
Abstract
Social determinants of health are acknowledged as the structural conditions (social and environmental forces) that influence the health outcomes of individuals and populations as they develop, live, and work within particular cultures. Social determinants are shaped by political systems, resources, and value systems. For instance, the United States spends far more money per capita on medical services than do other nations, while spending less on social services (Bradley, Elkins, Herrin, & Elbel, 2011); however, residents of nations that have higher ratios of spending on social services to spending on health care services have better health and live longer (Bradley & Taylor, 2013; Wolff & Aron, 2013). Thus, the culture and values of the political system in the United States becomes an important determinant of health outcomes. In addition, unequal distribution of money, power, and resources on global, national, and local levels produce health inequities or avoidable differences in health status seen within and among countries (Solar & Irwin, 2010; World Health Organization, 2017) and are now widely thought to be as important or more important determinants than biological mechanisms for preventing and treating disease.
The primary goal of recognizing social determinants of health is to improve the health status of individuals and populations through use in public health planning, implementation, and evaluation. For instance, in the United States, Healthy People 2020 includes both individual-level and population-level domains to describe the determinants of health and interventions (U.S. Department of Health and Human Services, The Secretary’s Advisory Committee on National Health Promotion and Disease Prevention Objectives for 2020, 2008). In addition, the importance of social determinants of health is emphasized by aligning the health professional education and research to that which supports and empowers communities, the health workforce, educators, and researchers. The rationale is that community stakeholders (persons or groups that have a vested interest in an issue) can best identify their needs, communicate those needs to trainees in service-based learning and to researchers in community-based research projects, design solutions that can work, and be part of the evaluation process.
While social determinants of health have received transdisciplinary attention, the role of the family has not been emphasized (McNeill, 2010). That is, family is included in the social, family, and community networks domain of multilevel, ecological models depicting social determinants of health and mentioned in terms of the importance of family support, the risk of accumulated risk (e.g., family conflict), and the resource of education completed by the family of origin. These ideas, however, are not developed. Moreover, while social, family, and community networks are often an understood value to interventions to enhance health, the family is not typically theoretically justified and identified as central to social determinants of health. Furthermore, in the United States, no family variables are included in leading health indicators measuring the outcomes of Health People 2020. While the lack of emphasis and acknowledgment of families can be typical of how family is conflated with other social groups, the absence of family is most perplexing given this topic. At any rate, this gap in the literature prompted me to ask myself the following questions: How families impact and are impacted by these social determinants? What are the implications for family nursing practice, research, education, and policy/leadership of the social determinants of health?
While these questions are difficult to answer at this time, I would like to explore how these questions can be used to frame opportunities for family nursing practice, research, education, and policy/leadership moving forward. I arrive at these questions and search for answers after 47 years in nursing practice, after two decades of membership in collaborative group of nurse scientists who focused on health disparities and health equity, and after three decades studying how families integrate the care of children with chronic conditions and the care of children who survived cancer into family life.
Why Focus on Social Determinants of Health?
Issues identified by the social determinants of health were not typically viewed as “health policies” but are now globally recognized and supported as having the potential to improve the health and longevity and reduce health disparities of individuals and populations. In fact, the best available evidence suggests that these health multilevel frameworks describing the social and behavioral determinants of health would achieve better population health, less inequality, and lower costs than traditional frameworks addressing either population or individual health (Adler et al., 2016).
An ecological perspective is typically used in the United States and elsewhere to acknowledge these multilevel factors that contribute to our collective health and illness. For example, Figure 1 shows the Action Model to Achieve Healthy People 2020 Overarching Goals. Health determinants are the range of factors that influence the health status of individuals or populations: individual; social, family, and community networks; living and working conditions; and broad social, economic, cultural, and environmental conditions and policies at the global, national, state, and local levels. Multilevel interventions to improve social determinants can come in the form of policies, programs, and information to improve outcomes including those that may be concerned with behavior, risk, injury, well-being and quality of life; and health equity. Finally, the process of assessment, monitoring, evaluation, and dissemination is monitored by selected leading health indicators (U.S. Department of Health and Human Services, The Secretary’s Advisory Committee on National Health Promotion and Disease Prevention Objectives For 2020, 2008).
