
Abstract
History has conflated the legacies of José Manuel Rodríguez Delgado and Walter Freeman, midcentury proponents of somatic therapies for neuropsychiatric conditions. Both gained notoriety: Delgado after he appeared on the front page of the New York Times having used his stimoceiver to stop a charging bull in Spain; Freeman as the proponent of lobotomy. Both were the object of critique by the antipsychiatry movement and those who felt that their methods and objectives posed a threat to personal liberty. Using archival sources, we demonstrate that this conflation is a misrepresentation of the historical record and that their methods, objectives, ethics, and philosophical commitments differed widely. Accurate knowledge about historical antecedents is a predicate for ethical analysis and becomes especially relevant information as neuroscience develops circuit-based treatments for conditions such as Parkinson disease, depression, and brain injury. Part of that corrective is to counter the conflation of Delgado’s and Freeman’s life and work. Appreciating their distinctive legacies can help guide neuropsychiatric research done today that might yet haunt future generations.
It is easy to get lost in the frontal lobe, and sometimes with results ranging from the negligible to the disastrous.
A Response to Lobotomy
In a late-life interview, José Manuel Rodríguez Delgado (1915–2011) spoke of how he became interested in the electrical stimulation of the brain (Horgan 2005). Delgado had gained international fame as the developer of the stimoceiver, a radio-operated brain electrode, that stopped a charging bull in his tracks in a small bullring outside of Cordoba, in his native Spain (Fig. 1). That story made the front page of the New York Times in 1965 (Delgado 1981; Osmundsen 1965). Ever since, Delgado was famous and infamous. Famous for his precocious midcentury abilities with emerging neurotechnology. Infamous for the ways in which people feared that these devices might be used and abused. Concerns about the latter were heightened by the publication of his monograph Physical Control of the Mind: Toward a Psychocivilized Society (Delgado 1969).
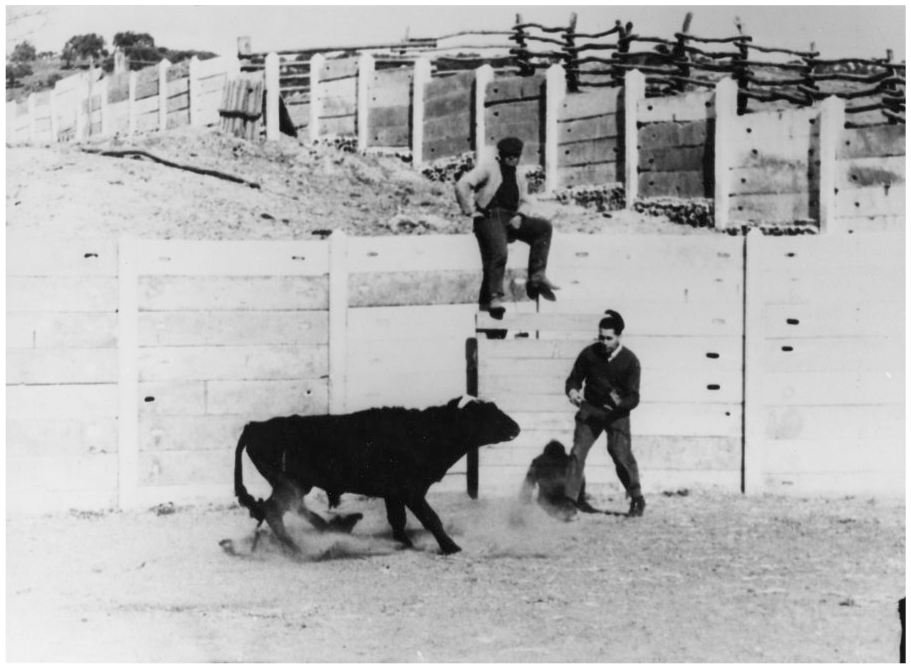
José Manuel Rodríguez Delgado testing his stimoceiver on a charging bull, Cordoba, Spain, 1963. Courtesy: Yale Events and Activities Photographs (RU 690). Manuscripts and Archives, Yale University Library.
Like many books with an evocative title, the message was more complex than it first appears. Delgado’s objective was not mind control, as some have too easily alleged, but rather a deeper understanding of the neurophysiology of aggression and violence, with an eye toward mitigation of personal and societal strife (Delgado 1969). But no matter. Amid the antipsychiatry movement of the 1960s and 1970s (Dain 1989; Nasser 1995), Delgado was often viewed in conspiratorial hues, linking his work to the excesses of lobotomy and its proponent, neurologist Walter Freeman (1895–1972).
History would write of Delgado and Freeman with the same broad strokes. Both engaged in somatic interventions that could threaten human dignity and breached the blood-brain barrier, what The Lancet, in a period editorial on psychosurgery, referred to as the popular delusion that to surgically treat the brain in this way carried “the penumbra of sacrilege” (Fins 2002;Lancet 1972). By tinkering with the brain with invasive technologies, Delgado and Freeman incurred the wrath of critics like Peter Breggin (Breggin 1973; Gallagher 1972), forever linking and marginalizing them together.
But the conflation was flawed, a kind of historical shorthand that misjudged the men and their biographies. While both Delgado and Freeman are of the same era and pioneered somatic therapies that tilted against psychoanalysis, then the dominant approach in psychiatry (Braslow 1999; Leveille 2002), their approaches and motives were antithetical. Delgado’s greatest gift was as an engineer and technologist whose innovative inventions were decades ahead of his peers (Vera and Martínez-Sánchez 2016). He even applied an electrode to a dog’s auricle (atria of the heart) in 1955 (Delgado 1955a; Nahum and others 1955), antedating the cardiac pacemaker by five years (Chardack and others 1960). Freeman disdained precision: he pioneered the icepick lobotomy. And therein lies the difference between the two men, a distinction not lost upon Delgado.
When interviewed in 2005, six years before his death, Delgado told John Horgan of Scientific American that his motivation to develop electrical stimulation of the brain was in response to the excesses of lobotomy. He told Horgan, “I thought Fulton and Moniz’s idea of destroying the brain was absolutely horrendous.” He preferred a far more “conservative” approach, telling Horgan, “My idea was to avoid lobotomy . . . with the help of electrodes in the brain” (Horgan 2005).
In another 2005 interview, with Joel Braslow for the American College of Neuropharmacology, Delgado was asked about why he focused on implanting electrodes in the brain. Speaking of procedures he did in Providence with Massachusetts General Hospital neurosurgeon Dr. Hannibal Hamlin (Delgado and others 1952; New York Times 1982), Delgado recalled, “Remember, 1952 was the age of lobotomy for which Egas Moniz won the Nobel Prize. I was not happy with lobotomy and wanted to see what we could do with implanted electrodes in schizophrenics, epileptics and depressed patients . . . I was asked whether I wanted to do lobotomies and I said no, let’s wait until the methodology is improved. But we had to treat epileptic, schizophrenic, and depressed patients” (Braslow and Delgado 2005).
