
Abstract
Introduction
Increasing demand for colonoscopy continues to strain healthcare systems worldwide. Colon capsule endoscopy (CCE) offers a minimally invasive alternative, but its adoption is limited by high re-investigation rates. The aim of this study is to develop and evaluate clinical prediction models for selecting faecal immunochemical test (FIT) positive patients most suitable for CCE versus colonoscopy.
Methods
We conducted a secondary analysis of data from CareForColon2015 randomized controlled trial (2020–2022), including individuals aged 50–74 years with a positive FIT. Logistic regression models were developed to predict CCE transit, bowel cleansing, completeness, and colonoscopy indication. Sixty candidate predictors were assessed, including demographics, lifestyle factors, FIT values, medications, perceived stress, and health literacy. Models were validated using repeated random subsampling and evaluated on a 10% hold-out set using the area under the receiver-operating-characteristic curve (AUC), Cohen’s K, and accuracy. Decision curve analysis (DCA) was performed to assess clinical utility.
Results
CCE achieved complete transit in 92.1% and acceptable bowel cleansing in 71.3% of participants, with 69.6% of investigations deemed complete. Colonoscopy was indicated in 68.0% of cases, based on broad inclusion criteria, and 55.9%, based on more stringent criteria. Models predicting colonoscopy indication showed moderate performance (AUC 0.69–0.71; accuracy 65–67%; Cohen’s K 0.28–0.30). DCA indicated positive net benefit for both models within threshold probabilities of 0.5–0.75, supporting their potential to identify FIT-positive patients unlikely to benefit from immediate colonoscopy.
Conclusions
Clinical prediction models may assist in post-FIT triage between CCE and colonoscopy. DCA suggests potential to reduce unnecessary colonoscopies by identifying low-risk patients suitable for initial CCE. External validation is needed before clinical implementation.
Keywords
Introduction
The growing demand for colonoscopies, driven by an ageing population, increased adoption of screening programs, and a rise in early-onset colorectal cancer (CRC), has placed significant pressure on healthcare systems worldwide. 1 Additionally, uncontrollable factors such as the recent pandemic have further strained already overwhelmed endoscopy units. 2 Colon Capsule Endoscopy (CCE) has emerged as a minimally invasive alternative to traditional colonoscopy, providing a non-invasive option that eliminates the need for sedation and hospital visits. 3 Despite its potential, CCE faces challenges, including a high re-investigation rate caused by incomplete visualisation, which can result from slow transit times, inadequate bowel preparation and positive findings, leading to therapeutic colonoscopy. 4 However, patient preference for CCE is high due to its convenience and comfort.5,6 Research has demonstrated that its polyp detection rate (PDR) is comparable to traditional colonoscopy.7-9
To address the issue of high re-investigation rates following CCE, pre-CCE Artificial Intelligence (AI) tools could help optimize patient selection by predicting successful CCE completion with no pathology identified. Certain factors, such as age, gender, BMI, diet, constipation and comorbidities, can be associated with poor bowel preparation and difficulty detecting pathology during endoscopic examinations.10-13 Some AI-based approaches have been attempted for assessing bowel cleansing quality and interpreting CCE findings, with reported high sensitivity for cleansing assessment and pathology detection. 14 However, to predict the CCE outcome based on patient characteristics has only been tested using regression models to identify predictors associated with pathology or incomplete investigation.15-18 This may help clinicians improve patient selection, but since the predictors’ associations are identified for the population as a whole, we may wrongfully allocate patients to an undesirable investigation, which could possibly have been avoided if we had included the full profile of the patient in predictions of odds of pathology and incomplete CCE. In an attempt to ensure lower re-investigation rates, enhancement of the patient experience, and an optimized resource utilisation within healthcare systems, the aim of this study is to develop algorithms for accurate patient selection according to complete CCE and negative CCE.
Methods
Data Collection
Patient data was retrieved from the CareForColon2015 (CFC2015) trial (ClinicalTrials.gov: NCT04049357).18,19 In CareForColon2015, all citizens of the Southern Denmark Region, who participated in the National Colorectal Cancer Screening program were randomised between the standard screening protocol (FIT followed by colonoscopy), and an intervention arm giving them the free choice between CCE and colonoscopy following positive FIT. 19 The study design is a secondary analysis of data from this randomized controlled trial (2020–2022). The individuals who chose to undergo CCE in the intervention arm make up the cohort included in the present analyses. All participants provided informed consent. A user board of former colorectal cancer patients contributed to the design of the study by reviewing and commenting on the protocol prior to ethical approval.
Individuals included in this study are all FIT positive screening participants aged 50-74 from the Region of Southern Denmark (N=2031). The trial tested CCE in a FIT positive population with awareness that the pathology rate, and thereby re-investigation rate, would likely be higher than preferred for CCE. This ensured sufficient statistical power to compare the rate of pathology between the trial arms. The CCE sensitivity to advanced neoplasia is directly transferrable to lower risk populations as long as the outcome targeted remains the same. 18 Even in this FIT positive population with increased risk of advanced neoplasia, three in four individuals did not have advanced neoplasia, making it useful to a large proportion of this population to predict who would benefit from CCE and who should go directly to colonoscopy.
