
Abstract
Introduction
Lymphomas are a heterogeneous group of haematological malignancies commonly treated with chemotherapy. Hodgkin lymphoma predominantly affects younger adults, while Non-Hodgkin lymphoma is more prevalent among older adults. Although survival outcomes have improved, treatment-related cardiovascular, musculoskeletal, and functional adverse effects contributing to fatigue, reduced cardiorespiratory fitness (CRF), diminished quality of life (QoL), and increased frailty risk, remain, particularly among older adults. Reduced CRF, measured by peak oxygen uptake (VO2peak), is an independent predictor of all-cause and cancer-specific mortality, and chemotherapy tolerance, making its preservation a clinically meaningful target. Evidence supporting exercise during active chemotherapy remains limited. This study aims to evaluate the effect of a 20-week combined exercise (EX) intervention on CRF in people with lymphoma receiving chemotherapy, compared with a treatment-as-usual (TAU) group.
Methods
EDONOLA is a randomised (1:1), multicentre, parallel-group, open-label controlled clinical trial involving adults aged >18 years (n=180, EX, n=90; TAU, n=90). The exercise intervention comprises supervised sessions (two days/week) of low-to high-intensity resistance and aerobic interval training, plus two days/week of unsupervised exercise. The TAU group will receive standard clinical care and physical activity advice. Assessments will be conducted at baseline, 10 weeks, and 20 weeks. The primary outcome will be CRF, measured as VO2peak. Secondary outcomes will include muscular strength, frailty, body composition, physical activity, sedentary behaviour, QoL, fatigue, sleep, and biochemical profile, including immune biomarkers. Older participants (≥70 years) will additionally undergo a comprehensive geriatric assessment, and EX participants will be invited to a voluntary semi-structured qualitative interview.
Discussion
This multidisciplinary project integrates structured exercise into standard oncology care, aligned with Sustainable Development Goal 3. The intervention aims to mitigate treatment-related side effects, preserve CRF and muscular strength, improve QoL, and reduce frailty risk in people with lymphoma undergoing chemotherapy, while potentially decreasing long-term healthcare burden.
Plain Language Summary
People with lymphoma often receive chemotherapy, which can cause tiredness, loss of strength and fitness, and make everyday activities more difficult. These effects can be especially challenging for older adults. Exercise may help reduce these problems, but there is still limited research on how helpful it is for people receiving treatment for lymphoma. The EDONOLA study will test whether a 20-week exercise programme can help people with lymphoma stay stronger and fitter during chemotherapy. The study will include 180 adults with Hodgkin and non-Hodgkin lymphoma. Half of the participants will take part in supervised exercise sessions that combine strength and aerobic activities, along with additional exercise at home. The other half will receive their usual medical care and general advice about physical activity. Researchers will measure changes in physical fitness, strength, tiredness, sleep, daily activity, and quality of life during the study. Older participants will also receive additional health assessments. The goal is to find out whether exercise can help people cope better with treatment, maintain independence, and improve wellbeing during and after chemotherapy.

Background
Lymphoma comprises a heterogeneous group of neoplasms arising from clonal proliferations of B cells, T cells, or natural killer (NK) cells, involving lymphocytes at different stages of maturation.1,2 According to the fifth edition of the World Health Organization classification of haematolymphoid tumours, a hierarchical system (i.e. category, family/class, entity/type, and subtype) is applied for classification. 3 In clinical practice, however, diagnosis and patient management typically rely on a broader dichotomy: non-Hodgkin lymphoma (NHL), which constitutes approximately 90% of cases, and Hodgkin lymphoma (HL), which accounts for the remaining 10%.2-4 The incidence of NHL is higher in men older than 65 years of European and Hispanic descent, 5 whereas HL exhibits a bimodal age distribution, with a higher incidence in young adults aged 20-40 years and in people aged 55 years and older.6,7 This distinct epidemiological profile, with HL predominantly affecting younger adults and NHL disproportionately affecting older ones, has important clinical implications for the long-term management of treatment-related toxicity across the full adult age spectrum.
Chemotherapy, administered either as monotherapy or in combination formats, remains the cornerstone of treatment and is often integrated with immunotherapeutic approaches. 8 Owing to advances in personalised and targeted therapies, outcomes have markedly improved, with more than 80% of patients with HL 9 and up to 60% of those with NHL, depending on subtype, 8 achieving favourable prognoses and long-term survival. Consequently, attention has increasingly shifted towards the late adverse effects of treatment. The primary chemotherapeutic agent used in both HL and NHL is doxorubicin, an anthracycline whose cardiotoxicity is well established and dose-dependent. The threshold between low and high heart failure risk is defined at cumulative doses of 250-300 mg/m2, a level routinely reached in standard lymphoma protocols. 10 Beyond treatment-related mechanisms, lymphoma itself generated a systemic inflammatory environment characterised by elevated levels of proinflammatory cytokines, including interleukin 6 and Tumour Necrosis Factor alpha, that promote endothelial dysfunction, a prothrombotic state, and accelerated atherosclerosis, further amplifying cardiovascular risk independently of chemotherapy. 11 In this context, patients are susceptible to developing non-ischaemic cardiomyopathy induced by chemotherapy-related oxidative stress and apoptosis,9,12 processes that also directly impair mitochondrial function and reduce cardiac output, leading to a clinically meaningful decline in cardiorespiratory fitness (CRF) of up to 25% during active treatment,13,14 as well as accelerated loss of muscle mass leading to mitochondrial dysfunction and sarcopenia, particularly among patients considered elderly (i.e. 70 years or older).15-18 These are key factors associated with cancer-related symptoms such as fatigue and exercise intolerance (i.e. reduced CRF), pain, cognitive impairment, sleep disorders, and decreased health-related quality of life (QoL).15,16 The long-term clinical relevance of these effects is particularly pronounced in younger HL survivors, who face a survival window of 30-40 years post-treatment during which late cardiovascular events represent a major cause of morbidity and mortality. 19
Critically, reduced CRF is not merely a physiological marker of treatment burden; it is an independent predictor of all-cause mortality, cancer-specific mortality, treatment tolerance, and functional independence in oncology populations. A systematic review and meta-analysis demonstrated a strong, graded, inverse association between CRF and total cancer mortality, with high CRF associated with a 45% reduction in mortality risk compared with low CRF, independent of adiposity. 20 These findings have been corroborated in adults diagnosed with cancer more broadly, 21 and in lymphoma survivors specifically, where higher physical activity and preserved peak oxygen uptake (VO2peak) have been associated with substantially lower cancer mortality risk. 22 Furthermore, pretreatment CRF has been shown to independently predict chemotherapy relative dose intensity (i.e., those patients with lower aerobic fitness are significantly less likely to complete optimal chemotherapy dosing), with evidence of a positive dose-response relationship between aerobic capacity and treatment tolerance. 23 In this sense, CRF may occupy a central mechanistic and prognostic position, because it is both a direct consequence of chemotherapy-induced cardiotoxicity and a key determinant of the capacity to tolerate treatment and maintain functional independence throughout and beyond it.
