
Abstract
Introduction
Human papillomavirus type 16 (HPV16) E6 antibodies may be an early biomarker of anal cancer. We cross-sectionally evaluated when in the course of anal disease, HPV16 antibodies are induced.
Methods
A nested case-control study of 846 men who have sex with men (MSM) was conducted within a prospective study of men with and without HIV. Cases of anal HPV16 (N=262), biopsy-confirmed high-grade squamous intraepithelial lesion (HSIL;N=140), and anal cancer (N=21) were individually matched to controls (N=423) on HIV status, study-participation duration, and age. Serum samples closest to diagnosis underwent HPV serologic testing; prediagnostic serial samples were tested for anal cancers only. Conditional logistic regression was used to calculate odds ratios (OR) and 95% confidence intervals (CIs).
Results
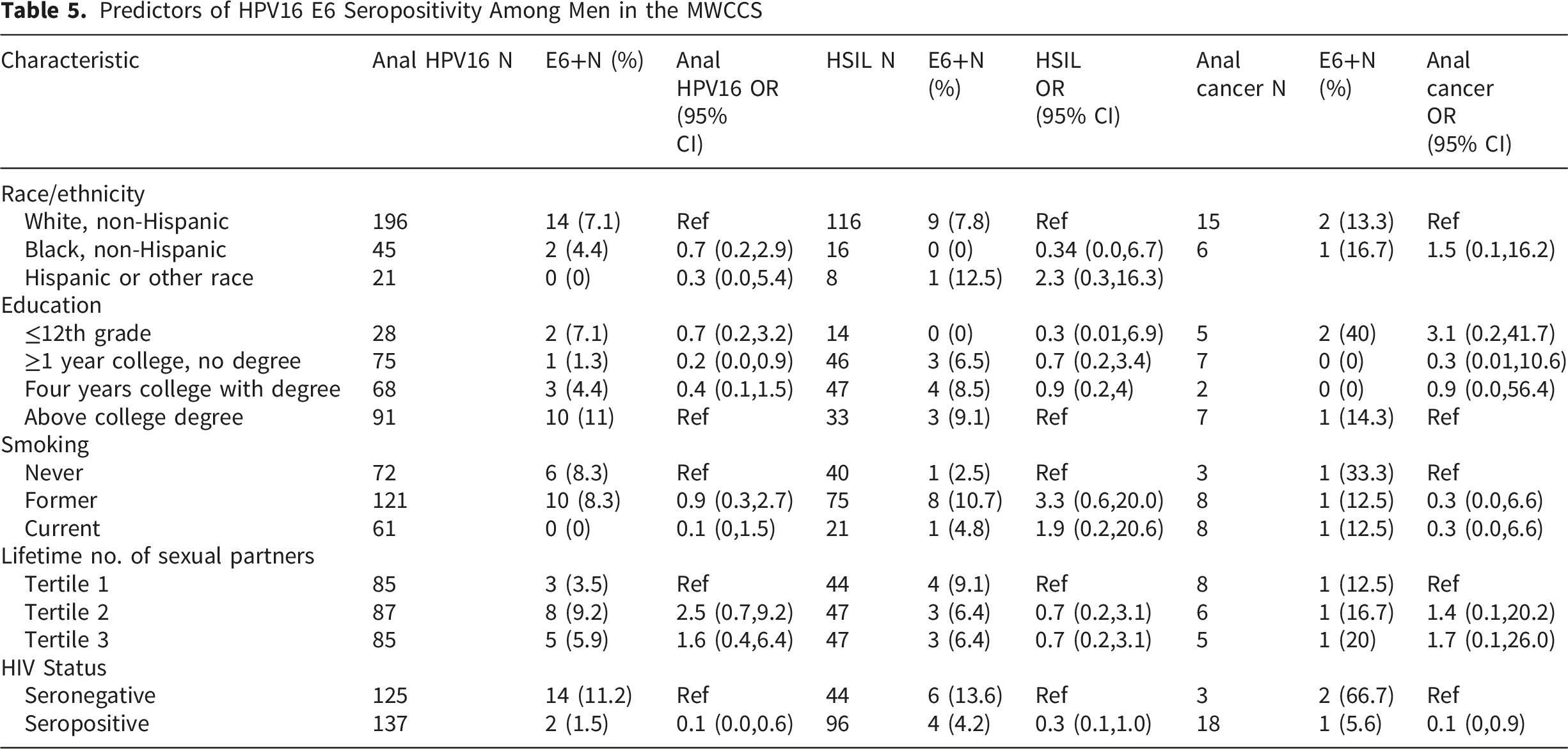
HPV16 E6 seroprevalence was non-significantly elevated in anal disease: OR:1.6 (95%CI:0.7-3.6) for HPV16 infection; OR:1.4 (95%CI:0.5-3.8) for HSIL; and OR:1.5 (95%CI:0.3-9.0) for anal cancer. HPV16 E6 seroprevalence was dramatically lower among men with versus without HIV with the same disease stage: 1.5% vs. 11.2% (P<0.001) for anal HPV16 infection; 4.2% vs. 13.6% (P=0.043) for HSIL; and 5.6% vs. 66.7% (P=0.005) for anal cancer. HPV16 E6 seroprevalence was only associated with anal HPV16 among men without HIV (OR:2.9 [95%CI:1.0-8.0]); no significant associations between HPV16 E6 seroprevalence and anal disease were observed among men with HIV. Among the 21 anal cancers, 66.7% (2/3) without HIV and 5.6% (1/18) with HIV were HPV16 E6 seropositive before diagnosis.
