
Abstract
In low- and middle-income countries (LMICs), leadership in cancer prevention and control is often concentrated among a small number of key individuals across the cancer continuum. While these leaders are crucial to system development, insufficient succession planning and mentorship mean that over-reliance on individuals places cancer prevention and control at risk of disruption during leadership transitions. Grounded in a critical synthesis of the field, this Perspective examines succession planning and mentorship in cancer prevention and control, highlighting how fragile leadership pipelines, the “missing middle” of mid-career professionals, and informal mentorship cultures and structural inequities, weaken system continuity and resilience. The article further examines barriers to effective mentorship in LMICs and proposes strategies centered on institutionalized mentorship, inclusive approaches, and distributed leadership to strengthen continuity and sustainable development of cancer prevention and control systems. A stable leadership structure requires collaboration across career stages, with senior leaders contributing institutional memory and strategic judgement, mid-career professionals anchoring operational delivery and governance, and early-career professionals contributing innovation and fresh perspectives. Importantly, we advocate for succession planning and mentorship to be institutionalized as core functions of cancer systems, rather than left to individual goodwill, to enable this collaborative structure to sustain leadership continuity and resilience.
Cancer prevention and control in low- and middle-income countries (LMICs) depends not only on funding, technology and infrastructure, but also on the people who lead and sustain these systems over time. Who leads, how leadership is transferred and whether the next generation of leaders are ready: these questions remain largely unaddressed. This perspective examines why succession planning and mentorship remain largely informal and individually driven in cancer prevention and control in LMICs, and what it would take to change that. It also considers how structural inequities, particularly those affecting women and other under-represented groups, shape access to mentorship, succession pathways and leadership throughout the cancer workforce.
The Leadership Dilemma
