
Abstract
Introduction
Advance Care Planning (ACP) is a patient-centered process that enables individuals to consider their goals and priorities and make plans with their healthcare team for future care. Oncology clinicians care for critically ill patients and are central to facilitating and documenting ACP. While Australian and international guidelines strongly support ACP in oncology, clinician engagement and documentation of ACP remain suboptimal. This study aimed to explore oncology clinicians’ ACP knowledge, decision-making, and practice, including factors influencing engagement in ACP.
Methods
A qualitative study was conducted using semi-structured interviews with oncology clinicians from three metropolitan hospitals in New South Wales, Australia. Participants were purposefully sampled and interviewed between November 2021 and March 2022. Interviews were audio-recorded, transcribed, and analyzed using deductive thematic analysis guided by the Theoretical Domains Framework (TDF). An inductive approach was subsequently applied to develop explanatory subthemes within identified domains.
Results
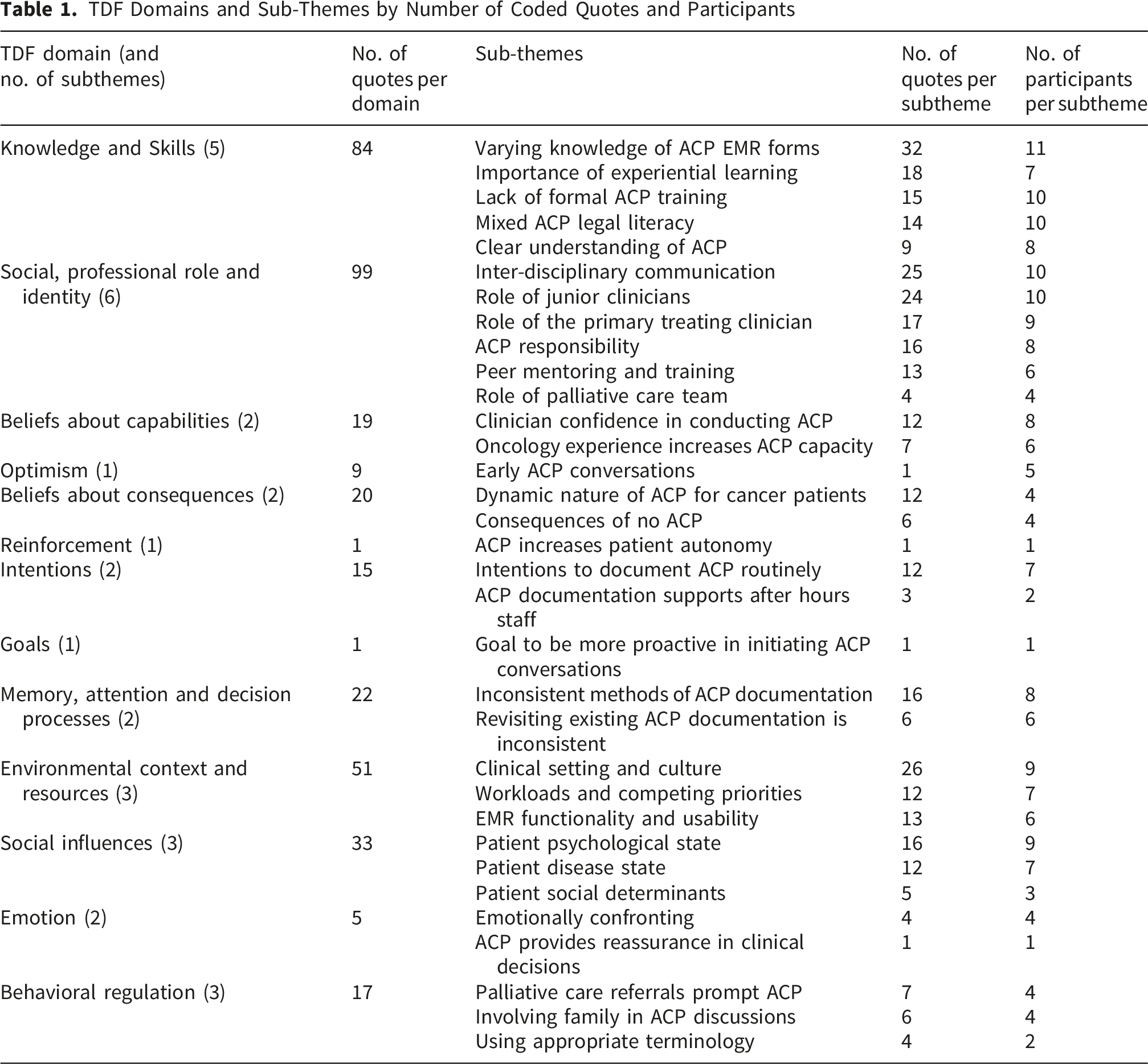
Eleven clinicians participated, including Medical/Radiation Oncology Consultants (54.5%) and Advanced Trainees (45.5%). Interview length ranged from 17.5 to 35.5 minutes. A total of 380 quotes were coded across all 14 TDF domains, generating 33 explanatory subthemes. Four domains were most influential: Knowledge and Skills, Social/Professional Role and Identity, Environmental Context and Resources, and Social Influences. Although all participants recognized ACP as best-practice care, engagement was influenced by limited formal training and legal literacy, uncertainty regarding responsibility for initiating and documenting ACP, variable inconsistent interdisciplinary communication, workload and time constraints, electronic medical record functionality, and patient characteristics (i.e.,psychological state, health literacy, cultural complexity).
