
Abstract
Background
Aldosterone excess contributes to uncontrolled and resistant hypertension, making aldosterone synthase inhibition a promising therapeutic strategy. Recent randomized trials have evaluated the selective aldosterone synthase inhibitors Lorundrostat and Baxdrostat; however, their efficacy and safety have not been comprehensively synthesized.
Methods
PubMed, Embase, and Cochrane CENTRAL were searched from inception through April 2026 for randomized controlled trials evaluating Lorundrostat or Baxdrostat in adults with uncontrolled or resistant hypertension. The primary efficacy outcome was placebo-adjusted change in systolic blood pressure (SBP). Safety outcomes included hyperkalemia, treatment-emergent adverse events (TEAEs), and serious adverse events (SAEs). Drug-specific pooled analyses were performed using random-effects models.
Results
Three randomized trials of Lorundrostat (n=1,568) demonstrated a significant reduction in SBP compared with placebo (mean difference [MD], -7.51 mmHg; 95% CI, -10.30 to -4.71; I2 = 0%). Lorundrostat increased the risks of hyperkalemia (RR, 8.06; 95% CI, 2.92–22.27) and TEAEs (RR, 1.45; 95% CI, 1.27–1.66), without a significant increase in SAEs. Three placebo-controlled Baxdrostat trials (n = 1,483) also demonstrated significant reductions in office SBP (MD, -8.63 mmHg; 95% CI, -11.30 to -5.96; I2 = 0%). Baxdrostat increased the risk of hyperkalemia (RR, 3.81; 95% CI, 1.82–7.97) but was not associated with significant increases in TEAEs or SAEs.
Conclusions
Selective aldosterone synthase inhibition with Lorundrostat and Baxdrostat produced clinically meaningful reductions in SBP in patients with uncontrolled or resistant hypertension. Hyperkalemia emerged as the principal safety concern, whereas serious adverse events were not significantly increased. Larger and longer-term studies are needed to define long-term safety and cardiovascular outcomes.
Keywords
Introduction
Hypertension remains the leading modifiable risk factor for cardiovascular morbidity and mortality worldwide, affecting more than one billion individuals globally. Its prevalence continues to rise due to an aging population and increasing rates of obesity and metabolic disease. Elevated blood pressure is a major contributor to ischemic heart disease (IHD), stroke, heart failure, and chronic kidney disease (CKD), and even modest reductions in systolic blood pressure substantially reduce cardiovascular events and mortality.1-6 Despite major therapeutic advances, blood pressure control remains suboptimal, with many treated patients failing to achieve guideline-recommended targets. This persistent burden underscores the need for improved therapeutic strategies targeting key pathophysiologic mechanisms of hypertension.7-12
Among treated hypertensive patients, uncontrolled and resistant hypertension represent particularly challenging clinical phenotypes. Resistant hypertension, typically defined as blood pressure that remains above target despite treatment with three or more antihypertensive agents, including a diuretic, affects approximately 10–20% of treated individuals and is associated with markedly increased cardiovascular and renal risk.13-15 Multiple mechanisms contribute to treatment resistance, including persistent volume expansion, sympathetic overactivity, and dysregulation of the renin-angiotensin-aldosterone system (RAAS).16-18
A growing body of evidence implicates aldosterone excess as a central contributor to uncontrolled and resistant hypertension.19-22 Beyond its role in sodium retention and extracellular volume expansion, excess aldosterone promotes vascular inflammation, endothelial dysfunction, oxidative stress, and myocardial and renal fibrosis, contributing to both blood pressure elevation and adverse cardiovascular remodeling.23-27 Notably, inappropriate aldosterone secretion is frequently observed in patients with resistant hypertension even in the absence of overt primary hyperaldosteronism, highlighting the importance of mineralocorticoid signaling in treatment-resistant disease.28-31
These observations have provided the mechanistic basis for the use of mineralocorticoid receptor antagonists (MRAs), which have demonstrated substantial antihypertensive efficacy. In the PATHWAY-2 trial, spironolactone produced the greatest blood pressure reduction among add-on therapies in patients with resistant hypertension. 32 However, MRAs are limited by adverse effects, including hyperkalemia and worsening renal function, particularly in patients with chronic kidney disease (CKD) or concomitant renin-angiotensin system (RAS) blockade, as well as endocrine-related side effects such as gynecomastia and menstrual irregularities. These limitations have prompted an investigation into therapeutic strategies that more directly target aldosterone biology.33-35
Aldosterone synthase inhibitors (ASIs) have emerged as a novel therapeutic strategy for hypertension by targeting aldosterone biosynthesis upstream of mineralocorticoid receptor activation.36-39 Recent advances in drug development have enabled the creation of highly selective CYP11B2 inhibitors, including baxdrostat and lorundrostat, which suppress aldosterone production while minimizing effects on cortisol synthesis.
Randomized clinical trials (RCTs) of baxdrostat and lorundrostat have demonstrated clinically meaningful reductions in systolic blood pressure (SBP) in patients with uncontrolled or resistant hypertension.40-45 However, differences in study populations, trial designs, dosing strategies, and outcome reporting have made it difficult to determine the overall efficacy and safety of selective aldosterone synthase inhibition. In addition, the incidence of clinically important adverse events, particularly hyperkalemia, has not been systematically evaluated across available trials.
Accordingly, we conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) evaluating baxdrostat and lorundrostat in patients with uncontrolled or resistant hypertension. The primary objective was to quantify their effects on SBP, while secondary objectives included assessment of hyperkalemia, treatment-emergent adverse events, and serious adverse events.
Methods
This systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 46
Literature Search Strategy
A systematic search of PubMed, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) was performed from database inception through April 2026 to identify randomized controlled trials (RCTs) evaluating selective aldosterone synthase inhibitors (ASIs) in adults with uncontrolled or resistant hypertension. Search terms included combinations of “aldosterone synthase inhibitor,” “baxdrostat,” “lorundrostat,” “CIN-107,” “hypertension,” “resistant hypertension,” and related keywords. The complete search strategy is provided in the Supplemental Appendix. Reference lists of relevant studies and review articles were also screened to identify additional eligible studies.