Across LMICs, governments and health systems are stepping up efforts to strengthen cancer prevention and control. However, these investments have a better chance of succeeding if they go hand in hand with developing and sustaining the people who keep cancer prevention, screening, early diagnosis, treatment, survivorship, palliative care, research and cancer registration programs alive, among others. In these settings, progress and innovation in cancer control tend to rely on fragile leadership pipelines, where only a few passionate individuals sustain momentum. These leaders are invaluable as they inspire, advocate and drive change in challenging healthcare environments. However, there is an inherent risk when reliance falls disproportionately on the same individuals with little to no succession planning in place. 1
Challenges to Sustainable Cancer Leadership in Low- and Middle-Income Countries
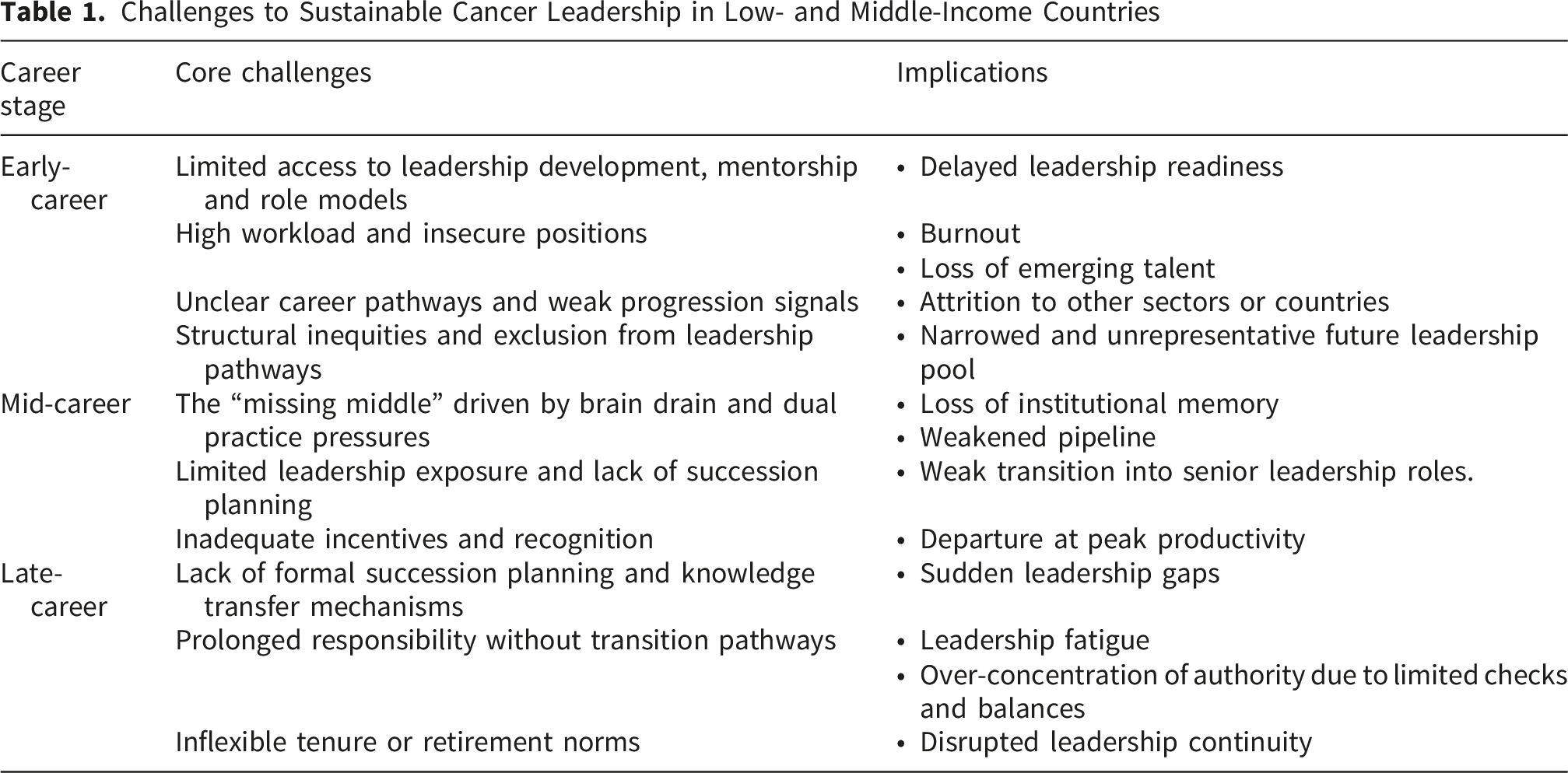
Ironically, some long-standing leadership customs may be part of the problem in the LMICs where it is not uncommon to appoint healthcare professionals to very senior leadership roles in their final years before retirement, often as a gesture of appreciation for long service. 4 Although this practice may reflect respect for seniority and experience, it can limit opportunities for forward-looking reform, structured knowledge transfer and preparation of future leaders. Another structural weakness is the hourglass-shaped workforce, in which cancer programs have many junior staff and a small number of senior leaders, but too few mid-career professionals. This may largely be attributed to both external brain drain1,5 and dual practice pressures, where mid-career specialists are stretched between public service and private practice, often alongside competing midlife responsibilities and family or financial obligations, leading to their withdrawal from the institutional mentoring and leadership roles necessary for a stable pipeline 6 (Table 1). This “missing middle” may also be compounded by earlier progression bottlenecks. In broader leadership literature, the “broken rung” describes the unequal first step into management, particularly for women, which narrows the pool available for later leadership progression. The concern in LMICs is nonetheless wider, with an actual thinning of the mid-career layer through attrition, competing professional pressures and weak succession pathways. When this mid-career layer is thin, early career professionals may be thrust prematurely into leadership roles, which can be problematic as their lack of experience and mentorship may lead to sub-optimal performance, or an inability to eventually become good mentors themselves as this has not been modelled for them. 7
Why Succession Planning and Mentorship Matter
Robust cancer control structures benefit from a balanced mix of early-, mid- and late-career professionals across key functions of the cancer continuum, although the exact composition will vary by setting, service level and available workforce capacity.
