
Abstract
Introduction
Surveillance of at-risk populations for pancreatic ductal adenocarcinoma (PDAC) is a potential strategy to reduce its incidence and improve its prognosis. However, there is considerable debate about who should participate and relatively little information about how people perceive different testing options.
Methods
Using the Health Belief Model as a framework, this qualitative, observational study including eleven focus groups and seven interviews, summarizes the knowledge, motivations, barriers and preferences for PDAC surveillance in underserved populations with low cancer screening rates and for high-risk individuals (HRI).
Results
HRIs have a high motivation to participate in PDAC screening and perceive few barriers to engage. Participants from underserved populations had little knowledge of PDAC and surveillance, but they were interested in surveillance for PDAC based on their perception of the benefits of cancer screenings. The main barriers for participation in PDAC surveillance programs were cost, distrust of the larger medical system, discomfort associated with the testing, lack of a provider’s recommendation, and fear of a positive result. These barriers varied based on a person’s race/ethnicity and geographic location (urban vs. rural). Preferences expressed by underserved populations suggest that tests for early PDAC detection will need to be accurate, no or low cost, minimally invasive, and convenient to access. There was a correlation between a person’s self-perceived susceptibility for PDAC and their willingness to tolerate more invasive and less convenient methods. In addition, participants were motivated to participate in early detection programs with clear guidelines accompanied by their doctor’s recommendations.
Conclusion
There appears to be an association between actual and perceived risk of PDAC and patient willingness to participate in an early detection program. For populations lower along the risk spectrum, there is limited knowledge about pancreatic cancer or its risk factors, and potentially significant barriers to participate in an early detection program if deemed eligible.
Plain Language Summary
Surveillance of at-risk populations for pancreatic cancer (PDAC) is a potential strategy to reduce its incidence and improve its prognosis. However, there is considerable debate about who should participate and relatively little information about how people perceive different testing options. Using the Health Belief Model as a framework, this qualitative study, including eleven focus groups and seven interviews, summarizes the knowledge, motivations, barriers and preferences for PDAC surveillance in underserved populations with low cancer screening rates and for high-risk individuals (HRI). We found that HRIs have a high motivation to participate in PDAC screening and perceive few barriers to engage. Participants from underserved populations had little knowledge of PDAC and surveillance, but they were interested in surveillance for PDAC based on their perception of the benefits of cancer screenings. People who lost a family member due to cancer also felt susceptible to PDAC and were more motivated to participate. The main barriers for participation in PDAC surveillance programs were cost, distrust of the larger medical system, discomfort associated with the testing, lack of a provider’s recommendation, and fear of a positive result. These barriers varied based on a person’s race/ethnicity and geographic location (urban vs. rural). Preferences expressed by underserved populations suggest that tests for the early detection of PDAC will need to be accurate, no or low cost, minimally invasive, and convenient to access. There was a correlation between a person’s self-perceived susceptibility for PDAC and their willingness to tolerate more invasive and less convenient methods. In addition, people were motivated to participate in early detection programs that had clear guidelines accompanied by their doctor’s recommendations. This study should inform the development and dissemination of novel PDAC detection tests that might be applied to at-risk patient populations.
Keywords
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is the fourth most common cause of cancer death in the United States, with one of the lowest survival rates of all cancers. 1 A primary reason for the high mortality rate is that PDAC is largely undiagnosed until the advanced stages due to the lack of specific symptoms. In addition, people have low knowledge of risk factors, and the benefit of PDAC screening programs remains unproven.2-5 Fortunately, there are some promising developments for surveillance options that may improve early diagnosis and treatment of PDAC, especially for high-risk groups.6,7
Since the prevalence of PDAC is low, routine screening of the general population is not considered feasible by the United States Preventative Services Taskforce. However, there is an ongoing effort to define HRIs who might benefit from screening. To date, the most widely accepted HRIs are those with genetic risk, intraductal papillary mucinous neoplasm (IPMN), or familial risk which is typically defined as two or more relatives with PDAC and one of these being first-degree. 8 Up to 15% of PDAC cases are due to hereditary risk, either from known genetic cancer predisposition syndromes or familial risk without a known genetic cause. 5 To expand upon this minority of incident cancer cases, another high-risk cohort may include a subgroup of individuals with new onset diabetes, though this remains under investigation.9,10 Compared to the general population risk of 1.5%, people with risk related to familial or hereditary factors face up to a 3–8-fold increase in risk for developing PDAC. 11
Developing effective surveillance programs to detect early-stage PDACs may help increase the survival rate. 7 As there are no blood tests approved for the early detection of PDAC, surveillance of at-risk populations is usually based upon imaging with endoscopic ultrasound (EUS), magnetic resonance imaging (MRI), or both.12,13 With substantial interest in the development of blood-based tests for the early detection of PDAC, including PDAC multi-cancer early detection tests, 14 it will be critical to understand when people are willing to pursue regular screenings, including their motivations, barriers and preferences for different screening modalities.
