
Abstract
Traumatic brain injury (TBI) is a family affair, affecting those with the injury and their families. Psychological distress, often measured as depression or depressive symptoms, is highly prevalent among family members. Predictors of depression in family members of civilians with TBI have been examined, but predictors of depression in family members of military veterans have received very little research attention and are poorly understood. To address the knowledge gap, this study explored factors related to depressive symptoms in family members of veterans in the United States, using an ecological framework. Baseline data from 83 family members were used. Family members with higher caregiver burden, presence of a veteran with posttraumatic stress disorder (PTSD), and greater financial difficulty experienced significantly more depressive symptoms. Findings suggest that efforts to support family members and decrease their depression should aim to reduce caregiver burden and financial difficulty, and help family members cope with veteran PTSD and TBI. Family-focused interventions are needed.
With growing recognition of the prevalence and impact of traumatic brain injury (TBI) in civilian and military populations, TBI has gained national prominence as a major public health problem in both populations (Centers for Disease Control [CDC], 2016; CDC, National Institutes of Health [NIH], Department of Defense [DOD], & Department of Veterans Affairs Leadership Panel, 2013). About 5.3 million persons in the United States are living with disability from TBI (Brain Trauma Foundation, 2018). About 20% of service members deployed in support of the Iraq and Afghanistan wars have experienced a TBI (Tanielian, Jaycox, Schell, et al., 2008), and TBIs in earlier war cohorts have recently been identified as a result of increased awareness and evaluation within the U.S. Veterans Affairs (VA) health system. The CDC (2016) define TBI as an injury caused by “a bump, blow or jolt to the head or a penetrating head injury that disrupts the normal function of the brain” (“What is a TBI,” para. 1). Many physical, cognitive, and behavioral symptoms are associated with TBI (Arciniegas, Held, & Wagner, 2002; Kim et al., 2007; Sayer et al., 2008; Schneiderman, Braver, & Kang, 2008) that also challenge veterans’ reintegration into the family and community upon return from deployment (Daggett, Bakas, Buelow, Habermann, & Murray, 2013; Lequerica et al., 2012; McCabe et al., 2007).
TBI is a family affair. TBI symptoms, whether subtle or more overt, may have a profound impact on the lives of individuals and their families. Research centered on family impact and needs is critical because families provide support necessary for successful rehabilitation of the person with TBI, and they also need support to manage the stress of caregiving (Kreutzer, Marwitz, Sima, & Godwin, 2015; Stejskal, 2012).
In the context of families living with a member with TBI, Bronfenbrenner’s (1979) ecological model is particularly useful for its focus on factors both within and outside the individual. This theoretical model emphasizes the individual’s interactions with the family and community and the interrelationships among all these systems. The model posits characteristics of the family member, the individual patient, and his or her injury, and community support as factors likely to contribute to individual well-being. Based on these propositions, the model was used to examine the contribution of multiple factors (individual, family, community) to family member depressive symptoms.
Overview of Research on Impact of TBI on Family Members
Considerable research has documented negative sequelae that family members of civilians with TBI often experience: significant levels of depression, stress, and anxiety (Kreutzer, Garvasio, & Complair, 1994; Kreutzer et al., 2009; Nabors, Seacat, & Rosenthal, 2002; Ponsford, Olver, Ponsford, & Nelms, 2003; Riley, 2007); caregiver burden (Knight, Devereux, & Godfrey, 1998; Kreutzer, Serio & Berquist, 1994; Malec, Van Houtven, Tanielian, Atizado, & Dorn, 2017; Marsh, Kersel, Havill, & Sleigh, 1998); social isolation (Marsh et al., 1998; Marsh, Kersel, Havill, & Sleigh, 2002); decreased quality of life (Verhaeghe, Defloor, & Grypdonck, 2005); financial difficulties (Riley, 2007); and worse perceived health (McPherson, Pentland, & McNaughton, 2000). Depression is one of the two most common psychosocial problems reported by civilian family caregivers of persons with TBI (Stevens et al., 2012). However, depression has been understudied in family members of veterans with TBI, and thus it is the outcome of interest in this article. Caregiver burden, the other most common problem, is considered a potential predictor of depressive symptoms in family members in this article, based on previous research supporting this relationship (Griffin et al., 2017; Machamer, Temkin, & Dikmen, 2002).
Correlates of Depression in Family Members
Previous research has examined potential correlates of family members’ depression (such as sociodemographics, type of family relationship, social support, and burden) in family members of civilians with primarily moderate to severe TBI. Findings with respect to these associations have been mixed. For example, some studies have shown that higher depression is associated with lower socioeconomic status (SES; Riley, 2007), African American race (Hart et al., 2007), spousal relationship (rather than other family relationship; Kreutzer, Garvasio, & Complair, 1994), lower social support (Calvete & de Arroyabe, 2012; Riley, 2007), and higher burden (Machamer et al., 2002). Other studies have shown no associations with family member SES (Harris, Godfrey, Partridge, & Knight, 2001), race (Sander et al., 2007), type of family relationship (Ennis, Rosenbloom, Canzian, & Topolovec-Vranic, 2013; Kreutzer et al., 2009), social support (Leach, Frank, Bouman, & Farmer, 1994), or burden (Rivera, Elliott, Berry, Grant, & Oswald, 2007). Inconsistency in findings has been attributed to differences in methods and measures (Blais & Boisvert, 2005).
In contrast to civilian TBI, a dearth of research has addressed correlates of depression in family members of veterans with TBI. In a study of 70 family caregivers of pre-9/11 U.S. veterans who had earlier received inpatient TBI rehabilitation (Phelan et al., 2011), caregivers who perceived more discrimination or stigma from caregiving reported greater depressive symptoms, after controlling for other characteristics. The other characteristics included caregiver demographics, type of relationship, social support, and other variables, but data on these relationships were not reported. A more recent study (Griffin et al., 2017) surveyed 564 family members (62% parents, 32% spouses) caring for post-9/11 veterans who had polytrauma, including TBI, and who had been discharged at least 3 months earlier from one of the four VA inpatient Polytrauma Rehabilitation Centers in the United States. Seventy percent of the veterans suffered moderate to severe TBI, the remainder mild TBI. Through structural equation modeling, the findings indicated that more caregiver burden was directly associated with poor mental health, conceptualized as depression and anxiety and measured by the PROMIS scales (Griffin et al., 2017).
Depression in family members of veterans with TBI deserves more attention in light of extensive evidence with other populations documenting the adverse effects of depression on everyday functioning, quality of life, work, and relationships (e.g., Lerner & Henke, 2008; Steger & Kashdan, 2009). Identification of factors contributing to depression in family members is essential to enable early assessment of those at highest risk and referral for treatment. Nurses interacting with these family members in varied VA and community settings are well positioned for these roles.
In summary, most previous research on depression in family members of persons with TBI has focused on civilian TBI, not military TBI. Findings from civilian families may not generalize to families of veterans with TBI. The present study aims to extend earlier work with civilians to family members of veterans with the goal to ultimately improve family-focused care for this population. Veteran families may be more vulnerable than civilian families because they have experienced stress from multiple and extended deployments prior to the veteran’s return home (Dausch & Saliman, 2009; Stevens et al., 2017). Furthermore, veterans with TBI often have other comorbidities, such as posttraumatic stress disorder (PTSD), other anxiety disorders, depression, pain, and polytrauma that heighten family vulnerability (Hoge et al., 2008; Nampiaparampil, 2008; Tanielian, Jaycox, Adamson, & Metscher, 2008). Given that a large proportion of veterans with TBI have a diagnosis of PTSD (about 73%) or depression (about 47%; Taylor et al., 2012), these comorbidities must be considered as individual veteran factors of interest in the present study.