8
We propose a framework to transcend traditional hierarchies, showing how a balanced professional mix ensures a self-sustaining cycle of leadership and institutional memory (Figure 1). This balance helps cancer systems sustain quality and equity through predictable shocks, such as leadership transitions as well as unexpected disruptions. In LMIC settings, mid-career leaders play a critical bridging role, both receiving mentorship from senior colleagues and serving as role models for early career professionals. For instance, translation of modern innovations such as HPV self-sampling,
9
into effective cancer-control strategies depends not only on the technology itself but critically on intergenerational exchange. This dialogue ensures that new strategies are anchored in the institutional memory of senior and mid-career leaders, encompassing lessons on community acceptability and hard-won failure knowledge from previous national rollouts that early-career professionals have not yet had the opportunity to acquire. This prevents the erosion of systemic knowledge while facilitating a more deliberate and resilient transfer of leadership where succession is shaped by shared experience rather than administrative handover alone. Mentorship and succession planning as an intergenerational ‘continuity system’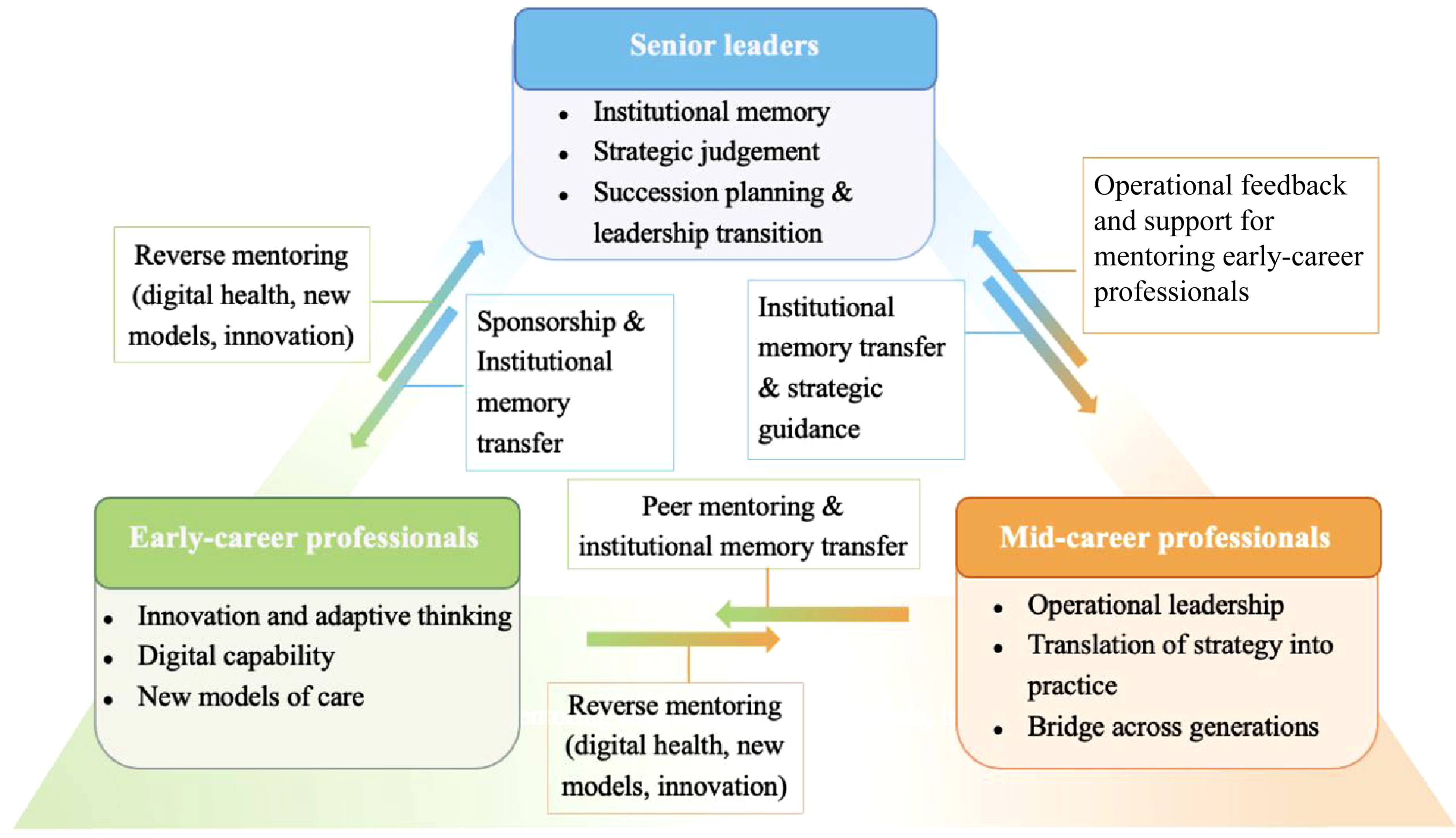
Central to the discussion is understanding that succession planning and mentorship are integral to the resilience of cancer programs. Consciously cultivating an ecosystem that nurtures emerging leaders, supports mid-career development and preserves and values the wisdom of senior mentors should therefore be a health system priority in LMICs. The challenge lies in intentionally balancing these interconnected stages.
It is important to acknowledge that senior leaders possess profound experience and wisdom that were forged from years of navigating complex challenges in cancer care and control. These leaders would have overcome many setbacks and witnessed cancer care and public health evolve. 10 Their knowledge as such may extend beyond medical textbooks, making them well qualified to offer deep insights into local cancer epidemiology, cultural nuances, political dynamics and practical strategies for working with constrained resources. 6 Sidelining these senior leaders erodes institutional memory and weakens the very systems they helped build.
