
Abstract
Introduction
Adolescent and young adult (AYA) cancer survivors are at significant risk for late treatment-related effects yet face challenges when transitioning to survivorship-focused care and longitudinal follow-up. Population-level tools in the electronic health record (EHR) offer a pragmatic approach to track patients and optimize care.
Methods
The Seattle Children’s Hospital Cancer Survivor Program created a population health management system, using tools embedded within the EHR, based on a validated registry of AYA survivors. We developed a dynamic dashboard to make care gaps visible survivorship care, provide exposure-based pulmonary and cardiac toxicity surveillance, and support transition to adult care. We also built reports to facilitate real-world data analysis of the transition to survivorship care and longitudinal follow-up in a retrospective cohort of AYA survivors. We analyzed data from the cohort to explore subgroup differences in survivorship care.
Results
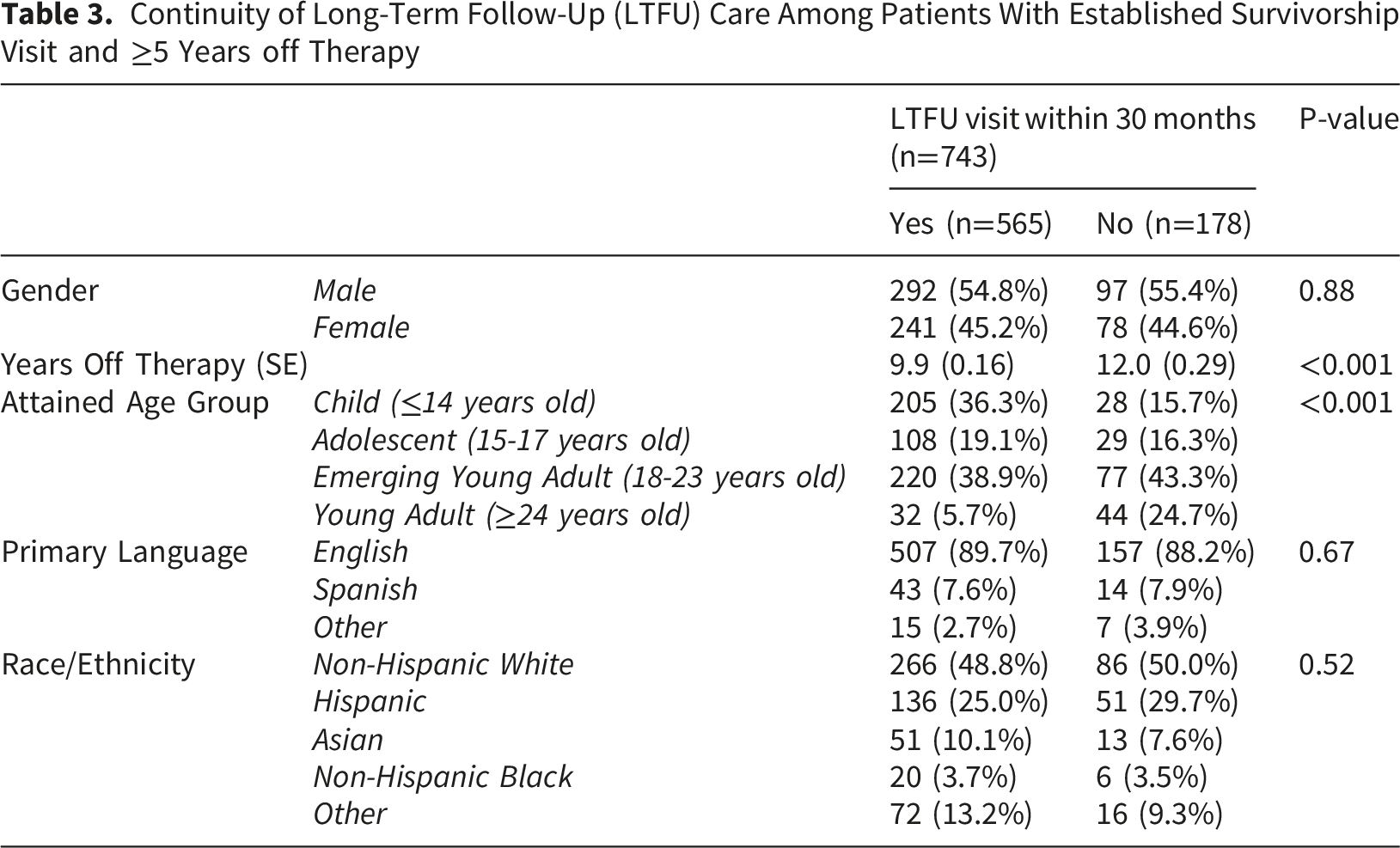
Among survivors who finished treatment between January 1, 2021, and April 30, 2022 (n=220), 47% completed a long-term follow-up visit. There were no differences in the likelihood of follow-up based on age categories (p=0.36). For survivors with established long-term follow-up (n=743), 76% received longitudinal care. Compared with children, adolescent survivors (OR 0.51, 95% CI 0.29-0.9), emerging young adults (OR 0.39, 95% CI 0.24-0.63), and young adults (OR 0.10, 95% CI 0.05-0.18) were less likely to have a survivorship visit in the preceding 30 months. This difference was attenuated when analysis was restricted to survivors <22 years old and adjustment for years off therapy, with OR of 0.67 (95%CI 0.37-1.21) and 0.82 (0.45-1.50) among AYAs compared to children as the referent group.
