
Abstract
Background
Vericiguat improves outcomes in heart failure with reduced ejection fraction (HFrEF), but its vascular and hemodynamic effects remain unclear. We explored changes in flow-mediated dilation (FMD) and invasive hemodynamics after vericiguat in symptomatic patients with HFrEF receiving guideline-directed medical therapy (GDMT).
Methods
In this single-center, open-label, single-arm exploratory pilot study, 10 patients with symptomatic HFrEF underwent assessment of FMD, right heart catheterization at rest and during 20-W supine exercise, echocardiography, laboratory testing, and 6-min walk distance (6MWD) before and after vericiguat. Vericiguat was uptitrated to 10 mg/day where tolerated.
Results
After treatment, FMD increased from 4.7 (3.0-6.1) to 6.9 (5.5-7.6)% (P = .015), GLS improved from −6.8 (−8.6 to −5.5) to −9.0 (−10.5 to −6.7)% (P = .009), resting cardiac output increased from 3.8 (3.6-5.4) to 4.6 (3.5-5.4) L/min (P = .047), resting systemic vascular resistance decreased from 1664.1 (1327.2-1781.2) to 1293.1 (1143.6-1623.5) dyn·s·cm−5 (P = .002), and 6MWD increased from 334.0 (251.3-395.0) to 355.0 (262.5-453.8) m (P = .036). During 20-W exercise, cardiac output increased from 5.4 (4.6-5.9) to 6.5 (4.8-6.9) L/min (P = .030), whereas exercise systemic vascular resistance showed only a decreasing trend (P = .070).
Conclusions
In symptomatic patients with HFrEF receiving GDMT, vericiguat was associated with changes in peripheral vascular function and resting hemodynamic indices. However, exercise systemic vascular resistance did not improve significantly. These findings are exploratory and hypothesis-generating.
Introduction
Treatment for heart failure with reduced ejection fraction (HFrEF) has advanced substantially in recent years. In particular, the introduction of guideline-directed medical therapy (GDMT), including angiotensin receptor-neprilysin inhibitors, mineralocorticoid receptor antagonists (MRAs), sodium-glucose cotransporter 2 (SGLT2) inhibitors, and beta-blockers, has improved clinical outcomes in patients with HFrEF. 1 Combination use of these agents can reduce worsening heart failure even when administered at relatively low doses, 2 and early implementation has been shown to improve prognosis compared with conventional treatment strategies.3,4 However, in real-world clinical practice, optimization of GDMT is often limited by hypotension, renal dysfunction, or other tolerability issues, making sufficient intensification difficult in some patients. 5 Therefore, an unmet need remains for additional therapeutic strategies in HFrEF.
Vericiguat is a soluble guanylate cyclase (sGC) stimulator that enhances the nitric oxide (NO)-cyclic guanosine monophosphate (cGMP)-protein kinase G (PKG) pathway. It has been reported to reduce the risk of death and rehospitalization in patients with HFrEF after worsening heart failure, without substantially increasing hypotension or renal dysfunction.6‐8 However, the vascular and hemodynamic changes underlying its clinical benefits remain incompletely understood.
From the perspective of vascular effects mediated by enhanced cGMP signaling, sildenafil, a phosphodiesterase-5 inhibitor, has been reported to improve endothelial function indices in patients with chronic heart failure, suggesting that increased cGMP may be associated with improved endothelial function and vasodilatory responses. 9 In addition, riociguat, another sGC stimulator, has been shown to reduce systemic vascular resistance (SVR) in patients with pulmonary hypertension associated with HFrEF.10,11 Increased SVR contributes to increased afterload, reduced cardiac output, worsening heart failure physiology, and reduced exercise tolerance. 12 Furthermore, recent reports have suggested that vericiguat may improve exercise tolerance in patients with HFrEF. 13
Taken together, these observations suggest that changes in vascular function and hemodynamics may contribute to the effects of vericiguat; however, these aspects have not been sufficiently investigated. Therefore, in this exploratory pilot study, we evaluated peripheral vascular function using flow-mediated dilation (FMD) and assessed changes in resting and low-intensity exercise hemodynamics using right heart catheterization in symptomatic patients with HFrEF receiving GDMT.
Methods
Study Population
All study procedures were approved by the Ethics Committee of Kindai University (R03-284) and were conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrollment. Hospitalized or ambulatory patients aged 20 to 90 years were considered eligible if they had chronic heart failure with New York Heart Association (NYHA) functional class II or III symptoms and a left ventricular ejection fraction (LVEF) < 40% on echocardiography within 1 month before enrollment. Eligible patients had a history of chronic symptomatic heart failure and were receiving GDMT for heart failure, except for vericiguat, but continued to have exertional dyspnea corresponding to NYHA class II–III. Exclusion criteria were uncorrected primary valvular disease, orthopedic limitations, use of hormone replacement therapy, dementia, severe heart failure (NYHA class IV), end-stage renal disease, symptomatic hypotension, severe renal dysfunction, and terminal malignancy.