Conclusion
ACP in oncology is shaped by complex, interdependent socio-cultural and organizational factors. Applying the TDF identified key behavioral and contextual determinants. Improving ACP requires multilevel strategies targeting clinician capability, role clarity, and system-level supports, including structured education, clearer documentation processes, improved electronic medical record functionality, and integration of ACP into routine multidisciplinary care.
Plain Language Summary
Advance care planning (ACP) helps people think about and discuss the care they would want in the future. For people with advanced cancer, ACP can improve quality of care, reduce unwanted treatments, and help patients and their families feel more supported. Although guidelines recommend early ACP in cancer care, it does not always happen consistently. This study explored why, by interviewing 11 cancer clinicians (both senior specialists and junior clinicians) from New South Wales, Australia. Researchers asked about their experiences with ACP conversations, documentation, and what helps or prevents them from doing ACP. The interviews were analyzed using a behavioral framework to identify key influences on practice. All clinicians agreed ACP is an important part of patient care. However, several challenges were identified. Many clinicians reported limited formal training in ACP, especially around legal aspects and how to document plans correctly in electronic medical records. Most had learned through experience. There was uncertainty about who is responsible. While senior cancer specialists were seen as best placed to lead discussions, junior clinicians often completed documentation. System barriers played a major role. Time pressures in busy outpatient clinics made it difficult to have early ACP conversations. Some clinicians found hospital electronic medical record systems hard to use or not well integrated with systems used in oncology. Finally, patient factors influenced timing. Clinicians found ACP more difficult to navigate when patients were distressed or not ready to have ACP conversations. The study concludes that improving ACP in cancer care requires better training, clearer role definitions, improved electronic systems, and stronger integration of ACP into routine care.
Keywords
1. Introduction
Advance Care Planning (ACP) is a patient-centered process that enables individuals, with their families/carers, to consider their goals and priorities and make plans with their healthcare team for their future care needs.1,2 A key component of ACP is the documentation of these conversations and decisions within electronic medical records (EMRs) to ensure that patient preferences are accessible across healthcare providers.3,4 In the Australian study context, EMR documentation in New South Wales (NSW) involves the creation of an ‘adult resuscitation plan’, a medically authorized order to use or withhold resuscitation measures, as well as documentation of patients’ goals and wishes. The EMR also allows for more comprehensive ACP documentation beyond resuscitation decisions, and storage of patient-derived Advance Care Directives. 5 Appropriate ACP, including resuscitation documentation, has been shown to positively impact the quality of end-of-life care by lowering rates of ventilation, resuscitation, intensive care unit admission, care costs, and provide earlier access to palliative care support.6,7 It also ensures the care patients receive is concordant with their wishes and preferences, increases satisfaction with the care provided for families and carers, and may reduce unwanted and unnecessary treatment.6,8,9
ACP is recommended for patients diagnosed with a life-limiting illness, including advanced frailty. Given their poor prognosis and increased risk of deterioration, advanced cancer patients are ideal candidates for ACP.10,11 The benefits of ACP in oncology are widely supported by Australian and international guidelines.11-16 It is increasingly an expectation of high-quality patient care that ACP occurs early for advanced cancer patients. 17 Despite this, ACP initiatives, policies, and procedures are not systematically implemented across Australian cancer services, as reflected in the suboptimal uptake of ACP. 18 In Australia, only 27% of cancer patients were reported to have ACP documentation in the National Advance Care Directive Prevalence Study, 19 with similarly low rates reported internationally.12,13,20-22 Evidence also indicates that inpatient hospital settings are the most common place of death for cancer patients,23,24 and that documented end-of-life conversations frequently occur for the first time during hospital admissions in patients’ final weeks of life.25,26 These findings highlight the importance of understanding how ACP is conducted within hospital oncology settings.
Although studies in ACP within the advanced cancer population have been published, these have largely been quantitative investigations, with limited qualitative studies, and a strong focus on patient perspectives.18,27,28 Oncology clinicians are central to facilitating and documenting ACP conversations to promote shared decision-making in accordance with their patients’ values and preferences for medical care.29,30 This lack of consistent implementation contributes to variation in practice and limits insight into how ACP is conducted in hospital settings, particularly from the clinician perspective. As a result, there is limited understanding of the contextual, organizational, and behavioral factors that influence clinicians’ engagement with ACP in cancer care and related ACP documentation.