Conclusion
An EHR embedded population health platform represents a feasible approach to measure longitudinal follow-up care and transitions among AYA survivors. Clinical informatics tools have the potential to drive innovation and enhance evidence-based, guideline-concordant care to mitigate late effects in this population.
Keywords
Introduction
Adolescent and young adult (AYA) cancer survivors face significant challenges in achieving recommended longitudinal follow-up after cancer-specific therapy. Recent improvements in the five-year overall cancer survival rates contribute to the growing number of AYA survivors across the United States. 1 Longitudinal follow-up is critical in order to effectively identify and manage chronic health conditions among survivors of childhood and adolescent cancers, as modifiable cardiovascular risk factors such as hypertension are often under-detected in adulthood. 2 Several factors contribute to challenges in engaging AYAs in follow-up, including the long latency period between treatment exposures and adverse outcomes. Survivors who received anthracyclines or radiation, for example, may experience minimal sequelae in the early survivorship period, but the risk for cardiovascular disease (CVD) and secondary malignancy increases substantially later in life.3-5 Survivors experience differing risks for late effects, as these are based on specific treatment exposures and complex health needs of this population.6,7
Simultaneously, AYA cancer survivors face a myriad of challenges after completing cancer-directed therapy. Understandably, the AYA years represent a critical stage for education, vocational training, employment, and building a foundation for independence. A cancer diagnosis disrupts this trajectory, incurs significant financial burdens, and the socioeconomic effects linger well beyond the initial time of treatment.8,9 Moreover, the long-term psychological trauma and mental health burden among survivors underscores the need for longitudinal, comprehensive support across the lifespan.10-12 Tackling inequities in survivorship-focused care, including transitions of care, requires creative, novel approaches to mitigate late treatment-associated toxicities.
Excellent evidence-based guidelines can assist clinicians and patients in managing the long-term effects of a growing variety of complex cancer treatment regimens, but are often underutilized. These guidelines and associated individualized risk prediction tools for major late effects are based on several rigorous survivorship studies, many of which were conducted with cohorts with meticulous, longitudinal follow-up, such as the Childhood Cancer Survivor Study, St. Jude Life, and numerous European cohorts.13-16 The implementation of the electronic health record (EHR) and the widespread adoption through the Health Information Technology for Economic and Clinical Health Act created an infrastructure to capture clinically important discrete data elements, which can be leveraged for previously validated prediction models in late effects risk prediction. 17
Systematic, reliable interventions are needed to surveil and evaluate patients once they complete cancer therapy. Previous studies identified disparities in optimal follow-up in the early survivorship period among AYA survivors, compared with survivors diagnosed at a younger age.18,19 Many primary care practices routinely use population health management tools for identifying care needs for patients with diagnoses such as diabetes, hypertension, and chronic kidney disease. Development of mechanisms to leverage data directly from the EHR for direct clinical application, quality improvement initiatives, and traditional research could accelerate translation of data into knowledge and action for population health management. Such tools have not yet been widely adapted for routine use in follow-up for cancer survivorship.20-24 Population health tools integrated in the EHR offer a pragmatic approach to routinely identify care needs for this patient population while simultaneously identifying inequities in at-risk AYA survivors.
