
Abstract
Introduction
The global status of core labor force (CLF) health is underestimated, particularly the burden of patients with early-onset gastrointestinal cancers (EOGICs), aged 15-49 years old. We aim to investigate the pattern and trend of EOGICs among CLF from 1990 to 2021.
Methods
EOGIC burden and its attributable risk factors were estimated using data from the GBD 2021. The ASR and EAPC by age, sex and SDI were utilized for measuring incidence rate trends. Joinpoint regression analysis was utilized to explore the variation in disease burden. The Bayesian Age-Period-Cohort (BAPC) model was performed to forecast the disease burden up to 2050.
Results
From 1990 to 2021, the global ASIR for EOGICs among core labor force remained broadly stable, moving from 10.9 to 9.62 per 100,000(EAPC=-0.42, -1.70 to 0.87), while incident cases increased from 295,514 to 379,709. The overall incidence pattern was driven largely by declines in early-onset GC. The age-standardized DALY rate declined from 375.16 to 238.40 per 100,000(EAPC=-1.46, -2.76 to -0.15). Only early-onset CRC showed increasing DALYs. Joinpoint analysis showed a continuous downward trend in the ASIR for overall EOGICs(AAPC=-0.97%; -0.81 to -1.08). Risk-factor decomposition indicated substantial contributions from modifiable exposures, mainly led by smoking, alcohol use, and dietary risks, with marked sex- and age-specific variation.
Conclusion
The results of the present study are significant for global health policy and practice in core labor force. Differentiated intervention and outreach strategies based on age and gender would be necessary to reduce the impact of EOGICs.
Introduction
Early-onset gastrointestinal cancers (EOGICs), typically defined as cancer diagnosed before age 50, 1 represents a growing clinical and public health challenge. The most common subtypes include early-onset colorectal cancer(EOCRC), early-onset gastric cancer(EOGC), and early-onset esophageal cancer(EOEC), which account for approximately a quarter of global incidence and about a third of cancer deaths, 2 underscoring the scale of the problem at the population level. Biologically, EOGIC is frequently characterized by more aggressive features, including higher prevalence of pathogenic germline variants, higher frequency of poorly differentiated tumors and a greater likelihood of metastasis compared to later-onset cancers,3,4 reinforcing the urgent need for enhanced awareness, specialized research, and tailored management strategies for this population. While advances in diagnostic technology contribute to increased detection rates, epidemiological studies5-8 confirm a genuine rise in the incidence of EOGICs that cannot be ascribed solely to detection bias, but correlate with changes in modifiable exposures, involving environmental and lifestyle factors as well as early-life risk accrual and birth-cohort effects. This trend translates into a significant societal burden,9,10 including heightened healthcare costs and productivity loss. On an individual level, patients with EOGIC face unique hardships, including severe financial toxicity 11 and psychological distress. 12
The labor force is generally defined as individuals aged 15 years and older by the International Labor Organization and is widely used in global labor statistics. 13,14 Here, we focused on the population aged 15-49 years old, representing the main working-age segment of society and largely overlaps with the population at risk for early-onset gastrointestinal cancers. We defined these individuals as the core labor force (CLF). In the context of rapid aging of population and rising old-age dependency ratios, the CLF bears a disproportionate share of production, tax contributions and caregiving to support more non-working dependents. 15 As the primary working-age population, the CLF plays a pivotal role in demographic and health-related policymaking, particularly in areas such as reproductive health, occupational exposure, and chronic disease risk. 16 Given that EOGICs carry a high share of disability-adjusted life years (DALYs) and often arise during peak earning and family-building years, 17 their productivity impact is especially pronounced for the CLF. Thus, mapping temporal trends and their distribution across the CLF is essential to directing etiological research and evidence-based policy.
EOGICs have shown a continuous increase in incidence globally, highlighting the need to understand their epidemiology. The CLF represents a high-risk group for EOGICs due to their age profile and potential occupational or lifestyle exposures. However, research on incidence, trends, and disease burden in this population is limited. Previous studies have primarily focused on general population trends, traditional risk factors, or single cancer types, leaving a gap in understanding disease burden among high-risk working-age populations. This study leveraged the 2021 Global Burden of Disease (GBD) dataset to estimate the number of cases, the crude incidence rate and the age-standardized incidence rate (ASIR) values for three EOGIC types from 1990 to 2021, covering variations in age, gender, SDI levels and geographical factors. Additionally, the Bayesian age-period-cohort (BAPC) model is used to forecast potential public health challenges related to EOGICs by 2050. The insights from this research offer critical epidemiological data to guide early cancer screening and prevention. These findings provide important evidence to shape effective, region-specific policies aimed at alleviating the global burden of EOGICs.
Methods
Data Sources and Definition
The GBD 2021 study incorporated data from 204 countries and regions pertaining to 371 forms of disease and injury, as well as 88 risk factors, 18 reporting on incidence, age-standardized rates(ASR), disability-adjusted life years(DALYs) of EOGICs (https://ghdx.healthdata.org/gbd-2021/sources). These data have been rigorously cleaned, transformed and modelled by researchers throughout the globe to generate appropriate estimates. Estimates and corresponding 95% uncertainty intervals (UIs) were reported for the number of cases, crude incidence rate and ASIR values for these three GI cancer types in the CLF based on GBD 2021 data, reporting all rates per 100 000 people. Incidence and DALYs rates are presented as estimates per 100,000 population, while case counts represent the absolute burden of EOGICs among CLF.
In this study, CLF are defined as adolescents and young adults aged 15–49 years. Gastrointestinal cancers were systematically categorized using International Classification of Diseases (ICD) topography codes: ICD-9 and ICD-10 (Table S1). We quantified the burden of EOGICs (esophageal, gastric, colorectal cancer) in individuals aged 15–49 years between 1990 and 2021, examined the role of associated risk factors, and predicted trends from 2022 to 2050. The 15–49 age group is subdivided into seven age groups at five-year intervals. Given the use of publicly available, anonymized aggregate data, no ethical approval or informed consent was required.
The Sociodemographic Index (SDI) is a composite of the geometric mean of average years of education, lag-distributed per capita income and fertility rates among women under 25 years for a given location, rescaling these SDI scores from 0 to 100.The 2021 SDI values were used to separate countries into quintiles (Table S2). The SDI ranges from 0 to 1, with countries and regions classified into five levels of development: low (0 < SDI
Temporal Trend Analyses
Joinpoint regression analysis on ASIRs was employed to assess global trends in GI cancer burden among the CLF. To stabilize variance and interpret changes on a relative scale, we fitted log-linear segmented regressions of ASIR on calendar year. We selected the number and locations of joinpoint using a Monte Carlo permutation test20,21 (4,499 permutations) and family-wise error was controlled at α=0.05 using Bonferroni adjustment. For each retained segment, the annual percent change (APC) and 95% confidence interval (CI) were obtained from the segment slope on the log scale and back-transformed. We summarized the overall period with the average annual percent change (AAPC), 22 computed as the length-weighted average of segment-specific APCs; its 95% UI was obtained by propagating the segment-level uncertainty. When both the APC/AAPC estimates and the lower boundary of the 95% CI were above 0, an increasing trend was considered to be present during a specific period. Conversely, if the estimates and the upper boundary of the 95% CI were both below 0, a decreasing trend was considered to be present. Otherwise, the trend was considered to be stable.
Risk Factor Analysis
Risk factors were identified based on established risk–outcome relationships defined by the World Cancer Research Fund and the Comparative Risk Assessment framework. 23 Within the Global Burden of Disease Study, exposure distributions were estimated using hierarchical modeling approaches, stratified by age, sex, year, and location. For each validated risk-outcome pair, population attributable fractions (PAFs) were calculated by integrating exposure distributions with pooled relative risks derived from meta-analyses. These PAFs were subsequently applied to overall disease burden estimates to quantify attributable DALYs. DALY rates attributable to individual risk factors were further estimated at the most detailed level of classification.
