, p < .05; r = .12, p < .05, respectively) but not the PROMIS-depression total score. The CABS future-oriented effectiveness subscale was significantly correlated with the OCI-R (r = .10, p < .05) but not the PROMIS-depression nor the PROMIS-anxiety. In sum, OCD and anxiety symptomatology was linked to more use of future-oriented compensatory strategies, but only the effectiveness of the future-oriented compensatory strategies was only related to OCD symptomatology.
Given the high comorbidity between ADHD and depression in adults (Katz, Wood, Goldstein, Auchenbach, & Geckle, 1998), follow-up partial correlations were calculated between the CABS present-oriented use, effectiveness subscales and the PROMIS-depression. Results indicated that when controlling for individuals’ ADHD symptomatology (i.e., ASRS), there was no relationship between the CABS present-oriented subscale (r = −.06, p > .05) use or the present-oriented effectiveness subscale (r = −.05, p > .05). In contrast, the relationships between the CABS present-oriented use, effectiveness subscales and the ASRS total score was robust to the effects of controlling for depressive symptomatology (r = −.20, p < .05; r = −.10, p < .05).
In parallel, the CABS future-oriented use subscale was significantly related to the OCI-R and PROMIS-anxiety total scores (but not the PROMIS-depression total score); the CABS future-oriented effectiveness subscale was significantly correlated with the OCI-R (but not the PROMIS-depression nor the PROMIS-anxiety). Follow-up partial correlations were calculated between the CABS future-oriented use and OCI-R and PROMIS-anxiety total scores, and the effectiveness subscale and the OCI-R total score, while controlling for ADHD symptomatology (i.e., ASRS total score). Results indicated that CABS future-oriented use scale still significantly correlated with OCD symptoms (r = .11, p < .05), but not anxiety symptoms (r = .08, p > .05). Controlling for ADHD symptoms, OCD symptomatology no longer significantly correlated with the CABS future-oriented effectiveness subscale (r = .07, p > .05).
Incremental Validity
We examined the incremental validity of the CABS by examining whether compensatory behaviors explain variance within functional impairment (i.e., WFIRS total score) beyond that of ADHD symptomatology (i.e., ASRS total score) and executive dysfunction (i.e., CBS total score). Within a hierarchical multiple regression predicting WFIRS total score, the first step included the ASRS and CBS total scores, the second step included use of present-oriented and use of future-oriented compensatory behaviors, and the third step composed of the effectiveness of present- and future-oriented compensatory behaviors.
The overall model was significant at the first step, F(1, 463) = 163.68, p < .0001, adjusted R2 = .26, where ASRS and, β = .51, t(485) = 12.79, p < .001, CBS total score, β = .79, t(485) = 13.87, p < .001, significantly predicted WFIRS total score. The second step did not significantly contribute to the model, ΔF(2, 463) = 1.26, p > .05; ΔR2 = .003, with both use of present- and future-oriented compensatory behaviors not significantly contributing to the model. The final step significantly contributed to the overall model, ΔF(6, 463) = 3.98, p < .05; ΔR2 = .01, adjusted R2 = .48, with the effectiveness of present-oriented, but not future-oriented, compensatory behaviors significantly predicting functional impairment, β = −.15, t(485) = −2.65, p < .05. These results suggest that the effectiveness, but not the use, of present-oriented compensatory behaviors predict functional impairment above and beyond that of ADHD symptomatology and executive dysfunction.
Next, we included an additional step within the model that included the interaction between use and effectiveness sections. Results indicated that the final step significantly contributed to the model, ΔF(2, 463) = 108.09, p < .0001, ΔR2 = .05, where the future-oriented use of compensatory behaviors significantly interacted with the effectiveness of the future-oriented compensatory behaviors to predict adults’ functional impairment, β = −.09, t(485) = −2.00, p < .05. In contrast, the interaction between present-oriented use and present-oriented effectiveness did not significantly predict adults’ functional impairment, β = −.08, t(485) = −1.36, p > .05. In sum, the results suggest that the use of future-oriented compensatory behaviors only predict functional impairment when the individual also reported that these future-oriented behaviors are effective.
