
Abstract
Exposure to potentially morally injurious events (PMIE) poses a threat to one’s moral beliefs that can lead to prolonged and impairing mental health outcomes related to moral injury (MI). In a large German-speaking sample (N = 364, 48.9% female) of high-risk populations (legal, health care, military, security, social sector, press), we administered the Moral Injury Outcome Scale (MIOS) and Moral Injury and Distress Scale (MIDS) to investigate the frequency of PMIE exposure and MI outcome and distress. About three-quarters of the sample endorsed having experienced a PMIE, while 11.5% and 5.5.% screened positive for clinically meaningful MI on the MIDS and MIOS, respectively. Both the MIOS and the MIDS demonstrated good to excellent internal consistency. The CFA provided further evidence for their factorial validity; correlations supported aspects of convergent and discriminant validity. Exposure to PMIE and MI is a highly prevalent phenomenon across different occupational fields in Germany. The German versions of both scales seem suitable for assessing MI outcome and distress.
Keywords
Introduction
After exposure to potentially morally injurious events (PMIE), a significant number of people develop clinical problems related to various mental and behavioral health outcomes (McEwen et al., 2021). These include symptoms of posttraumatic stress disorder (PTSD), depression, anxiety, substance use (e.g., cannabis use disorder: Ashwal-Malka et al., 2022; problematic alcohol use: Battles et al., 2019), suicidality (Maguen et al., 2012), and other negative health outcomes (e.g., pain, sleep disturbances; Hall et al., 2022; Williamson et al., 2018). One particular common symptom constellation is called Moral Injury (MI): In his seminal work, Shay (1994) defined moral injury (MI) as “betrayal of what’s right by someone who holds legitimate authority in a high-stakes situation”. Despite disagreements among clinical experts (Serfioti et al., 2023) and researchers (Frankfurt O’Brien et al., 2024) regarding the definition of PMIE and MI, Litz and Walker (2025) provided an operational definition of PMIE as a “distressing experience that entails doing or failing to do things or being the victim of/bearing witness to acts that transgress deeply held moral beliefs and expectations” distinguishing stressor exposure from MI as an outcome. The two best-studied measures incorporated this distinction during their development. In the Moral Injury Outcome Scale (MIOS), Litz et al. (2022) define a PMIE as a very stressful experience in which a person (a) did something (or failed to do something) that went against their moral code or values (e.g., harming someone or failing to protect someone from harm), (b) saw someone (or people) do something or fail to do something that went against their moral code or values (e.g., witnessing cruel behavior), or (c) were directly affected by someone doing something or failing to do something that went against their moral code or values (e.g., being betrayed by someone the person trusted). The Moral Injury and Distress Scale (MIDS), however, emphasizes personal agency (i.e., the person taking the decision for the transgressive act). The MIDS defines a PMIE as when a person “(a) acted in ways that violated their own morals or values, (b) violated their own morals or values by failing to do something the person should have done, or (c) saw things that violated their own morals or values.” The scales differ according to whether betrayal is classified as an event or an outcome. Although some stressors are both (life-)threatening (i.e., traumatic) and morally injurious, other stressful events do not meet the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) Criterion A trauma definition and therefore cannot result in PTSD. Because a PMIE need not qualify as a DSM-5 traumatic stressor, MI may occur in the absence of PTSD. Indeed, a wide range of stressful events may evoke morally injurious responses without qualifying as traumatic under DSM-5.
Shay (1994) conceptualized MI as a deep moral-existential wound in veterans, arguing that “betrayal of what’s right” is central to MI, especially by a legitimate authority in high-stakes contexts, and states that MI is an essential part of combat trauma. As such, he discussed particularly other-directed outcomes as part of MI (e.g., rage). In contrast, Jameton (1984) differentiated three types of moral problems in the hospital context: moral uncertainty, moral dilemmas, and moral distress. He defined moral distress as instances “when one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action.” For example, he describes situations in which nurses must carry out procedures they believe are morally wrong or potentially nonbeneficial and feel unable to refuse, while identifying incompetent or unsafe practice and medically unjustified pain as common sources of moral distress in nursing. Based on extensive clinical research following Litz et al. (2009), MI is now deemed a clinical problem comprising functionally impairing symptoms (Litz & Walker, 2025). According to Litz et al. (2022), these include self- and other-perception (e.g., beliefs about personal or collective humanity), moral thinking (e.g., self-censure/self-condemnation), social behavior (e.g., social exclusion/rejection and loss of significant others), self-harming/self-sabotaging, moral emotions, and beliefs about meaning and purpose (e.g., questioning faith and the meaning of life). Aligning well with a “resilient” PMIE trajectory (Levinstein et al., 2024), only 10.2% of all individuals exposed to a PMIE, as measured by the MIDS in one study, met the criteria for clinically significant MI (Maguen et al., 2024). In contrast, the prevalence of clinically significant levels of MI, as measured by the MIOS in one sample of U.S. veterans, was estimated to be 13.1% among PMIE endorsers and 5.9% in the full sample (Litz et al., 2025).
Although mostly studied in relation to PTSD (Currier et al., 2019), a cumulative body of research now points toward the distinctive psychopathology (Bryan et al., 2018) and trajectory of MI-related outcomes (Jordan et al., 2017) following exposure to PMIE relative to life threat–based PTSD. Exposure to PMIE is significantly associated with a variety of negative mental and behavioral health outcomes (Litz & Kerig, 2019). In high-stress, service-oriented professions, for example, MI is related to current suicidal ideation (Griffin, Maguen et al., 2025). Qualitatively, the categorization of index events into moral injury by self or others (Stein et al., 2012) highlights the distinction between self- and other-transgressions. Related to self-transgressive behavior, the distinction between acts of commission (i.e., being an active agent) and omission (i.e., being a passive agent) heightened precision, despite the overlap of their outcomes with events involving others’ transgressions (Yeterian et al., 2019). Moreover, betrayal by a leader/trusted authority was identified as a specific victimization-based subtype of PMIE (Shay, 2014).
Although various types of PMIE share similar consequences (e.g., spiritual/existential issues like loss of faith or questioning morality), there seem to be differences in individual psychopathology resulting from the type of PMIE (i.e., perpetration- vs. victimization-based events like betrayal). Events based on individual responsibility (e.g., self-transgressive behavior like perpetration or failing to prevent harm) are more likely to lead to negative internally directed emotions and cognitions (e.g., self-referential emotions like guilt and shame, or lack of self-forgiveness). In contrast, events involving other responsibility (i.e., other-transgressive behavior like witnessing disproportionate violence or betrayal by trusted others) are more likely to lead to negative externally directed emotions and cognitions (e.g., anger, trust issues, lack of other-forgiveness). Accordingly, guilt and shame are differentially associated with reactions to wrongdoing among perpetrators of interpersonal offenses (Griffin et al., 2016). Moreover, having committed moral violations likely results in more severe perpetration-based symptoms than failing to prevent others’ moral violations. Being the victim of others’ transgressive, morally violating behavior, however, probably leads to qualitatively different symptoms that are related to betrayal (e.g., trust violation). Although most of the MI research focused on self-oriented negative moral emotions such as shame and guilt (Tangney et al., 2007), anger can particularly be elicited by betrayal-based events (Potik et al., 2024; Sarkissian & Yalch, 2024). Indeed, the association between exposure to betrayal-based events and psychological distress is mediated by anger (i.e., other-condemning emotion), whereas the relationship between exposure to perpetration-based events and distress is mediated by shame (i.e., self-conscious emotion elicited by self and others’ norm violations) and/or guilt (Frankfurt et al., 2017; Jordan et al., 2017; Marx et al., 2010).
Although originally observed in soldiers and war veterans (Shay, 1994), MI can also affect civilians. Most prominently, MI can occur in health care professionals (Griffin et al., 2023) working in primary health care but also in forensic and psychiatric settings (Webb et al., 2023). Recently, MI has been developed in the context of morally difficult decisions around treatment prioritization and allocation of limited resources (Xue et al., 2022). This was evident both during the first wave (Fischer et al., 2022) and at the peak of the COVID-19 pandemic (Čartolovni et al., 2021), affecting their professional and personal well-being (Thibodeau et al., 2023). In many other professions, people also have a special responsibility for the physical and psychological safety of other people (e.g., in the legal and social sectors), which heightens risk for PMIE exposure. Beyond military and health care (Benfer et al., 2023), it can occur among teachers (Currier et al., 2015), police officers (Komarovskaya et al., 2011; Papazoglou & Chopko, 2017), and other public safety personnel such as firefighters and paramedics (Roth et al., 2022), child welfare workers (Haight et al., 2017), human rights advocates (Pfeffer et al., 2023), journalists (Osmann et al., 2024), and presumably other professions (e.g., juvenile judges; Griffin et al., 2019). Moreover, it may affect other vulnerable populations like refugees (Nickerson et al., 2015), first responders or prison inmates (Griffin et al., 2019). In a meta-analysis of 13 cross-sectional studies of PMIE exposure across different populations using a variety of measures, PMIE exposure correlated with PTSD with a mean weighted effect size of Pearson’s r = .30, with depression with r = .23, and with suicidality with r = .14 (Williamson et al., 2018). Although the estimates varied widely, the findings cautiously indicate the range of potential exposure throughout society and occupations and its impact on different mental health outcomes.
