
Abstract
Caregiver strain is associated with caregiver and child well-being and clinical outcomes. The present study examined the psychometric properties of a revised 11-item measure of caregiver strain, the Caregiver Strain Questionnaire–Short Form 11 (CGSQ-SF11). In a sample of 962 caregivers, we found support for a three-factor model of the CGSQ-SF11, consisting of objective (e.g., financial impact), subjective internalized (e.g., sadness about the child’s problems), and subjective externalized (e.g., anger directed toward the child) strain factors. Measurement invariance was supported across multiple demographic and clinical groups, and all three subscales displayed high internal consistency. Convergent validity was also supported through positive correlations with measures of child psychopathology symptoms and psychosocial impairment. Moreover, caregiver strain was associated with number of child disorders as well as breadth of child symptoms across both internalizing and externalizing domains. Findings provide initial validation of the CGSQ-SF11 as a comprehensive yet brief measure of caregiver strain.
Keywords
The role of caregiver is associated with numerous challenges. Caregiver strain is a construct that captures both the observable burden (e.g., financial strain, disruption of work obligations or family relationships) and the negative emotional consequences (e.g., sadness, worry, anger, resentment) of caring for another person, particularly someone who presents with special needs (e.g., physical or mental health problems, disability; Brannan et al., 1997). A substantial body of research has focused on caregiver strain as it relates to caring for children with emotional and behavioral difficulties. A number of (mostly cross-sectional) studies indicate that caregiver strain is positively associated with symptom severity across a wide range of child mental health disorders, including depression (Bussing, Gary, et al., 2003; Bussing, Zima, et al., 2003; Jaycox et al., 2009), anxiety disorders (Compton et al., 2014; cf. Bussing, Gary, et al., 2003), attention-deficit/hyperactivity disorder (ADHD; Babinski et al., 2019; Bussing, Gary, et al., 2003; Evans et al., 2009), oppositional defiant disorder (ODD; Bussing, Gary, et al., 2003; Bussing, Zima, et al., 2003; Tsai et al., 2015), and conduct disorder (CD; Tsai et al., 2015; cf. Bussing, Gary, et al., 2003).
In addition to symptom severity within diagnostic categories, research has examined associations between broader indices of child dysfunction and caregiver strain. For example, greater impairment in child psychosocial functioning is associated with greater caregiver strain (Brannan & Heflinger, 2006). Additionally, research has looked beyond diagnostic categories and found that caregiver strain is positively associated with the breadth of child symptoms. One study found that caregiver strain was highest among caregivers of youth with symptoms that spanned both the internalizing and externalizing domains, compared with youth with symptoms in only one domain (Vaughan et al., 2013). Another study in a sample of children with ADHD found that caregiver strain increased with each additional comorbid disorder for which the children’s symptoms met diagnostic criteria (Rockhill et al., 2013). Taken together, the literature indicates that caregiver strain is positively associated with a variety of child mental health concerns, including severity of symptoms within multiple diagnostic categories, psychosocial impairment, breadth of symptoms, and number of comorbid disorders.
In addition to being associated with child psychopathology symptoms, higher caregiver strain is associated with numerous negative outcomes for caregivers and their children. Caregiver strain can harm caregiver mental health, hinder caregiver–child relationships, and lead caregivers to engage in less effective parenting practices (Brannan et al., 1997; Brannan & Heflinger, 2001; Frank et al., 2017). From a mental health services perspective, although greater strain is associated with greater use of services overall (Brannan et al., 2003; Bussing, Zima, et al., 2003; Ryan et al., 2015), elevated strain may interfere with consistent treatment attendance as well as progress in treatment. For example, in one study greater strain was associated with a greater likelihood of having a long break in care (Brannan et al., 2003). Other studies have indicated that greater strain predicted less favorable response to treatment among children with anxiety and disruptive behaviors (Accurso et al., 2015; Compton et al., 2014), as well as lower caregiver-rated treatment satisfaction (Garland et al., 2007; Heflinger et al., 2004). The accumulation of adverse effects of caregiver strain (e.g., ineffective parenting practices, less consistent use of services, diminished response to treatment) can exacerbate or maintain child mental health concerns (Accurso et al., 2015; Blader, 2006), thereby fueling caregiver strain in a cyclical fashion.
A key implication of these findings is that the treatment of child psychopathology may be improved if caregiver strain is measured, monitored, and targeted as an area of concern in its own right. Treatments for child psychopathology do appear to significantly reduce caregiver strain (Accurso et al., 2015; Iadarola et al., 2018), and reductions in caregiver strain are, in turn, associated with improvements in child symptoms (Accurso et al., 2015; Schleider et al., 2015). Critically, adding a component focused on reducing caregiver strain has been shown to enhance the effectiveness of behavioral interventions for child psychopathology (Chronis-Tuscano et al., 2013; Kazdin & Whitley, 2003). Given the relevance of caregiver strain to caregiver and child well-being and clinical outcomes, it would likely be beneficial to assess, monitor, and even target caregiver strain in evidence-based treatment for child mental health concerns (Waschbusch et al., 2020).
The Caregiver Strain Questionnaire (CGSQ; Brannan et al., 1997) is a commonly used, reliable, and valid measure of caregiver strain (Holly et al., 2019). The original CGSQ consists of 21 items, and factor analyses indicate that these items form three subscales that assess overlapping yet separable types of caregiver strain: (1) objective strain, or the observable negative events resulting from the child’s problems (e.g., financial strain, disruption of family relationships; 11 items); (2) subjective internalized strain, or inwardly directed negative feelings resulting from the child’s problems (e.g., sadness, worry; 6 items); and (3) subjective externalized strain, or negative feelings directed toward the child (e.g., anger, resentment; 4 items). The CGSQ was later shortened to a 7-item version (CGSQ-SF7; Brannan et al., 2012), which only included items tapping objective strain and subjective internalized strain; items tapping subjective externalized strain were excluded based on arguments that this subscale tends to have lower internal consistency and weaker predictive validity relative to the other subscales (Bickman et al., 2010). Although a shorter version of the CGSQ is warranted (e.g., the CGSQ’s extremely high internal consistencies indicate potential item redundancy; Holly et al., 2019) and desirable (e.g., to increase ease and speed of administration in clinical settings; Becker-Haimes et al., 2020), the CGSQ-SF7 has some notable limitations.
First, excluding items associated with subjective externalized strain may omit an important aspect of caregiver strain. Numerous studies indicate that subjective externalized strain shows significant independent relationships with child psychopathology and treatment outcomes. Some evidence suggests that subjective externalized strain is particularly relevant for understanding outcomes of children with externalizing problems (Bussing, Gary, et al., 2003; Vaughan et al., 2013). Additionally, subjective externalized strain appears to be the aspect of strain that is most strongly associated with poorer caregiver-child interaction quality (Frank et al., 2017), poorer caregiver mental health (Wang & Anderson, 2018), and higher rates of treatment dropout (Foster, 1998). Finally, subjective externalized strain may take longer than other types of strain to show significant reductions following the initiation of child treatment (Iadarola et al., 2018). Thus, measures of subjective externalized strain appear to contribute useful and unique information about the experiences of caregivers, particularly those of children with externalizing problems. Given the centrality of caregiver–child interactions to multiple evidence-based child treatments (e.g., parent management training, parent–child interaction therapy), including items tapping subjective externalized strain in a measure of caregiver strain is clinically indicated.
Second, many of the items that make up existing versions of the CGSQ are written in the past tense (e.g., “How sad or unhappy did you feel as a result of your child’s problems?”), which may limit their ability to measure change in caregiver strain over time. Responses to past-tense items may capture previous periods of greater strain (e.g., when the child’s symptoms were more severe) rather than present levels of strain. In the context of treatment, the ability to measure changes in caregiver strain over time is crucial in order to successfully track progress (or lack thereof) over the course of treatment.
Thus, to overcome the limitations of previous versions of the CGSQ, we developed the 11-item Caregiver Strain Questionnaire–Short Form (CGSQ-SF11). In addition to the seven items from the CGSQ-SF7 (Brannan et al., 2012), the CGSQ-SF11 included four items from the original CGSQ (Brannan et al., 1997) that were omitted from the CGSQ-SF7. Three of these items were from the subjective externalized strain factor of the original CGSQ and assessed caregivers’ anger, resentment, and embarrassment in relation to their child’s problems (see Table 2 for item wording). The fourth item (also on the original CGSQ, but from the subjective internalized strain factor) assessed caregivers’ perceptions of the general toll taken on the family by their child’s problems (see Table 2). As noted above, to ensure a focus on present levels of strain to maximize the ability to detect change, all items were worded in the present tense, and the instructions were altered to prompt caregivers to focus on the present time (see the CGSQ-SF11 subsection of the Method section below for instructions).
The overarching goal of the present study was to assess the validity of the CGSQ-SF11 as a brief yet comprehensive measure of caregiver strain. To this end, the present study aimed to: (1) examine the factor structure, measurement invariance, and internal consistency of the CGSQ-SF11; (2) investigate associations between caregiver strain and demographic factors (i.e., child age, child sex, caregiver age, caregiver sex, caregiver ethnicity, caregiver race, income); (3) establish convergent validity of the CGSQ-SF11 by examining correlations between caregiver strain and theoretically related constructs (i.e., child psychopathology symptoms, child impairment); (4) investigate unique associations between caregiver strain and different forms of child psychopathology, given high rates of comorbidity among the disorders assessed (e.g., Rockhill et al., 2013); (5) examine whether the number of disorders for which children’s symptoms meet screening or diagnostic thresholds is related to caregiver strain; and (6) investigate whether caregiver strain is higher among caregivers of children whose symptoms span internalizing and externalizing domains, compared with being limited to either domain alone. We pursued these aims in a large, nationally representative sample of caregivers of children with varying levels of psychopathology symptoms and impairment.
We developed several hypotheses regarding the factor structure of the CGSQ-SF11 as well as the associations between CGSQ-SF11 scores and child psychopathology and impairment. First, based on previous research (Brannan et al., 1997), we hypothesized that the CGSQ-SF11 would exhibit a three-factor structure. Second, we hypothesized that caregiver strain would be positively correlated with child psychopathology and impairment variables. Third, drawing on previous research (Rockhill et al., 2013), we hypothesized that caregiver strain would increase as the number of child disorders increased. Finally, based on previous research (Vaughan et al., 2013), we hypothesized that caregiver strain would be significantly higher among caregivers of children who had clinically significant symptoms spanning both the internalizing and externalizing domains compared with being limited to either domain alone.
Method
Participants
The sample consisted of caregivers of 962 children (N = 482 males; 50.1%) ages 5 to 12 years (M = 8.42, SD = 2.31). The majority of the youth were identified by their caregivers as White (N = 756; 78.6%). In terms of ethnicity, 148 youth (15.4%) were identified as Hispanic. Children were rated by caregivers (N = 414 males, 43.0%; N = 849 biological parents, 88.3%) between the ages of 20 and 72 years old (M = 36.59, SD = 8.30). The most common household income range was $25,000 to $49,999, which was endorsed by 24.7% of the sample. All demographic information, including additional information about geographic characteristics of the sample, is summarized in Table 1. Sample size was determined based on the goal of recruiting a sufficiently representative sample.
Sample Characteristics.