Therefore, to prevent or reduce the risk of side effects and to preserve physical function (i.e. CRF and muscular fitness, as well as tolerance to exercise-induced symptoms such as breathlessness and fatigue),24,25 patients with cancer are advised to adhere to public health recommendations, namely multicomponent exercise programmes including aerobic and resistance exercises.25,26 Although patients with haematological malignancies were previously restricted from exercise because of severe anaemia and thrombocytopenia, a recent systematic review of patients with lymphoma identified evidence supporting the potential effectiveness of exercise-based interventions on muscle mass, functional performance, and health-related QoL during chemotherapy. 27 Furthermore, incorporating physical activity into the lives of adults with lymphoma appears feasible, reduces fatigue, and may limit the decline in physical function during treatment.28,29
According to the FITT (Frequency, Intensity, Type, Time) principle, high-intensity interval training (HIIT), alone or combined with resistance training, appears to be an effective method for improving CRF and QoL in patients with cancer undergoing chemotherapy.30-32 However, these studies have focused mainly on adults with solid tumours, and there remains a need for research in haematological cancers, including older adults. In addition, given the established cardiotoxicity of chemotherapy and the documented benefits of interval resistance training (using “cluster sets”) in patients with cardiovascular disease, 33 it is crucial to investigate this training modality in patients with lymphoma as well.
Moreover, participants in previous cancer research have reported awareness of the importance of exercise, hope of recovery, and the possibility of living longer with the disease, viewing exercise as an adjuvant therapy.34,35 Thus, identifying barriers and enablers to remaining physically active during treatment is of particular interest. 36
Given this evidence, VO2peak, the gold standard objective measure of CRF, was selected as the primary outcome of the present investigation. As an objective, reproducible, and physiologically integrative measure, VO2peak captures the global impact of both the disease and its treatment on the cardiopulmonary and musculoskeletal systems, and it is directly sensitive to the cardiotoxic mechanisms of chemotherapy described above. Patient-centred outcomes, including fatigue, QoL, and sleep quality, are of unquestionable clinical importance and will be addressed as pre-specified secondary outcomes. However, their inherent susceptibility to subjective variability makes them less suitable as primary endpoints in a controlled intervention study. By prioritising VO2peak, the study will be positioned to generate objective, comparable evidence that can inform clinical practice and strengthen the evidence base for exercise oncology in haematological cancers.
The primary aim of the present investigation will be to evaluate the effect on CRF, objectively measured by peak oxygen uptake (VO2peak), in people diagnosed with HL and NHL undergoing chemotherapy, following a 20-week combined exercise intervention. This intervention will include supervised sessions (2 days/week) combining low-to high-intensity resistance training and aerobic interval training, plus 2 days/week of unsupervised exercise, and will be compared with a treatment-as-usual (TAU) group receiving standard clinical care plus general physical activity recommendations. The secondary aims are organised into four thematic clusters:
It is hypothesised that a 20-week combined exercise programme, incorporating supervised low-to high-intensity resistance training and interval aerobic exercise alongside unsupervised sessions, will significantly improve CRF and physical function, reduce fatigue and treatment-related toxicity, enhance QoL, and support better treatment adherence compared with TAU, thereby offering a feasible and cost-effective adjuvant strategy for patients with HL and NHL undergoing chemotherapy.
Methods
Standard Protocol Approval, Registration, and Patient Consent
The present study will be conducted in accordance with Good Clinical Practice and the ethical standards outlined in the 1964 Declaration of Helsinki and its subsequent amendments. The study protocol was approved by Euskadi’s Medicine Research Ethics Committee (CEIm-E) (19 September 2024, version 2; 27 January 2025, version 2.1) under the internal code PI2024133, and registered on ClinicalTrials.gov (identifier: NCT06660446; Protocol ID: EDONOLA; 5 November 2024). Written informed consent will be obtained from all patients entering the study by medical personnel at the participating institutions. Participants will be informed that they may withdraw from the study at any time without providing a reason and without any impact on their current or future care. It is considered essential to keep general practitioners regularly informed of the study’s progress.
Design
The EDONOLA study is a randomised (1:1), multicentre, parallel-group, open-label, controlled clinical trial. The study protocol has been prepared in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2025 statement to enhance the quality of trial reporting. 37 This project is funded by the Department of Health of the Basque Government through the Grants for Health Research and Development Projects programme (2023111073). The Health Research Institute of Biogipuzkoa is the promoter of the study (Donostia/San Sebastian, Gipuzkoa, Basque Country) and, together with the Health Research Institutes of Bizkaia and Araba and the Department of Physical Education and Sport of the University of the Basque Country (EHU), will conduct the study in a coordinated manner.
