
Abstract
Introduction
Mantle cell lymphoma (MCL) constitutes an aggressive subtype of B-cell lymphoma and demonstrates significant clinical and biological heterogeneity. B symptoms are important clinical indicators in tumors. In the present study, we investigated the frequency and prognostic significance of B symptoms among different primary sites of MCL.
Method
We conducted an observational study of 2,025 MCL patients from the SEER database. We analyzed the frequency of B symptoms at different primary sites and evaluated their impact on prognosis.
Results
The highest incidence of B symptoms was observed in the small intestine (35.29%), and the lowest in the nasopharynx (6.67%). Among patients with primary lymph node involvement, the intrathoracic and abdominal lymph nodes showed the highest proportion of B symptoms (both 40%), while the head, face, and neck lymph nodes showed the lowest (9.3%). In patients with primary site involvement of lymph nodes or nasopharynx, those with B symptoms had a worse prognosis than those without B symptoms (P < 0.05). Similarly, patients with primary lesions involving multiple regional lymph nodes, lymph node not otherwise specified (NOS), or inguinal/leg lymph nodes exhibited worse prognosis when B symptoms were present (P < 0.05).
Conclusion
In summary, our study highlights the heterogeneity in both the frequency and prognostic significance of B symptoms across different primary sites in MCL patients.
Introduction
Mantle cell lymphoma (MCL) represents a mature B-cell subtype of non-Hodgkin lymphoma and is recognized as an aggressive malignancy with marked clinical and biological heterogeneity. MCL accounts for approximately 5-7% of all malignant lymphomas and predominantly occurs in older men. 1 MCL can involve lymph nodes as well as extranodal organs throughout the body, typically presenting with lymphadenopathy or symptoms associated with extranodal involvement, such as abnormal blood cells in bone marrow infiltration, splenomegaly and tonsillar enlargement, or gastrointestinal polyposis.2-5 MCL exhibits substantial clinical heterogeneity, varying from indolent disease that can remain untreated for years to highly aggressive forms associated with poor survival outcomes. 6 Therefore, identifying the heterogeneity of clinical manifestations in MCL is crucial for optimizing risk stratification and selecting appropriate therapeutic strategies.
Patients with MCL can clinically manifest B symptoms, including fever, excessive sweating, and weight loss. Such symptoms are commonly accompanied by elevated inflammatory indicators, such as IL-6 and CRP, and may be present in various pathological conditions. In clinical practice, the presence of B symptom is often easily overlooked. However, B symptoms serve as an important clinical indicator in tumors, particularly in the classification and prognostic assessment of lymphomas. Therefore, greater attention should be paid to the role of B symptoms in MCL. Previous studies have reported varying frequencies of B symptoms in MCL patients.7-10 However, no systematic investigation has comprehensively evaluated the frequency of B symptoms across different primary sites in MCL.
Numerous studies have demonstrated that B symptoms are important clinical manifestations in lymphoma and are closely associated with prognosis.11-14 The transformation of follicular lymphoma into an aggressive disease state is often characterized by the development of B symptoms and represents a major cause of disease-related mortality. 15 Previous studies have reported that B symptoms are associated with worse prognosis in NHL, although inconsistent findings have also been reported.16,17 In MCL, growing evidence suggests that patients with B symptoms tend to experience poorer clinical outcomes.18-20 Nevertheless, it remains unclear whether the frequency and prognostic significance of B symptoms differ according to the primary site of MCL involvement. Therefore, in the present study, we analyzed the frequency of B symptoms and their prognostic association across different primary sites in MCL.
Materials and Methods
Data Source and Patient Selection
Our observational study utilized the SEER database (https://seer.cancer.gov/) to extract clinical information on lymphoma patients and identify eligible MCL cases. A total of 5,798 patients with confirmed MCL were initially identified from the SEER database. Patients were sequentially excluded for following reasons: age of 0 years (n=1), unknown B symptom status (n=3,682), unknown surgical history (n=1), and primary sites that were neither extranodal nor lymph node sites (n=89). A total of 2,025 MCL patients with primary extranodal or lymph node involvement were retained after exclusions for subsequent analysis, including 1,670 cases with primary lymph node involvement and 355 with primary extranodal involvement (Supplemental Figure 1). The variables collected in this study comprised age, sex, race, marital status, and household income. Tumor stage, treatment modalities, and primary tumor sites were also collected. The age range of included patients was 15-99 years. Other racial groups included American Indians, Asians, Alaska Natives, and Pacific Islanders. The married group included married individuals and those cohabiting without marriage, whereas the unmarried group included divorced, separated, and widowed individuals.
The final study cohort included 2,025 patients, who were classified into two groups based on whether B symptoms were present. Among these patients, 1,670 MCL cases with different primary lymph nodes sites were further screened, and baseline characteristics were analyzed using the same approach. The proportions of MCL patients with B symptoms at different primary sites and different primary lymph node sites was calculated. Overall survival (OS) was selected as the main study endpoint and calculated as the duration from diagnosis to death from any cause or most recent follow-up. The reporting of this study conforms to the RECORD statement. 21 All patient information was de-identified prior to analysis.
Statistical Analysis
R software (v4.3.0) was applied for data analysis and visualization. Baseline characteristic tables for MCL patients with different primary sites were generated using the tableone R package. The ggpubr package was used to generate lollipop charts. Clinical baseline variables and the distribution of B symptoms were analyzed with the Chi-square test. The Kaplan–Meier method was applied to investigate the prognostic significance of B symptoms in MCL patients with different primary and lymph node sites, based on the survival and survminer R packages. Overall survival between groups was compared using the log-rank test, and P < 0.05 was considered statistically significant.