To address the gap in knowledge around TBI in military families in the United States, the present study sought to identify factors posited by the ecological model as likely to be related to depressive symptoms in family members of military veterans with TBI, the majority of whom have suffered a mild TBI. Understanding these factors can inform interventions and policies to support family members, and help tailor some existing interventions to the needs of specific families.
Study Aim
Using baseline data from a parent study (Moriarty, Winter, Robinson, Piersol, et al., 2015; Winter et al., 2016), the aim of this secondary analysis was to explore individual, family, and community factors related to depressive symptoms in family members of veterans with TBI. Selection of potential correlates was guided by Bronfenbrenner’s (1979) ecological model. Individual factors under consideration included the family member’s sociodemographic characteristics (age, gender, race, Hispanic ethnicity, financial difficulty) and the veteran’s psychiatric comorbidities (PTSD diagnosis and depressive symptoms). Family factors included type of family relationship (spouse vs. nonspouse) and caregiver burden. A community factor examined was social support experienced by the family member.
Method
Design
Data reported here were collected as part of a larger randomized controlled trial that evaluated the efficacy and acceptability of the Veterans’ In-home Program for veterans and their families (Moriarty, Winter, Robinson, Piersol, et al., 2015; Winter et al., 2016). The program consisted of an in-home intervention delivered by licensed occupational therapists.
This analysis is based on a cross-sectional design. Data reported in this article were collected at baseline from veterans and family members and occurred before randomization into the intervention or control groups.
Sample
Veterans were recruited from the Corporal Michael J. Crescenz Veterans Affairs Medical Center (CMC VAMC, USA) outpatient Polytrauma Program in the Rehabilitation Medicine Service, which conducts TBI evaluations for veterans after an initial positive TBI screen. Veterans from the post-911 period are automatically screened for TBI within the VA health system. Veterans from earlier war cohorts are not routinely screened but can be referred to the polytrauma program for TBI evaluation through other providers. All veterans in our sample, even those pre-911, had recently received a TBI evaluation and TBI diagnosis through the Polytrauma Program. All had a history of TBI events and had TBI-related symptoms at the time of the evaluation.
Study participants were 83 veterans with TBI and for each, a family member chosen by the veteran. The sample size for the parent randomized controlled trial was originally determined by powering for a medium-to-large effect size (0.25 to 0.4) and anticipating a possible attrition rate of 20%. Eligible veterans received a letter of invitation introducing the study. Letters were followed by a phone call that described the study further and determined the veteran’s willingness and eligibility for the study. Inclusion criteria included residence in the Philadelphia metropolitan region, diagnosis of TBI at the polytrauma program, postdeployment from the Vietnam War era to the present, ability to speak English, meeting VA Polytrauma Systems of Care criteria for TBI, and having a family member or partner living with him or her or living within close proximity (within 30 minutes travel time) willing to participate in the study. The family member was identified by the veteran as actively involved in his or her life. Although an exclusion criterion was recent violent behavior, as assessed by the clinical team, there were no veterans excluded from the study for this reason.
Letters of invitation were sent to 196 veterans, and telephone screens conducted with 110 veterans. Of these, 86 were enrolled, and 24 were not enrolled due to varied reasons: refused participation (7), had no family member (8), or could not schedule the baseline interview (9). Three of the 86 were not randomized because their TBI diagnosis had changed and other conditions explained their symptoms; thus the sample for the baseline data used in this article was 83. More details about recruitment and the CONSORT chart are reported elsewhere (Moriarty, Winter, Robinson, Piersol, et al., 2015; Winter et al., 2016).
Procedure
The institutional review board of the CMC VAMC approved this study. Study participants provided written informed consent before the baseline interview began. Family members and veterans were interviewed in their home on the same day. To maintain independent responses, the interviews were conducted separately, out of the hearing of the other. The data (for the standardized questionnaires) were collected via interviews. The interviewer read the questionnaire items aloud, and respondents could also read the questions on paper if they wished, whatever the participant preferred. The interviewer used response cards that presented each question’s response format on a card, and study participants could point to the response on the card or verbally give their response. The total number of questions answered by family members was 107. Most family members completed the interview in about 35 min. The interviewers were alert to signs of response burden and offered breaks during data collection, but response burden was not evident.
Most baseline interviews were conducted by a masters-prepared social worker with extensive experience in conducting in-home interviews; some baseline interviews were also conducted by the principal investigators. The social worker underwent 6 hours of initial training around TBI and PTSD, the interview procedures, administration of the instruments, human subjects’ protections, and data security. Additional oversight was provided via team meetings and phone calls on a regular basis throughout the study.
Measures
At the baseline interview with veterans and family members in the parent study, we collected data with multiple measures. In this article, we report specifically on select baseline data for the individual, family, and community factors tested as predictors of family member depressive symptoms.
Measures for individual factors for the family member and veteran
Family member sociodemographic characteristics
Family member’s age, gender, race, ethnicity, and financial difficulty were selected as individual sociodemographic factors in the regression model and were measured through self-report with a demographic questionnaire. Family members and veterans also provided data on other sociodemographics that were used to characterize the sample.
A common method to assess subjective financial difficulty is through the measurement of one’s perceived income inadequacy to meet basic needs (Chan, Ofstedal, & Hermalin, 2002). Reflecting this method, financial difficulty in our study was measured by one item: “How difficult is it to pay for basics like food, housing and medical care?” that was answered on a 4-point scale (0 = not at all, 1 = not very, 2 = somewhat, 3 = very). This one-item question was used to measure perceived income inadequacy in Sun’s (2009) report from the Resources for Enhancing Alzheimer’s Caregiver Health I (REACH I) study. Perceived income inadequacy and not household income predicted more self-reported depressive symptoms and anxiety symptoms in family caregivers of persons with Alzheimer’s disease in Sun’s (2009) study. Evidence for construct validity of the one item was also reported (Sun, 2009). Because this item represents a subjective assessment of a person’s financial situation, it provides a more meaningful and person-centered assessment of the person’s financial challenges than more objective measures, such as income. Sun (2009) also noted that research participants may be more willing to give information on their perceived income adequacy compared with an income measure and that missing data are less for this item compared with income questions. Of note, no one in our sample refused to answer this question, leading to no missing data for this variable in our sample.
Family member depressive symptoms
Family member depressive symptomatology, the outcome variable, was measured with the short form of Center for Epidemiologic Studies Depression Scale (CES-D short form; Andresen, Malmgren, Carter, & Patrick, 1994). This 10-item screening instrument assesses the frequency of each depressive symptom over the past week on a scale from 0 (never or rarely) to 3 (everyday). The possible range of scores is 0 to 30, with higher scores representing greater degrees of depressive symptomatology. A cut-off score of 10 or higher indicates the presence of significant depressive symptoms. The tool has demonstrated high internal consistency with Cronbach’s α ranging from 0.85 to 0.92 across different populations (Carpenter et al., 1998; Irwin, Artin, & Oxman, 1999). The tool also has evidence of strong criterion validity in its sensitivity (97%) and specificity (84%) in the screening of major depressive disorder (Irwin et al., 1999). Cronbach’s α for the family member sample was .83.