Effective strategies to enhance clinical care, health systems, and public health integrate multi-level targets to drive outcomes.25,26 Population health management tools in the EHR complement the aims of a learning health system at the intersection of research, real-world data, and direct impact on clinical operations. 27 Our central goal was to develop a reproducible, EHR-based population health platform that harnesses discrete data to construct and validate a survivorship cohort, to visualize guideline-based metrics, such as echocardiogram adherence based on cumulative anthracycline exposure and pulmonary function tests for survivors who received bleomycin, and track key transitions from active oncology to pediatric long-term follow-up to adult survivorship-focused care. As a secondary aim, we leveraged the platform to explore patient subgroup differences in transition to survivorship care.
Methods
The Cancer Survivor Program at Seattle Children’s Hospital (SCH) was established over two decades ago and conducts visits for approximately 600 survivors annually. Survivors generally transition from their primary oncology team to the survivor program between two to three years after completion of treatment and are followed every one to two years thereafter. SCH partners with the Fred Hutchinson Cancer Center for transition to adult survivorship at 21 years of age, or five years after completion of therapy, whichever occurs later. In 2020, SCH implemented Epic as the new EHR. Epic Systems designed Healthy Planet (HP) as a platform for population health management within the EHR. HP includes tools such as reports and dynamic dashboard with metrics relevant to population health goals, enables risk-based scoring using discrete data elements in the EHR, and catalyzes interventions through tools such as bulk ordering and bulk messaging. The data presented were included in the research protocol SC-N160, approved by the SC Institutional Review Board on October 30, 2023.
Cohort Construction and Validation
Careful construction and validation of the patient cohort within the EHR is essential (Figure 1). We started with a parent registry of active oncology patients treated at SCH who were identified based on the set of initial diagnosis codes (e.g. ‘diagnosis grouper’) in the EHR; however, upon cross-validation with our institutional database external to the EHR, only 2270 out of 4066 patients were appropriately identified (55.8%) based on these codes alone. Manual chart review revealed that the active oncology registry did not include patients with a history of malignancy but were not in active treatment. Additional SNOMED concept groupers were added as inclusion criteria, which improved the alignment with the institutional database to 4052/4066 (99.7%). Thus, the revised active oncology registry included patients with a living status of alive, and either an active problem from the cancer diagnosis grouper on their problem list or a problem from the history of cancer