In one qualitative study, Lewis 15 interviewed individuals at high-risk for PDAC and found that knowledge about PDAC surveillance was low, but people were interested, particularly when tests were “easy, fast, doctor-recommended, inexpensive, and accurate.” Cost was the most significant barrier identified by research participants, followed by invasiveness, inconvenience and avoidance-type personality. In other studies, individuals with a greater perceived risk or experience caring for a loved one with cancer were more receptive towards participation, yet perceptions of risk didn’t always correspond with a high-risk designation.15-17
There is little knowledge about how race affects PDAC surveillance motivations or barriers due to the lack of diversity in these studies.8,17 One aim of this study is to define PDAC motivations and barriers to participation in early detection programs in patient populations who are often underrepresented in other cancer screening programs. A secondary aim was to compare their opinions against those of patients who have already been defined as high-risk for PDAC and who are actively or considering participation in PDAC surveillance.
Methods
Study Population Characteristics
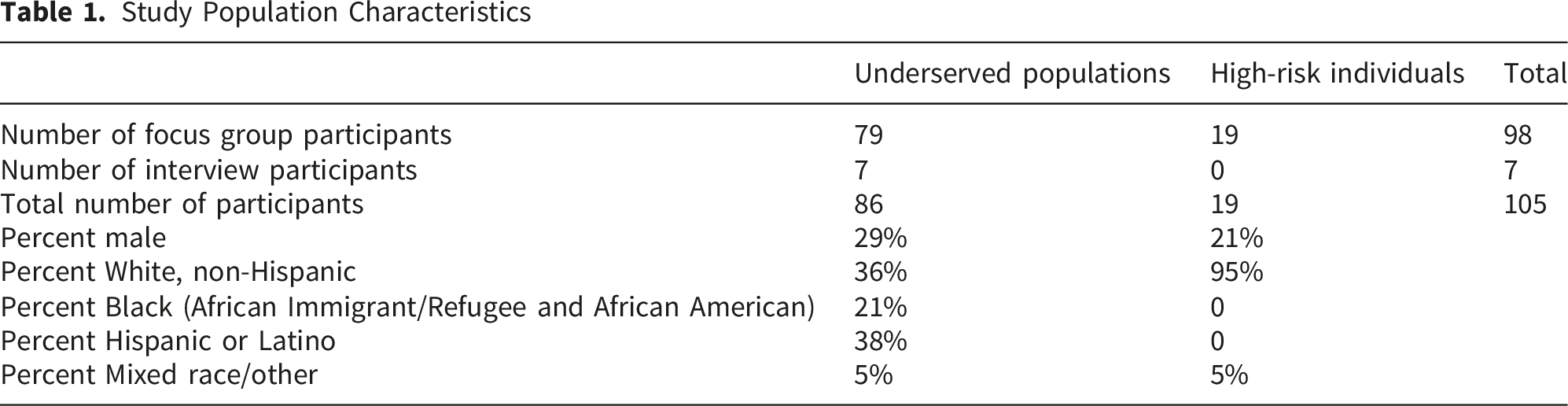
Participants were purposively sampled for this research in two groups: HRIs and underserved populations with low screening rates. The high-risk focus group participants were recruited from Oregon Health & Science’s (OHSU) High-Risk PDAC Clinic. The Clinic provided a list of 22 HRIs who live in a tri-county region of the State and had been seen at the Clinic at some point or regularly participated in high-risk surveillance. 19 HRIs agreed to participate in a focus group. Approximately five people joined per group.
Participants from underserved communities, were recruited from regions and communities with higher cancer incidence and lower screening rates. 19 These included Black and African American populations, Hispanic and Latino populations, and people from rural counties in Oregon. Recruitment for the underserved populations was enabled by the community partners and networks of OHSU’s Community Outreach, and Engagement (COE) team and enhanced using the Health Oregon Project research cohort. 20
This study was approved by OHSU’s Institutional Review Board (Study #00025950). The focus groups took place in community spaces such as libraries. All participants verbally consented to participate after the facilitator reviewed the information sheet with each person and answered their questions. Verbal consent was recorded on a written document by the study team. Each individual received a $50 gift card for participating. The average duration for the focus groups was 1.5 hours. All interviews and focus groups were audio-recoded and transcribed verbatim into English. One of the audio recordings for a Spanish language focus group malfunctioned, and we relied on our notes for this discussion. The transcripts were thematically analyzed with ATLAS.ti. Codes based on the Health Belief Model were defined a priori, while others emerged from an inductive approach to coding.