Qualitative research is therefore essential to address these gaps by exploring oncology clinicians’ lived experiences, perceptions, and decision-making processes, as well as the contextual and implementation factors that shape ACP practice in hospital settings. To move beyond descriptive accounts of barriers and facilitators, this study adopts a theory-informed approach using the Theoretical Domains Framework (TDF). While previous studies, not limited to cancer, have reported a range of social factors that affect the uptake and utility of ACP, many have not utilized behavioral theory, limiting their ability to inform targeted intervention design. The TDF synthesizes constructs from psychological, behavioral, and organizational theory into 14 domains, enabling systematic identification of potentially modifiable determinants of clinical behavior.31,32 Applying the TDF allows for a more comprehensive understanding of how individual clinician factors (such as knowledge, skills, and beliefs), social influences, and environmental or system-level influences shape ACP practice, thereby strengthening the translational relevance of the findings.
Guided by the TDF, this study aimed to explore oncology clinicians’ knowledge, attitudes, and experiences related to ACP conversations and end-of-life decision making in clinical practice, and to identify factors influencing their engagement in ACP.
2. Methods
2.1. Design and Setting
This qualitative study utilized semi-structured interviews with oncology clinicians from three hospitals in metropolitan New South Wales. This methodology was selected as it focuses on the knowledge of the participant and allows an in-depth description of context and practices, experiences in advance care planning. 33 The reporting of this study conforms to the Consolidated criteria for Reporting Qualitative Research (COREQ) guidelines. 34
2.2. Sample
A purposeful sampling strategy was used to recruit oncology clinicians within the participating sites, inclusive of Medical and Radiation Oncology Consultants and Advanced Trainees working in hospital outpatient cancer centers and on the inpatient oncology ward. 35 Advanced Trainees are clinicians completing advanced training in oncology at accredited network training sites over approximately 3-5 years as required for fellowship within their relevant Australasian professional college. Advanced Trainees are supervised by Senior Consultants.36,37
Potential participants were recruited via a promotional blurb distributed by a member of the research team to all 23 medical and radiation oncology staff and Advance Trainees, which include clinicians with varying levels of clinical experience and exposure to ACP. which included a link for participants to complete an expression of interest form. A researcher then followed up with the participation information statement and consent form. Sample size was determined using Francis et al.’s framework for theoretically-rooted interviewing, which sets an a priori minimum sample size of 10, with a ‘stopping criterion’ when three interviews do not identify new themes. 38
2.3. Interview Procedure
The interviews were semi-structured with an approved interview guide (Supplementary Material File 1) sent to participants prior to the interview. A responsive interviewing style to allow in-depth discussion in three key areas: (1) the participant’s understanding of ACP and professional experience, (2) documentation and interprofessional communication, and (3) perceived barriers and enablers to ACP. Field notes were taken during the interview to aid in a flexible and responsive interviewing style. Participants focused their responses on their professional experiences within their current employment in the study setting, allowing for reflection of prior working experiences. Interviews were conducted by videoconference between November 2021-March 2022 by one of three trained and experienced qualitative female researchers (CD – PhD, Research Fellow, AJ – PhD, Senior Research Fellow, KS – PhD, Research Officer). Only the interviewer and the participant were present throughout the interview. Certain researchers knew participants from previous projects. The interviewer provided a short introduction of themselves and the study prior to the interview.
2.4. Data Analysis
All interviews were audio-recorded and transcribed verbatim. Three researchers conducted the analysis (CD, AJ, KS). Interview data were analyzed using a framework analysis approach comprised of familiarization, identification of a framework, indexing, charting, and mapping and interpretation. 39 As the researchers conducting the interviews were also responsible for the analysis, the initial familiarization stage began during the interview process. Sets of transcripts were allocated to the three researchers, with each transcript coded by two researchers. Quotes within transcripts were coded according to the TDF using Microsoft Excel (version 16.99.2). A coding tree with context-specific definitions for each of the 14 TDF domains was developed and used to guide the deductive coding to index quotes to the TDF (Supplementary Material File 3 - TDF Framework Coding Interpretation). The researchers met to discuss all agreements/disagreements of independent coding.
The data were then analyzed utilizing an inductive approach to thematically chart explanatory subthemes within identified domains. Sub-themes are qualitative descriptions of interview findings that further provide context to the TDF domains. The decision to present the findings as both TDF domains and emergent subthemes was made to provide context to the theoretical findings and ensure that data were meaningful for the development of an intervention. This involved two researchers coding interview transcripts, which were then sent for collation prior to meetings to discuss all agreements/disagreements in coding. Any coding disagreements were resolved through discussion.
