
Abstract
The use of AI within psychological assessment has many potential benefits for psychologists and their patients, including improved access to care, workflow efficiency, and expanded clinical training through virtual patients; however, there are also potential risks, including data privacy and security, and introducing potential bias into clinical practice and training. In addition, other risks may be present within clinical training in assessment, including reduced supervisor oversight, cultural insensitivity, and biased or insufficient feedback. This paper presents two case vignettes to review ethical considerations of the use of AI in psychological assessment training and practice within an ethical decision-making framework. Current best practices, ethical guidelines, and potential barriers, as well as considerations for evaluating the use of AI and other technology as an area of competency for trainees are reviewed.
Introduction
Following the American Psychological Association (APA, 2024a) Pulse survey, it was reported in September 2024 that 29% of psychologists had used generative artificial intelligence (AI) in their practice in the previous year, with 11% of psychologists reporting that they use AI tools regularly (more than monthly) in their practice; rates were slightly higher for early career psychologists (41% within the past year, 19% more than monthly), however all practitioners also noted concern for the risk in use of AI technology. As AI technology continues to be developed and increasingly adopted into daily use for many, APA (2024b, 2024c) released a policy statement regarding AI and the field of psychology, as well as specific guidelines for selecting AI tools in practice, and specific ethical guidelines for the use of AI (APA, 2025). In their policy statement, the APA notes the “current and future transformative impacts present in artificial intelligence (AI) technologies,” and outlines domains in which psychology can impact the application of AI technology both within and outside of the field as a whole: Societal impact, promotion of health and wellbeing, and upholding ethics and privacy. Within these domains, psychologists are uniquely positioned to integrate processes into AI use and related policy creation that center equity and the reduction of bias, media literacy and combating mis/disinformation, ethics and human rights, and science and evidence-based practice (APA, 2024b).
AI tools have become increasingly accessible, including multiple tools designed for psychological and other health care practices, and, more recently, AI writing tool incorporation into online psychological assessment resources (see, for example, PAR AI Report Writer). Given these rapid changes in accessibility and improvements in a technology that is constantly learning from input data, it is clear that the use of AI is gaining stronger traction among psychologists (Abrams, 2025), placing them in the unique role of both guiding health care fields in ethical considerations to be made when incorporating the use of the tools into clinical practice, while also incorporating them into their own practice for assessment and treatment.
Potential Impact of AI on Psychological Practice
Nearly half of the U.S. population lives in a mental health professional shortage area, particularly those in rural areas (Kuehn, 2022), with child and adolescent populations being particularly impacted by a lack of access to care (Abramson, 2022). Psychologists report increased demand for services, and diminished capacity to provide them due to multiple barriers to care (APA, 2024a), as well as challenges in practice, and about 40% of psychologists in academic health care settings reporting being at full capacity or overextended in their practice (Williams et al., 2020). Although rates of self-reported clinician stress and burnout have reduced somewhat since the height of the COVID-19 global pandemic, 36% of psychologists completing the APA (2024a) Pulse survey continued to report burnout, with early career psychologists reporting burnout and stress at higher rates (51%) than mid or late career psychologists. Moreover, in their 2025 report, the Council of University Directors of Clinical Psychology Burnout Task Force reported that two-thirds of trainees in clinical psychology doctoral programs reported emotional exhaustion burnout, and nearly half of the trainees reported at least moderate symptoms of depression (Hunt et al., 2025). Technology can, and has, eased this burden somewhat with the more consistent use of tools such as electronic health records, telehealth, and, more recently, the use of generative AI tools. The use of AI in clinical practice has the potential to ease the burden on psychologists in areas related to practice management and administrative tasks, as well as clinical note taking, report generation, and summarization. In addition, AI has a long history and transformative future within psychology in areas related to clinical training, psychological assessment, treatment, and decision-making (Luxton, 2014). However, the use of AI also brings potential risks to clinicians, trainees, and their patients that result in complex ethical considerations, including issues related to privacy and confidentiality, data security, and bias (Farmer et al., 2025; Shymko & Babadzhanova, 2025).
This paper reviews ethical considerations that should be made when deciding whether, or how, to incorporate the use of AI into psychological assessment training and practice. A brief review of ethical decision-making models is presented, followed by a description of the socially responsive ethical decision-making model (Juntunen et al., 2023), which will be the primary decision-making framework used in this manuscript to evaluate ethical considerations. Two fictional case vignettes will be presented to review the use of this model within psychological assessment. The first vignette will address the use of AI tools in training graduate-level students in the use of psychological assessment. The second will examine ethical considerations in the use of AI tools for clinical practice in psychological assessment. The intent of the vignettes is to highlight ethical decision-making strategies and all details, including names, scenarios, and AI tools, were fabricated for educational purposes. The paper will conclude with a summarization of current guidelines and best practices to implement when utilizing ethical decision-making to determine how to incorporate AI tools into teaching and practice. Throughout this paper, “AI” will refer to tools using machine learning, natural language processing, large language models, and generative artificial intelligence.