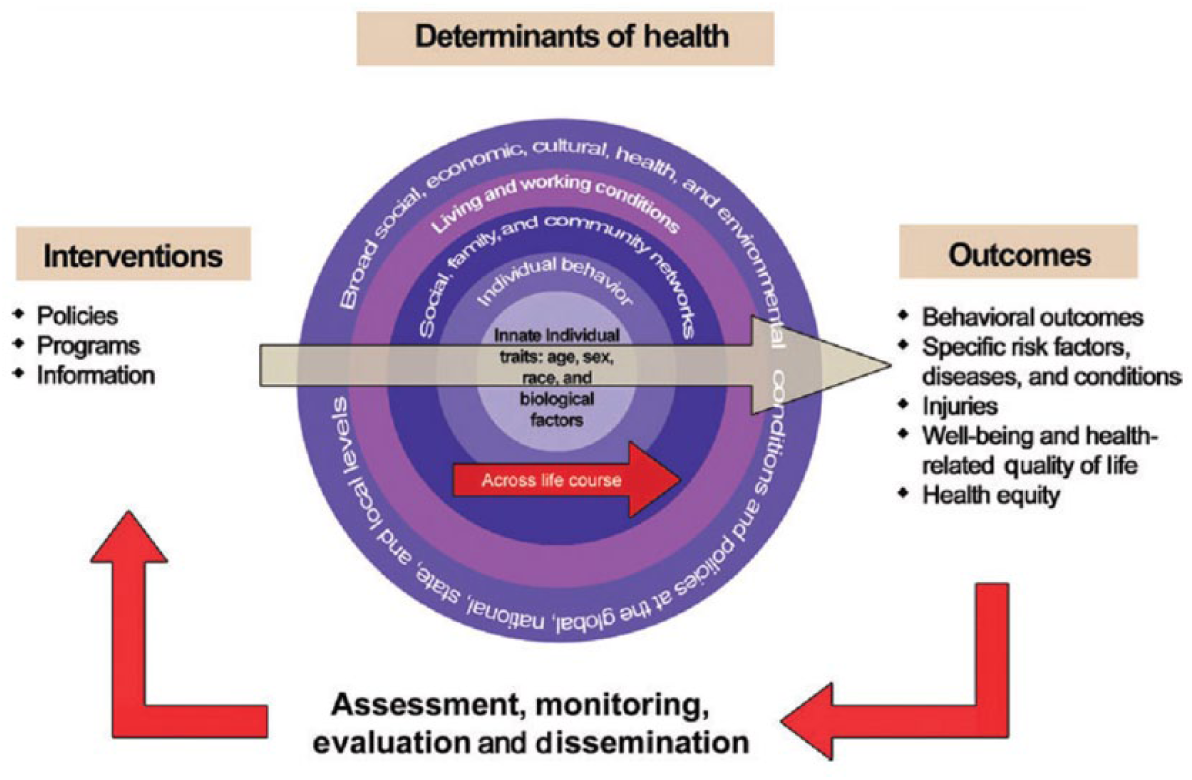
Action Model to Achieve Healthy People 2020 Overarching Goals.
While Healthy People uses an ecological perspective, the World Health Organization model uses a mechanistic conceptualization of social determinants of health to guide policy and practice. Social, economic, and political structural determinants of health stratify populations according to income, education, occupation, gender, race/ethnicity, and other factors which in turn shape intermediary determinants of health. Intersectoral policy approaches (those outside health care which may or may not be in collaboration with health care) are advocated to produce sustainable outcomes including addressing “upstream” social determinants of health such as the individual and collective contributions of education, labor, criminal justice, transportation, economics, and social welfare; fostering health-promoting resources and reducing health-damaging risk factors throughout the life; and improving access to, effects of, and the value of clinical health care services to health disparities (Solar & Irwin, 2010; U.S. Department of Health and Human Services, The Secretary’s Advisory Committee on National Health Promotion and Disease Prevention Objectives for 2020 (2008); World Health Organization, 2017).
Social determinants of health raise questions of social justice for nurses who are engaged with families. As practitioners, teachers, and researchers engage in activities with and for others, health can no longer be viewed as a transaction; that is, one does not “give” health care to another individual or family. Rather, multiple influences that may be at the root of health problems must become part of the process to improve outcomes and decrease structurally determined health inequities (described by the absence of unfair and avoidable or remediable differences in health among social groups; de Chesnay & Anderson, 2016; Kirkham & Browne, 2006; Perry, Willis, Peterson, & Grace, 2017). I was reminded of this recently when I was scanning the statistical analysis completed by a student. While the African American mothers in the sample were largely educated, some 40% of them lived in poverty according to U.S. standards. I was reminded that statistics about their income no longer should be used not only to merely describe the sample but also to help us understand income and other multilevel factors that influence their lived experiences and their health outcomes.