Beyond the science, Delgado and Freeman could not have been more temperamentally different. Despite the novelty of his ideas and the originality of his work, Delgado was an institutionalist and a conformist. A refugee from Republican Spain, his was an immigrant’s story of striving and a desire to fit in. He wrote grant proposals and reports for deans and department chairs, as well as traveled here and abroad to give lectures. He played by the rules of academe and was rewarded. Carried along by undeniable talent and a determined work ethic, he was readily accepted within elite medical and scientific circles, winning the approbation of colleagues. He developed a wide range of connections and friendships, both personal and professional, on both sides of the Atlantic, and a deep bond with his mentor, John Farquhar Fulton, the famed Yale neurophysiologist.
The relationship was both professional and personal. Fulton even had charming exchanges by mail with Delgado’s mother (Fulton 1951a), Amada. She wrote Fulton in impeccable English that it was a “great comfort for me to know that in the States he [José Manuel] has such good friends as you and Mrs. Fulton and that in your house he feels so much at home” (Delgado A 1951). After a trip to Madrid, Mrs. Delgado sent laundry back to Fulton he left behind at the Ritz Hotel (Delgado A 1953). Thereafter, he sent her a copy of his biography of Harvey Cushing (Fulton 1946) that was “most interesting” (Delgado A 1954).
In contrast, Freeman was a loner and not a collaborator. A perennial outsider, he looked for an elusive professional recognition that was never forthcoming. A neurologist, he abandoned James Watts, his neurosurgical colleague, taking on operative tasks well beyond his training. His work made him famous, but this never satisfied his desire to be accepted by his peers. Unlike Delgado, who benefited from his relationship with Fulton, Freeman had to go it alone, feeling the sting of rejection along the way. He never had a patron to advance his work and pave the way, despite a distinguished medical pedigree (El-Hai 2005).
Freeman was the grandson of the prominent surgeon, Dr. William Williams Keen, who edited the 1887 edition of Gray’s Anatomy (Gray 1887), and was a colleague of Osler (Keen 1920). Freeman emulated his grandfather even as he sought not to replicate the life course of his disenchanted physician father (El-Hai 2005). With this lineage, Freeman lived in the shadow of both greatness and failure. He hoped for the former and was driven to desperate measures to avoid the latter, seeking the same recognition his maternal grandfather had achieved. He was haunted by the prospect of failure. As late as 1933, two years before his introduction to the lobotomy he confessed in his memoir, “I recognized that I had done nothing important in either explaining mental disorders nor treating it” (Freeman 1972). And years later, despite an immense amount of public notoriety from his association with lobotomy, professional acceptance would be beyond his grasp. In a painful admission, he later acknowledged, “I achieved the respect of my superiors because of my research type of mind, but I was not really close to any of them” (Freeman 1972). He perceived himself on the margins of the academy until public adulation turned to scorn (El-Hai 2005).
While history has characterized both Freeman and Delgado as crusaders, their quests, methods, and motivations were different. Both men were passionate about their work, yet their pursuits and legacies are distinct. It is this contrast, this gloss that too easily passes for history, that we seek to correct. We will do so by turning to both primary and secondary sources. This includes an unpublished autobiography written by Freeman for his family (Freeman 1972) and papers from the John F. Fulton Archives at Yale University during a formative period in Delgado’s career.
Conflations and Conspiracies
History has linked the work of Freeman and Delgado for their family resemblance. Both lobotomy and direct electrical stimulation of the brain are somatic therapies. But the historic—and indeed family connection—runs deeper, linking Freeman to Delgado through the influence of John Fulton.
Egas Moniz (Fig. 2), the Portuguese neurologist, who would win the 1947 Nobel Prize for his work developing prefrontal leucotomy, is said to have been influenced by John Fulton’s work on the frontal lobe (Fulton 1949a). As Jack El-Hai recounts in The Lobotomist, the moment came at a conference in London in 1935 (El-Hai 2005). Carlyle Jacobsen, who was doing primate research in Fulton’s lab, reported on the effects of the removal of the frontal lobes in two chimpanzees. There was minimal impact on their problem-solving abilities and variable effects on their demeanor, or affect. One became less anxious and the other more frustrated and angry (Jacobsen 1935).
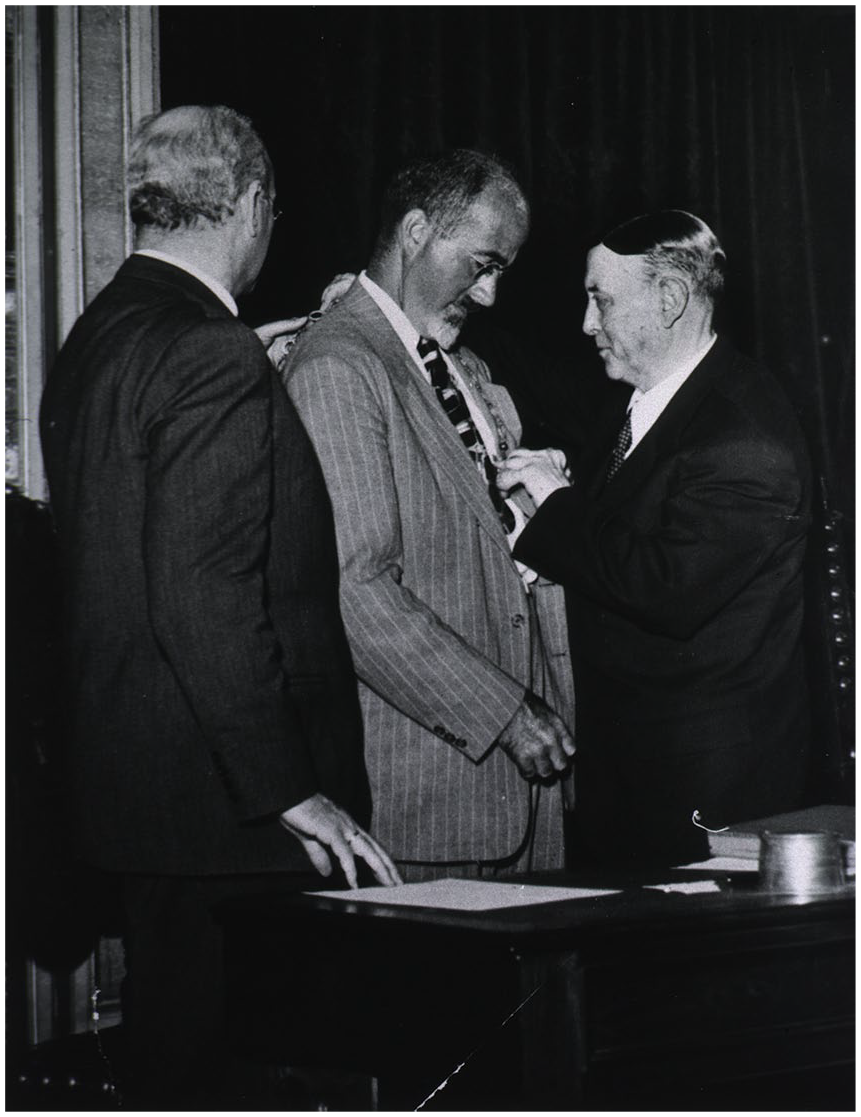
Walter Freeman receiving academy chain from Egas Moniz, Prof. Flores assisting, 1950. Courtesy: US National Library of Medicine. https://collections.nlm.nih.gov/catalog/nlm:nlmuid-101415445-img
Whether this conference was the source for Moniz’s inspiration is up for contention. Fulton maintained that Jacobsen’s talk, and the session that Fulton moderated in London, was where Moniz’s line of inquiry began. He recalled that Moniz asked if removal of the frontal lobe might be a surgical means to “relieve anxiety states in man” (El-Hai 2005). After the conference, Moniz went back to Portugal and began to experiment with prefrontal leucotomy in humans. He would publish his first paper on the topic the following year (Moniz 1937).