Results
Clinical Baseline Characteristics of MCL Patients
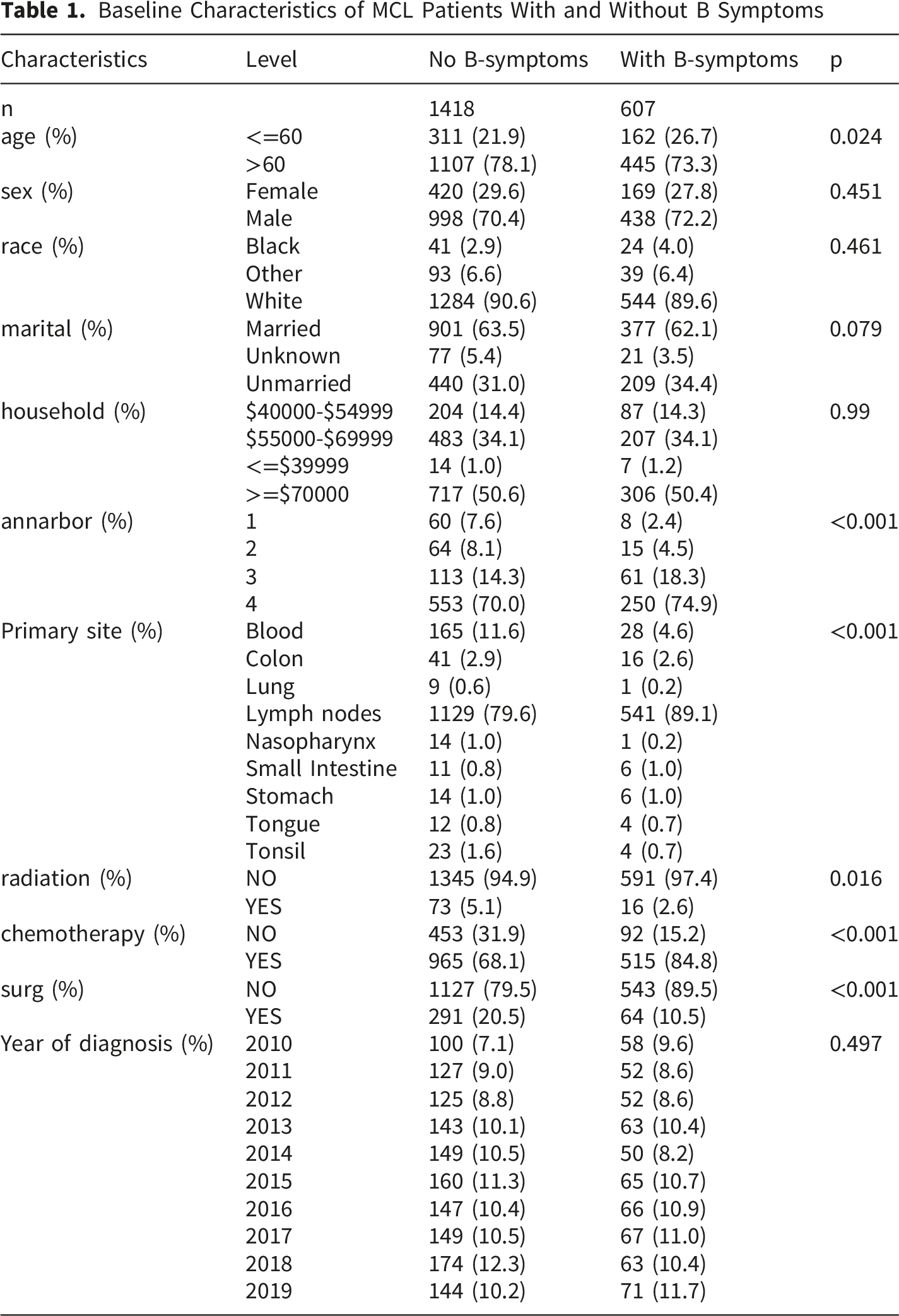
Baseline Characteristics of MCL Patients With and Without B Symptoms
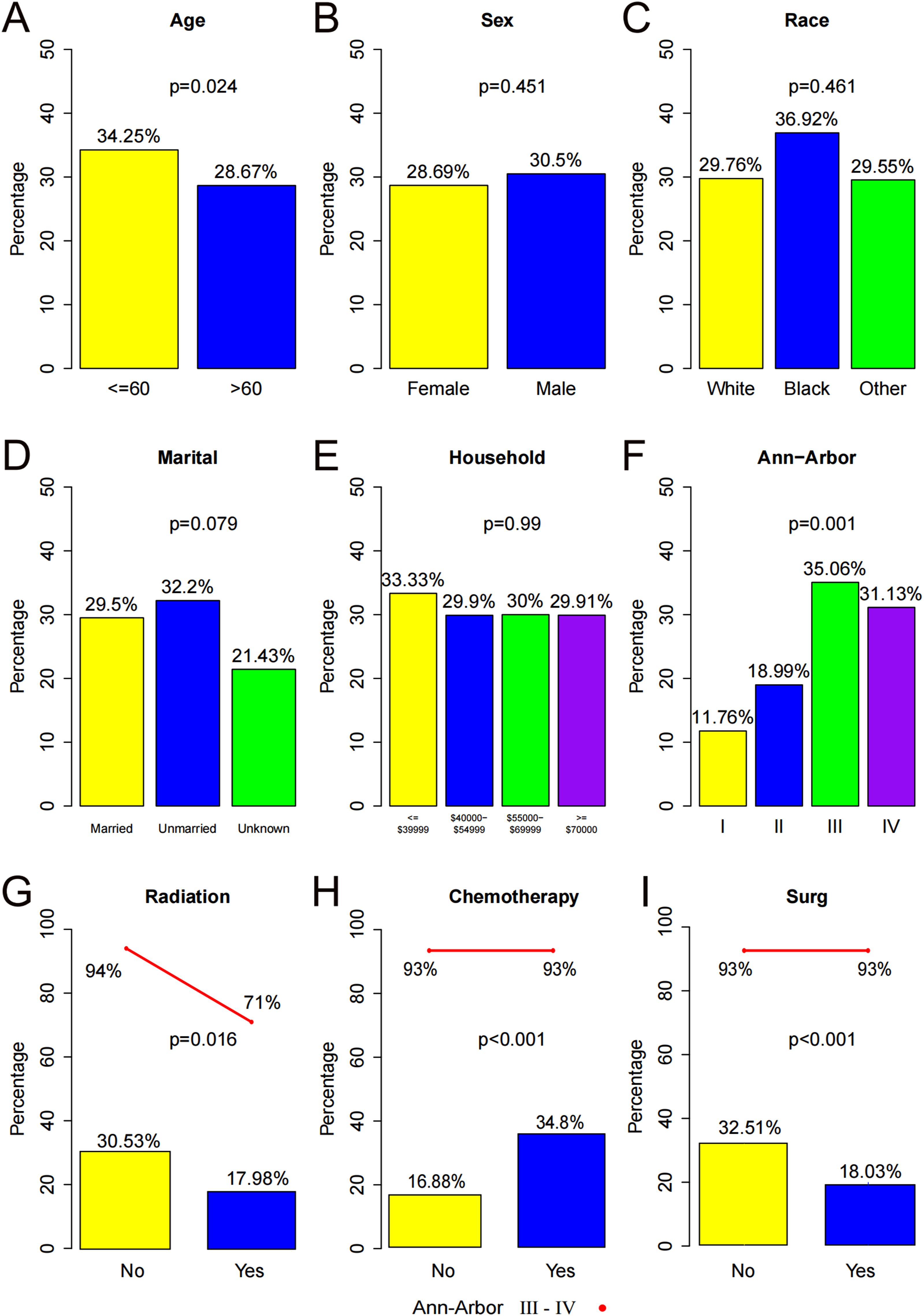
Proportion of baseline features in MCL patients with B symptoms. (A-I) Percentage of MCL patients with B symptoms by age, sex, marriage, household income, Ann−Arbor stages, radiation therapy, chemotherapy, surgery
Among the total MCL cohort in the SEER database, we further screened 1,670 patients with primary lymph node involvement and analyzed the clinical characteristics of different primary lymph node sites (Supplemental Table 1). Patients were similarly divided into B-symptoms and non-B-symptoms groups. The two groups showed no significant differences in age, sex, marital status, household income, or surgery status (Supplemental Table 1, all P > 0.05). However, significant differences were identified in race, Ann-Arbor stage, primary site, chemotherapy, and radiotherapy (Supplemental Table 1). White patients (483 cases) exhibited a higher proportion of B symptoms (P = 0.048). Compared with patients with stage I (2 cases) and stage II disease (14 cases), patients with stage III disease (57 cases) or more advanced disease showed a higher frequency of B symptoms (P = 0.001). Among MCL patients with B symptoms, the proportion of patients without radiotherapy (530 cases) was significantly higher than that of patients receiving radiotherapy (11 cases) (P < 0.004). Conversely, the proportion of patients receiving chemotherapy (466 cases) was significantly higher than that of patients without chemotherapy (75 cases) (P < 0.001).