How Families Impact and Are Impacted by Social Determinants of Health?
Social determinants of health include culture, social norms, social policies, and political systems that directly impact the health of families and to some extent are influenced by families. As families fulfill their functions to socialize and protect their members, they incorporate and interpret the larger sociocultural and political worlds for their members. Therefore, issues that affect any part of the ecological worlds of individuals can affect the health of families by potentially providing protection or increasing risk.
While families can be key to modifying risk for their members, they can easily fall prey to changing social policies and political systems, especially families who are potentially vulnerable. An urgent need exists to consider how the social determinants of health influence are influenced by families. For instance, in the United States, parents are most likely to report lack of partnerships with health care providers if their children have functional limitations, are from ethnic or racial minorities, have low incomes, do not have health insurance, and have limited English language skills. The consequences for families without perceived partnerships with health care providers are poorer outcomes (more missed school days, harder to obtain referrals for services, and unmet child and family needs) and less satisfaction with care (Kenney, Denboba, Strickland, & Newacheck, 2011; Smalley, Kenney, Denboba, & Strickland, 2014).
What Are the Implications for Family Nursing Practice, Research, Education, and Policy/Leadership of the Social Determinants of Health?
We know that the health of families is integral to the health of its members, our communities, and societies. Families are, however, largely absent from the policies and practices related to the social determinants of health. Families and family science is neither systematically included nor measurable within the present framework but much potential exists for contributions by family nursing practice, research, education, and policy/leadership.
Family Nursing Practice
How we address social justice and inequities is the responsibility of nursing practice, and the nature of our response will shape our profession into the future. While applicable to general nursing practice, the message is especially relevant to family nursing practice. One of the first steps toward meeting this responsibility is to examine the relational, contextual, and intersectional issues regarding family and social justice including other postcolonial feminist social signifiers that influence social relations, including class, gender, religion, sexual orientation or disability, social inequities, and health disparities, and address them as part of clinical care (Kirkham & Browne, 2006; Perry et al., 2017). In addition, as pointed out in a recent book about equality by Waldron (2017), we can easily become inured to differences represented by these social signifiers like poverty. He explains that the poor may seem so different to us that we become accustomed to their differences while agreeing that such differences are unjustified (Waldron, 2017). As nurses, we are most likely “guilty” of this kind of thinking because of our exposure to wide inequalities of income. Such exposure can reinforce perceived differences and erode our ability to remember that we are not different from our patients or from any other humans. We are their equals and that their lived experiences of feeling different are not abstractions; they are the lived experiences of poverty, hunger, homelessness, stigma, and racism in a land of privilege and plenty.
Second, in family nursing practice, we need to contribute to the professional and lay literatures about social determinants of health and take credit for our relevant practice innovations. When we frame clinical practice innovations by building on existing social determinants language or frameworks, we will also contribute to the family sciences. We have not included the language of social determinants in our writing and have not been recognized as building that science.
Third, we can build family nursing practice, this consistent with the International Family Nursing Association’s (IFNA, 2015, 2017) Position Statements on Generalist and on Advanced Practice Competences for Family Nursing Practice. IFNA’s practice competences complement the literature regarding practice implications of social determinants of health by examining how family needs to be acknowledged and included in practice, as well as how to engage and intervene with families. The following issues are included: diverse individual and family needs in all care settings and communities, cultural heritage of the family, and families’ capacity for transforming the quality of life and family health. Emphasis is also placed on the nurse, including our moral obligation to support family and societal health, leadership/systems skills, self-reflective practice, and ability to collaborate and lead.
Family Nursing Research
Carefully considered paradigms and approaches will enhance and enable strategic advances in family science (Knafl, 2015). Probably most basic to family research is acknowledging that structural and intermediary determinants are more than demographic variables. Such issues need to be addressed and acknowledged in theoretically relevant ways to meaningfully discern those issues that are of importance to any given population of families (Barakat, 2012).