Conclusions
HPV16 E6 antibodies show poor sensitivity for anal cancer and its precursors, particularly among men with HIV.
Introduction
Although rare, the incidence of anal cancer has been steadily increasing worldwide.1,2 The vast majority of anal cancers (∼85%) are caused by persistent human papillomavirus (HPV) infection, in particular HPV type 16 (HPV16), which is responsible for approximately 80% of all anal cancers.3,4 Individuals infected with human immunodeficiency virus (HIV) are at increased risk for anal cancer. Compared to their similarly aged peers without HIV, people living with HIV (PLWH) have up to a 19 times greater incidence of invasive anal cancer.5-7 Of PLWH, men who have sex with men (MSM) are at even higher risk, with up to a 39 greater incidence of anal cancer.5-7
A recent Phase III clinical trial found that treatment of anal cancer precursor lesions (high-grade squamous intraepithelial lesions [HSIL]) significantly reduced the incidence of anal cancer among PLWH.8,9 Prevalence of HSIL has been reported to be as high as 43% among MSM with HIV, 1 and many HSIL will regress to low-grade anal lesions; one study estimated that approximately 10% of HSIL will progress to anal cancer. 10 Given the increased efficacy of treatment, new anal cancer screening guidelines suggest screening for all MSM living with HIV beginning at age 35 and MSM not with HIV at age 45. 9 Given the high HSIL prevalence and rate of regression of HSIL, additional biomarkers may help to identify which HSILs are most likely to progress to anal cancer.
HPV16 E6 antibodies are a potentially promising early marker of anal cancer. A prospective study conducted with pre-diagnostic serum found that 63% of immunocompetent/general population individuals who developed anal cancer had detectable HPV16 E6 antibodies within 5 years before cancer diagnosis compared to 0.5% of cancer-free controls. 11 Additionally, HPV16 E6 antibodies were detectable up to 5 years before diagnosis, suggesting that this biomarker is likely induced during the precancerous stages of anal disease and may be an early marker of anal cancer.
Yet, few studies have comprehensively characterized when, in the course of anal disease development, HPV16 E6 antibodies are induced. Prior studies evaluating the association between HPV16 E6 seropositivity and anal HSIL were limited by small sample sizes of HPV16 E6 seropositive individuals.12,13 Additionally, only two prior studies investigated the kinetics of the HPV16 E6 seropositivity leading up to anal cancer diagnosis.14,15 One study of 1,013 individuals evaluated HPV16 E6 antibodies, HSIL, and anal cancer within the same population 16 ; however, this has not been well explored within the high-risk, MSM population that would benefit most from these studies. Thus, we conducted a nested case-control study within the Multicenter AIDS Cohort Study [MACS] (now the MACS/WIHS Combined Cohort Study, MWCCS), a prospective study including men with and without HIV with serial blood collection and detailed information on anal HPV infection, anal cytological/histologic abnormalities, and anal cancer. The objective of this study was to cross-sectionally evaluate HPV16 E6 antibody prevalence among men with different stages of HPV disease (i.e., anal HPV infection vs. HSIL vs. anal cancer) to inform when in the course of the anal disease these antibodies are induced. Additionally, among patients who developed anal cancer, we tested serial pre-diagnostic blood samples to evaluate the kinetics of HPV16 E6 seropositivity before diagnosis.
Methods
Study Cohort
Data were analyzed from the MACS, a prospective cohort study of MSM with and without HIV at four US sites (Baltimore, Chicago, Pittsburgh, and Los Angeles), now part of the MACS/WIHS Combined Cohort Study (MWCCS; mwccs.org). Study visits occur every 6 months and include detailed medical history questionnaires, a physical exam, and blood specimen collection. All participants who attended any study visits between June 2010 and July 2011 were eligible to participate in the Anal Health Study (AHS) 17 and were offered free anal cytology and HPV testing. Participants with inadequate cytology results were offered another test at the next study visit. Participants with HIV were offered annual cytology testing (up to 4 cytology tests total), and participants without HIV were offered a second cytology test two years later (total of 2 cytology tests). Additional questionnaires and medical record reviews were conducted to gather information on high-resolution anoscopy (HRA) procedures and the treatment of anal dysplasia that occurred outside the MACS study visits. The AHS was approved by the institutional review boards of each participating site. This study was deemed exempt from review by the University of Kentucky Institutional Review Board (9/15/2022) because it utilized de-identified specimens, and investigators had no access to identifiable information. The reporting for this study conforms to the STROBE guidelines. 18
Study Design
This was a matched case-control study stratified by three mutually exclusive case groups: 1) prevalent anal HPV16 infection, 2) anal HSIL, or 3) anal cancer. No sample size calculations were conducted. Instead, all available cases with the appropriate number of matched controls were selected for testing. Thirty-seven cases were excluded due to the inability to identify suitable matches, including 19 cases with prevalent anal HPV16, 10 cases with anal HSIL, and 8 cases with anal cancer. Cases of anal HPV16 infection were identified within the AHS substudy population only (as only this subpopulation had anal HPV ascertainment). For this analysis, cases with anal HPV16 infection only were defined as individuals with at least one detection of anal HPV16 who had no history of HSIL (through HRA or cytology) up to and including the time of anal HPV16 diagnosis. Cases of HSIL were required to be HRA-confirmed or identified by medical record review, as defined by ICD-9 codes 230.5 and 230.6. Anal cancers were identified by medical record review and/or cancer registry matching using the following ICD-O-3 codes: C21.0-C21.2, C21.8, C19.9 (rectosigmoid), and C20.9 (rectum), restricting to histology codes 8050-8076, 8083-8084, 8123-8124 (for squamous cell carcinoma). Each case had the blood specimen collected closest to the time of diagnosis selected for testing. For anal cancer cases only, all available preceding samples collected before diagnosis were also tested for HPV antibodies to explore the timing of seroconversion.