Study Design
Patients who met the inclusion criteria and provided written informed consent underwent baseline assessment before initiation of vericiguat. This study was designed as a single-arm, open-label, pre-post exploratory pilot study. Assessments included resting and exercise right heart catheterization data, blood tests, peripheral blood pressure, FMD, and 6-min walk distance (6MWD).
Vericiguat was initiated the day after baseline evaluation at 2.5 mg once daily and was uptitrated every 2 weeks over approximately 6 weeks, with a target dose of 10 mg/day. Follow-up assessments using the same protocol were performed 2 to 4 weeks after reaching the maximum tolerated dose.
Hemodynamic Assessment
A 7-Fr sheath was inserted through the internal jugular vein, and a 7-Fr Swan-Ganz catheter was advanced to measure right atrial pressure, right ventricular pressure, pulmonary artery pressure, pulmonary artery wedge pressure (PAWP), and cardiac output (CO) by thermodilution. Blood pressure, pulse rate, and peripheral oxygen saturation (SpO₂) were also measured in the upper extremity. After resting measurements, patients underwent 3 min of lower-limb exercise on a supine ergometer at a fixed workload of 20-W. This protocol was used to evaluate within-subject hemodynamic responses to a standardized low-intensity workload during right heart catheterization, not maximal exercise capacity. The workload was selected for feasibility and safety. However, because it has not been fully validated as an individualized test in HFrEF, relative exercise intensity may have differed among patients; therefore, the results should be interpreted as exploratory.
Flow-Mediated Dilation
FMD was assessed in accordance with established guidelines. 14 On the examination day, patients visited the laboratory approximately 3 h after taking vericiguat and remained in the supine position for at least 1 h before FMD measurement. Water intake was permitted, but caffeinated beverages were restricted. A blood pressure cuff was placed on the forearm after baseline brachial artery diameter measurement. The cuff was then inflated to 50 mm Hg above resting systolic blood pressure for 5 min. After cuff release, brachial artery diameter was continuously recorded for 2 min, and the maximum post-deflation change was quantified as FMD. Measurements were performed by 2 physicians blinded to patient details.
Primary Endpoints
The primary efficacy end points were the changes in resting and exercise SVR from baseline. Secondary end points included changes in FMD, other resting and exercise hemodynamic parameters, 6MWD, B-type natriuretic peptide (BNP), and echocardiographic parameters. Primary and secondary end points were prespecified in the study protocol; all additional analyses were considered exploratory.
Statistical Analysis
Categorical variables are presented as numbers (%), and continuous variables are presented as median (interquartile range). Because of the small sample size and exploratory nature of the study, normality was assessed using the Shapiro-Wilk test together with graphical assessment of the data distribution. Variables with approximately normal paired differences were analyzed using the paired Student's t test, and mean paired differences with 95% confidence intervals (CIs) were calculated. Variables with non-normal paired differences were analyzed using the Wilcoxon signed-rank test.
Because this was a small exploratory pilot study with multiple end points, there was a substantial risk of inflated type I error. No formal adjustment for multiple comparisons was applied, and all P values were interpreted as nominal and exploratory. Therefore, statistical analyses were intended to identify hypothesis-generating findings rather than provide confirmatory evidence of efficacy. All analyses were performed using JMP version 16.0 (SAS Institute, Cary, NC, USA). Two-sided P values <.05 were considered nominally significant.
Results
Baseline Characteristics
Ten patients with HFrEF were enrolled in this study. Median age was 73.0 (66.5-78.0) years, and all patients had NYHA functional class II or III symptoms (Table 1). Despite receiving GDMT, most patients had been hospitalized at least twice for heart failure. All participants underwent coronary angiography, and 2 had previously undergone percutaneous coronary intervention; however, no significant residual coronary stenosis was present at enrollment.
Baseline Characteristics of the Study Population.
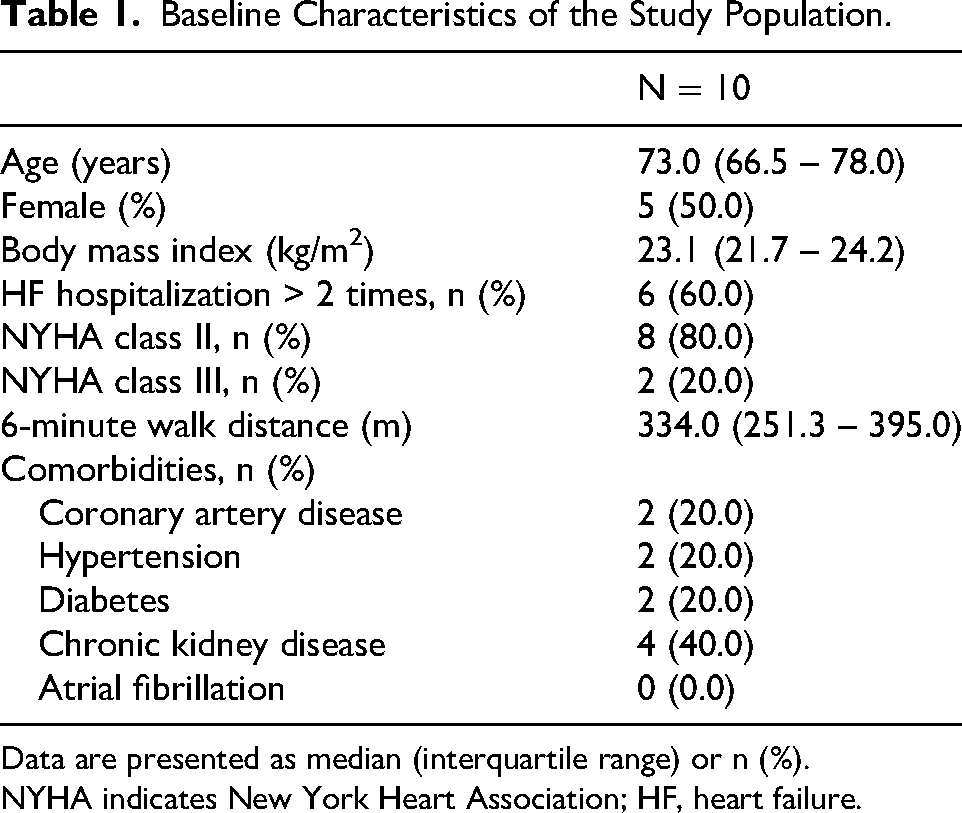
Data are presented as median (interquartile range) or n (%).