Percentage of MCL Patients With B Symptoms at the Different Primary Sites
We further examined the frequency of B symptoms across different primary sites in MCL. According to the primary site, MCL patients were categorized into nine subtypes, including lung, nasopharynx, tongue, small intestine, stomach, tonsil, colon, bone marrow, and lymph node involvement (Figure 2A–B). Significant differences were observed in the distribution of B symptoms among these primary sites (Figure 2A–B, P < 0.001). The frequency of B symptoms varied substantially among different sites. Higher frequencies of B symptoms were observed in MCL originating from the tongue (4 cases, 25%), colon (16 cases, 28.07%), stomach (6 cases, 30%), lymph nodes (541 cases, 32.4%), and small intestine (6 cases, 35.29%), with the small intestine showing the highest frequency, followed by lymph nodes. In contrast, B symptoms were less frequent in MCL originating from the nasopharynx (1 case, 6.67%), lung (1 case, 10%), bone marrow (28 cases, 14.51%), and tonsil (4 cases, 14.81%), particularly in the nasopharynx. Among these sites, tongue-origin MCL exhibited the lowest proportion of Ann-Arbor stage III–IV disease. Percentage of MCL patients with B symptoms at the different primary sites. A, The Y axis represents percentage B, The primary site with B symptoms corresponds to the mark on the body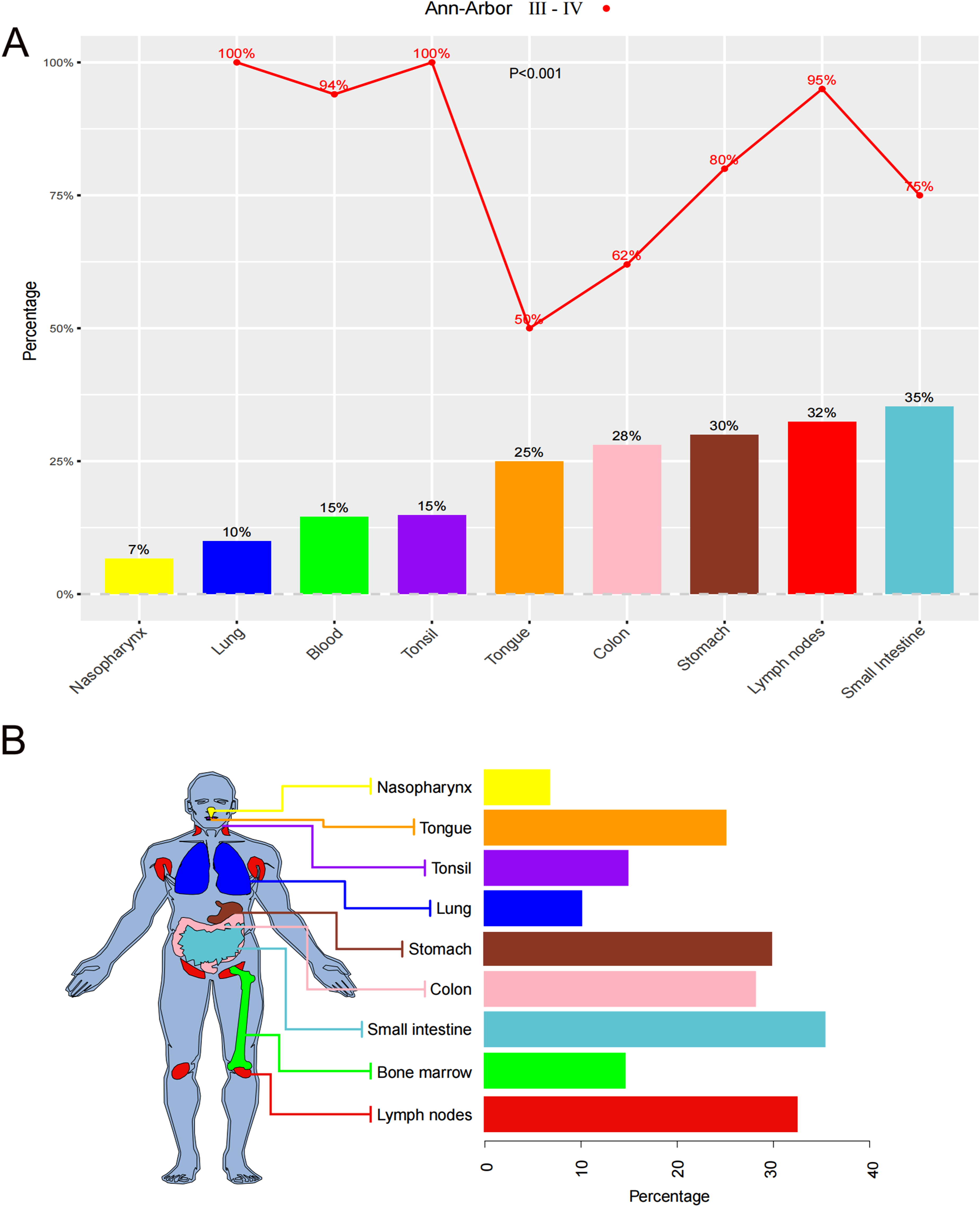
We also investigated the frequency of B symptoms across different primary lymph node sites in MCL patients. According to the anatomical location of primary lymph node involvement, patients were categorized into seven subgroups: multiple regional lymph nodes, lymph node not otherwise specified (NOS), inguinal/leg, head and neck, intrathoracic, abdominal, and axillary/arm lymph nodes (Figure 3A–B, P < 0.001). The frequency of B symptoms also differed