Patient and Public Involvement
Patients were not directly involved in the design, recruitment, or conduct of the present study; however, the development of this protocol was informed by prior patient-centred work conducted at our institution with a haematogeriatric programme for older adults with lymphoma. This programme included implementing a geriatric assessment pathway and a pilot study to evaluate frailty and establish a multidisciplinary care model involving internal medicine, pharmacy, haematology, and nursing services. Feedback and experiences reported by patients during this initiative helped to identify unmet needs and gaps in supportive care, particularly regarding functional decline, treatment tolerance, and feasibility of interventions during chemotherapy. The current EDONOLA study has been refined based on these insights, with adaptations made to enhance the feasibility, acceptability, and clinical relevance of the exercise intervention. Therefore, patients’ perspectives have indirectly contributed to shaping the study design. Future dissemination plans will consider strategies to share results with participants and relevant patient communities.
Participants: Recruitment and Selection Criteria
The EDONOLA trial targets adults aged 18 years and older, the threshold at which individuals are legally recognised as autonomous adults under Spanish legislation and European clinical trials regulation (EU No 536/2014), encompassing the full adult lymphoma population while excluding adolescents, whose distinct developmental, psychosocial, and clinical management needs warrant dedicated investigation.
Inclusion and Exclusion Criteria for the EDONOLA Study

The principal investigators may withdraw participants from the study for the following reasons, among others: voluntary withdrawal, loss of contact during follow-up, a decision by the investigators that continuation in the study is not in the best interest of the participant (e.g. intercurrent illness or disease), occurrence of serious or life-threatening adverse reactions, and injury or toxicity that prevents continuation of the physical exercise programme. At the time of withdrawal, the primary reason should be recorded and, where possible, the participant should be re-evaluated.
Randomisation
After fulfilling the selection criteria and providing written informed consent, participants will be assigned a trial-specific anonymous identification code (e.g. EDONOLA-1001-Gipuzkoa, EDONOLA-2001-Araba, EDONOLA-3001-Bizkaia) to ensure confidentiality and facilitate prospective meta-analysis. Allocation will be performed after completion of the baseline assessments.
The randomisation list was generated using an online tool developed in R Shiny (https://icostatistics.shinyapps.io/randlist/). Block allocation was applied, with randomly varying block sizes (range 4–8). The trial is stratified by recruitment site only (1, Gipuzkoa; 2, Araba; 3, Bizkaia). To ensure sufficient allocation at each site, 180 assignments were generated. In practice, 90 participants are planned for Donostia (Gipuzkoa), 45 for Araba, and 45 for Galdakao (Bizkaia). The trial includes two groups (treatment arms): treatment as usual (TAU) and the exercise intervention. The allocation variable is termed ‘group’. Participants will be randomly assigned to one of the two groups (Figure 1): the Exercise (EX) group or the TAU group. Exercise physiologists will be responsible for informing participants of their group allocation and providing the corresponding explanations. Accordingly, the EDONOLA study is not blinded; participants will be aware of their assigned group because of the nature of the intervention. Flow chart
Data Sharing and Accessibility
Data from each participant will be collected in an electronic case report form specifically designed for this study on the REDCap platform and stored under password protection on the Health Public Service (Osakidetza) computer. Once data collection is complete, analyses will be performed using SAS and R software by the Methodology Unit of the Biogipuzkoa Institute. Data will be collected at each research centre by appropriately qualified and designated staff. The identity of participants cannot be discerned from the data collected in the electronic case report form. For individuals who join the study but ultimately do not meet the selection criteria, the electronic case report will record the date of the screening visit, the reason for failure to meet the selection criteria, and the date of discontinuation. The research team must retain, at all times, the original records (i.e.,source documents) of each patient’s data. Likewise, they will maintain a confidential list identifying the patients, allowing for the unambiguous identification of each one. All documents related to the study must be retained for at least 15 years or until notified by the sponsor.