Meanwhile, the mid-career professionals tend to occupy a precarious space. Often considered too experienced to be “emerging”, and yet not always fully recognized as senior, they risk being overlooked in leadership strategies. Regardless, their contributions are essential as they are often the most operationally active and closest to the realities on the ground. Their dual capacity to both receive and provide mentorship makes them uniquely valuable to the pipeline. Investing in this group is critical in LMICs for continuity and the long-term strength of leadership pipelines in health systems.
Equally important is creating space for early career professionals, whose minds are ready to innovate, ask new questions and bring fresh energy to prevailing problems and challenges in cancer control in LMIC such as late-stage diagnosis, 11 financial toxicity, 12 lack of access to lifesaving cancer treatments and supportive care gaps. 13 They also tend to be well equipped with technological savviness, novel perspectives and willingness to challenge the status quo. Supporting early career professionals with these qualities is crucial for the evolution and sustainability of any cancer control programs, for without a vibrant and supported line-up of talent that is ready for leadership roles, cancer systems in LMICs risk a deepening leadership crisis.
Intergenerational collaboration therefore needs to be built intentionally. A balanced leadership structure is achieved when senior leaders contribute institutional memory, networks and strategic judgement; mid-career professionals translate this experience into operational delivery and governance; and early career colleagues bring innovation, digital capability and adaptive problem-solving (Figure 1). For example, the implementation of primary care-led palliative services can be operationalized through this intergenerational synergy: early-career professionals provide the digital fluency needed to manage home-based symptom monitoring and medication tracking; mid-career professionals draw on their proximity to communities to mobilize compassionate community networks as a practical solution to the limitations of operational budgets; 14 while senior leaders apply the institutional memory and political capital needed to navigate the opiophobia embedded in legislation that routinely stalls even well-designed programs. 15
Ultimately, none of this happens by accident. Structured succession planning is what creates the conditions for intergenerational collaboration to take root and endure.