Inclusion and Exclusion Criteria
Studies Were Eligible if They met the Following Criteria
• Enrolled adults (≥18 years) with uncontrolled or resistant hypertension; • Evaluated a selective aldosterone synthase inhibitor (baxdrostat or lorundrostat); • Included a placebo comparator group; and • Randomized controlled trials (RCTs).
Exclusion Criteria Included
• Observational studies, review articles, case reports, conference abstracts, editorials, letters, and commentaries. • Articles published in languages other than English. • Studies lacking a placebo comparator.
Study Selection
All records were imported into EndNote, and duplicates were removed. The preliminary screening was conducted using titles and abstracts. Two authors evaluated the titles/abstracts independently and then assessed the full texts, with any disagreements resolved through consensus or by involving a third author. Full-text articles were evaluated against predefined inclusion and exclusion criteria. The selection process is depicted in a PRISMA flow diagram (Figure 1). Prisma flow diagram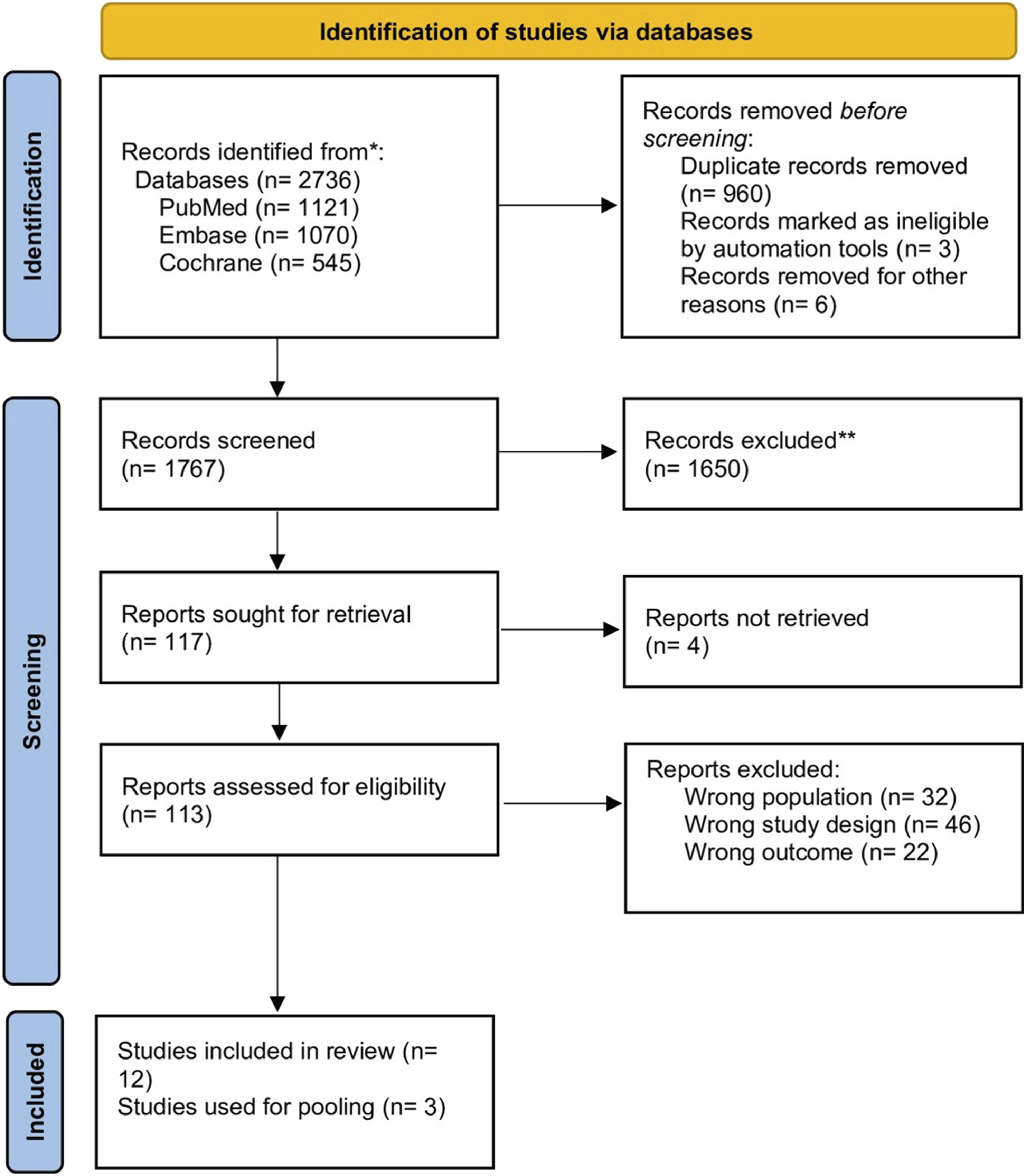
Data Extraction
Two authors independently extracted data from each eligible study. Extracted information included study characteristics, patient demographics, intervention details, comparator group, follow-up duration, and reported efficacy and safety outcomes. For efficacy analyses, placebo-adjusted changes in systolic blood pressure (SBP) were extracted. For safety analyses, numbers of participants experiencing hyperkalemia, treatment-emergent adverse events (TEAEs), and serious adverse events (SAEs) were collected from published manuscripts, supplementary appendices, and publicly available trial reports.
Risk of Bias and Quality Assessment
Two authors independently assessed risk of bias using the Cochrane Risk of Bias-2 (RoB-2) tool for RCTs. The following domains were evaluated: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. Each domain was judged as low risk of bias, some concerns, or high risk of bias, and an overall risk-of-bias judgment was assigned according to RoB-2 guidance. Disagreements were resolved through discussion and consensus, with consultation of a third author when necessary.