diagnosis grouper. The active oncology diagnosis grouper is a comprehensive collection of ICD-10 codes in the Epic release range that is developed and maintained directly by Epic. The history of cancer diagnosis grouper was developed using the following concept hierarchies with “OR” logic: History of neoplasm (SNOMED#275904003), H/O: Malignant Neoplasm (SNOMED#266987004), History of acute lymphoid leukemia (SNOMED#676112841000119101), and History of Leukemia (SNOMED#161436008). A complete list of ICD-10 codes is included as Supplemental Material 1 to facilitate reproducibility. Cohort construction and validation steps for parent and child registries in the EHR to construct the healthy planet survivor cohort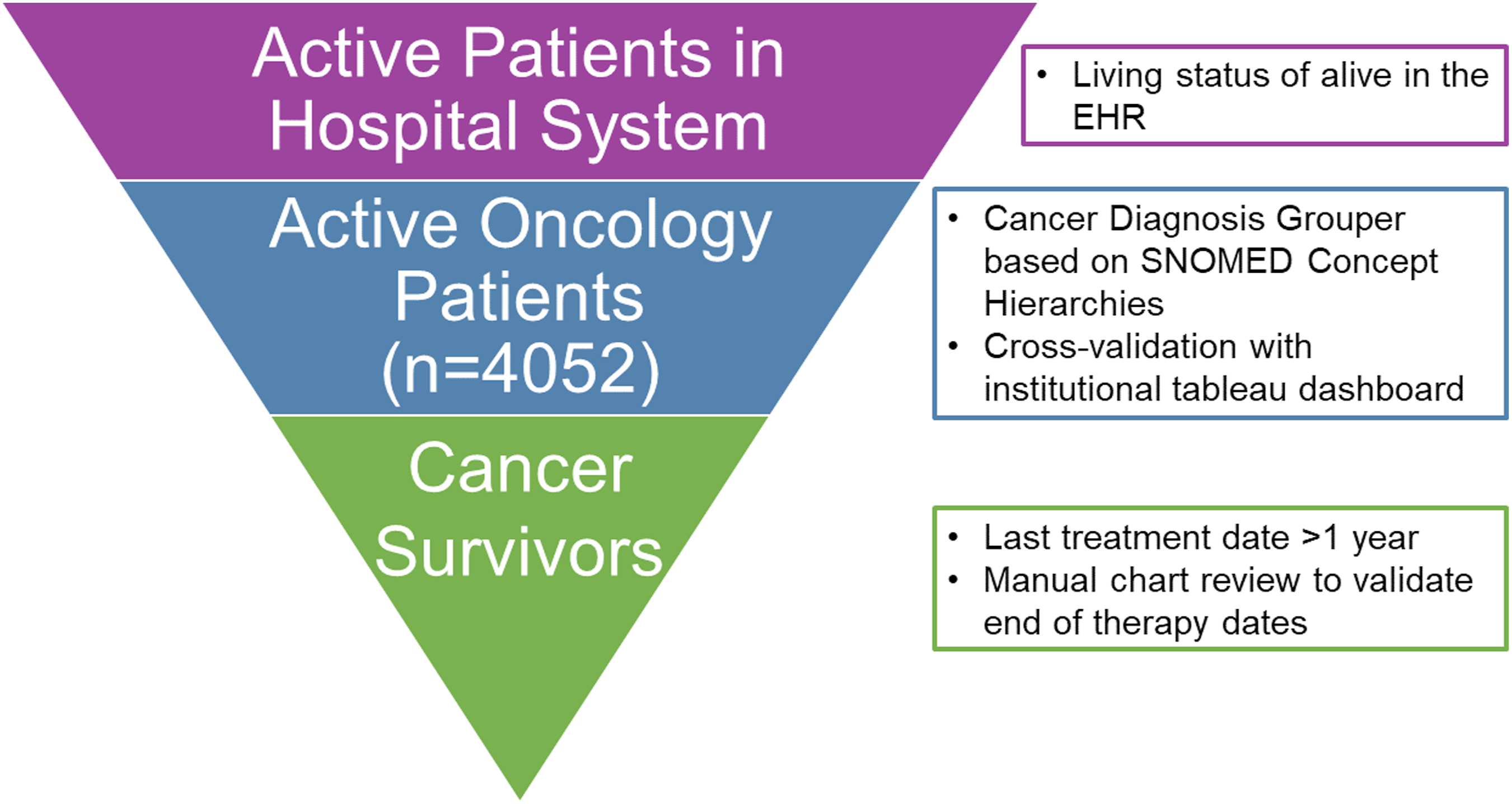
To further define the survivor cohort, the last treatment date at least one year prior to the current date was used. The last treatment date was defined as the date of last chemotherapy or, if this was unavailable, the discrete “End of Therapy” date recorded in the oncology history. The relapse date as recorded in the oncology history was also included in the logic to define the survivor cohort. Adding this logic ensured the survivor cohort included only patients without active cancer in the past year, and those with relapse in the years following their last treatment were automatically excluded.
Validation of the end of therapy date and last clinic date was initially conducted via manual review of 31 patients, among whom there was 100% concordance for the last clinic appointment date. Agreement between the end of therapy date reported by HP within 45 days of the end of therapy date from manual review yielded only 83.9% concordance. The five discordant patients had either transferred care to another institution or a treatment regimen was planned but not completed. The HP logic was subsequently updated to include the last date of completed therapy. A final manual review of 10% of patients who completed treatment post-Epic implementation between January 1, 2021, and April 30, 2022 (n=22), yielded 86.4% concordance. Discordant cases were primarily due to therapy completed at an outside institution, though one patient had a treatment plan documented as complete, which only had diagnostic testing orders.
Care Gap Definitions
Care gaps are created for key metrics within the EHR to illustrate specific aspects of care delivery for the population and allow for visibility of subpopulations at increased risk for long-term complications. For the HP survivor cohort, the initial care gaps included transition to long-term follow-up within 3 years from completion of therapy, transition to adult survivorship-focused care by age 22 or 6 years after discontinuation of therapy (whichever occurs later), and adherence to exposure-based COG Long-Term Follow-up Guideline recommendations (e.g. echocardiogram surveillance based on cumulative anthracycline exposure and pulmonary function test screening for survivors who received bleomycin).