Disease Burden Estimates
From 2022 to 2050, Bayesian Age-Period-Cohort (BAPC) 24 models were used with R software (BAPC 0.0.36 and INLA 24.05.10) to predict ASIR. The BAPC model tests the combined effects of age, period, and cohort. Second-order random walk priors were employed to smooth estimated effects and project posterior mortality rates. Integrated Nested Laplace Approximation (INLA) was utilized to approximate marginal posterior distributions, circumventing the mixing and convergence issues inherent in traditional Markov chain Monte Carlo sampling techniques for Bayesian inference.
Statistical Analysis
Age-standardized rates (ASRs) per 100,000 population were calculated for the core labor force (CLF) aged 15–49 years using standard formulas 25 and adjusting to GBD standard population. The estimated annual percentage change (EAPC) was calculated to assess temporal trends in ASRs. An ASR was considered increasing or decreasing if both the EAPC and its 95% confidence interval (CI) were above or below zero, respectively. If the 95% CI included zero, the change was considered statistically insignificant. In accordance with the GBD framework, uncertainty intervals (UIs) were derived from 1,000 posterior draws, with the lower and upper bounds defined by the 2.5th and 97.5th percentiles. Statistical significance was set at P < 0.05. All analyses and visualizations were performed using R software (version 4.2.2).
Role of the Funding Source
The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. All authors had full access to all the data in the study and accepted responsibility to submit for publication. The reporting of this study conforms to the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) statement. 26
Research in Context
Evidence Before This Study
Early-onset gastrointestinal cancer (EOGIC, including esophageal, gastric, and colorectal cancer) among the core labor force (CLF, ages 15-49) have not been systematically quantified with age- and gender-specific resolution. In order to gather existing evidence, we systematically searched several databases such as PubMed, Web of Science up to October 2025 with key words: “colorectal cancer”, “gastric cancer”, “esophageal cancer”, “core labor force”, “early-onset”, “global burden”. Prior works reported rising incidence in younger adults and wide regional disparities, but lacked a coherent global picture by cancer type, age, and gender, and rarely decomposed burdens by modifiable risks or projected future trends. This study aims to address these gaps by estimating the global burden and risk-factor contributions of early-onset GI cancers in the CLF, stratified by age and gender.
Added Value of This Study
Using GBD 2021 across 204 regions, we provide the integrated, age- and sex-resolved assessment of EOGIC burden in the CLF, with risk-factor decomposition and Bayesian age-period-cohort projections. Particularly noteworthy, the global trajectory reveals burden hotspots, clear age–sex gradients, distinct temporal dynamics, substantial contributions from modifiable risks, and forward projections. Our comprehensive analysis of descriptive, trend and health inequality aspects of EOGICs among the CLF enhance understanding of their epidemiology and provides a solid foundation for global public health policy and medical resource allocation.
Implications of all the Available Evidence