Outcomes
The primary efficacy outcome was the placebo-adjusted mean change in SBP from baseline.
Safety outcomes included: • Hyperkalemia: Hyperkalemia was defined according to trial-specific definitions. In the included studies, hyperkalemia was generally defined as serum potassium >5.5 mmol/L. • Serious adverse events (SAEs) • Treatment-emergent adverse events (TEAEs)
In addition, prespecified adverse events of special interest and notable TEAEs reported in the included trials were extracted and summarized descriptively.
Statistical Analysis
Drug-specific meta-analyses were performed separately for lorundrostat and baxdrostat. For continuous outcomes, pooled placebo-adjusted mean differences (MDs) and corresponding 95% confidence intervals (CIs) were calculated using the inverse-variance method. When multiple active treatment arms were compared with a common placebo group, treatment groups were combined using standard Cochrane-recommended methods to generate a single pairwise comparison while avoiding double-counting of participants in the placebo arm. Random-effects models were used for all primary analyses, with between-study variance estimated using restricted maximum likelihood (REML). Hartung–Knapp adjustments were applied to random-effects models to account for uncertainty in between-study variance estimates when a limited number of studies were available. A continuity correction of 0.5 was applied to studies with zero events in one treatment arm.
Statistical heterogeneity was assessed using Cochran’s Q test and quantified using the I2 statistic, with values of approximately 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively.
Sensitivity Analysis
Several sensitivity analyses were performed to assess the robustness of the findings.
For lorundrostat, leave-one-out analyses were conducted by sequentially removing each study to assess the influence of individual trials on the pooled efficacy estimate. A sensitivity analysis restricted to trials measuring office SBP was performed to evaluate the potential impact of outcome measurement modality, given that ADVANCE-HTN assessed ambulatory blood pressure rather than office blood pressure. An additional analysis using the highest evaluated lorundrostat dose from each trial was conducted to explore potential dose-related treatment effects. Finally, pooled estimates derived from fixed-effect and random-effects models were compared to assess the robustness of the findings under different statistical assumptions.
For baxdrostat, an analysis incorporating Bax24, which evaluated 24-hour ambulatory SBP, was conducted to examine the impact of outcome measurement modality on pooled treatment effects and heterogeneity.
Software
All analyses were conducted using R statistical software version 4.6.0 with the meta package version 8.3.0.
Publication Bias
Assessment of publication bias using funnel plots or statistical tests was not performed because fewer than ten studies were included in the analysis, which limits the reliability of such methods.
Results
Study Characteristics
A total of seven randomized, placebo-controlled trials evaluating selective aldosterone synthase inhibitors (ASIs) were identified. Three trials evaluated lorundrostat (TARGET-HTN, LAUNCH-HTN, and ADVANCE-HTN), while four trials evaluated baxdrostat (BrigHTN, BaxHTN, CKD-HTN, and Bax24).