The bowel preparation regimen was standardized across all centres and participants, and capsule instruction and delivery were performed by the same four nurses throughout the region. Participants received polyethylene glycol (PEG)-based bowel preparation beginning three days prior to capsule ingestion, followed by PEG with ascorbic acid on the evening before and morning of CCE. Sulphate-based booster solutions were administered according to capsule transit signals, and bisacodyl suppositories were used if capsule excretion had not occurred after the fourth signal. Prucalopride (2 mg, administered 45–60 minutes before capsule ingestion) was introduced after the initial 681 participants, as part of the otherwise standardized bowel preparation regimen.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki of 1975, as revised in 2024. The study was approved by the relevant ethics committee (ref. S-20190100, 7-Feb-2020) and the Danish data protection agency (ref. 19/29858). All participants provided informed consent. The reporting of this study conforms to the TRIPOD + AI statement. 19 All patient details have been de-identified.
Statistical Analysis
The following self-reported background data was collected on each patient: Demographics (age, sex, marital status, educational level, income, country of birth and culture growing up); physique (height and weight); lifestyle habits (time they woke up, smoking habits, coffee consumption, sleep hours and pattern, and physical activity); gastrointestinal (GI) tract transit and stools (constipation, use of laxatives, and score on the Bristol stool scale); use of medications and drugs (painkillers, anti-depressants, mental illness medication and illicit drugs); self-perceived stress level (10 validated questions20,21), health literacy (HLQ; 10 validated questions22,23); and prior screening (previous stool test, previous colonoscopy); and well as laboratory FIT results, (ng Hb/mL buffer). This yielded 60 potential predictor variables (supplemental information Table A1). The prediction models were developed to support pre-selection of FIT-positive patients for CCE versus colonoscopy using information available at the time of referral. Therefore, factors occurring after CCE allocation, such as bowel preparation adherence, timing of booster administration, and other procedure-related variables, were not included as candidate predictors.
An external partner (Corporate Health International, Hamburg, Germany) provided blinded CCE reporting by experienced CCE readers. All CCE reports were checked, corrected, and approved by a small group of physicians with extensive experience in gastroenterology and endoscopy from the external private contractor. Information from the CCE investigations was converted into the following five CCE outcomes of interest for use as output variables in the predictive models: • Transit: The outcome variable “Transit” refers to whether a complete colonic transit of the capsule was confirmed. • Bowel Cleansing: Evaluated based on Leighton-Rex grade, the bowel cleansing outcome variable had two levels: “Acceptable”, when cleansing in all 5 colon segments (cecum, right-sided colon, transverse, left-sided colon, and rectum) was assessed as “fair”, “good” or “excellent”; and “Not acceptable”, when cleansing in at least one segment was assessed as “poor”. • Completeness: A CCE investigation was considered “completed” when three conditions were fulfilled: 1. Complete transit was confirmed; 2. Bowel cleansing was acceptable; and 3. The quality of the CCE investigation was assessed as acceptable (that is, “with short interruptions”, “ok”, or “N/A”), as opposed to being assessed as “Unusable”. • Colonoscopy indication based on CCE findings using broad (weak) criteria, had two levels: “not indicated” when the patient had 0, 1 or 2 small polyps (≤5mm) and “indicated” when, either the patient had at least one poly >5mm, or the patient had >2 polyps of any size. • Colonoscopy indication based on CCE findings using more stringent (strong) criteria, had two levels: “not indicated” when the patient had ≤2 polyps; and all ≤9 mm, or “indicated”, when the patient had >2 polyps of any size or at least one large polyp (>9mm).
Univariate logistic regressions were used first to assess individual predictor–outcome associations, followed by multivariable models for adjusted estimates. We then reserved 10% of data (randomly selected, N=202) as a hold-out set and used five repeated random splits (90% training, 10% validation) for logistic predictive model development. The validation datasets were used to optimize the probability threshold value that resulted in maximum accuracy. Performance was assessed using area under the ROC (Receiver operating characteristic), Cohen’s Kappa, accuracy, selectivity and specificity; and clinical utility using Decision Curve Analysis (DCA), 24 in R v3.1.2.
Sample size was calculated for 1–60 predictors with 80% power, effect size (Cohens f2 = 0.15) and α=0.05 25 , requiring 54–260 cases; our sample exceeded this requirement. Missing data were minimal or limited to less critical variables, so no imputation was applied. Prior to model application, predictor data should be checked for completeness and plausibility. The model requires no additional user interaction beyond providing input variables and is intended for use by clinicians or researchers with basic clinical and analytical interpretation skills.