28
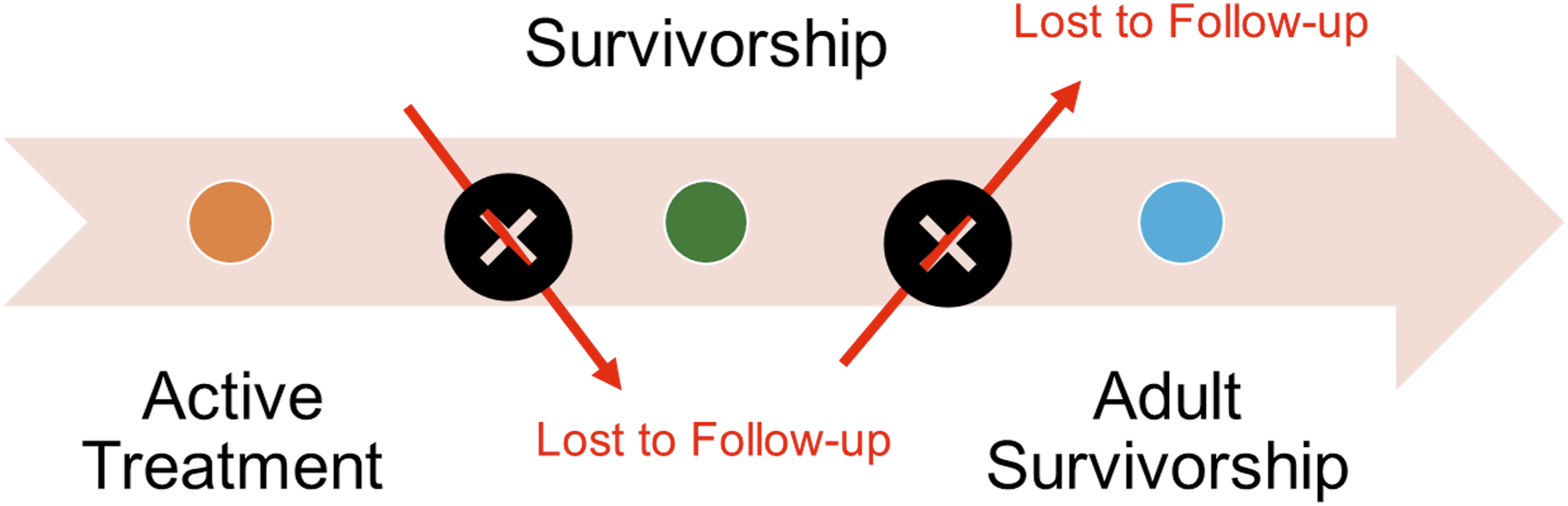
Figure 2 illustrates the survivor dashboard with each of these care gaps, and the associated hyperlinks that open full reports for the survivors with identified care gaps. Reports that focus on transitions and longitudinal care, can identify patients at risk for loss to follow-up (Figure 3). For operational purposes, a data feed from the Fred Hutchinson Cancer Center (a separate Epic site) pulls in completed appointments from the adult survivors of childhood cancer clinic directly to the HP dashboard. While data are not presented here due to restrictions in the research space for CareEverywhere, this real-time data linkage highlights the importance of interoperability and opportunity to enhance AYA transitions from pediatric to adult programs. Healthy planet dashboard with care gaps Transition from active oncology to long-term follow-up to adult survivorship-focused care. Patients generally transition to the survivor program 2-3 years after completion of treatment, are followed every 1-2 years thereafter, and transition to the adult survivor program at age 21 or five years off therapy, whichever occurs later. Measurement of clinic follow-up at key transitions informs population health interventions to optimize care.
