
Abstract
Introduction
Digital interventions for 24-hour movement patterns (i.e., physical activity, sedentary behavior, sleep) show promise for cancer prevention, particularly among Black and Hispanic women, who experience worse cancer outcomes and lower adherence to sleep and physical activity guidelines. This study examined whether neighborhood characteristics influence digital health use and attitudes among Black and Hispanic women and explored whether individual sociodemographic factors moderate these relationships.
Methods
In a secondary analysis of a cross-sectional study, a total of 992 Black and Hispanic women aged 18-49 completed an online survey assessing demographic factors, sleep quality, physical activity levels, digital health use, and attitudes towards digital health interventions for sleep and physical activity. Neighborhood-level data on socioeconomic status, racial composition, and access to health services were extracted from geocoded addresses. Multivariable binary logistic regression models tested associations between neighborhood characteristics and digital health outcomes. Moderation by age, race, and education was assessed.
Results
Black and Hispanic women living in neighborhoods with low or moderate-to-high socioeconomic risk were more likely to own wearable devices than those in high-risk neighborhoods. Health app use was more common among Black and Hispanic women in neighborhoods with higher rates of adults having personal doctors and greater out-of-pocket medical expenses. Among women in medically underserviced neighborhoods, Black women were more likely to use a health app, while Hispanic women were less likely. Race, age, and education moderated the influence of access to health services and racial structures on interest in digital health interventions for physical activity and sleep.
Conclusion
Neighborhood characteristics such as socioeconomic status, healthcare access, and racial structures play a vital role in shaping digital health use and attitudes among Black and Hispanic women. Tailored digital interventions that consider neighborhood-level factors may improve adoption, engagement, and effectiveness, and ultimately reduce cancer risk in these populations.
Keywords
Introduction
Cancer is the second leading cause of death among women in the United States, 1 especially for Hispanic and non-Hispanic Black women (hereafter referred to as Black women).2-7 Meeting 24-hour movement guidelines, including sufficient sleep (i.e., 7-9 hours for ages 18-64 and 7-8 hours for ages 65 and older), sufficient physical activity (i.e., 150 minutes or more of moderate to vigorous physical activity per week), and reduced sedentary behavior (i.e., less than 8 hours per day) can be protective factors for all-cause and specific cancers such as ovarian, breast, and uterine cancers.7-14 However, Black and Hispanic women in the US are less likely to engage in sufficient physical activity 15 and also experience more irregular sleep compared to non-Hispanic White women.16,17 This presents a crucial need to create tailored interventions in physical activity and sleep for cancer prevention in these populations.
While physical activity and sleep are behaviors that can be influenced at the individual-level, neighborhood characteristics also widely shape these health behaviors. For example, lower neighborhood socioeconomic status is associated with long sleep duration (i.e., beyond recommendations) in Black women, 18 and worse neighborhood cohesion is linked to poorer sleep quality in Black and Hispanic women. 19 Furthermore, commonly cited barriers to physical activity in ethnic minority women include neighborhood safety, limited access to physical activity resources, and inadequate infrastructure. 20 Considering these links, it is crucial to address physical activity and sleep for cancer prevention in the context of neighborhood characteristics.
Advancements in digital health technology and remote monitoring devices, featuring real-time tracking and feedback of physical activity, sedentary behavior, and sleep, provide novel solutions that integrate neighborhood characteristics. 21 For example, one digital intervention implemented place-based messaging to promote physical activity in Black women residing in lower-resourced neighborhoods. 22 However, despite the saturation of smartphone usage in the US, with 91% of Americans owning smart phones, including 87% Black and 93% Hispanic, 23 subsets of Black and Hispanic women still have lower digital health usage rates. 24 This may indicate that although smartphone usage is high, digital health may be less utilized and consequently feasibility and acceptability of digital interventions may be lower. In contrast, evidence suggests receptivity among some Black and Hispanic women towards remote interventions and the use of wearable devices for sleep and physical activity. 25 For example, 77% of a Black women cohort reported interest in a remotely delivered physical activity program and 64% were interested in receiving personalized feedback messages about their sleep based on a wearable device. 26 This mismatch between digital health use and receptivity among Black and Hispanic women suggests that there may be factors at a higher level, such as neighborhood characteristics, that influence digital health use and attitudes. Assessing the current digital health use and attitudes in Black and Hispanic women can provide a pragmatic proxy for likely interest, acceptability, and feasibility of future tailored digital interventions in cancer prevention for these populations, and may also inform recruitment, design, and implementation strategies. However, how objective neighborhood characteristics influence digital health use and attitudes in Black and Hispanic women in the US is not yet clear.
This study is informed by socioecological and health equity frameworks, which recognize that health behaviors are shaped by multilevel influences, including individual, social, and neighborhood-level factors. Neighborhood characteristics such as socioeconomic status, racial composition, and healthcare access represent key social determinants of health that may influence access to and engagement with digital health technologies, reflecting broader digital divide considerations. Understanding these multilevel influences is essential for developing equitable digital interventions targeting physical activity and sleep behaviors for cancer prevention among Black and Hispanic women. Accordingly, this study aims to (1) examine whether objective neighborhood-level characteristics (i.e., racial structures, neighborhood-level socioeconomic status, and access to health services) influence digital health use, and attitudes in Black and Hispanic women and (2) explore if person-level demographics (i.e., age, race, and education) moderate these relationships.
Methods
Participants
This study was a secondary data analysis of a cross-sectional survey study aiming to examine Black and Hispanic women’s digital health usage and attitudes towards remotely delivered interventions. Participants were recruited from Prolific Academic, a platform designed to recruit participants for online research studies. Participants who met our inclusion criteria (currently residing in the US, female, aged 18–49, and self-identified as Black/African American or Hispanic) were selected through convenience sampling through an opt-in basis. This study was originally conducted in Black women only in February 2021 and later was expanded to include Hispanic women in October 2022, which was offered in both English and Spanish. This study combines these two datasets. The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of the University of Texas at Arlington (Protocol # 2021-0207) in February 2021. Informed consent was obtained from all subjects involved in the study. The reporting of this study conforms to the STROBE guidelines. 27
Survey and Geocoding Process
Participants who provided informed consent electronically for the study subsequently completed the survey via QuestionPro, an institution-supported survey platform. The questions assessed participants’ current sleep quality and duration, physical activity level, health application usage, wearable device usage, perceptions of remotely delivered intervention, and demographic information. 26 These survey items were adapted from existing, validated survey instruments 28 and from national health surveys. 29 The present analyses is an extension of the original publication, as it integrates geolocation details to assess neighborhood characteristics and it includes an additional sample of Hispanic women.