NYHA indicates New York Heart Association; HF, heart failure.
Details regarding the content and intensity of background GDMT before vericiguat initiation are shown in Table 2. There was substantial interpatient variability in background treatment composition and dose, particularly with respect to renin-angiotensin system inhibitors and beta-blockers, for which target-dose achievement rates were relatively low. Echocardiography showed an enlarged left ventricular end-diastolic diameter (LVDd) of 60.0 (57.3-67.0) mm and a reduced ejection fraction (EF) of 33.5 (29.5-37.3) % (Table 3).
Intensity of Background GDMT Before Vericiguat Initiation.
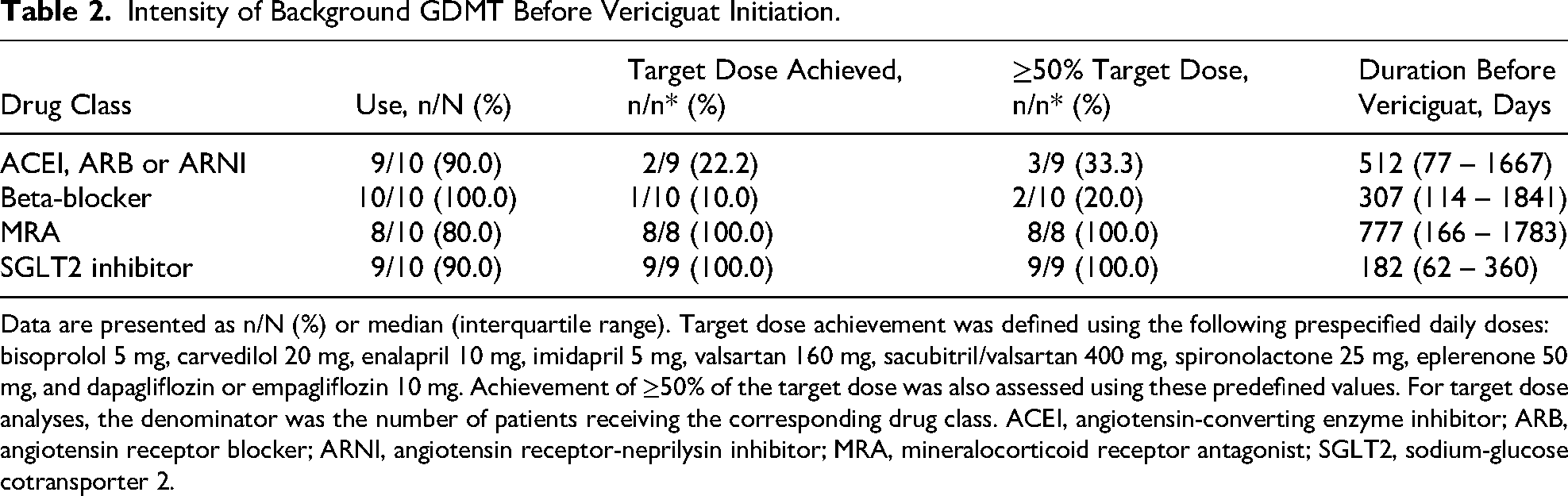
Data are presented as n/N (%) or median (interquartile range). Target dose achievement was defined using the following prespecified daily doses: bisoprolol 5 mg, carvedilol 20 mg, enalapril 10 mg, imidapril 5 mg, valsartan 160 mg, sacubitril/valsartan 400 mg, spironolactone 25 mg, eplerenone 50 mg, and dapagliflozin or empagliflozin 10 mg. Achievement of ≥50% of the target dose was also assessed using these predefined values. For target dose analyses, the denominator was the number of patients receiving the corresponding drug class. ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor-neprilysin inhibitor; MRA, mineralocorticoid receptor antagonist; SGLT2, sodium-glucose cotransporter 2.