The interview guide and analysis framework was designed by a multi-disciplinary team consisting of COE researchers and pancreatic cancer researchers. The focus groups were facilitated by COE researchers who live and work in their own communities. The analysis was conducted by three qualitative researchers from the COE team who have experience analyzing cancer studies. About a quarter of the transcripts were coded collaboratively, and the rest were individually coded by these same three members with frequent meetings to review the codebook and iteratively derive central themes. 21 Data saturation was achieved at inter-group level to clearly define the patterns between HRIs and underserved populations. 22 Participants have been de-identified in the manuscript and clean verbatim transcription has been used to improve readability and protect participant privacy. The reporting of this study conforms to the COREQ guidelines. 23
Health Belief Model
The Health Belief Model (HBM) is the theoretical framework that guides this study. This validated model is useful for explaining and predicting screening behaviors for the uptake of mammograms, prostate-specific antigen (PSA) analysis, and colonoscopy, and has been recently used for PDAC surveillance programs.8,17 Six factors comprise the health belief model, as adapted to the context of this study: 1) perceived susceptibility to PDAC, 2) perceived severity of PDAC, 3) perceived benefits of early detection of PDAC, 4) perceived barriers to participation in a surveillance program, 5) self-efficacy in program uptake, and 6) cues to action to begin participation in a surveillance program. 24
According to the HBM, individuals conduct an internal cost-benefit analysis, considering these six factors when they make their decisions about whether to undergo a particular screening (for any condition). 25 For example, when the perceived risks are high (susceptibility and severity), and the perceived barriers are low, the model predicts that people will be motivated to participate. The model also predicts that individuals who feel they are more susceptible to PDAC will be more willing to undergo more invasive imaging modalities like EUS, which requires sedation. 16 In a study with individuals at higher risk for PDAC, Underhill (2019) found people felt a moderate perceived susceptibility to PDAC and believed that it was a serious disease. Their high motivation for participating in a surveillance program enabled them to overcome the discomfort and dread that some people experience with MRI- or EUS-based surveillance.
Results
Study Population Characteristics
A total of 98 people participated in this research including 79 participants from underserved populations and 19 HRIs. While the HRI group was 95% White, non-Hispanic, the underserved population group was only 36% White, non-Hispanic. Both groups were more than 70% female.
Severity
Among rural and minority participants without specific risk for PDAC, most had little to no knowledge of PDAC. The few people who had some knowledge either had a single family member with PDAC or referred to a celebrity: Steve Jobs, Patrick Swayze, or Alex Trebek who died from the disease. Those with some knowledge about PDAC described it as deadly; other PDAC descriptors included, “fast moving,” “aggressive,” “painful”, “the worst type of cancer” and “hard to detect.” One rural participant described PDAC as, “pretty aggressive. It works fast, and usually, I’ve heard, by the time that they find it, you don’t have much chance of surviving it.” While most people were unfamiliar with PDAC, those having some knowledge perceived it as a highly lethal cancer with little hope of survival.
Among HRIs, everyone was aware of PDAC and most people knew someone close to them who died from the disease. Knowledge of the severity of PDAC was a strong motivator for the high-risk group to participate in a surveillance program as evidenced in the following quote: I think it’s one of the worst diagnoses a person can get. I mean because of the survival rate. It is not a friendly diagnosis. I just feel like when you hear pancreatic, there’s just very little hope. But I’m trying to have hope, which is why I participate in screening and like you mentioned try to have some control over it, you know the possibility that it lurks out there.
Susceptibility
Among rural and minority participants without specific risk for PDAC, there was limited knowledge of PDAC and people were therefore also unfamiliar with its risk factors. People guessed that some of the general factors that increased susceptibility for cancer such as age, smoking, alcohol consumption and diabetes might make someone more susceptible to PDAC. Some people talked generally about a family history of cancer, which they believed also made them more susceptible to PDAC. A few participants said that they did not feel at risk as they had no family history of cancer. One white, rural participant mentioned feeling more at risk because they lived in a county with elevated PDAC rates.
In the focus group with African immigrants and refugees, participants felt they were more susceptible to cancer due to the stress, racism, and suffering they had endured during their immigration journey and experiences in the U.S. A participant from this group commented: If you go through the racism that black people go through and go through the struggle that immigrants go through in this country to arrive, take 10 years or 20 years to get your papers to even be legal in this country. Why won’t you be sick? Stress causes sickness, right?
In this same focus group, participants attributed their poor health outcomes to social determinants of health and the inequalities they faced in relation to education, housing, and food access.
As expected, HRIs felt they were susceptible to PDAC. They attributed their higher risk to their genetic mutations (principally BRCA2) and/or family history. A few participants in this group were able to describe specific risk factors for PDAC. One HRI explained their perceived relationship between diabetes, pancreatitis, and pancreatic cancer as, “My understanding is that because diabetes and insulin is produced by the pancreas and therefore if the pancreas isn’t working properly, I think your risk of developing PDAC increases if you are a diabetic or you’ve had pancreatitis in your lifetime.” In this group, people were aware that PDAC had a genetic component and needed to be caught early to have a chance of survival and were therefore highly motivated to participate in a PDAC surveillance program.