After a participant completed a survey, QuestionPro automatically logged the approximate latitude and longitude coordinates based on the participant’s IP address. All participant details were de-identified prior to analysis, so that personal information would not be tied to these coordinates. Research staff then uploaded these coordinates to Batchgeo 30 to extract the complete street addresses. For the coordinates whose addresses could not be found on Batchgeo, research staff searched on Google Maps, 28 Mapquest, 31 or Bing Maps, 32 in the listed order, until a complete address was identified. The complete addresses were then uploaded to PolicyMap, an online geographic information system (GIS) mapping tool containing geographic characteristics of the United States. 33 Each variable was extracted at the most precise level when available (county, census tract, or block group for the selected variables in this study). Neighborhood characteristics related to socioeconomic status, racial structures, and access to health services were extracted from the database. Ten total neighborhood-level predictors were extracted from PolicyMap, which are detailed in the “Neighborhood Characteristics” section below.
Variables
Digital Health Use and Attitudes
The following five self-reported variables were used to assess digital health use and attitudes, and were dichotomized (“yes”, “no”) for analysis: 1) Wearable sensor ownership, 2) health-related app usage, 3) interest in a remotely delivered physical activity intervention, 4) interest in wearable sensor-based feedback messages for physical activity and 5) interest in wearable sensor-based feedback messages for sleep. Wearable sensor ownership originally had answer choices, “yes”, “no, but planning to”, and “no, but not planning to”. The latter two response were recoded as “no”. Health-related app usage originally had answer choices, “almost daily”, “couple times a day”, “couple times a month”, “couple times a year”, and “never”. The first four responses were recoded as “yes” and the last response as recoded as “no”. The last 3 variables regarding interest in digital interventions originally had the answer choices “yes”, “no”, and “not sure”. Responses of “not sure” were recoded to blank cells and treated as missing. These variables were selected to assess the use of digital health technology and interest in remote interventions.
Sleep and Physical Activity
Participants self-reported sleep duration, sleep quality, and physical activity levels in the past month. Sleep duration and sleep quality were measured through select questions from the Pittsburg Sleep Quality Index (PSQI). 28 Current physical activity level was measured by giving a definition and examples of moderate-intensity activities, followed by the question, “Considering the definition above, during the past 30 days, how many minutes of moderate-intensity activities you typically do in a week?”. Full questionnaires for these measures were not given because the primary purpose of this study was not to obtain participants’ complete sleep and physical activity behaviors. These variables were intended for descriptive purposes and were not included in the main statistical analyses.
Neighborhood-Level Characteristics
Socioeconomic Status
Socioeconomic Risk
Socioeconomic risk was represented by CDC’s 2018 Social Vulnerability Index (SVI) at the census tract level. 34 This composite index incorporated four indicators: the percentage of the population living below the federal poverty level, unemployment rate, per capita income, and the proportion of individuals without a high school diploma. Based on the overall SVI score, the variable was categorized into four quantiles of risk: low (tracts in the bottom 25th percentile), low to moderate (tracts in the 25-50th percentile), moderate to high (tracts in the 50-75th percentile), and high (tracts above the 75th percentile), with higher categories indicating greater socioeconomic risk.
Inequality of Household Income
Inequality of household income estimated the percent inequality of household income according to the Gini index between 2017-2021 at the Census Track level. 35 This continuous variable ranged from 0-1, with a higher score representing greater inequality of household income.
Median Household Income
Median household income estimated median income of a household between 2017-2021 at the Block Group level.
36
This continuous variable was analyzed as a categorical variable based on a median split:
Racial Structures
Racial Diversity Index
Diversity index measures the probability that two individuals chosen at random would be from different racial and ethnic groups between 2017-2021 at the block group level. 37 This continuous variable ranged from 0-100, with a greater score representing greater diversity.
Racial Segregation
Racial segregation as of 2010 was measured according to the Theil Index at the block group level. 38 This continuous variable ranged from 0-1, with a greater score representing greater racial segregation.
Access to Health Services
Personal Doctor
Personal doctor was measured by an estimated percent of all adults reporting to have a personal doctor or healthcare provider in 2018 at the census tract level. 39 This continuous variable ranged from 0-100 percent.
Rate of Physician’s Offices
Rate of physician’s offices per 100,000 people in 2019 was measured at the county level. 40 For this continuous variable, a higher number represented a greater amount of physician’s offices per 100,000 people.
Out-Of-Pocket Medical Expenses
Average annual dollars spent out of pocket per person on medical care was estimated in 2019 at the census tract level. 41 We dichotomized this categorical variable based on a median split: ≤ $900 and > $900, which is consistent with the average out-of-pocket expenditures in the United States in 2019. 42
Index of Medical Underservice (IMU) Score
The Index of Medical Underservice (IMU) score as of 2022 was calculated at the census tract level. 43 The medical underservice score is calculated using four factors: ratio of primary care physicians per 1000 population, infant mortality rate, percentage of population below the poverty level, and percentage of persons aged 65 or older. This continuous variable ranged from 0-100, with a greater score representing greater medical underservice.
Rate of Fitness and Recreational Sport Centers
The rate of fitness and recreational sport centers per 100,000 people was calculated in 2019 at the census tract level. 44 In this continuous variable, a higher number represented a greater amount of fitness and recreational sport centers per 100,000 people.