markedly among primary lymph node sites. B symptoms were most frequently observed in patients with intrathoracic lymph node involvement (8 cases, 40%) and abdominal lymph node involvement (24 cases, 40%). In contrast, lower frequencies of B symptoms were found in lymph nodes involving the axilla or arm (4 cases, 13.33%), head, face and neck (8 cases, 9.3%), and inguinal region or leg (8 cases, 19.51%), with the head, face and neck region showing the lowest frequency. Moreover, the proportions of Ann-Arbor stage III–IV disease were significantly higher in lymph node NOS and lymph nodes of multiple regions compared with other lymph node locations. Percentage of MCL patients with B symptoms at the different primary lymph node sites. (A) The Y axis represents percentage. (B) The primary lymph node site with B symptoms corresponds to the mark on the body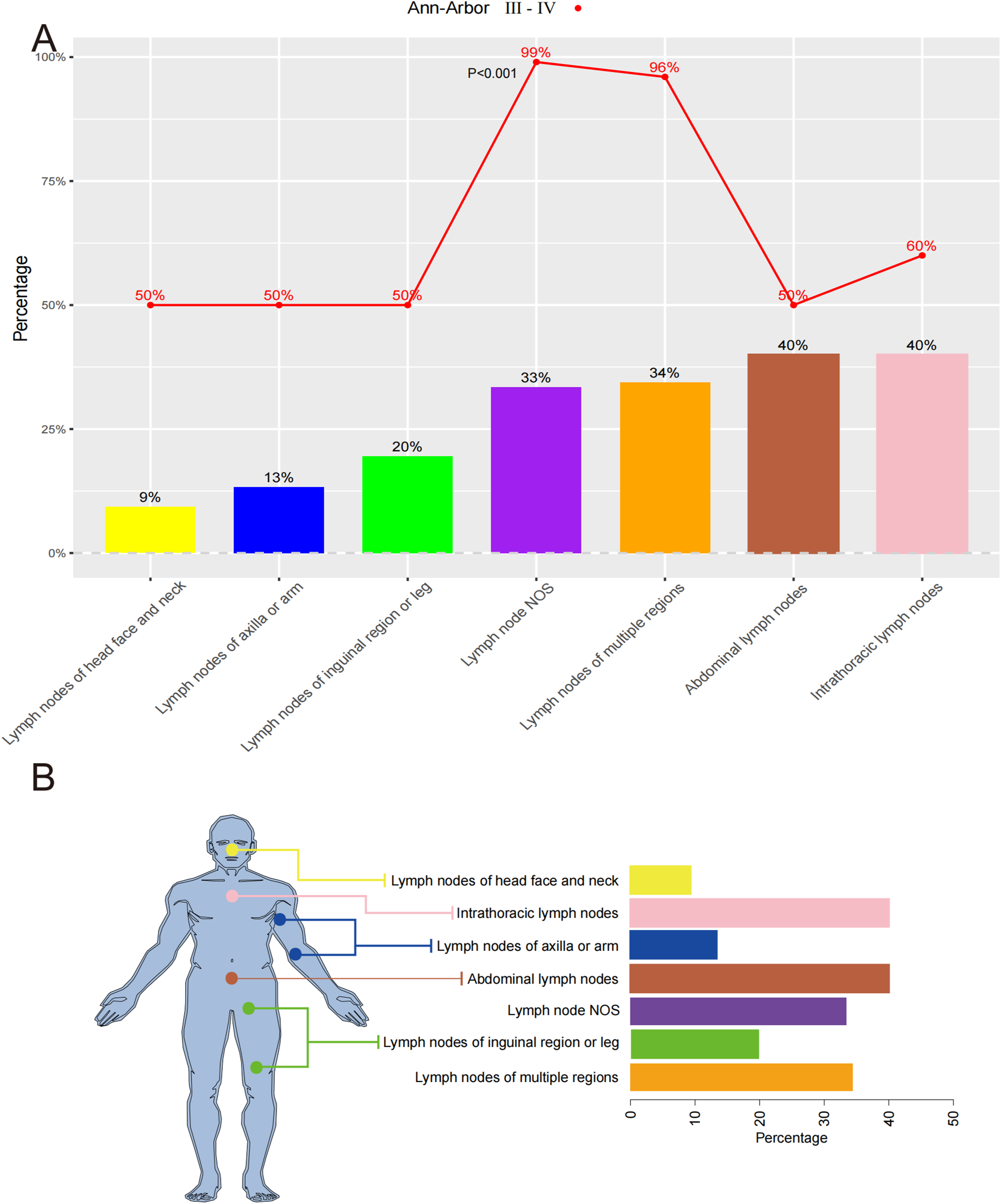
Prognostic Significance of B Symptoms in MCL Patients With Different Primary Sites
To investigate the association between B symptoms and survival outcomes in MCL patients with different primary sites, Kaplan–Meier survival analyses were performed (Figure 4A–C). Patients with B symptoms had significantly worse overall survival than those without B symptoms among MCL patients with lymph nodes as the primary site (Figure 4A, P < 0.0001). Similarly, MCL patients with nasopharyngeal involvement who presented with B symptoms exhibited worse prognosis than those without B symptoms (Figure 4B, P = 0.027). However, among patients with other primary sites, including bone marrow, tonsil, tongue, lung, stomach, small intestine, and colon, no significant differences in overall survival were observed between patients with and without B symptoms (Figure 4C, all P > 0.05). Association of B symptoms with survival in MCL patients at different primary sites. The