Veteran characteristics
Two psychiatric comorbidities of the veteran, PTSD and depressive symptoms, were considered as individual factors in the analyses. PTSD was operationally defined as the absence or presence of a current PTSD diagnosis documented in the VA Computerized Patient Record System (CPRS) during the study period—from the baseline interview to the follow-up interview. Documentation of PTSD was retrieved through the principal investigators’ review of the electronic medical record.
Veteran depressive symptoms were measured by the CES-D short form (Andresen et al., 1994), described earlier. This instrument has been used in detecting depressive symptomatology in veterans within VA health settings (Kilbourne et al., 2002; Street, Gradus, Giasson, Vogt, & Resick, 2013). The findings that depressive symptoms in veterans with HIV (measured by the CES-D short form) were significantly and positively associated with HIV symptom frequency and count, as expected, supports construct validity of the tool. In a large national sample of Operation Enduring Freedom (OEF, Afghanistan war) Operation Iraqi Freedom (OIF, Iraq war) and veterans, internal consistency of the CES-D short form was reported as .91 (Street et al., 2013). Cronbach’s α for the veteran sample in the present study was .85.
Data on military and TBI-related characteristics were also retrieved from the CPRS to characterize the sample. These data included war cohort, time since most recent TBI, cause of injury, number of TBIs, and other comorbidities (veteran depression diagnosis during study period, pain, tinnitus, and photosensitivity). To determine TBI severity, a coinvestigator with expertise in rehabilitation medicine reviewed the veteran’s electronic medical record and assessed the severity level of the most recent TBI using the Veterans Affairs/DOD Clinical Guidelines for Management of Concussion/Mild Traumatic Brain Injury (mTBI; U.S. Department of Veterans Affairs & DOD, 2009). TBI severity for the sample was characterized as across five levels of severity (mild, mild-moderate, moderate, moderate-severe, and severe) as explained in earlier reports (Moriarty, Winter, Robinson, True, et al., 2015; Winter et al., 2016). In the guidelines, TBI injury severity is stratified across three levels (mild, moderate, severe) based on five variables (reported findings on structural imaging based on radiographic reports, reported or documented length of time of loss of consciousness, reported or documented length of time of alteration of consciousness, reported or documented length of time of posttraumatic amnesia, and the Glasgow Coma Scale score at the time of the injury or injuries). For our sample, the Glasgow Coma Scales scores were unavailable; however, data for the other four variables were consistently available in veterans’ medical records. When three or four of the variables were reported or documented as falling within the specified severity level, then this level was assigned (mild/moderate/severe); if one or two variables fell across two or three specified severity levels, then the level was assigned as “transitional” in severity (mild to moderate; moderate to severe).
Measures for family factors
Type of family relationship
Data on type of relationship (spouse vs. other) was considered a potential predictor in the analyses. This was self-reported by the family member in the demographic questionnaire.
Caregiver burden
Another family factor considered in our model was caregiver burden, defined as the subjective perceptions of psychological distress, fatigue, anxiety, depression, poor health, social isolation, loss of freedom, feelings of being trapped, and resentment that are attributed directly to caregiving (Lawton, Kleban, Moss, Rovine, & Glicksman, 1989; Lawton, Moss, Kleban, Glicksman, & Rovine, 1991; Struchen, Atchison, Roebuck, Caroselli, & Sander, 2002) for the veteran with TBI. Burden in this definition refers to a dyadic relationship, and therefore it was viewed as a dyadic family factor. Caregiver burden was measured by a 15-item subscale of the Modified Caregiver Appraisal Scale (CAS; Struchen et al., 2002). The CAS, a 35-item multidimensional instrument, measures positive and negative appraisals of caregiving, based on the stress and appraisal framework (Lazarus & Folkman, 1984). Developed by Lawton and colleagues (1989), the CAS was later modified by Struchen et al. (2002) and tested in a sample of 241 family caregivers of adults with TBI. Internal consistency of the caregiver burden subscale was .91 in Struchen’s sample. Concurrent validity of the caregiver burden subscale was supported by its relatively high correlations with standard measures of burden. The burden subscale scores were also significantly related to overall psychological health, an indicator of construct validity. Family members were asked to state their degree of agreement on a 5-point scale from 1 (strongly disagree) to 5 (strongly agree) to each statement in reference to caring for the veteran with TBI, such as, “I feel isolated and alone as a result of caring for [the veteran],” “I am very tired . . .” and “My health has suffered . . .” Cronbach’s α in our sample of family members was .92.
Community factor
Social support
Social support experienced by the family members was measured by four items eliciting emotional support received from others in the community, aside from the veteran (e.g., others provide comfort, listen, express interest). The items were derived from other established social support tools that were combined in a hybrid instrument used in the REACH multisite study (Belle et al., 2006; Wisniewski et al., 2003). Items were rated on a 4-point Likert-type scale from 0 (not at all) to 3 (very much). Cronbach’s α for this sample was .78.
Data Analysis
Descriptive statistics to characterize the sample and to describe the major variables were generated. To assess potential multicollinearity, associations among the predictors of interest were tested using Pearson product-moment correlations or t tests as appropriate, and variance inflation factors were computed. Pearson product-moment correlations were also used to assess the relationship between TBI characteristics (time since the most recent TBI and TBI severity) and depressive symptoms. To answer the research question, a hierarchical multiple regression analysis (Cohen & Cohen, 1983) was conducted, guided by the ecological model. Hierarchical multiple regression was used to assess how the addition of each block contributed to the variance in depressive symptoms after controlling for the effects of the predictors previously entered (Cohen & Cohen, 1983). In Step 1, individual factors of the family member (sociodemographics) were entered into the model, followed by individual factors of the veteran (two psychiatric comorbidities often present with TBI) in Step 2, followed by the family factors (type of relationship and caregiver burden) in Step 3, and concluding with entry of the community factor (social support) in Step 4. The final regression model enables determination of the independent contributions of all predictors after controlling for other variables, along with the proportion of variance in depressive symptoms explained by all the individual, family, and community factors.
The a-priori α level is .05. Missing data were rare in our sample because the data were collected through interviews. All analyses were conducted with SPSS, version 20.
Results
Sample Characteristics
Tables 1 and 2 present sociodemographic characteristics of 83 family members and 83 veterans. Family members’ mean age was about 42 years with a range between 21 and 67 years. The family sample was primarily White (60%), 31% was Black, and 4% was Asian. Most were female and spouses to the veteran. The majority of family members was married and had children. About two thirds of family members were employed compared with one third of veterans who were employed. Veterans’ mean age was about 40 years, ranging from 23 to 67 years. The veteran sample consisted largely of White veterans (58%), and Black veterans constituted about one third of the sample. Most veterans (92%) were male, and the majority was married with children. Most (97.6%) of veterans lived with the family members who participated in the study.
Sociodemographic Characteristics of Family Members.