Results
Background Patient Data and Outcomes of the CCE Investigations
Participant Background Information: Demographics, Physique, Lifestyle, GI Tract Transit/Stools, Medications/Drugs, and Previous Investigations
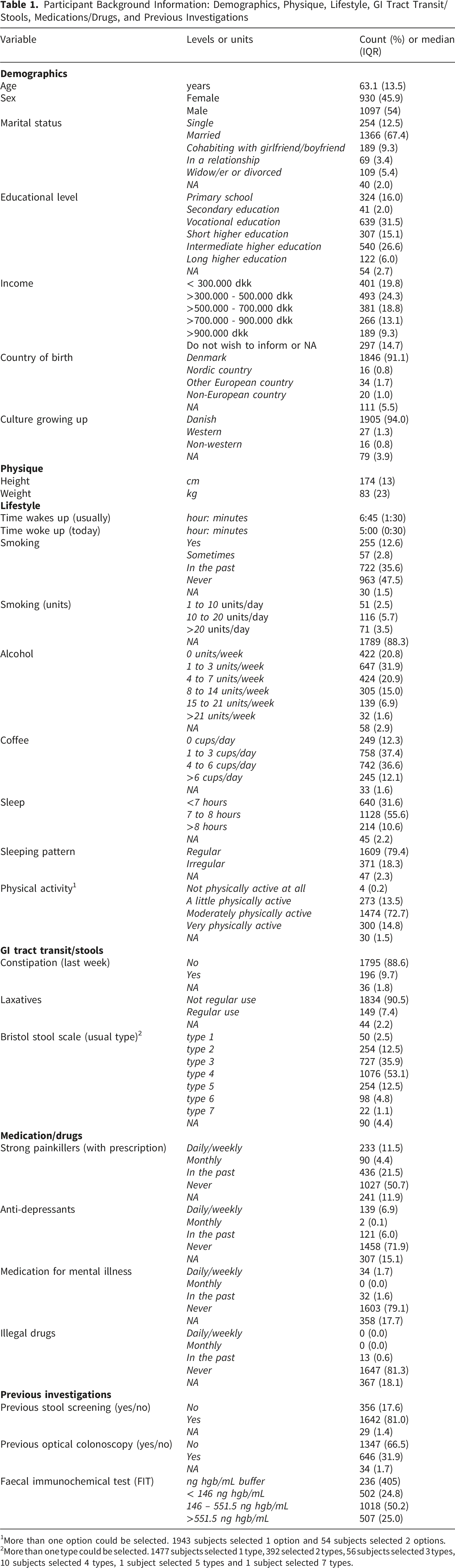
1More than one option could be selected. 1943 subjects selected 1 option and 54 subjects selected 2 options.
2More than one type could be selected. 1477 subjects selected 1 type, 392 selected 2 types, 56 subjects selected 3 types, 10 subjects selected 4 types, 1 subject selected 5 types and 1 subject selected 7 types.
Outcomes of the CCE Investigation in Terms of Transit, Cleansing, Complete Investigation, and Colonoscopy Indication Based on Weak and Strong Indication Criteria
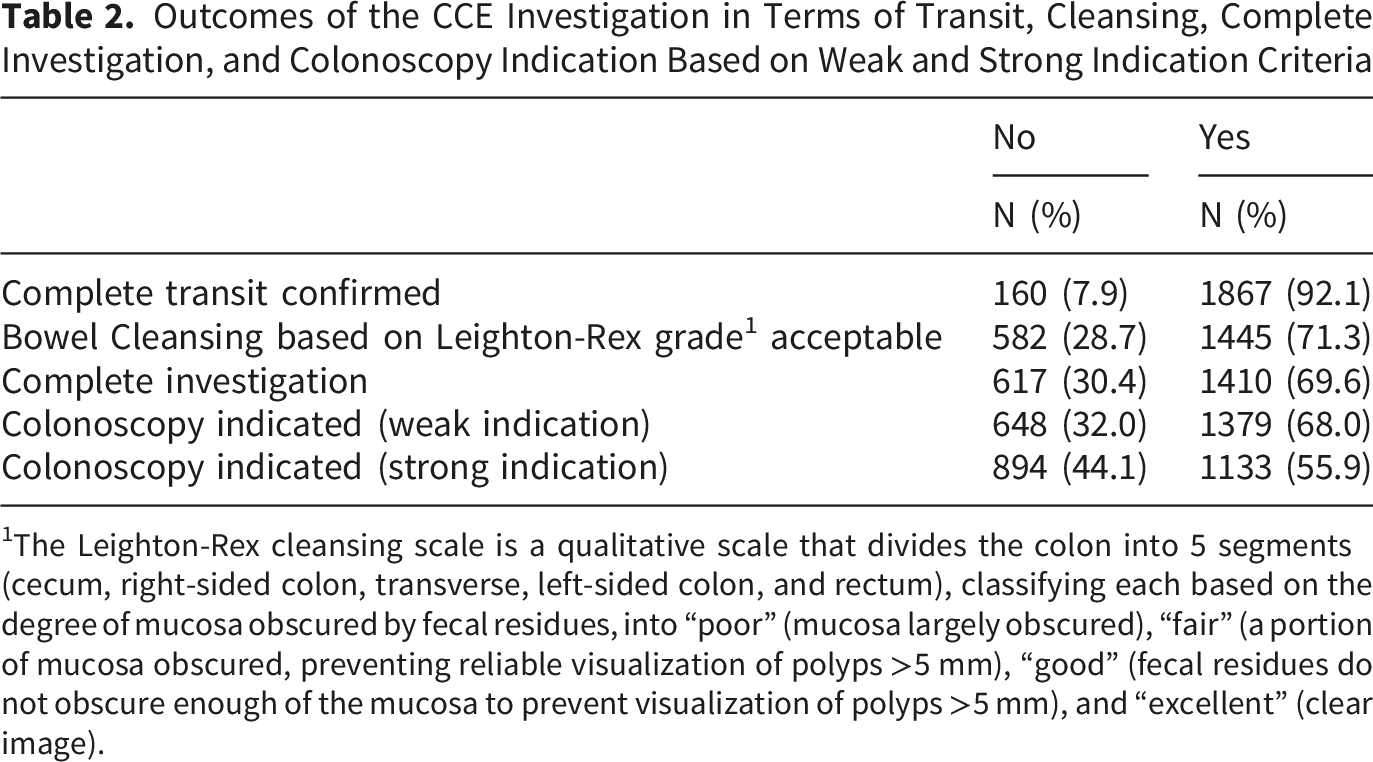
1The Leighton-Rex cleansing scale is a qualitative scale that divides the colon into 5 segments (cecum, right-sided colon, transverse, left-sided colon, and rectum), classifying each based on the degree of mucosa obscured by fecal residues, into “poor” (mucosa largely obscured), “fair” (a portion of mucosa obscured, preventing reliable visualization of polyps >5 mm), “good” (fecal residues do not obscure enough of the mucosa to prevent visualization of polyps >5 mm), and “excellent” (clear image).