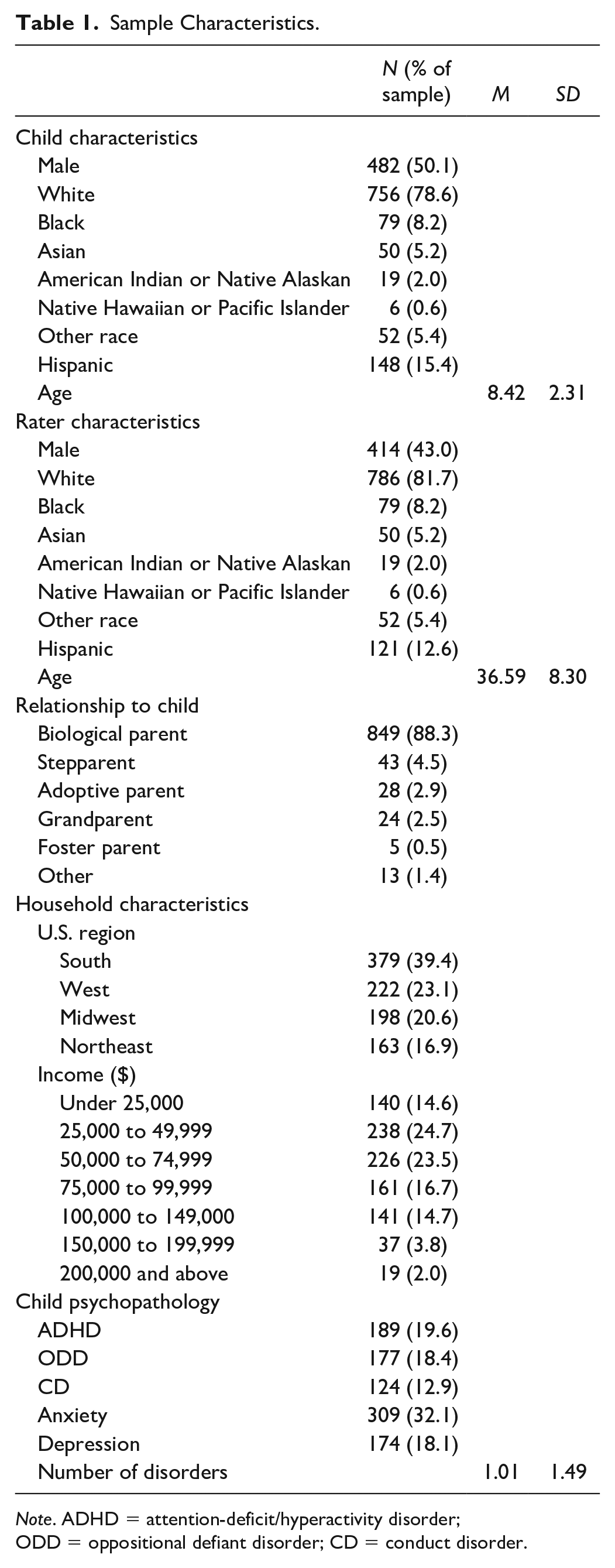
Note. ADHD = attention-deficit/hyperactivity disorder; ODD = oppositional defiant disorder; CD = conduct disorder.
Procedure
Participants were recruited via Qualtrics Panel, a subdivision of the research software company Qualtrics (www.qualtrics.com). Data were collected via internet from standing panels of respondents maintained by Qualtrics Panel. Several measures were implemented to ensure high-quality data (e.g., Bot Detection, RelevantID; Qualtrics, 2020). Procedures were also in place to confirm the identity and demographic characteristics of respondents, including digital fingerprinting and cross-validation with other data sources (e.g., LinkedIn, TrueSample, Verity, etc.). The study was approved by an institutional review board and respondents provided informed consent prior to participation. Caregivers completed ratings of their children in exchange for points that could be traded in for rewards (e.g., gift cards) administered by the survey company. Participants were required to be primary caregivers of children ages 5 to 12, to be U.S. residents, and to understand written English. We chose to focus on caregivers of school-age children (i.e., between the ages of 5 and 12 years) because the vast majority of the literature on caregiver strain focuses on this age group; moreover, caregivers of school-age children tend to play a more prominent role in evidence-based mental health treatment for their children compared with caregivers of adolescents. Responses were monitored to maximize the likelihood that the final sample was broadly representative of the U.S. population in terms of gender, race, income, and geographic region, and inspection of U.S. census data suggests this was largely accomplished. To compare the sample’s race and ethnicity distribution with the 2020 projections for the U.S. population, we accessed the U.S. Census data (U.S. Census Bureau, 2017). The difference in racial and ethnic distribution of our sample, compared with the projected 2020 U.S. Census data, did not exceed 6%; our sample had fewer participants identifying as either Black (difference = 5.3%), Asian (difference = 0.8%), or Hispanic (difference = 3.3%), but more participants identifying as White (difference = 2.5%), American Indian or Native Alaskan (difference = 0.7%), or Native Hawaiian or Pacific Islander (difference = 0.4%).
Participants were presented with a description of the study followed by a request to consent to participate. After participants consented, they provided demographic information for themselves, their child, and their household. Finally, a series of rating scales were presented in a randomized order, including the scales used in this study. The average time to complete the survey was 21.0 minutes.
Before arriving at the final sample size reported above, invalid data were identified and removed. First, 14 participants were excluded from all analyses because caregivers reported that they did not know whether the child was being treated with psychoactive medication, raising questions about the validity of their responses. Second, an additional 88 participants were excluded from all analyses because they completed the study questionnaires unusually quickly. These participants were identified by calculating each participant’s relative completion speed (i.e., sample median completion time divided by individual completion time). Then we used the recommended cutoff of 2 (Leiner, 2019) to exclude respondents who completed the questionnaires more than twice as fast as the typical respondent (i.e., in less than 6.85 minutes). We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Measures
Caregiver Strain Questionnaire–Short Form 11
The CGSQ-SF11 is a self-report questionnaire that consists of 11 items assessing the level of strain caregivers experience in caring for their child. 1 It is a shortened version of the original 21-item CGSQ (Brannan et al., 1997), which has been shown in numerous studies to be a reliable and valid measure (see Holly et al., 2019 for review). The items from the original CGSQ form a three-factor structure consisting of the following factors: objective strain, subjective internalized strain, and subjective externalized strain (Brannan et al., 1997). Unlike the CGSQ-SF7 (Brannan et al., 2012), which excluded subjective externalized strain items, the CGSQ-SF11 fully covers the caregiver strain construct by including items from each of the three caregiver strain factors.
Caregivers were presented with the following instructions for completing the CGSQ: We are trying to understand how things are for you and your family and how much your child’s problems or difficulties have affected you and your family. For each question below, please circle or check the response that best answers the question for you and your family at the present time.
Items are rated on a 5-point Likert-type scale that ranges from 1 (not at all) to 5 (very much). Means, standard deviations, and the percentage of the sample who endorsed each response option are summarized in Table 2 for all 11 items. Statistics supporting the reliability and validity of the CGSQ-SF11 are presented in the Results section.
Descriptive Statistics and Factor Loadings for the CGSQ-SF11 Items.
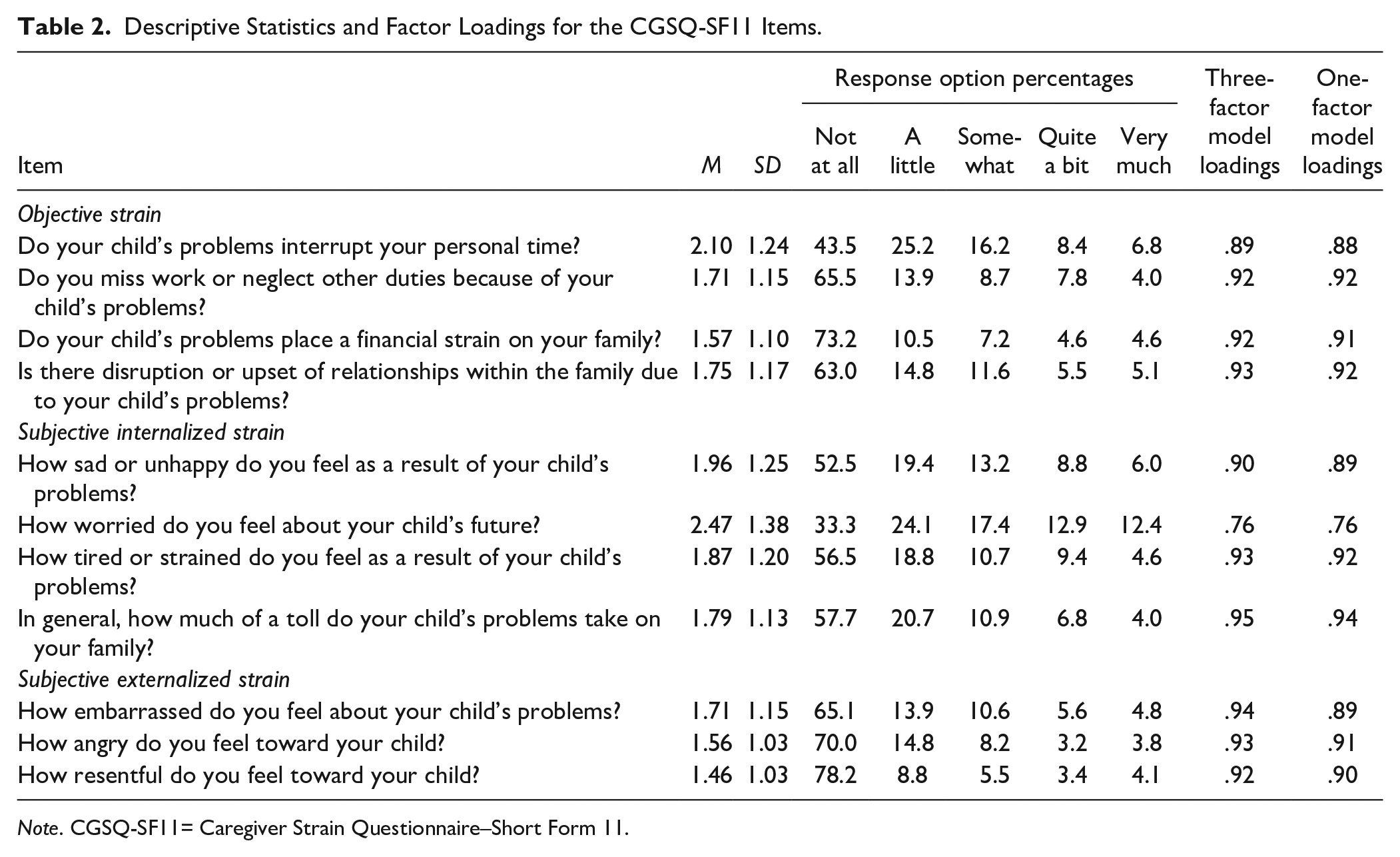
Note. CGSQ-SF11= Caregiver Strain Questionnaire–Short Form 11.
Disruptive Behavior Disorders Rating Scale (DBD; Pelham, Gnagy, et al., 1992)
The DBD is a caregiver-report questionnaire that consists of 45 items corresponding to the Diagnostic and Statistical Manual of Mental Disorders Fifth edition symptoms of ADHD, ODD, and CD. Items are rated on a 4-point Likert-type scale that ranges from 0 (not at all) to 3 (very much). Items assessing ADHD, ODD, and CD symptoms were averaged to compute an ADHD score (M = 0.83, SD = 0.75), an ODD score (M = 0.71, SD = 0.74), and a CD score (M = 0.29, SD = 0.57). The psychometric properties of the DBD are well supported (e.g., Pelham, Evans, et al., 1992; Wright et al., 2007). Internal consistency for the DBD in the present sample (Cronbach’s α = .96, .93, and .97 for the ADHD, ODD, and CD scales, respectively) was excellent.