Clinical, Laboratory, Echocardiographic, and Resting Hemodynamic Data at Baseline and after Vericiguat Treatment
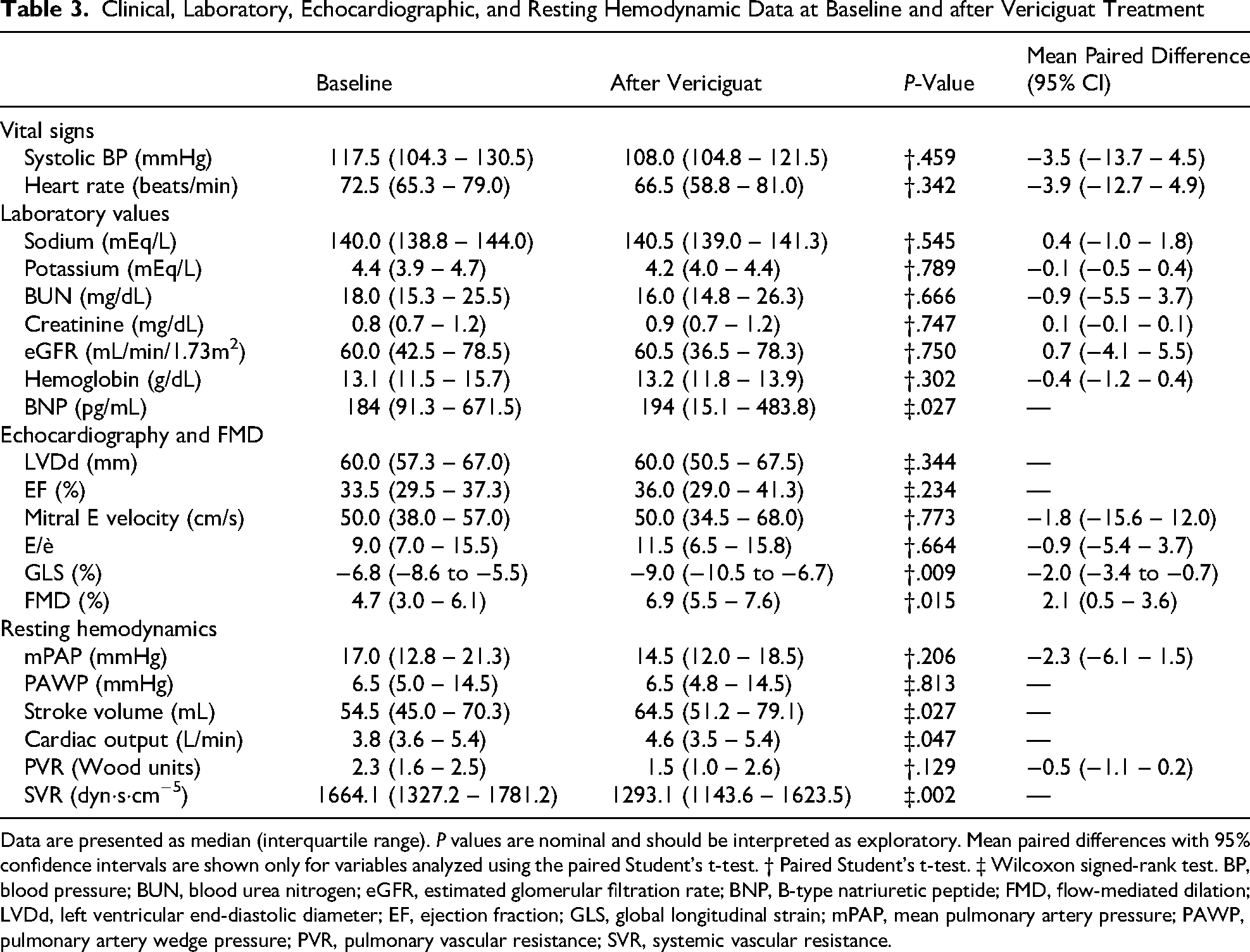
Data are presented as median (interquartile range). P values are nominal and should be interpreted as exploratory. Mean paired differences with 95% confidence intervals are shown only for variables analyzed using the paired Student’s t-test. † Paired Student’s t-test. ‡ Wilcoxon signed-rank test. BP, blood pressure; BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate; BNP, B-type natriuretic peptide; FMD, flow-mediated dilation; LVDd, left ventricular end-diastolic diameter; EF, ejection fraction; GLS, global longitudinal strain; mPAP, mean pulmonary artery pressure; PAWP, pulmonary artery wedge pressure; PVR, pulmonary vascular resistance; SVR, systemic vascular resistance.
Changes During Vericiguat Treatment
All baseline measurements were repeated at 75.5 (62.3-89.0) days after initiation of vericiguat. All patients were successfully uptitrated to 10 mg/day. No changes in heart failure medications other than vericiguat were made during follow-up, and no cardiovascular events occurred.