To prioritize themes for presentation of results, an assessment of frequencies was conducted using previously published criteria to determine the likely importance of TDF domains in influencing behaviors related to ACP; (1) number of quotes assigned to a domain, (2) number of quotes assigned to a subtheme, and (3) number of individual participants within a subtheme.
2.5. Ethics Approval Statement
This study was reviewed by an independent Human Research Ethics Committee and granted permission to conduct the study by Western Sydney Local Health District Human Research Ethics Committee on 2 July 2021 (HREC No. 2021/ETH00416). This study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2024.
2.6. Consent Statement
Informed consent was obtained from all participants in this study, including consent to have interviews audio-recorded and transcribed. The informed consent listed the investigators, role in the research project, and described the purpose of the research.
3. Results
A total of 11 oncology clinicians completed the expression of interest form for the study and participated in the study. There was no response from non-participants. The sample size met the priori minimum sample size of 10, and information saturation was met where no new sub-themes were identified in the final three interviews. Participants included senior Medical and Radiation Oncology Consultants (n=6, 54.5%) and oncology Advanced Trainees (n=5, 45.5%). Participants had professional experience within Australia and internationally across a range of clinical contexts. Interview length ranged from 17.5 to 35.5 minutes. All participants noted that ACP conversations are often complex and difficult but are essential to delivering high quality, patient-centered care.
TDF Domains and Sub-Themes by Number of Coded Quotes and Participants
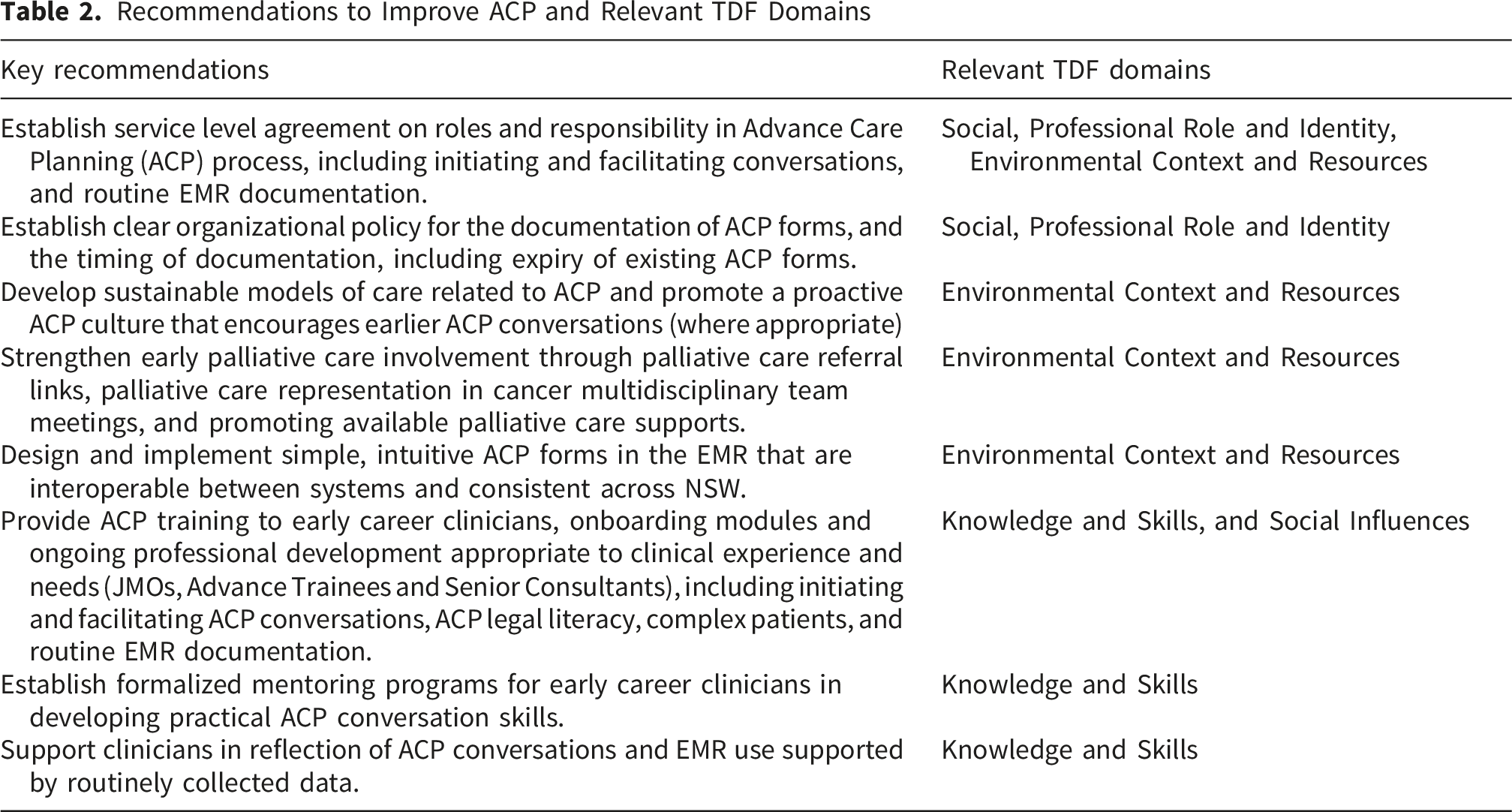
Recommendations to Improve ACP and Relevant TDF Domains
3.1. Social, Professional Role and Identity
The most prominent sub-themes within this domain focused on which healthcare professionals were responsible for conducting and documenting ACP conversations. Participants (n=9) identified Medical Oncology or Hematology Consultants as the primary treating clinicians to initiate and lead ACP discussions due to their established rapport with patients. “The surgeon is usually involved earlier on. The radiation oncologists tend to sort of be in and out of charge, rather than continually in charge. So, it's mostly medical oncology and hematology.” – P1
Participants (n=10) frequently discussed the role of junior clinicians in ACP. Some participants (n=8) acknowledged that Advanced Trainees may have ACP discussions, supported by and in consultation with a Senior Consultant, but that documentation was primarily the responsibility of Advanced Trainees and Registrars. “I think starting from being a registrar, we are put in positions we do lead those conversations… And always with support from a consultant in difficult situations. But I think from about that level, we do get involved in them.” – P9 “The Registrar often documents. I might have the conversation because I’ve seen the patient with them, but the Registrar is usually documenting.” – P2
One participant noted that Junior Medical Officers (JMOs) conduct multiple patient reviews when cancer patients are admitted to the hospital, so they may incidentally be involved in an ACP conversation initiated by the patient. One participant described Senior Consultants’ varied preferences for Advance Trainee involvement. “They [Senior Consultants] all have their own preferences. Some consultants want to have that conversation on their own, some are happy for us to have that conversation. So you get to know which bosses want to have those conversations and which don’t.” – P7
Participants (n=10) noted the responsibility of clinicians to communicate ACP discussions and any documentation with the healthcare team, however the methods for this interdisciplinary communication varied between participants. Some participants expressed that EMR documentation is a key part of their role, given that other clinicians may rely on this information to make clinical decisions, whereas others noted some reluctance to use the EMR forms for communication. “Sometimes the patient will tell you things that they haven’t necessarily told others in the team yet. I think communicating that back to the consultant who’s looking after them is part of the role.” – P3
3.2. Knowledge and Skills