The DBD was also used to determine whether children’s symptoms exceeded diagnostic thresholds associated with ADHD, ODD, and CD. Symptoms were defined as present if they were rated as 2 (pretty much) or 3 (very much). Children with six or more of the inattentive and/or hyperactive/impulsive symptoms of ADHD were identified as having ADHD. Children with four or more symptoms of ODD were identified as having ODD. Children with three or more symptoms of CD were identified as having CD.
Impairment Rating Scale (IRS; Fabiano et al., 2006)
The IRS is a caregiver-report questionnaire that consists of 10 items assessing the child’s impairment in a number of domains, including peer relationships, caregiver–child relationships, academic performance, classroom behavior, self-esteem, functioning in the family, and overall problems. Eight items on the IRS are rated via visual analogue scales anchored at the low end by 0 (no problem) and at the high end by 6 (extreme problem). These items were averaged to compute a total impairment score (M = 1.32, SD = 1.33). 2 An additional item assesses the caregiver’s perception of whether the child needs treatment or services for any of the problems they endorsed on the questionnaire. This item is rated using a visual analogue scale anchored at the low end by 0 (no need for treatment or services) and at the high end by 6 (extreme need for treatment or services). The IRS has been shown to have strong temporal stability, as well as convergent and discriminant validity as a measure of children’s impairment (Fabiano et al., 2006). Internal consistency for the IRS total impairment scale in the present sample (Cronbach’s α = .94) was excellent.
Short Mood and Feelings Questionnaire–Caregiver Report (SMFQ; Angold et al., 1995)
The SMFQ is a caregiver-report questionnaire that consists of 13 items assessing depressive symptoms in youth. Severity of symptoms for the past two weeks are rated on a 3-point scale that ranges from 0 (not true) to 2 (true). Items are added to compute a total score (M = 4.59, SD = 6.17). The SMFQ is a shortened version of a longer questionnaire, which has been shown to have strong psychometric properties (Costello & Angold, 1988). The SMFQ has similar psychometric properties to the longer measure (Angold et al., 1995; Messer et al., 1995). Internal consistency for the SMFQ in the present sample (Cronbach’s α = .95) was excellent. Sensitivity and specificity analyses indicate that a cutoff score of 11 on the SMFQ is appropriate for identifying youth who have depression in community samples (Thapar & McGuffin, 1998). This cutoff score was used to determine whether children’s symptoms exceeded diagnostic thresholds associated with depression.
Short Screen for Child Anxiety Related Emotional Disorders–Caregiver Report (SSCARED; Birmaher et al.,1999)
The SSCARED is a five-item caregiver-report questionnaire that was developed to screen for the presence of an anxiety disorder in youth. Severity of anxiety symptoms for the past 3 months are rated on a 3-point scale that ranges from 0 (not true or hardly ever true) to 2 (true or often true). Items are added to compute a total score (M = 2.10, SD = 2.37). The SSCARED is a shortened version of a longer questionnaire, which has been shown to have strong psychometric properties (Birmaher et al., 1997, 1999). The SSCARED has similar psychometric properties to the longer measure (Birmaher et al., 1999), and each item on the SSCARED was selected on the basis of displaying the strongest loading onto each of the five factors on the longer measure (i.e., panic/somatic, general anxiety, separation anxiety, social phobia, and school phobia). Internal consistency for the SSCARED in the present sample (Cronbach’s α = .80) was good. Sensitivity and specificity analyses indicate that a cutoff score of 3 on the SSCARED is appropriate for differentiating youth who have and do not have an anxiety disorder (Birmaher et al., 1999). This cutoff score was used to determine whether children’s symptoms indicated the possible presence of an anxiety disorder.
Analytic Plan
First, the factor structure of the CGSQ-SF11 was examined using confirmatory factor analysis (CFA). We tested two models using CFA: a three-factor model, which was supported in previous research on the 21-item CGSQ (Brannan et al., 1997); and a one-factor model, since numerous studies have used a “global strain” score derived by averaging all of the CGSQ items, yet we are unaware of factor analytic research supporting a one-factor model. The factor analysis used the weighted least squares means and variance adjusted estimator to accommodate the ordinal nature of item-level data. Model fit was evaluated by examining the root mean square error of approximation (RMSEA), comparative fit index (CFI), Tucker–Lewis index (TLI), and standardized root mean square residual (SRMR) and comparing them against the following thresholds for establishing good fit: RMSEA ≤ 0.05, CFI ≥ 0.95, TLI ≥ 0.95, and SRMR ≤ .08 (Hu & Bentler, 1999; MacCallum et al., 1996).
Second, we conducted multiple group measurement invariance analyses to determine if the factor structure of the CGSQ-SF11 differed as a function of several demographic and clinical factors, based on previous research suggesting that these factors can influence levels of caregiver strain. These factors were child sex, child age (5/6 years vs. 7/8 years vs. 9/10 years vs. 11/12 years), caregiver sex, caregiver age (≤31 years vs. 32-35 years vs. 36-41 years vs. ≥42 years, defined using sample quartiles), or child psychopathology (screening or diagnostic criteria met vs. not met, for each disorder separately). We conducted these analyses following the procedures outlined by Svetina et al. (2020), which were based on the propositions of Wu and Estabrook (2016) for establishing measurement invariance for ordered categorical variables (i.e., variables like the CGSQ-SF11 items). We imposed increasingly strong equality constraints on the model and determined whether these constraints significantly decreased model fit. Invariance was tested by examining fit statistics at baseline (i.e., allowing all parameters to vary across groups), after constraining thresholds to be equal, and after constraining thresholds and factor loadings to be equal. We evaluated change in model fit between these levels of invariance, and invariance was supported when models showed reasonable fit to the data and when more constrained models did not show significantly worse fit compared with less constrained models. More constrained models were classified as showing significantly worse fit compared with less constrained models based on the following criteria: Δχ2 p < .05, ΔCFI < −.004, and ΔRMSEA > .05 for threshold invariance compared with baseline; Δχ2 p < .05, ΔCFI < −.004, and ΔRMSEA > .01 for threshold and factor loading invariance compared with threshold invariance (Rutkowski & Svetina, 2017).
Third, internal consistency was assessed using Cronbach’s α. Fourth, we evaluated whether CGSQ-SF11 scores were associated with demographic variables (i.e., child age, child sex, caregiver age, caregiver sex, caregiver ethnicity, caregiver race, income), using both Spearman’s rho correlations and one-way analyses of variance (ANOVAs). Fifth, the convergent validity of the CGSQ-SF11 as a measure of caregiver strain was assessed by computing simple correlations to assess associations with child psychopathology (i.e., ADHD, ODD, CD, depression, and anxiety) and impairment (i.e., total impairment across domains and need for treatment). Spearman’s rho and bootstrapping procedures were used for correlations, as these nonparametric techniques are more appropriate for use with nonnormal variables such as the caregiver strain, child psychopathology, and impairment variables (de Winter et al., 2016; Erceg-Hurn & Mirosevich, 2008). For each analysis, 2,000 bootstrapping samples were drawn from our sample, and the bias-corrected 95% confidence intervals (CIs) of the statistical values were estimated, which adjusted for bias and skewness in the bootstrapped distribution.
Sixth, to examine whether child psychopathology measures exhibited unique associations with CGSQ-SF11, we conducted partial correlations (also using Spearman’s rho) between each child psychopathology measure and CGSQ-SF11 while controlling for scores on the other child psychopathology measures.
Finally, to assess the validity of CGSQ-SF11 scores with respect to differentiating children whose symptoms exceeded screening or diagnostic thresholds for more versus fewer forms of psychopathology, we summed the number of disorders for which each child’s symptoms met criteria and conducted a one-way ANOVA with number of disorders as the independent variable and caregiver strain as the dependent variable. Additionally, we conducted a one-way ANOVA to examine whether caregivers of children whose symptoms met criteria for both an internalizing disorder (depression, anxiety) and an externalizing disorder (ADHD, ODD, CD) had higher levels of strain compared with caregivers of children who met criteria for only one of these types of disorders.
Since the sample was so large, even small effects were likely to be statistically significant. Therefore, in addition to p values, we also relied on effect sizes and their respective CIs to make more informative statistical inferences (e.g., about which child psychopathology variables were more versus less strongly correlated with caregiver strain). We used the following guidelines suggested by J. Cohen (1988) to interpret effect sizes: d = 0.2 represents a small effect size, d = 0.5 represents a medium effect size, and d = 0.8 represents a large effect size.
Analytic Software
The CFA and measurement invariance analyses were conducted using the lavaan (Rosseel, 2012) and semTools (Jorgensen et al., 2020) packages in R, and the remaining analyses were conducted using SPSS 22.
Results
Factor Analysis
CFA supported the three-factor solution derived in previous research, χ2(41) = 298.96, p < .001, RMSEA = 0.046 (90% CI [0.037, 0.055]), CFI = 0.999, TLI = 0.999, SRMR = 0.027. All items included in the factor analysis loaded significantly onto their respective factors (see Table 2), with loadings that ranged from 0.76 (“How worried do you feel about your child’s future?”) to 0.95 (“In general, how much of a toll do your child’s problems take on your family?”).
Turning to the one-factor model, fit statistics indicated that the one-factor model provided an acceptable fit, χ2(44) = 498.70, p < .001, RMSEA = 0.068 (90% CI [0.060, 0.077]), CFI = 0.999, TLI = 0.998, SRMR = 0.036. However, RMSEA, TLI, and SRMR values indicated a worse fit for the one-factor model compared with the three-factor model, and RMSEA was above the recommended threshold for the one-factor model. A direct comparison of the two models’ fit suggested that the three-factor model provided a significantly better fit than the one-factor model, Δχ2 = 147.2, Δdf = 3, p < .001. Thus, the three-factor model was retained as the superior model, and all analyses that follow are based on the three-factor model. However, since the one-factor model evidenced reasonable fit, and since it is more parsimonious and widely used in previous research, we also conducted analyses and report results for the CGSQ-SF11 global strain (i.e., total) score.
Measurement Invariance
Tests of measurement invariance indicated support for invariance across all factors tested (i.e., child sex, child age, caregiver sex, caregiver age, and child psychopathology variables; see Table 3). All models showed reasonable fit (e.g., CFI ≥ .982), and there was no evidence that fit worsened significantly when increasingly strong equality constraints were imposed (e.g., ΔCFI ≥ −.003).
Multiple Group Measurement Invariance Analyses.