The London conference brought all the major players together in body and spirit. Fulton, Moniz, and Freeman were in London and, by extension, so too were James Watts and José Delgado. Watts, who would become Freeman’s surgical collaborator, had been a mentee of Fulton at Yale’s Laboratory of Primate Physiology, where Delgado would work decades hence. Although Fulton and Delgado would, as we will see, eventually renounce lobotomy, the shared provenance of this work became a convenient way to link Freeman and Delgado with each other. And in modern times, El-Hai, who was Freeman’s biographer (El-Hai 2005), also wrote a long form essay on Delgado (El-Hai 2016).
No one linked Freeman and Delgado more effectively than the antipsychiatry (Dain 1989; Nasser 1995) critic, Peter R. Breggin. Himself a psychiatrist and a libertarian (Breggin 1975, 1979), Breggin wove conspiratorial arguments about psychosurgery during the 1970s (Breggin 1972, 1973). An extensive critique by Breggin was inserted into the Congressional Record in February 1972 by Representative Cornelius E. Gallagher (D-NJ), who characterized his work as a “public service” (Gallagher 1972). Breggin explicitly linked Delgado’s electrical stimulation of the brain to Freeman’s lobotomy. Breggin describes Freeman as “America’s dean of lobotomy” (Gallagher 1972). His testimony is a devastating critique of the procedure and of Freeman for thousands of procedures he performed without adequate statistical assessment. But beyond questions of efficacy, Breggin writes of the incivility of the procedure itself, which he characterizes as mutilating. Its ability to destroy the “self,” which he asserts is “the ethical foundation of many modern psychological theories, where it often appears in terms of ‘identity’ or ‘self-insight,’” is a devastating critique (Gallagher 1972). In the public imagination, the reportage of the New York Times on Gallagher’s invocation of Breggin chose to highlight Breggin’s cautionary note that “if America ever falls to totalitarianism, the dictator will be a behavioral scientist and the secret police will be armed with lobotomy and psychosurgery” (Edson 1973).
Breggin asserted, “Delgado is working on the ultimate lobotomy” (Gallagher 1972). He characterized Delgado as “the theoretician of the lobotomists, the great apologist for Technologic Totalitarianism, complete with an outright attack on ‘liberal’ politics, meaning not the liberalism of the left, but principles of personal autonomy, independence and freedom, man’s ‘inalienable rights’ as annunciated in the Declaration of Independence” (Gallagher 1972). Breggin thus links Delgado to lobotomy and insinuates a political message that these technologies were linked to totalitarianism and could lead to a loss of personal liberty.
Edward A. Mearns Jr., in the Case Western Law Review, takes a more subtle tack exploring what is meant by the concept of psychocivilizing society (Mearns 1975). He critiques Delgado’s optimism about developments to manipulate the brain and understand violence and aggression. He finds Delgado’s assurances that the complexity of electrical stimulation of the brain would serve as a safeguard against abuse “not convincing,” arguing instead that “the complexity that gives Dr. Delgado confidence would most likely be a safeguard against the detection of ethical abuses.” While Mearns did not fear that psychosurgery would be the “primary technique used to eliminate freedom,” it would follow from other societal changes that make its application possible. Mearns observes that any society that allows itself to be subject to mind control is at risk of losing its freedom. In a chilling conclusion, he writes, “Psychosurgery might well be a means for control of the mind in a future psychocivilized society; but it will not be the means by which that psychocivilized society comes upon us” (Mearns 1975).
A 1970 New York Times editorial tied Delgado’s work to an Orwellian dystopia: “the horrifying prospect rises that in the 21st century the lexicographers may have to drop the verb ‘to brainwash’ and replace it with ‘to brainwave’” (New York Times 1970). Once again, the connection between Delgado, mind control, the loss of human agency, and the totalitarian state is made.
Delgado was vulnerable to these accusations because of his Spanish heritage and his connection to Francoist Spain. Among conspiracy theorists, he was often linked to Spanish fascism, making Breggin’s ad hominem attacks labeling him as an apologist for technologic totalitarianism all the more plausible. He came to Yale from the Spanish dictatorship and left New Haven for a high academic post in Madrid in 1970 while Franco was still in power. In fact, while he was working in Fulton’s lab during the 1950s and 1960s, he traveled regularly to Spain. There he maintained contacts with colleagues and was lauded as a local who made good on the international stage. Delgado’s background, travel history, and academic career path, coupled with his appeal to psychocivilize society through the physical control of the mind, made him ripe for political attacks by critics like Breggin.
So it would seem. But a more careful review of Delgado’s biography tells a different story. He was born in Ronda, a small town in Andalusia, in southern Spain, long a strong hold of Spanish Republicanism. From there he studied medicine in Madrid during the Spanish Republic just before the outbreak of the Spanish Civil War in 1936. One of his mentors was the socialist Juan Negrín, a physician and professor at the Complutense University in Madrid. Negrín was a monumental figure in Spanish medicine and Republican politics. He was instrumental in building University City in the north of Madrid during the Republic, a student of Santiago Ramón y Cajal (Giral 1994), and laboratory neighbor at the Complutense of Pío Río Hortega, Cajal’s student and long-time associate (Cannon 1949). Negrín would go on to be the wartime prime minister and president of the Spanish Republic that had been attacked by the Francoist forces (Preston 2006). Delgado described Negrín as an “enchanting and powerful person as he demonstrated during the Civil War” (Delgado 1958). He also credited Negrín with saving masterpieces housed in the Prado during the war (Delgado 1958). But he added, “On many occasions I thought that it was a shame that politics robbed us of the mind (the scientific contributions) of Negrín” (Martínez-Sánchez and Palmero Cantero 2004).
