
Abstract
Introduction
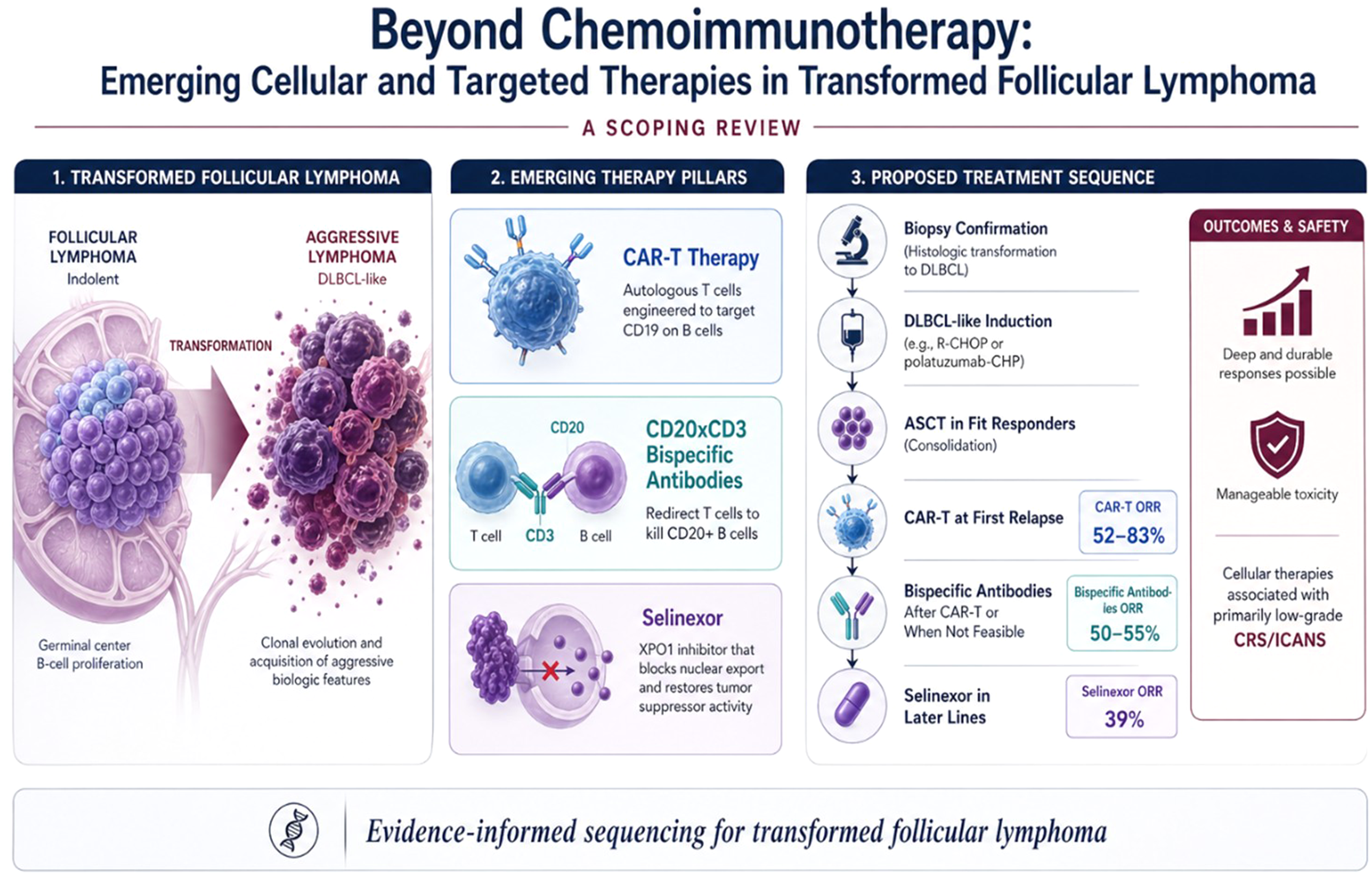
Transformed follicular lymphoma (t-FL) is an aggressive lymphoma with limited prospective evidence to guide treatment, particularly in the relapsed setting. We summarized the current evidence on emerging cellular and targeted therapies that extend beyond conventional chemoimmunotherapy.
Methods
This scoping review was conducted in accordance with the PRISMA extension for Scoping Reviews (PRISMA-ScR) and structured using the Population–Concept–Context (PCC) framework. Adults with histologically confirmed or strongly suspected t-FL were the population of interest. Findings were synthesized narratively.
Results
Seventeen studies met inclusion criteria across three therapeutic categories: CAR-T therapy (7 interventional trials, n = 130 t-FL patients in reported subsets), CD20×CD3 bispecific antibodies (BsAbs; n = 61 t-FL patients with extractable outcomes), and selinexor (n = 31 t-FL patients); together encompassing approximately 222 t-FL patients across primary interventional cohorts with extractable outcomes. CAR-T products achieved overall response rates (ORR) of 52–83% and complete response (CR) rates of 40–58%; randomized second-line trials favored axicabtagene ciloleucel and lisocabtagene maraleucel over standard care. In real-world CAR-T series, ORR ranged from 82–92% and CR rates from 64–67% across registry cohorts. BsAbs were active in heavily pretreated disease (epcoritamab ORR 50%/CR 44%; glofitamab ORR 55%/CR 35%), with predominantly low-grade cytokine release syndrome. Selinexor showed more modest efficacy (ORR 39%/CR 16%) but durable benefit in complete responders.