Consideration should be given to the state of knowledge in the family sciences and family nursing and match it to the approach that may be relevant to social determinants. First-generation research involves identifying and describing in qualitative and quantitative terms any disparities in health or health care between recognized and emerging vulnerable populations and their counterparts who may not be as vulnerable. Second-generation research involves identifying and understanding the multifactorial determinants of these disparities. Third-generation research involves designing and testing targeted interventions, evaluating the implementation process and outcomes, and translating successful interventions into widespread clinical practice. Use of community-based participatory research and elicitation research strategies must be routinely used throughout this process to match local need and conditions with interventions and strategies. As such, research teams need to include experts in these methods to insure rigor and fidelity to the methods (Ibrahim, Egede, Uchendu, & Fine, 2014). Fourth-generation research relative to social determinants is grounded in public health critical race praxis and uses comprehensive interventions to address race, racism, and structural inequalities and advancing evaluation methods to foster our ability to eliminate disparities (Thomas, Quinn, Butler, Fryer, & Garza, 2011).
Finally, the mechanisms underlying the effects of social determinants on health are yet to be understood and difficult to research; however, plausible hypotheses need to be advanced and debated. For instance, Braveman and Gottlieb (2014) advanced three pathways through which education can effect health which can be applied to family health, including health knowledge, literacy coping, and problem solving; work/employment; and control beliefs, social standing, and social networks. Such discussions can be based on our knowledge of working with other disciplines and our theoretical diversity and may enable family nursing to provide leadership to the field (Braveman & Gottlieb, 2014).
Family Nursing Education
While community and family experiences were plentiful in my undergraduate and graduate nursing education, such experiences have typically dwindled within current curriculums. While the reasons for these trends are many, calls now exist for remedying the situation within the framework of social determinants of health. We now understand that these experiences are important not only because students will experience and enact health care in different places, but they also experience and enact care related to structural and intermediary determinants of health inequities in different places. Most notably, the National Academy of Sciences made recommendations based on a model of strengthening health professions education in social determinants of health. The goal of the model is to educate a workforce that partners with the community to address social determinants of health, build a diverse workforce, and encourage continuing professional education. Effective teaching/learning strategies were endorsed including explicit recognition of social determinants of health in the curriculum, community-engaged learning/immersion experiences, community-oriented education, and problem-based learning (National Academies of Sciences, Engineering, and Medicine, 2016). The National Academy’s recommendations are consistent with the IFNA’s (2013) Position Statement on Pre-Licensure Family Nursing Education. IFNA’s position statement provides specific guidelines for family-based educational experiences including emphasis on diversity; links between individual, family, community, and all care/health systems; coordinated care; and the critical reflection of the nurse (IFNA, 2013).
Critical to these teaching and learning strategies is the idea that community-engaged learning/collaboration is between equal partners. For family nursing education, typically this means that the student is learning from the family and the family is learning from the student. One is not subordinate to the other. Problem-based learning is stressed to emphasize the systematic nature of approaches to families within the community context. Interprofessional learning is a necessity to model parallel processes among the student, family, and members of other disciplines. A focus on advocacy that acknowledges areas of social determinants of health is strategic to how we can engage families in that we must meet them where we have access to them; for example, this may mean social services through health care or child care through child health. Finally students on all levels of education need to be engaged in looking at outcomes of family nursing practice using the rubric of social determinants. Without knowledge of such outcomes, we are not ultimately visible to others, including the families (National Academies of Sciences, Engineering, and Medicine, 2016).
Family Nursing Policy/Leadership
Family nurses can take an active role in policy and leadership not only in health care but in social policy that covers the gamut of human concerns (Grady & Hinshaw, 2017). In doing so, we can become more effective in health care leadership because we better understand the health system and how external economic, financial, and policy forces can impact the home, family, and community in which a patient resides.
Understanding of both formal structures and informal social systems is important. Formal systems are often the arbiters of resources, while informal systems are formed among families, neighborhoods, and populations that share unique characteristics. While formal systems are integral to family safety nets, the informal support systems hold potential solutions to meeting many needs of community members (McNeill, 2010).
Family nurses’ knowledge and advocacy for policies and programs is also needed to support families because such programs have a profound influence on families by moderating social determinants of health. Policies include those related to employment (e.g., equal wages for women and minorities; minimum wage; concern for the working poor), child education and support programs (e.g., day care, early intervention, day long kindergarten, services to children with special health care needs), social safety net (e.g., monetary assistance, nutrition/food support, transportation), caregiver support across the life cycle, and wrap around services (Grady & Hinshaw, 2017; McNeill, 2010).
Conclusion
We now understand that social determinants of health can be more important determinants than biological mechanisms for preventing and treating disease. As family nurses, we understand the importance of families for the health of their members. Now is the time for family nursing to provide leadership to the integration of family science into practice, research, education, and policy/leadership related to social determinants of health.