The lorundrostat trials enrolled 1,568 participants and compared lorundrostat with placebo across varying dose regimens and follow-up durations.
Baxdrostat trials enrolled 1483 patients. The primary efficacy meta-analysis included three trials (BrigHTN, BaxHTN, and CKD-HTN). Bax24, which assessed 24-hour ambulatory SBP, was analyzed separately in sensitivity analyses. For safety outcomes, pooled analyses included BrigHTN, BaxHTN, and Bax24 trials, which reported sufficient data on hyperkalemia, treatment-emergent adverse events (TEAEs), and serious adverse events (SAEs). The CKD-HTN trial was excluded from quantitative safety analyses because the study population had substantially impaired renal function and a markedly different baseline risk of hyperkalemia, which was considered likely to introduce substantial clinical heterogeneity.
Characteristics of Included Trials
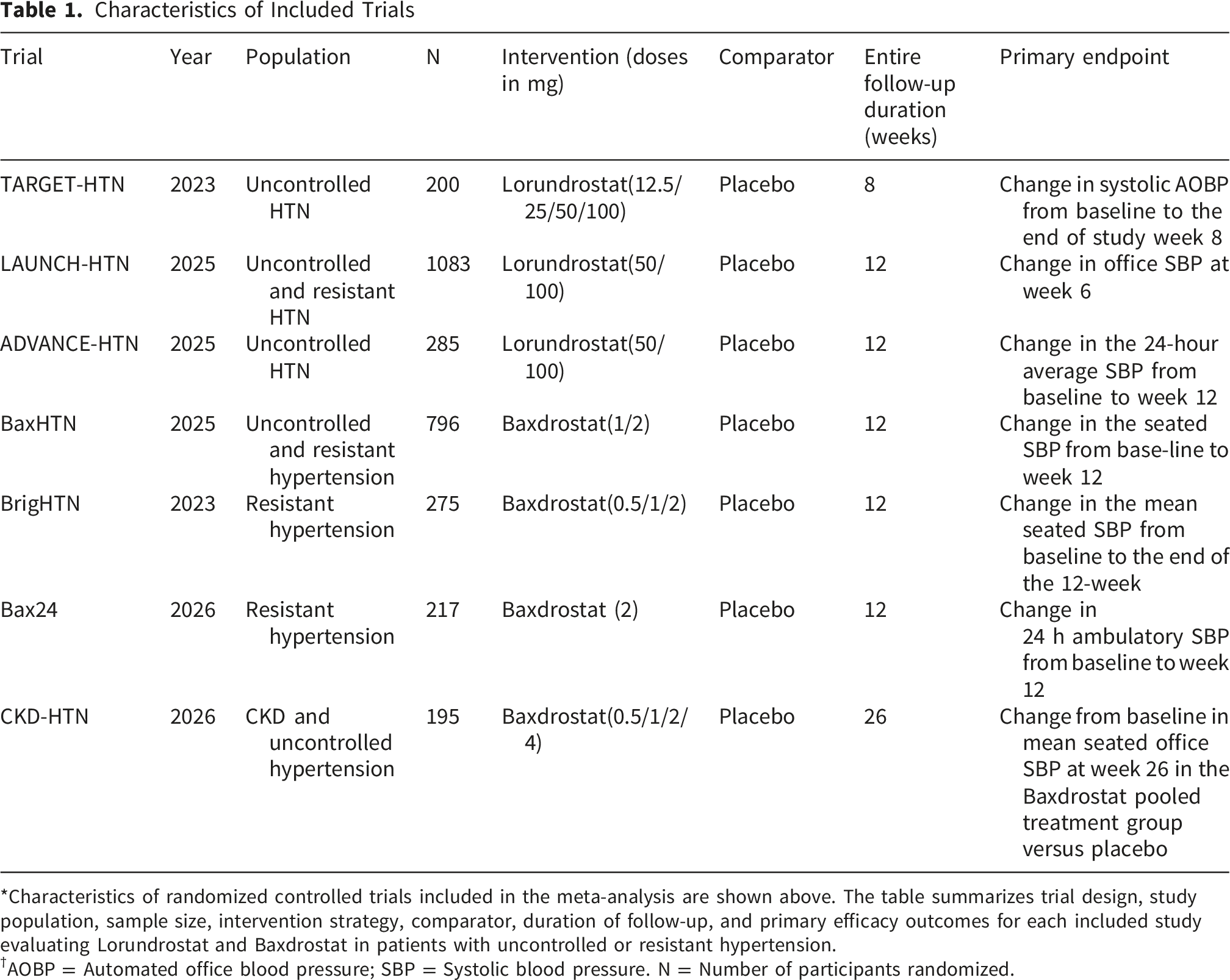
*Characteristics of randomized controlled trials included in the meta-analysis are shown above. The table summarizes trial design, study population, sample size, intervention strategy, comparator, duration of follow-up, and primary efficacy outcomes for each included study evaluating Lorundrostat and Baxdrostat in patients with uncontrolled or resistant hypertension.
†AOBP = Automated office blood pressure; SBP = Systolic blood pressure. N = Number of participants randomized.
Baseline Patient Characteristics
Across the included trials for lorundrostat, the mean age of participants ranged from 60 to 65.7 years, reflecting a population of older adults with hypertension. The proportion of male participants ranged from 40% to 60% across studies. Participants were generally overweight or obese, with mean body mass index (BMI) values ranging from 31.25 to 32.8 kg/m2. Baseline systolic blood pressure (SBP) was elevated across trials, ranging from 142.2 to 147.9 mm Hg, consistent with populations with uncontrolled hypertension despite therapy. The prevalence of diabetes mellitus (DM) ranged from 31.2% to 41.8%, indicating a substantial burden of cardio-metabolic comorbidity within the study populations. Baseline renal function was generally preserved, with mean estimated glomerular filtration rate (eGFR) values ranging from 75.3 to 91.4 mL/min/1.73 m2.
Across the included baxdrostat trials, mean age ranged from 60.5 to 66.0 years, and 56% to 68% of participants were male. Mean BMI ranged from 31.3 to 32.6 kg/m2, while baseline SBP ranged from 147.5 to 151.2 mmHg. The prevalence of DM varied substantially across studies, ranging from 34.0% to 80.0%, with the highest prevalence observed in CKD-HTN. Mean eGFR ranged from 44.0 to 85.5 mL/min/1.73 m2, reflecting inclusion of both preserved kidney function and chronic kidney disease populations.
Baseline Characteristics of Participants
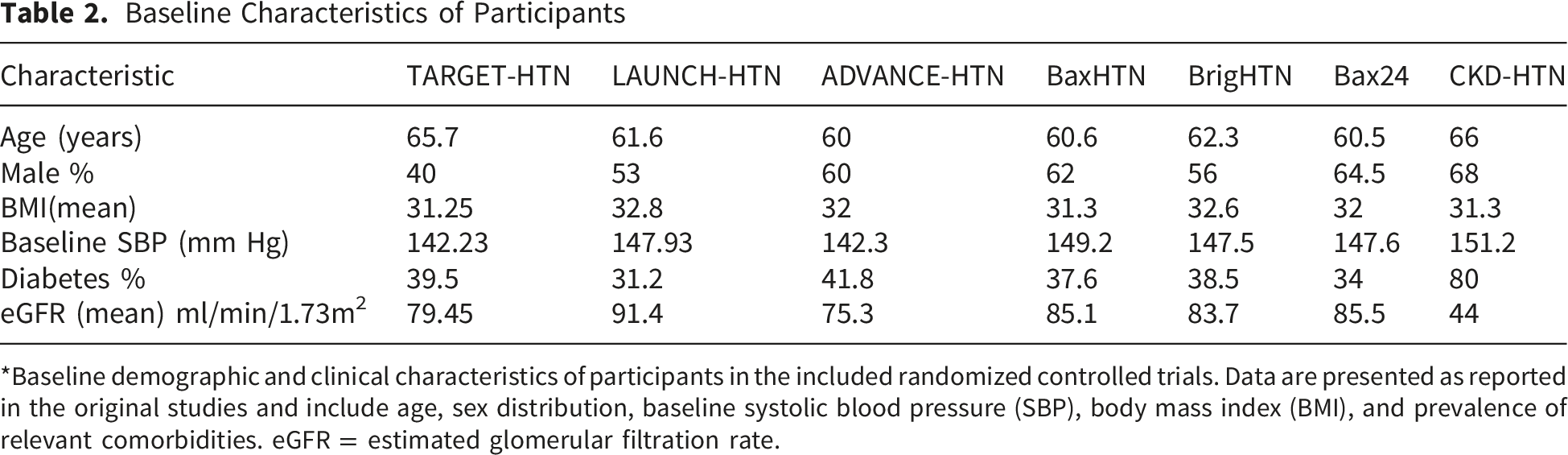
*Baseline demographic and clinical characteristics of participants in the included randomized controlled trials. Data are presented as reported in the original studies and include age, sex distribution, baseline systolic blood pressure (SBP), body mass index (BMI), and prevalence of relevant comorbidities. eGFR = estimated glomerular filtration rate.