Univariate Associations Between Background Patient Data and CCE Outcomes
Bristol Stool Scale type 5 was the only predictor significantly associated with increased odds of complete capsule transit (p<0.05) (supplemental information Table A4). Drinking 15–20 alcohol units weekly, no recent constipation, and no regular laxative use were linked to higher odds of acceptable bowel cleansing, while Bristol type 3, frequent strong painkiller, and antidepressant use were linked to lower odds (p<0.05). Older age, constipation, laxative use, Bristol type 3, and frequent painkiller or antidepressant use decreased odds of complete CCE; drinking 15–20 alcohol units weekly increased odds (p<0.05).
Older age, male sex, height >180 cm, higher weight, waking-up time, smoking, and alcohol increased odds of colonoscopy referral for >2 polyps or one >5 mm (p<0.05). Intermediate education, high income, irregular sleep, Bristol type 1/3 stools, or prior mental illness medication decreased odds.
Older age, male sex, height, weight, waking-up time, smoking, alcohol, coffee, and FIT concentration increased odds of colonoscopy referral for >2 polyps or one >9 mm. Intermediate education, high income, non-European origin, Bristol type 1/3 stools, and prior colonoscopy decreased odds. HLQ and PSS-10 scores correlated with colonoscopy indication (supplemental information Table A5).
Multiple Logistic Regressions Between Background Patient Data and CCE Outcomes
For each outcome, multiple logistic models included those predictors that were found significantly associated with the specific outcome in univariate models (supplemental information Table A6).
Sex and Bristol scale 5 remained positively associated with complete transit, showing only minor changes in the estimated effect sizes. Alcohol consumption (15 to 21 units/week) and Bristol scale 3 were associated with acceptable bowel cleansing. Age (>68 years old), alcohol consumption (15 to 21 units/week) and Bristol scale type 3 were significantly associated with investigation completeness.
Older age, past or current smoking and high alcohol consumption were positively associated with colonoscopy indication following the weak indication criteria; while Bristol scale type 1 was negatively associated.
Similarly, older age, past or current smoking, higher body weight class (>95 kg), high alcohol consumption (≥8 units/week) and higher amount of blood in faecal samples (FIT results≥146 ng hgb/mL) were positively associated with colonoscopy indication according to the strong indication criteria. Bristol scale type 1 and having had a colonoscopy in the past was negatively associated with colonoscopy strong indication.
Predictive Models
The final model for predicting complete transit included sex and Bristol scale type 5 stools. Predictors of bowel cleansing were alcohol consumption, constipation, laxative use, Bristol type 3 stools, painkillers, and antidepressants. Predictors of complete investigation were age, alcohol consumption, constipation, laxative use, Bristol type 3 stools, painkillers, and antidepressants. The model for weak colonoscopy indication included age, height, weight, waking time, education, income, smoking, alcohol, sleep pattern, Bristol type 1 stools, and mental illness medication. The model for strong colonoscopy indication included age, height, weight, waking time, education, income, country of birth, smoking, alcohol, coffee, sleep pattern, Bristol type 1 stools, prior colonoscopy, and FIT results.
Area Under the Receiver Operating Curve (AUC) in the Training (N=1642), Validation (N=183) and Hold-Out (N=202) Datasets, for Each of the Five Training/Validation Data-Splits. 1

1For each output variable, the AUC in training, validation and hold-out datasets were not significantly different from each other (p-value>0.05).