Conclusions
Current evidence supports a stepwise treatment framework: DLBCL-like induction at transformation, autologous stem-cell transplant in fit, chemosensitive responders, CAR-T as the preferred option at first relapse, BsAbs after CAR-T or when cellular therapy is not feasible, and selinexor in later-lines of therapy. Additional prospective t-FL–inclusive trials are needed to refine treatment selection and biomarker-guided sequencing.
Keywords
Introduction
Follicular lymphoma (FL) is the second most common non-Hodgkin lymphoma and the most common indolent subtype. 1 Although untreated patients typically survive for years, the natural history of FL can be dramatically altered by histologic transformation (HT) into a more aggressive lymphoma. The spectrum of indolent lymphomas susceptible to transformation includes FL, marginal zone lymphoma, lymphoplasmacytic lymphoma, and chronic lymphocytic leukemia/small lymphocytic lymphoma. 2
Among these, FL transformation has been the most extensively characterized, occurring at a consistent rate of 1–2% per year. 2 Transformation typically presents with rapid lymphadenopathy, extranodal disease, B symptoms, elevated lactate dehydrogenase (LDH), and occasional hypercalcemia. 2 Although historical outcomes were poor, contemporary management has improved survival, particularly when transformation occurs in patients with limited prior therapy.3-5
Despite these advances, prospective evidence specifically addressing transformed disease remains scarce. Most current treatment standards are extrapolated from subset analyses of trials in aggressive lymphoma, and several pivotal registration programs explicitly excluded transformed histology. This scoping review summarizes the available evidence on the diagnosis and management of t-FL, with a focus on emerging cellular and targeted therapies, and proposes an evidence-informed management algorithm to support clinical decision-making and identify research priorities.
Methods
Protocol and Registration
This scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist (Tricco et al, 2018), and the methodology of Arksey and O'Malley as refined by the Joanna Briggs Institute. The completed PRISMA-ScR checklist is provided as a supplementary file. A formal protocol was developed a priori and is available from the corresponding author on request. The review was not pre-registered; however, all eligibility criteria, search strategy elements, and data-charting variables were defined before screening.
Review Questions and PCC Framework
The review was structured around the Population–Concept–Context (PCC) framework. The Population comprised adults (≥18 years) with FL and histologically confirmed or strongly suspected histologic transformation. The Concept covered diagnostic strategies and therapeutic approaches, including chemoimmunotherapy, autologous and allogeneic stem-cell transplantation, CD19-directed CAR-T therapy, CD20×CD3 bispecific antibodies, and novel targeted agents (e.g., selinexor), with reported efficacy and safety outcomes. The Context included all care settings (clinical-trial and real-world) and all geographic regions, incorporating peer-reviewed studies and major hematology meeting abstracts with extractable t-FL data.
Eligibility Criteria
Eligible study designs were interventional trials and trial expansions (CAR-T, CD20×CD3 bispecific antibodies, selinexor); registries; and phase II/III randomized studies. Studies were required to report at least one efficacy endpoint — overall response rate (ORR), complete response (CR), duration of response (DOR), progression-free survival (PFS), event-free survival (EFS), or overall survival (OS) and/or safety outcomes including cytokine release syndrome (CRS), immune effector cell-associated neurotoxicity syndrome (ICANS), or grade ≥3 adverse events.
Reports published from 1 January 2000 through 31 May 2025, in any language, were considered. For mixed-histology datasets, inclusion required either explicit identification of a t-FL subset or sufficient detail to abstract t-FL–specific results. Single case reports, narrative editorials, and letters without primary data were excluded, as were studies with fewer than ten patients when no t-FL subgroup outcomes could be extracted, reports without separable t-FL data, pediatric-only studies, and purely diagnostic or radiologic reports.
Information Sources and Search Strategy
A systematic search was performed in three electronic databases: PubMed/MEDLINE, EMBASE, and the Cochrane Library. This was supplemented by manual screening of conference proceedings from the American Society of Hematology (ASH) and the European Hematology Association (EHA) from 2020 to 2025, as well as hand-searching the reference lists of recent narrative reviews.
The search strategy combined controlled vocabulary terms, including MeSH and Emtree, with free-text terms grouped under three core concepts and linked using Boolean operators: (i) “transformed follicular lymphoma” OR “histologic transformation” OR “Richter-like transformation”; AND (ii) “CAR-T″ OR “chimeric antigen receptor” OR “axicabtagene” OR “lisocabtagene” OR “tisagenlecleucel” OR “bispecific antibody” OR “epcoritamab” OR “glofitamab” OR “mosunetuzumab” OR “selinexor” OR “XPO1” OR “autologous stem cell transplant”; AND (iii) “efficacy” OR “response” OR “survival” OR “safety”.
Study Selection and Data Management
All retrieved citations were imported into EndNote 21 and de-duplicated. Reasons for full-text exclusion were recorded and are summarized in the PRISMA-ScR flow diagram (Figure 1). PRISMA-ScR flow diagram of the study selection process
Data Extraction
Extracted data items included bibliographic information, including first author, year, and country; study design and setting; sample size of patients with transformed follicular lymphoma; intervention and treatment line; key efficacy endpoints, including overall response rate (ORR), complete response (CR), duration of response (DOR), progression-free survival (PFS), event-free survival (EFS), and overall survival (OS); and safety outcomes, including cytokine release syndrome (CRS) grade, immune effector cell-associated neurotoxicity syndrome (ICANS), grade ≥3 adverse events, and treatment-related mortality.