Primary Efficacy Analysis
Lorundrostat
Across the three randomized trials, lorundrostat significantly reduced SBP compared with placebo (Figure 2). Using a random-effects model, the pooled mean difference in SBP was -7.51 mmHg (95% CI, -10.30 to -4.71; p = 0.007). The fixed-effects model produced a similar estimate of -7.51 mmHg (95% CI, -9.57 to -5.44; p < 0.001). There was no evidence of statistical heterogeneity among the included trials (τ2 = 0, I2 = 0). The Cochran Q test also suggested no significant heterogeneity (Q = 0.76, df = 2, p = 0.684). Efficacy forest plot of Lorundrostat. Forest plot showing the pooled mean difference in systolic blood pressure change between Lorundrostat and placebo across randomized controlled trials. Negative values indicate greater reductions in systolic blood pressure with Lorundrostat. Squares represent individual study estimates weighted by inverse variance, and horizontal lines represent 95% confidence intervals. The diamond represents the pooled effect estimate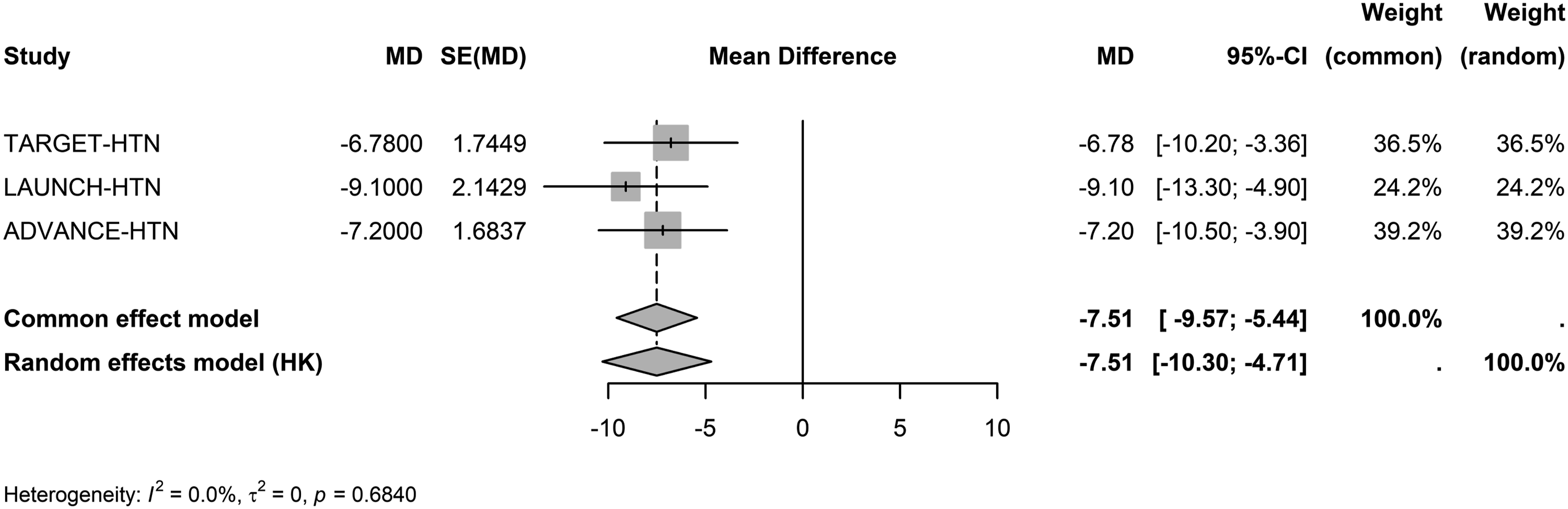
Baxdrostat
In the primary efficacy analysis, baxdrostat significantly reduced SBP compared with placebo (Figure 3). Using a random-effects model, the pooled mean difference in SBP was -8.63 mmHg (95% CI, -11.30 to -5.96; p = 0.005). No significant heterogeneity was observed across studies (τ2 = 0; I2 = 0%; Q = 1.17, df = 2, p = 0.558). Efficacy forest plot of Baxdrostat. Forest plot showing the pooled mean difference in systolic blood pressure change between Baxdrostat and placebo across randomized controlled trials. Negative values indicate greater reductions in systolic blood pressure with Baxdrostat. Squares represent individual study estimates weighted by inverse variance, and horizontal lines represent 95% confidence intervals. The diamond represents the pooled effect estimate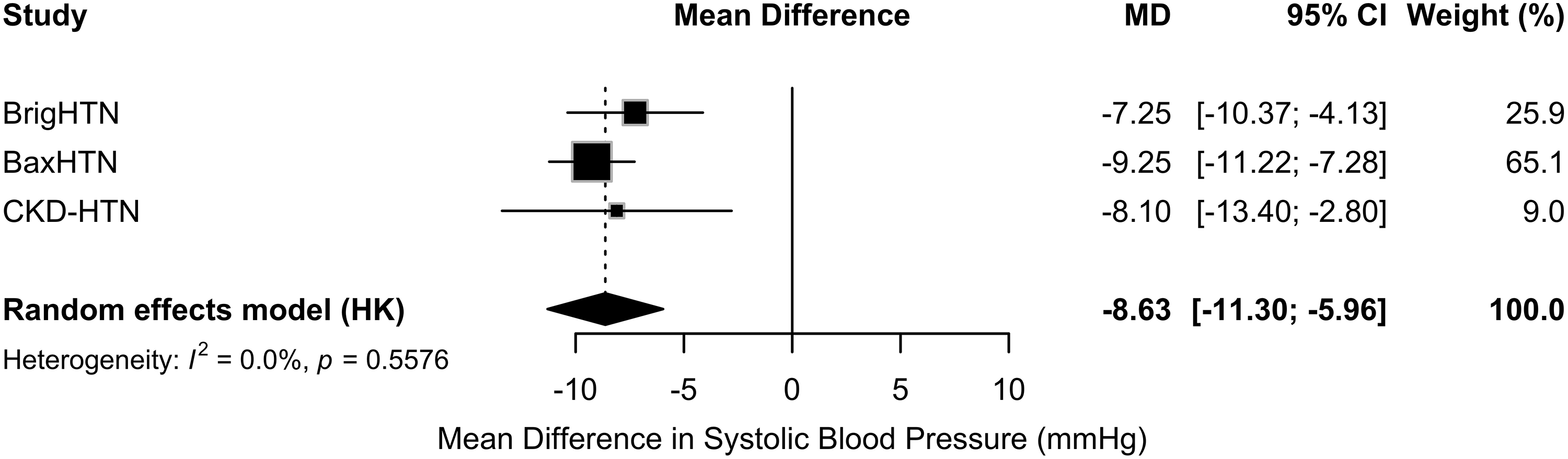
Safety Analysis
Lorundrostat
Hyperkalemia
Across the three trials, 49 hyperkalemia events were reported (Figure S1). The pooled analysis demonstrated a significantly increased risk of hyperkalemia with lorundrostat compared with placebo (RR 8.06; 95% CI, 2.92 to 22.27; p = 0.013). There was no evidence of statistical heterogeneity for this outcome (τ2 = 0, I2 = 0). The Cochran Q test was not statistically significant (Q = 0.22, df = 2, p = 0.898).
Treatment-Emergent Adverse Events
A total of 643 treatment-emergent adverse events (TEAEs) were reported among the included studies (Figure S2). Lorundrostat therapy was associated with a significantly higher risk of TEAEs compared with placebo (RR 1.45; 95% CI, 1.27 to 1.66; p = 0.007). No heterogeneity was detected across studies. The heterogeneity test was not statistically significant (Q = 0.41, df = 2, p = 0.814).
Serious Adverse Events
A total of 30 serious adverse events (SAEs) were reported across the three trials (Figure S3). The pooled analysis did not demonstrate a significant difference in SAEs between lorundrostat and placebo (RR 1.22; 95% CI, 0.10 to 14.69; p = 0.760). Moderate between-study heterogeneity was observed (τ2 = 0.73, I2 = 53.8%). However, the Cochran Q test did not reach statistical significance (Q = 4.33, df = 2, p = 0.115).