Preliminary Clinical Utility
Finally, we looked to provide preliminary evidence for the CABS clinical utility by first confirming that adults who reported a diagnosis of ADHD reported significant differences on ADHD symptomatology (i.e., total scores on the ASRS), executive dysfunction (i.e., total scores on the CBS), and total impairment (i.e., total score on the WFIRS). Following, we explored whether this subsample significantly differs from the larger sample in their reporting on the CABS. Finally, we examine whether differences in executive functioning within adults with ADHD are associated with variations in the self-reported use and effectiveness of compensatory behaviors, which predict functional impairment.
The sample of 31 adults reporting a diagnosis of ADHD had a significantly greater mean ASRS total score, t(73) = 7.20, p < .01, CBS total score, t(73) = 7.74, p < .01, and WFIRS total score, t(73) = 4.87, p < .01, when compared with a random sampling of 45 adults from the larger sample of 484 individuals. Moreover, they also reported using more future-oriented compensatory behaviors, t(72) = 3.59, p < .01, despite reporting that they are less effective, t(72) = −2.20, p < .05. They reported using more present-oriented compensatory behaviors, t(72) = −2.94, p < .01, but did not differ from the random sample on their reporting of the effectiveness of present-oriented compensatory strategies, t(72) = 1.42, p > .05 (see Table 5). These results provide corroborative evidence that the sample of 31 participants are validly reporting having an ADHD diagnosis.
Means and Standard Deviations of Study Measures Between Individuals Self-Reporting an ADHD Diagnosis Versus Individuals Not Self-Reporting a Diagnosis of ADHD (N = 76).
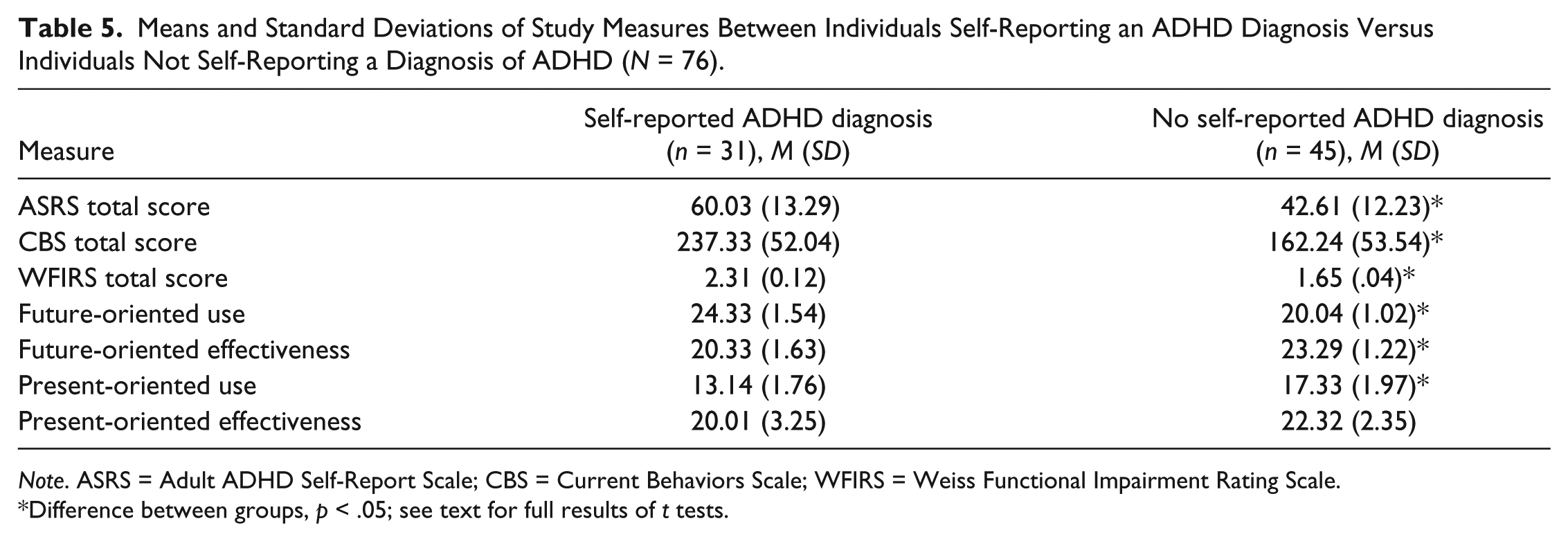
Note. ASRS = Adult ADHD Self-Report Scale; CBS = Current Behaviors Scale; WFIRS = Weiss Functional Impairment Rating Scale.
Difference between groups, p < .05; see text for full results of t tests.