Each of the three case groups was individually matched separately with eligible controls without anal HPV or disease in a 1:1 ratio (sampling was done without replacement), matching for follow-up time, age, and HIV status. Cases and controls were first matched by the following criteria: age (+/- 2 years), study time (+/- 2 years), and HIV status. For cases where no control was identified with those criteria, age and study time criteria were relaxed to (+/- 5 years) and then to (+/- 10 years) to gain additional matches. Controls were selected from among participants in the AHS. Controls were required to be: 1) never diagnosed with a prior history of HPV-related cancer (anal, oropharyngeal, penile), 2) never diagnosed with high-grade cytology/histology (either in the sub-study or per medical records) at AHS baseline, and 3) negative for HPV16 at both AHS baseline and their 2nd AHS visit. Among eligible controls, those with 2 consecutive normal cytology results (1 at the baseline visit and 1 at the visit immediately after baseline) were prioritized for control selection. The blood specimen collected at the visit where the second negative anal HPV16 test was recorded was selected for testing.
Serologic Testing
Multiplex serologic testing was performed at the German Cancer Research Center (Heidelberg, Germany) by staff blinded to the HPV and disease status of the patients.19,20 Antigens were affinity-purified, bacterially expressed fusion proteins with N-terminal Glutathione S-transferase. Samples were analyzed for antibodies against HPV16 L1, E1, E2, E4, E6, and E7. Antibody levels were quantified at 1:100 serum dilution as median fluorescence intensity (MFI) and dichotomized as positive or negative based on previously defined cutpoints.21,22 HPV16 E6 seropositivity was defined as an MFI value of 484 or greater.
Statistical Analyses
Participant characteristics were evaluated by case-control status. The proportion of cases and controls seropositive for HPV16 antibodies was calculated for each case group (HPV16 infection, HSIL, anal cancer) across all HPV16 proteins analyzed (L1, E1, E2, E4, E6, E7). Odds ratios (OR) and 95% confidence intervals (CIs) for the association between HPV16 E6 seropositivity and each case group and for determinants of HPV16 seropositivity were estimated using conditional logistic regression. Variables evaluated in univariate modeling included race/ethnicity, education, smoking, age at first sexual contact, lifetime number of sexual partners, history of anal sex, and HIV status. For anal cancer cases only, HPV16 E6 MFI values for each serial sample were plotted on a semi-log scale to evaluate HPV16 E6 kinetics before diagnosis. All analyses were performed using SAS version 9.4.
Results
Participant Characteristics
Characteristics of Study Population by Case Control Status (MWCCS)
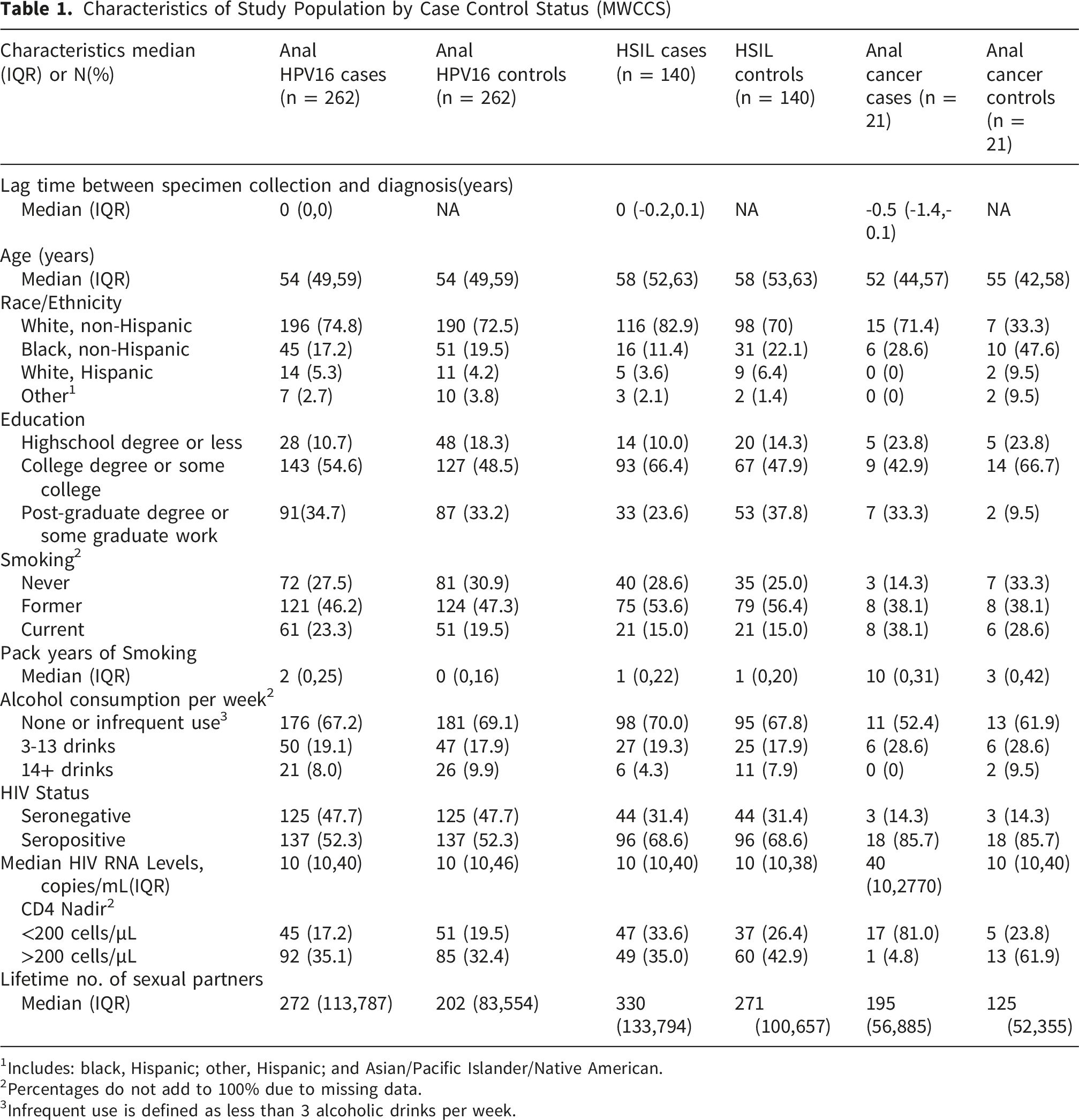
1Includes: black, Hispanic; other, Hispanic; and Asian/Pacific Islander/Native American.