However, there is still a lack of research in high-risk populations across different contexts. Inherently, (occupation-related) MI appears to be context-dependent (e.g., working conditions, society), emphasizing the role of systemic factors (e.g., hierarchical structures, resources). Yet, most studies were conducted in highly specific contexts (e.g., U.S. military, U.S. health care system), mostly in veteran and active-duty military samples (Hall et al., 2022), limiting generalizability. Therefore, studies in diverse societal, cultural and occupational contexts are needed to address the systemic nature in which MI occurs. Qualitatively, there are also different PMIE types related to self- and other-transgression (Stein et al., 2012). In the case of perpetrator-based events involving self-transgressing behavior, an important distinction is between commission (i.e., being an active agent) and omission (i.e., being a passive agent), despite the overlap of their outcomes with events involving others’ transgressions (Yeterian et al., 2019). In addition, betrayal by a leader/trusted authority (e.g., a supervisor) is considered as a specific victimization-based PMIE type (Shay, 2014). Studies examining systematic differences in PMIE type exposure among various high-risk populations are missing.
Despite the fact that long-standing conceptual ambiguity has slowed down progress in developing valid and reliable measures, there are now questionnaires available that demonstrate promising psychometric quality (Griffin, Price, et al., 2025). Overall, there are 42 scales for assessing moral stress and MI whose psychometric properties vary considerably (Houle et al., 2024). Following their systematic review, Houle et al. (2024) recommended the Moral Injury Outcome Scale (MIOS; Litz et al., 2022) and provisionally recommended the Brief Moral Injury Scale – Nieuwsma (BMIS-N; Nieuwsma et al., 2021), the Expressions of Moral Injury Scale – Military Version (EMIS-M; Currier et al., 2018), and the Moral Injury and Distress Scale (MIDS; Norman et al., 2024). In many cases, however, convergent and divergent validity were not examined (Houle et al., 2024).
In the present study, we sought to determine the frequency of exposure to PMIE, the prevalence of clinically significant levels of MI conditional on PMIE exposure, and the risk of different types of PMIE and MI in high-risk occupations in Germany. We therefore prioritized instruments that (a) explicitly target MI symptoms (without specifying a particular context or population), (b) reflect recent advances in the conceptualization of MI, and (c) have emerging psychometric support in relevant populations (Houle et al., 2024). Given the heterogeneity in MI measurement, we selected two recently developed instruments designed to assess MI-related symptoms rather than PMIE exposure alone. The MIOS (Litz et al., 2022) and the MIDS (Norman et al., 2024) are the only two measures that clearly distinguish between event exposure and symptom assessment by linking MI to specific PMIE(s). In addition, both instruments have received initial psychometric support in non-military populations. The initial validation study of the MIOS in a military sample provided factor-analytic evidence as well as support for its test–retest reliability using Bland-Altman Limits of Agreement and for convergent validity through correlational analyses with various mental and behavioral health outcomes (Litz et al., 2022). Cronbach’s α was reported to be excellent for MIOS total scores (α = .89), and good to very good for the shame-related (α = .88) and trust violation-related subscales (α = .78; Litz et al., 2025). Particularly, the theorized two-factor structure of the MIOS was supported by confirmatory factor analyses among military samples in Canada, the United Kingdom, and Australia (Litz et al., 2022) as well as in samples of acute care nurses (Tao et al., 2023) and Canadian health care workers (Plouffe et al., 2025). During the MIDS development process, a stakeholder engagement panel with veterans and individual interviews with health care workers and first responders were conducted, who provided feedback on the content validity and acceptability of the items. The initial validation study of the MIDS in a sample of military veterans, health care workers, and first responders provided factor-analytic evidence in a cross-validation subsample and support for convergent and discriminant validity through correlational analyses with various outcomes as well as incremental validity with regard to functional impairment using hierarchical multiple regression (Norman et al., 2024). In this study, the MIDS total scale demonstrated excellent internal consistency (Cronbach’s α = .95) and moderate 2-week stability (r = .68). For convergent validity, correlations between the MIDS, PMIE exposure measures and other MI proxies (e.g., guilt, shame) were large (r = .59–.69), as were associations with posttraumatic stress, depressive, and insomnia symptoms (r = .51–.67). Moreover, the MIDS predicted variance in functional impairment beyond variance explained by individual differences (e.g., gender, age, and race) and two existing measures of PMIE exposure (9% vs. 1%–1.3%). A single-factor structure of the measure was supported by confirmatory factor analyses (Norman et al., 2024).
Moreover, using both measures will enable us to examine whether observed associations are robust across two contemporary operationalizations of MI symptoms within the same sample. As both translated scales were recently translated into German (Herzog, 2024), the second objective was to examine their psychometric properties. The inclusion of a measure for socially aversive personality traits (i.e., dark factor personality) was intended to strengthen the construct validity evaluation by testing whether the MI assessment demonstrates theoretically coherent associations with a broader maladaptive personality disposition. Assessing these personality traits is relevant in this context because it captures a general propensity toward self-serving behavior accompanied by the devaluation of others’ interests, which may bear on how individuals perceive, interpret, or respond to PMIEs. Conceptually, MI should occur only in individuals who generally possess moral integrity. Therefore, we hypothesized an overall low scoring on this measure. Establishing this pattern of unrelatedness is important for demonstrating that the measure fits appropriately within its broader nomological network.
Method
The local ethics committee of the Department of Psychology at the RPTU University Kaiserslautern–Landau approved this study (reference number #LEK-544). This study was conducted in accordance with the ethical standards specified in the Declaration of Helsinki (1964) and its later amendments. Participation in this study was voluntary, and no financial benefit was offered. Before inclusion in this study, all patients gave written informed consent.
Participants and Procedure
Using a cross-sectional online study design, we recruited a large sample of high-risk populations in Germany. Of particular interest during recruitment were specific occupational groups that are highly likely to be exposed to PMIE through their professional activities. For this purpose, we a priori defined the following six target professional fields:
Legal Sector: judges, public defenders, etc.
Health care Sector: nursing staff, hospital staff, psychiatrists, psychotherapists, etc.
Military: for example, soldiers, veterans, etc.
Security Sector: for example, police, fire department, public order office, correctional officers, etc.
Press: for example, journalists, etc.
Social Sector: for example, youth welfare services, social workers, family assistance, teachers, employees of job centers, employment agencies, and immigration offices, etc.
We created an additional category (“Other”) for those whose work exposes them to PMIE but were not assignable (e.g., diplomats, HR sector, managers in industry, health insurance professionals, city administration such as homelessness program officers, ecclesiastical sector and church-affiliated organizations).
As part of the recruitment process, we contacted organizations whose members are at risk for exposure to PMIEs. For the legal sector, these included the Federal Association of Correctional Officers (Bundesverband der Strafvollzugsbediensteten, BSBD), State and Federal Criminal Police Offices (Landes- und Bundeskriminalämter, LKA & BKA), nationwide police stations, state fire department associations and stations, as well as the State Office for Fire and Disaster Protection (Landesamt für Brand- und Katastrophenschutz). Furthermore, the German Judges Association (Deutscher Richterbund, DRB), various courts (Higher Regional Courts, Regional Courts, and Local Courts), public prosecutor’s offices, bar associations, law firms, the German Lawyers’ Association (Deutscher Anwaltverein, DAV), legal advisory offices, and public defenders were contacted. For the military sector, the Bundeswehr (German Armed Forces including the Air Force and Navy), the Bundeswehr Association, reservist associations, the War Graves Commission, the Association of German Deployment Veterans, military chaplaincy, and psychosocial comrade support services were included. For the health and social sector, a wide range of civil society and social institutions were contacted, such as youth welfare offices, social and public order offices, counseling centers, schools, hospitals, job centers, employment agencies, immigration offices, refugee councils, medical chambers, professional associations (e.g., for health care professionals), and associations of statutory health insurance physicians. Moreover, psychiatric and forensic clinics, psychiatrists, psychotherapists, treatment centers, the Federal Chamber of Psychotherapists (Bundespsychotherapeutenkammer, BPTK), and professional societies like the German Society for Psychoanalysis, Psychotherapy, Psychosomatics, and Psychodynamic Psychology (Deutsche Gesellschaft für Psychoanalyse, Psychotherapie, Psychosomatik und Tiefenpsychologie, DGPT) were involved in the recruitment process. Other recipients included the German Life Saving Association (Deutsche Lebens-Rettungs-Gesellschaft, DLRG), the Workers’ Samaritan Federation Germany (Arbeiter-Samariter-Bund Deutschland, ASB), journalists and editorial offices, the German Association of Press Journalists (Deutscher Verband der Pressejournalisten, DVPJ), the German Journalists’ Association (Deutscher Journalisten-Verband, DJV), as well as relevant Facebook groups on topics such as the German Armed Forces, nursing, and journalism. Moreover, a list of publicly accessible email addresses of nationwide institutions related to the six defined occupational fields was compiled.