Ethical Decision-Making
Ethical codes are often intentionally vague to allow for interpretation by multiple types of providers in various situations across the field; therefore, ethical decision-making models provide a framework for analyzing ethical issues that may arise, allowing the individual to review relevant ethical principles and standards as they apply to their specific situation. Ethical decision-making models may apply to any number of situations in psychological practice, training, and research, and are critical elements of knowledge for both psychologists and trainees (Barnett et al., 2007; Fehr et al., 2017). There are many evidence-based models of ethical decision-making available within psychology (Knapp et al., 2017; Koocher & Keith-Spiegel, 2008; Pope et al., 2021; Welfel, 2016), all of which include similar steps of (a) identifying stakeholders; (b) reviewing the APA Ethical Principles of Psychologists and Code of Conduct (“APA Ethics Code;” APA, 2017) and other relevant laws and regulations; (c) determining possible courses of action, including consultation and assessment of potential consequences; (d) make a decision for how to proceed; and (e) monitor and evaluate outcomes, modifying as necessary. When considering ethical dilemmas, psychologists seek to adhere to the overall general principles of the APA Ethics Code (Beneficence and Nonmaleficence, Fidelity and Responsibility, Integrity, Justice, and Respect for People’s Rights and Dignity), as well as relevant standards within the 10 sections of the Ethics Code. When considering ethical issues within the use of AI tools, the standards most frequently referenced include Competence (Section 2), Human Relations (Section 3), Privacy and Confidentiality (Section 4), Education and Training (Section 7), Assessment (Section 9), and Therapy (Section 10).
In addition to the application of the APA Ethics Code in decision-making, the APA’s Mental Health Technology Advisory Committee established ethical guidelines for the use of AI in professional practice, a document that was supported by APA’s Office of Health Care Innovation and adopted by the APA Ethics Committee (APA, 2025). These guidelines are intended to highlight six primary areas of consideration for practitioners, in addition to the broader considerations of the Ethics Code and other regulations: (a) Transparency and informed consent, (b) mitigating bias and promoting equity, (c) data privacy and security, (d) accuracy and misinformation risks, (e) human oversight and professional judgment, and (f) liability and ethical responsibility. Within each of the primary areas, the authors provide specific recommendations for health service psychologists, including detailed informed consent processes, evaluating tools for potential bias before use as well as for issues that may arise while using these tools, working to build representative and comprehensive databases that may be used to enhance AI training, actively engaging in human oversight including monitoring AI tool output, patient use, and critical evaluation of the impact of AI use on clinical care and administrative tasks, and maintaining familiarity with regulations around data security, including HIPAA compliance, and monitoring to ensure this is maintained with use of the AI tools. The authors also note that, given the continued and rapid growth of AI use and policy, health service psychologists must maintain awareness of potential legal risks and other issues of liability as this obligation ultimately rests on the psychologist.
One model to determine whether an issue is ethical or related to another area of practice settings is the “four bin” approach (Behnke, 2014). In this model, psychologists determine whether issues fall into one of four bins: Legal, Ethical, Clinical, or Risk Management. Haug and Ghandi (2021) added a fifth bin to this model, the Socio-Cultural bin. When assessing situations, the Legal bin refers to any issues that may be relevant to laws and regulations at any level (federal, state, province, territory), the Ethical bin is for anything relevant to the APA Ethics Code or the “right” thing to do, the Clinical bin is for any issue related to treatment or assessment, the Risk Management bin holds any issues that may increase or decrease exposure to liability, and the Socio-Cultural bin refers to any influence of intersectional identities, including systemic and power dynamics. In addition to applying the five bin approach where applicable for issues that are more directly related to legal or risk concerns, the ethical decision-making model used primarily in this paper is the Socially Responsive Ethical Decision-Making model (SREDM; Juntunen et al., 2023). This model has seven steps to the decision-making process and incorporates socio-cultural influences throughout the decision-making process, as described in Table 1.