Among the CLF, the absolute burden of EOGIC is rising despite declining age-standardized rates. And EOCRC is projected to comprise most new cases. Given the substantial heterogeneity in disease burden and the non-linear, cancer-specific SDI–burden, prevention strategies should integrate both primary prevention and secondary prevention measures. These include earlier screening initiation, shortened screening intervals, and health-system strengthening to narrow disparities in outcomes. Policies should be context-specific, tailored to regional development levels, local epidemiological patterns, and healthcare capacity, with screening thresholds and intervals calibrated accordingly. Furthermore, enhanced cancer registration and standardized surveillance systems are essential to inform adaptive policy adjustments and enable robust international comparisons of disease trends and control performance.
Results
Global Disparities in the Burden of EOGICs
Age-Standardized Incidence and DALYs of Early-Onset Gastrointestinal Cancer Among Core Labor Force in 1990 and 2021, and Their Estimated Annual Percentage Changes From 1990 to 2021, Globally and by 21 GBD Regions
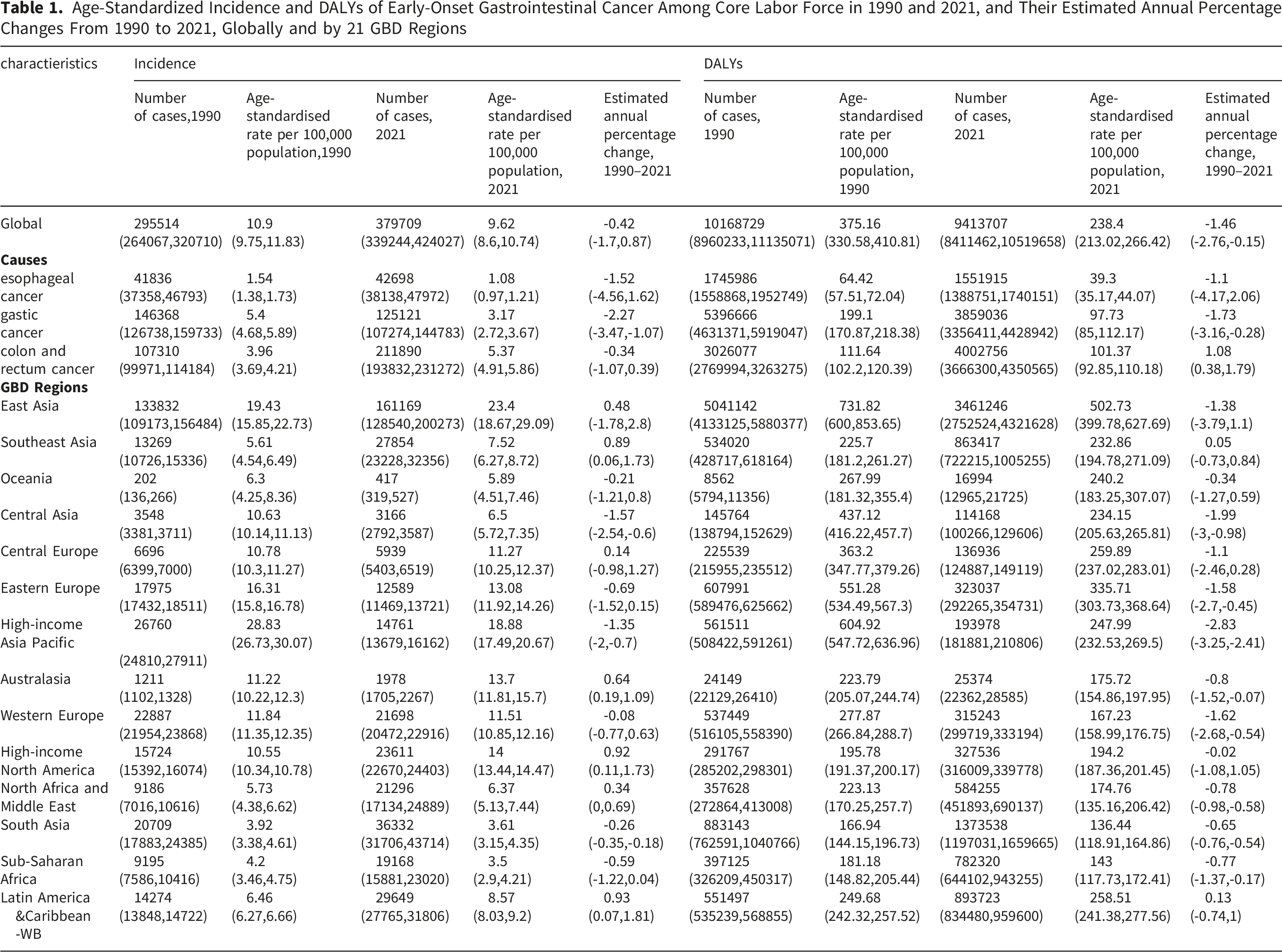
In 2021, EOCRC constituted both the highest proportion of all incident cases (55.80%) and DALYs (42.52%) globally among the three EOGICs, followed by gastric cancer (32.95% and 40.99%) and esophageal cancer (11.24% and 16.49%) (Fig. 1A, Fig. S1, and Table S3). Notably, EOCRC (55.8%) surpassed SC (49.53%) as the leading contributor of absolute number of early-onset cases in 2021 while EOCRC still maintain the first proportion of the DALYs (Table S3). Global and regional burden of early-onset gastrointestinal cancers in 2021 and trends from 1990 to 2021. Proportions of incident cases (A) and DALYs (B) attributable to each EOGIC subtype across the 14 GBD regions in 2021. Age-standardized incidence rate (C) and age-standardized DALY rate (D) in 2021, globally and by the 14 GBD regions. Estimated annual percentage change in ASIR (E) and ASDR (F) from 1990 to 2021, globally and by the 4 GBD regions. ASIR, age-standardized incidence rate; DALYs, disability-adjusted life-years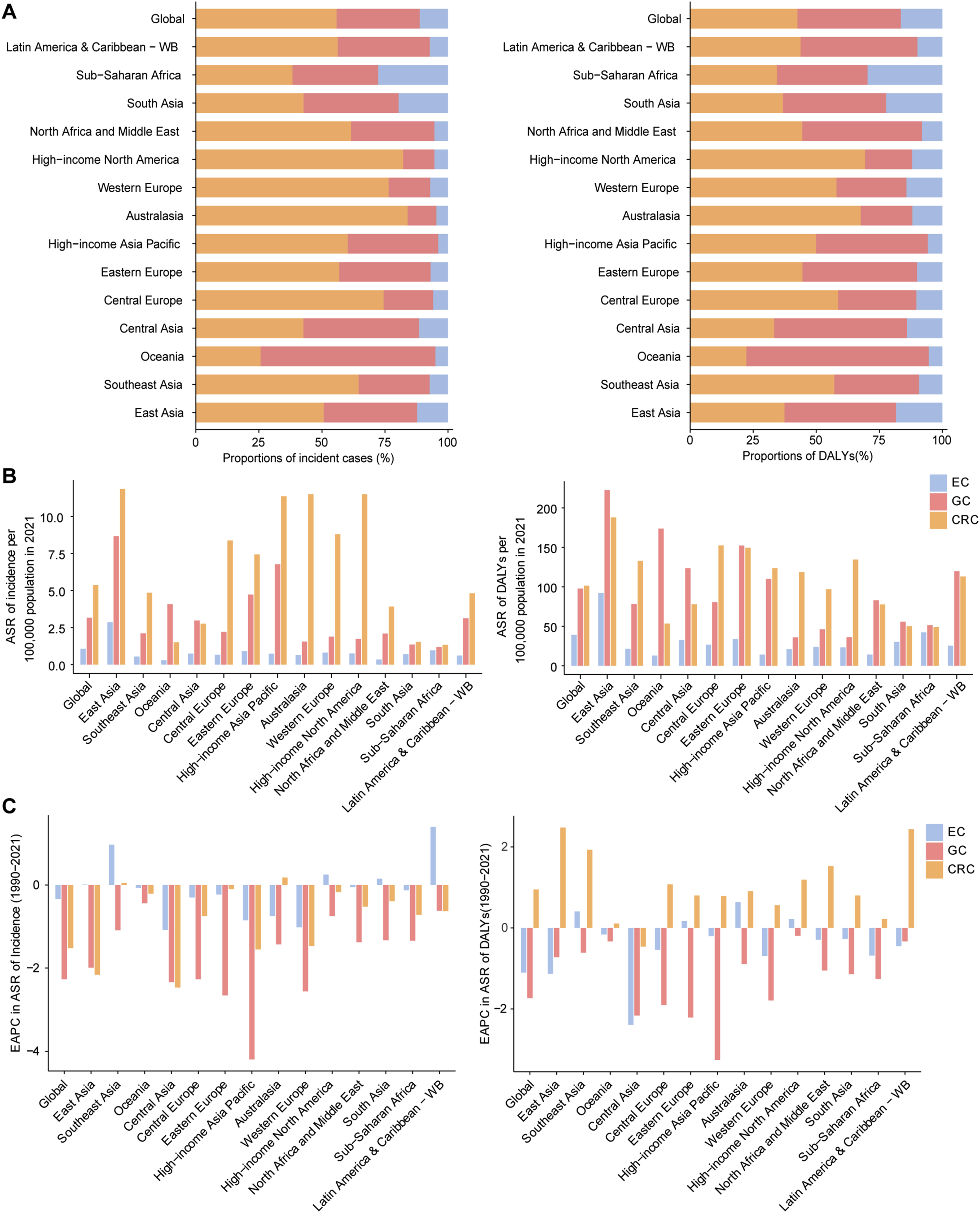
Regional and National Variations in the Burden of Three EOGICs
In 2021, marked geographical heterogeneity was observed in the ASIR of EOGICs across the 14 GBD regions and 204 countries. The highest incidence of EOGIC was reported in East Asia, South Asia, and Latin America & Caribbean – WB (Fig. 1B). In contrast, the highest DALY burdens were concentrated in East Asia, Eastern Europe, and Central Europe. This substantial disease burden in East Asia was also reflected in the highest ASIR (per 100,000 population) across all three EOGICs, including colorectal cancer (11.86), gastric cancer (8.67), and esophageal cancer (2.87). Likewise, the highest age-standardized DALY rates (per 100,000 population) of EOGICs were also all reported in East Asia: colorectal cancer (187.93), gastric cancer (222.6) and esophageal cancer (92.2), respectively (Table 1). Despite global downward trend, nearly half of the GBD regions (such as Latin America and Caribbean - WB, high-income North America) demonstrated a growing trend in incidence and DALYs for EOGICs. The ASIR declined significantly in Central Asia (-1.57, 95% UI: -2.54 to -0.60) and High-income Asia Pacific (-1.35, 95% UI: -2.00 to -0.70) from 1990 to 2021. High-income Asia Pacific also showed the fastest decline in DALYs (-2.83, 95%UI: -3.25 to -2.41), followed by Central Asia (-1.99, 95% UI: -3.00 to -0.98 (Fig. 1C, Table 1).