Covariates
Covariates at the individual-level included age (18-24 vs. 25-49, based on a standardized age split for young adults and adults), 45 household income (≤ $50,000 vs. > $50,000, based on median split), education (less than Bachelors vs. Bachelor or higher, based on median split), race (Black vs. Hispanic), marital status (single, married, vs. other), employment status (not employed, full-time employed, vs. other), health insurance status (uninsured, insured, vs. unknown), chronic disease status (no vs. yes to at least one), and region (West, Midwest, South, vs.Northeast). Age, education, and income were dichotomized to ensure sufficient group membership and create conceptually meaningful groups reflecting relatively lower versus higher status groups. Any variables with “prefer not to say” were treated as missing values.
Statistical Analysis
Binary logistic regression was conducted on SAS 9.4 (Cary, North Carolina, USA). Before running regression analyses, the data were assessed for clustering at the zip code, census tract, and county levels. There was no or minimal clustering at the zip code, tract, or county level, so multi-level logistic regression was not used. This approach is consistent with methodological guidance that recommends single-level models when there a very few observations per cluster. 46 To account for potential within-county correlation, cluster-robust standard errors were estimated at the county level. The unadjusted logistic regression model was clustered by county and only region was included as a covariate. The adjusted model clustered by county and included 9 individual-level covariates: age, household income, education, race, marital status, employment status, insurance status, chronic disease status, and region. Then, interactions were computed for race, education, and age.
Results
Participant Characteristics
Participant Characteristics (n = 986)
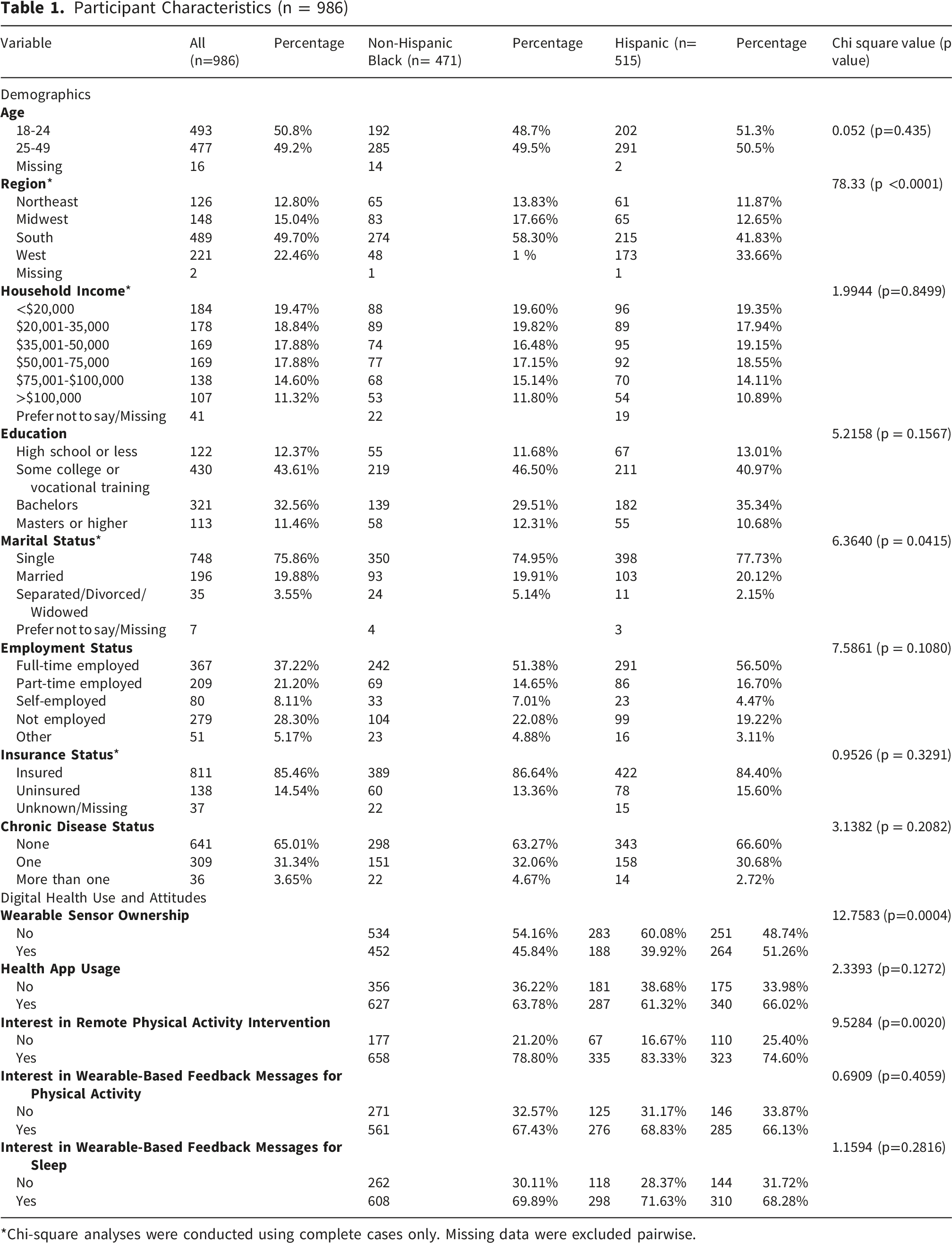
*Chi-square analyses were conducted using complete cases only. Missing data were excluded pairwise.
Digital Health Use and Attitudes
Most respondents reported that they would be interested in a remotely delivered physical activity intervention (78.7%). As detailed in Table 1, More Black women reported being interested in a remote intervention for physical activity compared to Hispanic women (χ2 = 9.5284, p = 0.0020). Most respondents also reported that they would be interested in wearable sensor-based feedback messages for physical activity (67.3%) and for sleep (69.8%). Many participants reported using health-related apps (63.8%), but less than half reported owning a wearable sensor (45.9%). Hispanic women were more likely to own a wearable sensor than Black women (χ2 = 12.7583, p = 0.0004).