SREDM Framework.
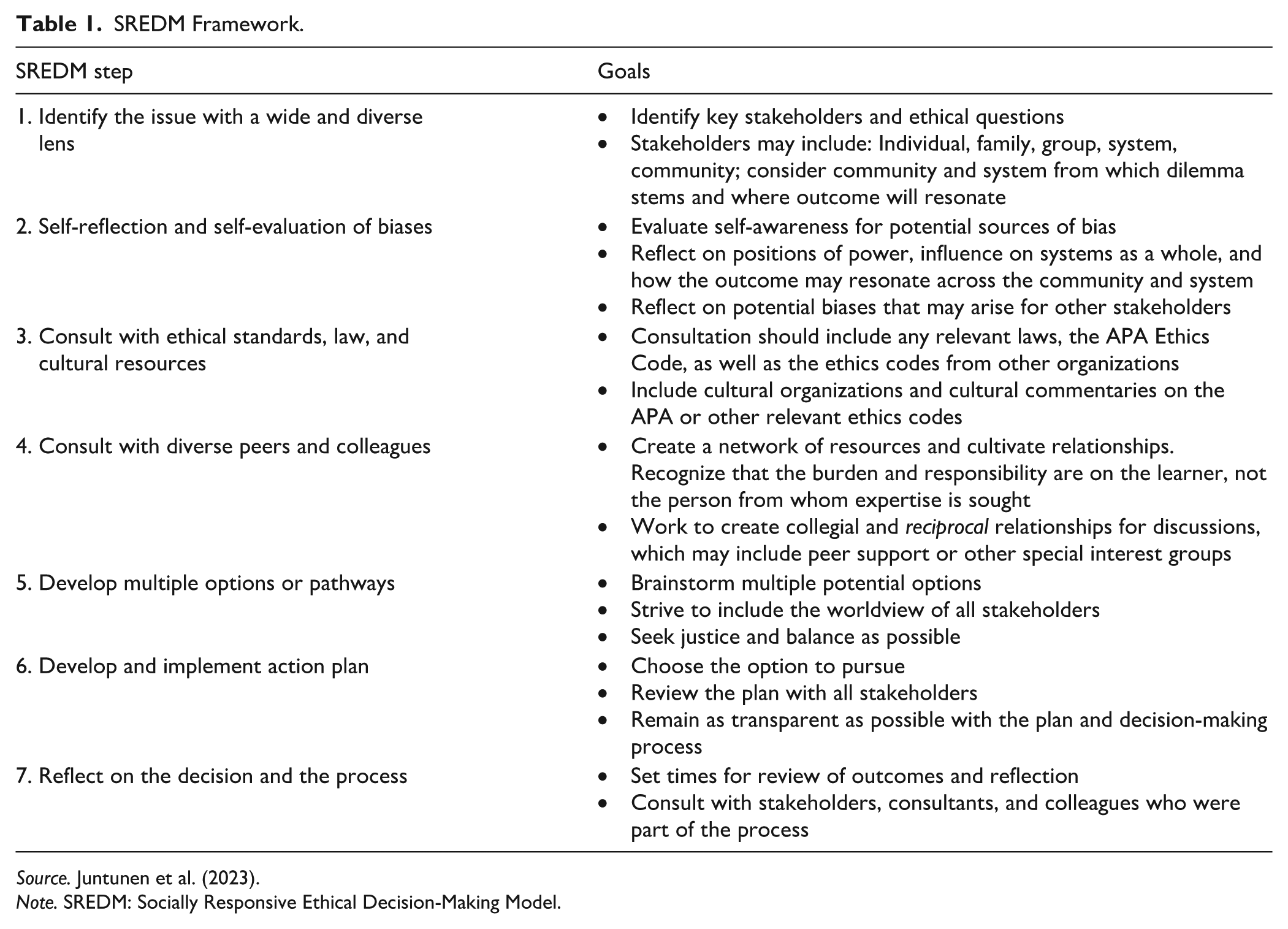
Source. Juntunen et al. (2023).
Note. SREDM: Socially Responsive Ethical Decision-Making Model.
AI and Clinical Training
AI tools may be used in various ways in clinical training, including creating simulated patient interactions, providing initial feedback and supervision for treatment and assessment, completing administrative tasks, and providing training in culturally adapted interventions (Sheperis & Sadeh-Sharvit, 2023). Use of AI tools in education can supplement teaching by acting as a teacher, a learning partner, and a domain expert; however, these systems are also continuously learning from data input into the AI model (Hwan & Chen, 2023). When using AI in clinical training, trainee development (i.e., pre-practicum, initial practicum or client experiences, advance practicum, or internship rotation) must be taken into consideration. As students progress through their training and become more independent with clinical skills they may begin to utilize AI tools with increasing independence; however, personal oversight, feedback, and supervision are critical in the early development of clinical skills. This training not only allows students increased confidence and security in their skills, but it also allows them to effectively and comprehensively evaluate the output of AI tools when used. Developmental considerations for trainees may include “hands-on” training in how to use AI tools ethically and effectively; for example, training in how to write effective prompts and in evaluating both input and output from AI-generated reports and summaries (Liu et al., 2024). Furthermore, training in how to document the use of, or prohibition of, AI in teaching, research, and clinical work can be beneficial to students as they become more independent in their practice, teaching them how to analyze whether AI is being used ethically and transparently (Overono & Ditta, 2024).
Case Vignette
Jordan is a first-year doctoral student in clinical psychology, learning to conduct comprehensive psychological assessments. The training program has recently introduced an AI-powered tool called “AssessmentAssist” that creates virtual patients to allow students to complete an intake interview, create a test battery, and input mock test data and behavioral observations from practice administration with peers asked to role-play as the patient presented in the intake interview. The tool then assists the students by walking through examples for how to analyze test protocols and generate preliminary interpretations, and suggests diagnostic impressions and recommendations based on assessment data. Jordan has been assigned an evaluation using AssesmentAssist for a 12-year-old virtual patient, Marcus, referred for academic difficulties and behavioral concerns. Jordan practices administering a cognitive measure and academic achievement measure with a peer role-playing as Marcus, then assigns behavioral observation rating forms and completes a clinical interview with Marcus through AssessmentAssist. The AI tool generates a narrative interpretation of cognitive strengths and weaknesses, suggests diagnostic impressions (specifically ADHD-Combined Presentation and possible specific learning disorder), and provides recommendations for school accommodations. Jordan is impressed by how professional the output looks and incorporates large sections into the draft report for their assignment. In addition, the AI tool generates transcripts of the interactions between the clinician and virtual patient for the supervisor to review and includes a suggested rating and grade based on competencies established by the clinical program.