Participants held similar definitions of ACP, but most participants (n=10) indicated limited understanding of the legal aspects of ACP in critical decision-making. Participants (n=10) noted a lack of training specific to ACP throughout their early medical training or orientation at the clinical site or identified ACP as a gap in education. “Even the idea that it’s a medical decision has kind of just been informally passed down. I can’t remember that there’s been formal training. I do remember being shown how to electronically document, once we had shifted from paper to electronic records, but again, there wasn’t formal training involved.” – P6
Participants (n=7) reflected on the importance of experiential learning and noted that clinical experience and observing Senior Consultants were large facilitators to their ACP knowledge and skills. Some participants (n=4) reflected on negative patient experiences throughout their career, describing these events as significant learning points in ACP. “I think we really learn by mistakes, which is not good because you upset people when you learn by mistakes in the real setting. I think it’s an art doing this discussion. We have to learn over the time. But I think some basic kind of a principle is necessary” – P8
The most prominent sub-theme, ‘knowledge of ACP EMR forms’ was discussed by all participants (n=11), but views were conflicting. Some participants stated that the EMR forms for documenting ACP details and resuscitation plans were simple and straightforward to complete. Whilst other participants reported the form as difficult to use, or not knowing where to access the form, and not having any training or guidance on how to complete the form. A clear distinction in familiarity with the EMR forms was observed between Advanced Trainees and Senior Consultants. “I have completed that documentation multiple times on my own accord, so I know where to find it. I don’t know necessarily whether all consultants know how to find that. There may be times when consultants have made those decisions, had those discussions, but may not have documented in the pro forma just because it’s difficult.” – P5 “I have no idea how to document it in the notes. I have been shown, but then it changed the next week. And then it changed again. And it’s a reality I’m not going to bother to learn because it’s not as simple as it sounds.” – P1
3.3. Environmental Context and Resources
Participants (n=9) discussed the clinical setting of ACP conversations, and that they don’t regularly occur in the outpatient clinic context. However, two participants noted starting those conversations in the outpatient clinic to ensure it is documented if the patient were admitted to hospital. “I think we definitely do ACP in the inpatient setting. It’s quite ingrained. But I guess in the outpatient setting, which is where it is important in order to have future planning, it’s not systematic. It’s still on an individual practitioner basis. Yeah. And a case-by-case basis as well.” – P9
Participants (n=7) recognized the time constraints of outpatient consultations, where discussion of the patients’ results, treatment, and side effects were the priority. “Unfortunately, we don’t have those conversations enough as an outpatient in the clinics due to the constraints of our clinics, unfortunately and the workload.” – P6 “That’s something I have to improve [ACP in outpatient clinic]. Because you’re getting through so much information with them in a clinic appointment, it’s hard. That’s one thing I struggle with - how to incorporate that into the clinic environment.” – P3
Another barrier to ACP in the outpatient clinic included the usability and interoperability between the hospital-wide EMR where ACP forms are located and the Oncology Management Information System (OMIS) used in cancer. “All of our documentation is on a different system. On [the EMR], there’s a very clear space for ACP and resuscitation plans. On [the OMIS], there’s not and there isn’t a pre-populated field. You have to go into [the EMR] to document it. So, that would be a trigger to do ACP if it was actually part of [the OMIS].” – P3
Two participants reflected on facilitators to ACP in past work experiences in other countries or organizations, where initiating ACP conversations in the outpatient setting was part of the organizational policy. Some participants (n=4) recognized facilitators, such as the local palliative care referral process, which requires ACP and resuscitation plans to be documented in the EMR before the patient is referred, acting as a prompt for clinicians to have ACP conversations and document them. Furthermore, one participant highlighted the value of Palliative Care Specialist attendance at tumor-specific Multidisciplinary Team (MDT) meetings to advocate for palliative care discussion and referral. “I think our MDTs are really helpful. Our head of palliative care was in ours, having palliative care there has been good at just reminding everyone what’s the big picture.” – P3