Neighborhood Characteristics
For neighborhood characteristics related to socioeconomic status, the mean Gini index was 0.426, estimating a mean percent inequality of household income of 42.6% (SD±0.075, ranging from 0.26-0.79). Almost one-third (31.6%) of neighborhoods were classified as high socioeconomic risk, 22.0% as moderate to high socioeconomic risk, 24.5% as low to moderate socioeconomic risk, and 21.9% as low socioeconomic risk. Over half (60.45%) of neighborhoods had a median household income of ≤ $70,000.
For neighborhood characteristics related racial structures, the mean racial diversity index was 43.1 (SD±19.7, ranging from 0-80.3) and the mean racial segregation score according to the Theil Index was 0.16 (SD±0.11, ranging from 0.01-0.64).
For characteristics related to health services accessibility, neighborhoods had an average of 73.6% of adults reporting having a personal doctor (SD±7.7, ranging from 52.1-90.6). The mean rate of physician’s offices per 100,000 people was 71.1 (SD±26.4, ranged 6.6-185.6), and mean rate of fitness and recreational sport centers per 100,000 people was 12.4 (SD±4.8, ranging from 3.1-35.6). The average Index of Medical Underservice (IMU) score was 55.8 (SD±5.8, ranging from 34.0-91.9). About half (50.3%) of participants spent > $900 a year on out-of-pocket medical expenses.
Main Effects
Odds Ratios for Wearable Ownership
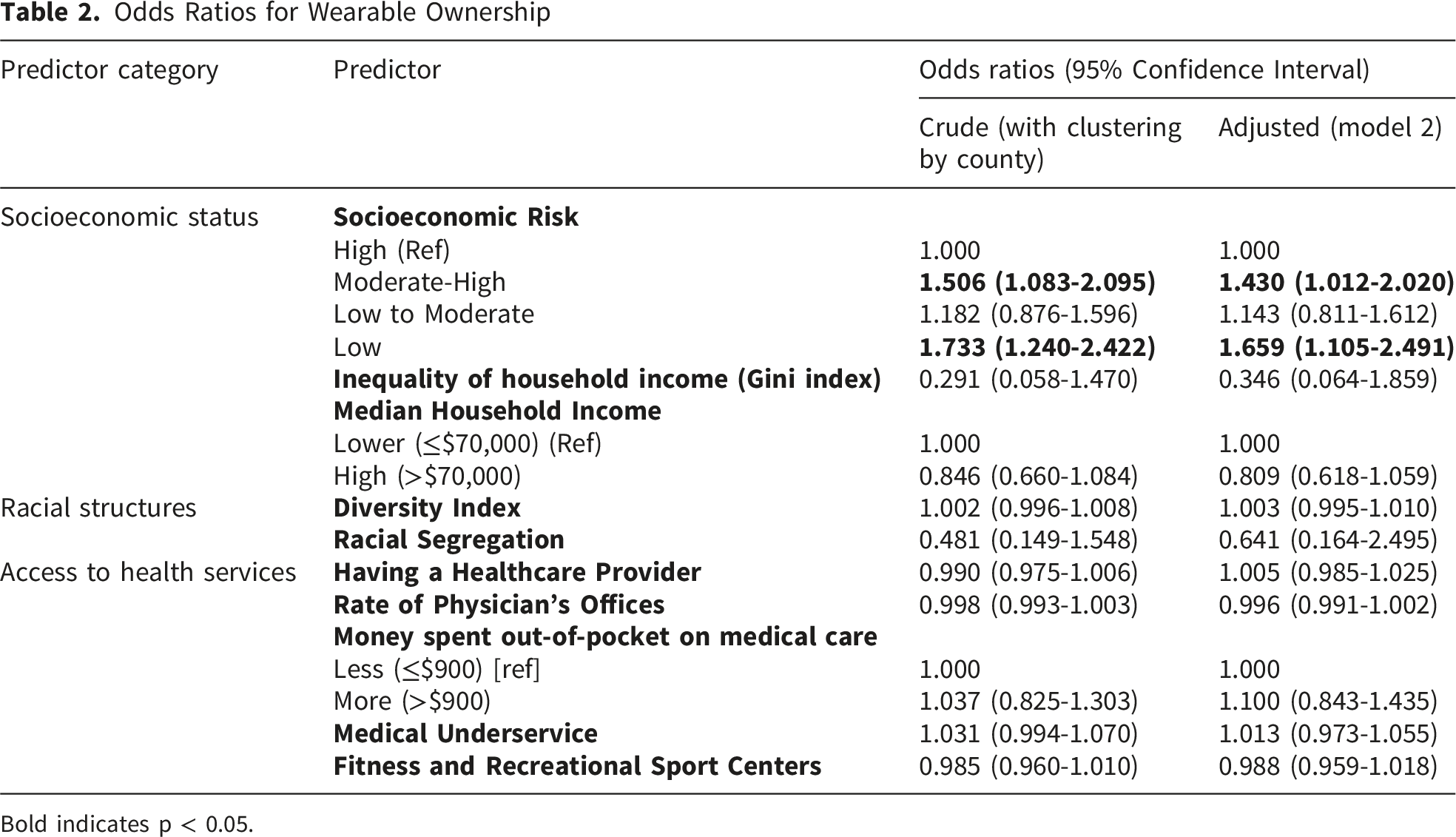
Bold indicates p < 0.05.
Odds Ratios for Health App Usage

Bold indicates p < 0.05.
Odds Ratios for Interest in Remotely Delivered Physical Activity Intervention

Bold indicates p < 0.05.