Assessments
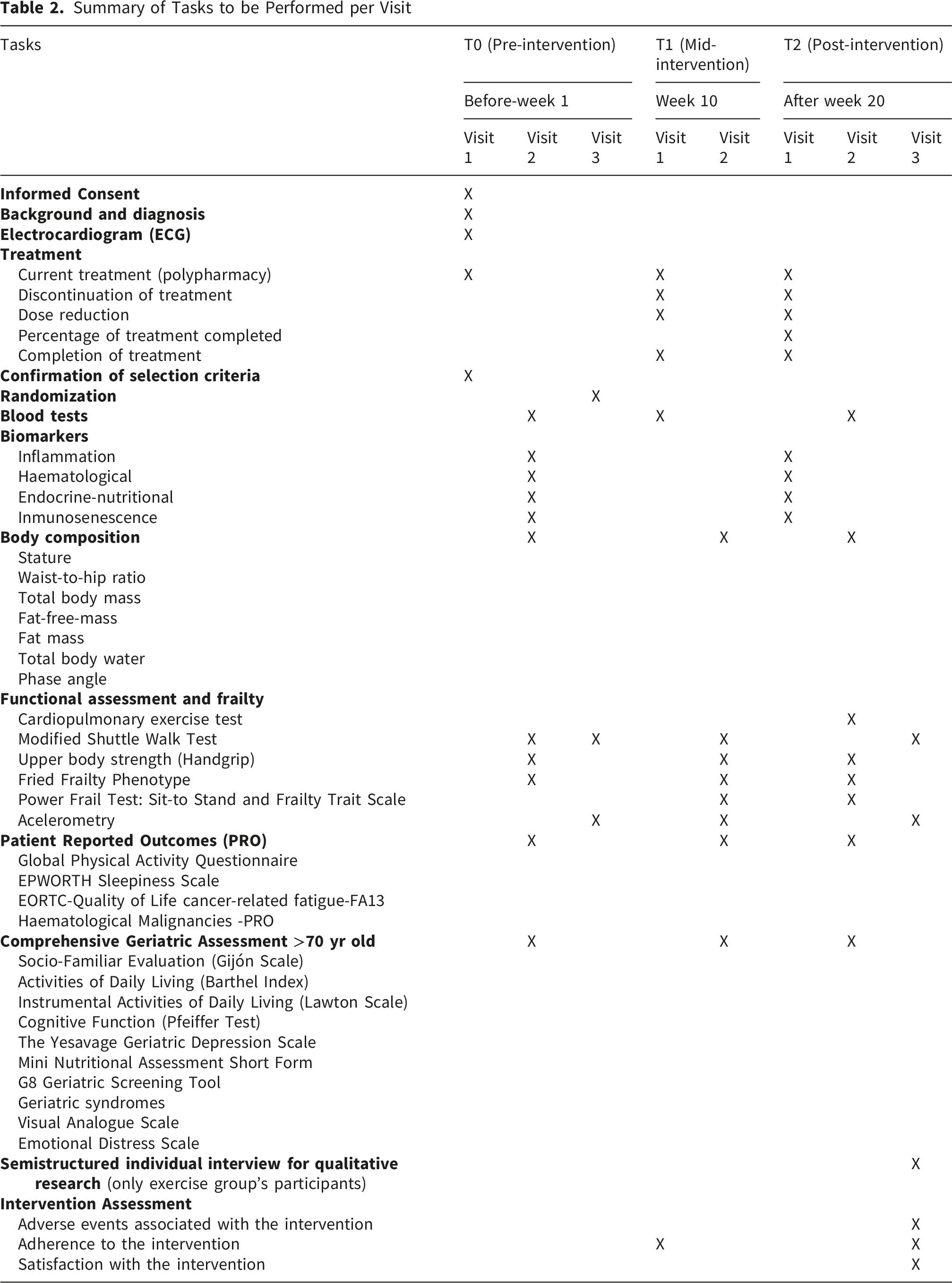
Summary of Tasks to be Performed per Visit
Haematology Data and Diagnosis
Participants with lymphoma diagnosed with either NHL or HL and receiving at least 8 weeks of chemotherapy will be stratified by disease type (indolent NHL [follicular lymphoma, marginal zone lymphoma] versus aggressive NHL [diffuse large B-cell lymphoma, primary mediastinal lymphoma, high-grade lymphoma] versus HL) and by planned chemotherapy protocol (R-CHOP [rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone], R-CVP [rituximab, cyclophosphamide, vincristine, prednisone], R-bendamustine, R-da-EPOCH [rituximab, dose-adjusted cyclophosphamide, doxorubicin, vincristine, prednisone], ABVD [doxorubicin, bleomycin, vinblastine, dacarbazine], CHOP, or CVP). Baseline demographic and disease-related characteristics will be collected, including age, sex, Eastern Cooperative Oncology Group performance status score, disease stage, disease-specific prognostic index, comorbidities, previous medical history (smoking status, alcohol intake, hypertension, diabetes, hypercholesterolaemia, cardiac history, depression, or anxiety), and chemotherapy regimen.
Chemotherapy Dose Determination
Medication list. The clinical team will provide a baseline medication list. Any additions, dose changes, or discontinuations of medications after enrolment, together with corresponding dates, will be documented. Chemotherapy treatment completion rates will be assessed as the number of cycles received divided by the number of cycles planned.
Recognition of frailty may prompt the haematology team to consider tailored treatment approaches, such as dose adjustments based on patient fitness. Conversely, accurate frailty assessment may also provide confidence to proceed with standard treatment in fitter older patients. Chemotherapy dosing, scheduling (including frequency), and any dose adjustments, together with the reasons for these modifications, will be recorded.
Adverse complications and events. At mid-intervention (T1) and post-intervention (T2), all adverse events associated with the intervention will be recorded and analysed by the study team to determine whether they have affected adherence to the intervention.
Biochemistry. At enrolment, all participants will provide a fasting blood sample at the facilities of the three participating hospitals. In addition to standard laboratory tests performed at T0, T1, and T2, which include glycaemia, lipid profile (total cholesterol, low-density lipoprotein, high-density lipoprotein, triglycerides), uric acid, haematometry with white blood cell count, serum albumin, ferritin, and C-reactive protein, biological samples will be obtained at T0 and T2 for the analysis of immune biomarkers.
Samples will be sent to the biobank in two tubes: whole blood collected in an EDTA tube (9 mL) for the extraction of mononuclear cells and plasma, and whole blood collected in a gel tube (4 mL) for serum collection. Plasma and white blood cell fractions will be isolated by centrifugation and stored at −80°C in biobanks for later processing. Biomarker analyses will be centralised at the Health Research Institute of Biogipuzkoa.
Inflammatory biomarker analyses will include the following two procedures: ELISA assays for endocrine-nutritional and muscle mass loss markers, including insulin-like growth factor 1 (IGF-1), dehydroepiandrosterone sulphate (DHEA sulphate), vitamin D, albumin, and myostatin (MSTN/GDF8); and multiplex ELISA assays for inflammatory markers, including interleukin (IL)-1β, IL-2, IL-4, IL-6, IL-8/CXCL8, tumour necrosis factor alpha (TNFα), interferon gamma (IFNγ), tumour necrosis factor receptor 1 (TNFR1), and brain-derived neurotrophic factor (BDNF).
For the cellular fraction, the study will focus on the phenotypic characterisation of the two main subpopulations of cytotoxic lymphocytes: CD8+ T cells and NK cells. Markers of immunosenescence will be analysed, including the expansion of terminally differentiated CD8+ T cells and the CD4/CD8 ratio. To this end, a flow cytometry panel with fluorochrome-conjugated antibodies targeting CD3, CD4, CD8, CD27, CD28, CD45RA, CD45RO, CD56, CD57, CD161, KLRG1, NKG2A, NKG2C, and viability will be used. The flow cytometry panel will be standardised for the assessment of immunosenescence markers in peripheral blood mononuclear cells from cryopreserved baseline and end-of-intervention samples. Samples will be processed using a BD Fortessa X-20. Given that samples will be collected across different locations in the Basque Country, analysis of fresh biospecimens is not feasible. Data analysis will be performed using FlowJo software, with graphical and statistical analyses conducted using GraphPad Prism.