On cross-national level, Monaco (23.56 per 100,000) recorded the highest age-standardized incidence rate in 2021, whereas Gambia (1.24 per 100,000) reported the lowest. For DALYs, Mongolia (278.8 per 100,000) exhibited the highest age-standardized DALY rate, followed by Democratic People’s Republic of Korea (563.26), and Palau (530.33), reflecting pronounced burden in high-SDI countries with small population size (Tables S8-S10). In terms of temporal trends, the most pronounced increases in incidence rates were observed in Kuwait (EAPC = 3.26, 95% CI:2.81 to 3.72), Thailand (EAPC = 3.03, 95% CI:1.19 to 4.9), and Saudi Arabia (EAPC = 2.77, 95% CI:2.33 to 3.21). For DALYs, the highest upward trends occurred in the Zimbabwe (EAPC = 2.53, 95% CI:2.06 to 2.99), Lesotho (EAPC = 2.16, 95% CI:0.41 to 3.93) (Tables S8-S10). It is noteworthy that the majority of countries exhibited negative EAPCs for DALYs, reflecting an overall global decline in EOGIC-related disease burden over the past three decades (Fig. 2A, Table S4). Specifically, the highest ASIR in 2021(per 100,000) of EOEC, EOGC, EOCRC are reported in Malawi (3.52), Palau (9.95), France (9.66) (Tables S4-S7). The highest ASR of DALYs (per 100,000) were reported in Malawi (154.71), Mongolia (382.52), Thailand (235.78), suggesting that high incidence did not always correlate with the highest DALY burden (Fig 2B–D, Tables S4-S7). National ASIR for EOGIC subtypes among the CLF in 2021. A global map of the 2021 ASIR for overall early-onset gastrointestinal cancer(A), early-onset esophageal cancer(B), early-onset gastric cancer(C), early-onset colorectal cancer(D) among the CLF. EOGICs, early-onset gastrointestinal cancers; ASIR, age-standardized incidence rate; CLF, core labor force
SDI-Associated Patterns in the Global Burden of EOGICs
The Socio-demographic Index (SDI), which combines information on the economy, education, and fertility rate, serves as a proxy for the level of social and economic development and the availability of healthcare across different countries. From 1990 to 2021, distinct disparities in the burden of EOGICs across SDI quintiles were observed. Overall, the age-standardized DALY rates (ASDRs) for EOGICs showed a declining trend with increasing SDI, particularly in high and high-middle SDI regions (Fig 3A-C). In contrast, low- and middle-SDI regions exhibited either slower declines or increasing trends, especially for EOCRC(Fig. 3A). Age standardized disability adjusted life year (DALY) rates of early-onset colorectal cancer(A), gastric cancer(B), esophageal cancer(C) for the 14 GBD regions by sociodemographic index, 1990–2021. 32 points are plotted for each region and show the observed age standardized DALY rates from 1990 to 2021 for that region. Expected values, based on sociodemographic index and disease rates in all locations, are shown as a solid line. Regions above the solid line represent burden higher than expected and regions below the line show burden lower than expected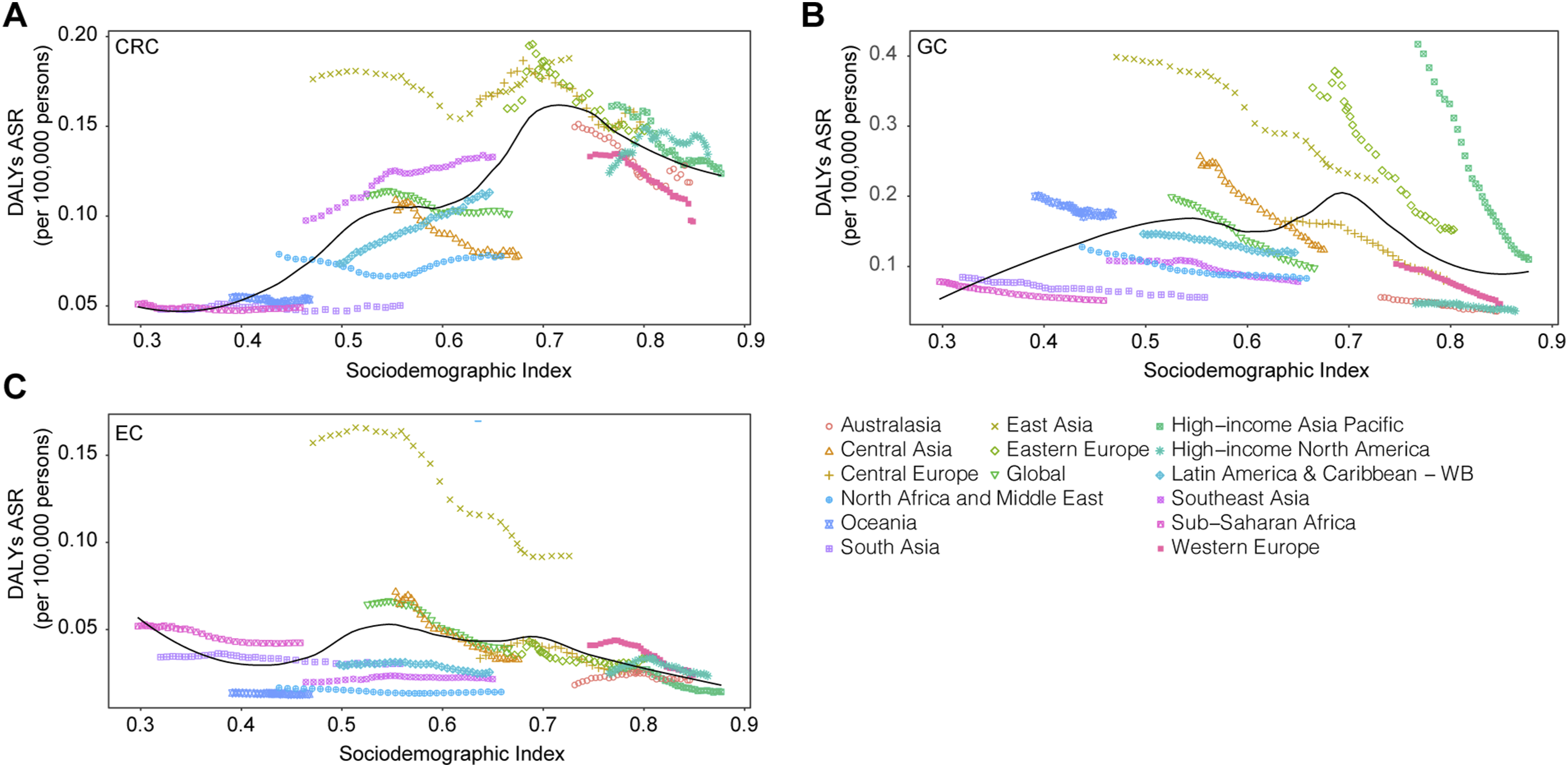
EOGC and EOEC displayed similar trends across the SDI spectrum. In terms of EOEC, regions with SDI levels between 0.6 and 0.75 exhibit a sharp peak in EOEC-related DALY burden, with East Asia standing out as a prominent high-risk region, showing markedly higher ASDRs (exceeding 0.15 per 100,000 population) compared to all other regions. This was largely explained by high ASDRs in China and the Democratic People’s Republic of Korea, pointing to extra risk to explain the extraordinary burden. For EOGC, ASDRs increases steadily with SDI, peaking around an SDI of 0.7, followed by a gradual decline in higher-SDI regions. The EOGC curve of High-income Asia Pacific and Eastern Europe is sheer, demonstrating steep declines in higher-SDI setting, reflecting the impact of established screening strategies and healthcare access (Fig. 3B).
Regarding EOCRC, the ASDR peaked at an SDI of approximately 0.7, with the highest values reaching 0.15 per 100,000 population in high-middle-SDI regions, more than three times greater than that in low-SDI regions. This sustained elevation contrasts sharply with a subsequent decline in high-SDI regions, suggesting a complex, non-linear relationship between development and disease burden in EOCRC (Fig. 3A).