Interest in Wearable Sensor-Based Physical Activity Feedback Messages
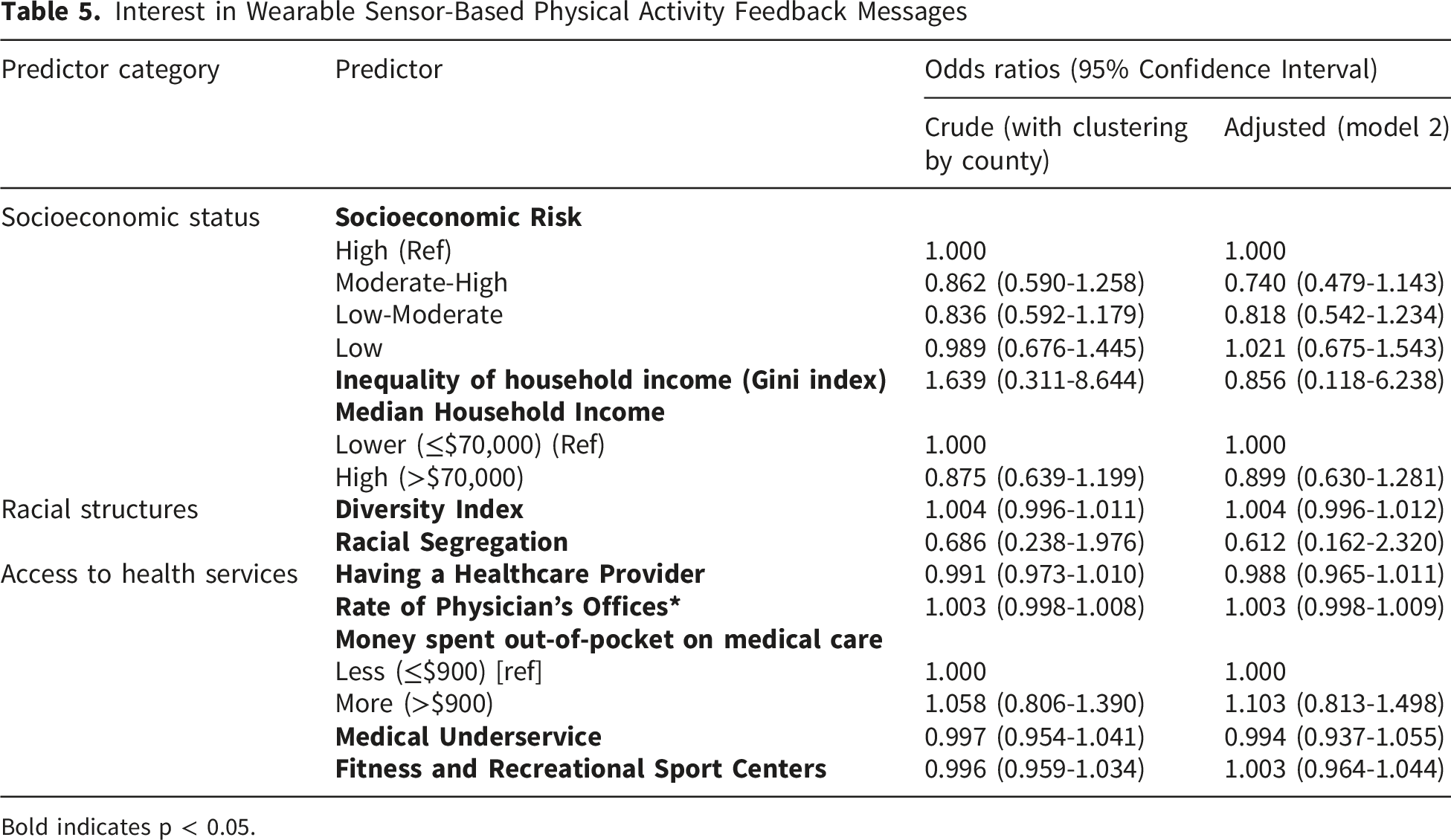
Bold indicates p < 0.05.
Interest in Wearable Sensor-Based Sleep Feedback Messages
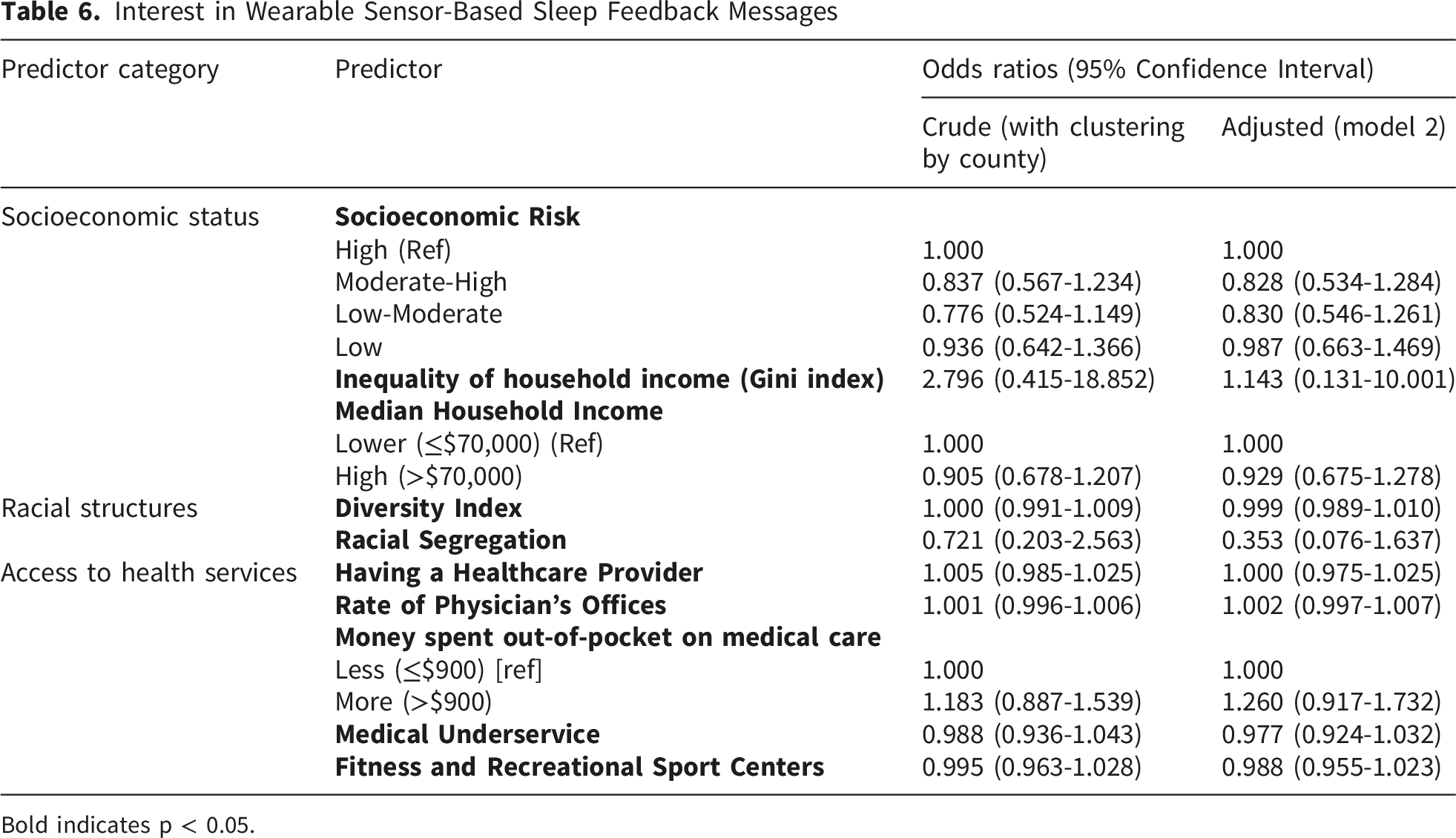
Bold indicates p < 0.05.