Benefits of Surveillance
Nearly everyone understood the principal that some type of testing is needed to catch cancer earlier, rather than waiting for symptoms to develop. For the most part, underserved groups we talked to were aware of common cancer screenings, but had almost no knowledge of PDAC surveillance programs. Therefore, the discussion focused on the general concepts associated with cancer screening. Participants were motivated to participate in cancer screening because they want to stay in good health to take care of family or “to be around” for their children. People who knew someone close to them who died of cancer expressed a strong desire for screening and avoiding that fate. “I’d rather know up front so that I can tackle it. That’s—like I said, my mom died [of cancer] very young, and I don’t have any intention of doing that.” [White, rural participant].
In contrast to the lack of knowledge of PDAC surveillance programs among rural and minority participants, HRIs were highly knowledgeable and could name the different testing options. In this group, people were also motivated to ensure their family members were aware of their hereditary risks: “I have three daughters, so having those conversations with them, making sure that they are talking to their providers to make sure that, based on the family risk factors, they are getting the kind of surveillance they need.”
Many participants in the high-risk group explained they participate in PDAC surveillance for their “peace of mind” because they felt particularly susceptible based on their family history and high-risk designation: “I have aunts who were diagnosed with PDAC, dying of PDAC, fighting PDAC. It’s very much an immediate thing for me, seeing people going through it. So my motivation is to try to not get to that point where it is so severe that they can’t treat it.” HRIs were also aware that PDAC was hard to detect and fast moving, which further increased their motivation to participate.
For HRIs, participation in a surveillance program seemed to be a way for people to take responsibility for their health and confront their fear and high-risk designation: Like everybody has already said, fear the fear of the unknown…Cause there’s also colon cancer in my family at an early age, like at the age of 50… My brother passed away at the age of 56 very quickly within nine weeks of his pancreatic cancer. My dad died of colon cancer. So just knowing that, I feel like my fear has turned into a fight: I’m gonna’ fight this.
Barriers to Participation in Early Cancer Detection Programs
Lacking specific knowledge about PDAC surveillance programs, underserved populations described the barriers they face in relation to general cancer screenings. Multifaceted barriers were mentioned in this group (Table 2). The most frequently mentioned barriers were distrust of the medical system and/or providers, cost, and insurance challenges. As this exchange with rural, white participants shows, cost was often the deciding factor: Participant 1: I won’t pay for it. If you can’t afford it, you can’t afford it, and I can barely afford our bills [laughter]. Participant 2: A hundred percent, yeah. Cost is a big thing. I wouldn’t even pay 20 dollars for it. Participant 3: No. I can’t afford that. So, if insurance won’t cover it… I wouldn’t be able to do it. So it does play a big factor. Barriers to Participation in Early Cancer Detection Programs Note. The table includes all barriers mentioned by more than one person in each focus group. The barriers are listed in order of overall frequency mentioned.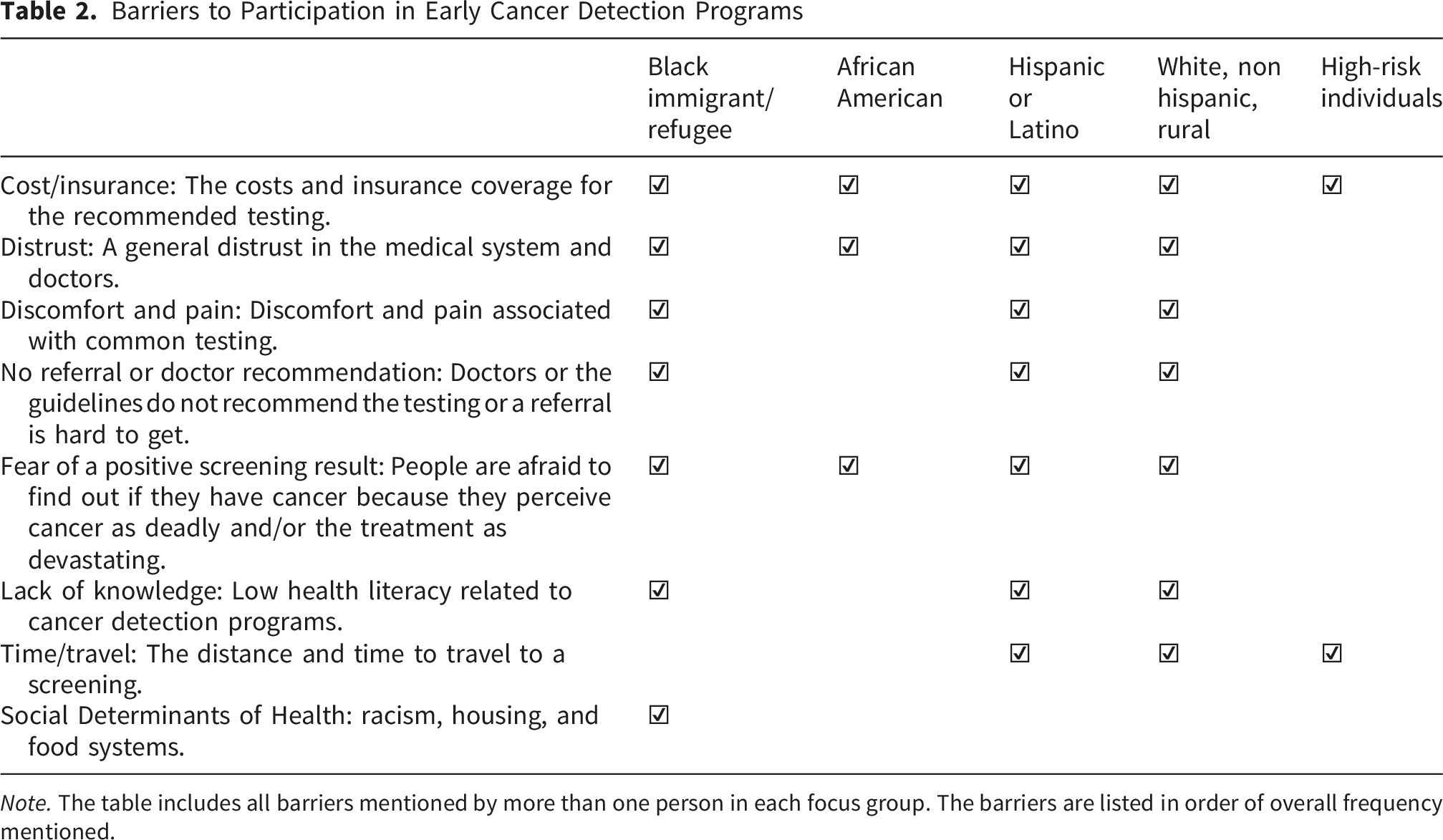