X-axis indicates time (months), while the Y-axis indicates survival probability. (A-B) Kaplan-Meier curve analysis predicts worse OS in MCL with B symptoms at lymph nodes and nasopharynx. (C) Kaplan-Meier curve showed no difference in OS between MCL patients with and without B symptoms in different primary sites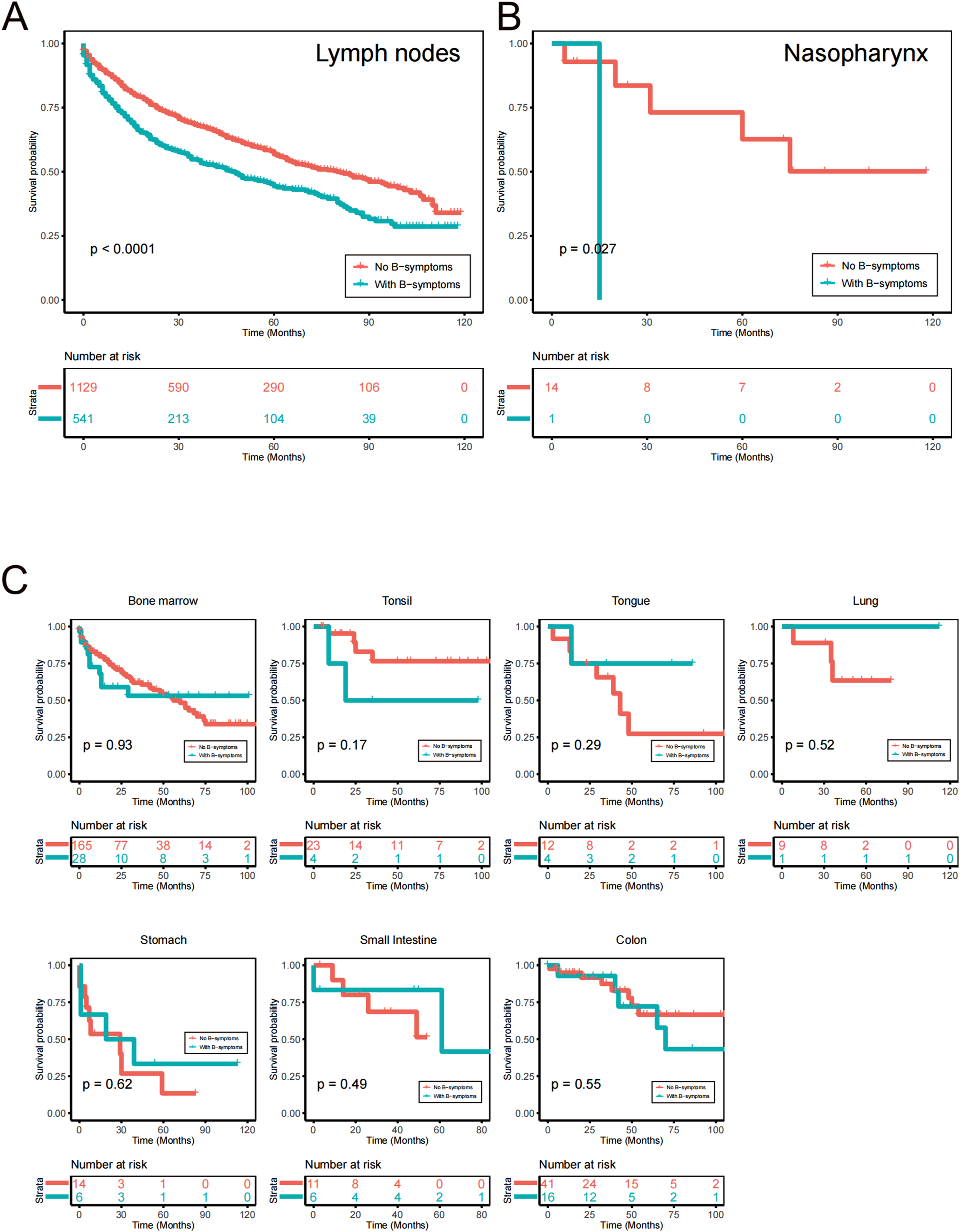
We further explored the prognostic significance of B symptoms in MCL patients with different primary lymph node sites (Figure 5A–B). Among the seven analyzed lymph node subtypes, B symptoms were significantly associated with worse survival in patients with involvement of multiple lymph node regions, lymph node NOS, and inguinal/leg lymph nodes (Figure 5A, all P < 0.05). By contrast, prognosis did not differ significantly between patients with and without B symptoms at other primary lymph node sites, including the head and neck, intrathoracic, abdominal, and axillary or arm lymph nodes (Figure 5B, all P > 0.05). Association of B symptoms with survival in MCL patients with different primary lymph nodes. The X-axis indicates time (months), while the Y-axis indicates survival probability. (A) Kaplan-Meier curve showed that MCL with B symptoms predicted worse OS in different primary lymph nodes sites. (B) Kaplan-Meier curves showed that no difference in OS between MCL with and without B symptoms in different primary lymph node sites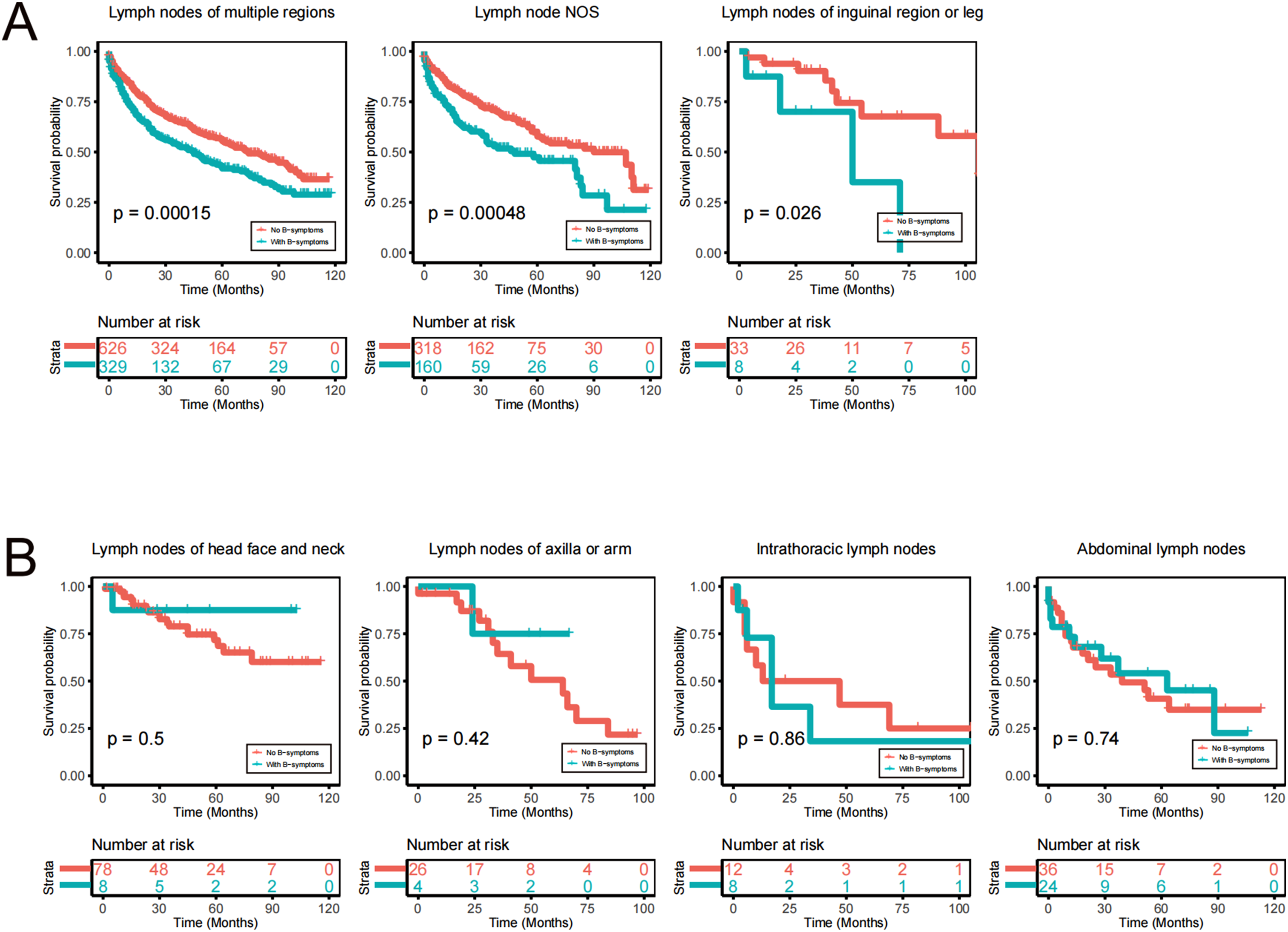
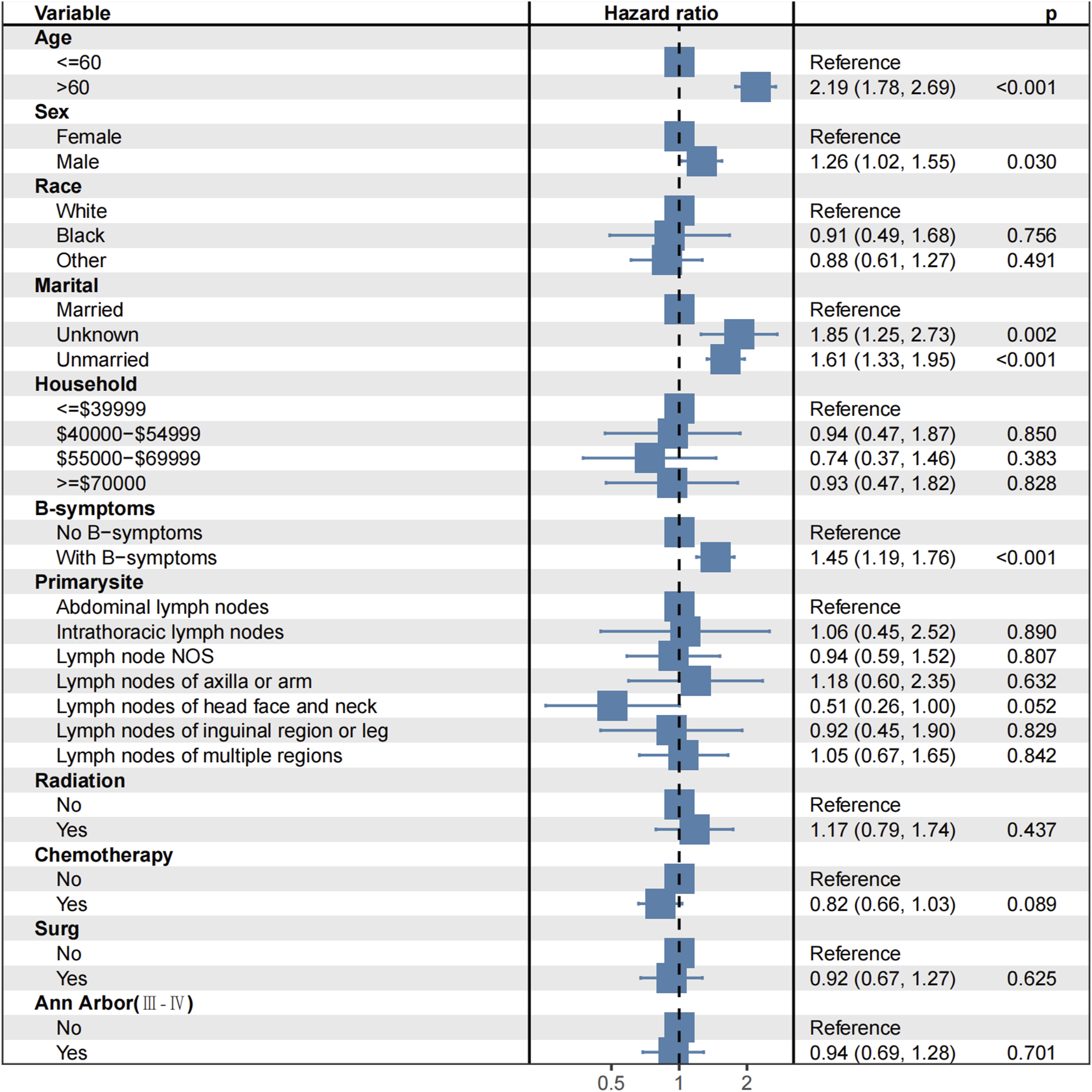
Furthermore, multivariate analyses were performed using clinical variables including age, B symptoms, primary extranodal and nodal sites, radiotherapy, and chemotherapy (Figures 6 and 7). The results demonstrated that patients with B symptoms had significantly poorer prognosis than those without B symptoms. In addition, patients aged >60 years and unmarried patients also exhibited