Clinical Laboratory Data
No significant changes were observed in electrolyte levels or estimated glomerular filtration rate (eGFR). In contrast, serum BNP levels showed a nominally significant paired change after vericiguat treatment from 184 (91.3-671.5) to 194 (15.1-483.8) pg/mL, (P = .027) (Table 3, Figure 1A). However, per-patient analysis showed BNP decreased in 7 of 10 patients and increased or remained unchanged in the remaining 3, indicating substantial inter-individual variability.

Changes in BNP (A) and flow-mediated dilation (B) after vericiguat treatment. Individual paired values are shown (n = 10). BNP was analyzed using the Wilcoxon signed-rank test, and flow-mediated dilation was analyzed using the paired Student's t test. Although the post-treatment median BNP was slightly higher, 7 of 10 patients showed lower BNP values at follow-up.
Echocardiography and Flow-Mediated Dilation
No clear changes were observed in LVDd or EF. However, global longitudinal strain (GLS) improved significantly from −6.8 (−8.6 to −5.5) to −9.0 (−10.5 to −6.7) %, (P = .009), and FMD increased significantly after vericiguat treatment from 4.7 (3.0-6.1) to 6.9 (5.5-7.6) %, (P = .015) (Table 3, Figure 1B).
Resting Vital Signs and Hemodynamics
No significant changes were observed in systolic blood pressure or heart rate (Table 3). On right heart catheterization, systolic blood pressure, mean pulmonary artery pressure (mPAP), and PAWP did not change significantly during treatment (Figure 2A-C). In contrast, stroke volume increased from 54.5 (45.0-70.3) to 64.5 (51.2-79.1) mL, (P = .027), cardiac output increased from 3.8 (3.6-5.4) to 4.6 (3.5-5.4) L/min, (P = .047), and SVR decreased from 1664.1 (1327.2-1781.2) to 1293.1 (1143.6-1623.5) dyn·s·cm−5, (P = .002) (Figure 2D-F). Pulmonary vascular resistance did not change significantly from 2.3 (1.6-2.5) to 1.5 (1.0-2.6) Wood units (P = .129) (Table 3).
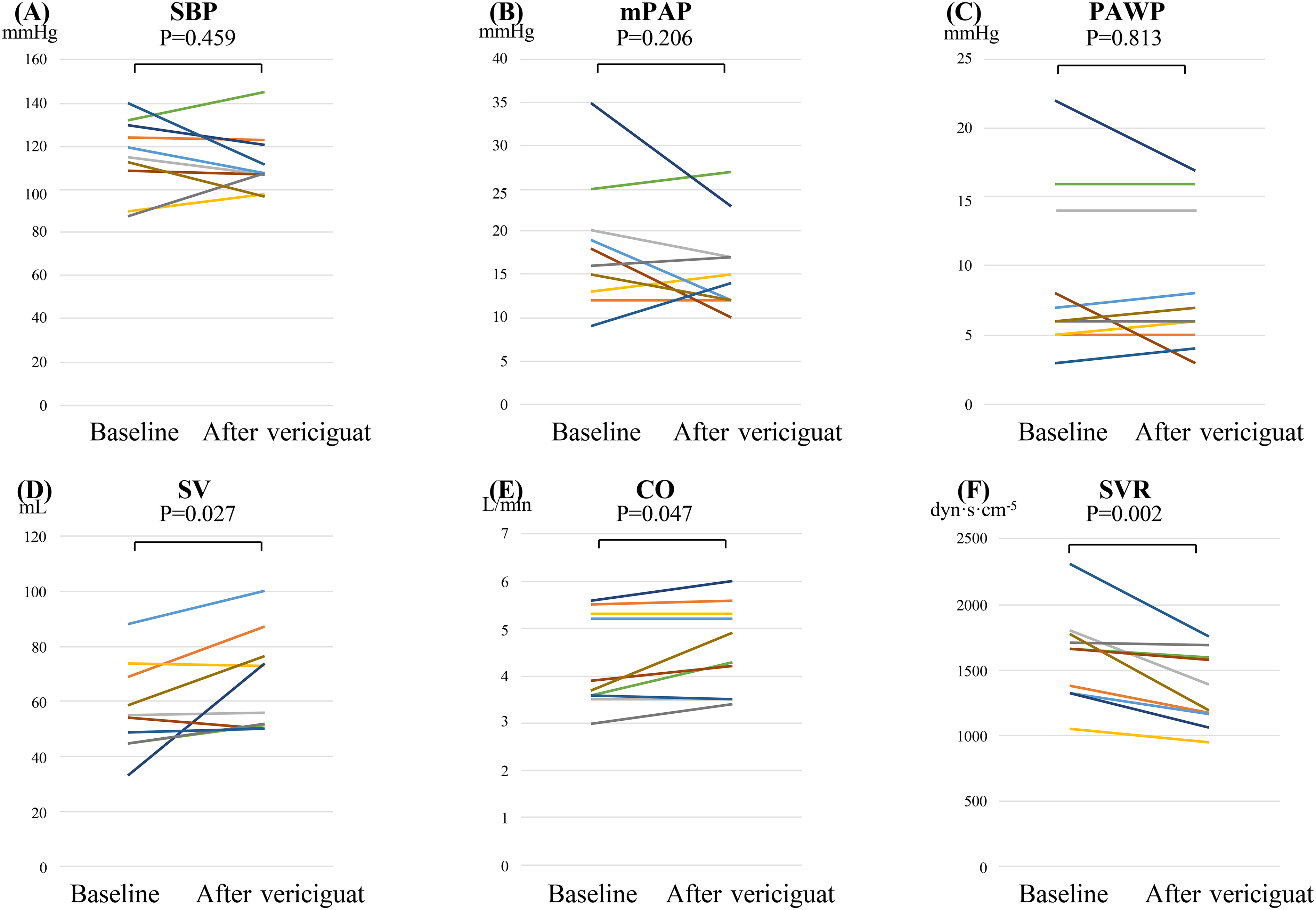
Changes in resting hemodynamic parameters after vericiguat treatment. Paired data are shown for systolic blood pressure (
Exercise Hemodynamics
Heart rate, systolic blood pressure, mPAP, and PAWP during exercise did not change significantly. Exercise CO increased after vericiguat treatment from 5.4 (4.6-5.9) to 6.5 (4.8-6.9) L/min, (P = .030). However, the primary exercise vascular end point, exercise SVR, did not reach statistical significance and showed only a decreasing trend from 1276.2 (1079.4-1570.0) to 1041.4 (961.3-1522.7) dyn·s·cm−5, (P = .070) (Table 4, Figure 3A and B). In addition, 6MWD increased after treatment from 334.0 (251.3-395.0) to 355.0 (262.5-453.8) m, (P = .036) (Figure 3C).
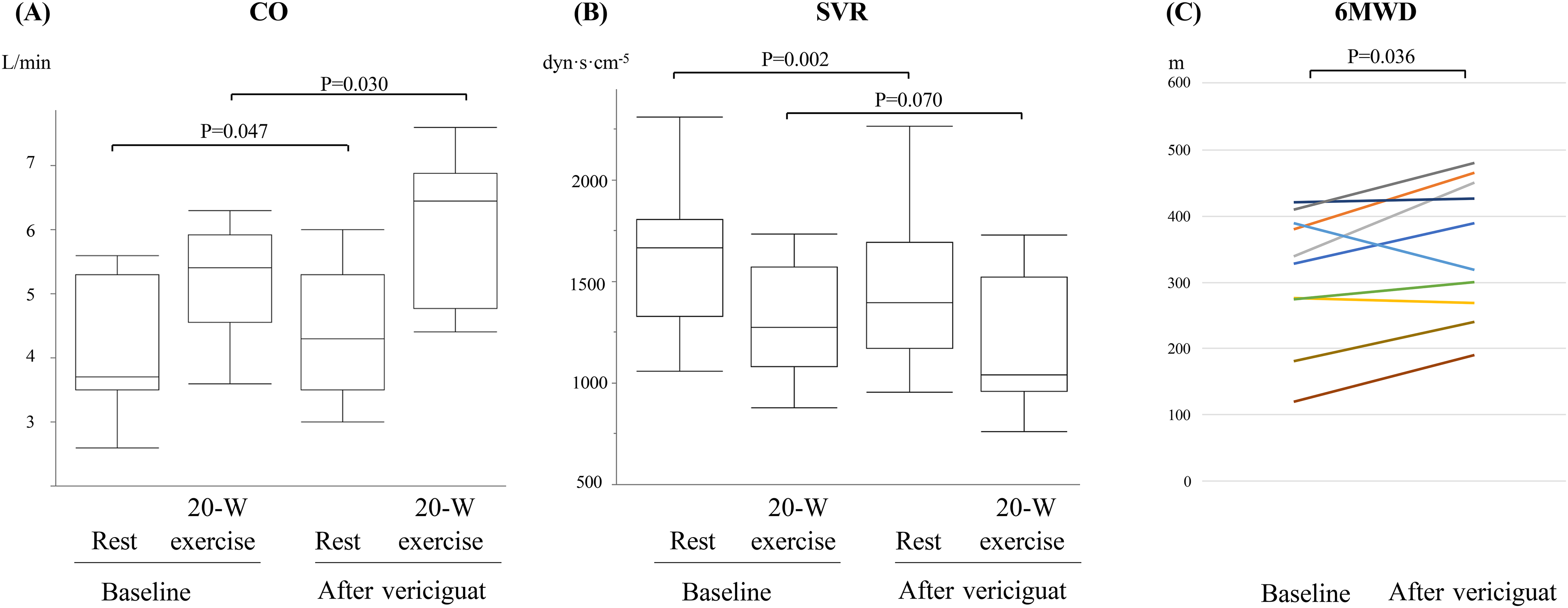
Changes in cardiac output, systemic vascular resistance, and 6-min walk distance after vericiguat treatment. Cardiac output (
Hemodynamic Data Obtained by Right Heart Catheterization During 20-W Exercise
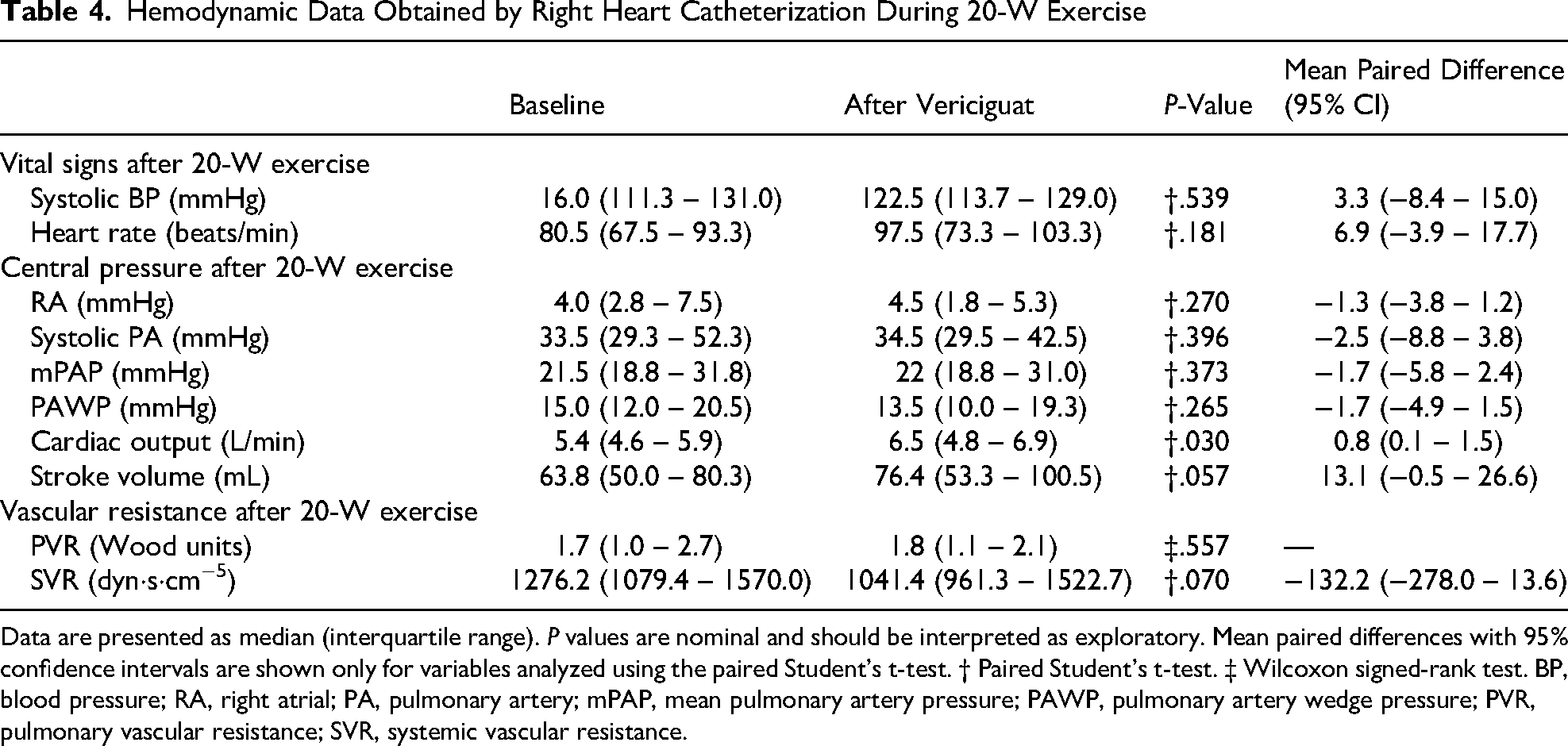