In one of the Spanish language focus groups, participants discussed not having insurance and the difficulties in qualifying for insurance. People without insurance shared that it was difficult to get an appointment at the clinic because “the clinic doesn’t want to see you and screen you because of no insurance.”
There was distrust across underserved population groups. Distrust was related to doctors being dismissive, disrespectful, and/or being too busy or unavailable. Some participants also perceived doctors to be incompetent and inexperienced; giving the wrong diagnosis, missing a critical piece of information, or doing something to make health worse. One African American participant commented: They are dismissive…I think there’s a lotta bias in hospitals. I think we have to, as a culture, I think we have to, press harder to get our needs met. …Like you get a late [cancer] stage, like this young lady’s mom got caught in the late stage. Why? I mean, she probably went and said this is what I have, this is how I feel, and, you know, they dismissed her until she’s like late stage. It’s, like, there’s nothin’ we can do for her.
Black individuals’ perceived systematic racism in the medical system and many didn’t feel they were cared for or respected. One African American participant shared: “I think as a culture too, I think we get thrown in a box and I think, African Americans are often looked as just being disposable, you know. I just don’t think they take the interest in us.”
Some rural participants also felt that some providers were dismissive and/or unresponsive. In rural counties, people are often challenged to find a doctor in their area, and the high turnover makes it difficult to build this relationship. A rural participant shared, “It is extremely difficult to get medical care. And, in fact, my doctor has said, “Go to immediate care first, and, um, I’ll read your chart later.”
Only two participants expressed distrust around the efficacy of early detection programs; in these cases, they perceived surveillance programs as a profitable industry that does not necessarily improve their health. This skepticism is expressed by a rural participant: “It feels like—for me, it feels like there might be some cure out there, but they might just be putting it on the shelves ‘cause they’re making money off of those other stuff.”
The third most common barrier was pain and discomfort associated with past medical testing, particularly mammograms, pap smears, and colonoscopies. This discomfort was often connected to how invasive the procedure was or how long it lasted. One person in a Spanish language focus group shared that she felt dehumanized and embarrassed when a male doctor conducted her pap smear. Nobody in Black groups mentioned pain or discomfort as a barrier, and only one HRI commented that getting an endoscopy was “tough and painful” because they could not be sedated adequately.