worse prognosis, with significantly increased hazard ratios (P < 0.001). However, no statistically significant association was identified between primary site and prognosis in MCL patients (P > 0.05). Multivariate Survival Analysis of clinical data from patients with primary extranodal MCL Multivariate Survival Analysis of clinical data from patients with primary nodal MCL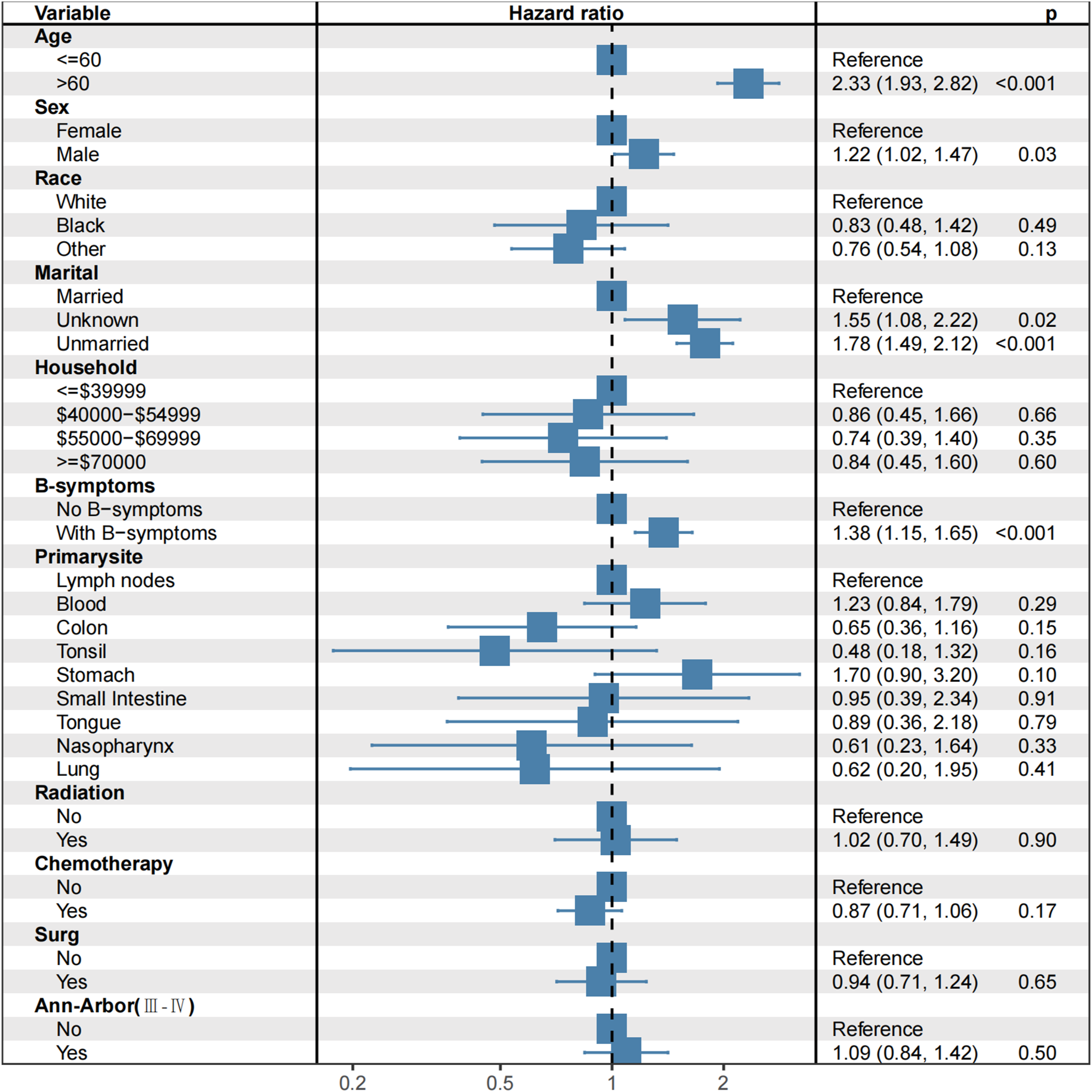
Discussion
Our study comprehensively analyzed the heterogeneity in the frequency and prognostic significance of B symptoms among MCL patients with different primary sites using a cohort of 2,025 patients. Previous studies have suggested that older patients aged ≥60 years present with B symptoms more frequently than younger MCL patients. 22 However, our study showed that B symptoms were more frequently observed in MCL patients aged ≤60 years than in those older than 60 years. Most MCL patients are diagnosed at Ann-Arbor stage III or IV when symptoms appear or when multiple lymph node lesions are present. Previous studies have reported that over 80% of MCL cases are identified at advanced stage III–IV disease. 23 Consistent with these findings, our results demonstrated that patients with stage III–IV disease exhibited a higher proportion of B symptoms. In addition, our analysis showed that most MCL patients with B symptoms received systemic chemotherapy, whereas fewer patients underwent local treatment modalities such as radiotherapy or surgery. Since no significant difference in disease stage was observed between patients receiving chemotherapy and those undergoing surgery, we speculate that the lower use of local treatment approaches may reflect the need for systemic treatment in patients presenting with B symptoms.