Anthropometry and body composition. Anthropometric data will be collected in accordance with the standards of the International Society for the Advancement of Kinanthropometry. 38 Measurements will include standing height assessed using a SECA 213 stadiometer (Hamburg, Germany), as well as waist and hip circumferences to calculate the waist-to-hip ratio. Body composition variables, including total body mass, fat-free mass, fat mass, total body water, and phase angle, will be assessed using bioelectrical impedance analysis. All measurements will be performed after a minimum fasting period of 3 hours.
Functional Assessment, Strength, and Frailty. Different Procedures Will be Performed
1. CRF will be objectively assessed using VO2peak and ventilatory thresholds (VT1 and VT2) via a symptom-limited peak cardiopulmonary exercise test (Modified Bruce ramp protocol or Naughton ramp protocol, at the discretion of the specialist) under controlled laboratory conditions on a treadmill at T0 and T2. Continuous ECG monitoring will be implemented throughout the procedure, and participants will receive standardised verbal encouragement from the exercise specialist. Gas exchange and ventilatory variables will be analysed, with calibration performed before each session according to the manufacturer’s guidelines. Breath-by-breath data will be collected continuously and averaged over 60-second intervals. Peak VO2 will be considered valid when at least two of the following four criteria are met: achievement of >85% of age-predicted maximal heart rate, near-maximal perceived exertion (>18 on the Borg scale), a peak respiratory exchange ratio of ≥1.10, or no further increase in oxygen uptake or heart rate despite increasing workload.
39
Perceived exertion (6–20 Borg scale) will be recorded at the end of each minute or stage, and blood pressure will be measured every 2 minutes. Both VT1 and VT2 will be identified using standard V-slope and ventilatory-equivalent methods.
39
After completion of maximal effort, a 5-minute recovery period will be recorded. Participants will remain walking on the ergometer during the first minute of recovery and seated for the remaining four minutes, while ECG and blood pressure continue to be monitored. Absolute and relative criteria for test termination will also be followed.
40
Based on VT1 and VT2, three exercise intensity zones will be defined: R1 (light to moderate), corresponding to heart rates below VT1; R2 (moderate to vigorous), between VT1 and VT2; and R3 (vigorous to severe), corresponding to heart rates above VT2.
39
2. The MSWT will require participants to walk or jog back and forth along a 10-metre course, following progressively increasing pace cues, according to the standard protocol.
41
The test will be terminated under any of the following five conditions: completion of level 15; inability to maintain the prescribed pace due to breathlessness; falling more than 0.5 metres behind the marker at the beep; heart rate exceeding 85% of age-predicted maximum; or onset of symptoms such as chest discomfort, angina, dizziness, confusion, or severe muscular fatigue.41,42 3. Upper body strength will be assessed using hydraulic handgrip dynamometry (e.g. Jamar) following a standardised protocol. Measurements will be taken in a seated position, with the elbow flexed at 90°, the forearm supported, and the arm in a neutral position. Each contraction will be sustained for at least 3 seconds, with bilateral assessment consisting of three trials per hand and a minimum 30-second recovery interval between trials, accompanied by verbal encouragement. The highest value obtained across all measurements will be used for analysis.
43
4. The Frailty Trait Scale (Short Form 5-item) provides a validated measure for identifying individuals at risk of frailty. The scale comprises five components: nutritional status (body mass index), balance (Romberg test), physical activity level, handgrip strength, and gait speed. Each item contributes to a total score ranging from 0 to 50, with higher scores indicating greater frailty.
44
5. Frailty will also be assessed using the Fried Frailty Phenotype, which defines frailty based on five physical criteria: unintentional weight loss, self-reported exhaustion, weakness, slowed walking speed, and low physical activity. Participants will be categorised as robust (no criteria met), pre-frail (one or two criteria met), or frail (three to five criteria met).
45
6. The sit-to-stand muscle power test has been previously validated. Participants will be instructed to rise from a standard chair to a full standing position and sit back down as quickly and safely as possible five times, with their arms crossed over their chest. The total time required to complete the five repetitions will be recorded using a stopwatch.46,47
Physical activity, sedentary behaviour, and sleep quality. Physical activity and sedentary behaviour will be assessed using two complementary approaches. First, participants will complete the Global Physical Activity Questionnaire, developed by the World Health Organisation to measure physical activity across multiple domains, including work, transportation, and recreational or leisure time. The questionnaire also collects information on sedentary behaviour and provides estimates of total physical activity expressed as metabolic equivalent minutes per week (MET-min/week), allowing classification of participants into activity levels (low, moderate, or high).48,49 Second, participants will wear a triaxial accelerometer (ActiGraph wGT3X-BT, Pensacola, FL, USA) on their non-dominant wrist for sleep assessment for 7 consecutive days, in accordance with established research guidelines. 50 Participants will receive verbal instructions on correct device use and on completing a corresponding activity diary. On the eighth day, accelerometers and completed diaries will be collected. Movement behaviours, including sleep, sedentary behaviour, low-intensity physical activity, and moderate-to-vigorous physical activity, will be classified using a published machine-learning model. 51 Data from each monitor will be downloaded and processed using the manufacturer’s software (ActiLife version 6.15.0) with a 60-second epoch. Extracted sleep parameters will include total sleep time, defined as the total number of minutes spent asleep between sleep onset and final awakening; wake after sleep onset, calculated as the total duration of wakefulness occurring after initial sleep onset; and sleep efficiency, calculated as the ratio of total sleep time to time in bed multiplied by 100. Sleep–wake patterns will be identified using a validated algorithm based on the Cole–Kripke method, 52 which processes raw ActiGraph data to estimate sleep duration.
Other Patient-Reported Outcomes
1. The Epworth Sleepiness Scale (ESS) assesses general daytime sleepiness by rating the likelihood of dozing off in eight common situations. The total score ranges from 0 to 24, with higher scores indicating greater daytime sleepiness. Scores of 11 or higher suggest excessive daytime sleepiness and the potential need for further medical assessment.