Evidence Synthesis and Risk-Of-Bias Assessment
Consistent with PRISMA-ScR guidance, no formal risk-of-bias assessment was performed, as the aim was to map the breadth and nature of available evidence rather than to generate pooled comparative estimates. Quantitative meta-analysis was not performed because of marked clinical and methodological heterogeneity. Limitations of the underlying evidence base, including selection bias, small t-FL subgroups, and heterogeneous transformation definitions, are discussed in the limitations section.
Results
Selection of Sources of Evidence
The database search retrieved 680 records, supplemented by 45 records from conference proceedings and reference screening. After removal of 276 duplicates, 449 records were screened by title and abstract; 89 full texts were assessed for eligibility, and 17 studies fulfilled the inclusion criteria (Figure 1). The most frequent reason for full-text exclusion was lack of extractable t-FL data (n = 45).
Characteristics of Included Studies
Observational and Chemoimmunotherapy Studies in Transformed Follicular Lymphoma

DLBCL, diffuse large B-cell lymphoma; OS, overall survival; PFS, progression-free survival; t-FL, transformed follicular lymphoma; R-CHOP, rituximab-cyclophosphamide-doxorubicin-vincristine-prednisone.
CD19-Directed CAR-T Interventional Trials in Transformed Follicular Lymphoma
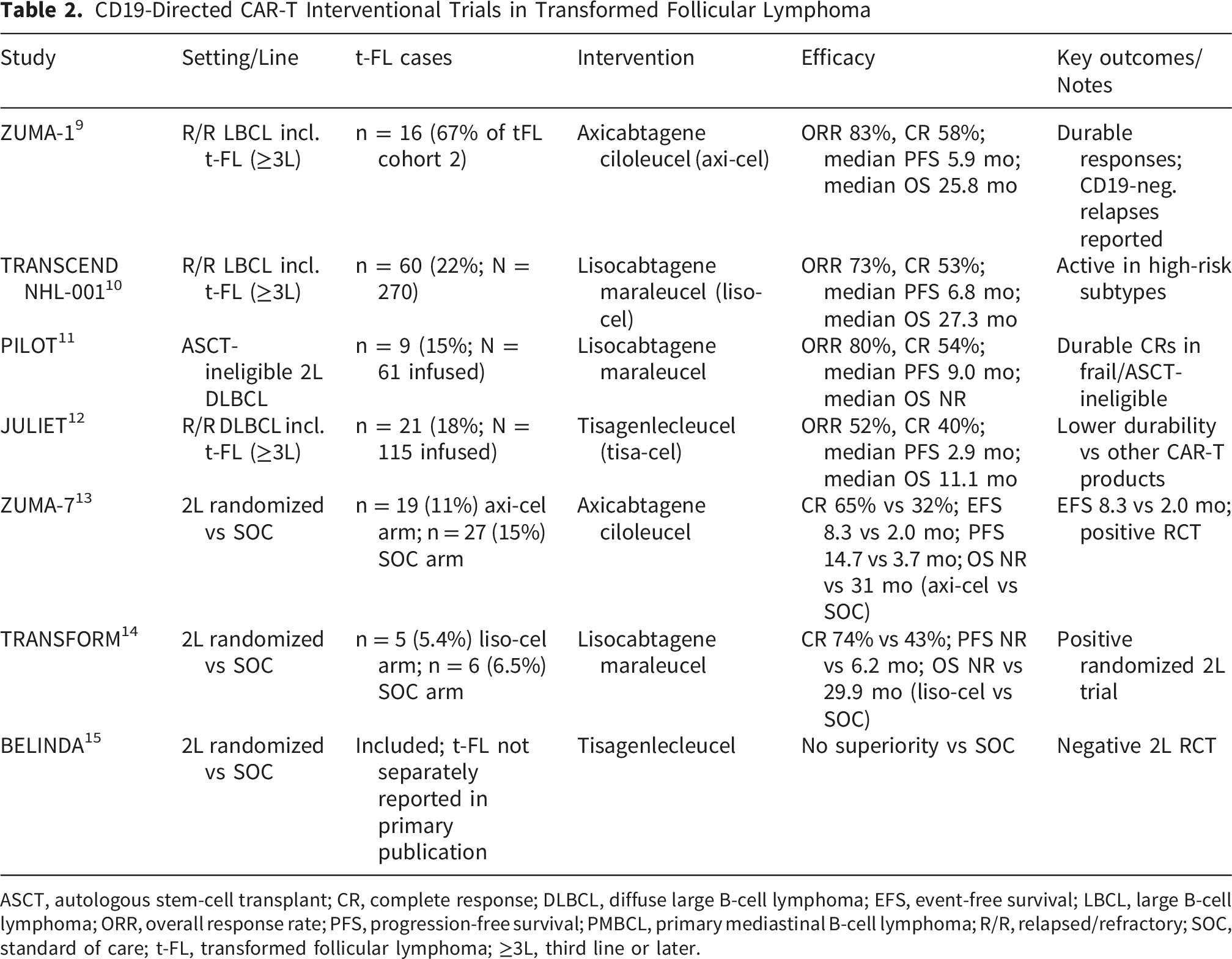
ASCT, autologous stem-cell transplant; CR, complete response; DLBCL, diffuse large B-cell lymphoma; EFS, event-free survival; LBCL, large B-cell lymphoma; ORR, overall response rate; PFS, progression-free survival; PMBCL, primary mediastinal B-cell lymphoma; R/R, relapsed/refractory; SOC, standard of care; t-FL, transformed follicular lymphoma; ≥3L, third line or later.