When the war broke out, Delgado served with the Republican side. He was at the Battle of Teruel, served as a physician, and rose to the rank of captain (Igual 2019). He later told a New York Times reporter that “I fought with them [the Republicans] until the triumph of France [sic], then I was thrown in a concentration camp. Those few months had a great effect upon me; they shaped me” (Scarf 1970).
Nonetheless, he seemed to have been accepted by the Francoist regime. After his release from imprisonment, he was allowed to return to Madrid to continue his studies. Interestingly, he either did not complete his course of study (Igual 2019) or had to repeat his medical degree because the credentials granted during the Republic were no longer recognized by nationalist authorities. He subsequently graduated (again) from the University of Madrid in 1942. A review of an application to Yale’s Department of Physiology—in his own hand—completed in 1946 makes no mention of a medical degree under Republican auspices. There is a notable nine-year gap between his BE and BS degrees from Vitoria (1928) and Valladolid (1931) and his ML (1940) and MD (1942) degrees from Madrid University (also known as the Complutense) (Delgado 1942; Yale Department of Physiology 1946). In 1946, he obtained a grant from the Spanish Foreign Ministry to study for six months at Yale with Fulton (Discursos 1999).
At the time when many Spanish neuroscientists went into exile after the Civil War (Dosil 2013), Delgado traveled freely back and forth to Spain, maintaining collaborations and professorships in Madrid and even winning the 1952 Ramón y Cajal Prize (Fulton 1952a) on the centenary of the Nobelist’s birth. Fulton described the honor as “the highest award that can come to anyone in Spanish medicine,” adding “we are all delighted by the news” (Fulton 1952b).
So it is an ambiguous story (Vera-Ferrandiz and Martínez-Sánchez 2017). If Delgado was a confirmed Republican, how did he become so quickly rehabilitated within an academy ruled over by the Francoist regime? How did he ever win the Cajal Prize at such a young age and during a commemorative year? How did he have freedom of travel to and from Spain under the dictatorship? What does this say about his political allegiances?
In a 2004 interview, Delgado recounts a conversation with Fulton about his activities during the Civil War. He told Fulton, “This has nothing to do with science” (Martínez-Sánchez and Palmero Cantero 2004). Later, after his arrival at Yale, he learned that colleagues were saying, “He is a scientist of Franco. We are going to block him so that he can’t work.” To which Delgado replied that he had passed the war in the Republican zone and was a captain in the medical corp. After that, he encountered a “marvelous reception on the part of everyone” (Igual 2019; Martínez-Sánchez and Palmero Cantero 2004) (Fig. 3).

Fulton Lab: members of the laboratory of physiology. From left to right, back row: John F. Fulton and Eric A. Turner; front row: Robert B. Livingston, Bal Krishan Anand, José Manuel Rodríguez Delgado, Hsiang-Tung Chang, and Rajinder S. Sikand. Yale Medical School, 1952. Courtesy: Yale Journal of Biology and Medicine.
Perhaps most convincingly, we discovered a contemporaneous letter of recommendation written by Fulton for Delgado. The letter was addressed to Dr. Tom D. Spies of Hillman Hospital in Birmingham, Alabama, and dated March 5, 1947. The document is important because it speaks to Delgado’s politics (Fulton 1949b). After praising Delgado as “an extraordinarily intelligent fellow with a great drive for work” who he has “no hesitancy in recommending him warmly,” Fulton gets to the question of political allegiances. He wrote,
When he came here, we were under some apprehensions about him because he had been officially recommended by Franco’s Ambassador, and also by Alva, one of the principal aristocrats of Spain. I can’t go into the details, but we found that he was completely reliable politically, that he was definitely not a Franco Fascist and the he was sincerely interested in scientific medicine. (Fulton 1949b)
Fulton concludes the letter by noting that he hopes that Delgado “doesn’t go to Birmingham when he returns because we were hoping he might come back to us” (Fulton 1949b). This correspondence, to the best of our knowledge, is new to the archival scholarship on Delgado.
The endorsement of Delgado by Fulton—personal, professional, and political—is dispositive as a contemporaneous document and because of its political provenance. Fulton, himself, was deeply enmeshed in left-wing politics of the day. Described in an obituary as a “forthright liberal” (Stevenson 1961), Fulton’s political allegiances were never in doubt. He despaired over the rise of fascism in Spain and Europe and assisted academics like the historian Henry Siegerist of Johns Hopkins who had been marginalized in the academic establishment because of his left-leaning views. In his essay addressing Fulton’s relationship with Spain, Igual wrote that Fulton “defended Henry Sigerist, who since the early 1940s has been excluded from the country’s academic and philanthropic elite due to his left-wing political ideas; this isolation was aggravated by the outbreak of the Cold War. Fulton understood Sigerist’s decision to leave Johns Hopkins University in 1946 and return to Switzerland” (Igual 2019). During and briefly after World War II, Fulton was a member of the American-Soviet Medical Society and worked on the American Review of Soviet Medicine. He was friends with Spanish Republicans, including Juan Negrín, who had been Delgado’s professor and, as noted, led the Republic (Igual 2019). Fulton’s ties with the left suggest that he had excellent sources to vouch for Delgado’s political bona fides, perhaps at the highest strata of Republican elites.
Freedom and Insight
Delgado’s own writings on politics also suggest that he had a liberal orientation. An essay dating from 1983, entitled “The Psychophysiology of Freedom,” is a manifesto promoting personal freedom and outlining how it might be achieved, drawing upon knowledge of our neurobiology, education, and training (Delgado 1983). He describes freedom as a mental activity that is dependent upon social inputs of information and the learning of intellectual skills, which maximize “available behavioral options.” This optimization—in pursuit of “personal happiness” (Delgado 1988)—can be achieved by a “democratization of psychological knowledge [that] will give each individual a better understanding of his own personality, cerebral mechanisms, basic needs and attitudes” (Delgado 1983).
The argument builds upon his 1969 volume to psychocivilize society (Delgado 1969), asserting that such a state can be achieved by “intelligent choices with plans and purposes that can be shared by all mankind, because all share similar basic neurological mechanisms” (Delgado 1983). The argument is more than a biological one: it is contextualized within the political polarities of a totalitarian versus a democratic system. And it is here that Delgado reveals himself to be a partisan of the latter and not the former.
Definitionally, Delgado observes that in contrast to a democracy, the “totalitarian theory grants not ‘rights’ but ‘privileges’ to the individual in the interest of the welfare of society as a ‘state’ (fascism), ‘race’ (national socialism), or ‘proletarian class’ (Russian communism).” And then importantly telegraphing his political loyalties, Delgado adds, “Liberals value freedom in the interest of the individual, while totalitarians allow freedom in the interest of society” (Delgado 1983). He voices concerns (relevant to our own era of social media) that “mass media and distortion of information are well-known procedures used to restrict freedom of thought and behavior” (Delgado 1983). As observed in Physical Control of the Mind: Toward a Psychocivilized Society, “Liberal societies are based on the principle of individual self-determination, with the assumption that each human being is born free and has the right to develop his own mind” (Delgado 1969b).