Moderating Effects
Among Black and Hispanic women, interest in digital health interventions for sleep and physical activity was influenced by several variables related to access to health services and racial structures across different individual demographic moderators (race, education, age), as detailed below.
Racial Structures
In neighborhoods with lower racial diversity, Black women were more likely to be interested in sleep feedback messages, while Hispanic women were less likely to be interested in sleep feedback messages (Supplemental Figure 1, Racial Diversity x Race beta = 0.00895, SE = 0.00422, p = 0.0361). Furthermore, in neighborhoods with lower racial diversity, Black and Hispanic women aged 18-24 were less likely to be interested in a remote physical activity intervention, while Black and Hispanic women aged 25-49 were more likely to be interested in a remote physical activity intervention (Supplemental Figure 2, Racial Diversity x Age beta = -0.0149, SE = 0.00479, p = 0.0024).
In neighborhoods with greater racial segregation, Black and Hispanic women aged 18-24 were less likely to be interested in physical activity feedback messages, while Black and Hispanic women aged 25-49 were more likely to be interested in physical activity feedback messages (Supplemental Figure 3, Racial Segregation x Age beta = 1.1169, SE = 0.5447, p = 0.0425).
Access to Health Services
In neighborhoods with greater medical underservice scores, Black women were more likely to use a health app, while Hispanic women were less likely to use a health app (Supplemental Figure 4, Medical Underservice x Race beta = -0.0558, SE = 0.0225, p = 0.0148). Furthermore, in neighborhoods with greater medical underservice scores, Black and Hispanic women aged 18-24 were less likely to be interested in physical activity feedback messages, while Black and Hispanic women aged 25-49 were more likely to be interested in physical activity feedback messages (Supplemental Figure 5, Medical Underservice x Age beta = 0.0619, SE = 0.0299, p = 0.0413).
In neighborhoods where average annual dollars spent out-of-pocket on medical expenses ≥ $900, Black and Hispanic women aged 18-24 were less likely to be interested in a remote physical activity intervention, while Black and Hispanic women aged 25-49 were more likely to be interested in a remote physical activity intervention (Supplemental Figure 6, Out-of-Pocket Medical Expenses x Age beta = 0.1788, SE = 0.0798, p = 0.0270).
In neighborhoods with more fitness and recreation centers per 100,000 people, Black and Hispanic women with lower education (less than Bachelors) were more likely to be interested in a remote physical activity intervention, and Black and Hispanic women with higher education (Bachelors or higher) were less likely to be interested in a remote physical activity intervention (Supplemental Figure 7, Fitness and Recreation x Education beta = 0.0542, SE = 0.0198, p = 0.0073).
In neighborhoods with fewer physician offices per 100,000 people, Black and Hispanic women with higher education (Bachelors or higher) were less likely to be interested wearable-based feedback messages for sleep and physical activity, while Black and Hispanic women with lower education (less than Bachelors) were more likely to be interested in both wearable-based feedback messages for sleep (Supplemental Figure 8, Physician Office x Education beta = 0.00583, SE = 0.00282, p = 0.0408) and physical activity (Supplemental Figure 9, Physician Office x Education beta = 0.00535, SE = 0.00263, p = 0.0445).
Discussion
This study examined whether neighborhood characteristics, including socioeconomic status, racial composition, and access to healthcare services, influence digital health use and attitudes among Black and Hispanic women, with implications for cancer prevention through modifiable behaviors such as physical activity and sleep. Because digital health tools can support improvements in 24-hour movement behaviors associated with reduced cancer risk, understanding how neighborhood context shapes digital health engagement is critical for designing equitable cancer prevention interventions. These findings align with socioecological and health equity frameworks, suggesting that neighborhood-level social determinants influence digital health engagement and subsequent opportunities for cancer prevention. In this study, neighborhood socioeconomic risk was associated with wearable device ownership, while multiple indicators of healthcare access were associated with health app usage. Additionally, individual-level factors such as race, education, and age moderated the effects of neighborhood racial composition and healthcare access on interest in digital interventions for physical activity and sleep.