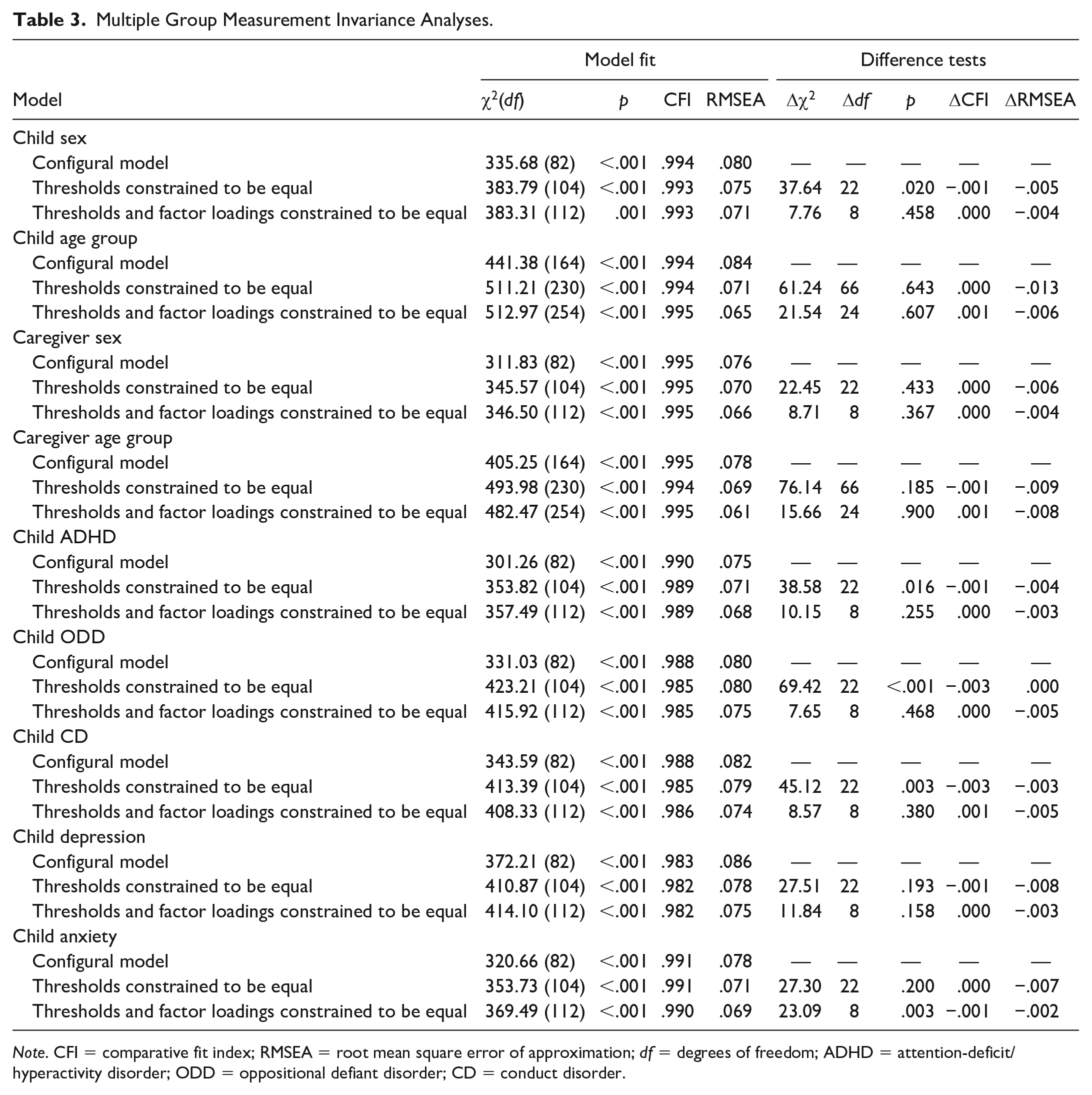
Note. CFI = comparative fit index; RMSEA = root mean square error of approximation; df = degrees of freedom; ADHD = attention-deficit/hyperactivity disorder; ODD = oppositional defiant disorder; CD = conduct disorder.
Internal Consistency
Based on the results of the CFA, the items of the CGSQ-SF11 were averaged to create scores for each of the three caregiver strain factors: objective strain, subjective internalized strain, and subjective externalized strain (see Table 2). A global strain score was also created by averaging all of the CGSQ-SF11 items. Each subscale demonstrated very good to excellent reliability, as did the scale as a whole (i.e., Cronbach’s α ranged from .88 [subjective externalized strain] to .96 [global strain]; see Table 4 for descriptive statistics).
Descriptive Statistics and Correlations (Spearman’s Rho) for CGSQ-SF11 Factors.
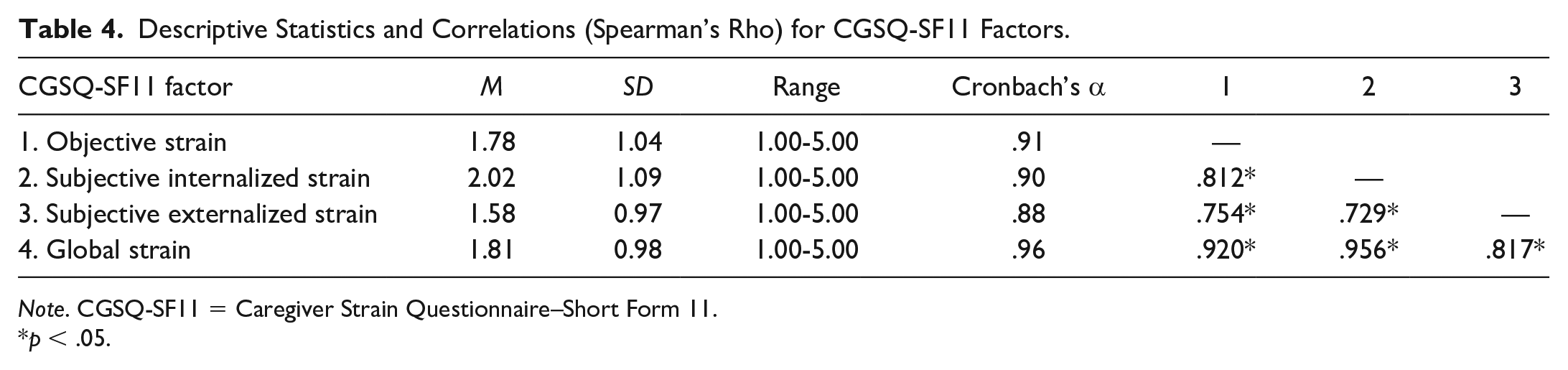
Note. CGSQ-SF11 = Caregiver Strain Questionnaire–Short Form 11.
p < .05.
Demographic Factors
Spearman’s rho correlations indicated that caregiver age showed very weak negative correlations with objective strain, rs(960) = −.081, p = .011, 95% CI [−.142, −.022], subjective externalized strain, rs(960) = −.085, p = .008 , 95% CI [−.149, −.018], and global strain, rs(960) = −.068, p = .035, 95% CI [−.133, −.002]. However, caregiver age was not correlated with subjective internalized strain, rs(960) = −.057, p = .077, 95% CI [−.119, .003]. Child age and income level were not significantly correlated with caregiver strain (see Table S1 in Supplemental Material [available online] for statistics for nonsignificant effects).
Furthermore, one-way ANOVAs indicated that male caregivers reported higher levels of subjective externalized strain (M = 1.65, 95% CI [1.55, 1.76], SD = 1.07) compared with female caregivers (M = 1.52, 95% CI [1.45, 1.60], SD = 0.87), Welch’s F(1, 78168) = 3.87, p = .049. 3 This effect was, however, small (d = 0.14, 95% CI [0.01, 0.26]). Caregiver sex was unrelated to the other two types of strain and global strain. Turning to child sex, caregivers of males reported higher levels of strain than caregivers of females, a small effect that was consistent across all three types of strain as well as global strain, F(1, 961) = 13.75, p = .001, d = 0.22 [objective]; F(1, 961) = 14.89, p < .001, d = 0.25 [subjective internalized]; F(1, 961) = 9.08, p = .003, d = 0.19 [subjective externalized]; F(1, 961) = 13.75, p < .001, d = 0.24 [global] (see Table 5). Finally, caregiver strain did not differ with respect to caregiver race or caregiver ethnicity (see Table S2 in Supplemental Material [available online] for statistics for nonsignificant effects).
ANOVA Results (2,000-Sample Bootstrap) for Caregiver Strain as a Function of Child Sex.
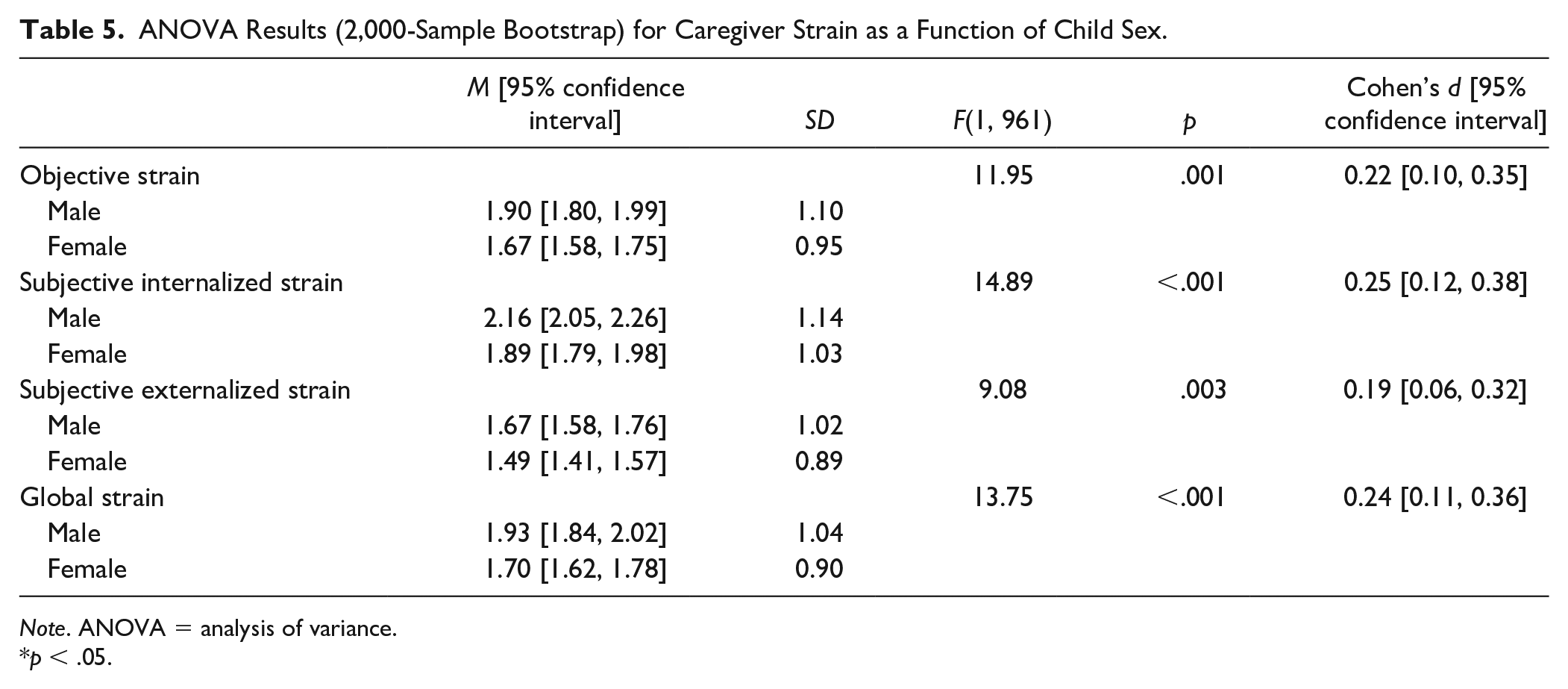
Note. ANOVA = analysis of variance.
p < .05.
Convergent Validity
Correlations indicated that all child psychopathology and impairment variables were positively correlated with each of the three caregiver strain factors as well as global strain (rss ranged from .463 to .729; see Table 6). Inspection of CIs and their patterns of overlap/nonoverlap suggested that some forms of child psychopathology/impairment (e.g., depression) were more strongly associated with caregiver strain than others (e.g., anxiety). Moreover, there was some evidence that certain forms of child psychopathology/impairment were more strongly associated with some types of caregiver strain (e.g., subjective internalized strain, rss ranged from .483 to .702) than others (e.g., subjective externalized strain, rss ranged from .463 to .659).