3.4. Social Influences
Patients’ psychological state was repeatedly highlighted by participants (n=9) as influential in initiating ACP conversations and revisiting previously documented ACP. ACP in cancer was described as dynamic, and patient wishes can change depending on their disease and psychological state. “I think a barrier is the patient’s psychological state, whether they’re in the mindset to embrace some of these conversations, whether they have a clear understanding of their prognosis. When someone feels well, they might want to have all measures. When they’re feeling terrible, they’re very much understanding that there may not be much we can offer them” – P3
Some participants noted that fluctuations in this psychological state were a barrier to recording ACP details in the EMR. Participants reflected on highly complex patient cases including patients who are younger, culturally and linguistically diverse, have lower health literacy, have complex family dynamics, lack acceptance of prognosis or have additional mental health issues. Participants noted in these cases the increased importance of involving family for in-person discussions and using appropriate terminology tailored to the patient and family.
3.5. Other Prominent Sub-Themes
In the Memory, Attention, and Decision-Making domain, there was one other prominent sub-theme, ‘inconsistent methods of ACP documentation’. Participants (n=8) reported differing locations and timing of ACP documentation. One participant noted that if the patient is being treated with curative-intent and would like full measures, they don’t typically document that information. One participant described following a set rubric for their documentation, whereas others described writing a general reflection of the discussion, sometimes in the free-text clinical notes of the OMIS used in outpatient clinics, rather than the ACP forms in the hospital-wide EMR. “It depends. If they’re for full measures, I wouldn’t generally write anything there, which I probably should.” – P4 “If I have actually had that formal discussion with the patient, then I will go into [the EMR] and document it.” – P3
There was also inconsistency in clinicians checking existing ACPs in the EMR. Whilst some participants reported routinely revisiting a patient’s ACP as standard practice, but noted that not all clinicians will, and one participant noted that once they document an ACP, they often never revisit it.
4. Discussion
This study investigated the knowledge, opinions, and experiences of Medical and Radiation Oncology Consultants and Advanced Trainees, in facilitating and documenting ACP, underpinned by a theoretical framework to systematically identify factors influencing ACP discussions and documentation. Participants consistently recognized ACP as an essential component of high-quality, patient-centered oncology care, and agreed that early discussions, led by the primary treating oncology clinician and communicated across the multidisciplinary team, represent best practice. However, it was also acknowledged that translation into routine clinical practice is inconsistent, with multiple co-dependent barriers and enablers identified across individual, team, and organizational levels.
Using the TDF, interview quotes principally reflected subthemes under Social/Professional Role and Identity, Knowledge/Skills, and Environmental Context and Resources, and Social Influences. This study identified inconsistent interdisciplinary communication practices, and some ambiguity in professional roles, which may limit accountability for ACP processes. Similarly, a lack of formal training, reliance on experiential learning and variable legal understanding highlight areas for professional development. Organization and system level factors including competing clinical priorities, limited consultation time, and challenges navigating EMR systems illustrate how environmental constraints can restrict opportunities to engage in ACP. In addition, highly complex cancer patients appear to influence clinicians’ decision-making processes around when and how to initiate ACP, contributing to variability in practice. The findings of this Australian-based study draw parallels with existing international studies in ACP and end-of-life care. Previous literature has identified several patient-, health professional-, and system-level factors affecting ACP across various areas of healthcare,27,40 Whilst the identified sub-themes in this study are particularly complex and dynamic in nature, the use of the framework reinforces important factors to target in improving clinicians’ ACP engagement across multiple system levels.