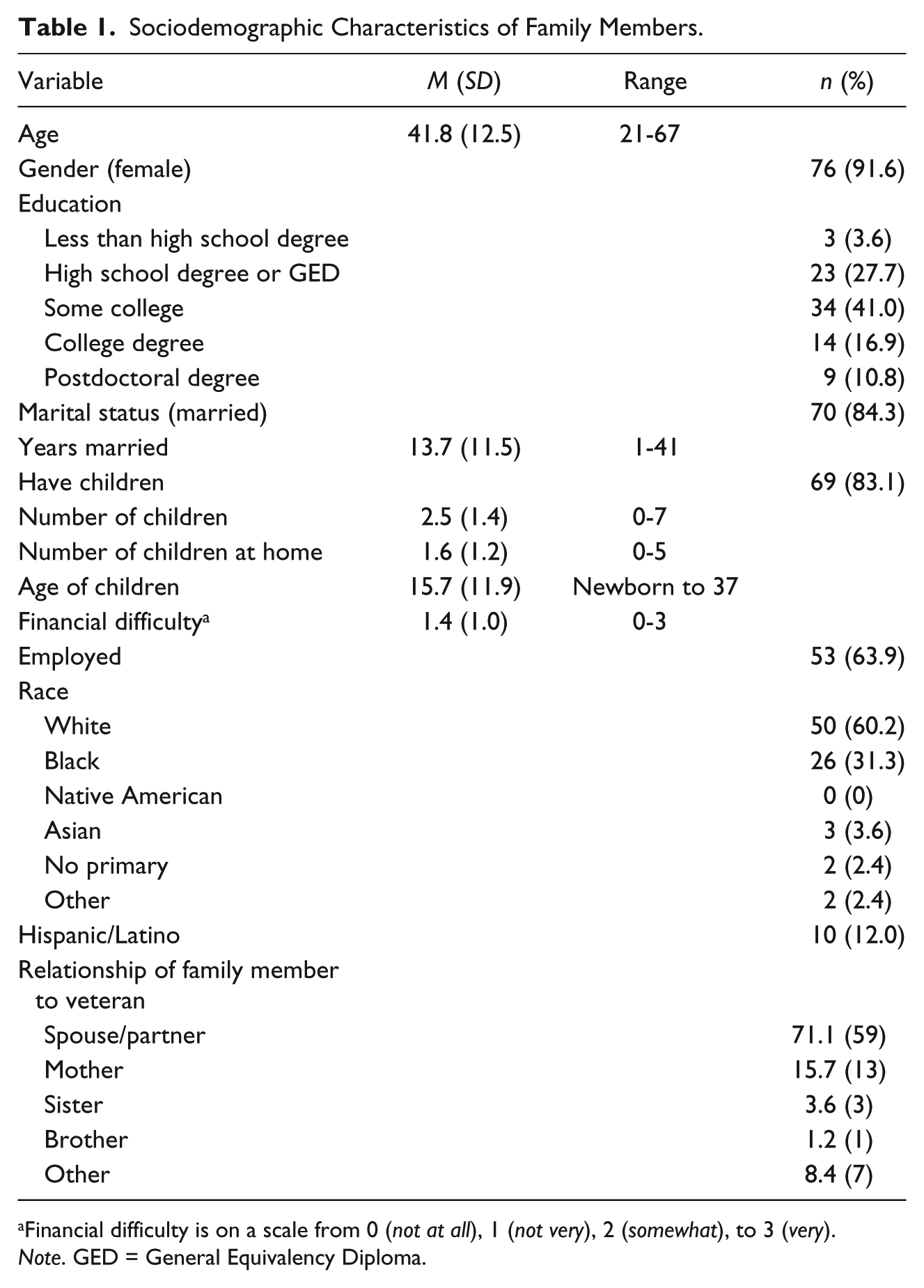
Financial difficulty is on a scale from 0 (not at all), 1 (not very), 2 (somewhat), to 3 (very).
Note. GED = General Equivalency Diploma.
Sociodemographic Characteristics of Veterans (N = 83).
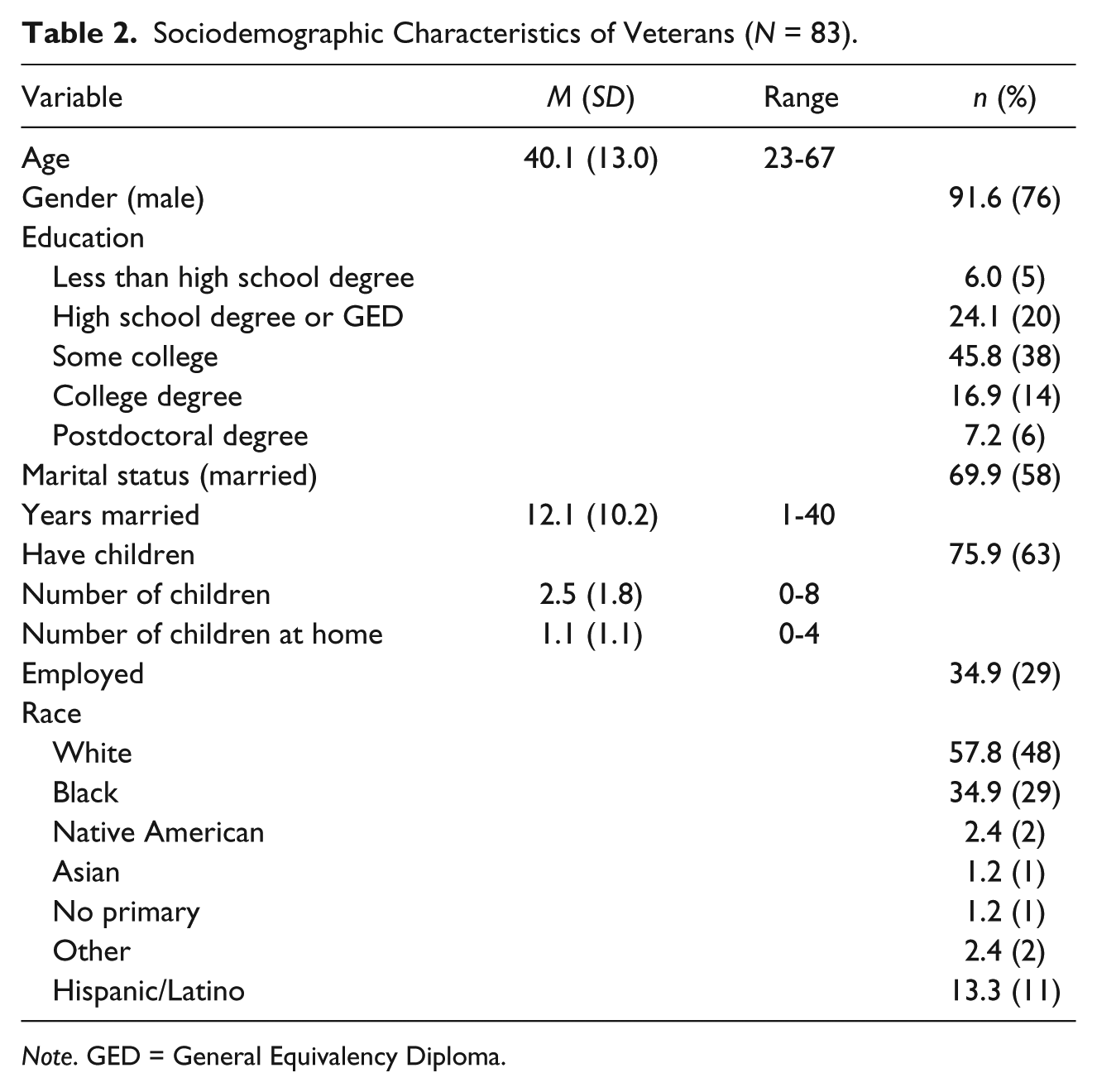
Note. GED = General Equivalency Diploma.