Statistical Analysis
The secondary aim of this work was to evaluate differences in care, specifically the initial transition from the active oncology team to the survivor program and proportions of the population with optimal longitudinal follow-up among the retrospective cohort of established cancer survivors. The initial transition to survivorship care from the primary oncology team was defined as a clinic visit with the long-term follow-up (LTFU) team, for survivors who completed treatment between January 1, 2021, and April 30, 2022, to reflect the transition to Epic and allow for a minimum of 42 months from the end of therapy to the date of analysis. For longitudinal survivorship-focused care, we restricted to survivors with a documented survivorship visit and who were ≥5 years off therapy. Optimal survivorship care was defined as an LTFU visit within the previous thirty months (to reflect that most survivors are recommended to return every 1-2 years). The study size included all eligible patients who met the aforementioned criteria. Predictor variables included gender, attained age group at time of analysis (child, age<15 years; adolescent, ages 15-17 years; emerging young adult, ages 18-23 years), primary language (English, Spanish, other), and race and ethnicity as documented in the EHR. Additionally, for survivors with end-of-therapy post-EHR transition, radiotherapy, cumulative anthracycline dose, and bleomycin exposure were included as these were validated and pulled directly into HP. All outcome and predictor variables were categorical; thus, differences were compared using the χ2 test. For longitudinal care, unadjusted odds ratios (OR) were calculated with child age group as the referent group and restricted to survivors with attained age <22 years old to reflect institutional practices for transitions to adult survivorship-focused care. To address potential bias for years off therapy and confounding with age group as the primary predictor of interest, OR were also adjusted for years off therapy, as survivors further from treatment may have been less likely to follow up and have a greater attained age. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines informed the reporting of this analysis. 29 All statistical analyses were conducted using Stata/SE version 14.2 (Stata Corp LLC, College Station, Texas).
Results
Population Health Dashboard Components and Workbench Data Elements
Full Survivor Cohort Characteristics
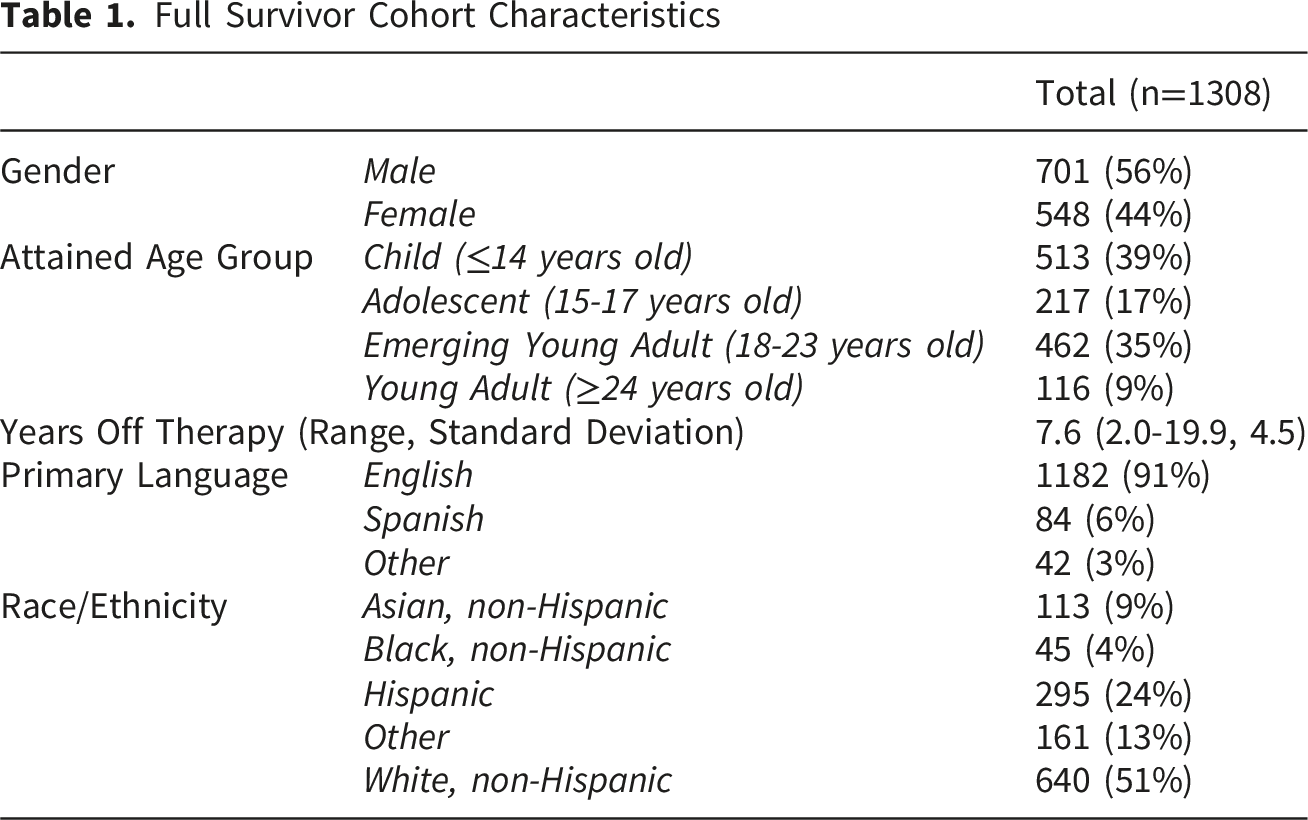
The reports include patient-level data for the full cohort of survivors to facilitate further evaluation of care metrics, enable interventions, such as bulk communication and bulk ordering, or integrate the tool for patient tracking among key survivorship team members. Age, gender, race/ethnicity, and preferred language represent demographic characteristics to promote strategies toward health equity and identify patients who are eligible for research studies, peer support groups, or other opportunities for survivors. Filtering by disease-based teams stratifies survivors to assess diverse needs and systems-level nuances among those treated for leukemia/lymphoma, solid tumor, brain tumor, and transplant. Discrete data elements, such as the last oncology clinic visit date, provider, date of last oncology treatment, last long-term follow-up clinic, future appointments, last and next scheduled echocardiogram date, cumulative anthracycline and bleomycin doses, radiation exposure, and last survivorship visit at the adult cancer center, were included in the initial reports.
Transition to Survivorship
Survivors With End of Therapy From January 1, 2021-April 30, 2022

*For primary language, Spanish included in “Other” due to small cell sizes. Similarly, non-Hispanic Black, Asian were also included in “Other” due to small cell sizes.
Longitudinal LTFU Care
Continuity of Long-Term Follow-Up (LTFU) Care Among Patients With Established Survivorship Visit and ≥5 Years off Therapy