Spearman’s Correlations Between CGSQ-SF11 Factors and Child Psychopathology/Impairment Variables (2,000 Sample Bootstrap).
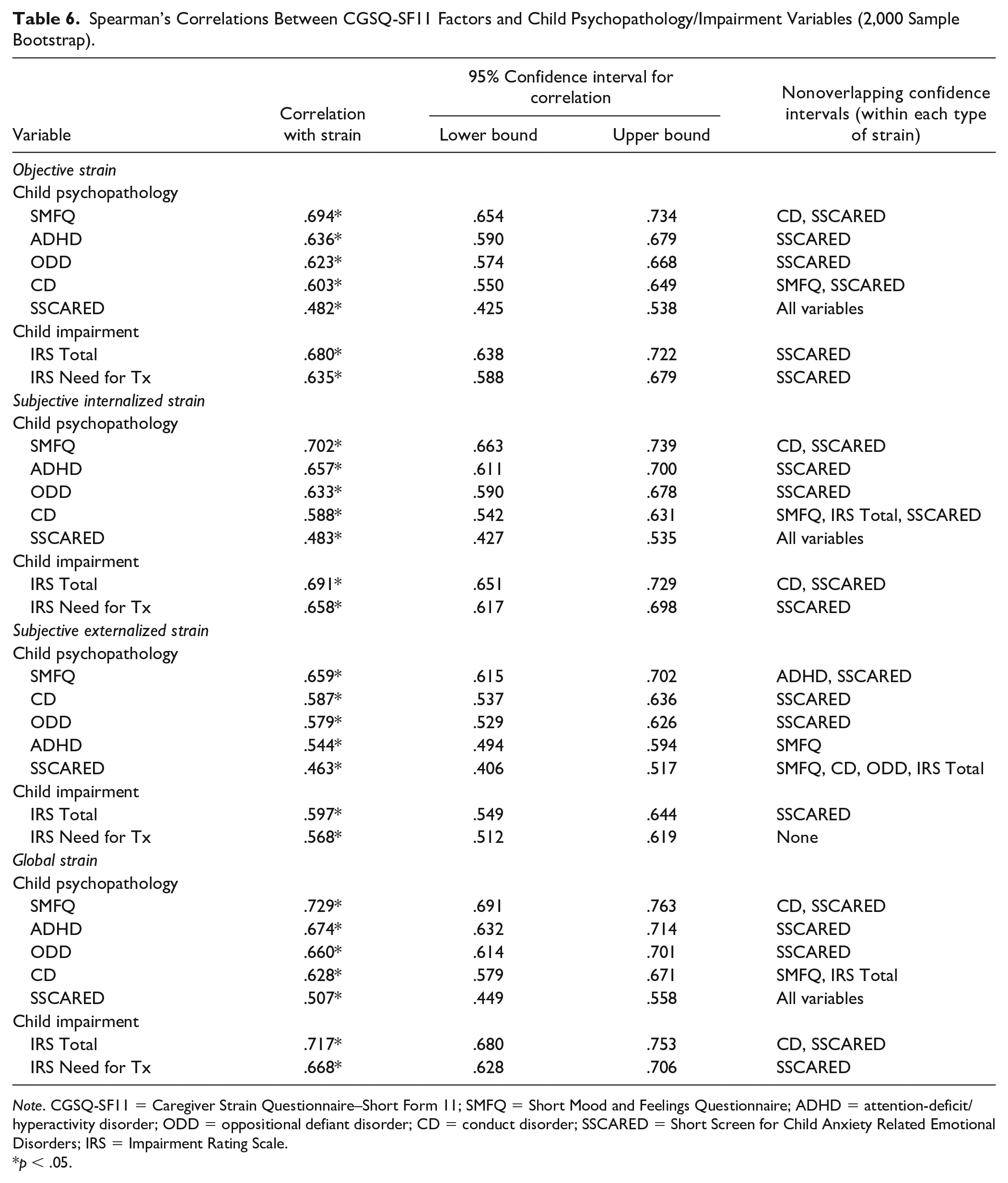
Note. CGSQ-SF11 = Caregiver Strain Questionnaire–Short Form 11; SMFQ = Short Mood and Feelings Questionnaire; ADHD = attention-deficit/hyperactivity disorder; ODD = oppositional defiant disorder; CD = conduct disorder; SSCARED = Short Screen for Child Anxiety Related Emotional Disorders; IRS = Impairment Rating Scale.
p < .05.
In terms of which forms of child psychopathology/impairment exhibited stronger and weaker associations with caregiver strain, there was evidence that depression was most strongly correlated with caregiver strain, and this pattern was consistent across all three types of caregiver strain as well as global strain (rss ranged from .659 to .729). Additionally, there was evidence that anxiety was most weakly associated with caregiver strain, which was again consistent across all three types of caregiver strain and global strain (rss ranged from .463 to .507; see Table 6 and Figure 1).
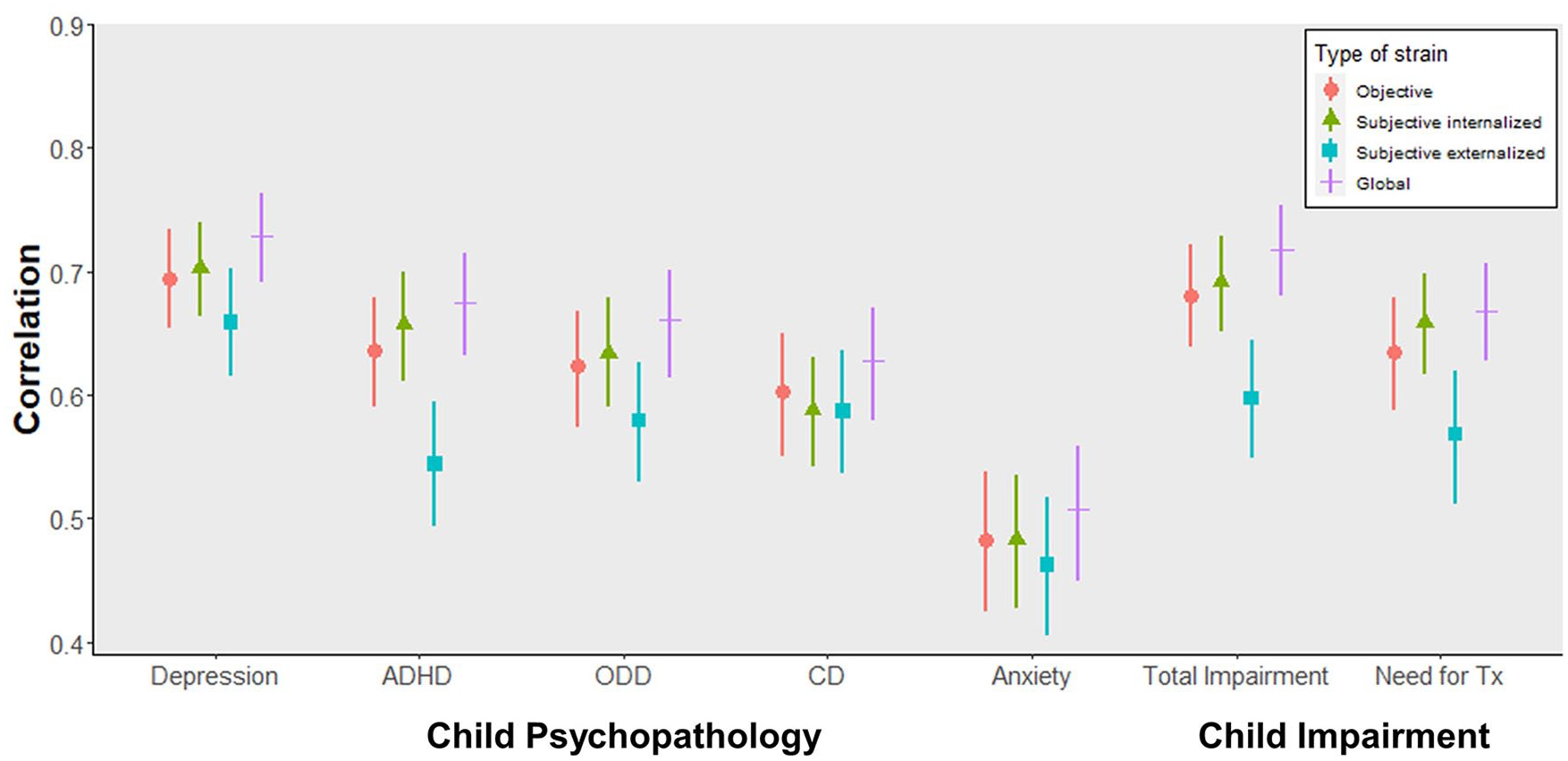
Correlation coefficients for the correlations between each form of child psychopathology and impairment (x-axis) and type of caregiver strain (see legend), plotted along with the lower and upper bounds of the associated 95% confidence intervals.
Examination of CI overlap within each form of child psychopathology/impairment indicated that ADHD seemed to be the only form of child psychopathology that was more strongly associated with some types of caregiver strain than others. More specifically, ADHD appeared to be more strongly associated with subjective internalized strain, rs(960) = .657, and global strain, rs(960) = .674, compared with subjective externalized strain, rs(960) = .544 (see Figure 1).
In terms of impairment, IRS Total appeared to be more strongly associated with subjective internalized strain, rs(960) = .691, and global strain, rs(960) = .717, compared with subjective externalized strain, rs(960) = .597. Moreover, IRS Need for Treatment appeared to be more strongly associated with global strain, rs(960) = .668, compared with subjective externalized strain, rs(960) = .568 (see Table 6).
Partial Correlations
Partial correlations using Spearman’s rho indicated that, after controlling for all other forms of child psychopathology assessed in the present study, almost every child psychopathology variable exhibited significant positive associations with the caregiver strain factors and global strain (rss ranged from .016 to .407; see Table 7). However, the partial correlations were noticeably weaker than the simple correlations reported in Table 6, suggesting that the overlap among the various forms of psychopathology helped account for the associations among caregiver strain and child psychopathology variables. Moreover, the correlation coefficients indicated that child depressive symptoms displayed the strongest unique associations with strain (rss ranged from .356 to .407 and were in the weak to moderate range), consistent with the results of the simple correlations, whereas the remaining child psychopathology variables displayed correlations in the very weak to weak range. The single exception to the general pattern of significant positive correlations was for ADHD symptoms—more specifically, the correlation between ADHD symptoms and subjective externalized strain was no longer significant after controlling for other forms of child psychopathology. Thus, with only one exception, each form of child psychopathology exhibited unique (albeit weak) positive correlations with each caregiver strain factor, and correlations for child depressive symptoms appeared to be the strongest.
Partial Correlations (Spearman’s Rho) Between Caregiver Strain and Child Psychopathology Variables.