The fourth most common barrier was the lack of a doctor’s recommendation or referral. Many people wanted to undergo testing earlier than the recommended guidelines, often because someone in their family had cancer, but they could not get a referral or insurance to cover the test. This experience is evidenced in this quote form an African American participant: Pushback does happen. Even if you go in and you say, “I’d like to be screened for A, B and C.” They look at you and figure out your age. Anything to discount as to why you should not have to take that test. And that I think is wrong. If this is what a person is feeling, that they’re anxious about this issue, then you need to listen to that. But I think a lot of times they don’t do it because of insurance purposes.
Fear was the fifth most common barrier. Fear of a positive test result was especially prominent with people who witnessed the effects of the disease up close with relatives. As one rural white participant described: “I do [have fear] because I’ve seen the effects of family members with chemo and how it affects them. And so, I would have fear if I found out I had a diagnosis.” Generally in our focus groups, this fear motivates people to participate in screenings so they can catch the disease early, as a Latina participant shared: “The mammogram, my mom had told me that it hurts, but I was more scared of having it than not doing it.”
However, the fear in the African immigrant and refugee focus groups and to some extent in the Hispanic and Latino groups was so strong that people did not participate in any cancer screening or early detection programs. In these groups fear is commonly based on a perception that cancer is deadly and untreatable; therefore, early detection is not beneficial. As one African immigrant participant described it, the fear is so strong that it will kill you before the disease: I seen people who were told that you might have cancer and just for the fear that it caused them, the stress, it makes them like lose hope. And instead of fighting and having that positive attitude, they lose the momentum. They get into depression. The awareness of having a cancer and the early test, it also needs a lot of work. ‘Cause a lot of people, they don’t trust the doctors and also they don’t like cancer. It’s just like a disease that everybody wants to run away from it.
Low health literacy was a barrier that limited self-efficacy and was especially pronounced in the Hispanic, Latino and African immigrant and refugee focus groups. In these groups people expressed low awareness of the benefits of early detection programs, and little knowledge about cancer in general. Many people in these groups had little confidence navigating the health system and had never been screened for any cancer.
One of the last barriers mentioned in general populations was inconvenience: the time needed to travel to the testing site and challenges associated with scheduling the test around work and family responsibilities. This was a main factor of concern for rural focus group participants and some of the Spanish speaking participants as well. The final barrier was only expressed by the Black immigrant and refugee group. This group perceived social determinants of health, such as racism, poor transportation, education, and housing, exacerbating their challenges in getting screened.
HRIs rarely mentioned barriers to participation. The two main barriers for this group were: financial (out-of-pocket costs and insurance coverage), and the convenience of the tests.
Self-Efficacy and Cues to Action in Uptake
Participants generally had a high level of self-efficacy to participate in common cancer screenings. Most saw screening (e.g., breast and colon) as a routine and painless part of their lives and felt confident navigating the process. As one rural resident described his screening process, “It’s very straightforward. You’re in and out. It doesn’t take long, and most of your friends and neighbors are doing it, and you just do it.” However, three people mentioned only going in for testing when they had worrisome symptoms.
Most participants were aware of general cancer screening guidelines, even if they did not remember the exact ages for different tests. Screenings were typically initiated based on doctor’s recommendations. “Mine is because the doctor says, you know, we’re gonna’ be doing this, and I just kinda’ follow along with” [Rural, white participant]. This cue to action was not expressed in the Black or Spanish language focus groups; in fact several Black participants noted that they did not trust their doctors and would not follow their recommendations.
Some people who felt marginalized or dismissed by the healthcare system expressed the need for self-advocacy. As a rural resident commented: “I don’t think there is any screening here, hardly, unless you advocate for yourself to get screening.” In some cases, people with cancer in their family fought to get tested for this same cancer before the recommended age even when they had to pay out of pocket.
HRIs were confident in their ability to navigate the system to participate in a PDAC surveillance program. Most also initiated testing based on their doctors’ recommendations.
Test Preferences and Decision Making
Before each focus group ended, participants discussed preferences for different tests specific to detecting PDAC. They were presented with three different testing options: endoscopic ultrasound, MRI, and a theoretical blood test and asked their concerns or questions about the tests, and which they preferred under different conditions. Among rural and minority participants, most asked first about the level of invasiveness and then the accuracy of the different tests. Cost and convenience were also major factors they considered. Often people are trying to weigh all these factors in their decision making: I guess I’d wanna’ know, like, what the procedure entailed, any risks or side-effects that happen because of it. And also, I would wanna’ know what it is they’re looking for, and what they then do with that information, and what can be done, depending on what they find. [Rural, white participant].
Here the participant’s decision making considers how invasive the procedure is, side-effects or risks, the purpose of the test, and what can be done based on the test outcomes.