Table 3 provides information about veterans’ war cohort, source of TBI, number of TBI-incidents, severity of the most recent TBI, time since the most recent TBI, psychiatric comorbidities (depression and PTSD), and prevalence of major TBI-related symptoms. Most veterans served in OIF, followed by those from OEF. Sources of the TBI varied. Over one third had experienced multiple TBIs (>4), and about one third reported one TBI incident. About 65% had a PTSD diagnosis documented as active in the veteran’s medical record during the time between the baseline and follow-up interview. Fifty-eight percent had a depression diagnosis documented during this time period, and 50% of the sample was in treatment for depression during this time period.
Characteristics of Veterans: War Cohort, TBI Severity, Time Since the Most Recent TBI, Source of Injuries, Number of TBI-Related Events, Comorbidity, and Major Symptoms (N = 83 veterans).
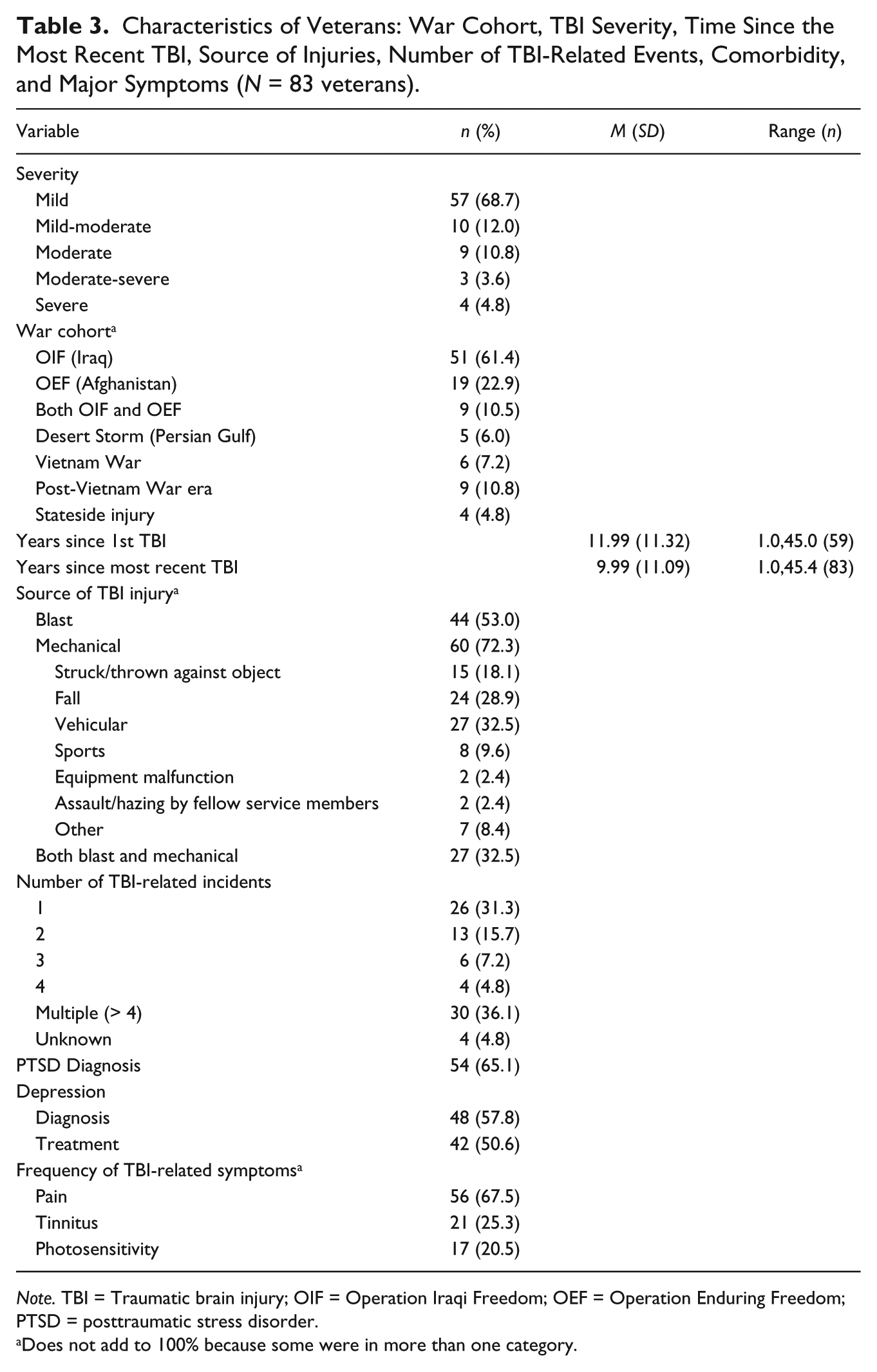
Note. TBI = Traumatic brain injury; OIF = Operation Iraqi Freedom; OEF = Operation Enduring Freedom; PTSD = posttraumatic stress disorder.
Does not add to 100% because some were in more than one category.
Table 4 presents descriptive statistics for family member depressive symptomatology, caregiver burden, family member social support, veteran PTSD diagnosis, veteran depressive symptoms, and financial difficulty at baseline. The mean of 9.74 (SD = 6.10) for family member depressive symptoms is close to the threshold score for presence of significant depressive symptoms (10). About 45% of family members had a score of 10 or higher.
Descriptive Statistics for Family Member Depressive Symptoms, Caregiver Burden, Family Member Social Support, Veteran Depressive Symptoms, and Financial Difficulty at Baseline (N = 83).
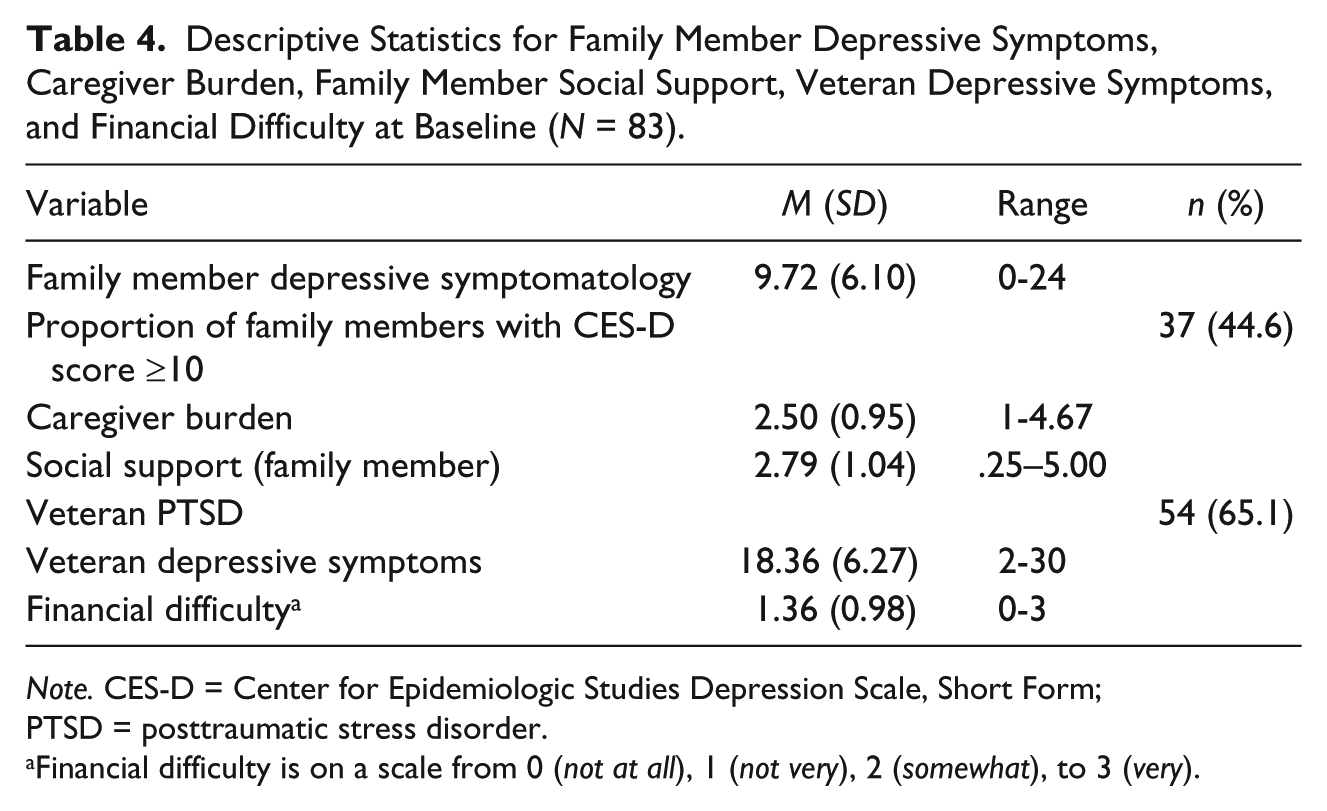
Note. CES-D = Center for Epidemiologic Studies Depression Scale, Short Form; PTSD = posttraumatic stress disorder.