Differences by Age Group in Long-Term Follow-Up Care Among Patients With Established Survivorship Visit and ≥5 Years off Therapy

1Adjusted for years off therapy.
Discussion
The EHR-based platform for population health management of AYA cancer survivors represents a feasible and innovative approach to enhance transitions to survivorship-focused care, assess guideline adherence, and track longitudinal follow-up. As a use case for the utility of this platform, the secondary aim was to harness this tool to evaluate differences in patterns of care within the cohort. In this single institution cohort, the likelihood of longitudinal follow-up for adolescents and emerging young adults was half of that observed for children. Although this was attenuated by years off therapy, longitudinal care to address modifiable risk factors during the AYA years, as the burden of chronic health conditions and secondary malignancies rises for many survivors, is essential to mitigate late effects.3,4,30
The primary intended use of dynamic, near-real-time population health dashboards supports the operational needs and informs a clinical survivor program. A snapshot of key metrics, such as the transition to survivorship and longitudinal follow-up, illustrates the added utility for real-world data, measures for quality improvement work, and the implementation of risk-based, guideline-adherent care on a population health level. This is particularly relevant for AYA survivors, both those diagnosed in the AYA years and childhood cancer survivors approaching the critical transition to adulthood. The build of the dashboard supports near real-time analytics, such as the differences in establishment of survivorship care and longitudinal follow-up and facilitates population-based interventions. For example, HP can drill down on eligible survivors overdue for transition to LTFU and provides the functionality of bulk in-basket messaging of active oncology teams to nudge consideration for a referral. Similarly, for established survivors overdue for follow-up, bulk communications, and bulk ordering of return to clinic requests may spark re-engagement in care. The interplay between analytics, population-based interventions, patient engagement, and near-real time feedback is critical to iteratively validate, expand, and demonstrate effectiveness of such platforms.
Interpretation and generalization of these data requires contextualization and caution regarding potential biases and limitations in this initial launch of HP. For example, the associations with radiotherapy and cumulative anthracycline dose we observed in those who made the initial transition from the active oncology team to survivorship-focused care likely represent variations in disease-based team practices in timing for transition to survivorship, as solid tumor and brain tumor survivors are more likely to receive radiation and transition to LTFU closer to five years off therapy. Similarly, brain tumor survivors without anthracycline exposure likely account for this observed difference, as many are well served in a local comprehensive brain tumor clinic. Our study cohort was limited to survivors with clinical documentation post-Epic implementation at our institution in 2020. Thus, for longitudinal follow-up, this may have introduced selection bias toward higher levels of follow-up. The end of therapy date, despite multiple iterations to the coding, yielded <90% concordance, and manual review confirmed the challenges with patients moving in and out of a single healthcare system for their oncology care. The creation of a discrete “Transferred Care” field within the EHR and a manual “End of Therapy Date” field are solutions, yet these strategies rely on uptake in the workflow of the care team. Furthermore, as the tool is dynamic within the EHR, validation at routine intervals is needed to ensure the sustainability and integrity of the care metrics.