Ethical Considerations
This case vignette raises multiple areas to be evaluated related to clinical training: Development of competency in clinical skills, assessment and diagnostic skills, cultural competency, and technological competency (including specific direction on when and how to incorporate AI use), developmental level of the trainee, issues related to providing supervision and feedback, and patient autonomy. Table 2 outlines ethical questions within the SREDM framework. The initial step is to identify the issue and all key stakeholders. At this stage of training, current key stakeholders include Jordan and their supervisor; however, the training in the AssessmentAssist model may also impact the future patients Jordan sees in more advanced practicum rotations and, eventually, in their clinical practice, such that supervision should include direct feedback using the transcripts from the virtual patient interaction as well as discussions about considerations Jordan will make as they begin to see patients in their future clinical practice with actual patients. Furthermore, consideration should be given to the research into the use of the tool itself, which can have implications for the educational program. When evaluating bias, as with the introduction of any new educational or technological approach, transparency in the use and reasoning behind the use can be beneficial and guide discussions related to awareness of biases. For example, while Jordan may be impressed by the output of the AssessmentAssist report, they may have concerns about how the feedback from this report may be used by their supervisor. Similarly, the supervisor’s grading process may be easier using the AI-generated feedback, but this may also bias their evaluation of Jordan’s work. Clear expectations and guidelines for how feedback will be used, reviewed, and provided, in addition to personal supervision and feedback, will be necessary to ensure thorough evaluation of Jordan’s development in clinical assessment skills as they are in the initial stages of training. Finally, addressing anxiety around the use of AI for the student clinician, supervisors, and other program stakeholders may also be beneficial in discussing potential biases, ideally reducing bias or anxiety by correcting inaccurate beliefs (Sheperis & Sadeh-Sharvit, 2023).
SREDM Framework Case Vignette 1.
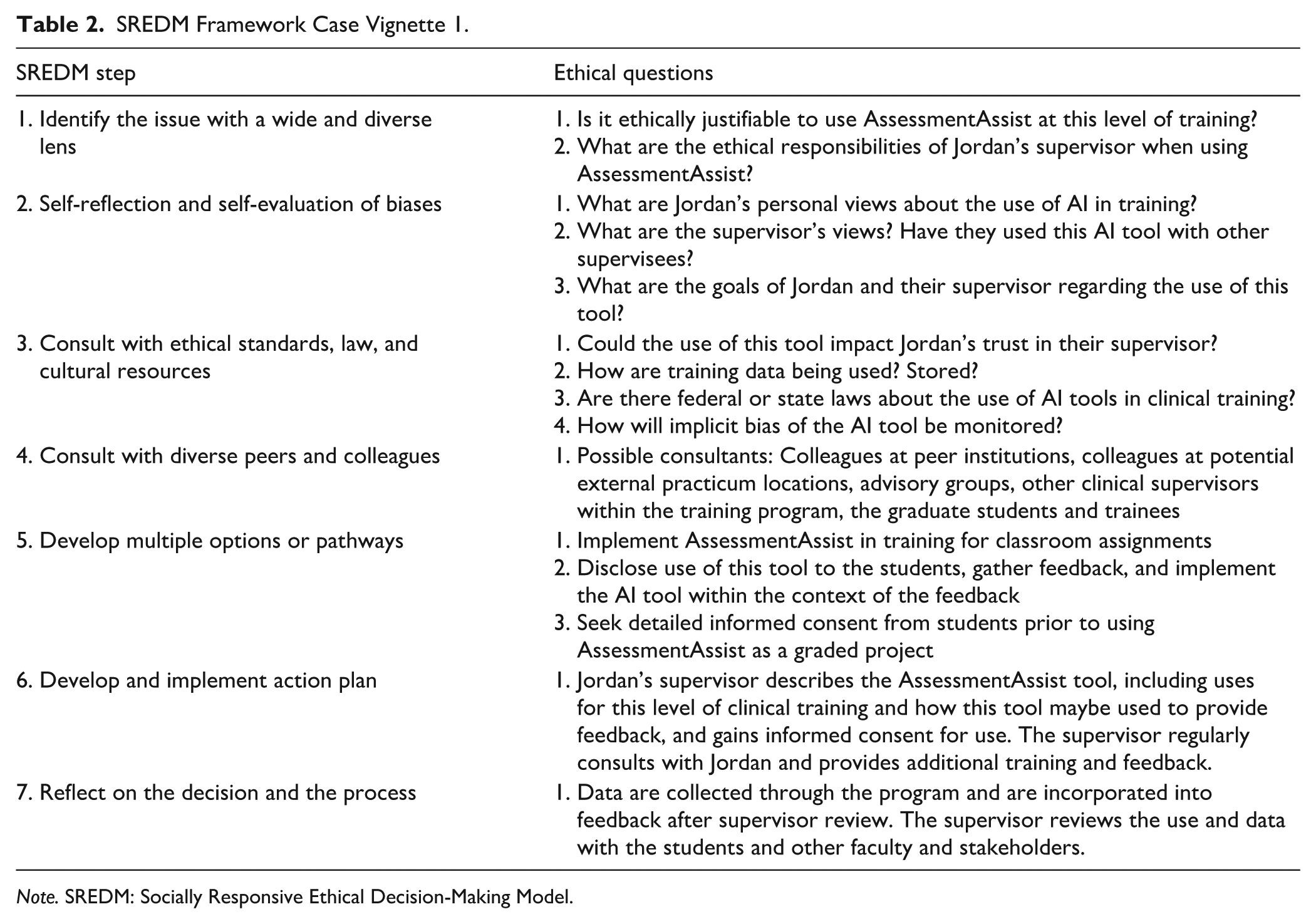
Note. SREDM: Socially Responsive Ethical Decision-Making Model.