4.1. Social, Professional Role and Identity: ACP Roles and Responsibility, Inter-Disciplinary Communication and Documentation of ACP in the EMR
Although participants identified medical oncology consultants are best positioned to conduct ACP conversations in an ideal clinical scenario, participants acknowledged that most cancer patients have a non-linear care path with various care providers. As a result, ACP discussions may occur opportunistically with emergency department clinicians, junior doctors during night shifts, or other specialty teams managing comorbidities. This underscores the need to clearly define responsibility and roles within the ACP process, strengthen inter-disciplinary communication, and ensure reliable and accessible ACP documentation.
The purpose of EMR ACP forms is to record patients’ end-of-life goals and care preferences and communicate these with other health professionals who may need this information. 3 However, the findings reveal a disconnect between the intention of EMRs and clinical practice. Participants differed in how they understood their responsibilities regarding documentation, with expectations reflecting the professional hierarchy, with early-career clinicians commonly expected to undertake EMR documentation. Some participants reported not knowing how to document or access existing ACP records or considered documentation not part of their professional role. In addition, considerable variation was reported in documentation practices, with some clinicians recording ACP discussions in free-text notes, others using different electronic systems, and not documenting ACP conversations at all. This suggests not only technical fragmentation but also cultural and governance gaps.
Consistent with international findings, there remains a lack of standardization in ACP documentation practices and limited guidance on the use of EMR ACP forms across diverse digital platforms.3,4,27 Fragmented and inconsistent documentation increases the risk that cancer patients may receive interventions that are misaligned with their values and preferences. Addressing this issue requires system-level improvements, including enhanced EMR forms and interoperability between data platforms, clear service-level agreements delegating ACP roles and responsibilities, organizational policies for standardized ACP documentation, and targeted staff training in best-practice ACP. Strengthening these processes may improve inter-disciplinary communication and promote continuity of care for patients with cancer.
4.2. Environmental Context and Resources: Integrating Routine ACP in Clinical Workflows
While ACP discussions were commonly reported in inpatient settings, considerable variability was described regarding ACP in outpatient cancer clinics. Participants highlighted the limited time allocated for outpatient clinic appointments where treatment discussions are prioritized, hindering the capacity to conduct ACP discussions. An American paper by Goswami 2021 suggested patients be scheduled for ACP discussions as an independent clinic visit, promoting time and space for shared decision-making and patient autonomy. 41 However, in the United States, ACP discussions can be billed as a separate visit, and patients can be scheduled for such discussions. 42 In Australia, there is no separate medical item billing to make the often long complex conversations of ACP adequately renumerated. These funding mechanisms may act as a systematic barrier to proactive ACP. Public health systems recording the value of ACP conversations could benefit the health service and community by avoiding expensive, futile care in the future.
The literature supports early palliative care involvement as beneficial to patients’ end-of-life care. 27 This study also highlighted the importance of the established palliative care support and palliative care referral links within this health service. For ACP in a cancer care setting, this study emphasizes the value of palliative care representation in cancer multidisciplinary team meetings. However, this would have an increased demand on specialist palliative care services, as found in previous interventions to improve ACP. 43 Cancer services need to consider how to redesign sustainable models of care to support timely initiation of ACP by oncology clinicians and provide access to specialist palliative input.
4.3. Knowledge and Skills and Social Influences: Building ACP Knowledge and Capacity
A lack of formal training emerged as a clear and modifiable factor to support clinicians in conducting ACP. Participants identified critical career stages for targeted education, including early career (JMO, registrar, and Advanced Trainee), onboarding at new cancer centers, and ongoing professional development. Knowledge gaps identified in this study included legal literacy of ACP, initiating ACP conversations among highly complex patient cases, and tailoring discussions to patients’ psychological readiness. Importantly, participants highlighted the need for culturally sensitive communication and appropriate terminology when engaging diverse patient populations. In a multicultural healthcare context, and with rising rates of early-onset cancers 44 it becomes increasingly important to build oncology clinicians’ capacity to engage in ACP conversations with younger patients cohorts and culturally and linguistically diverse communities.
In addition to formal education, participants reported learning through experience. Experiential learning and mentorship were strongly valued, with participants describing informal observation and modelling as central to skill development. While informal learning contributes to professional development, reliance on this method may perpetuate variability in ACP practice. Formalized training programs that incorporate evidence-based communication frameworks, role-play, and reflective practice have been shown to increase clinician competence and willingness to engage in ACP. 45 Embedding practical training, structured mentorship, and using routinely collected data to support audit, feedback, and reflective practice may further strengthen implementation. 11 This investment in both technical knowledge and social competencies may support the integration of ACP into routine care and promote more equitable engagement across diverse patient populations.