Previous studies have reported that the frequency of B symptoms in MCL ranges from 22.4% to 64.8%.8,9,24 In our dataset, the overall proportion of B symptoms was lower than the previously reported 64.8%, which may be attributable to differences in sample size, population characteristics, or geographic distribution. Importantly, our comprehensive analysis revealed substantial heterogeneity in the frequency of B symptoms across different primary extranodal sites. Among extranodal sites, the highest incidence of B symptoms was observed in the small intestine (35.29%), whereas the lowest incidence was found in the nasopharynx (6.67%). To date, the relationship between Ann-Arbor stage and primary extranodal sites in MCL patients with B symptoms has not been clearly established. We speculate that the small intestine, as a major component of the digestive system with a unique immune and microenvironmental milieu, may more readily trigger systemic inflammatory responses and subsequently increase the occurrence of B symptoms. In contrast, the relatively confined anatomical structure of the nasopharynx may contribute to the lower frequency of systemic symptoms. The gastrointestinal tract is one of the most commonly involved extranodal organs in MCL. 25 Previous studies reported that B symptoms occurred in 32.4% of patients with gastrointestinal MCL and that the frequency of B symptoms was generally lower than that observed in nodal MCL.24,26 However, our results further demonstrated heterogeneity within gastrointestinal involvement itself. Specifically, the frequency of B symptoms in primary small intestinal MCL was higher than that in nodal MCL, whereas the frequencies in colon and stomach involvement were lower than those observed in lymph node-origin MCL. These findings suggest that even within gastrointestinal MCL, the biological and clinical characteristics associated with B symptoms may differ according to the involved anatomical site.