It could be argued that there is a reductionistic, indeed utopian, tenor to Delgado’s prescriptions, given the knowledge of brain science when he was writing in the 1980s. A careful reading of the essay suggests that it is less about technology and neurobiology than about advancing a liberal educational policy to prevent indoctrination in the service of the state or the fostering of an ideology. To prevent these antidemocratic developments requires a structured and scientifically informed educational approach that counteracts “outside manipulation of his own self.” This comes from scientific knowledge “placed at the service of the masses in order to increase personal freedom through better knowledge of its cerebral mechanisms” (Delgado 1983). Fundamentally, it is not about a loss of control because of technology but rather a means to gain additional dominion over one’s self through the understanding of neurobiology and the development of social structures that enable personal freedom. Delgado’s conception of agency hinged on being informed by self-knowledge so as to have better control over one’s own actions.
Contrast this with Freeman’s perspective as articulated in his memoir. There, he wrote that “insight is a terrible weapon, and few know how to use it constructively” (Freeman 1972). Unlike Delgado, who sought to liberate the individual through a deeper knowledge of the self, Freeman cautioned against “the vicious circle of preoccupation with the self.” In his cosmology, too much self-scrutiny “and preoccupation with the self was the sine qua non of emotional disorders” (Freeman 1972). He warned that when we get to know ourselves, “when we realize, really get to know what stinkers we are, it takes only a little depression to tip scales in favor of suicide.” Whereas Delgado thought that self-knowledge was liberating, Freeman maintained that “insight does not equip the patient to overcome his handicaps” (Freeman 1972). In his view, it was the opposite, as people “had gotten in trouble with too much self-scrutiny” (Freeman 1972).
In response, Freeman offers lobotomy, which causes the individual to lose interest in the self. He couched this as the reverse of psychoanalysis where people “were asking for further trouble by undergoing any exploratory psychotherapy” (Freeman 1972). Historian Mical Raz cites an unpublished essay by Freeman from the Freeman/Watts Archives at George Washington University, entitled “With Camera and Ice-Pick in Search of the Super-Ego,” in which Freeman writes, “For nearly a quarter of a century I have been hunting the Super Ego, not in the conventional Freudian sense of attempting to understand all the ramifications in each individual patient but, rather, by recognizing the handicap the patient experiences from excessive elaboration of self-centered psychic exploration” (Raz 2008). Raz describes Freeman’s effort “to use an icepick in order to free the self from the superego” (Raz 2008).
Freeman’s “therapeutics” reflects an antiliberal vision of the mind and self-determination. Less is more when it comes to self-knowledge, even when it is obliterated by a leucotome or an icepick. Indeed, it is a Weltanschauung (worldview) of loss. That loss could be devastating and irreparable. Wolfhard Baumgartel, a staff physician in a hospital in which Freeman operated, described to National Public Radio what occurred to a patient after lobotomy: “There was something missing—emotions, I would say. You know, if you were to converse with somebody, there’s always emotion with it. Just take all of your emotion out of a conversation with somebody and what’s left?” (Baumgartel 2005). A patient, Howard Dully, who underwent a lobotomy at the hands of Freeman, said it most starkly when he observed, “I’ve always felt different—wondered if something’s missing from my soul” (All Things Considered 2005).
At the 1947 meeting of the Association for Research in Nervous and Mental Disease in New York, Fulton orchestrated a confrontation between Swedish psychiatrist Gosta Rylander and Freeman. Rylander challenged Freeman, invoking the legacy of loss sustained by patients after lobotomy. He presented a patient who “for years [she] lay in the hospital constantly saying that she had committed sins against the Holy Ghost. . . . When the operation was finished, she was quite silent . . . I asked her, ‘How are you now? What about the Holy Ghost?’ Smiling, she answered, ‘Oh, the Holy Ghost; there is no Holy Ghost’” (Pressman 2002; Rylander 1948). Freeman immediately appreciated the threatening accusation: “It seems to me that Dr. Rylander’s conclusion that lobotomy takes something from an individual should be judged in light of what lobotomy gives back to the individual in relation to his prepsychotic adjustability in his social surroundings” (Pressman 2002).
Notwithstanding Freeman’s intent to free a patient from illness through lobotomy, his methods were one of subtraction in contrast to Delgado’s desire to liberate individuals with additional freedom. It is a fundamental distinction that speaks against conflating these two proponents of somatic therapy (Braslow 1999).
Scientific Methods
Distinguishing John Fulton from Walter Freeman in his magisterial volume Last Resort, the late Jack D. Pressman notes “the distance between the world of the laboratory scientist and that of the practicing clinician.” For the former, it was rigorous laboratory studies. For the latter, it was clinical utility. As Pressman observed, “Most important of all to Freeman was the question, ‘Did it work?’” (Pressman 2002). He was skeptical of laboratory metrics and more impressed with whether the patients could resume their lives, even if this was a judgment based on subjective assessment.
Delgado clearly followed in Fulton’s “laboratory scientist” lineage. A review of the archival evidence reveals a committed scientist who was an innovative engineer and physiologist at the vanguard of bioengineering in the 1950s and 1960s. While his methods would not withstand the rigor of current approaches, by contemporary standards, he was decades ahead of his peers as an engineer and developer of neurotechnology.
Freeman, in contrast, was subjective in his assessments and approach. Lawrence M. Weinberger, a young neurosurgical trainee, met Freeman at Delaware State Hospital to learn how to perform lobotomies. He recalled that Freeman’s approach to patient selection was “purely observational.” When he inquired about Freeman’s selection criteria, he was “answered with a prolonged silent stare and finally one word: ‘Experience!’” (Weinberger 1998). More seasoned practitioners such as the psychoanalyst Roy Grinker, who would become the editor-in-chief of Archives of General Psychiatry, worried about Freeman’s idiosyncratic approach, noting that “once one cuts, there is no return” (Fins 2003; Panel Discussion at Cleveland Session 1941).
But beyond their rigor, or lack thereof, there was another fundamental difference to Freeman and Delgado’s methods. The former was an anatomist, the latter a physiologist. Freeman turned to postmortem studies to infer the effects of lobotomy, most notably his theory that destruction of white matter connections between the frontal lobe and the thalamus caused retrograde degeneration of the thalamus, which he thought was the seat of emotion. Reporting on 12 necropsies of lobotomized patients, he observed that the “thalamus and emotion have long been connected, hence the further importance of these anatomic studies” (Freeman and Watts 1947).
Freeman also returned to the anatomy lab to develop the transorbital lobotomy. Freeman tested the technique on cadavers at Gallinger Municipal Hospital. In his memoir, he recounts how he “selected an icepick as being the only instrument possessing the necessary qualities of sharpness and toughness to do the job” (Freeman 1972). These were not physiologic studies but rather anatomic ones.