Taken together, these patterns indicate that while improvements in socio-economic development and healthcare systems are generally associated with reduced burden of EOGICs, the relationship is complex and cancer-specific, necessitating tailored regional prevention strategies.
Age and Gender-Based Temporal Trends in EOGIC Incidence
Joinpoint regression of EOGICs were next conducted (Figure 4). From 1990 to 2021, a continuous downward trend in the ASIR for overall EOGIC was noted (AAPC=-0.97%; 95% CI -0.81 to -1.08) (Table S11). The ASIR for overall EOGIC in the 40-49 years age group consistently remained above the global average throughout the study period, whereas age groups below 40 years exhibited below. Specifically, for EOCRC and EOGC, the 35-49 years cohorts consistently showed higher-than-average ASIRs, underscoring a disproportionate burden in older early-onset populations (Tables S13-S14). For EOEC, the ASIR curve for the 35-39 years group intersected with that of the total population around 1993, after which the total ASIR surpassed it slightly but remained closely aligned (Table S12). Among all EOGICs, the 45–49 years group showed the most fluctuations, with multiple inflection points possibly reflecting shifts in risk exposure or diagnostic practices (Fig. 4A). Joinpoint regression analyses of the ASIR for overall and EOGIC three subtypes in the CLF by age group from 1990 to 2021. (A) Overall EOGIC, (B) early-onset colorectal cancer, (C) early-onset gastric cancer, and (D)early-onset esophageal cancer. EOGICs, early-onset gastrointestinal cancers; ASIR, age-standardized incidence rate; CLF, core labor force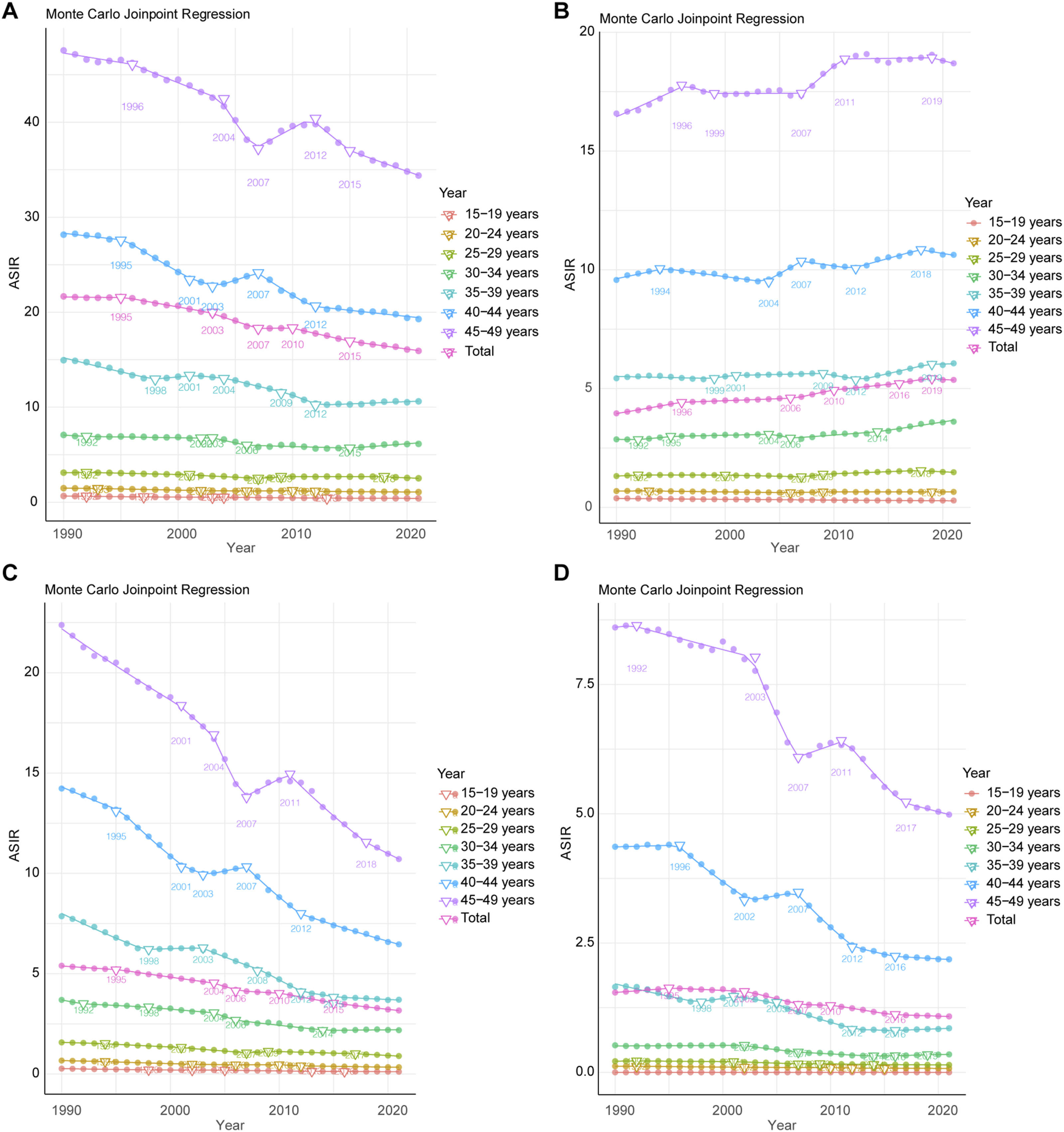
EOCRC was the only subtype exhibiting a continuous and statistically increase in ASIR from 1990 to 2021 (AAPC = 0.94%; 95% CI: 0.94 to 0.95). A particularly sharp rise was observed between 2006 and 2008 (APC = 2.13%; 95% CI: 1.83 to 2.43). From 2018 to 2021, incidence declined significantly (APC = -0.52%; 95% CI: -0.81 to -0.23), indicating a potential turning point in EOCRC incidence in the most recent years. From 1990 to 2021, the EOCRC burden showed a sustained increase in individuals aged 45-49 (AAPC = 0.38%) and 40-44 (AAPC = 0.29%), with notable spikes during 2007-2009 (APC = 2.22%) and 2003-2006 (APC = 2.62%), respectively. Both age groups experienced a recent decline from 2019 (APC = -0.63% and -0.71%, respectively), though not statistically significant. These patterns suggest that elder early-onset age groups primarily drive the rising EOCRC burden (Fig. 4B).
EOGC showed a significant downward trend in ASIR across the entire period (AAPC = -1.70%), with multiple phases of accelerated reduction. Both 40-44 and 45-49 age groups showed transient rebounds, suggesting non-linear incidence dynamics. For individuals aged 45-49, the overall ASIR decreased significantly (AAPC= -2.30%), with a particularly sharp drop of -6.98% observed from 2003 to 2005, followed by a brief but notable rebound (+1.97%, 2006-2009). In the 40-44 group, the decline was even steeper (AAPC = -2.51%), featuring rapid drops interrupted by modest short-term increases (+1.11%, 2003-2005) (Fig. 4C).
EOEC also experienced a substantial and consistent decline in ASIR (AAPC = -1.12%), with the most marked decrease occurring between 1994 and 2006. Most strikingly, between 2002 and 2005, there was a sharp and statistically significant drop in incidence with an APC of −6.37% (95% CI: −7.17 to −5.55%), marking the steepest decline observed among all age groups and periods (Fig. 4D).
Age and Gender-specific Disparities
Global Incidence and DALYs Rate of Early-Onset Gastrointestinal Cancer Among Core Labor Force in 2021