We used the online survey tool SoSci Survey for study implementation. The order of the scales presented in the questionnaire was: the MIOS, the MIDS, the LEC-5 and the D scale (see Measures below). For participants who responded negatively to the first MIOS item on PMIE exposure, the questionnaire continued directly to the LEC-5. The translation of both the MIOS and MIDS into German were done by a person with English skills at native level, and back translated and proofread by another person equally skilled in English to assure content-related consistency (Herzog, 2024).
Measures
PMIE Exposure and MI Outcome
Moral Injury Outcome Scale
The German version of the Moral Injury Outcome Scale (MIOS; Litz et al., 2022) assessed exposure to PMIE and MI. The MIOS is a self-report scale that first measures exposure to a PMIE, as well as the different PMIE types, before the associated distress of those affected is assessed with 14 items on a 5-point Likert-type scale (0 = strongly disagree to 4 = strongly agree). The MIOS comprises two subscales with seven items each: the shame-related and trust-violation-related subscales. Scores are calculated by summing item responses across the full scale for a total score and across both subscales, respectively. Litz et al. (2025) used a norm-referenced (standardized) T-score approach to derive a cut-off value of 31 (T ≥ 65) on the MIOS total score to indicate clinically significant cases of MI in a sample of U.S. veterans. To ease comparability with previous research, we reported total scores as well as subscale scores for the MIOS. We applied a cut-off value of 31 on the MIOS total score to screen for MI in our sample.
Moral Injury and Distress Scale
The German version of the Moral Injury and Distress Scale (MIDS; Norman et al., 2024) assessed the moral distress related to MI. The MIDS is a self-report questionnaire with 18 items. Participants rate each item on a 5-point Likert-type scale from 0 = “Not at all” to 4 = “Extreme”. In contrast to the MIOS, betrayal is conceptualized as an outcome of a PMIE rather than a nonagentic PMIE itself. A total score is calculated by summing item responses across the full scale. Maguen et al. (2024) applied receiver operating curve analysis with clinically significant symptoms of PTSD, depression, trauma-related guilt and functional impairment as criteria to establish a cut-off score of 27 that was most efficient in identifying clinically meaningful MI in a sample of U.S. first responders, health care workers and veterans. We applied a cut-off value of 27 on the MIDS total score to screen for MI in our sample. 1
Trauma Exposure and PTSD Outcome
Life Events Checklist for DSM-5
The German version of the Life Events Checklist for DSM-5 (LEC-5; Weathers et al., 2013) assessed trauma history. The LEC-5 is a self-report scale to assess previous traumatic experiences. Following a commonly used approach for calculating a scale score for the LEC-5 (Weis et al., 2022), we summed all endorsed items from all exposure types to generate a total LEC-5 score (minimum/maximum for each scale = 0/17, total score minimum/maximum = 0/68).
Primary Care PTSD Screen for DSM-5
In the MIOS, the Primary Care PTSD Screen for DSM-5 is included. Following Prins et al. (2016), we chose a cut score of 4 to optimize the trade-off between sensitivity and specificity, thereby reducing both false negatives and false positives.
Psychosocial Impairment
Brief Inventory of Psychosocial Functioning
The Brief-Inventory of Psychosocial Functioning (B-IPF; Kleiman et al., 2020) is part of the MIOS. The B-IPF is a context-sensitive self-report measure consisting of seven domains that assess PTSD-related psychosocial functional impairment over the past 30 days: romantic relationships, family relationships, work, friendships/social interactions, parenting, education, and self-care. Responses are rated on a 7-point Likert-type scale ranging from 0 (never) to 6 (always). A composite score reflects the overall functional impairment, with higher values indicating more severe impairment. Two additional items were added to cover the domains of religiousness/spirituality and solo hobbies/leisure activities.
Other Constructs
Dark Factor of Personality (D)
A short version of the Dark Factor of Personality (D) inventory was used to differentiate between participants with restricted and unrestricted moral sensitivity based on their personality traits, as these could represent potential confounding variables (Moshagen et al., 2020). Aversive personality traits are associated with aggression, criminal and deviant behavior, a lack of empathy, increased distrust toward others, and the attribution of lower importance to moral identity in the self-concept. The short version consists of 16 items (D16) that are rated on a 5-point Likert-type scale (1 = not at all to 5 = extremely; Moshagen et al., 2020). The D16 was used to test discriminant validity. One additional item was included as an attention check.
Sociodemographics
Sociodemographic questions recorded participants’ age, gender, ethnicity, geographical origin, current employment status, occupation, professional education, education level, family status, children, and living conditions.
Statistical Analyses
Transparency and Openness
This study’s design and its analysis were not preregistered. All data and analysis code are available on OSF: https://doi.org/10.17605/OSF.IO/AEVFW. To ensure the confidentiality of participants’ data, we generalized participants’ age and suppressed other demographic information as well as explicit descriptions of experienced PMIE. All analyses were performed using R Version 4.5.0 (R Core Team, 2025). Additional packages included psych (Revelle, 2025), codebook (Arslan, 2019), descr (Aquino et al., 2023), dplyr (Wickham et al., 2023), lavaan (Rosseel et al., 2024), finalfit (Harrison et al., 2024), MVN (Korkmaz et al., 2021), naniar (Tierney et al., 2024), tidyr (Wickham et al., 2024), ggplot2 (Wickham et al., 2025), semPlot (Epskamp, 2022), irr (Gamer et al., 2019), purrr (Wickham & Henry, 2025), WSR2 (Mair & Wilcox, 2025), Rstatix (Kassambara, 2025), Pastecs (Grosjean & Ibanez, 2024), Interactions (Long, 2024), Car (Fox et al., 2024), apaTables (Stanley & Spence, 2018), pacman (Rinker & Kurkiewicz, 2019).
Preprocessing
We performed data screening for careless and insufficient effort responding following recommendations from DeSimone et al. (2015) and Ward and Meade (2023). First, we identified data-entry errors and implausible values for open questions (e.g., a respondent reported having 25 children or a PMIE taking place in the year 1111) and set them to missing. One respondent who consistently gave unserious and unrelated answers across open questions (e.g., “This survey is nonsense”) was eliminated. Second, five respondents (0.01%) who failed an instructed response item (“This statement serves as an attention check: Please select Strongly agree”) were eliminated. Long-string analysis was applied following Curran’s (2016) rule of thumb, considering a string of consistent responses greater than half the length of the total scale as an indicator of careless or insufficient effort responding. Long-string analysis flagged 42 respondents (11.32%) as potentially careless respondents. We then inspected univariate outliers for scale scores and computed robust Mahalanobis distance (Leys et al., 2018) across scale scores to determine multivariate outliers; 20 respondents (0.05%) were identified as univariate outliers, and 17 respondents (0.04%) were identified as multivariate outliers. Combining these three techniques, we eliminated six respondents (0.02%) who were flagged by both long-string analysis and outlier analysis, indicating a higher likelihood of careless or insufficient effort in responding.
To assess whether missing values were missing completely at random (MCAR), we used the MCAR test (Little, 1988). The MCAR test showed a significant result, χ2(1,389) = 2,276.00, p < .001, indicating that the assumption of data MCAR did not hold. Questionnaire design only allowed for missingness in open questions and due to conditional branching as well as dropout. We assumed missing data due to dropout likely arose from questionnaire fatigue and thus handled missing data as missing at random (MAR). For correlations, missing data were addressed by using pairwise deletion. For confirmatory factor analyses (CFAs), missing data were handled by using listwise deletion. We performed descriptive item and scale analyses and computed bivariate Pearson’s correlations between the scales and p-values. We corrected p-values according to the Holm method for multiple comparisons.