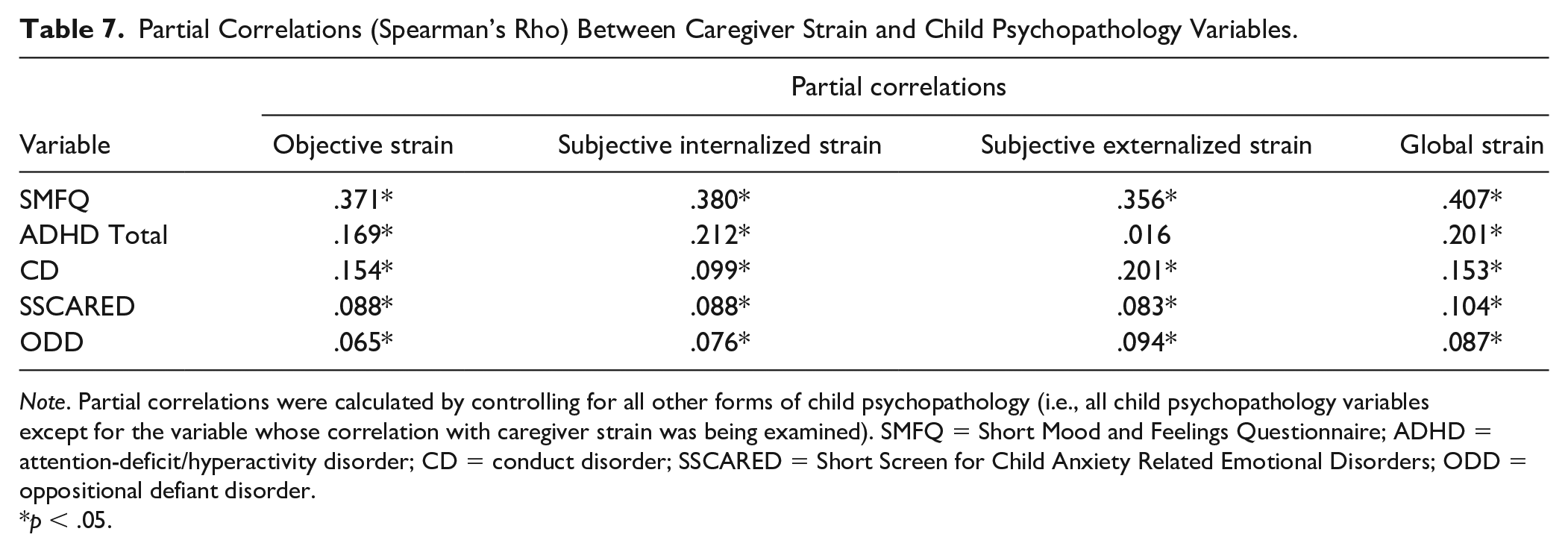
Note. Partial correlations were calculated by controlling for all other forms of child psychopathology (i.e., all child psychopathology variables except for the variable whose correlation with caregiver strain was being examined). SMFQ = Short Mood and Feelings Questionnaire; ADHD = attention-deficit/hyperactivity disorder; CD = conduct disorder; SSCARED = Short Screen for Child Anxiety Related Emotional Disorders; ODD = oppositional defiant disorder.
p < .05.
Number of Disorders
Number of disorders was computed for each child by summing the number of disorders for which the child’s symptoms exceeded screening or diagnostic thresholds, resulting in a number that ranged from 0 (no disorders) to 5 (five disorders). One-way ANOVAs indicated that caregiver strain differed with respect to the number of disorders children were reported to have. 4
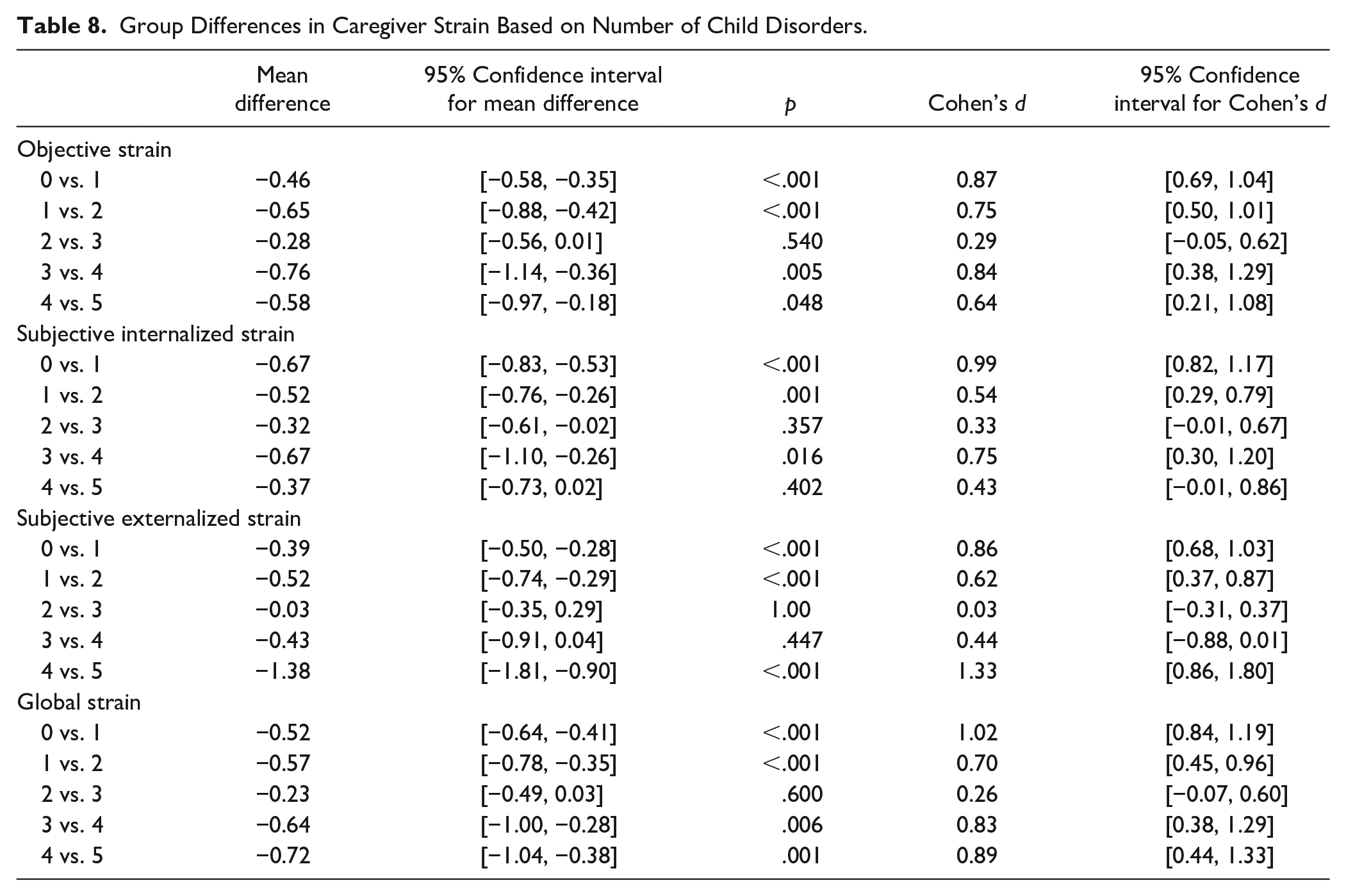
All three caregiver strain factors as well as global strain differed with respect to number of child disorders, F(5, 145.16) = 187.87, p < .001 [objective]; F(5, 148.73) = 181.37, p < .001 [subjective internalized]; F(5, 142.70) = 131.48, p < .001 [subjective externalized]; F(5, 145.56) = 216.76, p < .001 [global strain]. Examination of means and post hoc comparisons indicated that, in general, caregiver strain was higher among caregivers who reported that their children had more disorders (see Table 8 and Figure 2). Moreover, trend analyses indicated that these patterns followed linear trends, F(1, 956) = 1390.60, p < .001 [objective]; F(1, 956) = 1031.06, p < .001 [subjective internalized]; F(1, 956) = 1155.72, p < .001 [subjective externalized]; F(1, 956) = 1532.00, p < .001 [global strain]. Across all types of strain, however, caregivers of children whose symptoms met thresholds for two forms of psychopathology compared with three did not report different levels of strain; additionally, several other groups did not report significantly different levels of strain (see Figure 2). Effect sizes for significant differences between adjacent groups ranged from 0.54 (medium effect) to 1.33 (large effect).
Group Differences in Caregiver Strain Based on Number of Child Disorders.
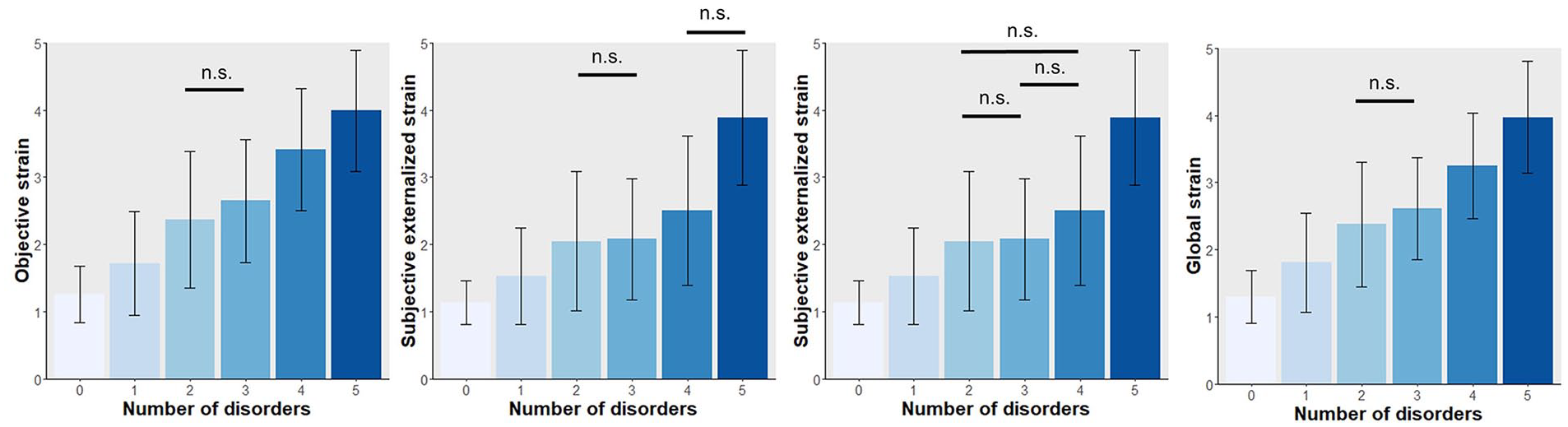
Depiction of means for objective strain, subjective internalized strain, subjective externalized strain, and global strain (left to right) associated with different numbers of child disorders.