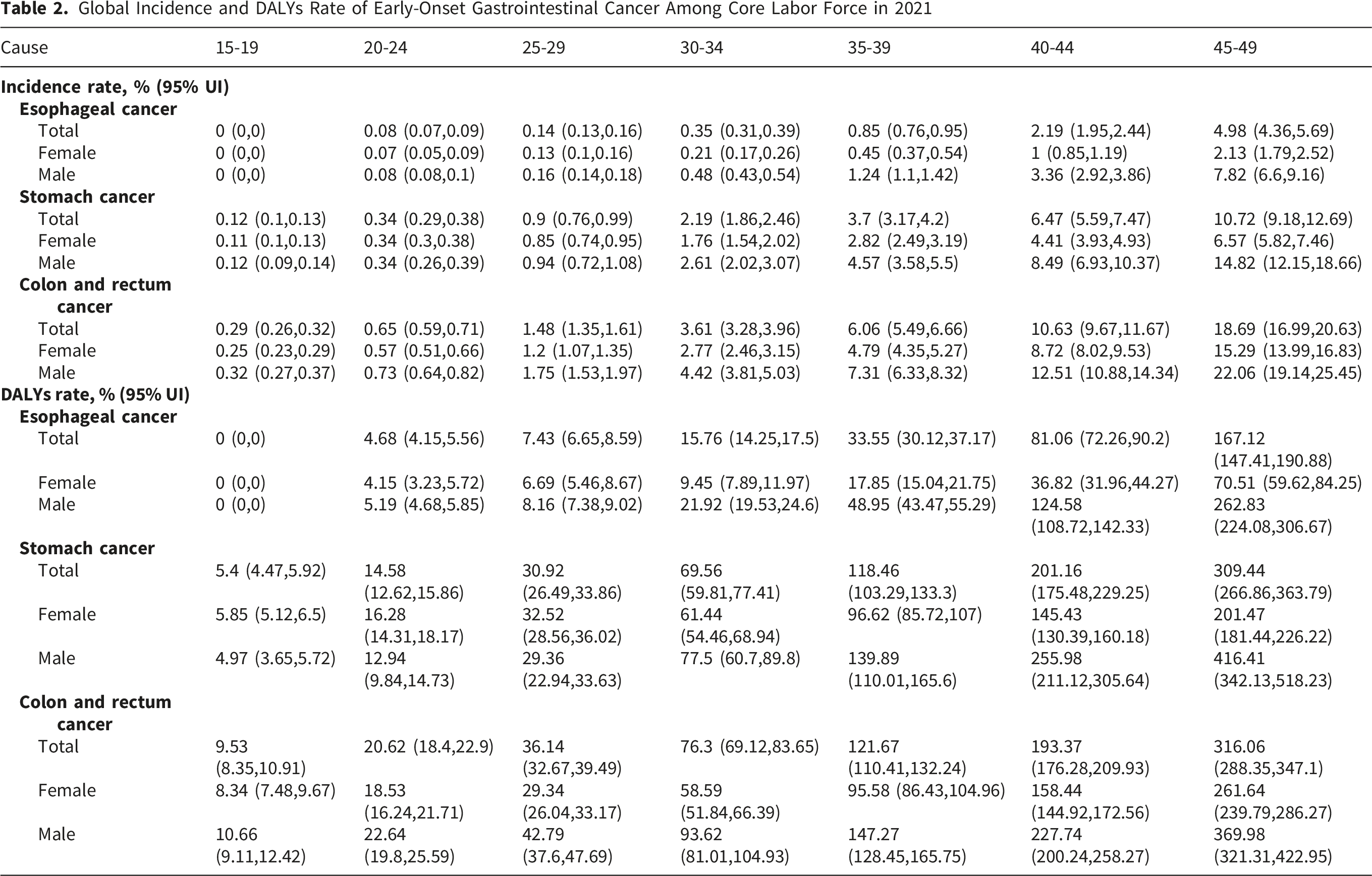
Among the early-onset population, the age-specific absolute numbers of both incidence and DALYs for esophageal, gastric, and colorectal cancers rose steadily with age, peaking in the 45–49-year-old group. In this age bracket, the incidence rates were highest for colorectal cancer (18.69%), followed by gastric cancer (10.72%) and esophageal cancer (4.98%) (Figure 5). Notably, within the 40–44-year age group, the DALY rate for EOGC (201.16 per 100,000) exceeded that of colorectal cancer (193.37 per 100,000), highlighting a disproportionate functional or mortality impact despite a lower incidence (Table 2). Cross-sectional patterns and risk-factor trends for EOGICs within the CLF by age group in 2021. ASIR and DALY rate of EOCRC(A), EOEC(B), and EOGC(C), by gender: female(red), and male(blue). Trends of percentage contribution of risk factors to the DALYs of EOCRC(D), EOEC(E), and EOGC(F) from 1990 to 2021. ASIR, age-standardized incidence rate; DALYs disability-adjusted life years; EOCRC, early-onset colorectal cancer; EOGC, early-onset gastric cancer; EOEC, early-onset esophageal cancer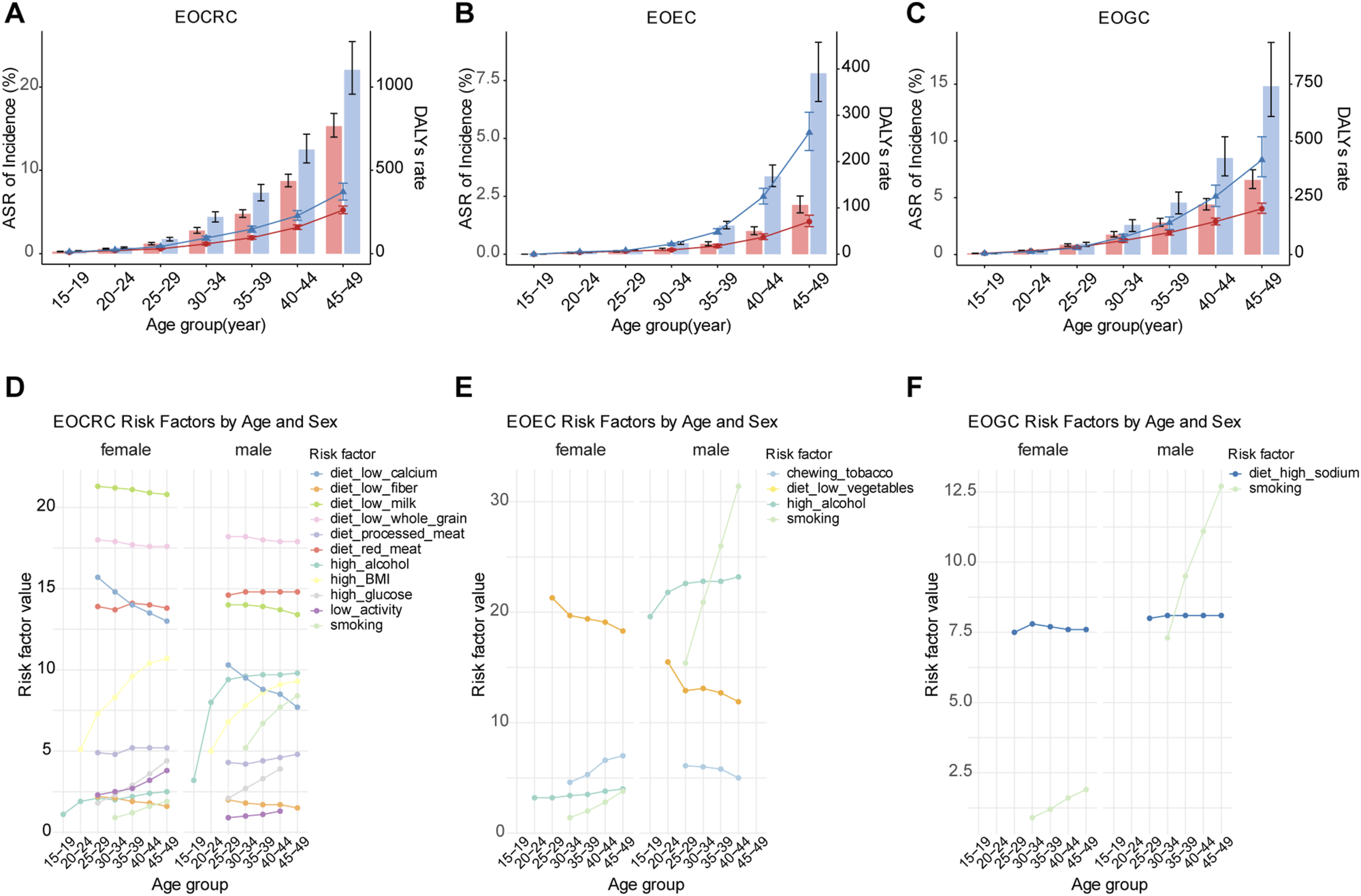
Moreover, sex disparities were consistently pronounced. Males consistently showed higher incidence and DALY rates than females, with the male-to-female DALY burden gap widening with age, especially in esophageal and gastric cancers (Fig 5B–C). For instance, for EOGC, male DALYs reached 416.41 per 100,000, almost double that of females (201.47) (Fig. 5C). Similarly, in the 45-49-year-old group, the incidence rate of EOEC in males (7.82%) was nearly four times of that in females (2.13%), and the DALYs rate was nearly four-fold higher in males (262.83 per 100,000) compared to females (70.51 per 100,000) (Fig. 5B). These findings underscore not only an age-dependent rise in EOGIC burden but also a sharp divergence in sex-specific disease impact, especially in EOEC and EOGC. Overall, the burden of EOGICs is progressively shifting toward younger age groups and disproportionately affects young males.
Age and Gender-specific Risk Factors
According to Global Burden of Disease (GBD) estimates, multiple modifiable risk factors contribute substantially to the burden of EOGICs, with notable variations across sex and age groups. We found that smoking, alcohol consumption, and dietary deficiencies were identified as major contributors to the rising EOGICs burden, with distinct sex- and age-specific patterns. The disease burden attributable to smoking in males is estimated to be approximately four times higher than in females, highlighting a pronounced sex disparity in smoking-related EOGIC risk (Fig 5D-F). EOCRC incidence shows a sharp rise after age 20, while its relative rarity before adulthood may be partially linked to underage alcohol restrictions, suggesting long-term protective effects of early alcohol control policies. In addition, insufficient calcium and milk consumption has been linked to increased EOCRC risk in females, underscoring the protective role of adequate dietary calcium intake (Fig. 5D). EOEC is strongly associated with alcohol intake, with the attributable risk increasing exponentially with age. Dietary risks also contribute significantly, particularly among females. Low vegetable intake is strongly associated with EOEC in women, especially within the 25 to 29-year age group (Fig. 5E). For EOGC, High sodium intake was identified as a consistently significant risk factor across all age groups and both sexes, with similar risk magnitudes observed between males and females (Fig. 5F). These findings highlight the importance of targeted, population-specific interventions to mitigate risk and reduce disease burden.