Reliability Analyses
We estimated reliability by computing internal consistency indicated by Cronbach’s α. In addition, we reported McDonald’s ωh, McDonald’s ωt, average item correlation, and average split-half reliability as recommended by Revelle and Condon (2019).
Confirmatory Factor Analyses
We conducted CFA using lavaan (Rosseel et al., 2024). We used the mean- and variance-adjusted weighted least squares (WLSMV) estimator to account for the ordinal nature of the data at the item level (Brauer et al., 2023). For the MIOS, we specified both a one-factor and a two-factor model following Litz et al.’s (2022) distinction between outcomes unique to an MI-Self experience (shame-related outcomes) and MI-Other experiences (trust-violation-related outcomes). For the MIDS, we specified a one-factor model.
Results
Sample Characteristics
The sociodemographic characteristics of the full sample (N = 364) and for each subsample [i.e., PMIE endorsers (n = 276) and non-PMIE endorsers (n = 88)] are displayed in Table 1. Most participants were between 40 and 59 years old. Most were White Western Europeans who were employed and held a university degree. About half were women and most were married or partnered. About two-thirds had children.
Sociodemographics for the Full Sample and PMIE Endorsing Participants vs. Non-PMIE Endorsing Participants.
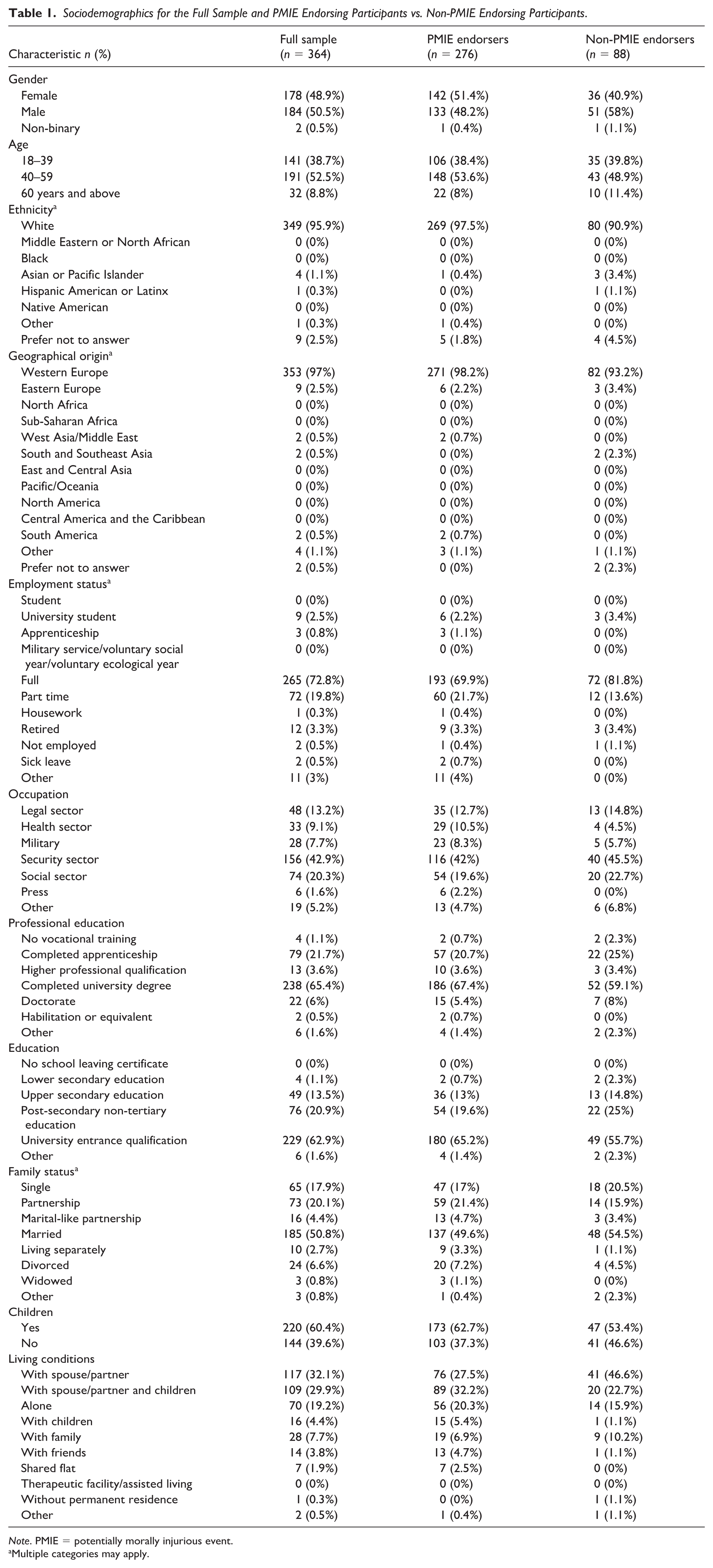
Note. PMIE = potentially morally injurious event.
Multiple categories may apply.
Scale Analyses
Descriptive Scale Statistics
Table 2 portrays the descriptive statistics. The mean total MIOS score (n = 196) was M = 17.24 (SD = 9.91) with the mean score of the Shame-related subscale (MIOS-SR) M = 5.92 (SD = 5.35) and Trust-violation-related subscale (MIOS-TVR) M = 11.33 (SD = 6.29), while the mean total score was M = 17.45 (SD = 13.82) on the MIDS (n = 189). The item characteristics, inter-item correlations and corrected item-total correlations of the Moral Injury Outcome Scale (MIOS) and Moral Injury and Distress Scale (MIDS) are depicted in the Supplements (see Tables A2–A5 in the Supplemental Material).
Descriptive Statistics of All Scales.
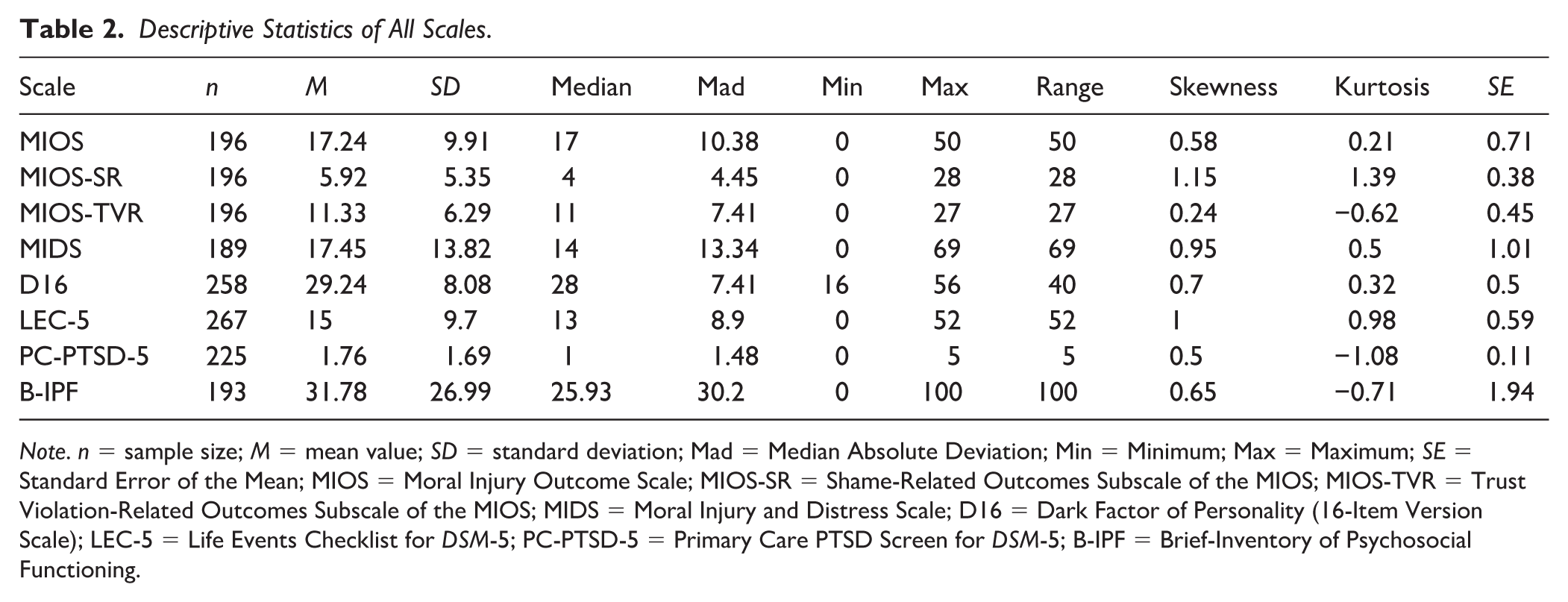
Note. n = sample size; M = mean value; SD = standard deviation; Mad = Median Absolute Deviation; Min = Minimum; Max = Maximum; SE = Standard Error of the Mean; MIOS = Moral Injury Outcome Scale; MIOS-SR = Shame-Related Outcomes Subscale of the MIOS; MIOS-TVR = Trust Violation-Related Outcomes Subscale of the MIOS; MIDS = Moral Injury and Distress Scale; D16 = Dark Factor of Personality (16-Item Version Scale); LEC-5 = Life Events Checklist for DSM-5; PC-PTSD-5 = Primary Care PTSD Screen for DSM-5; B-IPF = Brief-Inventory of Psychosocial Functioning.