Delgado, in contrast, was a physiologist using those methods to amplify traditional means of inquiry. In an address to the American Museum of Natural History in 1965, Delgado articulated his vision for inquiry into the brain (Delgado 1965). He argued it was time to move beyond “when observation and reason were the main tools for the acquisition of knowledge, philosophical speculation flourished” and simple psychological “correlations between sensory input and behavioral output” were made. Instead, it was time to explore “the processes . . . hidden in the mystery of brain physiology” (Delgado 1965). He then outlined how “science has developed a new electrical methodology for the study and control of cerebral functions in animals and humans.” Yet as capacious as was his vision, Delgado possessed a humility that Freeman did not. In his address at the museum, he is careful to note the limits of what science, his science, can achieve:
I am not so naive as to think that cerebral research holds all the answers to mankind’s present problems, but I do believe that an understanding of the biological bases of social and antisocial behavior and of mental activities, which for the first time in history can now be explored in the conscious brain, may be of decisive importance in the search for intelligent solutions to some of our present anxieties, frustrations, and conflicts. (Delgado 1965)
Delgado’s acknowledgment of the epistemic limits of his work contrasts with Freeman’s scientific hubris. This is implied in what Wilder Penfield, the famed neurosurgeon and founder of the Montreal Neurologic Institute (Fins 2008), wrote Freeman upon the publication of Psychosurgery (Freeman and Watts 1942). Penfield observed, “It is beautifully and thoughtfully done. It will prove to be a building stone in a structure of therapy in a field where little therapy has stood the test of time” (Pressman 2002). Penfield, a master writer and editor, chose his words carefully: the implication is that Freeman’s monograph represents a starting point for the construction of a field, not its summation (Fins 2008). To invoke the titles of two of Penfield’s monographs, this was a quest where no man alone could unravel the mysteries of the mind (Penfield 1975, 1977).
Freeman’s hubris was made all the more problematic by his utilitarian ethos that would place individual patients at risk in pursuit of a perceived greater good. This is evident in a 1953 New England Journal of Medicine essay on the ethics of psychosurgery (Freeman 1953). In this response to his critics, Freeman advances a humanitarian stance to relieve “mental pain or anguish [that] is often more real than physical pain.” Despite this patient-centric approach, he appears willing to endanger some patients—some mortally so—in order to provide relief to many. Framing the “moral problem” of surgical innovation and psychosurgery, Freeman invokes Gottlieb Burckhardt, a 19th-century Swiss psychiatrist who wrote that “every new surgical approach must find its special indication and contradictions and methods, and every path that leads to new victories is lined with crosses of the dead” (Freeman 1953). Later, Freeman writes of the legitimacy of psychosurgery to preserve the family unit group. Here he invokes the benefit to the group to justify surgery on an individual under his care. He wrote, “Fortunately, the performance of leukotomy before the group has disintegrated and when there is still a place in the group for the member after his disorder is relieved will rebuild the group into a harmonious and effective whole” (Freeman 1953).
Ethics and Exculpation
In September 1936, Freeman performed his first lobotomy, and from the start, there were ethical concerns. As recounted in his unpublished autobiography, Freeman writes of the patient, a Mrs. Hammatt with “typical agitated depression” who had been referred to him. In his opinion, “it was a choice of operation or institutionalization.” Mrs. Hammatt and her husband decided to “take a chance on surgery,” but Mrs. Hammatt changed her mind because in preparation for surgery, her head would be shaved and “she didn’t want to lose those curls in front.” Freeman tells how “we got around her objection by promising to spare the curls if we could.” Then the admission, “Of course it was impossible.” And then the exculpation, that after the surgery, “she never mentioned the curls” (Freeman 1972).
The episode is problematic in the framing of options. After his engagement with Moniz, Freeman was eager to find a candidate for surgery, and he presented this as a therapeutic option when it was as yet experimental. There was no mention that this was the first case that he and the neurosurgeon James Watts would perform. On the issue of Mrs. Hammatt’s curls, something that was important to her, he made a promise he knew he could not keep, misleading his patient. That she seemed unconcerned about this loss after surgery in no way exonerated his deception during the consent process.
Freeman viewed the result as “spectacular,” although a hemorrhage three days postoperatively caused her to become transiently stuporous, hemiparetic on the right side, and aphasic. But no matter, she recovered completely and went on to live, according to Mr. Hammatt, “the happiest years of her life” (Freeman 1972). Her loss of “terror” and ability to go to theater without obsessive thoughts in Freeman’s assessment constituted a success, and he lost no time in spreading the word that she had been “cured.” He presented to his local medical society within a month and reached out to the science writer of the Washington Post, inviting him to come to George Washington Hospital to see the procedure and interview patients. Instead of going through the peer-review process and gaining professional approbation—which was not forthcoming—he reached out to a journalist because, “I wanted to get an accurate account on record” (Freeman 1972).
Freeman’s description of that first procedure, using Moniz leucotomes ordered from a Parisian instrument maker, also foreshadowed the professional misjudgment that would taint his work for decades. He writes, “Watts performed the operation on one side and I on the other” (Freeman 1972). One would expect that Watts, as a neurosurgeon, would perform the procedure on both sides and Freeman, as a neurologist, would bear witness and observe its effects. But from the start, Freeman overstepped his professional role and training.
This lack of insight into his role and the limits of training culminated in Freeman’s development of the transorbital lobotomy, a procedure he began in 1946, which he performed alone using an icepick. He did 10 cases before he was “sufficiently confident” to ask Watts to see the procedure. This transgressive act horrified Watts. Freeman wrote, “Jim was so distressed that he threatened to break off our association if I continued” (Freeman 1972).
Freeman’s response betrayed a lack of insight into his long-time colleague’s horror. Instead of abandoning the procedure outright, his response was merely transactional: “Consequently I did no more in Washington for the next year” (Freeman 1972). Like Mrs. Hammatt’s disinterest in her lost curls after the operation, the ethical impropriety of a misdeed was negated if Watts was unaware that Freeman had moved the procedure out of his partner’s gaze. So out of sight and out of mind, Freeman continued performing the transorbital procedure. Over the course of the next year, he did nine more cases. Only then, he approached Watts again with what he describes as results that were “quite beneficial.” With the hiatus and Freeman’s results, Watts was persuaded to resume his collaboration with Freeman as he pursued the transorbital approach. But after five of six patients “relapsed,” Watts abandoned the procedure, forever destroying their partnership (Valenstein 1986).
How Freeman describes this episode and its effect on his relationship with Watts suggests a failure to assume personal responsibility for their parting of ways. Notably, Freeman writes in the passive voice that “a rift between Jim and me came early in 1946 when I started performing transorbital lobotomies” (Freeman 1972). It is a curious construction where the rift comes before the admission of the causative actions that prompted the fissure. This is a well-worn way of linguistically evading responsibility for one’s actions and their consequences, a technique employed historically when individuals in power abused their authority and then used language to obscure culpability (Beckerman 2019; Mangione and others 2021; Paechter 1944). Instead of acknowledging he caused a harm, Freeman can evade culpability semantically for the precipitant that came between him and Watts. The “rift” begins without clear causality and without an acknowledgment—in the first person by Freeman—that his actions caused the rupture.