Transition of care from the pediatric to the adult healthcare represents a perennial challenge and calls for innovation to develop effective implementation practices based on consensus statements to ensure equitable, patient-centered care for AYAs.31,32 For AYA survivors, few pediatric oncology institutions offer formal readiness programs for transition to adult care, and we lack routine reporting on quality standards for this transition. 33 Recent attention to transitions for AYAs impacted by cancer offers evidence-based recommendations and potential paths forward.34-37 Frameworks for pediatric-to-adult health care transition provide measurable steps toward transition readiness and guideline-based metrics across the continuum of care. 38 Consequently, health systems need population-health level methods to track and support AYA survivors, particularly those at high risk for late effects, through the critical transition to adult care.
As next steps for the population health management platform, the inclusion of additional key treatment exposures will facilitate the implementation of previously validated risk calculators to further refine survivors at risk for specific late effects. Risk for premature ovarian insufficiency, for example, can be predicted from discrete data elements such as cumulative alkylator dose and ovarian radiation exposure. 39 Similar risk calculators for late CVD, chronic kidney disease, and breast cancer, among others, offer tools for clinical decision-making and survivor empowerment.40-43 Even without access to granular treatment details, rough risk stratification to distinguish between survivors at high, intermediate, and low risk for late effects demonstrates some utility.18,19,44 The International Guideline Harmonization Group (IGHG) and the exposure-based format of the Children’s Oncology Group (COG) Long-Term Follow-up Guidelines help identify patients at greatest risk for late effects.28,45 Population health management leveraging established guidelines for AYA survivors provides an opportunity for improved patient tracking and a risk-based approach to prioritize outreach for the most vulnerable patients.
Clinical informatics tools, embedded with health information systems, can enhance clinical decision support and support population health management. For AYA survivors confronted by fragmented care, educational needs, vocational challenges, and financial toxicity, navigating adulthood and health systems is increasingly complex.8,9,46,47 Novel strategies, such as the HP, provide a population health platform to longitudinally follow AYA survivors, track risk-based care gaps, inform quality improvement work, and drive research to reduce current disparities in the AYA population. Adherence to guidelines poses a significant challenge, and the complexities of risk-based survivorship care continue to grow with new evidence in the changing landscape of modern therapy.30,48-50 Health-systems approaches to measure and intervene on population health-level outcomes among survivors are synergistic with recent efforts to define quality and standards in quality of care in survivorship.51-53
Conclusion
Population health management tools, embedded within the EHR, offer invaluable insight into local survivor cohorts and the opportunity to directly implement population-level interventions. The development of tools within the EHR to evaluate real-world data to examine AYA transitions serves as a use case to spark future innovation to impact evidence-based, guideline-adherent care to mitigate late effects. Furthermore, expansion, adaptation, and scalability of the methods described herein to established survivor programs or cancer centers looking to launch a program have the potential to break barriers and build solutions for AYA survivors.
Supplemental Material
Supplemental material - An Informatics Approach to Enhance Care for Childhood, Adolescent and Young Adult Cancer Survivors Through Population Health Management
Supplemental material for An Informatics Approach to Enhance Care for Childhood, Adolescent and Young Adult Cancer Survivors Through Population Health Management by David H. Noyd, Lindsey Coons, Jonathan D. Bank, Emily Larimer, Gayle Garson, Vicky Aliferakis, Taylor Giovannetti, Carlos Villavicencio, Yu-Hsiang Lin, Michael G. Leu, Eric J. Chow, Carrie L. Heike in Cancer Control
Footnotes
Ethical Considerations
The data presented were included in the research protocol SC-N160, approved by the Seattle Children’s Institutional Review Board on October 30, 2023.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Seattle Children’s Hospital Electronic Health Record Support Optimization Provider Program.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.