Internalizing Plus Externalizing Psychopathology
On the basis of whether the child’s symptoms exceeded screening or diagnostic thresholds for depression, anxiety, ADHD, ODD, and CD, each child was classified as having neither internalizing nor externalizing psychopathology (N = 538, 55.9% of the sample), internalizing psychopathology only (i.e., depression or anxiety in the absence of ADHD, ODD, and CD; N = 165, 17.2% of the sample), externalizing psychopathology only (i.e., ADHD, ODD, or CD in the absence of depression and anxiety; N = 94, 9.8% of the sample), or both internalizing and externalizing psychopathology (N = 165, 17.2% of the sample). One-way ANOVAs indicated that caregiver strain differed with respect to the child’s internalizing/externalizing classification. 5
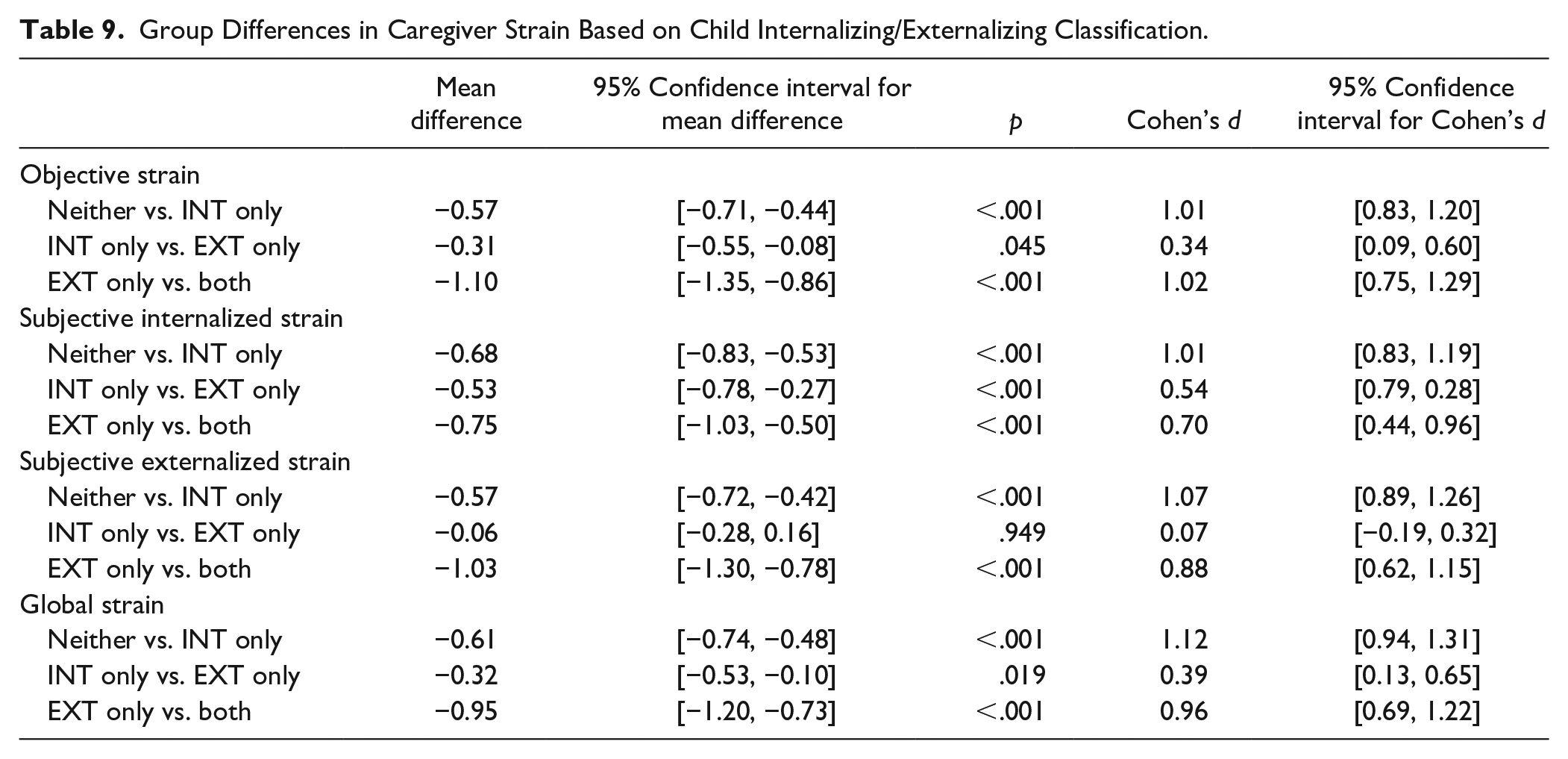
All three caregiver strain factors as well as global strain differed with respect to child internalizing/externalizing psychopathology, F(3, 23609) = 192.49, p < .001 [objective]; F(3, 24610) = 208.54, p < .001 [subjective internalized]; F(3, 22953) = 116,79 p < .001 [subjective externalized]; F(3, 23596) = 212.96, p < .001 [global]. Examination of means and post hoc comparisons indicated that, in general, caregiver strain was highest among caregivers who reported that their children had both internalizing and externalizing psychopathology (see Table 9 and Figure 3). The only nonsignificant group difference was for subjective externalized strain reported by caregivers of children with internalizing psychopathology only versus externalizing psychopathology only (see Figure 3). However, effect sizes for the differences between these two groups were also relatively small across the other two strain factors and global strain (Cohen’s d ranged from 0.34 to 0.54, or small to medium). Effect sizes for other group differences (i.e., neither class of psychopathology compared with internalizing only, externalizing only compared with internalizing plus externalizing psychopathology) were noticeably larger (Cohen’s d ranged from 0.70 to 1.12, or medium to large; see Table 9).
Group Differences in Caregiver Strain Based on Child Internalizing/Externalizing Classification.
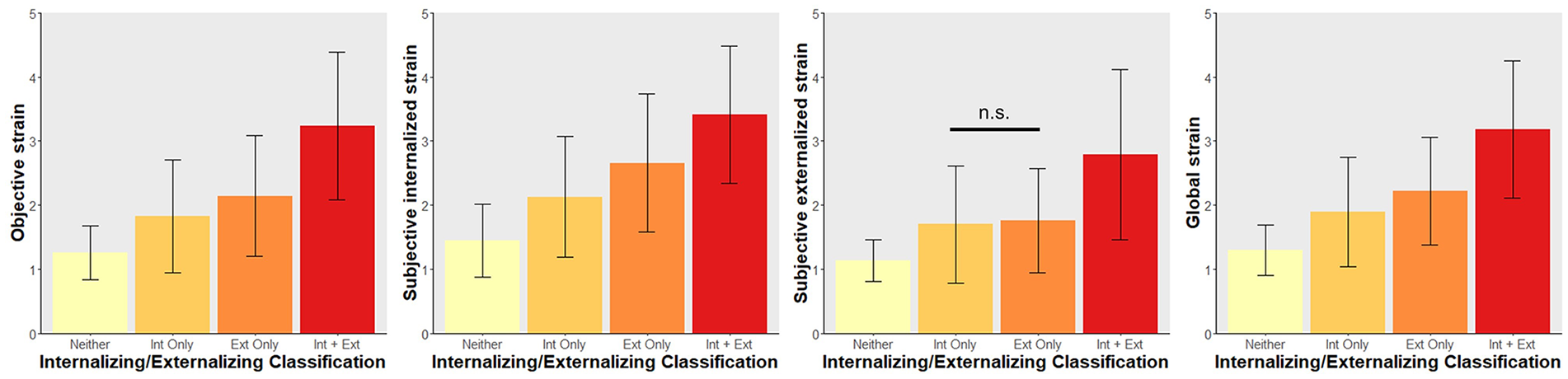
Depiction of means for objective strain, subjective internalized strain, subjective externalized strain, and global strain (left to right) reported by caregivers of children whose symptoms met criteria for neither an internalizing nor externalizing disorder (yellow), an internalizing disorder only (light orange), an externalizing disorder only (dark orange), or both internalizing and externalizing disorders (red).
Discussion
In a large, nationally representative sample of caregivers of school-age children, we found initial evidence for the reliability, validity, measurement invariance, and three-factor structure of the CGSQ-SF11. Support for convergent validity was provided by a consistent pattern of positive correlations between all types of caregiver strain and all forms of child psychopathology symptoms (i.e., depression, ODD, CD, ADHD, anxiety) as well as child impairment. Results are discussed and interpreted below.
The three-factor model (consisting of objective, subjective internalized, and subjective externalized strain) supported by the present results is consistent with previous research on the factor structure of the original CGSQ (Brannan et al., 1997; Kang et al., 2005; Khanna et al., 2012). We also tested a one-factor model, since a “global strain” score is commonly used in previous research and also represents a more parsimonious model. We found that this model fit the data reasonably well, but not as well as the three-factor model. These results suggest that scores on each of the CGSQ-SF11 subscales as well as the global strain score can be used as indices of caregiver strain. Although results were similar across each of the three CGSQ-SF11 subscales, the presence of some differences suggests the potential value of examining subscale scores separately.
Results also provided ample evidence of measurement invariance of the CGSQ-SF11 across child age, child sex, caregiver age, caregiver sex, and child psychopathology. Although previous research has examined whether responses on the CGSQ differ according to certain demographic factors (e.g., Kang et al., 2005), we are unaware of any previous research that has directly tested measurement invariance of the CGSQ across different demographic or clinical groups. Based on the results, the CGSQ-SF11 appears to function similarly for younger versus older school-age children, male versus female children, younger versus older caregivers, and male versus female caregivers. In terms of child psychopathology, the finding that the CGSQ-SF11 has a similar factor structure and measurement properties across clinical versus nonclinical groups suggests that the caregiver strain construct is just as relevant to caregivers of children with subclinical levels of symptoms as it is to caregivers of children with clinical levels of symptoms.
Results indicating high internal consistency of the CGSQ-SF11 and its three subscales are consistent with previous research indicating excellent reliability for the original 21-item CGSQ, particularly the objective strain and subjective internalized strain subscales. A recent review even suggested that the exceedingly high internal consistency values for the CGSQ indicate that some of its items may be redundant and that a shortened questionnaire would be warranted (Holly et al., 2019). The present study provides a shortened questionnaire, without sacrificing reliability. Consistent with previous research, we found slightly lower internal consistency for the subjective externalized strain subscale relative to the other subscales. However, internal consistency for this subscale was still very good (α = .88) and was above the range of internal consistencies found for the subjective externalized strain subscale on the original CGSQ (Holly et al., 2019), suggesting that the omission of one of the four items from the original subscale may have contributed to improved reliability.
Turning to the associations between caregiver strain and demographic factors, results indicated that caregiver age, caregiver sex, and child sex were related to caregiver strain. First, caregiver age displayed very weak negative correlations with objective, subjective externalized, and global strain, potentially reflecting age-related declines in negative affect (Shallcross et al., 2013). Second, male caregivers reported higher externalized strain than female caregivers, a finding that is somewhat at odds with previous research indicating lower subjective internalized and externalized strain among male caregivers (Fawley-King et al., 2020). This divergence may be at least partly explained by the fact that caregivers in the present study identified themselves as the primary caregiver for their child, whereas Fawley-King et al. (2020) did not specify that participants were primary caregivers. Males are generally less likely than females to occupy the role of primary caregiver (e.g., Gamble & Roberts, 2005), and it is likely that nonprimary caregivers experience less strain due to spending less time in direct caregiving activities or having fewer caregiving-related responsibilities. Thus, a lower likelihood of occupying the role of primary caregiver may account for previous findings of lower strain in male caregivers, rather than caregiver sex per se. Higher levels of subjective externalized strain among male caregivers in the present study may reflect a generally greater tendency among males to express anger and related emotions (Chaplin, 2015). Finally, caregivers of males reported higher strain across all three types of strain as well as global strain, largely consistent with previous findings (Bussing, Gary, et al., 2003; Bussing, Zima, et al., 2003; Fawley-King et al., 2020). Higher levels of strain among caregivers of males may be due to higher rates of psychopathology in school-age males compared with females (driven in large part by higher rates of externalizing disorders; P. Cohen et al., 1993), an interpretation that was supported by follow-up analyses (see Table S3 and S4 [available online] in Supplemental Material). This disparity may be more pronounced in preadolescent children because it is not until adolescence that females surpass males in terms of rates of psychopathology (P. Cohen et al., 1993). Thus, caregiver age, child sex, and caregiver sex are important variables to consider when assessing caregiver strain. However, the effects associated with these demographic factors were small, in contrast with the larger effects associated with child psychopathology and impairment.