This displacement of responsibility is characteristic of Freeman when recounting his work. His report on his first 20 cases of transorbital lobotomies blandly noted that “one patient was dead of hemorrhage” without a clear attribution for the death (Freeman 1972). Elsewhere, he reported results from Greystone Park State Hospital from October 1948. He reported that “the results were as bad as anticipated” because “of the 18 patients operated upon . . . there was not a single one that I would have chosen from my own practice” (Freeman 1972). Here the failure is displaced upon the collection of patients who were chosen for him, not on his decision to perform the procedures. Instead of acknowledging the failure of the icepick lobotomy or his faulty decision to perform the operations in ill-suited surgical candidates, Freeman inverts responsibility upon them. The only exception, itself problematic and distasteful for its self-referential musings, concerns a surgical mishap. He reports that “in one patient the icepick broke, leaving a small bit embedded in the base of the brain.” He continued, “Fortunately, there were no unfavorable results, but the embarrassment was mine” (Freeman 1972), a rather gross displacement of concern away from an injured patient.
Research and Responsibility
While Freeman operated directly on patients, even against their will, Delgado’s work was dramatically different. Most obviously, Delgado spent the majority of his career doing experimental work on animals, including primates. He even went out of his way in Psychocivilized Society to make sure that the reader knew that there were no ill effects from his procedures on the animals on whom he conducted his experiments (Delgado 1969). When Delgado did discuss studies on humans, he noted that everything was for the “welfare of the sick patient” and later—in a chapter explicitly devoted to ethical considerations—asserts that physicians should “do nothing harmful or unpleasant for the sake of science” (Delgado 1969). This is a far cry from Freeman, who—as noted (Freeman 1953)—believed that the death of some of his patients was justified to achieve scientific progress.
Yale’s Fulton Archive from 1951 to 1955 provides insight into Delgado’s ethical concerns and his adherence to institutional norms (Fig. 4). In April 1951, he shared a proposal, “Implanted Electrodes in Humans,” with Fulton. The research plan lays out his prior work stimulating the “pyriform-amygdaloid complex” with chronically implanted electrodes in cats and monkeys, affecting emotions, feeding, levels of reactivity, and motor response. Building on this experience, he proposes to study electrical stimulation of the temporal lobe in patients undergoing lobectomy. His first objective was to make “inferences with respect to the role of the temporal lobe in the disorder which affects the patient.” From there he sought to study motor, vegetative, and psychological responses, with direct observations, filming, and electroencephalogram (EEG) recordings. He sought to study a corticogram of the pyriform-amygdaloid area and correlate direct recording with standard EEGs, evoked potentials, conduction, suppression, and related phenomena as well as changes related to sleep and alterations in the environment. He noted that “the possible harm is small”; the electrodes are “eight times smaller than the intraventricular needle” and are made of “non-reactive material” (Delgado 1951a).
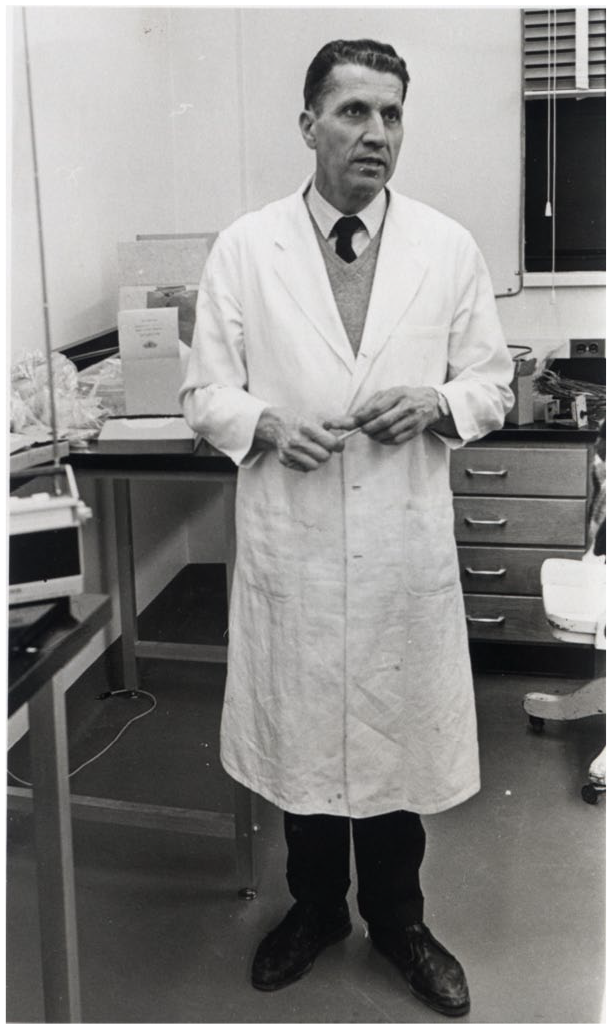
Delgado in his lab at Yale. Courtesy: Yale Events and Activities Photographs (RU 690). Manuscripts and Archives, Yale University Library.
Delgado’s proposal is ethically salient for a number of reasons. First, his plan invokes the modern notion of incremental risk (Chiong and others 2018). Patients who would be implanted were already undergoing surgery for a clinical indication, and data generated from the studies might be beneficial to their medical care. Harms from the implantation would be incremental to neurosurgery, which was already being done for a patient-centered reason. Finally, he spoke to the risk of electrodes that would remain, noting they were inert and small (Delgado 1951a).
Fulton was favorably disposed to the proposal and had a “constructive suggestion” that Delgado go into additional detail about factors that could reverse emotional changes following stimulation of the pyriform-amygdaloid area. As Delgado embarked on one of his many academic road trips, Fulton hoped that during this upcoming collaboration, “you will have full opportunity to extend your experimental observations from animal to human subjects” (Fulton 1951b). As a further indication of his support, Fulton invited Delgado to accompany him to the University of Louvain in 1951 to serve as an assistant, “thoroughly trained, as you are, in neurological surgery and in the technique of operating the Horsley-Clarke stereotaxic instrument and also in the methods for implanting electrodes . . . for purposes of stimulation” (Fulton 1951c).
Yet despite a flurry of letters across the Atlantic, Delgado was having ethical reservations about the work. From Madrid, in September 1951, he wrote to Yale’s Committee on Funds and Fellowships with a change of heart and mind. The correspondence is illustrative of Delgado’s incremental approach and ethical prudence (Delgado 1951b). He explains that working under a Hudson Brown Memorial Fellowship, he had “developed a method for chronic implantation inside the brain.” To foster that work, he asked the committee for permission to spend an additional 45 days in Madrid to do stereotactic research on cadaver brains to guide electrode placement. Cadaver brains were evidently available in Spain but for “lack of materials and legal reasons makes this work impossible in the States” (Delgado 1951b).