Data are presented as median (interquartile range). P values are nominal and should be interpreted as exploratory. Mean paired differences with 95% confidence intervals are shown only for variables analyzed using the paired Student’s t-test. † Paired Student’s t-test. ‡ Wilcoxon signed-rank test. BP, blood pressure; RA, right atrial; PA, pulmonary artery; mPAP, mean pulmonary artery pressure; PAWP, pulmonary artery wedge pressure; PVR, pulmonary vascular resistance; SVR, systemic vascular resistance.
Discussion
This study was a single-arm, open-label, pre-post exploratory pilot study in 10 symptomatic patients with HFrEF receiving GDMT. We assessed peripheral conduit vessel function using FMD together with invasive resting and low-intensity exercise hemodynamics before and after vericiguat treatment. To our knowledge, reports combining FMD with invasive resting and low-intensity exercise hemodynamic assessment in a vericiguat-treated HFrEF cohort remain limited. In this study, changes were observed in BNP, 6MWD, FMD, resting CO, and resting SVR after vericiguat treatment. However, because this study lacked a control group, the observed changes cannot be definitively attributed to vericiguat. They may instead reflect natural variation, regression to the mean, temporal changes in congestion status, measurement variability, or learning effects in 6MWD. Therefore, the present findings should be interpreted as hypothesis-generating findings of association rather than evidence of causality.