Consistent with previous research (e.g., Bussing, Gary, et al., 2003), all types of caregiver strain were positively correlated with child symptoms of depression, ADHD, ODD, CD, and anxiety, as well as with child impairment and need for treatment. Moreover, comparisons of the correlation strengths between caregiver strain and symptoms of different forms of psychopathology yielded some noteworthy patterns. Across all three caregiver strain subscales, depression and ODD exhibited the strongest correlations, while anxiety exhibited the weakest correlations. ADHD and CD exhibited less consistent associations: ADHD was just as strongly correlated with objective and subjective internalized (but not externalized) strain as depression and ODD, and CD was just as strongly correlated with subjective externalized (but not objective or internalized) strain as depression and ODD.
The finding that depressive symptoms exhibited such strong correlations with caregiver strain was striking, since previous research has suggested that externalizing symptoms are stronger contributors to caregiver strain than internalizing symptoms (Brannan & Heflinger, 2006). However, this research combined depressive and anxiety symptoms into a single internalizing category, potentially obscuring differences in the strength of associations for depressive versus anxiety symptoms, which in the present study were substantial (see Table 6 and Figure 1). Our findings align with previous research that examined symptoms within separate diagnostic categories. For example, Bussing, Zima, et al. (2003) found that depression was associated with subjective internalized and externalized (but not objective) strain, while Bussing, Gary, et al. (2003) found that depression was associated with all types of strain (including global) except for subjective externalized strain. Thus, previous research suggests reliable correlations between child depression and subjective internalized strain, while correlations with objective and externalized strain do not appear as reliable. From this perspective, then, the strong correlations between child depression and all types of caregiver strain in the present study are slightly surprising. The consistently strong correlations should, however, be considered from a developmental perspective. The average age of onset for depression is during adolescence, which is later than the average age of onset for the other disorders investigated in the present study (i.e., anxiety, ADHD, ODD, CD; Kessler et al., 2007; Merikangas et al., 2010; Ormel et al., 2015). Thus, it may be that the presence of elevated depressive symptoms in school-age (i.e., predominantly preadolescent) children indicates a particularly severe course of depression and one that distinguishes the child from same-age peers to a greater extent than elevated levels of anxiety, ADHD, ODD, or even CD. Thus, depression in children of this age group may be particularly salient and troubling for caregivers. Future research should explore this possibility by examining whether associations between child depressive symptoms and caregiver strain are weaker among caregivers of adolescents, given higher prevalence rates and more common onset of depression during adolescence (Kessler et al., 2007).
The consistently strong correlations between child ODD symptoms and all types of caregiver strain echoed previous findings (e.g., Tsai et al., 2015). Child ADHD symptoms, however, exhibited more variable correlations with caregiver strain. We found evidence of a weaker association between ADHD symptoms and subjective externalized strain compared with other types of strain. Moreover, the association between ADHD and subjective externalized strain was no longer significant after controlling for other forms of psychopathology. These findings are generally consistent with previous research. Multiple studies have failed to detect significant associations between ADHD symptoms and subjective externalized strain, despite finding significant associations with other types of strain (Bussing, Gary, et al., 2003; Bussing, Zima, et al., 2003). Other studies have found that the associations between ADHD and caregiver strain are accounted for by symptoms of other disorders that commonly co-occur with ADHD (i.e., ODD, CD; Babinski et al., 2019; Evans et al., 2009).
Child CD symptoms were as strongly correlated with subjective externalized strain as child depression and ODD symptoms, consistent with research indicating a positive association between CD and parental hostility (Hoeve et al., 2009). The finding of relatively attenuated associations between child CD symptoms and other types of caregiver strain (i.e., relative to depression) may seem surprising on its face, since the behaviors associated with CD (e.g., robbery, fire-setting) can be so severe and harmful. However, this pattern overlaps partially with that identified in previous studies, which have either failed to detect any associations between CD and strain (Bussing, Gary, et al., 2003), or found inconsistent or relatively weak associations. Notably, one study found that CD symptoms were associated with objective strain but not the other two strain factors (Bussing, Zima, et al., 2003), and another study found that strain appeared to be more strongly associated with ODD compared with CD (Tsai et al., 2015). Moreover, in a study that found that ODD and CD symptoms mediated the effect of ADHD on global strain, the mediating effect was stronger for ODD compared with CD symptoms (Babinski et al., 2019). Multiple factors might account for why CD symptoms are not more strongly associated with objective, subjective internalized, and global strain. First, many symptoms of CD are, by definition, expressed outside of the home (e.g., breaking into someone else’s property, shoplifting); thus, caregivers may be more removed from the effects of these symptoms compared with those that are likely to manifest strongly in the home (e.g., defiance of caregivers’ rules in ODD). Second, CD is associated with reduced parental monitoring (Hoeve et al., 2009), which may reflect lower levels of supportive involvement among caregivers of children with CD. Caregivers who are less engaged with their children might naturally experience less strain in the context of problematic child behaviors (e.g., less worry resulting from behaviors such as staying out late into the night).
Child anxiety was most weakly associated with all four measures of caregiver strain, which is fairly consistent with multiple studies that have detected significant associations between strain and a range of child psychopathology symptoms, but not child anxiety (Bussing, Gary, et al., 2003; Bussing, Zima, et al., 2003). The weaker correlations for anxiety observed in the present study may be explained by research showing that anxiety disorders are among the most common and least severe (at least in terms of psychosocial impairment and the presence of severe distress) forms of psychopathology in youth (Ormel et al., 2015).
Finally, child impairment indices were less strongly associated with subjective externalized strain compared with other types of strain. In terms of total impairment, it appears that although impairment is strongly associated with global strain and, in particular, emotional consequences such as sadness, it may be less strongly associated with emotional consequences such as anger. It is possible that caregivers’ recognition that their child is struggling across multiple domains of functioning helps mitigate the impression that the child is having emotional problems or acting out intentionally—attributions associated with the experience of anger (Smith & Lazarus, 1993). In terms of need for treatment, this finding could be interpreted as paralleling previous research suggesting that higher subjective externalized strain is associated with higher rates of dropout from treatment (Foster, 1998). It may be that caregivers with higher levels of anger and related emotions attribute fault for the child’s problems to the child, and instead of perceiving them as needing help, they perceive them as bearing responsibility for changing their own emotional and behavioral problems.
Turning to number of child disorders, the finding that caregiver strain showed a linear increase as the number of child disorders increased is generally in line with previous research (e.g., Rockhill et al., 2013). Moreover, the finding that the breadth of child symptoms (i.e., the presence of clinically significant symptoms spanning both the internalizing and externalizing domains of psychopathology) was associated with the highest levels of strain mirrors previous findings (Vaughan et al., 2013). Within these analyses, strain was generally higher among caregivers of children with externalizing symptoms only compared with internalizing symptoms only, which is also consistent with previous research (Brannan & Heflinger, 2006). This pattern highlights how internalizing symptoms can appear to be less robustly related to strain than externalizing symptoms when depressive and anxiety symptoms are combined into a single internalizing measure. However, subjective externalized strain was not significantly higher for children with an externalizing disorder only compared with children with an internalizing disorder only. Considering that ADHD was classified as an externalizing disorder and it exhibited notably weaker associations with subjective externalized strain compared with depression, this pattern may be explained by many of the children in the externalizing-only group (i.e., 37.2%) having ADHD only. Additionally, this finding does parallel research indicating a positive association between parental hostility and child symptoms across both internalizing and externalizing domains (Lewis et al., 2014; McKee et al., 2008). Taken together, the conclusion drawn in previous studies that child externalizing symptoms are more strongly associated with caregiver strain than child internalizing symptoms (Brannan & Heflinger, 2006) may be oversimplified. Overall, we found evidence that all three caregiver strain factors appear to be just as relevant for child internalizing symptoms—particularly depression—as child externalizing symptoms.
Before concluding, limitations of the present study should be noted. First, this study was cross-sectional, which constrained our ability to test the temporal and causal relationships between child psychopathology symptoms/impairment and caregiver strain. Second, this study relied exclusively on caregiver reports of both child psychopathology symptoms and caregiver strain. The lack of other informants regarding children’s psychopathology symptoms and impairment (e.g., child self-report, teacher report) may have led to biases in responses (e.g., a negativity bias) that inflated correlations between child psychopathology symptoms/impairment and caregiver strain. Third, since this sample only included children ages 5 to 12 years, more research is needed to examine whether the CGSQ-SF11 exhibits measurement invariance across age groups as well as convergent validity in samples of youth with a wider age range, including preschool-age children and adolescents. Fourth, one of the child psychopathology measures (i.e., the SSCARED) was designed for screening purposes and thus may have had limited specificity to detect the presence of an anxiety disorder; future research should seek to replicate and extend the present findings using more specific diagnostic measures of anxiety disorders (e.g., separation anxiety disorder). Finally, since we used a nonclinical sample, future research should examine the psychometric properties of the CGSQ-SF11 in a clinical sample, particularly to assess its ability to detect changes in caregiver strain over the course of treatment.
One notable strength of the present study was the use of a large, nationally representative sample of caregivers of school-age children, which allowed for several novel contributions not possible in most previous studies on caregiver strain due to their use of clinical samples. First, we were able to examine measurement invariance across clinical groups and provide evidence that the caregiver strain construct as measured by the CGSQ-SF11 is not significantly different among caregivers of children with clinical versus subclinical symptoms of psychopathology. Second, we were able to provide descriptive statistics for the CGSQ-SF11 (see Table 4) that can be used to begin developing clinical cutoff scores for this new measure.
The CGSQ-SF11 has the potential to inform and enhance clinical practice. It is short, minimizing burden on caregiver respondents if administered on a repeated basis over the course of treatment. Furthermore, given the documented associations between heightened caregiver strain and poor treatment outcomes (e.g., treatment dropout), the CGSQ-SF11 can be used to identify and provide targeted support to increase treatment engagement for caregivers who may be at high risk for poor outcomes. Overall, CGSQ-SF11 scores can be used to identify caregivers who might benefit from additional support, skills, and resources to support their efforts as key players in the evidence-based treatment of their children. Finally, as more evidence emerges regarding the ability of the CGSQ-SF11 to detect changes in caregiver strain over time, the CGSQ-SF11 may be a useful tool for assessing progress in treatment as well as a springboard for addressing stressors that emerge during treatment.
In conclusion, the present study provides preliminary evidence that the CGSQ-SF11 is a reliable, valid, and clinically meaningful measure of caregiver strain among caregivers of school-age children. The CGSQ-SF11 has several advantages over existing caregiver strain measures, namely brevity, full construct coverage, and a focus on the present to maximize the ability to detect and track change over time. Additionally, the CGSQ-SF11’s inclusion of the subjective externalized strain subscale may help providers identify caregivers at greater risk for mental health problems, difficulties in the relationship with their child, treatment dropout, and dissatisfaction with treatment. Overall, the CGSQ-SF11 is a promising tool for assessing caregiver strain that has the potential to inform and enhance treatment for children with mental health concerns and their families.
Supplemental Material
sj-docx-1-asm-10.1177_10731911211015360 – Supplemental material for Caregiver Strain Questionnaire–Short Form 11 (CGSQ-SF11): A Validation Study
Supplemental material, sj-docx-1-asm-10.1177_10731911211015360 for Caregiver Strain Questionnaire–Short Form 11 (CGSQ-SF11): A Validation Study by Grace M. Brennan, Dara E. Babinski and Daniel A. Waschbusch in Assessment
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.