Delgado explains he needs to delay his return to the United States and take this investigational detour precisely because he had ethical concerns about operating upon humans prematurely and without adequate preparation. While he had done preliminary studies on “rats, cats and monkeys” (Delgado 1952), he was not yet ready to extend his work to humans. His caution reflects a strong ethical sensibility:
The two aims of implanted electrodes in humans—treatment and research—and the tremendous responsibility of working with human beings need great accuracy of method. Electrodes must be placed with stereotaxic technique, using stereotaxic maps of the brain. We have excellent stereotaxic charts of the brains of cat and monkey but we lack proper stereotaxic information concerning the human brain. Our work in man is therefore stopped by lack of necessary data. (Delgado 1951b)
Beyond demonstrating Delgado’s concern about potential human subjects, asking for permission to stay in Madrid illustrates Delgado’s adherence to institutional norms. Unlike Freeman, he was not going it alone but negotiating his way through channels, the Yale bureaucracy, and his own conscience. He knew he had to slow down.
Of course, he had the backing of Fulton, who wrote that he “mustn’t worry . . . if the Hudson Brown people make a fuss, he [Robert Livingston, a professor of physiology at Yale and later head of the National Institute of Mental Health and the National Institute of Neurological Disease and Blindness] wants you to know that the Unit will carry on with your work.” It was the power of Delgado being an institutionalist and his documentation: “these two documents seems so powerful that we’re pretty sure everything will be all right” (Fulton 1951d).
The episode ended productively with Delgado sending the committee a comprehensive report on his work in Spain and Louvain, mentioning that he made contact with the great Spanish physician Gregorio Marañón and the Yale-trained neurosurgeon Dr. Sixto Obrador, who would later recruit him back to the Hospital Ramón y Cajal in Madrid decades later (Delgado 1951c; Sociedad Española de Neurocirugía 2018).
By 1954, Delgado used his method of electrode implantation to study physiology in animals. In a research report, he noted that stimulation of the head of the caudate nucleus induced a “functional and transitory ‘lobotomy’” in animals. He also reported on what he described as “electrolobocoagulation” in psychiatric patients, three with intractable pain, one with anxiety neurosis, four with schizophrenia, and two with psychomotor epilepsy to see if “electrolytic ablation of selective discrete intracerebral areas produced therapeutic benefits.” This was done without complications (Delgado 1954).
Soon thereafter, George Mahl of the Department of Psychiatry, who chaired the Research Committee at the medical school, wrote Fulton at the urging of Delgado and others to “have a thorough discussion of the use of the implanted electrode technique in human patients suffering from illnesses involving the central nervous system.” Delgado was asked to present an “outline of the pros and cons” in advance of the meeting scheduled for January 6, 1955 (Mahl 1954).
Delgado prepared a systematic report that provided a balanced assessment on “intracerebral implantation of electrodes in human patients” (Delgado 1955b). Diagnostically, electrode implantation could be useful when “direct exploration of the brain is advisable” as in challenging cases of epilepsy. Electrical stimulation could be therapeutic and “may improve intractable pain” and be helpful in “some mental patients.” Electrocoagulation might have similar effects. The advantages—compared to conventional surgery—included less trauma, decreased anesthesia time, no need to expose brain, constancy of method, and the ability to leave electrodes in for days for additional studies. Risks were noted to be “brain destruction,” but this was described as “negligible” and less than that from ventriculography. He also responded to questions about the precision of placement, histological reactivity, and local trauma, noting that these were not at issue in experimental animal studies. Finally, he provided morbidity and mortality data citing his own work and that of Heath (Delgado 1955b).
Although not articulated as an ethics formulation, Delgado invoked both the primacy of patient welfare and the doctrine of proportionality (Hermeren 2012) in his arguments. He was careful to note that implantation of electrodes was contraindicated “when no direct benefit to the patient could be expected” (Delgado 1955b). And he viewed this benefit against the burdens, notably their implantation “in patients for whom more drastic procedures, such as lobotomy, had been recommended.”
A half century before his 2005 interview with John Horgan for Scientific American (Horgan 2005) and his conversation with the American College of Neuropsychopharmacology (Braslow and Delgado 2005), we see contemporaneous evidence of Delgado viewing electrical stimulation of the brain as an alternative to ablative procedures like lobotomy. This is not a post hoc justification but rather archival evidence of Delgado’s motivations, both scientific and ethical, during a formative period in his career, part of a historical record that distinguishes his legacy from Walter Freeman.
Coda
The response to Delgado’s report was not found in the Yale archives. And perhaps fittingly, the next entry was a letter thanking Smith, Kline and French Laboratories for an eight-channel electroencephalograph in which Delgado observes that “‘Thorazine’ appears to be a most intriguing drug and I think we are pinning down some of the brain structures which are particularly affected by it and by some other drugs” (Delgado 1955c). That aside foreshadowed the passing of an era: the decline of somatic therapies and the rise of neuroleptics.
For decades, given the ascendance of psychopharmacology, it was easy to remember psychosurgery with easy formulations of its promise and peril (Valenstein 1986) and gloss over nuances of biography and scientific contribution. But as neuroscience enters a new era of somatic therapy informed by circuit-based knowledge of brain maladies and emerging therapeutics like deep brain stimulation for Parkinson disease, depression, brain injury, and other conditions (DeLong and Benabid 2014; Dougherty 2018; Mayberg and others 2005; Schiff and others 2007), accuracy about the historical record becomes central to our ethical analysis (Fins 2003, 2021; Schleim 2021). Part of that corrective is to counter the conflation of Delgado’s and Freeman’s life and work. Appreciating their distinctive legacies can help guide research done today that might yet haunt future generations.
After a life at the vanguard of neuroscience, Delgado spoke of lessons learned. He observed that “even more important than research . . . is thinking about research ethics, about the philosophical implications of implanting electrodes, injecting chemicals into the brain” (Braslow and Delgado 2005). And perhaps anticipating the advent of neuroethics as an emerging discipline (Dana Foundation 2002), he admonished current researchers: “I think the newer generation of investigators should do more thinking about the implications of their research” (Braslow and Delgado 2005). His admonition points to the instrumentality of history as neuropsychiatric research progresses.
Footnotes
Acknowledgements
The authors wish to acknowledge the Oskar Diethelm History of Psychiatry Library at Weill Cornell Medical College and The John Fulton Papers in the Yale University Archives. Dr. Fins is grateful to Professor Krishna Winston of Wesleyan University for directing him to the writings of Heinz Paechter.
Dedication
The authors would like to dedicate this essay to Professor Donald Moon for fostering our collaboration and for decades of mentorship and scholarship at Wesleyan University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.