Internal Consistency
The internal consistency of the MIOS total scale was high, as indicated by α = .85 (95% CI [.83, .87]). For the MIOS subscales, the internal consistency ranged between α = .81 (95% CI [.78, .84]) for the MIOS-TVR subscale and α = .82 (95% CI [.79, .85]) for the MIOS-SR subscale. The internal consistency of the MIDS scale was excellent with α = .92 (95% CI [.91, .93]). 2 In addition, the average item correlation was r = .31 for the MIOS total scale, r = .41 for the MIOS-SR subscale, r = .39 for the MIOS-TVR subscale, and r = .40 for the MIDS.
PMIE Exposure and MI
Of N = 364 participants, a subsample of n = 276 (75.8%) endorsed having experienced a PMIE. In case of multiple types for the same event, 35 participants (12.7%) reported self-transgression, 46 observations (16.7%), and 57 being directly impacted (20.7%) as the worst aspect of the PMIE. A total of 42 respondents (11.5% of the sample) screened positive for MI, applying a cut-off score of 27 for the MIDS (Maguen et al., 2024), indicating a clinically meaningful MI. Applying a cut-off score of 31 for the MIOS (Litz et al., 2025), a total of 20 respondents (5.5% of the sample) screened positive for MI. To assess agreement between both instruments and their respective proposed cut-off scores, we followed Xu and Lorber’s (2014) recommendation and report Holley and Guildford’s G statistic for overall chance-corrected agreement, as it is insensitive to base rate, and separately report the rates of agreement on the presence of MI and the absence of MI. Overall, agreement between both scales was fair according to both Cohen’s κ = .322, p < .001 and G = 0.322. Consistency was especially strong for negative cases (pneg = 0.89) compared to positive cases (ppos = 0.42).
The PMIE types and MI for the full sample and by subgroup appear in Figure 1 (and Table A1 in the Supplemental Material). In most professional fields, the PMIE type “other event” prevailed, except for the military (n = 28) and legal sector (n = 48), where the PMIE type “other directly impacted event” was the most prevalent. Experiencing a clinically significant impact after exposure to a PMIE was most likely in the military group.
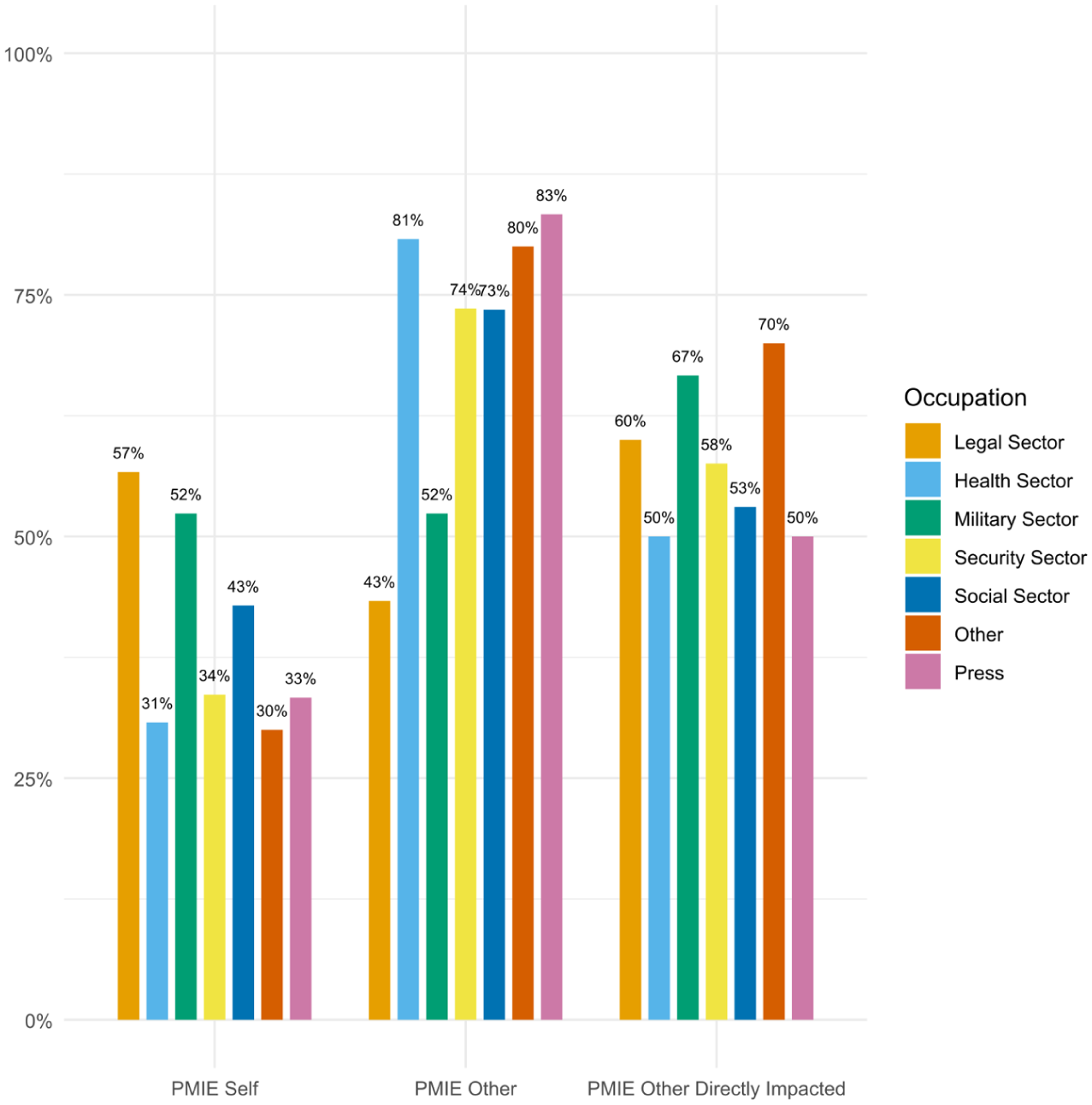
Frequency of potentially morally injurious event types by professional field
We used backward stepwise logistic regression to assess associations between different PMIE types and the likelihood of screening positive on the MIDS and the MIOS (as an indicator of a clinically significant MI), respectively. PMIE types as predictors were removed sequentially based on the Akaike Information Criterion (AIC). In the MIOS model, χ2(3) = 1.00, p = .80, R2 = .01 (Nagelkerke), none of the PMIE types were associated with higher odds of screening positive for MI. In the MIDS model, χ2(1) = 4.23, p = .04, R2 = .03 (Nagelkerke), only experiencing a PMIE-self event was associated with higher odds of screening positive for MI (OR = 2.07, SE = 0.35, 95% CI [1.03, 4.17], p = .004).
Additional comparison tests of mean differences in MIOS total and subscale scores as well as MIDS total scores across occupational subgroups can be found in the Supplemental Material (see Tables A6 to A9). The findings show that groups did not differ significantly in the MIOS total score, MIOS-SR score and MIDS total score, but did differ significantly in the MIOS-TVR score.