Socioeconomic Risk
Current literature suggests that individuals with higher education, greater income, and full-time employment are more likely to own a wearable device.47-49 However, a person’s individual socioeconomic status may not necessarily align with that of their neighborhood. The present study findings suggest that neighborhood socioeconomic risk predicts current wearable ownership after adjusting for individual education, income, and employment. This has several implications for future digital interventions for cancer prevention tailored to Black and Hispanic women that utilize wearable sensors. First, among current owners of wearables, 50% are willing to share and 32% would consider sharing wearable-derived data for research purposes. 48 However, interventions that require prior wearable ownership may inadvertently exclude women living in neighborhoods with higher socioeconomic risk, where ownership is less common. Thus, researchers should carefully consider how neighborhood-level socioeconomic conditions shape both access to and use of wearable technologies when designing and recruiting for such interventions. While this study’s findings suggest that wearable ownership is less likely for Black and Hispanic women living in neighborhoods with high socioeconomic risk, there remains an interest and willingness to use wearable health tools in Black and Hispanic communities. Future digital interventions for cancer prevention may consider providing wearable sensors or seeking alternative ways for engagement. However, other non-quantifiable factors may also impact wearable ownership. Additional explorations, including qualitative, should seek to understand what Black and Hispanic women desire from wearable-based interventions involving physical and sleep for cancer prevention. 50,51
There was no significant difference in wearable device ownership between women residing in neighborhoods with low to moderate socioeconomic risk and women residing in neighborhoods with high socioeconomic risk. Pair-wise analysis shows that the difference was between the following groups: low risk vs. high risk, low risk vs. low to moderate risk, and moderate to high risk vs. high risk. This may be due to lack of specificity in which of the four different factors used to calculate socioeconomic risk most influences wearable ownership (i.e., population below the federal poverty level, unemployed population, per capita income, and population with no high school diploma). As a composite measurement, it is possible that one or more of these factors heavily influenced this outcome but in different directions. Therefore, in a low to moderate socioeconomic risk category, various combinations of the four factors at different magnitudes are possible. While composite measures for neighborhood-level socioeconomic characteristics are recommended over single indicators to fully characterize a neighborhood, 52 future studies may extract these factors individually to gain a clearer understanding of the relationship between specific neighborhood socioeconomic risk factors of interest and wearable ownership. This can further inform relevant content and implementation strategies for place-based digital interventions for cancer prevention in Black and Hispanic women that utilize wearable devices.
Racial Structures
Black and Hispanic women living in neighborhoods with lower racial diversity and greater racial segregation show greater interest in remote, wearable-based physical activity interventions, likely because these neighborhoods may offer fewer physical, social, and healthcare resources that support physical activity and health engagement.
For example, segregation of racial and ethnic minority populations have been found to be associated with fewer health-related facilities, including physical fitness facilities, health care resources, and social service organizations. 53 Reduced access to these resources undermines cancer prevention efforts in these populations, and should be a critical consideration when designing digital physical activity interventions for cancer prevention in Black and Hispanic women. Racial diversity and segregation in a neighborhood may also influence health behaviors and attitudes. For example, low rates of medical service utilization (e.g., office-based physician visits, visits to nurses and physician’s assistants, and visits to other health professionals) was observed in individuals living in predominantly Hispanic zip codes. 54 Furthermore, in neighborhoods with less racial diversity, Black and Hispanic women may feel a reduced sense of belonging, 55 which may contribute to perceptions of reduced social cohesion and consequently psychological distress. 56 Altogether, future physical-activity-based, cancer-prevention digital interventions for Black and Hispanic women should be tailored to the community’s available resources for physical activity and current utilization of health resources. Interventions may also consider incorporating virtual strategies that foster social connection and cultural belonging, such as peer support networks. 57 However, successful virtual social connection may be limited by trust and familiarity, so this trust should be established by the research team early, both amongst community members and the research team.
Access to Health Services
Health App Usage
The rise in digital monitoring and electronic patient portals 58 may explain why greater out-of-pocket medical expenses and having personal doctors in a neighborhood increase likelihood of using a health app in Black and Hispanic women. For example, greater out-of-pocket medical expenses may signify a chronic condition or a high-deductible insurance plan, 59 and such chronic conditions may require monitoring that potentially uses a health app. 60 Alternatively, individuals with greater out-of-pocket expenses due to lack of insurance or a high-deductible insurance may be more willing to use health apps to self-monitor their health due to limited opportunities to see a healthcare provider. 61 While Black and Hispanic women residing neighborhoods with greater out-of-pocket expenses and greater personal doctors may be willing to engage in digital interventions with health apps, another important factor to consider is data usage and internet availability. Limited data usage and internet availability in low-income communities poses a significant barrier to engaging in digital interventions. 62 Consequently, Black and Hispanic women affected by limited data or internet may be less likely to engage in digital interventions for cancer prevention. Future studies should investigate how cancer-prevention digital interventions can best serve these communities, with a health app or other modalities, while accounting for neighborhood context, data usage, and internet availability.
Furthermore, considerations for digital interventions should be made for the medical underservice of neighborhoods. In neighborhoods with greater medical underservice scores, Black women were more likely to use a health app, and Hispanic women were less likely to use a health app. This contrasts with an existing study that found that Hispanic adults, in general, were more likely to use health apps. 63 However, this study did not consider how neighborhood medical underservice could influence health app usage. This lower likelihood of using a health app as medical underservice increases may be due to health apps not being offered in the Spanish language, lack of a health provider’s guidance or recommendation on using these apps, or cultural preferences of using a health app. Future research can investigate more about the reduced engagement in health apps in Hispanic women especially in medically underserviced areas. For future cancer-prevention digital interventions that plan to utilize a health app, there are several takeaways. This finding highlights the need to consider access to medical services within a participant’s neighborhood during the recruitment and design of the digital intervention. For example, future digital interventions can benefit from understanding that for Black women, medical underservice may not be a barrier for current usage of health apps. Instead, there may be other factors that contribute to willingness and ability to engage in digital interventions, such as internet and data availability as mentioned previously. On the other hand, this finding also presents an opportunity to explore strategies to increase interest, awareness, or education about digital interventions for cancer prevention that utilize health apps among Hispanic women living in neighborhoods with lower medical underservice.