With respect to prior studies, the LEPHT trial showed that riociguat, another sGC stimulator, was associated with reduced SVR and increased CO in patients with HFrEF. 11 In addition, Suzuki et al reported that, in 12 patients with HFrEF and worsening heart failure, vericiguat was associated with lower PAWP in the chronic phase, whereas Cardiac Index and SVR did not change significantly. 15 This discrepancy may partly relate to differences in the proportion of patients able to reach the target dose. In SOCRATES-REDUCED, the 10-mg group showed a reduction in NT-proBNP, 16 and in the present study, all patients were uptitrated to 10 mg/day. Thus, the changes observed here may have been obtained under sufficient-dose vericiguat treatment, although dose-dependent effects cannot be established from this study design alone.
Although changes were observed in resting CO, SVR, FMD, BNP, GLS, and 6MWD, statistical significance and clinical significance should be interpreted separately. In particular, BNP responses were heterogeneous and should be interpreted cautiously. Although the paired analysis yielded a nominally significant result, the post-treatment group median was slightly higher, while most individual patients showed downward trajectories. The absolute increase in resting CO was modest, and 6MWD is susceptible to learning effects and day-to-day variation. Likewise, FMD reflects peripheral conduit vessel endothelial function but is subject to operator dependence and technical variability; therefore, changes observed in such a small sample should not be overgeneralized. These findings should be viewed as exploratory observations rather than confirmation of clinical efficacy.
Previous reports have shown improvements in cardiopulmonary exercise testing (CPET) parameters after vericiguat treatment in patients with HFrEF. 13 In contrast, the present study used only 6MWD, which does not allow separation of ventilatory response, oxygen uptake kinetics, peripheral skeletal muscle function, or circulatory reserve. Therefore, the present data do not allow a mechanistic interpretation of the observed change in 6MWD. In particular, we cannot conclude that changes in FMD or hemodynamic parameters mediated the improvement in walking distance. Rather, the results suggest that vascular function indices, resting hemodynamics, and functional measures may have changed in parallel.
Exercise hemodynamics were assessed after 3 min of supine ergometer exercise at a fixed workload of 20-W. This approach was practical and safe during right heart catheterization and allowed for a within-subject comparison under standardized low-intensity conditions. However, a fixed absolute workload does not provide physiologically equivalent stress across patients with different functional capacities. Accordingly, the exercise findings should be interpreted as exploratory within-subject observations under a standardized low-level workload rather than as a definitive assessment of exercise hemodynamic improvement. Importantly, although exercise CO increased, the primary exercise end point, exercise SVR, did not reach statistical significance and showed only a decreasing trend (P = .070). Therefore, our findings do not conclusively demonstrate improved exercise hemodynamics.
Mechanistically, the NO-cGMP-PKG pathway plays an important role in hemodynamic regulation and cardiovascular protection.17‐19 In chronic heart failure, this pathway is thought to be impaired because of reduced NO bioavailability, oxidative stress-related sGC dysfunction, and increased phosphodiesterase activity.20‐22 The observed changes in resting SVR, CO, FMD, BNP, and GLS are consistent with this pharmacologic framework. Nevertheless, the present study was not designed to establish mechanism and should be regarded as an exploratory study describing associations rather than mechanistic proof.
Limitations
This study has several important limitations. First, it was a small, single-arm, open-label, pre-post exploratory pilot study involving only 10 patients and no control group; therefore, the observed changes cannot be distinguished from natural variation, temporal changes in congestion status, measurement error, or learning effects on 6MWD. Second, exercise tolerance was assessed only by 6MWD rather than by more physiologically informative methods such as CPET, which limits mechanistic interpretation. Third, exercise hemodynamics were evaluated after 3 min of fixed 20-W supine ergometer exercise; although this low-level protocol was selected for safety and feasibility, it does not provide equivalent relative exercise intensity across patients. In addition, the primary exercise endpoint, exercise SVR, did not reach statistical significance and should therefore be interpreted with caution. Finally, the duration and intensity of background GDMT varied across patients, and the effects of ongoing background therapy cannot be completely excluded.
Conclusion
In this exploratory pilot study of symptomatic patients with HFrEF receiving GDMT, vericiguat treatment was associated with changes in resting SVR, CO, FMD, BNP, and 6MWD. However, the primary exercise endpoint, exercise SVR, did not show a statistically significant change. In addition, because this was a single-arm, open-label, pre-post study, no conclusions can be drawn regarding causality or underlying mediating mechanisms. Accordingly, these findings should be regarded as hypothesis-generating with respect to the vascular and hemodynamic effects of vericiguat and warrant confirmation in larger, controlled, prospective studies.
Footnotes
Ethical Considerations
All the experimental protocols were approved by the Kindai University Ethics Committee (R03-284) and complied with the principles set forth in the Declaration of Helsinki for studies involving human patients.
Author Contributions
All authors reviewed, revised, and approved the manuscript for submission. K.K. and M.U. contributed to data curation. Y.F. and T.T. performed the data analysis. G.N. supervised the study. Y.F. drafted the manuscript, and T.T. reviewed and edited it.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Institutional Review Board
Approving Organization: Ethics Committee, Kindai University School of Medicine