Challenges to Effective Mentorship and Leadership Development in LMICs
Challenges and Recommended Strategies for Effective Mentorship in Low- and Middle-Income Countries

Beyond structural barriers, relational and cross-setting factors tend to fragment the mentorship landscape.(Table 2) Hierarchical cultures for instance may result in irregular and unstructured feedback, leaving mentees with unclear expectations and limited guidance. Also, mentorship that is siloed within clinical, research or policy domains can restrict cross-sector exposure such as between civil society organizations, clinical services, and public health and policy, which is required for holistic leadership development.
Cross-setting dynamics present a further layer of complexity. It is common for mentees from LMICs to pair with mentors from high-income countries (HICs) to accelerate their professional growth as well as open doors for brokered opportunities including fellowships and research grants that they otherwise may not have access to. However, such mentorships can potentially be problematic given the inherent power asymmetry. Mentees from LMICs for example may internalize the ‘foreign gaze’, which prioritizes HIC agendas.17,18 As a result, they could end up approaching local problems through an external lens that inadvertently diminishes the value of local expertise and priorities. Cross-border mentorship must therefore be reframed as equitable, co-owned partnerships where the professionals in LMICs drive the agenda to ensure that they are anchored on local cancer burden, prevention opportunities and health system capabilities (Table 2).
A major challenge further relates to gender equity, particularly women’s access to mentorship and leadership roles in cancer care and control. Our work from the Lancet Commission on Women, Power and Cancer has shown how gender norms, unequal caregiving responsibilities, harassment and subtle discrimination may collectively constrain women’s access to mentorship as well as leadership trajectories, even in fields where women are highly represented such as nursing. 19 We also uncovered that women remain under-represented in senior oncology positions and in key cancer system leadership positions including national cancer control planning, directorships of cancer centers and registry leadership, reflecting both conscious and unconscious bias. We also see evidence from Africa, highlighting barriers faced by women oncologists namely limited mentorship and sponsorship, exclusion from informal networks where opportunities are shared and inadequate institutional support to reconcile professional responsibilities with family life. Similar constraints have also been reported among women working in public health leadership roles in cancer prevention and control 20 (Table 2). These barriers do not simply limit individual careers. They narrow the succession pipeline itself and weaken the mentorship ecosystem that cancer systems in LMICs depend on.
It is worth noting that several of these challenges are not unique to LMICs. Their consequences are however particularly acute in cancer-control settings where leadership pipelines are thinner, institutional buffers are weaker and the loss of even a small number of key individuals can disrupt system continuity.
In sum, mentorship and leadership that does not explicitly address gender or other forms of structural inequity in fact risks reproducing existing inequities in the next generation. When framed as “gender-blind” or “color-blind”, 21 the status quo may be reinforced as opportunities tend to flow towards those who already resemble current mentees or leaders rather than towards a deliberately diverse cadre that reflects the communities they serve. A resilient cancer leadership pipeline therefore has to be intentionally inclusive, with safe and supportive environments where the disadvantaged and other under-represented groups can access mentors, build networks and be visible as leaders across the cancer system. 22
Strategies for Sustainable, Inclusive Mentorship and Leadership
Building resilient, inclusive cancer leadership pipelines demands action on multiple fronts, from dismantling structural barriers to cultivating the intentional mentorship and succession cultures that cancer systems in LMICs so urgently need.
A culture of sustainable leadership in cancer control begins with openly giving recognition where it is due. When applied fairly across all ranks, recognition can serve as a very powerful strategy for establishing vibrant cancer leadership pipelines in LMICs. Celebrating senior champions who built foundational cancer services, while recognizing the contributions of mid-career professionals who keep programs alive and running, and actively recognizing rising stars help in motivating aspiring leaders and allaying concerns about being overlooked by the system. Ultimately, such actions not only set the tone for how institutions should value both legacy and potential, but also help normalize leadership transition as a natural and positive evolution, and not a threat.