Baxdrostat
Hyperkalemia
Across the three trials, 70 hyperkalemia events were noted. Baxdrostat was associated with a significantly increased risk of hyperkalemia compared with placebo (RR 3.81; 95% CI, 1.82–7.97; p = 0.016) (Figure S4). No significant heterogeneity was observed among studies (τ2 = 0, I2 = 0%, Q = 0.45, df = 2, p = 0.797).
Treatment-Emergent Adverse Events
A total of 569 treatment-emergent adverse events were reported across the included trials (Figure S5). Baxdrostat was not associated with a significant increase in TEAEs compared with placebo (RR 1.17; 95% CI, 0.87–1.56; p = 0.150). There was no evidence of statistical heterogeneity (I2 = 0%, Q = 1.88, df = 2, p = 0.391).
Serious Adverse Events
A total of 33 serious adverse events were reported across the included studies (Figure S6). Baxdrostat was not associated with a significant increase in SAEs compared with placebo (RR 1.07; 95% CI, 0.73–1.58; p = 0.530). No significant between-study heterogeneity was observed (τ2 = 0, I2 = 0%, Q = 0.11, df=2, p = 0.945).
Descriptive Safety Findings
Prespecified adverse events of special interest and notable treatment-emergent adverse events reported in the included trials for both lorundrostat and baxdrostat are summarized in Supplemental Table S1. Frequently reported events included hyperkalemia, hyponatremia, reductions in kidney function, symptomatic hypotension, and adrenal steroidogenesis-related abnormalities. The pattern of reported adverse events was generally consistent across studies and aligned with the expected pharmacologic effects of aldosterone synthase inhibition.
A summary of safety outcomes is presented in Table S2.
Sensitivity Analysis
Lorundrostat
Office Blood Pressure Sensitivity Analysis
A sensitivity analysis restricted to trials measuring office SBP yielded similar results (Figure S7). Across the two trials reporting office blood pressure measurements, the pooled reduction in SBP was -7.71 mmHg (95% CI -22.14 to -6.73) using the random-effects model. No heterogeneity was detected (I2 = 0%, Q = 0.70, p = 0.401).
Highest-Dose Sensitivity Analysis
An analysis restricted to the highest lorundrostat exposure from each trial demonstrated a consistent treatment effect (Figure S8). The pooled reduction in SBP was -8.35 mmHg (95% CI -12.25 to -4.44) using the random-effects model. No heterogeneity was observed among these estimates. The heterogeneity test was not statistically significant (I2 = 0%, Q = 0.70, df = 2, p = 0.705).
Leave-One-Out Analysis
Sequential exclusion of individual trials demonstrated that the overall treatment effect remained consistent (Figure S9).
When the TARGET-HTN trial was excluded, the pooled SBP reduction was -7.93 mmHg (95% CI -19.65 to -3.80) using the random-effects model. After exclusion of the ADVANCE-HTN trial, the pooled estimate was -7.7 mmHg (95% CI -22.14 to -6.73). Exclusion of the LAUNCH-HTN trial resulted in a pooled estimate of -7.00 mmHg (95% CI -9.66 to -4.33).