CD20×CD3 Bispecific Antibody Trials in Transformed Follicular Lymphoma

CAR-T, chimeric antigen receptor T-cell therapy; CR, complete response; CRS, cytokine release syndrome; DOR, duration of response; FL, follicular lymphoma; ICANS, immune effector cell-associated neurotoxicity syndrome; LBCL, large B-cell lymphoma; NR, not reached; ORR, overall response rate; PFS, progression-free survival; R/R, relapsed/refractory; t-FL, transformed follicular lymphoma.
Selinexor as a Targeted Agent in Transformed Follicular Lymphoma
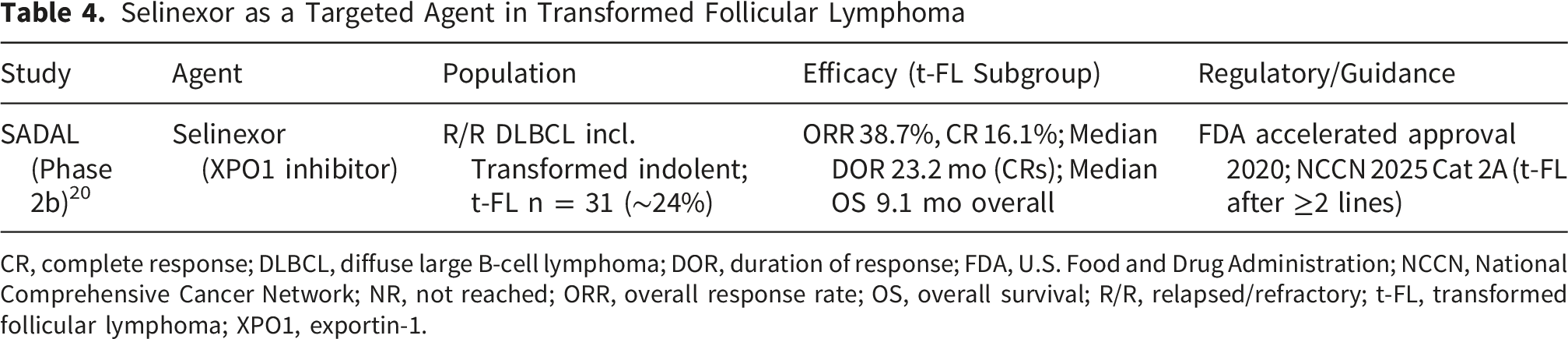
CR, complete response; DLBCL, diffuse large B-cell lymphoma; DOR, duration of response; FDA, U.S. Food and Drug Administration; NCCN, National Comprehensive Cancer Network; NR, not reached; ORR, overall response rate; OS, overall survival; R/R, relapsed/refractory; t-FL, transformed follicular lymphoma; XPO1, exportin-1.
Real-World, Case-Based, and Preclinical Evidence in Transformed Follicular Lymphoma