When the tests were described as having the same level of accuracy, everyone wanted the least invasive - nearly always perceived as the blood draw. Participants described invasive procedures as those that required sedation, were painful, had side-effects, and/or took a long time. If participants were told that a blood draw was less accurate, most people preferred a more accurate test even if it was more invasive. However, some people in the underserved group still preferred the less accurate test: It’s [endoscopy] just a level of invasiveness that I wouldn’t probably partake on a regular basis just for a cancer screen. I mean, that’s like a full sedation and it’s pretty invasive and there’s a certain amount of prep needed, time off work. I mean, there’s a lot of things. And yes, is that gaining me a 25 percent more accurate result… I’m just talking off the cuff, like, that’s my gut reaction to that.
Other people qualified their preference for the least invasive test even at the expense of some accuracy, by saying their preferences would shift if they had symptoms or risk factors that required a more accurate test.
Among HRIs, respondents considered cost and accuracy most commonly in determining their preference. While everyone did appreciate a less invasive test, HRIs were willing to undergo more discomfort or inconvenience for the most accurate test because they were quite concerned with their susceptibility to PDAC. As one HRI put it, “The one that gave me the more certain result. So whichever one of those gives me, the more certain that’s the one I’m going to choose.” Another HRI expressed, I probably wouldn’t even question it just because of the family history and watching people go through that, it’s a no brainer for me. Whatever test is available.”
Discussion
There is considerable debate about who should be considered for participation in PDAC early detection programs. It is possible that the definition of “HRI” may evolve with the changing epidemiology of PDAC, longer life expectancies, and discovery of new high-risk groups. 1 For example, there is interest in using the electronic health record or incidental abdominal computed tomography scans to identify at-risk populations that could be directed to an early detection program.26,27 Understanding the knowledge, motivations, and barriers to participation in PDAC early detection programs for HRIs and underserved individuals less likely to participate in other cancer screening will inform the development and marketing of new tests specific to PDAC. With the advent of novel cancer detection tests that may be marketed directly to patients, such as multi-cancer detection blood tests, this research offers insights about how people view the pros and cons of different testing options, and under what conditions they might theoretically decide to participate in a PDAC surveillance program.
As expected, our findings confirm that HRIs are willing to participate in PDAC surveillance programs.15,16 In this study, HRIs, identified previously based on their genetic profile and/or family history of PDAC, perceived PDAC to be particularly severe. As many people in this group experienced loved ones dying of PDAC, they were motivated to take control of their health. Other researchers have also concluded that HRIs see many benefits to participation and limited barriers.16,17 The main barriers identified in this study for HRIs were the cost of the tests and the time and travel involved. These observations suggest the most important steps to screening HRIs are first to proactively identify these persons and then to expand the number of participating health systems; this might include the development of novel early detection tests that could be disseminated widely, such as blood-based testing. To accomplish the first step, providers could take a more intentional family history from patients newly diagnosed with pancreatic cancer and then notify first-degree relatives about opportunities to participate in an early detection program, if appropriate. Additionally, greater compliance with National Comprehensive Cancer Network guidelines to perform germline testing on all patients diagnosed with PDAC could be followed by offering genetic testing to relatives of persons found to have a relevant germline mutation.
Our study provides new insights into the perceptions related to PDAC and early detection programs among rural and minority populations, who have been historically underrepresented in cancer screening studies. In these groups, we observed an overall low level of knowledge of PDAC, but an interest in early detection particularly among individuals who lost family members to other cancers. For these individuals, the tests need to be accurate, covered by insurance, minimally invasive, and convenient. These preferences are like those expressed by HRIs in an earlier study: People prefer the easiest, least invasive tests unless they feel they are at high-risk and willing to tolerate more invasive and less convenient methods. 15 Since risk for PDAC falls along a continuum, it is possible that some relatively lower risk populations who are eligible for PDAC early detection programs, such as those with an IPMN, may be less tolerant than particularly high-risk populations, such as those with Peutz-Jeghers syndrome.
As the HBM model predicts, people are weighing the costs and benefits of participating in a early detection program and deciding what makes sense for themselves. This decision making is evident in this quote from a rural, white participant: I mean, it’s never very comfortable, and it’s always a little scary ’cause you never know what’s gonna’ come from it. You hope that things are gonna’ be fine, but, for the most part, I would say I’m fortunate ’cause I have health insurance. So it makes it a little bit easier for myself to get screenings and I have a primary physician for a long time, so that also helpful.
Here the participant is considering discomfort, fear, cost (health insurance coverage), and a trusted physician when they are making their decision. When the circumstances of life shift, barriers might be reduced or elevated. As this Spanish speaking participant explains, “We had the opportunity once I had insurance so, I said, ‘Sometimes money can stop you, now it’s not the money so let’s do it.’ It was that and the kids, my children, because you want to see them.” As this participant indicated, cost was also a key determinant in our study, with many participants unwilling to pay out-of-pocket for an early detection test.