The AUC’s in the hold out dataset for each data split, are shown in Figure 1. AUCs in the hold-out dataset did not differ across data splits (p-value>0.05), indicating model robustness, that is, the model performs consistently across various subsets of the data, suggesting that it generalizes well and is not overly sensitive to the specific data split used for training. Receiver operating characteristic (ROC) curves for the prediction of complete transit, bowel cleansing, complete investigation, colonoscopy indication (weak) and colonoscopy indication (strong) in the hold-out dataset (N=202), for the five data splits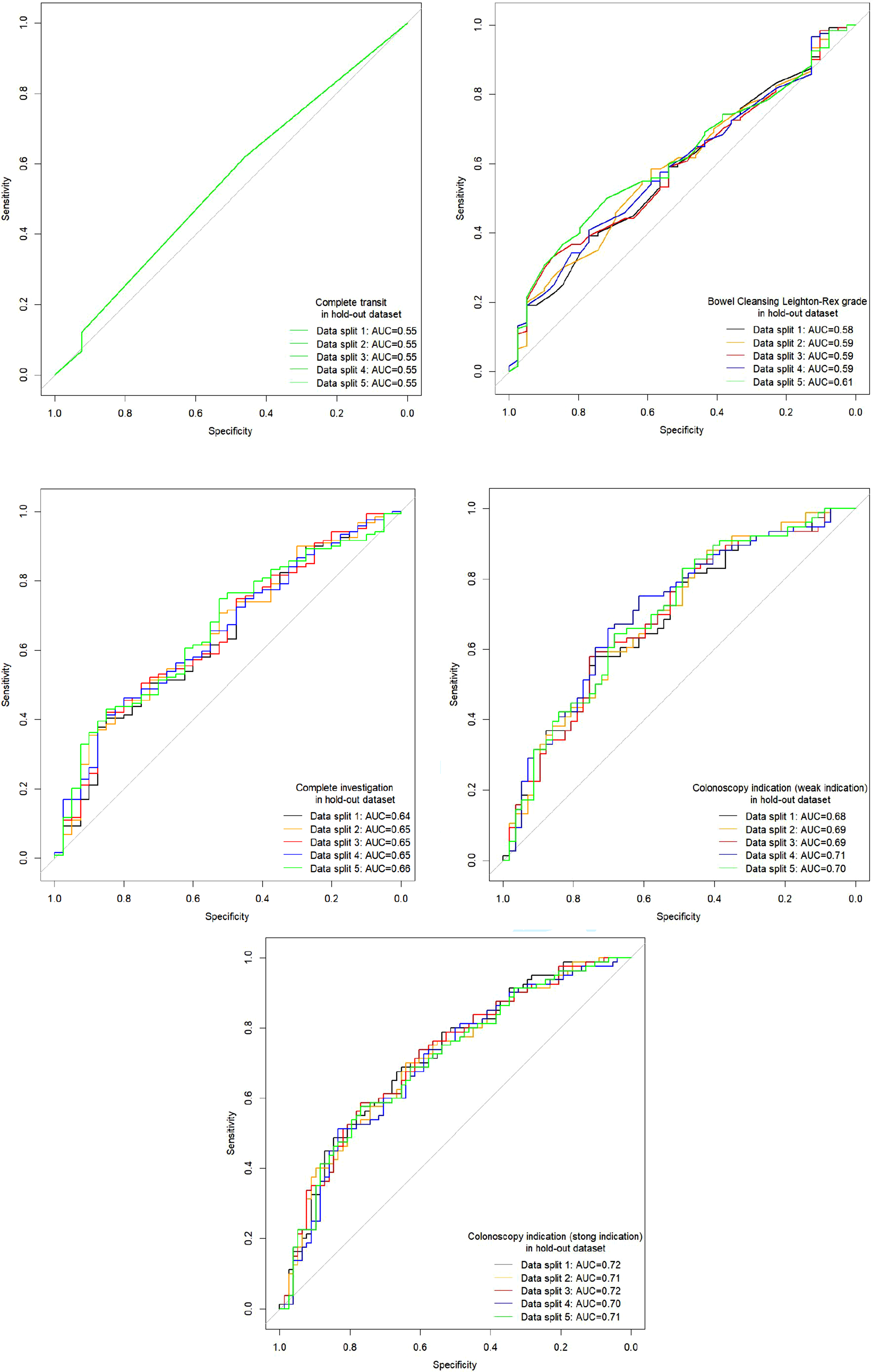
On average, over the five data splits, the AUCs were 0.55 for complete transit, 0.60 for bowel cleansing, 0.65 for complete investigation, 0.69 for colonoscopy indication (weak indication) and 0.71 for colonoscopy indication (strong indication).
Predictive Performance of Models in the Hold-Out Data Set (N=202)

The models developed for prediction of complete transit, bowel cleansing, and complete investigation yielded the poorest overall results for predictive ability, with p-values>0.05 showing that the models’ accuracies were not significantly better than the NIR’s. This is particularly evident in the case of complete transit, in which the prevalence of patients with confirmed complete colonic transit of the capsule was very high (94%), and the model was clearly unable to identify the 6% of patients with incomplete transit of the capsule. Likewise, predictive models were not able to successfully predict which patients will have acceptable bowel cleansing and complete investigation.