53
2. Cancer-related fatigue will be assessed using the EORTC QLQ-FA13, a 13-item patient-reported questionnaire developed by the European Organisation for Research and Treatment of Cancer Quality of Life Group. The instrument evaluates physical, emotional, and cognitive aspects of fatigue, as well as its impact on daily activities and social functioning. Items are rated on a 4-point Likert scale, with higher scores indicating greater symptom severity.
54
3. Haematological Malignancy Patient-Reported Outcome Measure (HM-PRO). The Validated HM-PRO Questionnaire Is a Composite Measure Assessing the Impact of Disease and Treatment on Quality of Life (Part A) and Associated Signs and Symptoms (Part B).
55
Comprehensive Geriatric Assessment (CGA). The CGA will be administered to participants aged 70 years and older to predict treatment-related toxicity, treatment adherence, quality of life, ability to inform treatment decision-making, and overall survival. The CGA will incorporate standardised tools recommended by the American Society of Clinical Oncology, including assessments of functional and cognitive status, comorbidities, falls, and social, nutritional, and psychological status.56,57
Intervention
Participants randomised to the TAU group will receive general physical activity recommendations, including individualised intensity ranges for aerobic exercise programmes (150-300 min/week of moderate aerobic intensity) and resistance training focused on basic motor patterns. To facilitate monitoring of activity, participants will be asked to carry their mobile phones with a step-counting application installed.
For participants allocated to the EX group, all sessions will begin and end with blood pressure measurements. Exercise intensity will be monitored using heart rate monitors and the Borg Rating of Perceived Exertion scale (6–20) during aerobic exercise. Each session will include a 5- to 10-minute warm-up consisting of joint mobility exercises, followed by a 10-minute cool-down including basic stretching and controlled breathing. The central component of each session will comprise resistance training and aerobic interval exercise.
Resistance training will include eight exercises targeting the main muscle groups and fundamental movement patterns (hip-dominant, knee-dominant, upper-body vertical traction, upper-body horizontal traction, micro-jumps, and core exercises). A progressive design will be applied, advancing from low-intensity interval resistance training (LIRT) to high-intensity interval resistance training (HIRT), incorporating cluster sets of 20 repetitions (4 × 5 repetitions with intra-set recovery periods of 20–30 seconds), with progressive increases in load. Aerobic exercise will be performed on a cycle ergometer, progressing in both volume (from 10 to 20 minutes) and intensity (light to moderate to vigorous), following a progression from low-intensity aerobic interval training (LIIT) to low-volume high-intensity interval training (HIIT), defined as less than 10 minutes of total exercise time at moderate-to-vigorous intensity per session.
During the first month, the programme will allocate more time to resistance training (30 minutes) than to aerobic exercise (10 minutes). By month four, session time will progress to 20 minutes for each component. Aerobic exercise intensity zones (R1: light; R2: moderate; R3: vigorous) will be individually prescribed based on ventilatory thresholds identified during the baseline cardiopulmonary exercise test. All supervised exercise sessions will be monitored in real time using heart rate sensors paired with Polar software, which transmits participants’ physiological responses via Bluetooth to a dedicated iPad operated by the supervising exercise professional. This setup allows continuous, session-by-session verification that participants are exercising within their prescribed intensity zones, enabling immediate adjustments to training load when necessary. This approach will provide a robust, objective framework for quantifying both intensity compliance and intervention fidelity throughout the programme. Resistance training intensity will be determined by the ability to complete each set with appropriate technique, using a repetitions-in-reserve (RIR) value of two. Each supervised session will last approximately 80 minutes.
The structure of the exercise intervention is designed according to three evidence-based principles. First, given that chemotherapy-induced muscle wasting begins early in the treatment course and represents a primary driver of functional decline, sarcopenia, and reduced treatment tolerance in patients with lymphoma, resistance training will be prioritise in the early phase of the programme to maximise the window for muscle mass preservation, as recommended for cancer patients where preservation of muscle mass is the dominant clinical concern. 58 Second, the initial low aerobic volume was deliberately chosen to minimise the potential interference effect of aerobic exercise on neuromuscular adaptations during the early treatment period, 59 as well as to ensure tolerability in patients who may present with peak treatment-related fatigue in the first weeks of chemotherapy. Third, the progressive equalisation of resistance and aerobic components across the five months reflects an evidence-based periodisation strategy: as participants adapt to the combined exercise stimulus and treatment-related burden stabilises, increasing aerobic volume and intensity becomes both feasible and necessary to generate clinically meaningful improvements in CRF, consistent with evidence from concurrent resistance and HIIT trials conducted during chemotherapy. 60
To minimise dropout and promote adherence, sessions will include musical accompaniment. Adherence to the exercise intervention will be assessed as the number of supervised sessions attended out of the 40 sessions scheduled for each participant in the EX group. In addition, participants in the EX group will receive recommendations to perform unsupervised exercise on two additional days per week. During these sessions, they will be encouraged to walk at light-to-moderate intensity and to perform core exercises at home. To facilitate monitoring of walking activity, participants will be asked to carry their mobile phone with a step-counting application.
Qualitative Study Design and Data Collection
Participants allocated to the EX group will be offered the opportunity, on a fully voluntary basis and following completion of the exercise intervention, to participate in a semi-structured, in-depth interview. Qualitative interviews will explore the participants’ experiences and engagement with the exercise programme, perceived effects on overall health, and perceived barriers and facilitators, as well as the personal meaning attributed to physical activity and sport. All interviews will be conducted face-to-face, audio-recorded with consent, and transcribed verbatim. NVivo software (QSR International) will be used for data management and coding. Content analysis, as described by Smith and Sparkes (2017), will be applied to analyse the data, 61 and information saturation will be used as a criterion for discontinuing data collection and/or analysis. 62
Endpoints
The primary endpoint will be the between-group difference in change in CRF from T0 to T2, assessed by VO2peak measured objectively using an ergospirometric treadmill test. The secondary endpoints will include between-group differences from T0 to T2 in sociodemographic variables, muscle power (Power Frail test), frailty (Power Frail test, Frailty Trait Scale, Fried Frailty Phenotype), physical condition (MSWT), upper body strength (handgrip dynamometry), body composition (bioelectrical impedance analysis), physical activity levels (GPAQ and accelerometery), sleep quality (Epworth Sleepiness Scale and accelerometery), QoL (HM-PRO), fatigue (EORTC QLQ-FA13), and biochemical biomarkers (inflammatory, haematological, endocrine-nutritional, and immunosenescence markers).