Compared to other cancers with existing screening or early detection tests available in practice, there are some barriers which might be especially pronounced in the context of a pancreatic cancer surveillance program. The lack of knowledge specific to PDAC risk factors, its severity, and unclear benefits of participating in a surveillance program will impact participation in lower risk groups (e.g., IPMN without high-risk features on initial imaging). Many perceived EUS to be invasive and uncomfortable yet is widely used for surveying HRIs and is included in the most recent NCCN guideline on pancreatic cancer screening. 13 EUS typically requires patients to travel to higher population dense health systems and may incur substantial out-of-pocket costs. Based on these findings, we believe this highlights the importance of introducing lower cost and more scalable solutions (e.g., blood-based tests) to improve compliance among individuals on the lower end of the risk spectrum.28-30
Our study suggests that there are racial/ethnic differences related to perceived motivators and barriers to PDAC surveillance. For example, most of the African immigrants and refugees and some of the Spanish speaking participants feared testing and had significant barriers to participation related to distrust of the medical system, low health literacy and self-efficacy, and the lack of engagement in the health system. However, more research is needed to understand race-mediated barriers to PDAC surveillance.
These findings indicate the need for tailored education and outreach. For example, in the African immigrant and refugee group, educating HRIs within this demographic about the severity and aggressive nature of PDAC will only push them further away; instead, the potential benefits of early detection could be emphasized. To overcome the significant distrust of medical systems that many of our underserved participants expressed, trusted relationships need to be in place for people to participate, and a solid evidence base for the surveillance program itself. As one African immigrant participant recommended: First and foremost would be building the trust amongst patients and the caregivers, the doctors…Once you build that relationship, like if I am a doctor, and I have my patient, I know how many children she has, where she lives, her economics, what she goes through, her stress level, everything. We build that connection, that relationship that way so it translates into, “Hey, it’s time for you to take, to check your mammograms. It’s time for you to check this and that.” But if you come and it’s just a business as usual and you just ask your questions and you don’t know what’s going on. That’s it. There’s no like connection. It’s not gonna’ work because I don’t trust you.
Limitations
One limitation of this study is the lack of diversity in the high-risk group. Nearly all HRIs were non-Hispanic White females from a tri-county region in Oregon, and our findings might be different for a more racially diverse high-risk population. This study is not unique; the lack of racial, ethnic and sex-based diversity is a pervasive limitation in PDAC surveillance focused studies.8,17
However, our engagement with rural and minority populations provides new insights for how these factors influence perspectives related to PDAC and early detection programs. This study indicates potential differences in motivations and barriers by race and rural/urban location, yet the sample size was small and these participants did not also meet criteria for participation in a PDAC surveillance program. Further research will be needed to identify the unique factors that specific cultures or social groups consider in their decision making about participation in a PDAC early detection program.
Conclusions
This research suggests that participation in PDAC early detection programs will be informed by a person’s perceived risk and the types of early detection tests available. When individuals feel particularly susceptible – the most dramatic example being a person with multiple affected relatives and a relevant germline mutation – they are intrinsically motivated to participate and remain compliant with recommendations, even if the surveillance test is costly, time consuming, inconvenient, or associated with some degree of discomfort. On the other hand, a patient with a relatively lower risk for PDAC such as an individual with an IPMN but no high-risk morphologic features, but still meeting guidelines for participation in a surveillance program, would benefit from novel approaches to early detection and is more susceptible to barriers such as cost, discomfort, distrust, and lack of perceived benefit. The importance of individual barriers appears to vary somewhat depending upon race/ethnicity and rural/urban location. This understanding can help researchers and clinicians personalize their approaches to presenting the role of PDAC early detection program to an at-risk individual. With the advent of novel PDAC-specific tests or multi-cancer detection tests that include PDAC in their algorithm, targeted outreach and education efforts can be developed for different at-risk patient groups to optimize participation and retention rates in research studies and with clinical practice guidelines.
Footnotes
Acknowledgments
The study team acknowledges the work of the Community Outreach and Engagement Team in facilitating focus groups and earning community trust for this project: Kaitlin Greene, Tiffani Howard, Danita Tracy-Carter, Sarah Swanson, Liliana Will, Natalie Bonilla, and Ryan Lutz. Dedicated to the memory of Mr. Ryan Lutz.
Ethical Considerations
This study was approved by Oregon Health & Science University’s Institutional Review Board (Study #00025950). All participants verbally consented to participate in this research and to publication.
Consent to Participate
All participants verbally consented to participate in this research after the facilitator reviewed the information sheet with each person and answered their questions. All participants received a $50 gift card for their participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The primary grant supporting this research was the NCI Pancreatic Cancer Detection Consortium [grant number U01CA278923]. This work was also supported by Oregon Health & Science University’s National Cancer Institute [grant number U01CA278923], and the Clinical and Translational Science Award [grant number UL1TR002369].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to ethical considerations and privacy concerns as outlined by the IRB.