The following analyses explore whether variations in adult executive functioning are differentially related to the use and effectiveness (respectively) of compensatory behaviors when predicting impairment. Within a hierarchical multiple regression predicting impairment, the first step included the executive dysfunction and present- and future-oriented effectiveness subscales; the final step included the interaction between executive dysfunction and the effectiveness of present-oriented compensatory behaviors, as well as the interaction between executive dysfunction and the effectiveness of future-oriented compensatory behaviors.
When predicting functional impairment, F(3, 27) = 13.19, p < .0001, adjusted R2 = .55; executive dysfunction, β = .80, t(30) = 6.05, p < .001; and the interaction between executive dysfunction and the use of future-oriented compensatory behaviors, β = −.39, t(30) = 2.06, p < .05, were significant, ΔF(2, 25) = 9.02, p < .05; ΔR2 = .17, adjusted R2 = .72. The interaction was robust to the effects of executive dysfunction alone, β = .98, t(30) = 8.57, p < .0001, within the third step. The independent contribution of the use of future-oriented compensatory behaviors also significantly contributed to the model, β = −.32, t(30) = −2.60, p < .05. The overall pattern of results indicated that, in adults reporting an ADHD diagnosis, those with elevated levels of executive dysfunction, who use less future-oriented compensatory behaviors, reported more impairment (compared with those using more future-oriented compensatory behaviors). Moreover, the use of future-oriented compensatory behaviors, especially in adults reporting higher executive functioning, predicted less impairment in a sample of adults reporting an ADHD diagnosis.
The model was significant, F(3, 27) = 13.59, p < .0001, adjusted R2 = .74, where executive dysfunction, β = .82, t(30) = 6.23, p < .001, and the interaction between executive dysfunction and the effectiveness of future-oriented compensatory behaviors, β = −.46, t(30) = 3.39, p < .01, significantly predicted impairment, ΔF(2, 25) = 10.03, p < .05; ΔR2 = .17, adjusted R2 = .72. Again, the interaction was robust to the effects of executive dysfunction, β = .99, t(30) = 9.12, p < .0001, and the independent contribution of the effectiveness of future-oriented compensatory behaviors was also significant, β = −.37, t(30) = −2.16, p < .05.
In sum, the pattern of results indicated that, in individuals reporting an ADHD diagnosis, those with elevated levels of executive dysfunction, who endorsed noneffective future-oriented compensatory behaviors, reported more impairment (compared with those reporting effective future-oriented compensatory behaviors). Moreover, the effectiveness of future-oriented compensatory behaviors, regardless of executive functioning level, also predicted less impairment in a sample of adults reporting an ADHD diagnosis.
Discussion
The current study aimed to establish the reliability, validity, and factor structure of a measure to assess adults’ use, and the effectiveness, of compensatory behaviors related to executive functioning deficits that can be found in those with ADHD. Empirically supported CBT for adults with ADHD (Safren et al., 2005; Solanto et al., 2008; Solanto et al., 2010) focuses on teaching and developing compensatory behaviors to help eliminate maladaptive strategies often associated with functional impairment (e.g., time management, organizational, and planning skills). However, the assessment of ADHD symptoms or executive functioning deficits to gauge skill-based treatment progress can be problematic. The purpose of developing the CABS was to fill this critical void by providing a reliable and valid measure of ADHD-related compensatory behaviors in order to guide treatment progress and further the research on strategies adults with ADHD can use to ameliorate symptoms associated with functional impairment.
The EFA indicated two factors on both the use of compensatory ADHD behaviors and the effectiveness of compensatory ADHD behaviors subscales: compensatory behaviors that aid in functioning in the moment (i.e., present-oriented use and present-oriented effectiveness) and compensatory behaviors that aid in skill deficits related to keeping track of future events and/or activates (i.e., future-oriented use and future-oriented effectiveness).
Compensatory ADHD Behaviors, ADHD Symptomatology, Executive Functioning Deficits, and Functional ADHD-Related Impairment
With regard to our hypotheses, the CABS demonstrated adequate to good internal consistency and normally distributed scores across all subscales. Furthermore, we found partial support for our first set of hypotheses; the CABS present-oriented use and effectiveness subscales demonstrated significant negative correlations with the ADHD symptomatology and executive functioning deficits, whereas the CABS future-oriented use and effectiveness subscales were not significantly related to the ADHD symptomatology or executive functioning deficits. Our second hypothesis (i.e., more compensatory behaviors would be related to less impairment) was partially supported. Again, the CABS present-oriented use and effectiveness subscales demonstrated a significant correlation with total functional impairment. In contrast, the CABS future-oriented use and effectiveness subscales were not significantly related to the total functional impairment.