2Percentages do not add to 100% due to missing data.
3Infrequent use is defined as less than 3 alcoholic drinks per week.
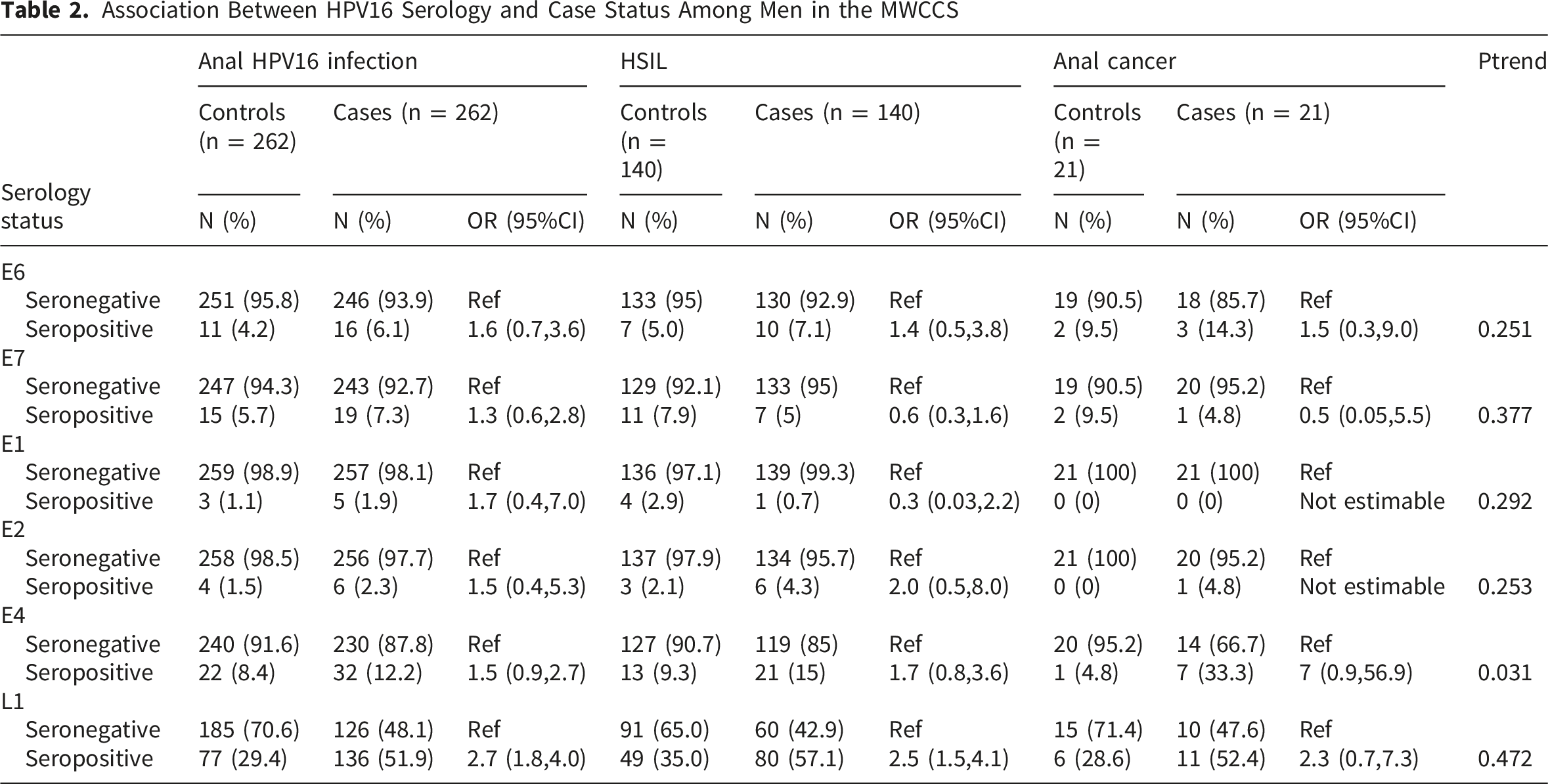
HPV Seropositivity by Increasing Severity of Anal Disease
Association Between HPV16 Serology and Case Status Among Men in the MWCCS
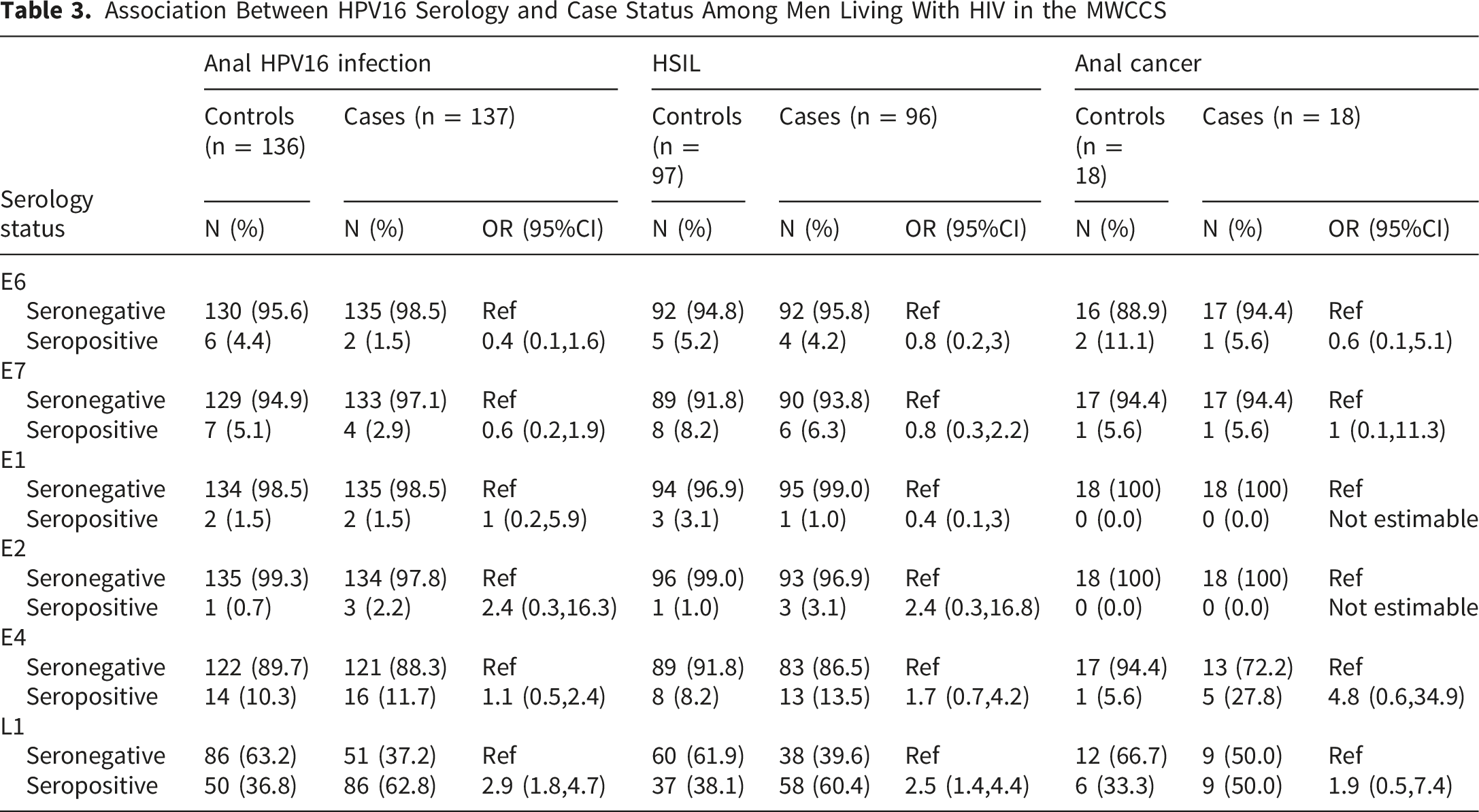
Association Between HPV16 Serology and Case Status Among Men Living With HIV in the MWCCS
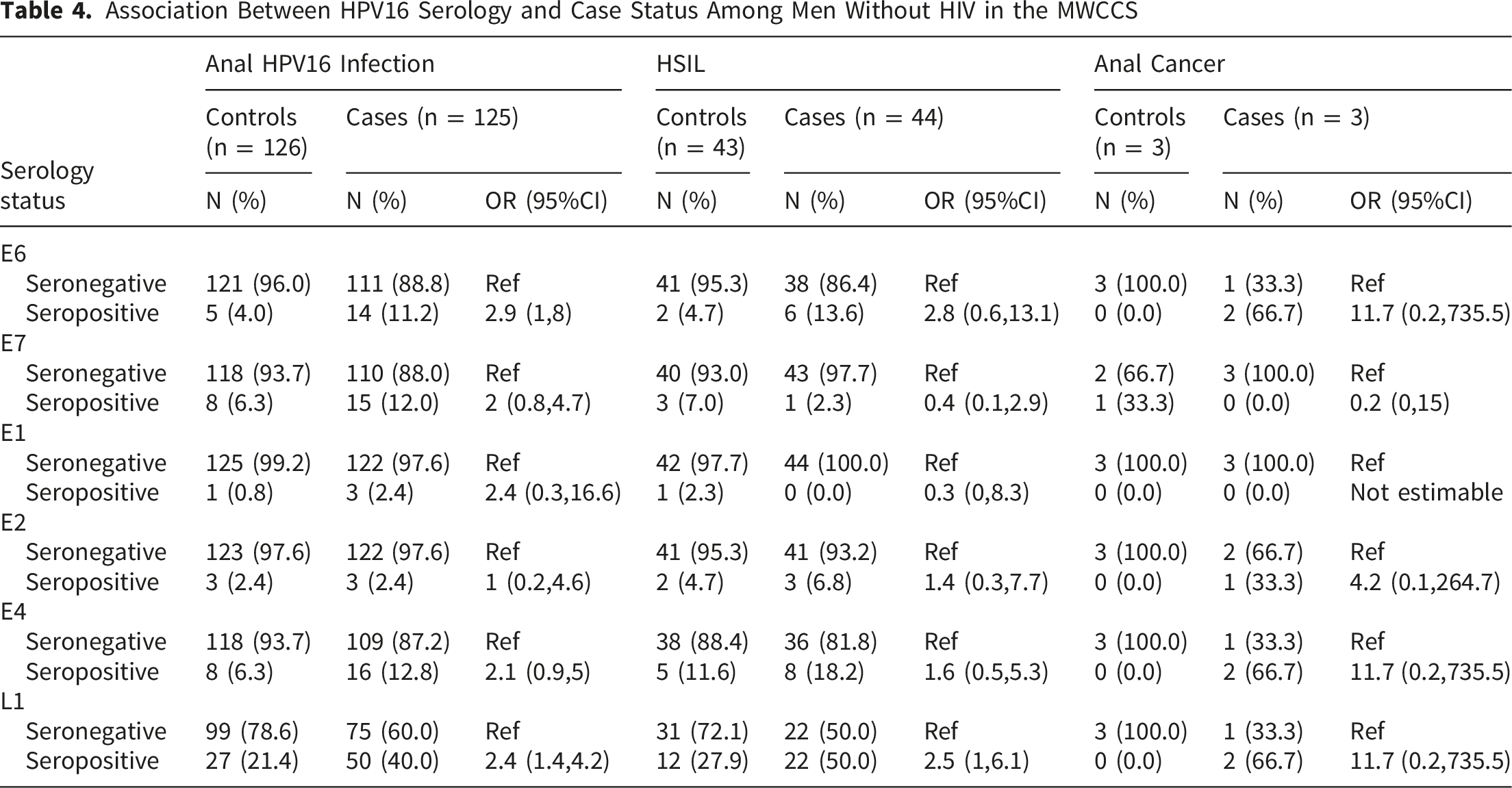
Association Between HPV16 Serology and Case Status Among Men Without HIV in the MWCCS
Predictors of HPV16 E6 Seropositivity Among Cases
Predictors of HPV16 E6 Seropositivity Among Men in the MWCCS
Kinetics of HPV16 E6 Seropositivity Before Anal Cancer Diagnosis
All serial blood samples collected from anal cancer cases before diagnosis were evaluated for HPV16 E6 antibodies (Figure 1). Among 18 anal cancer cases living with HIV, 17 were persistently HPV16 E6 seronegative at all visits