When consulting ethical standards, laws, and cultural resources, initial considerations are to determine the appropriate bins for each area. For example, supervisors must consider any potential federal or state laws that may impact their use of AI tools in training, and advise their students into engaging in similar monitoring as they transition to work with clinical populations, as this is rapidly changing as states are developing, introducing, or passing laws related to the use of AI in clinical practice (see, e.g., the Wellness and Oversight for Psychological Resources Act of Illinois). In addition, should concerns arise for the use of AssessmentAssist as an evaluative tool, one key risk management question would be to determine liability and whether this may be held by the supervisor, program, AssessmentAssist developer, etc. For example, the supervisor may be advised to have clear benchmarks for evaluation, including how they will review the transcripts and feedback provided by the AI tool, should Jordan have questions regarding the impact on their grade or other feedback on their performance. Another consideration is whether the university, program, or training clinic has specific policies or guidelines around the use of AI to which the faculty and students must adhere. Ethically, considerations must be made for all Principles of the APA Ethics Code (APA, 2017) such as taking steps to: Determine if the program (a) is beneficial to the students, supervisors, and future patients (Principle A) while minimizing potential harm, such as inadequate or inaccurate provision of feedback; (b) may be used within a relationship of trust between supervisor and supervisee and how the supervisor maintains their professional obligation to Jordan and their training (Principle B); and (c) promotes accuracy, honesty, and transparency in the supervision and feedback process (Principle C) while maintaining student rights to privacy and confidentiality (Principle E) and monitoring for potential bias (Principle D) or risk to vulnerable populations (i.e., the students and their future patients; Principle E).
Further, specific relevant Standards of the APA Ethics Code to evaluate include Competence (Section 2), specifically to ensure the supervisor is providing training within their Boundaries of Competence (2.01) and that they are monitoring to ensure that the work of their trainees is performed competently (2.05), Human Relations (Section 3), specifically ensuring that the supervisors are avoiding potential harm (3.04) and engaging in informed consent processes with their trainees and future patients (3.10), and Education and Training, ensuring that accurate descriptions were provided for the use of AI in training (7.02), and that there is transparency in the supervision process (7.06). One frequently cited area of anxiety around the use of AI for students, supervisors, and clinicians is the ability to maintain Privacy and Confidentiality (Section 4; Hutnyan & Gottlieb, 2025). When using AI, specific care must be taken to evaluate and understand how data are being stored, how data will be used (i.e., for internal use only, to train the AI tool, etc.), and how data provided will be used in the relevant context, including how data may be used to evaluate trainee competence, understanding, clinical skills, and performance, as well as how they may be used to determine grades or other evaluative measures. These issues around data security apply both to the training environment as well as to future patient care in clinical training and practice environments and should be discussed throughout the process. Not only would it be recommended for Jordan’s supervisor to discuss these issues related to AssessmentAssist and how their data will be stored and used within the clinical training program, it is also recommended that Jordan’s supervisor review with them how to evaluate future AI tools to determine how the developers are implementing data security including evaluating how data are stored, how tools maintain patient confidentiality, and how HIPAA compliance standards are evaluated, met, and maintained.
In addition to maintaining adherence to the ethical principles and standards, it is also important that Jordan and his supervisor engage in training to evaluate potential bias that may be inherent in the AI-generated evaluation report, with the goal of teaching the necessity of human oversight of AI-generated products, implementing clinical judgment and critical review of AI-generated report output, and training in how to adapt AI or other recommendations to match the needs, capabilities, and capacity of the patient when using AI tools in future clinical settings. As Jordan and their supervisor discuss future application of AI tools based on their training with AssessmentAssist as a virtual model, it will be important to include education that addresses these areas of potential biases. More specifically, AI models are trained on existing data that may hold historical and systemic bias and therefore training to evaluate for potential bias should be inherent in the learning process. Farmer and colleagues (2025) propose several steps for considering potential bias when using AI tools for psychological assessment, intervention, and other uses including evaluating the degree to which multiple factors are considered in the AI-generated reports. These factors include patient demographics, intersectional identities, over- or under-emphasis of demographic and cultural information, how data will be used and protected, alignment of evaluation, intervention, and diagnosis with patient values, and whether the use of AI promotes or discourages accessibility and other potential health care disparities. The authors provide a comprehensive outline of considerations for practitioners and trainees as well as for companies developing AI tools.
Following consideration of multiple potential options that range from refusing to use AssessmentAssist as a training program to using the tool with informed consent of the students, Jordan’s supervisor develops and implements an action plan to use AssessmentAssist as an early tool for training clinical assessment skills in their program. The supervisor discloses the decision-making process behind using this AI tool (allowing students initial practice with various clients, getting feedback from the model on clinical interviewing and differential diagnosis skills, providing examples in crafting beneficial recommendations, and improving readability and accessibility of psychological reports), and provides information on how training data will be stored and used by the program and AssessmentAssist developers. Jordan and their supervisor will meet regularly to discuss feedback provided by AssessmentAssist and how to interpret, analyze, and adapt the AI-generated report information, including training on how to match the virtual patient needs and goals with specific recommendations. All data used for feedback or provided for grades or other evaluation will be reviewed by the supervisor prior to inclusion in evaluative measures. As they reflect on the decision and process, Jordan and their supervisor agree to this approach and continue to discuss any adjustments needed throughout the semester. In addition, training will include strategies for implementing these methods with future patients in direct clinical settings.