Financial difficulty is on a scale from 0 (not at all), 1 (not very), 2 (somewhat), to 3 (very).
Bivariate Relationships
An intercorrelational matrix (Table 5) presents bivariate relationships among the predictor variables and depressive symptoms. Multicollinearity among the predictor variables was not present as the variance inflation factor values were all less than 4. Bivariate relationships between TBI characteristics (severity and time since most recent injury) and depressive symptoms were also examined, as TBI characteristics were considered as potential covariates.
Bivariate Associations (r or t) Among All Variables With Significance Levels (p).
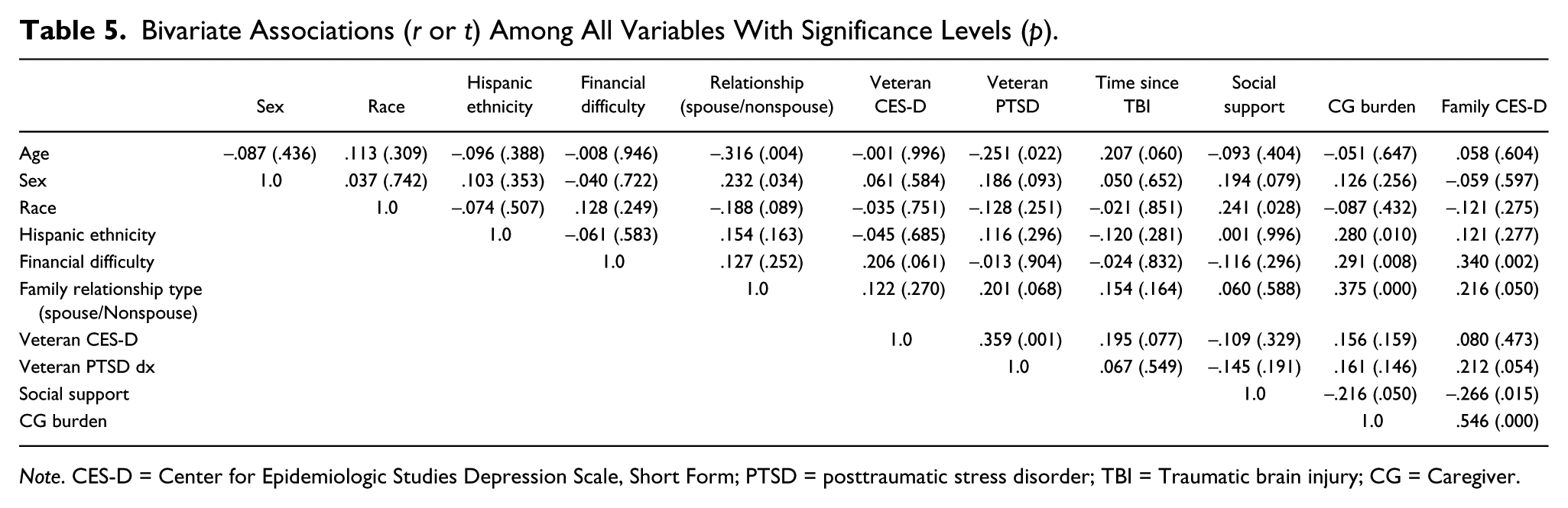
Note. CES-D = Center for Epidemiologic Studies Depression Scale, Short Form; PTSD = posttraumatic stress disorder; TBI = Traumatic brain injury; CG = Caregiver.
Regression Analyses: Predictors of Family Member Depressive Symptoms
The regression models for depressive symptoms had residuals (error terms) that were approximately normally distributed. Results of the regression analysis are displayed in Table 6. When family member sociodemographic characteristics were entered in Block 1, financial difficulty had a significant positive relationship with family member depressive symptoms (p = .001), and the effect remained significant when other variables were entered in the subsequent three blocks. The predictors entered in Block 1 yielded an R2 value of 17.1% and explained significant variability in family member depressive symptoms (p = .012). In Block 2, when veteran PTSD and veteran depressive symptoms were entered, veteran PTSD was a significant predictor, and it remained significant in Blocks 3 and 4, even after family and community factors were entered. Despite the individual significance of veteran PTSD, the marginal increase in R2 was only 5.6 percentage points and not significant (p = .071). In Block 3, when two family factors (type of family relationship and caregiver burden) were entered, only caregiver burden was significant, and it remained significant in Block 4 after a community factor was entered. The additional predictors in Block 3 accounted for an increase of 18.1 percentage points in the model R2, which was significant (p = .000). Finally, in Block 4, when all individual, family, and community factors were entered, the predictors, financial difficulty, veteran PTSD, and caregiver burden, were all significantly associated with family member depressive symptoms, accounting for 40% of the variance in depressive symptoms. Increased predicted values for family member depressive symptoms were associated with higher burden, the presence of veteran PTSD, and greater financial difficulty. The lack of significance of the community factor, social support (p = .938), is accompanied by no change in the overall model R2.
Multiple Regression of Family Member Depressive Symptoms on Veteran Depressive Symptoms, Veteran PTSD, Type of Family Relationship, Caregiver Burden, and Social Support, After Controlling for Family Member Sociodemographic Characteristics.