Convergent, Discriminant and Factorial Validity
Along with the intercorrelations of all scales used in the present study, the reliabilities are displayed in Table 3. The MIOS and MIDS were significantly intercorrelated, providing support for their convergent validity: The correlation between MIDS and the MIOS total score was r = .78 (p < .001), and slightly lower for the MIOS subscales and the MIDS with r = .71 (p < .001) for the MIOS-SR subscale and r = .62 (p < .001) for the MIOS-TVR subscale. The MIOS subscales were significantly intercorrelated with the MIOS total score, with r = .82 (p < .001) for the MIOS-SR subscale and r = .88 (p < .001) for the MIOS-TVR subscale. Screening positive on the MIDS was strongly associated with screening positive on the PC-PTSD-5, χ2(1) = 74.91, p < .001, φ = .65, suggesting substantial co-occurrence of MI and PTSD. In contrast, there was only a small to moderate association between screening positive on the MIOS and screening positive on the PC-PTSD-5, χ2(1) = 8.99, p < .01, φ = .23. No significant correlations were found between both MI measures (i.e., MIOS and MIDS), and D16 as well as LEC-5, demonstrating discriminant validity.
Intercorrelations and Reliabilities of All Scales.
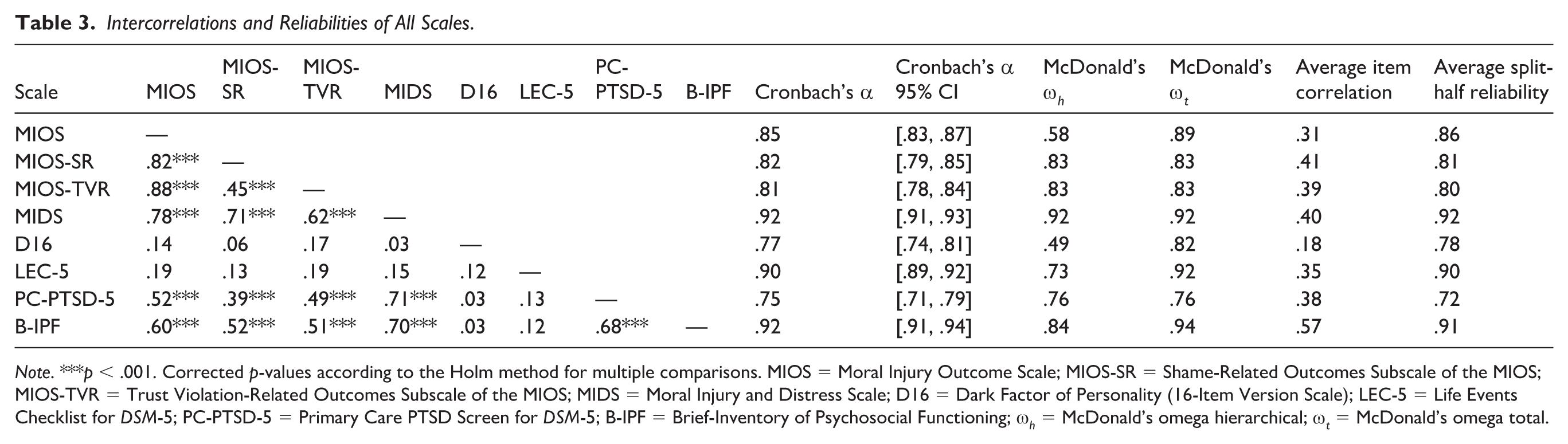
Note. ***p < .001. Corrected p-values according to the Holm method for multiple comparisons. MIOS = Moral Injury Outcome Scale; MIOS-SR = Shame-Related Outcomes Subscale of the MIOS; MIOS-TVR = Trust Violation-Related Outcomes Subscale of the MIOS; MIDS = Moral Injury and Distress Scale; D16 = Dark Factor of Personality (16-Item Version Scale); LEC-5 = Life Events Checklist for DSM-5; PC-PTSD-5 = Primary Care PTSD Screen for DSM-5; B-IPF = Brief-Inventory of Psychosocial Functioning; ω h = McDonald’s omega hierarchical; ω t = McDonald’s omega total.
The results of the confirmatory factor analyses are depicted in Figure 2 (for the MIOS) and Figure 3 (for the MIDS). We used established fit indices thresholds to judge model fit (Schermelleh-Engel et al., 2003). In this sample, the 14-item two-factor model underlying the MIOS showed an acceptable fit, χ2(76) = 163.899, p < .001, CFI = 0.960, TLI = 0.953, RMSEA = 0.077 (90% CI = 0.061, F 0.093), SRMR = 0.075. Factor loadings were mostly strong, ranging from 0.23 (“I no longer believe there is a higher power”) to 0.88 (both “I have trouble seeing goodness in others” and “I lost trust in others”), and the factors were significantly correlated at 0.63. Although this correlation appears high, it does not exceed the cut-off values of 0.80 to 0.85, and the factors are therefore not considered redundant (Brown, 2015). 3
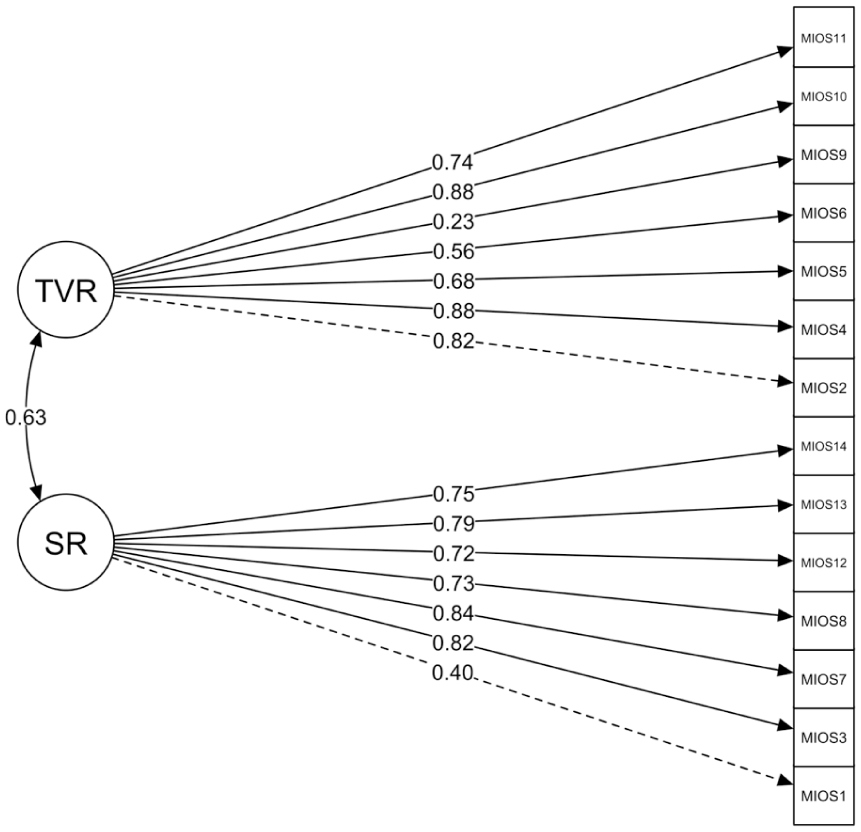
Results of confirmatory factor analysis for MIOS
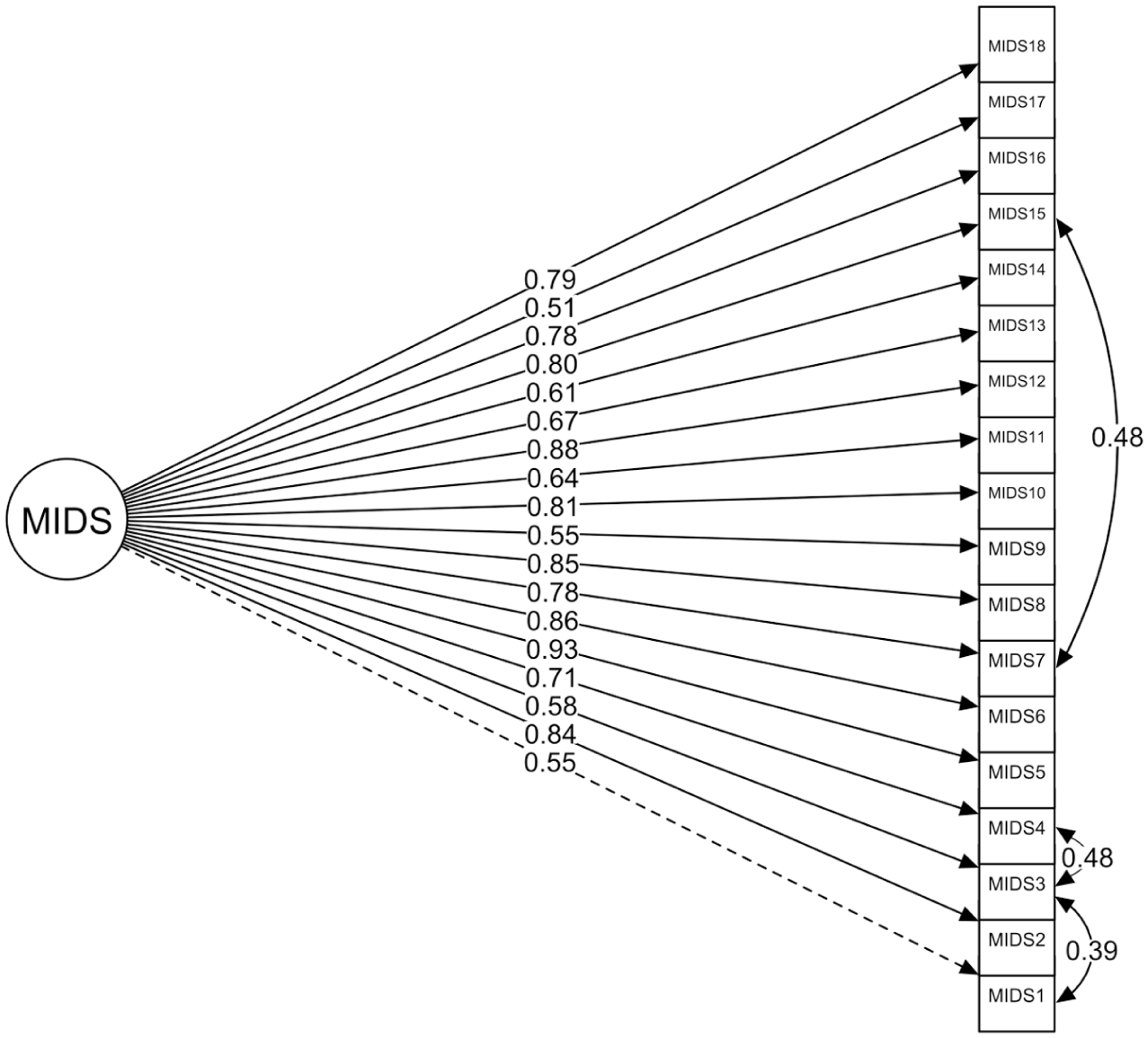
Results of confirmatory factor analysis for MIDS
The single-factor measurement model of the MIDS showed a lack of fit to the data in our sample: χ2(135) = 355.311, p < .001, CFI = 0.946, TLI = 0.939, RMSEA = 0.093 (90% CI = 0.081, 0.105), SRMR = 0.089. All items loaded significantly on the general factor, ranging from 0.50 (“My spirituality/faith is no longer a source of comfort”) to 0.93 (“I do not feel like I deserve to be happy”). Subsequently, we tested the revised model proposed by Norman et al. (2024), allowing for covariance between the residuals of “I don’t feel like I deserve to be happy.” and “I should not be forgiven.” This modified model showed similar lack of fit: χ2(134) = 354.270, p < .001, CFI = 0.946, TLI = 0.939, RMSEA = 0.094 (90% CI = 0.082, 0.105), SRMR = 0.089.
Subsequent examination of modification indices revealed that allowing residual covariances between the item pairs “I feel helpless.” and “I feel powerless.”, “I feel guilty.” and “I think about how I should have been able to do more.” as well as “I feel guilty.” and “I doubt my own judgement.”, could improve model fit. As “I feel helpless.” and “I feel powerless.” are very similar in item structure and both constructs of helplessness and powerlessness have substantial content overlap (e.g., lack of control, lack of self-efficacy), we allowed their residuals to covary. As feelings of guilt and “I think about how I should have been able to do more.” as a cognition both might reflect internalized responsibility of perceived wrongdoing, and share variance not accounted for by MI, we also allowed their residuals to covary. The same logic applies to feelings of guilt and “I doubt my own judgement.” Revising the measurement model significantly improved model fit, χ2(132) = 275.880, p < .001, CFI = 0.965, TLI = 0.959, RMSEA = 0.076 (90% CI = 0.063, 0.089), SRMR = 0.080.
Discussion
Following exposure to potentially morally injurious events (PMIE), some people develop clinical symptoms related to moral injury (MI). In this study, two measures of moral injury outcome and distress – the MIOS and the MIDS – were applied in a large German-speaking sample of high-risk populations to (a) examine the frequency of exposure to PMIE and MI as well as the relationship between different types of PMIE and MI across different occupations in Germany, and (b) determine their psychometric properties.