Overall, AI has shown promising use in clinical training, including increased diagnostic accuracy and improved counseling microskills in mental health fields (Sheperis & Sadeh-Sharvit, 2023), as well as to be beneficial in health care clinical training settings (Ko et al., 2025); however, competent training, supervision, and intentional education, including evaluating ethical concerns, in the use of AI is warranted (Hutnyan & Gottlieb, 2025; Perle et al., 2025).
Case 2: Clinical Assessment Practice
There is potential for psychologists to use AI tools in their clinical practice to relieve some of the significant administrative burdens they experience that may lead to additional stress and burnout. In psychological assessment, report-writing is essential to convey evaluation findings; however, it is also fraught with issues that are challenging for both providers and patients. For providers, the process of scoring measures, interpreting results, and writing evaluation reports is time-consuming and often not included in productivity assessments, billable hours, or insurance reimbursement. For patients, accessibility to the data within the reports has been a long-standing challenge for psychologists, including issues with length, readability, and focusing solely on scores or computer-based generated narratives rather than integrating the scores within the broader patient context and life-experiences (Groth-Marnat & Horvath, 2006). Each of these broader challenges may be improved with the use of AI tools; however, continued psychologist oversight and interpretation remains required as psychological assessment should integrate evaluation data into the patient’s current situation, including evaluation of cultural and community factors (Wright et al., 2021). Furthermore, there is evidence to suggest that AI may also be used to address concerns with accurately evaluating client contextual factors beyond behavioral rating scales by using AI tools to evaluate natural language processing and communication (Kjell et al., 2024).
To further evaluate the efficacy of AI written psychological reports, Lockwood et al. (2024) evaluated the performance of generative AI and human psychologists when provided the prompt to write a comprehensive psychological report that included a Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) diagnosis and recommendations based on mock child assessment data that include developmental history, clinical interview data, behavioral observations, and psychometric test data. Data were collected via survey and the reports were reviewed by blinded content experts. The authors found that the human-generated reports took, on average, about 2.5 hours to write, while the AI-generated reports took approximately 91.5 seconds to complete. Human-generated reports were rated higher overall for writing – style, organization, and summarization; however, AI-generated reports were rated higher for quality of recommendations, although all effect sizes were small. This study suggests that, while psychological review will still be necessary, there is some promise to the benefit of AI tools in reducing the administrative burden of report-writing.
Case Vignette
A licensed clinical psychologist, Dr. Mas, has been using an AI-powered assessment tool called “PsychEval AI” to help analyze protocols and generate interpretive reports, as well as to provide initial diagnostic suggestions and recommendations. They find this tool saves significant time and provides comprehensive narrative reports that they review and modify before finalizing. One of their clients, Elena, a 28-year-old woman, is referred for a psychological evaluation due to concerns about challenges with productivity at work. Dr. Mas conducts a clinical interview and administers measures for a comprehensive evaluation. They input the client data into PsychEval AI, which generates a 15-page interpretive report suggesting “significant pathology” and “impaired cognitive functioning.” Dr. Mas reviews the AI output and notices some interpretations are overly pathologizing and do not take into consideration contextual factors, and that significant discrepancies among cognitive scores (specifically that verbal and perceptual reasoning skills are above average, but Elena’s working memory and processing speed skills are slightly below average for her age) are present but unaccounted. Dr. Mas is under time pressure to complete the report for Elena’s upcoming job performance review and modifies a few sections, but keeps most of the AI-generated language and diagnostic impressions.
Ethical Considerations
This case presents a number of ethical concerns that may arise in clinical assessment practice, including issues related to informed consent, accuracy in assessment, minimizing harm to patients, fidelity to the patient and practice, competence, cultural competency, professional deskilling, and transparency of the AI tool. Table 3 outlines ethical questions within the SREDM framework. In identifying the ethical dilemma, key stakeholders are Elena and Dr. Mas, as well as Elena’s employer and the broader community, as future patients may be impacted should Dr. Mas utilize PsychEval AI for psychological evaluations, as such evaluations can be used to determine various personal situations including employment, accommodations, education, and treatment. Potential areas of bias on which to reflect include evaluating biases held by Dr. Mas, Elena, Elena’s employer, and inherent bias within the PsychEval AI tool. For example, key reflections in this scenario may emphasize the motivation of Dr. Mas to use the PsychEval AI tool, such as a reduction in documentation time at work, being over capacity within their practice, or attempting to maximize the number of evaluations they can complete. For the AI tool itself, data output may be influenced by data used in training the generative AI, requiring additional evaluation by Dr. Mas if the demographic data used in training the model differ from the demographic identities held by Elena. These biases may also result in misdiagnosis or over-pathologizing of symptoms if not evaluated within the client’s individual background. In addition, consideration must be made of the beliefs of Elena and her employer around the use of AI within clinical assessment, including whether they were made aware of the use of this tool.
SREDM Framework Vignette 2.