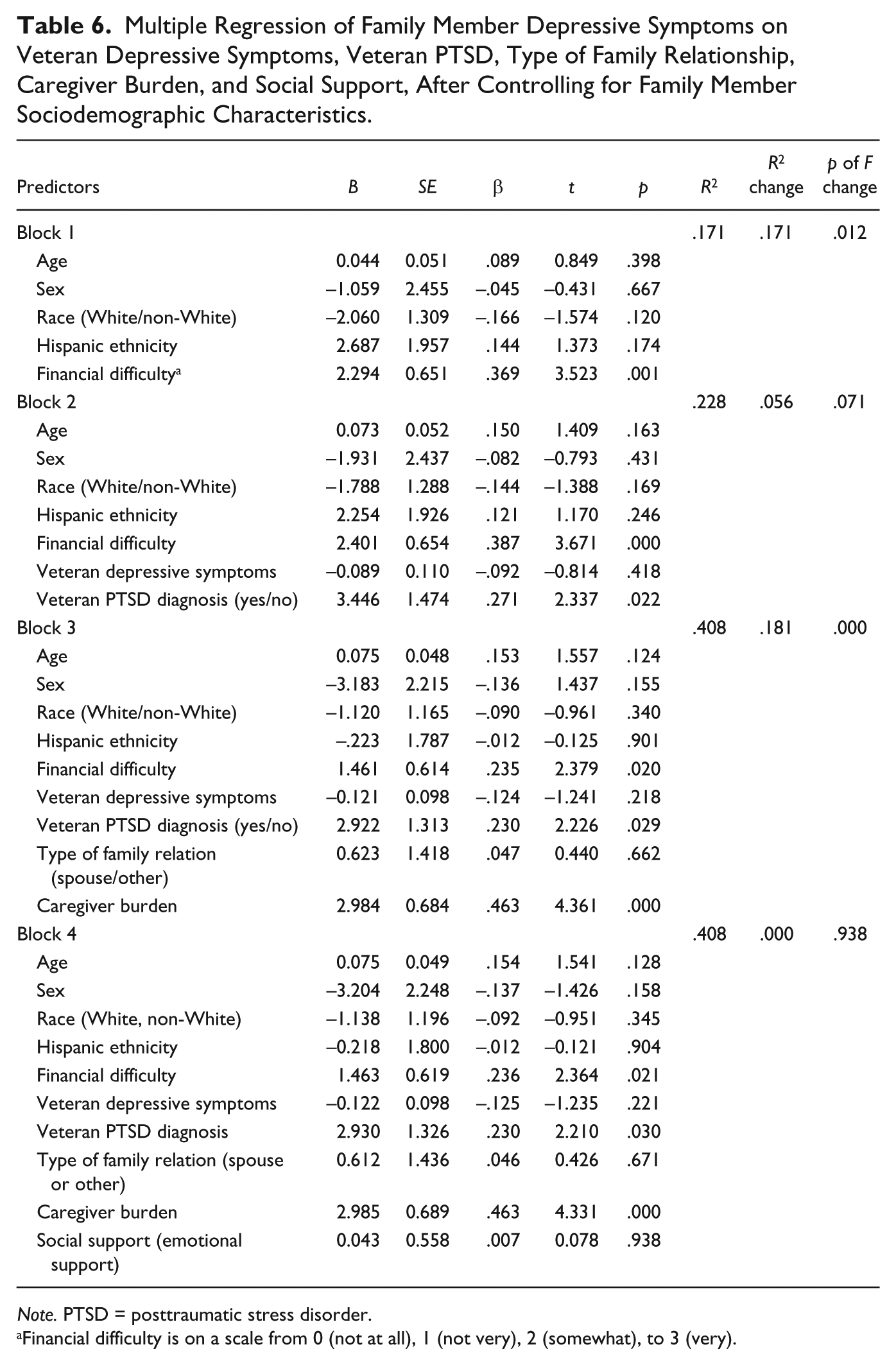
Note. PTSD = posttraumatic stress disorder.
Financial difficulty is on a scale from 0 (not at all), 1 (not very), 2 (somewhat), to 3 (very).
Discussion
The ecological model provided a useful framework for understanding the interrelationships among and contributions of individual, family, and community factors to family member depression. In the final regression model, only one family factor (caregiver burden) and two individual factors (veteran PTSD and financial difficulty perceived by the family member) were significant predictors of family members’ depressive symptoms. Family members who had greater burden, greater financial difficulty, and the presence of veteran with a PTSD diagnosis experienced more depressive symptoms. These findings underscore the importance of caring for the whole family of the veteran with TBI and the need to engage patients and families in family-centered care.
Other factors examined in the study (veteran depressive symptoms, type of family relationship, social support, and family sociodemographics) were not significantly associated with family member depressive symptoms. Social support initially showed a significant negative bivariate relationship with family member depressive symptoms, as reported in previous literature (Calvete & de Arroyabe, 2012; Douglas & Spellacy, 2000; Riley, 2007). However, when considered with other factors in the model, social support lost its independent contribution. This demonstrates the need to consider not just the bivariate relationship but also the contribution of multiple factors to the outcome of interest, as purported by the ecological model. Because our measure of social support captured only emotional support, it is possible that another instrument encompassing other aspects of social support, such as instrumental support, could have revealed relationships with depressive symptoms. In addition, the somewhat lower internal consistency of our four-item measure of emotional support could have influenced our findings.
Among the veterans, about two thirds had a current diagnosis of PTSD, and the presence of this diagnosis contributed to greater family member depressive symptomatology. This finding aligns with earlier studies reporting that partners living with veterans with PTSD experienced more psychological distress, including depression, than partners of veterans without PTSD (Yambo & Johnson, 2014). In civilian TBI populations, little research has considered the role of civilian PTSD in family members’ depression. Our findings support increased attention to this because civilians with TBI may also experience PTSD from traumatic situations (Zatzick et al., 2007) causing their brain injuries, such as car accidents, falls, and assaults, and it is possible that this contributes to depression in their family members.
Identification of veteran PTSD as a risk factor for family member depressive symptoms is clinically important for family nurses and other health professionals because of the high prevalence of PTSD in military veterans and the proportion of veterans with TBI who also suffer PTSD. A recent review concluded that about 23% of veterans serving in the military over the last decade have been diagnosed with PTSD (Fulton et al., 2015). Rates of PTSD among veterans and active duty military with TBI are reported as ranging from 33% to 68% (Wall, 2012). Thus, a large number of family members of veterans are facing unique challenges imposed by the challenges of concurrent TBI and PTSD. Given the well-documented negative impact of PTSD on individuals’ physical health, emotional health, and relationships (Driesenga, Rodriguez, & Picard, 2015; Wagner, Wolfe, Rotnitsky, Proctor, & Erickson, 2000), PTSD in the veteran may add to the stress of family members trying to support their loved one with TBI. Furthermore, PTSD in veterans has been associated with increased verbal and physical aggressive behavior toward their partners and children, increased marital difficulties, and increased behavioral problems among children of the veteran (Monson, Taft, & Fredman, 2009, U.S. Department of Veteran Affairs, 2004), which may also intensify depressive symptoms in the family member.
Family members who experienced more burden had higher depressive symptoms, a finding also observed in family members of civilians with moderate to severe TBI (Machamer et al., 2002) and family members of post-9/11 veterans with TBI severity ranging from mild to severe, with the majority (70%) having moderate to severe TBI (Griffin et al., 2017). Similarly, burden has been identified as a significant predictor of depression in partners of veterans with PTSD (Calhoun, Beckham, & Bosworth, 2002). Because caregiver burden in our study encompassed subjective perceptions of many domains, including anxiety, fatigue, depression, poor health, and resentment attributed to caregiving (Struchen et al., 2002), the relationship found with depression in our study is not surprising. From a clinical perspective, these findings suggest that nursing assessments of what is most burdensome to families could be used to develop and test interventions designed to minimize the specific burdens and at the same time reduce depressive symptoms. The development of a brief burden measure that nurses and other clinicians could routinely use to assess burden would be a worthwhile direction for future research.