Better results were obtained for prediction of colonoscopy indication, both for weak and strong indications. The accuracy, or proportion of correct predictions, was 67% for the colonoscopy indication (weak), and 65% for the colonoscopy indication (strong). These accuracies were significantly higher than non-information rates (57% and 51%, respectively) (p-value<0.001 and p-value=0.01-0.03). The Cohen’s Kappa statistics were 0.28 and 0.30 (for weak and strong indication criteria, respectively) indicating a fair agreement between observed and predicted outcomes.
When applying the predictive models in a clinical context to new patients, we can expect that: out of 100 patients that based on their demographic and clinical characteristics, are predicted as “patients that will not require colonoscopy” (based on the weak indication criteria), 73 patients will indeed not be referred to a subsequent colonoscopy investigation after CCE, while 23 patients will require a subsequent colonoscopy, due to relevant clinical findings. If the strong indication criteria is used; out of 100 patients that are predicted as “patients that will not require colonoscopy” (based on strong indication criteria), 63 patients will indeed not be referred to a subsequent colonoscopy investigation after CCE, while 37 of these patients will require a subsequent colonoscopy. The distribution of outcomes in the training, validation, and hold-out datasets is provided in supplemental information Table A7.
The DCA curves showed that the models for colonoscopy indication provided a positive net benefit across a range of threshold probabilities, particularly between 0.5 and 0.75 (Figure 2). In this range, using the model to guide decision-making (by selecting patients with lower predicted probability of significant findings, for CCE rather than direct colonoscopy), outperformed the strategies of referring all (and none) FIT-positive individuals, showing potential for reducing unnecessary colonoscopy referrals in patients unlikely to have significant findings. Decision curve analysis (DCA) for the prediction model of colonoscopy indication using weak (a) and strong (b) indication criteria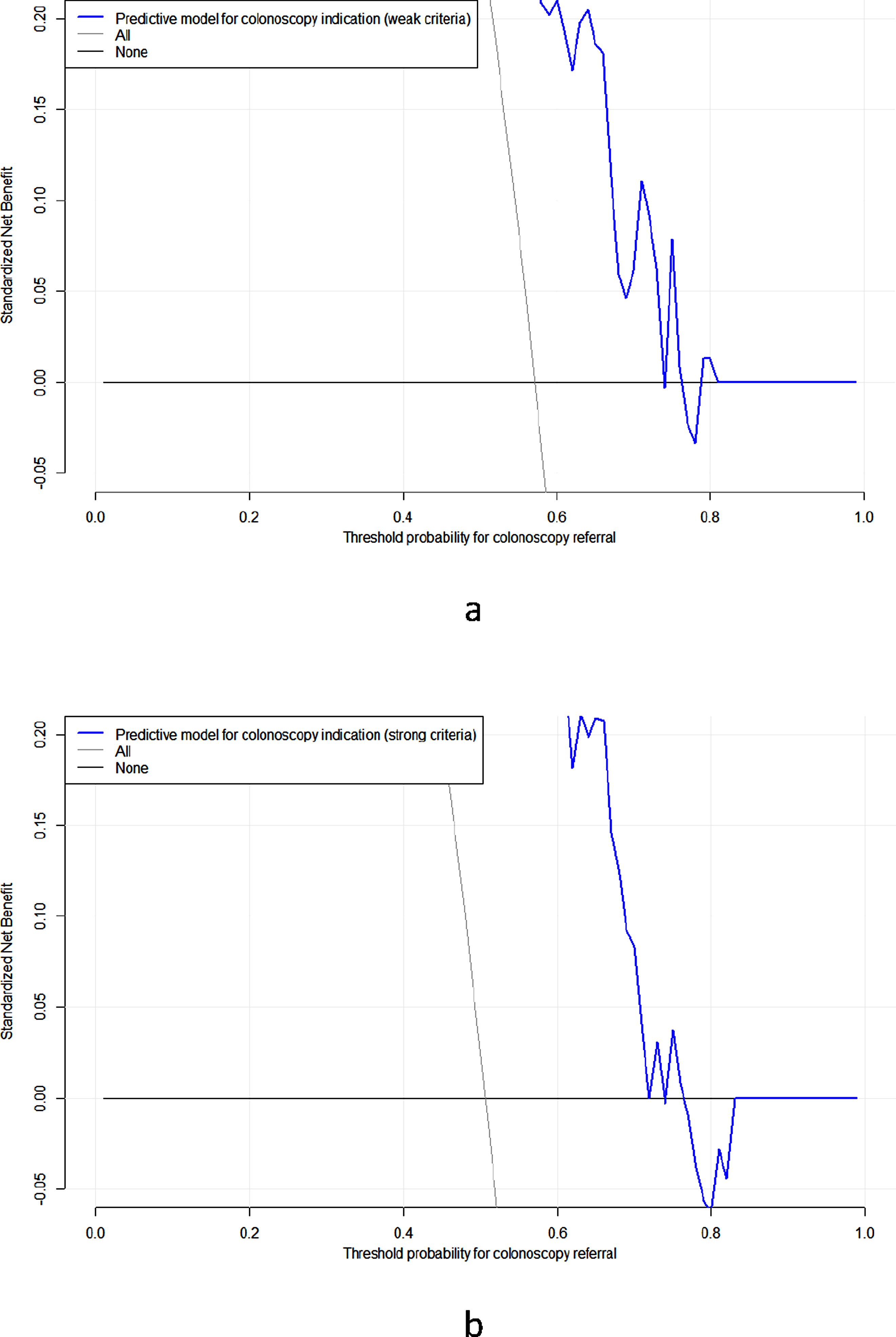
Discussion
The findings of this study contribute to the expanding research on predictive models for CCE in a population with a positive FIT. Prior research 14 has examined various aspects of bowel preparation and polyp detection rates in CCE. Our study is consistent with these findings, demonstrating that predictive models can help categorize patients based on their likelihood of needing a follow-up colonoscopy. However, our work goes further by incorporating a wider range of patient-specific variables, including socioeconomic factors and health literacy scores, to refine criteria for patient selection. This approach enhances predictive capability and highlights disparities in access to follow-up procedures.