Sample Size and Statistical Analysis
The sample size for the study was calculated to ensure a sufficient number of participants to detect statistically significant differences in VO2peak between the control and intervention groups at the end of the intervention, which constitutes the primary objective of the study, with adequate statistical power. The calculation was based on results from a similar trial. 63 To achieve 80% power to detect differences in mean VO2peak between groups at a two-sided significance level of 5%, assuming a mean (SD) of 25.2 (9.1) in the TAU group and 29.4 (8.6) in the EX group, and a ratio of participants in the TAU group to the total sample of 50%, a minimum of 72 participants per group will be required. Based on findings from a previously unpublished pilot study indicating a loss to follow-up of approximately 30%, but assuming a lower attrition rate in the present population, losses are expected not to exceed 20%. Accordingly, the planned recruitment target is 90 participants per group, yielding a total sample size of 180 participants.
To address additional secondary objectives, a descriptive and exploratory interim analysis is planned once 50% of recruitment has been completed (i.e. 90 participants). This interim analysis is not intended for hypothesis testing or modification of the primary analysis. This sample size will allow the development of a predictive equation to estimate CRF (VO2peak) using the MSWT and other covariates related to body composition and heart rate. Following the general guideline of a minimum of 10 observations per predictor, a sample of 90 individuals would permit the inclusion of up to nine predictors in a linear regression model.
Statistical analyses will include descriptive analyses, data quality assessments, evaluation of the efficacy of primary and secondary outcomes, and assessment of intervention safety. As deviations from the protocol may occur during the study, analyses will be conducted using both intention-to-treat and per-protocol approaches. Missing data will not be imputed. Analyses will be conducted using a complete case analysis approach. The extent and patterns of missing data will be transparently described and reported.
All hypothesis tests related to the primary outcome will be performed using a significance level of 0.05. Thus, the null hypothesis (H0) will be rejected when the p-value is less than 0.05, corresponding to a type I error rate of 5%. The primary outcome is confirmatory in nature. All secondary outcomes and subgroup analyses are considered exploratory and hypothesis-generating; therefore, no adjustment for multiple comparisons will be applied to these analyses.
Descriptive analyses will be conducted for all study variables. Categorical variables will be summarised as frequencies and percentages, while continuous variables will be presented as mean and standard deviation when normally distributed, or as median with 25th and 75th percentiles when normality assumptions are not met.
A participation analysis will be performed to compare baseline characteristics between responders and non-responders.
To evaluate the effect of the 20-week exercise intervention on CRF and other continuous outcomes, the primary analytical approach will consist of between-group comparisons of mean values (control vs intervention) at the end of the intervention, using independent t-tests or non-parametric equivalents as appropriate. For categorical variables, Pearson’s chi-square test will be used, or Fisher’s exact test when assumptions are not met.
To assess intervention effects over time, linear mixed-effects models will be applied as a secondary analytical approach to explore the temporal evolution of outcomes across repeated measurements. These models will include participant-specific random effects to account for correlations arising from repeated measures. Time-by-treatment interactions will be examined, and models will be adjusted for relevant confounding variables such as age and sex, selected based on their clinical relevance. In addition, lymphoma subtype (e.g. HL, diffuse large B-cell lymphoma, indolent NHL, including follicular and marginal zone subtypes) and planned chemotherapy protocol will be included as explanatory variables to account for clinical heterogeneity in the study population.
The inclusion of different lymphoma subtypes and chemotherapy regimens reflects the real-world clinical setting. The primary aim of the study is to compare the intervention versus control group, rather than to estimate subtype-specific effects. Accordingly, heterogeneity is not ignored, but modelled statistically through covariate adjustment, and any findings related to lymphoma subtype or treatment regimen will be considered exploratory and hypothesis-generating rather than confirmatory.
Subgroup analyses will also be conducted to explore whether intervention efficacy differs between men and women, and between participants aged 70 years or older and those younger than 70 years. These subgroup analyses are exploratory and not powered to provide definitive subgroup-specific conclusions.
All statistical analyses will be performed using R software (version 3.5.0) and SPSS (version 29.0 or later).
Potential Benefits for Participants
All participants will receive a comprehensive physical and functional assessment, together with personalised follow-up providing emotional support throughout treatment. This project offers an opportunity to improve the health of people with lymphoma undergoing chemotherapy through a structured exercise programme designed to prevent losses in CRF and muscle strength, thereby reducing the risk of frailty and early fatigue.
Feasibility, Potential Risks and Burdens for Participants
The feasibility and safety of exercise interventions in patients with haematological malignancies undergoing chemotherapy have been supported by the literature. A previous systematic review reported no indication of long-lasting harm attributable to exercise, independent of the modality employed, and noted good to excellent retention rates across included studies, suggesting that participants who engage in exercise programmes experience meaningful benefits and remain motivated throughout. 64 These findings have been corroborated by a more recent systematic review and meta-analysis, confirming that exercise interventions were either feasible or associated with high participation rates in this population. 65 Consistent with this evidence, the EDONOLA intervention has been designed with a multi-layered individualisation framework to maximise both safety and tolerability, as has been presented previously.
The primary potential risks associated with participation relate to the clinical treatment itself, including chemotherapy-related fatigue and immunosuppression, which may increase susceptibility to infection when attending supervised exercise sessions or using shared facilities. To mitigate these risks, the study will implement infection-prevention strategies, including postponing exercise sessions for participants presenting with fever or signs of infection, and limiting training groups to a maximum of four participants with fixed group composition to minimise exposure networks. These measures are consistent with recommendations derived from exercise trials in haematological malignancies. 64 Secondary potential risks relate to the exercise intervention and include musculoskeletal effects (e.g. delayed-onset muscle soreness, muscle strains, or exacerbation of pre-existing musculoskeletal conditions), as well as transient increases in heart rate and blood pressure. These risks will be minimised by the highly individualised progression of the exercise programme, close supervision by qualified exercise specialists, and ongoing adaptation to participants’ day-to-day treatment-related effects.