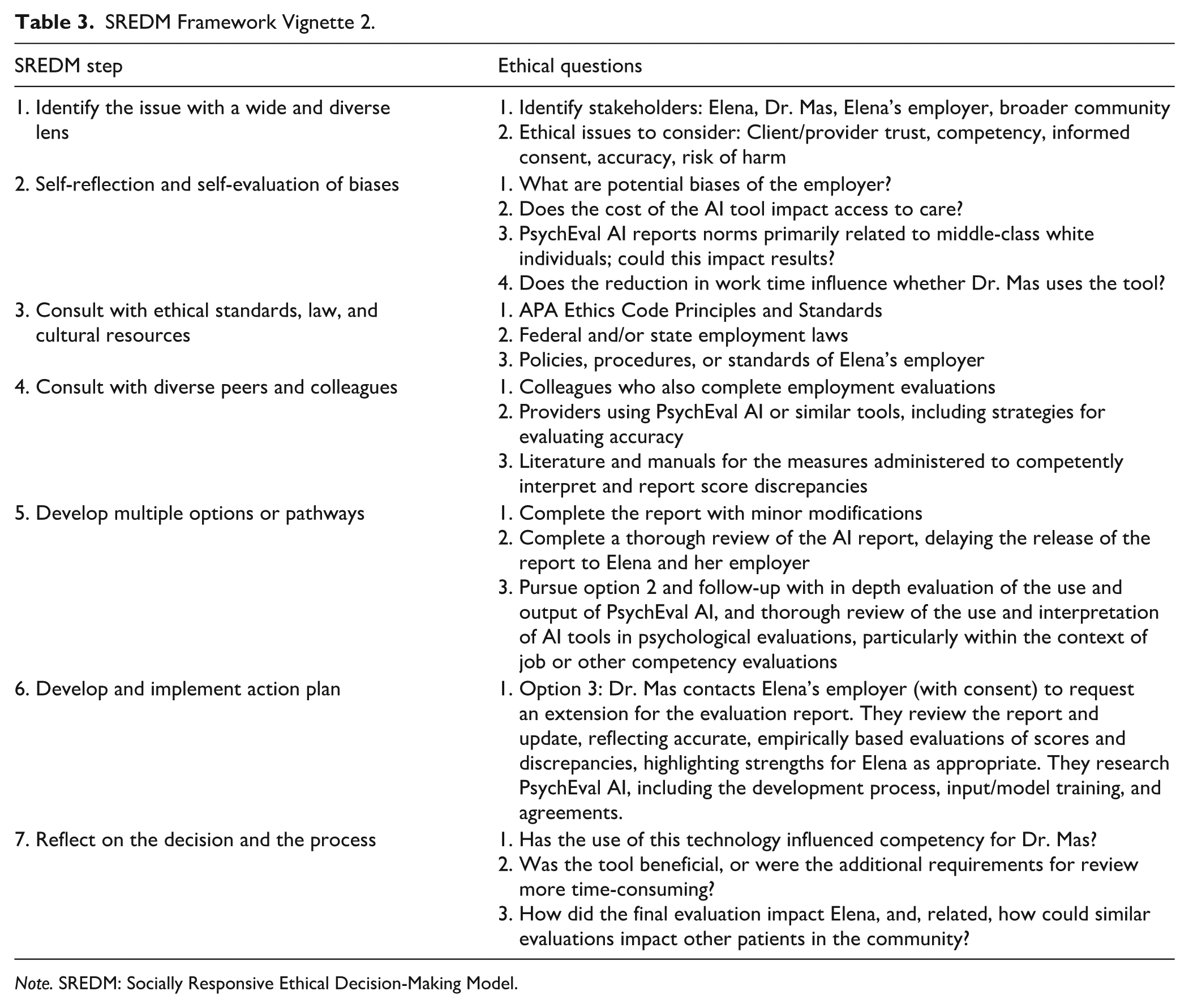
Note. SREDM: Socially Responsive Ethical Decision-Making Model.
In considering ethical, legal, and cultural standards, Dr. Mas must consider potential risk or liability with the release of the report generated by PsychEval AI, as the AI-generated report overlooks significant areas of functioning and discrepancies, which may negatively impact Elena’s current and future employment. Further, policies for the use of AI within the practice setting as well as Elena’s employment setting, must be considered, as well as the standardization requirements and manualized procedures for the specific test interpretation. It may be beneficial for Dr. Mas to consult with colleagues who complete similar evaluations to determine the most appropriate course of action in the incorporation of the AI technology to her practice. In this case, considerations for all Principles in the APA Ethics Code apply: Dr. Mas must evaluate whether the use of this AI tool is benefiting Elena’s care, or if it has the potential to increase harm to her (Principle A), assuming employment evaluations are within their area of competence, Dr. Mas also has an ethical obligation to maintain trust with their client (Principle B), including implementing thorough informed consent procedures for the use of AI (Principle C), considering how these data align with Elena’s cultural values and will be used by her employer and, therefore, may impact her livelihood (Principle D), and how her data will be stored and maintained, also considering how the report information will be shared with her employer (Principle E).
In this case, Dr. Mas must also consider numerous ethical standards including Competence, specifically regarding whether they have specific training in psychological assessment and specialized training in employment evaluations (2.01) and whether their work is based on established professional and scientific knowledge (2.04), and Privacy and Confidentiality, specifically regarding discussions of the limits of confidentiality (4.02), including disclosure for how information may be shared with Elena’s employer as well as how data are shared, and stored, with use of the PsychEval AI tool (4.01), and risks to confidentiality inherent in electronic storage and transmission (4.02). Further, psychologists must ensure that they are completing evaluations based on patient data and substantiated assessment procedures (9.01), using and interpreting measures in light of the standardization and research basis (9.02), providing informed consent related to the purpose of testing and disclosure of results (9.03), interpreting test results within a contextual framework of the individual client (9.06), are responsible for reviewing and interpreting those results (9.09), and accurately explain the results to the individual or representative (9.10). In addition, Dr. Mas must consider the nature of data storage and the learning model of PsychEval AI to ensure that they are not violating copyright laws or test security (9.11).