The quality of predictor variables is crucial for model performance. We sourced data from a well-characterized cohort within the CFC2015 trial, ensuring a robust dataset. However, relying on self-reported data for several predictor variables can introduce potential biases, such as recall bias and social desirability effects. The outcome measures, including bowel cleansing quality and complete transit, were evaluated through standardized criteria, strengthening our findings’ validity. Nonetheless, variations in subjective assessments of bowel preparation by different CCE readers may introduce some measurement variability. We selected logistic regression due to its interpretability and everyday usage in medical predictive modelling. The models exhibited reasonable predictive performance, with AUC values ranging from 0.55 to 0.72 across different outcomes. While logistic regression allows a clear understanding of variable contributions, alternative machine learning models might enhance predictive performance. Future research should examine the balance between model interpretability and accuracy in clinical decision-making.
A significant strength of this study lies in its focus on a FIT-positive screening population, inherently representing a higher-risk group for colorectal cancer. Unlike general population screenings, which typically have a lower prevalence of pathology, our study suggests that data-driven patient selection could significantly optimize resource utilization by reducing unnecessary colonoscopies. However, these findings may not apply to other groups, such as symptomatic patients or those undergoing surveillance, where different risk profiles and levels of bowel preparation adherence may influence predictive accuracy. 11
Individual factors for prediction of the need for a follow-up investigation have previously been studied in symptomatic and surveillance patients11,16 considered to be low-risk individuals compared to the FIT-positive screening population included in the present study. Building on those findings, our approach towards creating algorithms for accurate patient selection based on the collective sum of characteristics of our patients is advancing the ambitions for prediction models in CCE taking us closer to a clinically implementable and accurate system. Algorithms estimating individual odds of complete and negative CCE investigations will by nature be more personalised than a few selected predictors based on population odds. One would therefore expect the successful patient allocation rate to be higher using the algorithms compared to using singled out markers for patient selection.
Bowel preparation is a critical factor in the success of CCE, yet its effectiveness can vary widely among patients. Elements such as dietary habits, medication use, and individual gastrointestinal transit times play a role in this variability. Our findings indicate that patients who regularly consume alcohol, do not use laxatives, and report less constipation are more likely to achieve acceptable bowel cleansing. This suggests that personalized bowel preparation regimens, tailored based on predictive models, could improve CCE completion rates and reduce the necessity for repeat procedures.
A notable finding of our study is the link between socioeconomic variables and colonoscopy referral rates. Participants with higher education and income levels were less likely to be referred for colonoscopy compared to those with lower socioeconomic status. This raises concerns about potential healthcare disparities, as individuals with lower literacy may face challenges in understanding and adhering to bowel preparation protocols, thereby impacting CCE outcomes. Addressing these disparities through targeted patient education and support strategies is vital for ensuring equitable access to quality screening.
Looking at the large number of colonoscopies carried out with no significant findings reported, CCE can be a great alternative provided that we can identify the right patients. In previous studies,15,26,27 negative colonoscopy rates of 36.8%-56.6% were reported while the rates increased markedly when including the non advanced polyps (61.9%-94.3%) that would not need therapeutic intervention if detected in CCE. The DCA’s offer important insights into the clinical applicability of our predictive models. Notably, the models yielded a higher net benefit than the default strategy of referring all FIT-positive patients for colonoscopy, across a reasonable range of threshold probabilities (approximately 0.5–0.75). This supports the use of CCE in patients with a low predicted probability of significant findings, thereby reducing unnecessary colonoscopies and optimizing resource allocation, and indicating that a personalized approach to post-FIT triage may be clinically advantageous. The present models extend existing approaches by integrating routinely available clinical and socioeconomic variables into a unified predictive framework for practical triage in FIT-positive populations.