Overall, these results revealed a consistent pattern: Present-oriented, but not future-oriented, compensatory behaviors were more associated with ADHD symptoms, executive functioning deficits, and total functional ADHD-related impairment. There are several of plausible explanations. First, the present-oriented compensatory behaviors may be more common in individuals with ADHD, thus, also relating to executive functioning deficits and total functional impairment; however, our preliminary clinical utility analysis does not support this conclusion. Although a small sample with self-reported ADHD diagnoses, this diagnostic group reported using more, less effective future-oriented, but fewer present-oriented, compensatory behaviors. Given their preliminary nature, however, these results should be interpreted with caution. Alternatively, the future-oriented items include behaviors that are generally viewed as being positive behaviors to engage in (e.g., I use planners to keep track of my day-to-day tasks or activities,” and “I use to-do lists to keep track of tasks or activities I need to complete). Individuals may be more likely to endorse using these strategies to be viewed favorably or because they know that they “should” be using them. Moreover, individuals may be also more likely to endorse that they are effective simply because it is well known that these strategies are helpful and possibly to resolve any cognitive dissonance (e.g., “these strategies must be effective if I am using them”); though the latter could be said about the present-oriented effectiveness subscale. Taken together, these results would countervail and lead to no relationship between ADHD symptoms and future-oriented compensatory behaviors. Finally, these findings may reflect differences in relationships among variables collected from a community sample versus a clinical sample of adults with ADHD. In sum, future research will be needed to better understand our finding that present-oriented compensatory behaviors are more related to ADHD symptomatology, executive functioning deficits, and total functional ADHD-related impairment within a community sample. In addition, future studies should aim to determine if a similar pattern of results is found in clinical sample of adults with ADHD.
Compensatory ADHD Behaviors, Obsessive-Compulsive, Anxious, and Depressive Symptomatology
We also explored the relationship between the CABS and disorders commonly comorbid with ADHD (i.e., anxiety, depression, and OCD symptomatology). Overall, these findings provide evidence for the validity of the CABS as a measure of compensatory behaviors that relate to ADHD. It was expected that because the CABS items are diagnostically agnostic, they would relate to OCD and anxious symptomatology, given the overlap between these compensatory behaviors and some symptoms of OCD and anxiety disorders (e.g., generalized anxiety disorder). It was also expected to be negatively related to depressive symptomatology, given their relationship to executive functioning deficits. However, our results provide evidence that these compensatory behaviors are more related to ADHD symptoms; nearly all of these associations (c.f., CABS future-oriented use scale and OCD symptoms) were no longer significant when controlling for their association to ADHD symptomatology, whereas the association between compensatory behaviors and ADHD symptomatology was still significant when controlling for depression, OCD, and anxiety symptomatology. Alternatively, however, these findings could be related to executive functioning deficits rather than ADHD, as we did not run partial correlations with self-reported executive functioning as a covariate.
Incremental Validity of Compensatory ADHD Behaviors
The CABS present-oriented effectiveness subscale significantly predicted functional impairment above and beyond that of ADHD symptomatology, executive function, and use of present-oriented and future-oriented compensatory behaviors. In contrast to our hypothesis, none of the other CABS subscales significantly contributed to the model. These results suggest that the effectiveness of the present-oriented compensatory behaviors is useful in understanding and individuals’ impairment. Moreover, these results provide support for the validity of the effectiveness subscales, as well as their clinical utility. Where the use of compensatory behaviors can be useful to a clinician in understanding whether certain compensatory strategies are being used day-to-day, the effectiveness subscales may be useful to a clinician better understanding whether these strategies are helping to reduce an individual’s functional impairment.
CBT is recognized as one of the most promising psychosocial treatments for adults with ADHD (Ramsay, 2017). The modified approach of CBT personalizes patient treatment by both identifying and mitigating avoidant behaviors commonly used by those with executive dysfunction (Ramsay, 2017). While current treatment measures assess levels of executive functioning, symptom impairment, and overall quality of life (Ramsay, 2017), none appear to measure the effectiveness of the compensatory behaviors used by their patients. These findings suggest that the CABS may improve progress monitoring and goal setting by providing a deeper understanding for the inconsistencies found between the effectiveness of certain empirically based strategies and a patient’s reported symptom severity. Understanding these limitations may lead to more effective, personalized treatments for individuals with varying levels of symptom severity.