Interest in Remotely Delivered Physical Activity Interventions
There may be greater interest in remotely delivered physical activity interventions in Black and Hispanic women residing in neighborhoods with less access to fitness and recreation, higher medical underservice, and less physician offices due to the lack of health services where they reside, 64 caretaking responsibilities, or lack of social support that present barriers to participating in in-person physical activity interventions. 65 However, this increased interest in a remote health intervention contrasts with previous findings where people with lower access to medical services and less education are less likely to participate in telehealth services, 66 even after the rise in digital medical services since COVID-19. 67 One explanation for this discrepancy is that health technologies used for clinical care may be perceived differently than those used for remote interventions for physical activity and sleep. 68 This may also explain why Black and Hispanic women with less education and living in areas with less physician’s offices were less interested in wearable-based feedback messages for physical activity and sleep. Aligned with existing literature, Black and Hispanic women with limited access to health services and less education may be more wary of the use of technology for health care. In this case, messages based on biological data from wearable devices may be closer in concept to health care services than a remote physical activity intervention.
This presents an important distinction between wearable-based feedback messages and remotely delivered physical activity interventions. Future digital interventions for Black and Hispanic women targeting physical activity and sleep for cancer prevention should be designed with user receptivity in mind. While remotely delivered physical activity interventions have promising engagement from this population, researchers should be conscious of the hesitancy towards wearable-based biological feedback messages. To enhance acceptability and impact, future qualitative studies should investigate the perceptions, needs, and goals of Black and Hispanic women in physical activity and sleep feedback and monitoring to design relevant wearable-based feedback messages in future digital interventions for cancer prevention. Digital cancer prevention interventions for this population involving wearable-based feedback messages should also consider transforming technical jargon (e.g., EMAs, assessments) into more approachable terms (e.g., activity calls, interviews), or using less clinical titles for medical providers (e.g., coaches) may enhance receptivity. 57
Strengths
This study contributes a novel perspective by integrating neighborhood-level social determinants of health with individual-level factors to examine digital health use and attitudes among Black and Hispanic women. By leveraging geocoded data and GIS mapping, the study moves beyond individual predictors to reveal how neighborhood characteristics shape wearable ownership, app usage, and interest in digital interventions for physical activity and sleep
The use of comprehensive neighborhood-level information through GIS and the exploration of these variables with person-level characteristics provides a comprehensive approach to understanding how social determinants of health at multiple levels influence digital health use and attitudes in Black and Hispanic women. This study provides insightful information on how neighborhood characteristics may be considered in the design and implementation of digital health interventions targeting physical activity and sleep for cancer prevention. Another strength of this study includes a specified population of interest for tailoring digital interventions for physical activity and sleep: Black and Hispanic women at reproductive age who are mostly insufficiently active and may not be achieving optimal sleep duration and quality. This also included Spanish-speaking Hispanic women through the offering of a Spanish survey. Finally, exploring the moderating effects of age, race, and education aided in understanding more nuanced relationships in how neighborhood-level characteristics influence digital health use and attitudes.
Limitations
Due to the cross-sectional design of the study, temporality is limited, and no causation can be assumed. In addition, geolocation was used as a proxy to identify a person’s neighborhood instead of directly asking for their home address. It is possible that the geolocation captured was a place of work, living, or other area. It also does not account for the tenure of that person’s home or workplace. However, social determinants of health include where people live, work, and spend their time, and such geolocations gathered still would have captured a place where they were physically present. Future studies may investigate the length of time within a work or living environment to assess its influence on digital health usage and attitudes. Sole online recruiting through Prolific Academic may mostly capture digitally literate Black and Hispanic individuals. The sample may not be representative due to the higher education level compared to the general population of Black and Hispanic women in the US. Considering these limitations, future studies should employ community-based, in-person recruitment methods to capture a broader audience. Furthermore, data were collected during the COVID-19 pandemic, which may have influenced perceptions and adoption of digital health technologies. The two data collection periods were conducted approximately one and a half years apart, reflecting separate recruitment phases for Black and Hispanic participants. This temporal separation and pandemic context may limit generalizability, and findings should be interpreted with caution. Despite these limitations, the study provides important insights into how neighborhood-level social determinants may influence digital health engagement and opportunities for cancer prevention among Black and Hispanic women.
Conclusions
This study’s findings highlight critical considerations for the design of digital health interventions for physical activity and sleep for cancer prevention among Black and Hispanic women. Residing in neighborhoods with higher socioeconomic risk was associated with a lower likelihood of wearable ownership, indicating that interventions that require participant-owned devices may inadvertently exclude women living in neighborhoods with greater socioeconomic risk. Therefore, digital interventions should avoid assuming wearable access and instead consider device provisioning or alternative engagement strategies. At the neighborhood level, greater annual out-of-pocket medical expenses and higher prevalence of having a personal doctor were associated with increased use of health apps, suggesting that connections to healthcare systems and routine medical engagement may facilitate digital health adoption. Intervention developers should therefore consider integrating digital health tools within trusted clinical or community-based healthcare settings to support uptake and sustained use, with consideration of internet and data availability within their community of interest. Finally, the interaction of education, age, and race with neighborhood socioeconomic conditions, racial structures, and healthcare access underscores that digital health use and intervention interest are shaped by intersecting individual and contextual factors. As a result, digital health interventions for physical activity and sleep in the context of cancer prevention should be tailored not only to individual characteristics but also to neighborhood-level conditions, including access to healthcare and structural inequities.
Supplemental Material
Supplemental material - Neighborhood Characteristics and Digital Health Use and Attitudes in Black and Hispanic Women: Insights for Physical Activity and Sleep Interventions for Cancer Prevention
Supplemental material for Neighborhood Characteristics and Digital Health Use and Attitudes in Black and Hispanic Women: Insights for Physical Activity and Sleep Interventions for Cancer Prevention by Anita On, Feinuo Sun, Najmeh Ghalamsiah, Grace E. Brannon, Christine Spadola, Kyrah Brown, Gabriela Wilson, and Yue Liao in Cancer Control.
Footnotes
Acknowledgments
The authors would like to thank Jocelyn Moza and Hannah Affleck from the University of Texas at Arlington for their help with data processing, and Karen Black from the University of Texas at Arlington for translating research materials into Spanish.
Ethical Considerations
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of the University of Texas at Arlington (Protocol # 2021-0207) in February 2021.
Consent to Participate
Informed consent was obtained from all subjects involved in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Research Enhancement Program at University of Texas at Arlington (PI: Liao).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.