up to and including serology collected at the closest pre-diagnostic visit (usually <6 months of diagnosis). The one participant with HIV was persistently HPV16 E6 seronegative for approximately 8 years before seroconverting to HPV16 E6 seropositivity just before anal cancer diagnosis. Among three anal cancer cases in men without HIV, two had detectable HPV16 E6 antibodies before anal cancer diagnosis. One of the participants without HIV seroconverted to HPV16 E6 seropositivity approximately 11 years before diagnosis, and the other was persistently HPV16 E6 seropositive from approximately seven years before diagnosis. Kinetics of HPV16 E6 seropositivity prior to anal cancer diagnosis (N=21)
Discussion
This large matched case-control study, nested within the MWCCS, is one of the first studies to evaluate the association of HPV16 E6 seropositivity with anal HPV16 infection, HSIL, and anal cancer endpoints within an MSM population. HPV16 E6 seroprevalence was 4.7% among controls and 6.9% overall among cases. HPV16 E6 seropositivity was not significantly associated with increased odds of anal disease in this study overall, given the low seropositivity among those living with HIV with anal disease in this study. HIV was associated with reduced HPV16 E6 seropositivity in each of the three anal disease stages explored. Of the 18 anal cancer cases that occurred among men with HIV, only 1 was HPV16 E6 seropositive, and seroconversion occurred just prior to diagnosis. In contrast, of the three anal cancer cases that occurred among men without HIV, two were HPV16 E6 seropositive and seroconverted years prior to diagnosis. Of the multiple HPV16 antibodies tested, only HPV16 L1 antibodies were significantly associated with HPV16 infection and HSIL. These results suggest that HPV serology may not be a sensitive marker of anal disease within this population of middle-aged MSM living with HIV.