In addition to the standards noted above, informed consent is a process that must be adhered to throughout the course of this evaluation, including the disclosure of the use of technology and the AI tool (3.10, 9.03). As noted in the ethical principles, psychologists must work to maintain a relationship of trust with their patients and protect vulnerable populations. Being a mental health provider is a relationship that has inherent power, and informed consent and transparency in the assessment process is essential to maintain the relationship of trust. To that end, psychologists have an obligation of disclosure of the use of AI tools in clinical practice as their patients have a right to know how their data may be used and how it will be secured and stored to maintain their confidentiality (APA, 2025; Farmer et al., 2025; Hutnyan & Gottlieb, 2025; Shymko & Babadzhanova, 2025). Relatedly, when considering the use of AI tools into psychological assessment, Dumas and colleagues (2025) have created guidelines for implementation that include key features relevant to this case: (a) Disclose the use of AI to patients before they are assessed, (b) account for uncertainty in the AI responses, (c) have a clear and outlined protocol for how human oversight and auditing will be completed, and (d) explain how AI was used to the patients in the final report and feedback. These guidelines provide a functional “Dos and Don’ts” framework for incorporating the use of AI technology into psychological assessment. Regarding the AI tools, APA has also created guidelines for practitioners to ensure they are informed about the nature of the tools utilized in their practice (APA, 2024c). Specifically, these guidelines walk practitioners through multiple considerations to make prior to implementing the use of the AI tools including (a) researching the product vendor, including whether the developers incorporated consultation from mental health providers; (b) ensuring the tool provides value and improves or enhances clinical practice; (c) ensuring clinical tool development utilized empirically based information and methods; (d) ensuring that the tool meets HIPAA compliance standards and offers a business associate agreement; (e) researching the data security policies of the tool itself including data storage, security, and encryption; (f) reviewing all privacy policies and terms of service agreements in full; and (g) engaging in ongoing review of terms and policies, practicality of use in practice, informed consent options or examples for patient use, and documentation of the reviews completed prior to implantation of the AI tool into the practice.
After evaluating multiple possible options, including using the PsychEval AI report as is, requesting an extension to complete a more thorough review, and re-evaluation use of the PsychEval AI tool, Dr. Mas decides to complete a more thorough review of the report for Elena, editing the report to reflect her contextual factors, including noting that the slight weaknesses in working memory and processing speed are diagnostic, rather than reflecting cognitive impairment. In addition, they further evaluate the PsychEval AI tool to ensure that the tool meets the clinical needs of their practice. Upon review, they find that this tool is beneficial in crafting initial report drafts, with patient consent, but that these drafts will need review and adaptation before being released to the patients and other relevant stakeholders. As they reflect on the process and continue to evaluate this decision, Dr. Mas continues to assess the reports generated by PsychEval, finding that, even with the time for additional review and editing, their overall time spent on documentation is lessened significantly.
Similarly to the use of AI in clinical training, AI has also shown promising use within the clinical practice of assessment, specifically in scoring, interpretation, report-writing, and recommendations. However, as is the case with clinical training, human oversight remains necessary to thoroughly review findings, ensure test and diagnostic accuracy, and integrate test data into the contextual presentation of the patient, including any relevant cultural factors. In addition, although there are increasing guidelines for using AI within assessment (APA, 2025; Dumas et al., 2025) as well as for addressing and potentially mitigating bias within AI output (Tay et al., 2022), diligence in monitoring results and data provided to patients also remains essential.
Conclusion
In the realm of the rapid development and adoption of AI technology, psychologists are at the forefront of guiding how these tools may be used in clinical assessment, treatment, and training. Inclusion of psychologists as consultants and collaborators in the development of these tools can be integral to maximizing the potential benefits AI may have on the field as a whole, including advocacy for transparent AI tools, improvements in the breadth of clinical care (assessment and treatment) and documentation, as well as improved products, such as evaluation reports, for patients. If, and when, psychologists choose to move forward with adopting these tools in their practice, full evaluation of the risks and benefits, as well as considering the breadth of potential ethical concerns within an empirically based ethical decision-making framework, can maximize benefit to psychological assessment practice while adhering to the ethical standards of the field and maintaining patient safety. This safety may be optimized as psychologists utilize the current, and, given the rapid nature of change with the adoption of this technology, future guidelines for ethical incorporation of these technological tools into their practice (APA, 2024c, 2025; Dumas et al., 2025; Farmer et al., 2025; Huntyan & Gottlieb, 2025; Shymko & Babadzhanova, 2025), as well as through teaching the incorporation of the practical and ethical use of technological tools as an area of competency (Perle et al., 2025) in graduate level psychology training programs.
Footnotes
Ethical Considerations
This article does not contain any studies with human or animal participants.
Informed Participate
This article does not contain any studies with human or animal participants.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This review article does not contain any original data for availability.