Discussion
In the era of ‘precision medicine’, in which treatments are tailored to specific diseases, physical exercise as a lifestyle-modulating intervention in cancer care is increasingly recognised as a necessity. 66 Exercise therefore functions as a powerful, personalised therapeutic strategy rather than merely a supportive measure, by improving treatment effectiveness (e.g. enhancing chemo- and immunotherapy efficacy and reducing side effects such as fatigue and cachexia) and by promoting favourable long-term outcomes, including reduced recurrence risk and improved QoL.67,68 Nevertheless, further research is required to define optimal exercise prescription parameters for haematological malignancies, such as lymphoma, across different phases of treatment.
This project represents an innovative initiative aligned with Sustainable Development Goal 3 (Good Health and Well-Being), promoting health and well-being through a multidisciplinary approach that integrates medical care with structured physical exercise. The programme is designed to support people with lymphoma undergoing chemotherapy, with the dual objective of improving patient health outcomes and reducing the burden on the healthcare system. Through a tailored exercise intervention, the study aims to alleviate treatment-related symptoms, preserve CRF and muscular strength, and prevent the development of frailty and early fatigue. By enhancing treatment tolerance and reducing toxicity-related complications, the intervention is expected to improve chemotherapy adherence and decrease hospital admissions and emergency care utilisation.
Achieving these objectives requires close coordination beyond the healthcare sector to address relevant social determinants of health and ensure adequate patient support.
Several limitations of the EDONOLA trial warrant acknowledgment. First, as with most exercise oncology trials, the present study is susceptible to selection bias. Participants who consent to enrol in a structured exercise programme during active chemotherapy are likely to differ systematically from those who decline, potentially being more motivated or less burdened by treatment-related side effects, which may limit the generalisability of findings to the broader lymphoma population. However, it is important to contextualise this concern within the specific clinical reality of the EDONOLA population. Patients diagnosed with lymphoma and undergoing active chemotherapy are granted sick leave for the duration of their treatment, which substantially reduces the occupational time constraints that represent the primary barrier to exercise participation in otherwise healthy or working populations. Moreover, a particularly relevant subgroup consists of participants aged 70 years or older, who, by definition, are largely retired and therefore entirely free from occupational commitments. In this sense, to partially address the broader selection bias concern, the protocol incorporates broad eligibility criteria across both HL and NHL subtypes, explicitly includes older participants (>70 yrs) as a target subgroup, and combines supervised with unsupervised sessions to accommodate varying levels of capacity and availability. Furthermore, the qualitative component of the study exploring participants’ perceived barriers, facilitators, and engagement with PA will provide direct insight into the factors shaping participation and dropout, thereby informing the interpretation of any differential adherence patterns and strengthening the external validity of the findings. Second, given the nature of the exercise intervention, blinding of participants is not feasible. As an open-label study, participants will be aware of their allocation to either the intervention or TAU group, which may influence their motivation, adherence, and self-reported outcomes. This issue is inherent to behavioural and exercise-based interventions. However, the inclusion of objective measures, such as accelerometry and CRF assessed by VO2peak measured objectively using an ergospirometric treadmill test, will complement and validate subjective assessments, thereby strengthening the evaluation of the intervention’s effectiveness. Third, the possibility of participant dropout during the 20-week programme, particularly given the clinical context of active chemotherapy, has been anticipated and accounted for in the sample size calculation by incorporating an estimated attrition rate. Finally, the present study protocol does not include a long-term follow-up beyond the 20-week post-intervention assessment. Although it is plausible that the effects of the exercise programme on CRF, fatigue, frailty, and QoL may persist or evolve, the present study is not designed to capture these longer-term outcomes. Hence, future studies are warranted to examine the sustainability of exercise-induced benefits in patients with lymphoma over longer periods.
Conclusions
The findings of this study may contribute to the development of complementary care models operating alongside traditional healthcare pathways, grounded in multi- and interdisciplinary interventions. Such an approach would encourage collaboration across policy areas, leverage specialised expertise, and ultimately improve population health outcomes while promoting more efficient use of public healthcare resources.
Footnotes
Ethical Considerations
The study protocol was approved by Euskadi’s Medicine Research Ethics Committee (CEIm-E) (19 September 2024, version 2; 27 January 2025, version 2.1) under the internal code PI2024133. Written informed consent will be obtained from all patients entering the study by medical personnel at the participating institutions.
Author Contributions
Resources: SMM, IZE, AVGV, EGG, Supervision: SMM, IZE, MTE, Biogipuzkoa Clinical Research, Validation: Biogipuzkoa Clinical Research, Visualization: Biogipuzkoa Clinical Research, Writing-original draft: SMM, IZE, MMRZ, JMM, Writing-review & editing: SMM, IZE, MMRZ, JMM, MTE, AVGV, EGG, Biogipuzkoa Clinical Research, Conceptualization: SMM, IZE, MMRZ, JMM, Data Curation: IZE, MMRZ, JMM, MTE, Biogipuzkoa Clinical Research, Formal Analysis: Biogipuzkoa Clinical Research, Funding acquisition: SMM, IZE, Investigation: Smm, IZE, Mmrz, JMM, Mte, AVGV, Egg, Methodology: SMM, IZE, MMRZ, JMM, MTE, Biogipuzkoa Clinical Research, Project administration: Biogipuzkoa Clinical Research. The manuscript is submitted with the consent of all contributing authors. All authors met the criteria for authorship: contributed to the concept and design of the protocol; drafted the article; and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Department of Health of the Basque Government Health Research and Development Projects Programme (2023111073).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
ClinicalTrials.gov ID: NCT06660446 (last update: 2024, May 11).