Considerable interest has focused on HPV16 E6 antibodies due to the ability to detect this marker more than 10 years prior to HPV-driven oropharyngeal cancer diagnosis in several studies.22,23 A limited number of previous studies have evaluated the association between HPV serology and anal HSIL and/or anal cancer,11-16 including some studies that evaluated anal HSIL only,12,13 or anal cancer only,11,14 and some that evaluated both anal HSIL and anal cancer within the same population. 16 Of the studies that evaluated anal HSIL,12,13,16 some were in the general population, 16 and others were among MSM.12,13 Interesting, only the general population study reported a significant association between HSIL and HPV16 E6 antibodies. 16 While both studies within the MSM population noted an increased HPV16 E6 seroprevalence among HSIL cases, neither reached statistical significance.12,13 Similar to our study, these prior studies reported HPV16 E6 seroprevalence ranging from 3% to 4.5% among HSIL cases. Yet, in this study, we found a higher seroprevalence among all controls combined (average 4.7%) than in prior studies (1.3% to 1.4%). Although the exact reason for our elevated HPV16 E6 seroprevalence among controls is unclear, unlike previous studies, we matched cases and controls on follow-up time, age, and HIV status.
A recent meta-analysis of available studies reported that HPV16 E6 seropositivity was associated with a 4-fold increased risk of HSIL and 26-fold increased risk for anal cancer. 24 Of the previous studies that evaluated HPV16 E6 seropositivity and anal cancer,11,14-16 all found significant associations, despite evaluating very different populations, and all reported very similar estimates of HPV16 E6 seroprevalence among anal cancer cases (range: 23.3% to 29.2%). A population-based case-control study in Washington State evaluated 116 anal cancer cases; 29.3% were HPV16 E6 seropositive. 16 The nested study within the European Prospective Investigation into Cancer (EPIC) cohort, which included healthy individuals from 10 European countries, found that 7 out of 24 individuals who later developed anal cancer (29.2%) were HPV16 E6 seropositive at study enrollment. 11 Likewise, a nested study within the Swiss HIV Cohort Study, an ongoing study of people living with HIV/AIDS in Switzerland (Swiss HIV Cohort Study), reported that 20 out of 91 anal cancer cases (23.3%) were HPV16 E6 seropositive within two years of diagnosis. 14 While our study only found 14.3% of anal cancer cases with HPV16 E6 seropositivity, it is important to note that our study only included MSM, most of whom were living with HIV, which may account for the differences in our findings. Of the seven HPV16 E6 seropositive anal cancer cases in the published EPIC study, 11 all were women. Similarly, the Swiss HIV Cohort Study 14 reported that 40% of women with anal cancer were HPV16 E6 seropositive compared to 28.6% of non-MSM men, and seroprevalence was only 17.0% among MSM, which is more in line with our findings. Together, these studies suggest an effect of HIV and possibly of sex at birth on the sensitivity of HPV16 E6 antibodies for anal cancer. As noted in prior studies,12,16 we observed significant associations between L1 seropositivity and anal disease, as well as with E4 antibodies. L1 seropositivity is a marker for past HPV infection; however, seroconversion following an HPV infection does not always occur, and men are less likely to seroconvert than women. 25 However, close to one-third of controls were L1 seropositive; thus, this marker lacked specificity. Taken together, these findings suggest that HPV serology may not be a sensitive marker of anal disease among men living with HIV; yet, due to small numbers, additional studies are needed.
Our study had several strengths and limitations. This study was nested within the MACS cohort – a long-standing prospective study of HIV infection among MSM that had high-quality data regarding anal HPV infection, HSIL, and anal cancer during the time period evaluated, as well as repeated risk factor data collection. This study is also unique in evaluating the association of HPV16 E6 seropositivity with anal HPV infection, HSIL, and anal cancer endpoints within the same population. Additionally, this is one of the first studies to use a matched case/control design to control for potential confounding and, thus, reduced potential bias in our results. Additionally, all cases of HSIL and anal cancer were confirmed by biopsy and chart review. However, we did not have access to the HSIL and anal cancer tissues for HPV genotype testing – over 80% of anal cancers are HPV positive, of which approximately 90% are due to HPV16.4,26 One possible explanation for the low sensitivity of HPV16 E6 antibodies could be the involvement of non-HPV16 types in the anal lesions, particularly among men living with HIV, as some studies have reported a lower proportion of anal cancers attributable to HPV16 in this population. 26 We also cannot rule out the possibility of misdiagnosis (or seropositivity for early-stage undiagnosed oropharyngeal cancer), particularly among the controls, where we observed HPV16 E6 seroprevalences as high as 9.5%. We also cannot rule out misclassification in our case groups. Cytology currently lacks sufficient sensitivity and specificity to reliably predict HSIL; consequently, HSIL may be underdiagnosed. Additionally, although there were over 2000 participants in the anal health study used to sample controls, evaluation of anal cancer associations was limited by small sample sizes. We had limited statistical power to evaluate associations with anal cancer, as our study included only 21 cases of anal cancer, resulting in unstable estimates and wide confidence intervals. Additionally, the AHS only included men, and therefore, we were unable to evaluate possible effect modification by sex. Finally, while our participants were recruited from several locations, our results are not generalizable to the larger United States population.
Conclusion
Taken together, our findings suggest that while HPV16 E6 seroprevalence was higher among MSM without HIV compared with those with HIV, it may not be a sensitive marker of HPV-related anal disease among MSM, despite this population being at the highest risk. 5
Supplemental Material
Supplemental Material - The Association Between Human Papillomavirus Type 16 E6 Seroprevalence and Degrees of Anal Disease Among Men With HIV: A Nested Case Control Study
Supplemental Material for The Association Between Human Papillomavirus Type 16 E6 Seroprevalence and Degrees of Anal Disease Among Men With HIV: A Nested Case Control Study by Krystle A. Lang Kuhs, Christopher Otieno, Staci Sudenga, Tim Waterboer4, Weiqun Tong, Dorothy Wiley, Jay H. Bream, Steven Wolinsky, Jeremy Martinson and Gypsyamber D’Souza in Cancer Control.