We also identified significant heterogeneity in the frequency of B symptoms among different primary lymph node sites. In nodal MCL, high frequencies of B symptoms were primarily observed in abdominal, intrathoracic, and multi-regional lymph node involvement. Further analysis showed that MCL patients with intrathoracic lymph node involvement had a higher proportion of stage III–IV disease than those with superficial lymph node involvement. This may be related to the deeper anatomical location of thoracic lymph nodes, which are less accessible for early detection, resulting in delayed diagnosis and a higher frequency of B symptoms at advanced stages. In contrast, superficial lymph node regions, such as the head, face, neck, and axillary regions, exhibited lower frequencies of B symptoms, possibly because palpable lymph node enlargement facilitates earlier diagnosis before systemic symptoms develop. To our knowledge, this is the first study to systematically characterize the frequency of B symptoms across different primary extranodal and lymph node sites in MCL, highlighting the substantial site-specific heterogeneity of B symptoms in this disease.
The prognostic significance of B symptoms in MCL has been reported previously. Some studies demonstrated that B symptoms were associated with inferior survival in univariate analysis but lost significance after multivariate adjustment. 27 In our multivariate Cox analysis, however, B symptoms remained independently associated with poor prognosis, together with older age and unmarried status. In contrast, primary site itself was not independently associated with prognosis. Previous studies have also demonstrated that B symptoms are important prognostic indicators in MCL and may improve prognostic stratification when incorporated into established prognostic indices.18-20,28 Nevertheless, our findings further suggest that the prognostic value of B symptoms differs according to the primary site of involvement. In the present study, B symptoms were associated with significantly poorer survival in MCL patients with primary lymph node or nasopharyngeal involvement. Although B symptoms were relatively uncommon in nasopharyngeal MCL, their presence appeared to indicate particularly adverse prognosis. Previous studies reported that MCL originating from the head and neck or gastrointestinal tract generally presents with fewer B symptoms and better survival outcomes than nodal MCL.26,29 However, whether the prognostic differences among different primary sites are directly related to the presence of B symptoms has remained unclear. In our cohort, although gastrointestinal MCL exhibited relatively high frequencies of B symptoms, particularly in the small intestine, B symptoms were not significantly associated with prognosis in gastrointestinal involvement. These findings suggest that the prognostic impact of B symptoms may depend not only on their presence but also on the biological characteristics of the involved primary site.
Further subgroup analysis of primary lymph node sites demonstrated additional heterogeneity in the prognostic significance of B symptoms. Specifically, the occurrence of B symptoms predicted inferior prognosis in patients with involvement of multiple regional lymph nodes, lymph node NOS, and inguinal or leg lymph nodes. In contrast, no significant prognostic association was observed in patients with head, neck, intrathoracic, abdominal, axillary, or arm lymph node involvement. These findings indicate that the prognostic implications of B symptoms vary considerably across different nodal sites in MCL.
Several limitations of this study should be noted. First, a formal sample size calculation was not carried out, as all eligible SEER patients were incorporated into the study; however, the final cohort of 2,025 patients provided sufficient statistical power for the primary analyses. Second, due to the inherent limitations of the SEER database, detailed information regarding chemotherapy regimens, treatment intent, progression-free survival, performance status, lactate dehydrogenase levels, and other variables required to calculate the MIPI was unavailable. Therefore, clinically relevant endpoints such as POD24 could not be evaluated, and comprehensive adjustment for established prognostic indices was not feasible. Third, B symptoms were recorded only as a composite binary variable in the database, without separate documentation of fever, night sweats, or weight loss. Moreover, B symptoms in clinical practice may also be influenced by infection or other non-malignant conditions. Consequently, we were unable to determine which specific component contributed most strongly to the observed prognostic associations. Future prospective studies incorporating detailed treatment information, individual B symptom components, inflammatory biomarkers, and comprehensive prognostic indices are warranted to further validate the prognostic significance of B symptoms in MCL and to clarify their role in predicting disease progression.
Conclusions
Our study demonstrated substantial heterogeneity in both the frequency and prognostic significance of B symptoms across different primary sites in MCL. Patients with nodal involvement, particularly abdominal and intrathoracic lymph nodes, as well as those with gastrointestinal involvement, exhibited relatively high frequencies of B symptoms. Moreover, the prognostic impact of B symptoms varied according to the primary site of disease involvement. These findings highlight the potential value of incorporating site-specific assessment of B symptoms into prognostic evaluation and clinical management strategies for MCL patients.
Supplemental Material
Supplemental Material - A Comprehensive Landscape of B Symptoms in Mantle Cell Lymphoma Reveals Heterogeneity Associated With Different Primary Sites
Supplemental Material for A Comprehensive Landscape of B Symptoms in Mantle Cell Lymphoma Reveals Heterogeneity Associated With Different Primary Sites by Fan Yang, Ying Song, Qihui Li, Chaoling Wu, Min Li, Chao Chen, Changjian Yan, Qizhao Long, Jinyuan Xiao, Xiaoni Liu, Xiaoyu Hao, Yuqi Zhang, Wenxin Qi, Yan Liu, Jing Wang, Mingxia Zhu, Ping Yang, Xiaoliang Yuan, Yuansheng Lin, Zining Yu, Hongmei Jing, Weilong Zhang in Cancer Control.
Footnotes
Ethical Considerations
This study used de-identified SEER data; therefore, it did not involve human or animal subjects and no informed consent was required, consistent with the Declaration of Helsinki for retrospective analyses.
Author Contributions
WLZ, HMJ, YSL and ZNY conceived the project. FY, YS, QHL, CLW and ML analyzed the data. FY, YS, QHL, CLW, ML, CC, CJY, QZL, JYX, XNL, XYH, YQZ, WXQ, YL, JW, MXZ, PY, XLY, ZNY, HMJ, and WLZ contributed towards the interpretation of the data. All authors wrote and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by National Natural Science Foundation of China; 81800195, Beijing Physician Scientist Training Project (BJPSTP-2025-06), Peking University Medicine plus X Pilot Program-Artificial Intelligence and Medical Development Initiative (BMU2025YXXLHAIYX022), Natural Science Foundation of Beijing, China (L241076), Key Clinical Projects of Peking University Third Hospital (BYSYZD2019026 and BYSYZD2023014), Beijing Xisike Clinical Oncology Research Foundation (Y-NCJH202201-0049), the special fund of the National Clinical Key Specialty Construction Program, P. R. China (2023).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data analyzed in this study were obtained from the SEER database (![]() ). SEER data are publicly available upon request and approval from the SEER program. The authors confirm that they had no special access privileges. All code used for analysis is available from the corresponding author upon reasonable request.
). SEER data are publicly available upon request and approval from the SEER program. The authors confirm that they had no special access privileges. All code used for analysis is available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.