Subscale Validation
The use of compensatory behaviors interacted with how effective these strategies were rated to predict functional impairment. Importantly, this was only found for the future-oriented domain. This was somewhat surprising because the future-oriented domains (i.e., use and effectiveness) were not independently related to functional impairment. It may be hypothesized that future-oriented compensatory strategies are related to impairment only when they are also reported to be ineffective. However, since this finding was in a convenience sample, it should be interpreted with caution and may not reflect the relationships among these variables in a clinical sample.
Clinical Utility of the CABS
We provide preliminary evidence that the CABS may have clinical utility. Given the nature of these analyses, however, the results should be interpreted with caution. The sample is small (n = 72) and composed of 31 adults who self-reported a primary diagnosis of ADHD. Although the diagnosis was corroborated by their scores on well-validated measures of ADHD symptomatology, executive functioning, and functional impairment, their self-reported diagnoses could not be confirmed. Exploratory results indicated that individuals with ADHD report using more future-oriented compensatory behaviors but reported that they are significantly less effective (when compared with a control sample). In addition, this diagnostic group reported using less present-oriented compensatory strategies but did not differ from the control group on their reported effectiveness. Taken together, these results are in line with the independent relationships among study variables, and they indicated that there may be a differential relationship between present- and future-oriented compensatory strategies in a sample of adults with ADHD, where they report using more future-oriented, but less present-oriented, compensatory strategies.
Limitations and Strengths
Although this study utilized a large, diverse sample of adults to analyze the reliability of this measure, the same sample may have some limitations. First, the anonymity of the MTurk workers leaves researchers vulnerable to the potential of repeat responders. While this study utilized certain safeguards to identify authentic responses (e.g., validity checks, inclusion criteria, etc.), it is difficult to account for individuals who have created multiple accounts. Previous articles have suggested that Amazon may regulate the number of accounts provided to an individual user (Rand, 2012), but this does not eradicate the notion that some workers may have been able to work around the system (Holden, Dennie, & Hicks, 2013). Additionally, the financial benefits of completing multiple surveys quickly may incentivize dishonest participation. Finally, although the current study is the first to report the development and initial validation of the CABS, our sample allowed only for an exploratory, not a confirmatory, factor analysis to be completed. Future research should look to confirm this factor structure in a separate community, as well as a clinical, sample.
The generalizability of the sample may also limit the findings of this study. Specifically, our sample was not restricted to a clinical population. Although many participants endorsed a history of mental health concerns, participants were not excluded if they denied having ever received a formal psychological diagnosis. Additionally, the sample was predominantly female (i.e., 57%). The implication of this gender ratio for a measure of behaviors associated with a male-dominated disorder (i.e., ADHD) is a limitation of the current study. Since the CABS was originally designed as a clinical measure, future studies should utilize participants with formal mental health diagnoses in order to further assess how well items discriminate across disorders.
The current study had a number of strengths as well. The sample was large, composed of individuals from a wide age range from across the United States, as well as participants from heterogeneous racial and educational backgrounds. In addition, a number of validity checks were incorporated to ensure the validity of the responses. The use of MTurk has been shown to be useful in initial scale development (e.g., Knouse, Mitchell, Kimbrel, & Anastopoulos, 2017).
Future Directions
Enhancing the internal and external validity of a newly developed measure is both a necessary and continuous process. Future studies may benefit from comparing specific clinical populations with individuals with formal ADHD diagnoses, in order to establish a more homogeneous response group. Given the prevalence of ADHD among adolescents, future studies may also benefit from adapting a version of the CABS into an adolescent measure. CBT for adolescents with ADHD seeks to mitigate clinical symptoms by improving both self-control and problem-solving techniques (Abikoff, 1985). However, it has been suggested that in order to maximize treatment efficiency with adolescents, clinicians would benefit from placing greater emphasis on organization and time management skills and recognizing the client’s need to retain their independence (Young & Myanthi Amarasinghe, 2010). An adolescent version of the CABS would address these issues by providing a measure that both monitors the progression of treatment and helps identify useful strategies. Moreover, the increased collaboration between clinician and patient may also serve to enhance the personalization of treatment and support the client’s need for independence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.