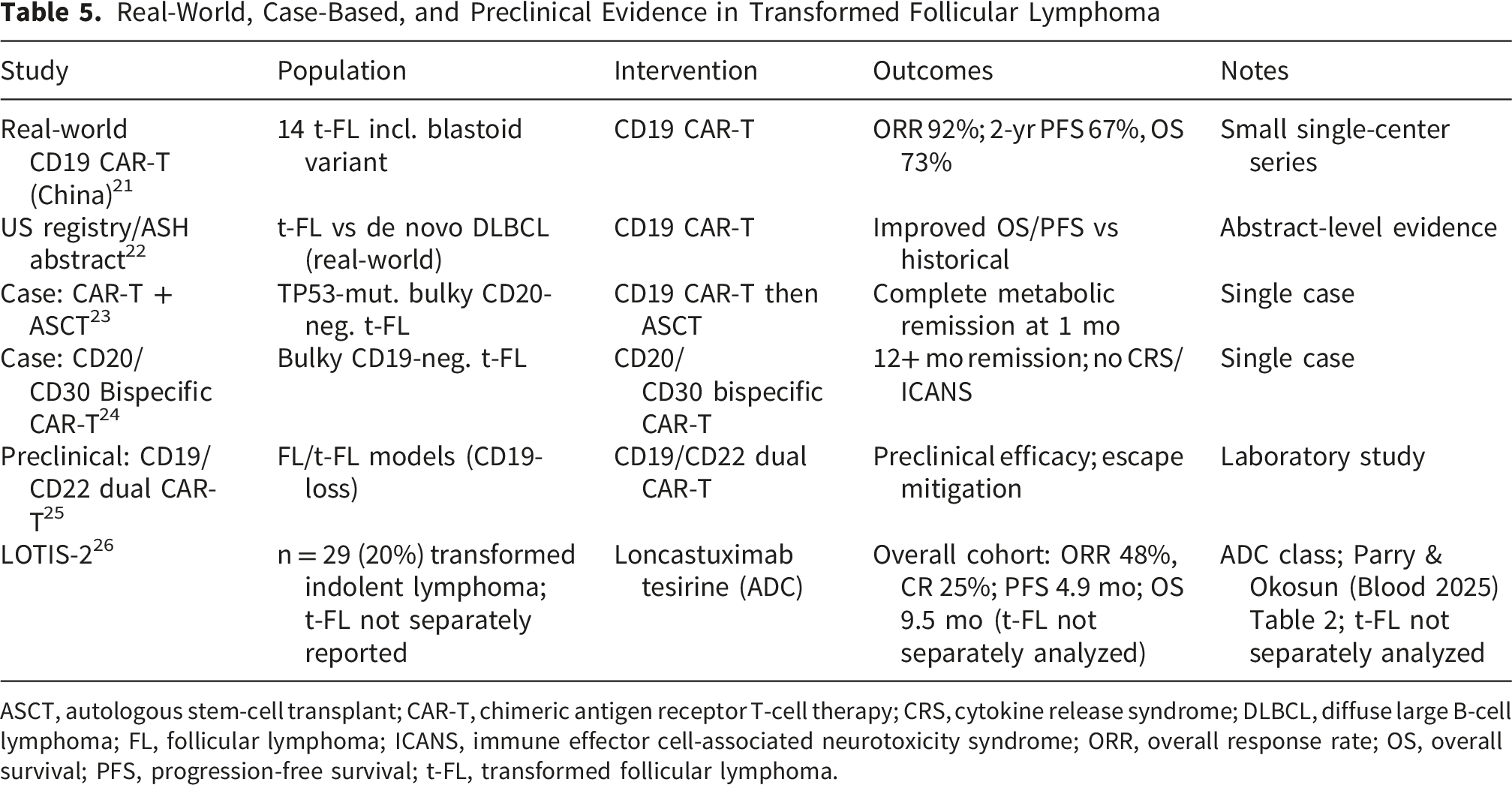
ASCT, autologous stem-cell transplant; CAR-T, chimeric antigen receptor T-cell therapy; CRS, cytokine release syndrome; DLBCL, diffuse large B-cell lymphoma; FL, follicular lymphoma; ICANS, immune effector cell-associated neurotoxicity syndrome; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; t-FL, transformed follicular lymphoma.
Practical Positioning of Available Therapies in Transformed Follicular Lymphoma
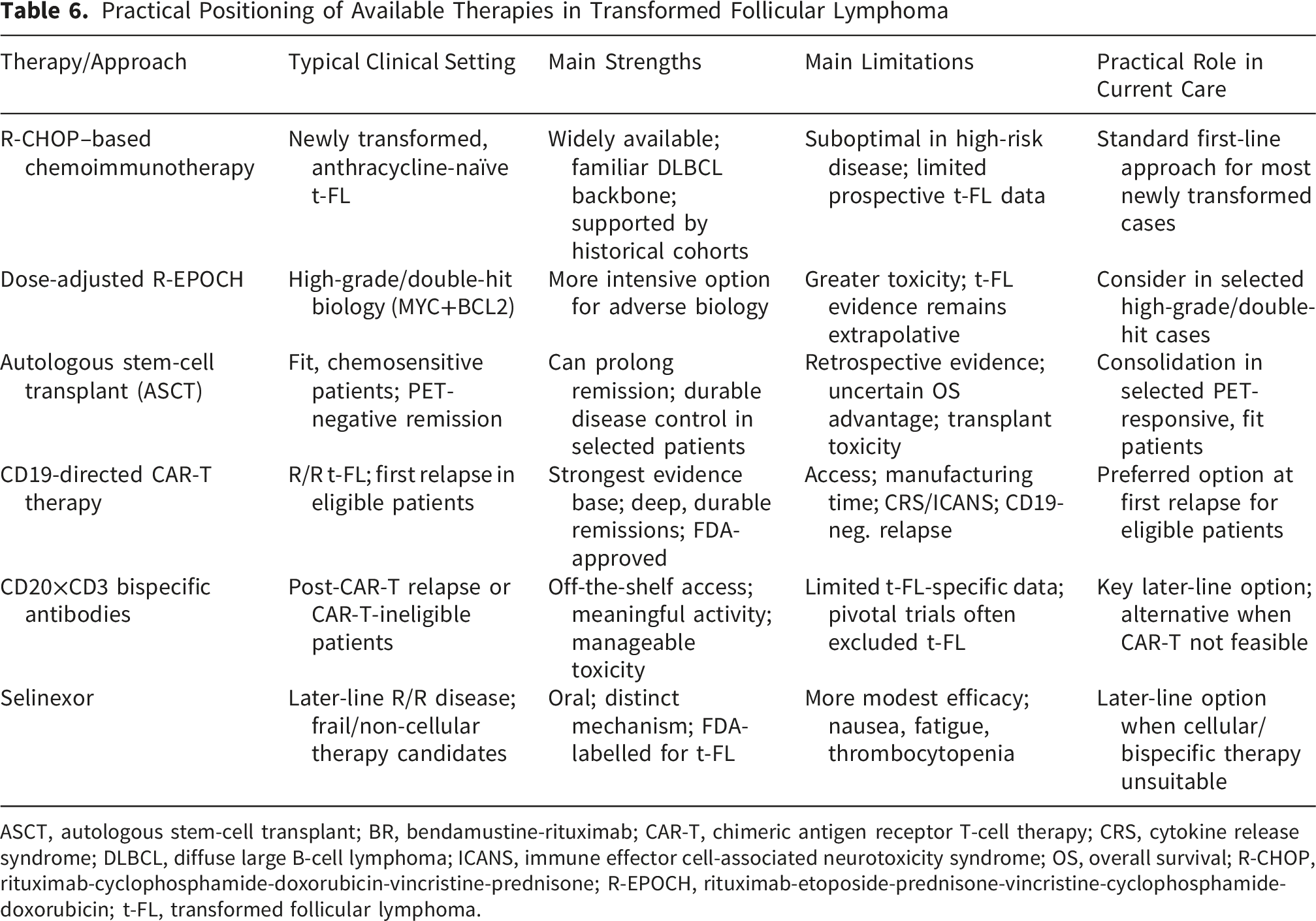
ASCT, autologous stem-cell transplant; BR, bendamustine-rituximab; CAR-T, chimeric antigen receptor T-cell therapy; CRS, cytokine release syndrome; DLBCL, diffuse large B-cell lymphoma; ICANS, immune effector cell-associated neurotoxicity syndrome; OS, overall survival; R-CHOP, rituximab-cyclophosphamide-doxorubicin-vincristine-prednisone; R-EPOCH, rituximab-etoposide-prednisone-vincristine-cyclophosphamide-doxorubicin; t-FL, transformed follicular lymphoma.