4.4. Implications for Policy and Practice
Despite the existence of state and national policy directives to create top-down governance processes for ACP and integrate resuscitation plans into the EMR,5,46-48 this study demonstrates a gap between governance frameworks and ACP in clinical practice. ACP documentation remains inconsistent, variable inter-disciplinary communication, and limited clarity regarding ACP roles and responsibilities suggest that policy endorsement alone is insufficient to achieve sustainable integration. Acknowledging these gaps is important to the development of strategies to proactively discuss and document ACP to mitigate these scenarios.
This study identified modifiable factors influencing ACP completion, which have been summarized in a Table 2 as a set of recommendations. Acting on these recommendations for system wide change in cancer care delivery requires the top-down support of organization policies coupled with well-established departmental processes.
4.5. Limitations
Some limitations of the study must be noted. Although oncology clinicians with various characteristics were invited, 50% of the invited staff participated in the study. There may be potential for responder bias, meaning that clinicians who were especially interested in end-of-life and ACP agreed to be interviewed, which may have influenced responses. This study did not include recruitment of other professional staff involved in cancer related ACP, including cancer nurse coordinators, and ED clinicians who have an important touchpoint with these patients. Furthermore, this study did not interview patients. The theoretical framework was used to conduct the analysis but not the development of the interview guide, which may have improved extraction of themes. Given that all participants work within New South Wales, Australia, this may limit the generalizability of the identified sub-themes. Furthermore, interviews were conducted from November 2021-February 2022, and the implementation of ACP documentation may have improved in some organizations, however many of the findings in this study are socio-cultural and environmental and have relevance beyond technological advances.
5. Conclusion
This study demonstrates the value of applying the TDF to understand factors influencing oncology clinicians’ engagement in ACP. Four domains were most influential in shaping clinicians’ ACP knowledge, decision-making, and practice: Knowledge and Skills, Social/Professional Role and Identity, Environmental Context and Resources, and Social Influences. Limited formal training, gaps in legal literacy, and reliance on experiential learning reflected potentially modifiable knowledge barriers. Uncertainty regarding responsibility for initiating and documenting ACP, alongside inconsistent interdisciplinary communication, highlighted the importance of defining professional roles and team processes. Organizational constraints including workload pressures, outpatient clinic appointment times, and EMR usability demonstrated the strong influence of environmental context on clinician behavior. Patient-related factors, such as the patients’ psychological state and cultural complexity, further affected timing and clinician confidence in initiating ACP conversations. Overall, these findings indicate that meaningful improvement in ACP implementation will require coordinated, multi-level strategies that align policy, funding, organizational processes, digital infrastructure, and workforce development.
Supplemental Material
Supplemental material - Factors Influencing Advance Care Planning in Oncology: A Qualitative Study of Clinician Perspectives Using the Theoretical Domains Framework
Supplemental material for Factors Influencing Advance Care Planning in Oncology: A Qualitative Study of Clinician Perspectives Using the Theoretical Domains Framework by Candice Donnelly, Kavisha Shah, Sally Greenaway, Paul Harnett, Tim Shaw, Anna Janssen in Cancer Control.
Supplemental Material
Supplemental material - Factors Influencing Advance Care Planning in Oncology: A Qualitative Study of Clinician Perspectives Using the Theoretical Domains Framework
Supplemental material for Factors Influencing Advance Care Planning in Oncology: A Qualitative Study of Clinician Perspectives Using the Theoretical Domains Framework by Candice Donnelly, Kavisha Shah, Sally Greenaway, Paul Harnett, Tim Shaw, Anna Janssen in Cancer Control.
Supplemental Material
Supplemental material - Factors Influencing Advance Care Planning in Oncology: A Qualitative Study of Clinician Perspectives Using the Theoretical Domains Framework
Supplemental material for Factors Influencing Advance Care Planning in Oncology: A Qualitative Study of Clinician Perspectives Using the Theoretical Domains Framework by Candice Donnelly, Kavisha Shah, Sally Greenaway, Paul Harnett, Tim Shaw, Anna Janssen in Cancer Control.
Footnotes
Acknowledgements
The research team would like to acknowledge the health professionals who participated in the qualitative interviews.
Ethical Considerations
Permission to conduct this study was granted by Western Sydney Local Health District Human Research Ethics Committee HREC No. 2021/ETH00416.
Consent to Participate
Informed consent was obtained from all participants in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Sydney West Transitional Cancer Research Centre (SWTCRC). The SWTCRC was funded by The Cancer Institute NSW under the Translational Cancer Research Centres (TRC) [15/TRC/1-01]. Funding provided salary support for Author CD.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due in accordance with the informed consent obtained from participants, the raw data (interview transcripts) cannot be shared or made public. Only aggregated findings and representative quotes are included in this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.