About 75% had experienced a PMIE, while 11.5% screened positive for clinically meaningful MI on the MIDS – similar to the 10.2% reported by Maguen et al. (2024). Using the MIOS, the prevalence of clinically significant levels of MI was lower (5.5%). Litz et al. (2025) recently reported a prevalence of 13.1% among PMIE endorsers in a sample of U.S. veterans (5.9% in the full sample). This finding might be explained by differences between the MIDS and MIOS in terms of their structure. Particularly, both have shared and distinct structural components that impact content validity (Litz, 2025). Most importantly, betrayal is conceptualized as a response to a PMIE in the MIDS, whereas the MIOS considers betrayal a nonagentic PMIE. The PMIE type “other event” was the most prevalent in most professional fields, whereas the PMIE type “other directly impacted event” was most common among military and legal participants. Experiencing a clinically significant impact after PMIE exposure was most likely in the military group. Of note, only the PMIE-self event increased the likelihood of developing a clinically significant MI. Moreover, significant differences between occupational groups in relation to MIOS-TVR outcomes were found. This is in line with a recent study examining occupational differences in the prevalence of PMIEs exposure and MI outcomes in nationally representative samples of three high-risk professions (Combat Veterans, Health care Workers, and First Responders): They found that, compared to first responders, combat veterans were more likely to endorse self-transgressions and health care workers were more likely to endorse other-transgressions, while both occupational groups were over twice as likely to screen positive for clinically meaningful MI (Maguen et al., 2025). However, direct comparisons in our sample must be interpreted with caution due to unbalanced group sizes.
While MIOS and MIDS total scores were strongly correlated, there are noteworthy differences in how they identified cases of MI and how they were associated with other scales. In our sample, the MIOS estimate of prevalence of clinically significant levels of MI (5.5%) was substantially lower than the MIDS estimate (11.5%). This discrepancy in estimates and the moderate rate of agreement in positive identification may partly be explained by the preliminary nature of the applied cut-off scores and the different approaches that underlie their identification. The MIOS cut-off score was established based on distributional properties of the MIOS total score in a large U.S. military sample, so that case classification was determined by statistical abnormality (T ≥ 65). In a second step, comparison of criteria (e.g., depression symptom severity, PTSD symptom severity and functional impairment) supported this differentiation between MI cases and non-MI cases (Litz et al., 2025). In contrast, the MIDS cut-off score was established using criterion-based ROC analysis, optimizing discrimination against four external criteria (probable PTSD, probable depression, trauma-related guilt and functional impairment). Both instruments cut-off scores could not be determined against a gold-standard criterion, as there is none. Optimal cut-off scores are likely to differ for different populations and contexts (Maguen et al., 2024). Consequently, the identification of optimal MIOS and MIDS scores to screen for MI in more diverse populations requires further investigation.
The total scoring algorithm of the MIOS may influence case identification and prevalence estimates as well. Screening based on a total score that is composed of both the unique internalizing outcomes arising from personal transgressions and the externalizing outcomes from being victimized by others’ transgressions (Litz & Walker, 2025) may dilute or inflate the presence of MI depending on which outcomes are more relevant for an individual. For example, people who score high on Shame-related outcomes indexed to an act of commission might score low on Trust-violation-related outcomes and in consequence might be screened negative due to a moderate total score. Focusing on subscale scores may give more nuanced and accurate classifications.
Our findings support the reliability and factorial, discriminant, and convergent validity of the German versions of the MIOS and the MIDS. The MIDS exhibited excellent internal consistency, whereas the MIOS total scale and subscales exhibited high internal consistency, respectively. Moreover, our results confirm previous findings of a correlated two-factor structure of the MIOS (Litz et al., 2022). Findings of multidimensionality often lead to questioning the adequacy of using total scale scores as reflections of the general construct (Reise et al., 2013). As Griffin et al. (2025) noted, in the absence of evidence supporting a higher-order factor or bifactor solution, the interpretation of a total scale score may be confounded, and estimates of associations between MI and predictors, correlates, and consequences may be biased, as the subscales might represent rather distinct concepts that may relate differently to external criteria. In our sample, we could not find confirmatory evidence of a bifactor or higher-order structure that may support the use of the MIOS total score. This does not necessarily mean that the use of the MIOS total score is inadequate. However, we argue that further psychometric evaluation of the MIOS structure is needed to judge the adequacy of its total score as an indicator of general MI symptom severity. This is especially relevant, as depending on the applied scoring algorithm, the MIOS may perform differently in screening for MI, estimating prevalence, association with other constructs, or monitoring change in symptoms over the course of treatment. In our sample, we initially found a mismatch between the proposed measurement model for the MIDS and the data. After allowing for theoretically justifiable residual covariances between three item pairs, model fit improved to an acceptable standard. Although this may be specific to our sample or the German version of the MIDS and should be replicated both in German and in other languages, we regard this as cautionary support for the proposed unidimensional structure of the MIDS. Therefore, both measures seem suitable for assessing MI and related distress in German-speaking populations.