Evidence-informed management algorithm for transformed follicular lymphoma. ASCT, autologous stem-cell transplant; BR, bendamustine-rituximab; CAR-T, chimeric antigen receptor T-cell therapy; CR, complete response; ORR, overall response rate; POD24, progression of disease within 24 months
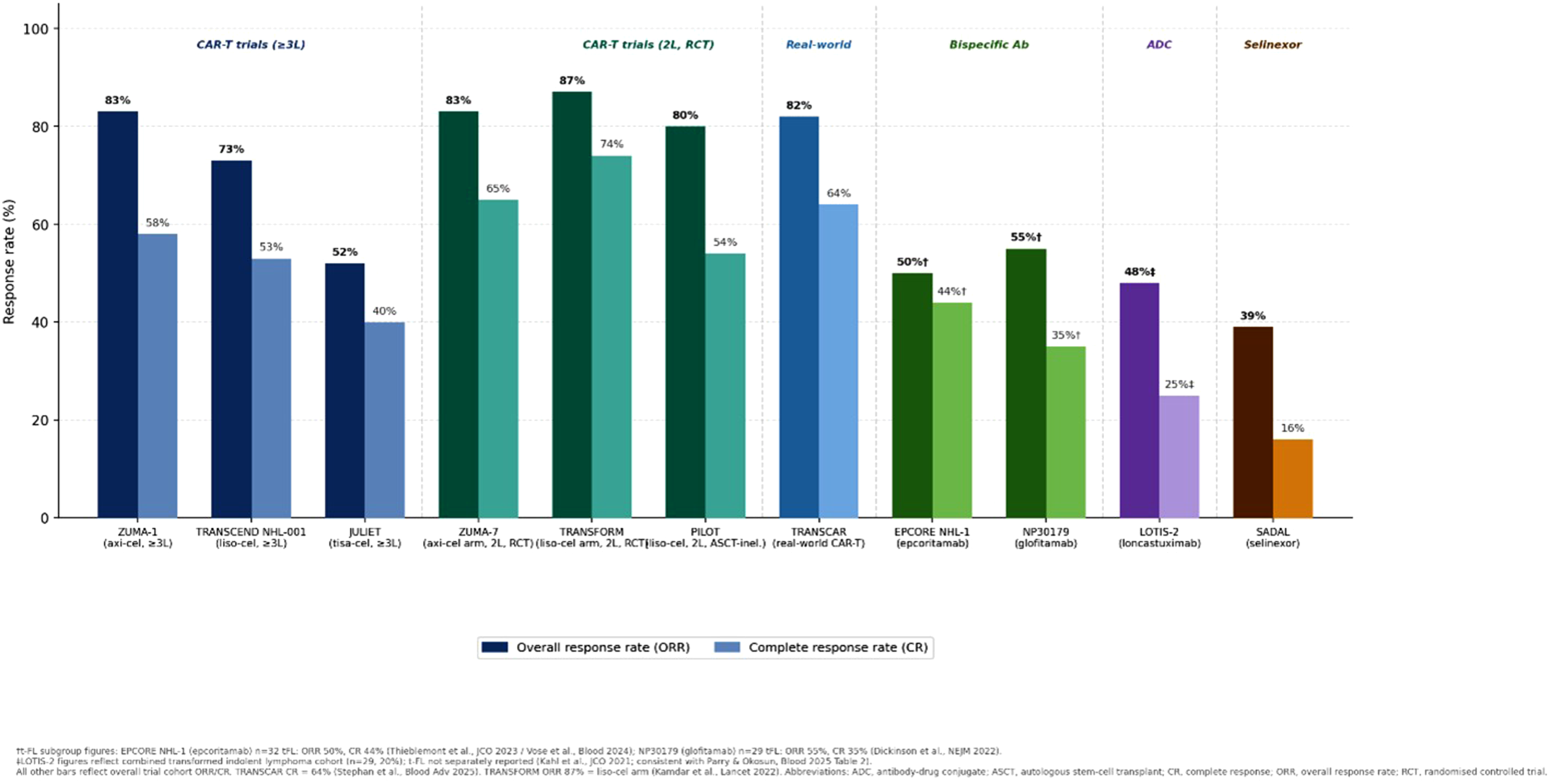
Overall response rate (ORR) and complete response (CR) rate across included studies in transformed follicular lymphoma, stratified by therapeutic class

Key safety signals across therapy classes in transformed follicular lymphoma. Rates are approximate estimates from pivotal trial safety tables and represent the overall trial population (t-FL subgroups were too small for separate safety reporting in most trials). CRS = cytokine release syndrome; ICANS = immune effector cell-associated neurotoxicity syndrome
Notably, five pivotal registration programs (ZUMA-5, ELARA, TRANSCEND FL, STARGLO, OLYMPIA-5) excluded transformed histology, despite broader approvals in DLBCL settings.18,27-29 This persistent exclusion underscores the need for dedicated, t-FL–specific prospective studies to refine treatment selection and sequencing.