Across all leave-one-out analyses, heterogeneity remained negligible (I2 = 0%), indicating that no individual study disproportionately influenced the pooled treatment effect.
Fixed-Effect Versus Random-Effects Model
Lorundrostat demonstrated a similar reduction in SBP relative to placebo in both models (Figure S10).
A summary of sensitivity outcomes for lorundrostat is presented in Table S3.
Baxrodrostat
In a sensitivity analysis incorporating BAX24, baxdrostat remained associated with a significant reduction in SBP compared with placebo, -9.75 mmHg (95% CI, -14.54 to -4.96; p = 0.008). However, inclusion of BAX24 resulted in substantial heterogeneity (I2 = 69.5%, Q = 9.85, df = 3, p = 0.020), suggesting that differences in blood pressure measurement methodology contributed to between-study variability.
Discussion
In this systematic review and meta-analysis of randomized controlled trials (RCTs), selective aldosterone synthase inhibitors (ASIs) were associated with meaningful reductions in systolic blood pressure (SBP) in patients with uncontrolled or resistant hypertension. Both lorundrostat and baxdrostat demonstrated significant placebo-adjusted reductions in SBP, with pooled treatment effects of similar magnitude across agents. Importantly, these benefits were observed despite differences in study populations, trial designs, follow-up durations, and blood pressure assessment methods, supporting the reproducibility of the antihypertensive effect of aldosterone synthase inhibition. Although treatment was associated with an increased risk of hyperkalemia, neither agent was associated with a significant increase in serious adverse events (SAEs).
Consistency of Treatment Effect
A notable finding of this analysis was the consistency of the antihypertensive effect observed across both ASIs. For lorundrostat, the reduction in SBP remained robust across multiple sensitivity analyses, including restriction to office blood pressure measurements, analyses of the highest-dose treatment arms, and sequential leave-one-out analyses, with no evidence of between-study heterogeneity.
Similarly, baxdrostat demonstrated a stable treatment effect across the primary efficacy studies reporting office SBP. Inclusion of BAX24, which evaluated 24-hour ambulatory SBP rather than office measurements, resulted in a larger pooled treatment effect but increased statistical heterogeneity. This finding suggests that differences in blood pressure assessment methodology contributed to between-study variability rather than reflecting inconsistency in the antihypertensive efficacy of baxdrostat.
Antihypertensive Efficacy of Aldosterone Synthase Inhibition
Aldosterone excess is a well-established contributor to the development and maintenance of hypertension, particularly in patients with resistant hypertension and those with heightened mineralocorticoid pathway activation. Beyond its effects on renal sodium retention and potassium excretion, aldosterone promotes vascular remodeling, endothelial dysfunction, inflammation, and arterial stiffness, all of which contribute to elevated blood pressure and increased cardiovascular risk. Consequently, suppression of aldosterone signaling has emerged as an important therapeutic target in difficult-to-control hypertension.
Historically, pharmacologic modulation of this pathway has relied on mineralocorticoid receptor antagonists (MRAs), particularly spironolactone, which remains an effective treatment for resistant hypertension. However, the use of MRAs may be limited by adverse effects such as gynecomastia, menstrual irregularities, hyperkalemia, and compensatory increases in circulating aldosterone concentrations.
Aldosterone synthase inhibitors (ASIs) represent a novel therapeutic approach that targets aldosterone biosynthesis through inhibition of CYP11B2, the enzyme responsible for the final steps of aldosterone production. By reducing aldosterone synthesis upstream of receptor activation, these agents may attenuate mineralocorticoid-mediated sodium retention and adverse vascular effects while potentially overcoming some limitations associated with receptor antagonism.
The findings of the present meta-analysis provide clinical evidence supporting this therapeutic strategy. The observed reduction in SBP was clinically meaningful and comparable to that achieved with several established antihypertensive therapies. Importantly, epidemiologic and meta-analytic data have demonstrated that even modest reductions in SBP are associated with substantial reductions in cardiovascular risk. A 5-mmHg reduction in SBP has been associated with approximately a 10% reduction in major cardiovascular events, whereas a 10-mmHg reduction has been associated with an approximately 20–30% reduction in stroke and other cardiovascular outcomes.7,8 Therefore, the magnitude of blood pressure reduction observed with lorundrostat and baxdrostat may have important implications for long-term cardiovascular risk reduction, although dedicated outcome trials will be required to confirm this hypothesis.
Comparison With Existing Literature
There have been no direct head-to-head randomized trials comparing selective ASIs with MRAs. Nevertheless, the magnitude of SBP reduction observed with both lorundrostat and baxdrostat falls within the range reported in studies of MRAs for resistant hypertension. In the PATHWAY-2 trial, spironolactone demonstrated superior blood pressure reduction compared with placebo and other add-on antihypertensive therapies, underscoring the central role of aldosterone-mediated mechanisms in resistant hypertension. 32 However, because no head-to-head randomized trials have compared ASIs with MRAs, these observations should be interpreted cautiously and should not be considered evidence of comparative efficacy. Despite their established efficacy, MRAs may be limited by adverse effects, including gynecomastia, menstrual irregularities, hyperkalemia, worsening renal function, and compensatory increases in circulating aldosterone concentrations.
Earlier ASIs provided important proof-of-concept for this therapeutic strategy. 37 LCI699 (osilodrostat), a first-generation ASI, demonstrated effective aldosterone suppression and blood pressure reduction in early hypertension and primary aldosteronism studies. Subsequent phase III trials in Cushing disease confirmed its clinical efficacy and demonstrated improvements in blood pressure and cardiometabolic parameters.38,39 However, because osilodrostat also inhibits CYP11B1 (11β-hydroxylase), clinically significant suppression of cortisol synthesis may occur, limiting its suitability as a chronic antihypertensive therapy. 39 The development of highly selective CYP11B2 inhibitors, including lorundrostat and baxdrostat, has therefore represented a major advance in the field by enabling targeted suppression of aldosterone while minimizing off-target effects on cortisol production.