Creating meaningful value around mentoring efforts is equally paramount. As a first step, mentorship should be incorporated into leadership key performance indicators (KPIs) for heads of clinical departments, public health units, academic institutions, research centers and civil society organizations (Table 2). This may include ‘counting’ efforts to support early-career professionals be it through project supervision, structured skills training, co-leading multidisciplinary meetings, leading screening campaigns or planned succession discussions. At its heart, institutionalizing mentorship serves to send strong signals that developing future cancer leaders is part of a leader’s responsibility and not an optional act of goodwill
1
(Figure 2). Strategies to promote effective mentorship and cancer leadership in low- and middle-income countries
Furthermore, structured collaboration and joint leadership opportunities help reinforce shared ownership. Examples include co-authoring institutional position papers on cancer service delivery or screening reforms, leading guideline development processes together or mandating research funding applications that pair experienced leaders with early- or mid-career professionals. These joint endeavors allow developing leaders to gain real experience while anchoring their efforts in institutional memory and collaborative guidance.
Cancer systems must also intentionally retain and support mid-career professionals 23 It must be remembered that their role as institutional memory-holders, role models and future-ready leaders is crucial for stability. Succession planning efforts need to include structured career development pathways, leadership exposure and incentives that keep this group engaged within the organization. This is particularly important in LMIC contexts where underemployment coexists with workforce shortages and where internal and external brain drain quietly erodes capacity.
Among these strategies, reverse mentoring may be the most radical, which is precisely its strength as it invites a deliberate and necessary shift in hierarchy (Figures 1 and 2). Beyond promoting openness and intergenerational learning, 24 it also allows early career professionals to guide senior colleagues on fast-evolving areas such as digital health, artificial intelligence, tele-oncology and implementation science. Such practices represent a fundamental shift in how we understand leadership, expertise and institutional adaptability in modern cancer care and control. 25
Cancer systems in LMICs must also actively guard against deeper structural barriers that can sabotage these efforts namely discriminatory norms and practices. Ageism poses a threat. By undervaluing the insights of older professionals or dismissing the credibility of younger voices, it can erode the foundation of meaningful intergenerational collaboration. Gender bias, racism and other forms of discrimination are also threats that shrink the pool of potential leaders. Addressing these ultimately requires genuine commitments from health systems in LMICs to establish clear anti-discrimination policies, equitable promotion pathways, transparent selection processes for leadership roles and mentorships, as well as an institutional culture that values diverse contributions across all career stages, disciplines and genders 26 (Figure 2). Complementing this, training in inclusivity and respectful communication reinforces the everyday behaviors needed to sustain these shifts.
Ultimately, placing the burden of mentoring and leadership on isolated leaders is the biggest pitfall to avoid in cancer systems in LMICs. It must be remembered that fostering broad networks of champions distributes responsibility and helps prevent burnout (Figure 2). This also strengthens knowledge sharing, peer support and collective problem-solving across clinical, public health and community settings. 27 As illustrated in the ‘continuity system’ (Figure 1), peer mentoring and consistent operational feedback help ensure that leadership is a distributed and collaborative effort rather than a solitary burden.
Moving Forward by Building a Culture of Continuity in Cancer Control
In conclusion, succession planning and mentorship in cancer systems across LMICs cannot rest on the shoulders of a few dedicated individuals. Organizational commitment to formal succession planning and structured mentorship is critical to addressing long-standing vulnerabilities in these systems. This means deliberately cultivating an ecosystem where mentorship is structured, succession is planned and both are institutionally embedded as core functions of cancer systems, rather than left to individual goodwill. These efforts must be consciously inclusive, ensuring women and other under-represented groups can grow into their potential across the full spectrum of cancer care and control. Ultimately, getting leadership succession and mentorship right is not just about protecting programs; it is about better patient care, stronger health systems and the long-term well-being of entire nations.
Footnotes
Author Contributions
NBP and NH conceived the paper and wrote the first draft. Y.Z. and NBP developed the figures and tables. All authors contributed to critical revision of the manuscript and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No primary data were generated or analysed in this study.