Footnotes
Acknowledgments
Grammarly was used for proofreading.
Ethical Considerations
This study was deemed exempt from review by the University of Kentucky Institutional Review Board (9/15/2022) because it utilized de-identified specimens, and investigators had no access to identifiable information.
Author Contributions
Conceptualization: All authors. Data curation: All authors. Formal analysis: All authors. Funding acquisition: KLK. Investigation: All authors. Project administration: KLK, TW, GD. Resources: GD, TW. Supervision: KLK, GD, TW, Validation: KLK, GD, TW, XL. Visualization: KLK, XL. Writing (original draft): KLK, GD. Writing (review & editing): All authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Intramural Research Program of the US National Institutes of Health (National Cancer Institute, Division of Cancer Epidemiology and Genetics). K.A. Lang Kuhs (K07 CA218247) and S.L. Sudenga (K07 CA225404) were also supported by the National Cancer Institute. Data in this manuscript were collected by the Multicenter AIDS Cohort Study (MACS), now the MACS/WIHS Combined Cohort Study (MWCCS). The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). MWCCS (Principal Investigators): Atlanta CRS (Ighovwerha Ofotokun, Anandi Sheth, and Gina Wingood), U01-HL146241; Baltimore CRS (Todd Brown and Joseph Margolick), U01-HL146201; Bronx CRS (Kathryn Anastos, David Hanna, and Anjali Sharma), U01-HL146204; Brooklyn CRS (Deborah Gustafson and Tracey Wilson), U01-HL146202; Data Analysis and Coordination Center (Gypsyamber D’Souza, Stephen Gange and Elizabeth Topper), U01-HL146193; Chicago-Cook County CRS (Mardge Cohen, Audrey French, and Ryan Ross), U01-HL146245; Chicago-Northwestern CRS (Steven Wolinsky, Frank Palella, and Valentina Stosor), U01-HL146240; Northern California CRS (Bradley Aouizerat, Jennifer Price, and Phyllis Tien), U01-HL146242; Los Angeles CRS (Roger Detels and Matthew Mimiaga), U01-HL146333; Metropolitan Washington CRS (Seble Kassaye and Daniel Merenstein), U01-HL146205; Miami CRS (Maria Alcaide, Margaret Fischl, and Deborah Jones), U01-HL146203; Pittsburgh CRS (Jeremy Martinson and Charles Rinaldo), U01-HL146208; UAB-MS CRS (Mirjam-Colette Kempf, James B. Brock, Emily Levitan, and Deborah Konkle-Parker), U01-HL146192; UNC CRS (M. Bradley Drummond and Michelle Floris-Moore), U01-HL146194. The MWCCS is funded primarily by the National Heart, Lung, and Blood Institute (NHLBI), with additional co-funding from the Eunice Kennedy Shriver National Institute Of Child Health & Human Development (NICHD), National Institute On Aging (NIA), National Institute Of Dental & Craniofacial Research (NIDCR), National Institute Of Allergy And Infectious Diseases (NIAID), National Institute Of Neurological Disorders And Stroke (NINDS), National Institute Of Mental Health (NIMH), National Institute On Drug Abuse (NIDA), National Institute Of Nursing Research (NINR), National Cancer Institute (NCI), National Institute on Alcohol Abuse and Alcoholism (NIAAA), National Institute on Deafness and Other Communication Disorders (NIDCD), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institute on Minority Health and Health Disparities (NIMHD), and in coordination and alignment with the research priorities of the National Institutes of Health, Office of AIDS Research (OAR). MWCCS data collection is also supported by UL1-TR000004 (UCSF CTSA), UL1-TR003098 (JHU ICTR), UL1-TR001881 (UCLA CTSI), P30-AI-050409 (Atlanta CFAR), P30-AI-073961 (Miami CFAR), P30-AI-050410 (UNC CFAR), P30-AI-027767 (UAB CFAR), P30-MH-116867 (Miami CHARM), UL1-TR001409 (DC CTSA), KL2-TR001432 (DC CTSA), and TL1-TR001431 (DC CTSA). The authors gratefully acknowledge the contributions of the study participants and the dedication of the staff at the MWCCS sites. We would like to acknowledge the National Program of Cancer Registries of the Centers for Disease Control and Prevention (CDC) for the funds that helped support the collection and availability of the cancer registry data and thank the following state cancer registries for their help: AL, CA, FL, GA, IL, MD, MS, NY, NC, PA, and VA. The authors assume full responsibility for the analyses and interpretations of these data.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TW serves on advisory boards for Merck (MSD) Sharp & Dohme. The other authors have no conflicts of interest to declare.
Data Availability Statement
Access to individual-level data from the MACS/WIHS Combine Cohort Study (MWCSS) may be obtained upon review and approval of a MWCSS concept sheet. Links and instructions for the online concept sheet are on the study website.
Statement of Novelty and Impact
This large matched case-control study, nested within the MWCCS, is one of the first studies to evaluate the association of HPV16 E6 seropositivity with anal HPV16 infection, HSIL, and anal cancer endpoints within an MSM population. Our results suggest that HPV serology may not be a sensitive marker of anal disease within this population of middle aged MSM living with HIV.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.