CAR-T Therapy in t-FL
Seven interventional CAR-T trials with extractable t-FL subgroup data (total n = 130 t-FL patients across reported subsets; Parry and Okosun, Blood 2025) informed the CAR-T evidence base (Table 2). In TRANSCEND NHL-001, 60 patients with t-FL (22% of 270 treated) received lisocabtagene maraleucel and achieved ORR 73%/CR 53% with a median PFS of 6.8 months. 10 ZUMA-1 included a t-FL subset treated with axicabtagene ciloleucel (ORR 83%/CR 58%, with sustained CR rates). 9 JULIET (tisagenlecleucel) showed lower durability in t-FL relative to other products. 12 Among randomized second-line trials, ZUMA-7 (axi-cel) and TRANSFORM (liso-cel) demonstrated superiority over standard chemo-transplant strategies (CR 65% vs 32% and 74% vs 43%, respectively), whereas BELINDA (tisa-cel) did not.13-15 Real-world data corroborate meaningful activity. In the TRANSCAR registry, 60 patients with transformed indolent NHL treated with CAR-T achieved ORR 82% and CR 64%, with superior outcomes compared to de novo LBCL. 22 A complementary US multicenter analysis of 691 patients (139 t-FL, 20%) similarly demonstrated improved PFS and OS for t-FL versus de novo DLBCL following CAR-T therapy. 22
CD20×CD3 bispecific Antibodies
Two BsAb studies provided extractable t-FL outcomes (epcoritamab and glofitamab; n = 61 t-FL patients). A third study of mosunetuzumab enrolled 23 t-FL patients within an 88-patient DLBCL/t-FL cohort, but did not report t-FL outcomes separately, precluding efficacy extraction.26,30 BsAb activity in heavily pretreated disease (Table 3). In EPCORE NHL-1, 32 patients with t-FL achieved ORR 50%/CR 44%, with 55% responses ongoing at 36 months. 16 NP30179 (glofitamab) reported ORR 55.2%/CR 34.5% with median DOR of 5.5 months in 29 t-FL patients. 17 Cytokine release syndrome was predominantly low grade and manageable with step-up dosing and corticosteroid prophylaxis.
Selinexor
Selinexor remains the only non-cellular agent with FDA labeling that explicitly includes t-FL (Table 4). The pivotal SADAL phase 2b study enrolled 31 patients with t-FL (24% of 134) and reported ORR 38.7%/CR 16.1%, numerically higher than the de novo DLBCL subgroup (ORR 26.2%). 20 Among complete responders, the median DOR was 23.2 months, and median OS in the t-FL subgroup was 9.1 months. 31
Real-World, Case-Based, and Preclinical Evidence
Six additional reports provided supportive evidence, including real-world CAR-T cohorts, an antibody-drug conjugate study with a t-FL subgroup (LOTIS-2), single-patient experiences with bispecific or sequential CAR-T strategies, and a preclinical CD19/CD22 dual-targeting program addressing CD19-loss escape (Table 5).
Summary of Findings
Biology and Pathogenesis
Transformation of FL is associated with retained lineage but higher-grade biology. Most cases remain germinal-center B-cell type, with a smaller subset shifting to activated B-cell phenotype. MYC deregulation is a key event and, when combined with BCL2 rearrangement, defines double-hit biology associated with inferior outcomes.32,33 Cooperating lesions in cell-cycle regulation, DNA-damage response, immune escape, and survival signaling are common. ABC patterns frequently involve MYD88, CD79B, and BCL10, whereas GCB patterns more often show REL amplification and TP53/CDKN2A/B abnormalities.32,34-36 Multi-omic studies confirm clonal relatedness between t-FL and antecedent FL through shared t(14;18) breakpoints and aberrant somatic hypermutation patterns.32,37 Whole-genome analyses describe biologically distinct FL subtypes, including DLBCL-like FL with greater transformation risk, and microenvironmental remodeling marked by reduced T follicular helper cells and increased exhausted T-cell populations.38-46 Collectively, these data support PET-directed re-biopsy of the highest-SUV lesion and molecular evaluation at transformation, including MYC/BCL2/BCL6 testing. 47
Epidemiology and Clinical Presentation
Approximately 10–15% of patients with FL experience HT during the disease course, at an annual rate of 1–2% across multiple cohorts, though contemporary rituximab-era registries suggest a lower cumulative rate of 4–13% at 10 years.6,7,48 Two large cohorts illustrate this risk and the value of biopsy 49 : a prospective study of >600 newly diagnosed FL patients reported HT in 11% over a median of 5 years, with biopsy confirmation in 85% 6 ; in the PRIMA trial, 21% of 194 patients with biopsy-proven relapse showed transformation, and transformation was associated with markedly shorter time to recurrence (9.6 vs 22.8 months). 8 Established baseline risk factors include multiple extranodal sites, ECOG performance status >1, elevated LDH, B symptoms, advanced stage, low albumin, high FLIPI/IPI, failure to achieve CR after first-line therapy, and POD24. 4 Treatment exposure may also influence transformation risk, with population-based data suggesting higher t-FL rates after rituximab–bendamustine than after R-CVP. 42 Early transformation (<18 months) is associated with substantially worse 5-year survival than later events.6,50 Clinically, HT should be suspected with rapid nodal growth, focal SUV >10, unexpected extranodal involvement, early treatment failure, B symptoms, or hypercalcemia; biopsy remains the diagnostic gold standard despite documented underuse.42,51-53
Current and Emerging Treatment Strategies
Treatment of t-FL at transformation remains anchored in DLBCL-directed chemoimmunotherapy. R-CHOP is the standard for most anthracycline-naïve patients,7,8,48 whereas dose-adjusted R-EPOCH is reserved for high-grade biology with MYC and BCL2 rearrangements.54-56 Non-anthracycline rituximab-based regimens (BR or polatuzumab-based combinations) are options when anthracyclines are contraindicated. 57 ASCT remains a selective option in fit, chemosensitive responders, with the strongest signal for durable disease control in PET-negative remission58-61; randomized t-FL–specific evidence is lacking, and treatment-related morbidity must be balanced against potential benefit (Table 1).