Future Burden of EOGICs
BAPC-based projections indicate markedly divergent trajectories among the three EOGICs between 1990 and 2050, with notable sex-specific differences (Figure 6). Specifically, the incidence of EOCRC is projected to rise steeply across both sexes, with male incidence rates increasing most dramatically among all groups. By 2050, EOCRC is expected to account for the majority of new EOGIC cases in both men (59.68%) and women (67.35%), suggesting a rapidly intensifying burden that spans the early-adult to midlife population (Fig 6A-B). In contrast, EOEC is projected to increase modestly in males while remaining relatively stable in females, reflecting the most pronounced sex disparity among the three cancers (Fig 6C-D). EOGC shows the mildest growth trajectory, with rates plateauing among females and rising only slightly among males before leveling off after 2030 (Fig 6E-F). Forecasts of ASIR of early-onset gastrointestinal cancer by subtypes, stratified by sex, over the next 30 years using the BAPC model. EOCRC (A, female; B, male), EOEC (C, female; D, male), EOGC (E, female; F, male). Predicted ASIR values for each year are provided in Supplementary Table 2. ASIR, age-standardized incidence rate; BAPC, Bayesian age-period-cohort; EOCRC, early-onset colorectal cancer; EOEC, early-onset esophageal cancer; EOGC, early-onset gastric cancer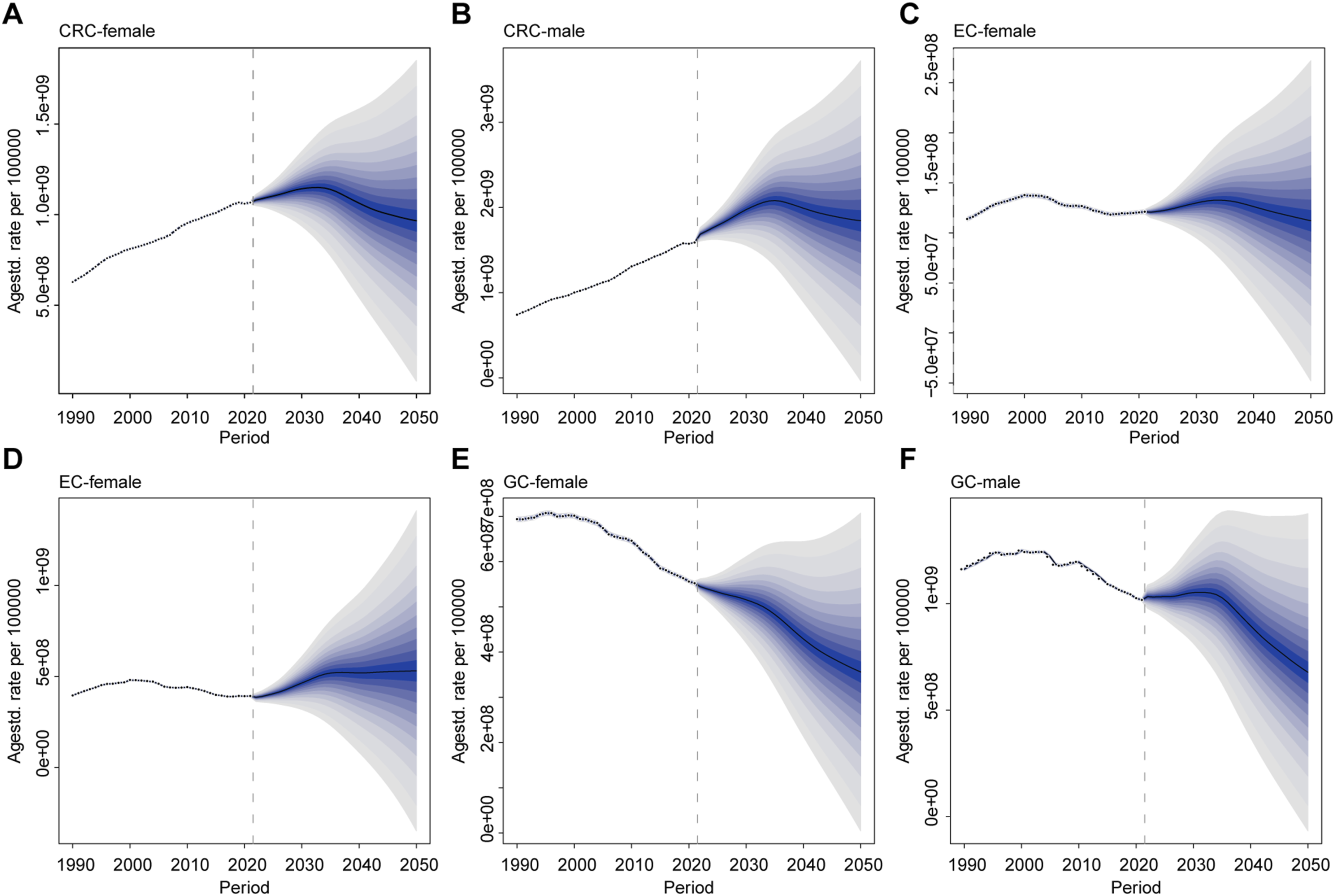
Global EOGICs are projected to continue declining overall, whereas ERCOC in males is expected to increase, reaching 36.16 (22.28–50.05) per 100,000 by 2050 (Supplementary Table 2). EOCRCs will still be the most burdensome EOGICs. Specifically, by sex, the incidence of case among CLF in males will decrease by 19.54%; the decline in females will be more, with the number of CLF-age cases decreasing by 37.86%. These predictions indicate that while the global EOGICs burden will decline, notable sex and regional disparities will persist.
Discussion
This study provides a comprehensive analysis to date of EOGICs, revealing divergent trends across EOEC, EOGC, EOCRC subtypes from 1990 to 2021. While the global ASIR of EOGICs has declined modestly, the absolute burden has increased, primarily driven by EOCRC, which was the only subtype to exhibit a continuous and statistically significant rise in ASIR throughout the study period (Table 1). This divergence between incidence rate stabilization and rising absolute burden indicates a growing per-case health impact, suggesting that younger patients may experience delayed diagnosis, more aggressive tumor biology, or limited access to early screening. These findings highlight the need for targeted public health interventions and underscore the potential value of early detection strategies tailored to the CLF population. By 2021, EOCRC accounted for over half of all EOGIC incident cases and DALYs worldwide, a shift likely fueled by lifestyle and metabolic changes such as increasing obesity,27,28 westernized diets, 29 physical inactivity, 30 and insulin resistance. 31 These trends align with mounting epidemiological evidence from other databases32-34: EOCRC rates in adults under 50 continue to rise, in contrast to stable or declining rates in older populations.
The disproportionate rise in EOCRC burden is further underscored by its divergent DALY trajectory, which continues to increase even as ASIR plateaus in some subgroups—reflecting a divergence between population aging and disease rate control. This suggests a growing per-case burden, potentially due to insufficient cognition of abnormal symptoms, 35 more aggressive tumor biology, 36 or limited access to screening in young adults. Notably, EOCRC is more likely to present with left-sided, poorly differentiated tumors at stage III/IV compared to its late-onset counterpart, contributing to higher morbidity and mortality per case.37,38 These patterns raise urgent concerns regarding healthcare system preparedness, as many current screening programs still exclude individuals under 50.39-41 Recent studies have highlighted the value of dual-modality imaging approaches to assess tumor-specific versus non-specific tracer uptake, demonstrating the potential of PD-L1–specific markers in accurately visualizing tumor burden and improving diagnostic precision in preclinical models. 42 Without earlier detection or tailored care models, DALY reductions may continue to lag behind treatment advancements, particularly in under-resourced or policy-inflexible settings. These findings underscore the critical importance of early detection strategies for EOGICs, particularly for the CLF population. Identifying reliable biomarkers specific for early-onset disease could facilitate targeted screening and timely intervention.
Bayesian projections paint a concerning picture of EOCRC’s future trajectory. The incidence of EOCRC is projected to surge through 2050, particularly among males and individuals aged 40–49. The projected dominance of EOCRC within the early-onset cancer landscape aligns with sustained increases in modifiable risk exposures, including alcohol consumption, 43 sedentary behavior, 30 and dietary westernization. 44 The steepest increases are expected in middle-aged early-onset adults, further amplifying the urgency to revise screening thresholds and intensify public health education targeting early- to mid-adulthood. Recent policy changes such as the USPSTF’s adjustment of screening age to 45 are a step forward, but may prove insufficient in the face of rapidly shifting age-onset distributions. 45
East Asia emerged as the most prominent regional outlier in our SDI analysis, bearing the highest ASIR and DALY rates across all EOGIC subtypes. For instance, ASIR of EOCRC in East Asia reached 11.86 per 100,000, well above global averages, while DALY rates of EOGC and EOEC were 222.6 and 92.2 per 100,000, respectively (Table 1). Several contextual factors help explain this burden. First, the baseline prevalence of gastric and esophageal cancers has historically been high in East Asia,46,47 partly due to dietary risk factors 48 such as high salt and preserved food intake. Second, endoscopic screening programs in countries like Japan 49 and South Korea 50 enable early detection, making DALYs more responsive to shifts in SDI. Third, aging population structures in these countries, despite the early-onset focus, concentrate cancer burden in narrower age bands. 51 This pattern suggests a complex interaction between development level, risk factor exposures, and healthcare response, underscoring the need for region-specific etiological research and screening policy adaptations.