Limitations and Future Research Directions
Constraints on generality include the limited diversity of our sample in terms of ethnicity. While gender was balanced in our sample, most participants were White Western Europeans, aged 40 to 59, employed, partnered, and university-educated, limiting to some extent the generalizability of the findings to more diverse populations. Despite efforts to include a diverse sample, however, this demographic composition was expected given the nature of these occupational fields in Germany, where a university degree is often a prerequisite, and systemic inequalities in access to higher education. Nonetheless, these characteristics and the cultural context should be considered when interpreting the findings.
As with most studies on MI, a major limitation concerns our cross-sectional design. With few exceptions (e.g., Levinstein et al., 2024), most research comprises retrospective and cross-sectional studies that are based on self-report. Particularly, an important limitation is related to unaccounted third variables (e.g., shared method variance, mood, or response biases) and directionality problems (e.g., impact of current stressors, functional impairment and other symptoms on PMIE exposure) present in cross-sectional studies (Litz, 2025). In fact, this reporting bias was also found in the assessment of trauma exposure and PTSD symptoms (Roemer et al., 1998; Southwick et al., 1997). Moreover, most of the few longitudinal studies (e.g., Levinstein et al., 2024) relied on panel data rather than intensive longitudinal data required for multilevel modeling and network analyses. Person-specific approaches (e.g., idiographic study designs) would enable personalized models of psychopathology (Wright & Woods, 2020). In fact, the individual psychopathology reported by people suffering from MI likely results from the type of PMIE (i.e., perpetration- vs. victimization-based events like betrayal). Thus, longitudinal observational studies that collect time-series data could illuminate the development and persistence of MI-related psychopathology (Koenig & Al Zaben, 2021). Ecological momentary assessment (EMA)/experience sampling methods (ESM; Myin-Germeys & Kuppens, 2022) could be used to collect data on the frequency of exposure to PMIE, their perception of moral transgressions, post-event processes related to updating moral beliefs, and their impact on MI-related mental health outcomes (Herzog & McNally, 2025). Such studies could reveal risk and protective factors that moderate the connection between exposure to PMIEs and sustained MI-related health outcomes, and mediators of outcomes over time.
Further, the results of the D16 should be interpreted cautiously. While a strength of this study was to include a measure for socially aversive personality traits, a self-report instrument cross-sectionally applied cannot determine the dynamics of (critical) life events and the formation of personality.
Moreover, following Litz et al. (2022), allowing participants who did not endorse a PMIE to rate the MIOS and MIDS (instead indexed to the worst and most currently distressing life stressor) would enable tests of the assumption that MI is a PMIE-related phenomenon. Also, future studies could investigate the relationship with trauma-related cognition scales such as the PTCI (Foa et al., 1999) or PTES (Herzog et al., 2023) to determine the incremental validity of MI scales (Bryan et al., 2018). Considering that the perception of PMIE and their outcome is highly context-dependent, future research should investigate various systemic factors, but also contextual peculiarities (e.g., situational characteristics) that influence moral decision-making in high-risk situations.
In future MI research, extensive stakeholder involvement will be crucial for moving the field of MI science forward. Stakeholders may include, but are not limited to, philosophers, theologians, military personnel, police, firefighters, paramedics, nurses, physicians, social psychologists, psychiatrists, social workers, religious ministers, teachers, and prison guards.
Finally, while the construct validity process for psychological constructs like MI is generally of an ongoing, indeterminate nature (Strauss & Smith, 2009), research needs more informative theory tests regarding fully specified theories with falsifiable hypotheses and predictions (e.g., by using experimental paradigms; Stenkamp et al., 2026) to lift MI science to a more paradigmatic state.
Implications
On a general note, the field of PMIE exposure and MI screening faces the same challenges as for trauma exposure and PTSD screening (e.g., PCL-5) in the last decades (McDonald & Calhoun, 2010): Reported rates demonstrate significant variation across populations, settings, and research methods, that may be affected by confounding factors related to mental health stigma and the economics of employment and disability compensation, leading potentially to under- and over-reporting. As such, screening tools should never be used as a diagnostic or gatekeeping threshold for categorical caseness determination. Therefore, self-report measures for occupational mental health such as the MIDS and MIOS can only serve as (pre-clinical) screening instruments and should be treated as one data point in the context of a comprehensive assessment to trigger further face-to-face diagnostic evaluation and access to care. While both measures now provide cut-off scores that help to estimate population-wide prevalence, these scores are not indicative or decisive for determining the treatment needs of an individual, but to identify people in need of further clinical assessment. Thus, they should be incorporated into a comprehensive occupational mental health prevention program as one component of Selective Prevention. Once a gold-standard method for assessing MI has been established, future studies should calculate reproducible Receiver Operating Characteristics (ROC) curves aiming to determine optimal diagnostic threshold scores on these self-report measures, considering maximized sensitivity and specificity. For this purpose, developing a (structured) clinical interview for assessing MI will be an important step in this direction, along with more theoretical work to support the construct validity of MI (Strauss & Smith, 2009). However, the efficacy of such a strategy for MI needs to be determined empirically. For example, in the context of PTSD, a large cluster RCT in the U.K. military found that post-deployment screening plus tailored advice did not reduce later prevalence of PTSD and other mental disorders (depression, anxiety, alcohol misuse) and did not increase help-seeking compared with general advice (Rona et al., 2017).
Supplemental Material
sj-docx-1-asm-10.1177_10731911261457278 – Supplemental material for Measuring Moral Injury Outcome and Distress in High-Risk Populations in Germany: A Validation Study
Supplemental material, sj-docx-1-asm-10.1177_10731911261457278 for Measuring Moral Injury Outcome and Distress in High-Risk Populations in Germany: A Validation Study by Philipp Herzog, Simon Stenkamp, Sonya B. Norman, Richard J. McNally and Julia A. Glombiewski in Assessment
Supplemental Material
sj-pdf-2-asm-10.1177_10731911261457278 – Supplemental material for Measuring Moral Injury Outcome and Distress in High-Risk Populations in Germany: A Validation Study
Supplemental material, sj-pdf-2-asm-10.1177_10731911261457278 for Measuring Moral Injury Outcome and Distress in High-Risk Populations in Germany: A Validation Study by Philipp Herzog, Simon Stenkamp, Sonya B. Norman, Richard J. McNally and Julia A. Glombiewski in Assessment
Supplemental Material
sj-pdf-3-asm-10.1177_10731911261457278 – Supplemental material for Measuring Moral Injury Outcome and Distress in High-Risk Populations in Germany: A Validation Study
Supplemental material, sj-pdf-3-asm-10.1177_10731911261457278 for Measuring Moral Injury Outcome and Distress in High-Risk Populations in Germany: A Validation Study by Philipp Herzog, Simon Stenkamp, Sonya B. Norman, Richard J. McNally and Julia A. Glombiewski in Assessment
Footnotes
Acknowledgements
The authors are very grateful to Clarissa Trey, who likewise contributed to the study.
Ethical Considerations
The local ethics committee of the Department of Psychology at the RPTU University Kaiserslautern–Landau approved this study (reference number #LEK-544). This study was conducted in accordance with the ethical standards specified in the Declaration of Helsinki (1964) and its later amendments.
Informed Consent Statements
Participation in this study was voluntary and no financial benefit was offered. Before inclusion in this study, all patients gave written informed consent.
Author Contributions
PH: Conceptualization, Data curation, Investigation, Methodology, Project administration, Validation, Visualization, Writing—original draft, review and editing. SS: Methodology, Formal analysis, Visualization, Writing—review and editing. SBN: Supervision, Writing—review and editing. RJM: Conceptualization, Supervision, Writing—review and editing. JAG: Investigation, Resources, Supervision, Writing—review and editing. All authors approved the final version of the paper for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.