Among emerging therapies, CD19-directed CAR-T currently has the strongest evidence base in relapsed/refractory t-FL (Table 2) and is the preferred option at first relapse for eligible patients. Confirmation of CD19 expression is essential, and CD19-negative relapse is an established mechanism of post-CAR-T resistance. 1110, 12 and 62 CD20×CD3 bispecific antibodies (Table 3) provide an off-the-shelf alternative after CAR-T failure or when CAR-T is not feasible because of age, comorbidity, logistics, or access.17,26,30,63 Their toxicity profile is generally manageable and is dominated by low-grade CRS.17,63 Selinexor (Table 4) remains a useful later-line option, particularly for frail or heavily pretreated patients, and is the principal targeted agent with regulatory inclusion of t-FL.20,31
Practical Positioning and Proposed Algorithm
The practical positioning of available modalities is summarized in Table 6, and an evidence-informed management algorithm is presented in Figure 2. In brief, transformation should be biopsy-confirmed whenever feasible (PET-CT-guided when possible)64,65; first-line treatment follows a DLBCL-like strategy tailored to disease biology and prior anthracycline exposure; ASCT is offered to fit, chemosensitive responders 61 ; CAR-T is prioritized at first relapse in eligible patients; and bispecific antibodies and selinexor are reserved for later lines or CAR-T-ineligible settings.
Limitations
This scoping review is descriptive by design and was intended to map the available evidence rather than generate pooled comparative estimates; accordingly, no formal risk-of-bias assessment or meta-analysis was performed, consistent with PRISMA-ScR guidance. Several limitations in the underlying literature should be acknowledged. First, many pivotal trials excluded transformed histology or reported only small t-FL subgroups, creating underrepresentation and potential selection bias. Second, definitions of transformation and diagnostic methods varied across studies, including biopsy-proven and clinically suspected cases.5,7 Third, heterogeneity in prior therapy, anthracycline exposure, timing of transformation, and biomarker characterization (e.g., double-hit status, TP53 alterations, cell of origin) limits external validity. Fourth, real-world datasets often lack centralized pathology review, standardized response assessment, and complete follow-up, with possible overlap between cohorts. Finally, several findings derived from subgroup analyses, post-hoc reports, or conference abstracts with immature follow-up, increasing the risk of selective reporting. Few studies directly address optimal sequencing, including CAR-T versus early bispecific use, or the management of CD19-negative relapse.
Conclusion
Although the evidence base for transformed follicular lymphoma remains limited, the current literature supports a coherent treatment framework. Biopsy confirmation should be pursued whenever feasible, and initial management should follow a DLBCL-like approach tailored to disease biology and patient fitness. ASCT remains an option for selected chemosensitive patients, while CAR-T is the preferred strategy at first relapse in eligible patients. Bispecific antibodies provide an important option after CAR-T failure or when cellular therapy is not feasible, and selinexor is best reserved for later-line or oral-therapy settings. Across these therapies, careful toxicity management and infection prophylaxis remain essential. Future progress will depend on prospective, t-FL–inclusive trials and biomarker-guided sequencing studies.
Supplemental Material
Supplemental Material - Beyond Chemoimmunotherapy: Emerging Cellular and Targeted Therapies in Transformed Follicular Lymphoma: A Scoping Review
Supplemental Material for Beyond Chemoimmunotherapy: Emerging Cellular and Targeted Therapies in Transformed Follicular Lymphoma: A Scoping Review by Abdulrahman F. Al-Mashdali, Rola Ghasoub, Shrouq Hwafdeh, and Mohamed A. Yassin in Cancer Control.
Footnotes
Acknowledgements
The authors acknowledge Qatar Foundation for covering the open-access publication fees upon acceptance. The authors used OpenAI solely for language polishing, graphical abstract/figures creation, and refinement during manuscript preparation; all content was subsequently reviewed and edited by the authors, who take full responsibility for the final manuscript.
Ethical Considerations
This study is a review of previously published literature and did not involve human participants, human tissue, or animal experiments conducted by the authors.
Consent to Participate
This study did not involve direct patient participation or the collection of identifiable individual data.
Author Contributions
Abdulrahman F. Al-Mashdali and Rola Ghasoub contributed equally to this work and share first authorship. A.F.A. and R.G. contributed to conceptualization, methodology, investigation, formal analysis, and drafting of the original manuscript. Shrouq Hwafdeh contributed to investigation and data curation. Mohamed A. Yassin contributed to resources, critical revision, and supervision. All authors reviewed, edited, and approved the final manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Open-access publication fees for this manuscript will be covered by Qatar Foundation upon acceptance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No new datasets were generated or analyzed in this study. All data supporting the findings of this review are available within the article and the cited references.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.