Collectively, these findings support selective aldosterone synthase inhibition as an effective therapeutic strategy for uncontrolled and resistant hypertension and suggest that the antihypertensive benefits of aldosterone synthase inhibition may extend across multiple agents within the class.
Safety Considerations
Despite the favorable antihypertensive efficacy observed in this analysis, safety considerations remain important. Across both the lorundrostat and baxdrostat trials, aldosterone synthase inhibition was associated with an increased risk of hyperkalemia compared with placebo. This finding is biologically plausible and consistent with the pharmacologic consequences of aldosterone suppression, which reduces renal potassium excretion and may increase susceptibility to hyperkalemia, particularly in patients with impaired kidney function or concomitant use of renin-angiotensin-aldosterone system (RAAS) inhibitors.19-28 Differences in hyperkalemia rates across trials should be interpreted cautiously because of variations in study populations, baseline kidney function, and event definitions.
Importantly, the increased incidence of hyperkalemia was not accompanied by a significant increase in SAEs for either agent. Across the included trials, hyperkalemia events were generally identified through protocol-mandated laboratory monitoring and managed with dose modification, temporary interruption, or treatment discontinuation when necessary. In addition, adverse events of special interest included hyponatremia, reductions in kidney function, symptomatic hypotension, and laboratory abnormalities related to adrenal steroidogenesis, all of which are mechanistically linked to aldosterone synthase inhibition.
Treatment-emergent adverse events (TEAEs) were significantly more frequent with lorundrostat, whereas baxdrostat was not associated with a statistically significant increase in overall adverse events. Nevertheless, most reported adverse events were mild to moderate in severity, and neither agent demonstrated an excess risk of serious adverse events. Collectively, these findings suggest that selective aldosterone synthase inhibition has an acceptable safety profile when accompanied by appropriate patient selection, laboratory surveillance, and dose adjustment strategies. However, the relatively short duration of follow-up in available studies warrants continued evaluation of long-term safety.
Limitations
Several limitations should be considered when interpreting the findings of this study. First, the number of available randomized trials remains limited, particularly for lorundrostat, restricting the precision of pooled estimates and limiting the ability to explore potential sources of heterogeneity. Second, follow-up durations were relatively short, ranging from 6 to 26 weeks in most studies, precluding assessment of long-term cardiovascular outcomes, renal outcomes, and sustained safety.
Third, differences existed among studies with respect to patient populations, baseline cardiovascular and renal risk, blood pressure measurement methods, and dosing strategies.
Fourth, the CKD-HTN trial was not included in pooled baxdrostat safety analyses because of substantial differences in baseline kidney function and hyperkalemia risk compared with the other study populations. Consequently, the pooled safety estimates may not fully reflect the safety profile of aldosterone synthase inhibition in patients with moderate-to-severe chronic kidney disease.
Fifth, no direct comparisons between lorundrostat and baxdrostat were available, and the present study was not designed to compare the relative efficacy or safety of individual agents. Finally, because fewer than ten studies were available for most analyses, formal assessment of publication bias was not performed. Despite these limitations, the consistency of treatment effects across studies and sensitivity analyses strengthens confidence in the overall findings.
Future Directions
Future research should focus on larger randomized trials with longer follow-up to determine whether the blood pressure reductions observed with ASIs translate into improvements in cardiovascular and renal outcomes. Additional studies are needed to identify patient populations most likely to benefit from this therapeutic strategy, including individuals with primary aldosteronism, obesity-associated hypertension, and other conditions characterized by heightened mineralocorticoid pathway activation.
Further investigation is warranted to define optimal dosing strategies and to better characterize the long-term safety profile of selective ASIs. Whether blood pressure reductions achieved with aldosterone synthase inhibition translate into reductions in cardiovascular events, heart failure, kidney disease progression, and mortality remains unknown and represents a critical area for future investigation. Finally, direct comparative studies evaluating ASIs against established therapies, particularly MRAs, would help clarify their relative efficacy, safety, cost-effectiveness, and positioning within future hypertension treatment algorithms.
Conclusions and Clinical Implications
In this systematic review and meta-analysis of randomized controlled trials, selective aldosterone synthase inhibition with lorundrostat and baxdrostat was associated with clinically meaningful reductions in systolic blood pressure among patients with uncontrolled or resistant hypertension. Although treatment increased the risk of hyperkalemia, neither agent was associated with a significant increase in serious adverse events. These findings support aldosterone synthase inhibition as a promising therapeutic strategy for difficult-to-control hypertension and provide evidence that the antihypertensive benefits of aldosterone synthase inhibition may extend across multiple agents within this therapeutic class. Nevertheless, the current evidence base remains limited by the relatively small number of available trials and short follow-up durations, highlighting the need for larger studies evaluating long-term safety, cardiovascular outcomes, and comparative effectiveness.
Supplemental Material
Supplemental material - Targeting Aldosterone Biosynthesis in Uncontrolled and Resistant Hypertension: A Systematic Review and Meta-analysis of Randomized Trials of Lorundrostat and Baxdrostat
Supplemental material for Targeting Aldosterone Biosynthesis in Uncontrolled and Resistant Hypertension: A Systematic Review and Meta-analysis of Randomized Trials of Lorundrostat and Baxdrostat by Ravi Pandey, Muhammad Ahmad, Ali Rohan, Iqra Nurie, Shano Sherani, Aliya Noor, Mahnoor Baloch, Amal Usmani, Muhammad Shahid, Muhammad Saffi Ullah, Muhammad Zaheer and Aimen Shafiq in Journal of Cardiovascular Pharmacology and Therapeutics.
Footnotes
Acknowledgements
AI-assisted language editing was used to improve clarity and readability.
Ethical Considerations
This study used publicly available, de-identified data and did not require Institutional Review Board approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.