Beyond regional outliers, our SDI-stratified analysis revealed a non-linear pattern in disease burden. While DALY rates generally declined with increasing SDI, EOCRC diverged, peaking in high-middle SDI regions before falling in high-SDI countries. This transitional peak may reflect the accumulation of lifestyle risks (Fig.S2-S4), such as processed food intake 52 and sedentary work, 53 outpacing the capacity of evolving healthcare systems to detect and manage disease early. It highlights how DALY rates do not uniformly track development and that cancer control success depends as much on systemic responsiveness as on socioeconomic indicators. The finding also affirms that rising development alone is not sufficient to reduce disease burden unless coupled with adaptable healthcare infrastructure and targeted public health strategies.54,55
Age remains a dominant axis along which EOGIC burden escalates. Both incidence and DALY rates rise steeply with age among early-onset patients, peaking in the 45–49 group. EOCRC shows a particularly sharp increase beginning after age 20, coinciding with increased exposure to behavioral risk factors and the latency of carcinogenesis. By the 45–49 age bracket, EOCRC DALY rates nearly double compared to the 40–44 group. Risk decomposition indicates marked sex-age heterogeneity. In males, smoking is the leading contributor to DALYs, most notably in EOEC, where the male-attributable burden is about fourfold that of females, and alcohol-related DALYs increase steeply with age. This pattern likely reflects higher tobacco and alcohol exposure, occupational risks, and the predominance of esophageal squamous cell carcinoma.56,57
In contrast, dietary risks dominate the female burden: low vegetable intake is the top contributor to EOEC DALYs in young women aged 25–29, while calcium and milk deficiencies are more salient for EOCRC, highlighting the need for targeted prevention, highlighting the need for targeted prevention. These findings support the hypothesis 58 that risk accumulation begins early in life, with long-latency mechanisms—ranging from mucosal inflammation 59 and metabolic stress60,61 to gut microbiome disruption62-64—culminating in middle-age disease. Age-targeted public health interventions, including earlier lifestyle counseling and stratified risk surveillance, are urgently needed. 65
Not all countries fit expected incidence-to-burden patterns. For example, France reported one of the highest EOCRC ASIRs in 2021 (9.66 per 100,000) yet ranked relatively low in DALY burden, likely reflecting effective screening and treatment. In contrast, Thailand and Malawi reported modest incidence but high DALY rates, indicating weaknesses in early diagnosis or access to care. Similarly, Mongolia exhibited the highest EOGC DALY rate despite being a high-SDI country, highlighting the persistent influence of localized risk factors such as diet, infection, and diagnostic capacity. These mismatches between incidence and DALY underscore the importance of evaluating not just disease occurrence but also outcome quality, survival, and healthcare system performance in understanding cancer burden.
This study is based on aggregated data from the Global Burden of Disease Study 2021 with some inherent limitations inevitably. As a model-based framework, GBD estimates depend on statistical methods to address missing or incomplete data, combine heterogeneous sources of varying quality, and account for uncertainty. Therefore, the reported incidence and DALY trends should be interpreted as estimates rather than exact values. In addition, the use of population-level data may introduce ecological bias and limit inference at the individual level. Our analysis focused on individuals aged 15–49 years and included only three major subtypes (EOCRC, EOGC, and EOEC), which may limit overall comprehensiveness. Moreover, some residual heterogeneity is likely, particularly in comparisons across regions with differing data availability and quality. Despite these limitations, the standardized methodology of the GBD framework enables robust relative comparisons across regions, sexes, and socioeconomic groups. Overall, our findings provide a comprehensive assessment of global trends in incidence and DALYs, offering valuable evidence to inform public health strategies and future research.
Together, these findings reflect a dynamic and increasingly complex epidemiology of EOGICs. EOCRC is now the dominant subtype, with a burden expected to grow, particularly among men and those in their 40s. EOGC and EOEC, though stabilizing in some regions, continue to pose significant challenges, especially in high-burden settings like East Asia. Age and sex remain critical axes of disparity, with risk factors varying across demographics. DALY patterns reveal the inadequacy of current screening thresholds, especially in younger adults, and the non-linear response of burden to development indicators such as SDI. These trends underscore the need for proactive, demographically tailored strategies centered on the CLF, including integrating risk-adapted early screening, workplace-enabled access to care, and targeted public health interventions. Policies should also ensure financial and psychosocial protections that sustain labor participation and household stability. In parallel, region-specific etiologic research and CLF-focused prevention and early detection programs are critical to mitigate the growing global burden of early-onset gastrointestinal malignancies.
Conclusion
EOGICs represent a growing global health challenge among CLF, with EOCRC emerging as the most prevalent and increasing subtype. Our analysis highlights substantial disparities in disease burden across regions, sexes, and socioeconomic contexts, indicating that existing cancer prevention and control strategies may not adequately address the needs of CLF. These findings underscore the importance of targeted research to better understand the drivers of early-onset gastrointestinal cancers and to inform evidence-based public health strategies aimed at mitigating their impact globally.
Supplemental Material
Supplemental Material - Global Burden of Early-Onset Gastrointestinal Cancers Among Core Labor Force From 1990 to 2021: Insights From the Global Burden of Disease Study 2021
Supplemental Material for Global Burden of Early-Onset Gastrointestinal Cancers Among Core Labor Force From 1990 to 2021: Insights From the Global Burden of Disease Study 2021 by Yi-Meng REN, Zi-Er FAN, Xin-Yang LIU, Quan-Lin LI, Ping-Hong ZHOU in Cancer Control
Supplemental Material
Supplemental Material - Global Burden of Early-Onset Gastrointestinal Cancers Among Core Labor Force From 1990 to 2021: Insights From the Global Burden of Disease Study 2021
Supplemental Material for Global Burden of Early-Onset Gastrointestinal Cancers Among Core Labor Force From 1990 to 2021: Insights From the Global Burden of Disease Study 2021 by Yi-Meng REN, Zi-Er FAN, Xin-Yang LIU, Quan-Lin LI, Ping-Hong ZHOU in Cancer Control
Supplemental Material
Supplemental Material - Global Burden of Early-Onset Gastrointestinal Cancers Among Core Labor Force From 1990 to 2021: Insights From the Global Burden of Disease Study 2021
Supplemental Material for Global Burden of Early-Onset Gastrointestinal Cancers Among Core Labor Force From 1990 to 2021: Insights From the Global Burden of Disease Study 2021 by Yi-Meng REN, Zi-Er FAN, Xin-Yang LIU, Quan-Lin LI, Ping-Hong ZHOU in Cancer Control
Footnotes
Acknowledgements
This study was supported by National Natural Science Foundation of China [grant numbers 82203227]. We acknowledge the Institute for Health Metrics and Evaluation (University of Washington), the GBD Collaborators, and all staff who provided the data necessary for this study. The opinions expressed here are those of the authors and do not necessarily represent the official position of the organizations with which they are affiliated.
Ethical Considerations
Given the use of publicly available, anonymized aggregate data, ethical approval or informed consent are not applicable to this study.
Author Contributions
Y.M.R and P.H.Z designed the research study; Y.M.R collected the data; Z.E.F and Y.M.R validation and visualisation the data.
Y.M.R, Z.E.F, X.Y.L, Q.L.L contributed to the statistical analysis and interpretation of data.
Z.E.F and Y.M.R drafted the manuscript, and other authors critically revised the manuscript.
Z.E.F and Y.M.R accessed and verified the underlying data.
All authors have read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China [grant numbers 82203227].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data from this study can be accessed openly through the GBD 2021 online database, as outlined in the Methods section.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.