These findings may also have broader implications for healthcare resource utilization and sustainability within FIT-positive screening pathways. From a cost-effectiveness perspective, previous studies have demonstrated that CCE pathways are currently associated with higher procedural costs than colonoscopy-first strategies, and that their economic viability is highly sensitive to reinvestigation rates and downstream colonoscopy demand. 28 Moreover, cost-effectiveness has been shown to depend not only on reinvestigation rates, but also on capsule cost and screening adherence, with substantially improved efficiency when participation rates approach those typically observed for FIT screening. 29 Integrating predictive models into clinical workflows could improve resource allocation within overburdened endoscopy units. By identifying patients with a high likelihood of adverse CCE outcomes, we could minimize unnecessary colonoscopies, enhancing efficiency and patient experience. It is widely acknowledged that the reinvestigation rates must be reduced for CCE to be a viable and economically competitive modality in the endoscopic field. A rate less than 25-30% has been suggested as an acceptable threshold from a cost-efficiency and patient preference perspective.28,30 Targeted use of CCE in carefully selected low-risk populations has been proposed as a key strategy to reduce unnecessary colonoscopies and improve endoscopic capacity in screening programs. 31 Beyond economic considerations, environmental sustainability has emerged as an additional and increasingly important dimension of endoscopy service planning. Colonoscopy is associated with substantial CO2-equivalent emissions, driven by consumables, decontamination, energy use, and patient and staff travel. 32 In contrast, CCE may reduce emissions related to endoscope reprocessing and sedation, although its overall footprint is influenced by device manufacturing, logistics, and downstream colonoscopy requirements. 33 Recent “green endoscopy” initiatives emphasize reducing unnecessary procedures and improving patient selection as central strategies to decrease environmental impact. 33 In this context, predictive models that improve selection of patients for CCE or colonoscopy may contribute not only to more efficient resource utilization but also to more sustainable endoscopy practice.
The ethical implications of algorithm-driven patient selection must be scrutinized to ensure that decisions remain transparent, equitable, and aligned with clinical judgment. Additionally, real-world implementation would necessitate robust validation across diverse populations to guarantee generalizability. In the context of the present study, the observed predictive performance may therefore have direct implications for clinical, economic, and environmental efficiency. Using the weak and strong indication models, approximately 73% and 63% of patients, respectively, who were predicted to avoid colonoscopy were correctly classified as not requiring subsequent colonoscopy after CCE, indicating a potential reduction in downstream colonoscopy demand.
Despite its strengths, this study has several limitations. First, while the predictive performance of the models is statistically significant, it remains modest, particularly regarding complete transit and bowel cleansing outcomes. Suboptimal bowel preparation may have introduced variability in CCE-related outcomes. Additional clinical and behavioural variables, such as gut microbiome composition or wearable sensor data, could enhance the models’ accuracy. Second, the generalizability of the findings is limited to FIT-positive screening populations in Denmark, highlighting the need for external validation in other settings. Third, variability in FIT measurement across laboratories and analytical thresholds may limit generalisability. Future models could incorporate laboratory-level variability and alternative faecal biomarker strategies for colorectal cancer risk stratification, such as COLOFIT-type approaches. Lastly, further research should focus on integrating predictive models into clinical decision support systems and assessing their impact on patient outcomes in prospective trials.
Conclusion
This study supports the feasibility of predictive models for optimizing patient selection for CCE within a FIT-positive screening population. Although the predictive performance shows promise, model development and validation improvements are necessary before widespread clinical adoption. Addressing healthcare disparities and ensuring ethical implementation will be crucial for leveraging AI to enhance colorectal cancer screening strategies.
Supplemental Material
Supplemental material - Clinical Prediction Models to Guide the Selection of Patients for Colon Capsule Endoscopy Versus Colonoscopy Following FIT-Positive Screening
Supplemental material for Clinical Prediction Models to Guide the Selection of Patients for Colon Capsule Endoscopy Versus Colonoscopy Following FIT-Positive Screening by Victoria Blanes-Vidal, Esmaeil S. Nadimi, Benedicte Schelde-Olesen, Gunnar Baatrup, Lasse Kaalby Møller, Ulrik Deding, on behalf of the AICE Consortium Author Group in Cancer Control
Footnotes
Acknowledgment
The authors acknowledge the contributions of the AICE (Artificial Intelligence in Capsule Endoscopy) consortium for their support and collaboration.
Ethical Considerations
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki of 1975, as revised in 2024. Approval of the research protocol by an Institutional Reviewer Board: Approvals from the regional ethics committee (ref. S-20190100; Approved 7-Feb-2020) and the Danish data protection agency have been obtained (ref. 19/29858). Registry and the Registration No. of the study/trial. The study has been registered with ![]() under: NCT04049357.
under: NCT04049357.
Consent to Participate
All participants provided informed consent.
Author Contributions
All authors conceptualized and designed the study. B.S.O, L.K., U.D. and G.B. collected the data. V.B.V. and E.S.N. developed the methodology and performed the data analysis, results presentation and interpretation. V.B.V. drafted the manuscript. All authors reviewed and approved the final manuscript, and are accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript was prepared as part of the AICE project Funded by the European Union. Views and opinions expressed are however those of the author(s) only and do not necessarily reflect those of the European Union or the European Commission. Neither the European Union nor the European Commission can be held responsible for them.
Declaration of Conflicting Interests
VBV and ESN declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. GB is co-founder and co-owner of Stratos AI. UD has received honoraria from Norgine. BSO received honoraria from Jinshan Ltd.
Data Availability Statement
The data from the current study will not be publicly available as this is not permitted by Danish legislation. All data are stored at secure, logged governmental servers at ‘Statistics Denmark’. The analytical code is available from the corresponding author upon reasonable request, subject to institutional and data governance approvals.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.