Financial difficulty remained significant in the final regression equation, consistent with a study on civilian TBI that revealed financial difficulty as a significant predictor. In Riley’s (2007) study, financial difficulty contributed to increased stress and decreased coping ability in family members of civilians with TBI; severity of TBI was not reported. TBI may diminish employment opportunities for veterans, thus affecting the family’s income and possibly the resources available for families. In our sample, only one third of veterans were working, possibly leading to financial pressure, particularly in families with children at home. Similarly, family members of veterans with TBI may experience employment interruptions or reduced employment opportunities related to caregiving demands (Malec et al., 2017). Of note, none of the family members in our sample were enrolled in the VA Program of Comprehensive Assistance for Family Caregivers that provides financial stipends directly to caregivers of veterans who are severely injured during military service after September 11, 2001 (Malec et al., 2017). Our findings suggest that financial assistance for family members of veterans with varied levels of TBI severity warrants consideration by policy makers.
Clinically significant levels of depressive symptoms were observed in 45% of our sample of family members. This finding corroborates previous research showing significant distress, including depression and anxiety, in about one third of family members caring for civilians with severe brain injury within 1 year after the injury (Marsh et al., 2002) and another study showing clinically significant depressive symptoms in 45% of family members of civilians with primarily moderate to severe TBI at 2 years and 5 years postinjury (Ponsford & Schonberger, 2010). This finding also is consistent with data from 20 wives of Israeli war veterans with postconcussive syndrome (presumably mild TBI) who reported significantly higher levels of depression compared with 20 women married to healthy controls (Ben Arzi, Solomon, & Dekel, 2000). A larger, nationally representative study of 1,129 U.S. military caregivers found that nearly 40% of post-911 caregivers (165 out of 414) met criteria for probable major depressive disorder; 20% of the post-911 group were caring for loved ones with TBI (Ramchand & Tanielian, 2014). Interestingly, our sample consisted of family members of veterans with primarily mild TBI, yet the prevalence of significant depressive symptomatology in our sample was comparable to that seen in the earlier civilian studies involving more severe injuries and in the national sample of military caregivers. Also, of note, severity of TBI and time since the most recent TBI, despite the wide range of severity and years since the last TBI, were not significantly associated with family member depressive symptoms in our sample, a finding consistent with studies with civilians (Blais & Boisvert, 2005; Ponsford & Schonberger, 2010). Our findings suggest that family members of veterans with TBI are a vulnerable high risk group who need support no matter the length of time since the injury and the level of injury severity. A better understanding of the prevalence of depression among these family members is essential to inform policy making around allocation of national resources for families of veterans.
Implications for Practice and Future Research
Taken as a whole, the findings reinforce the need for family nurses and other health professionals to engage in ongoing collaboration with families of veterans with TBI, consistent with the International Family Nursing Association (IFNA) Position Statement on Generalist Competencies for Family Nursing Practice (IFNA, 2015) and the Position Statement on Advanced Practice Nursing Competencies for Family Nursing (IFNA, 2017). This collaboration has dual benefits: (a) It provides opportunities to support families and refer them to community resources and (b) It promotes family engagement in rehabilitation of the person with TBI, which is particularly paramount to the success of rehabilitation.
The high prevalence of significant depressive symptoms observed in our sample and previous studies reinforces the need for family nurses and other health professionals to conduct early assessments and identification of family members at higher risk for depression and for interventions that include the patient with TBI (whether veteran or civilian) and family members. Systematic assessments of family members are not typically performed in outpatient TBI rehabilitation settings, and thus health professionals may be missing opportunities to offer supportive interventions to families or to refer family members for additional services. Emerging literature has emphasized consideration of the entire family after a TBI and called for interventions that address both patient and family needs post-TBI (Boschen, Gargaro, Gan, Gerber, & Brandys, 2007; Dausch & Saliman, 2009; Foster et al., 2012; Stejskal, 2012). However, there is very little evidence-based family-focused care, as only a limited number of rigorous intervention studies have targeted both the person with TBI and a family member or only the family member (Backhaus, Ibarra, Klyce, Trexler, & Malec, 2010; Carnevale, Anselmi, Johnston, Busichio, & Walsh, 2006; Hanks, Rapport, Wertheimer, & Koviak, 2012; Moriarty, Winter, Robinson, Piersol, et al., 2015; Rivera, Elliott, Berry, & Grant, 2008; Winter et al., 2016), and only one of these studies involved military veterans with TBI and their families (Moriarty, Winter, Robinson, Piersol, et al., 2015; Winter et al., 2016). Our findings underscore the importance of continued research to design and evaluate family-inclusive interventions in both civilian and veteran TBI populations. Consistent with this, Veterans Health Administration priorities now direct increased attention to family well-being, and the VA is systematically expanding family-centered approaches to care (Ford et al., 2014; Glynn, 2013; Malec et al., 2017). For example, a VA Family Care Collaborative has implemented a Family Care Map in five regional inpatient Polytrauma Rehabilitation Centers to standardize and promote family-centered care in this setting (Ford et al., 2014). However, challenges in engaging family members in outpatient VA polytrauma services are reported by clinicians and a focus of growing attention within the VHA (U.S. Department of Veteran Affairs, QUERI, 2015).
Even after all other factors were entered into the regression model, the single-item measure of perceived financial distress remained a significant predictor of family members’ depressive symptoms. Family nurses and other clinicians could easily pose this question to assess financial situations within families and work with interprofessional teams and community resources to plan interventions to reduce financial distress.
Taken as a whole, our findings suggest that the efforts of family nurses, other health professionals, and communities to support families and decrease depression in family members should aim to reduce caregiver burden and financial stress, and assist family members in their efforts to manage PTSD and TBI. Connecting veterans and their family members with VA and community programs that offer treatment for PTSD may be helpful for the entire family, as studies have shown positive effects of couples and family therapy (U.S. Department of Veterans Affairs & DOD, 2010). Crisis services, such as the Veterans Crisis Line and the VA Caregiver Support Line, are also available for family members (Driesenga et al., 2015). VA and community programs that provide families of veterans with TBI with strategies for symptom management and problem-solving may attenuate caregiver depression and burden, as demonstrated in two randomized controlled trials (Moriarty, Winter, Robinson, Piersol, et al., 2015; Rivera et al., 2008; Winter et al., 2016). Programs that integrate treatment for veterans with TBI and PTSD are also emerging in the literature (Carlson et al., 2011; Jak et al., 2015; Otis, McGlinchey, Vasterling, & Kerns, 2011; Tanev, Pentel, Kredlow, & Charney, 2014) and may have indirect benefits for families. Evaluation of varied approaches to support both veteran and civilian families is critical given the limited evidence in this area. Data from these studies are also necessary to drive and sustain national policies and programs to assist families of veterans. For example, Public Law 10-87 requires that the VA health system offers or arranges for veterans to receive marital and family counseling (Glynn, 2013), and our data support the need for this counseling.
Almost one out of eight Americans is a veteran or related to a veteran (Newport, 2012). About 40% of veterans returning from Iraq and Afghanistan seek health care outside the Veterans Health Administration system (U.S. Department of Veterans Affairs, 2015), and some of these may include veterans with TBI who have not accessed VA health care services, despite being eligible for VA care (Bagalman, 2013). Thus, nurses in varied civilian settings are frequently caring for veterans and their families and need to be aware of their strengths, struggles, and complex issues. As part of the national “Joining Forces” campaign and the Bob Woodruff Foundation initiative in the United States, nurses are called upon to ask every patient, “Have you ever served in the military?” to elicit veteran status and subsequently address issues that may be associated with military experience, such as veteran TBI, PTSD, and depression (American Academy of Nursing, 2014; Collins, Wilmoth, & Schwartz, 2013). Health professionals who recognize that when veterans serve, their families serve too, as our data indicate, will also be sensitive to the challenges family members face and strive to deliver patient- and family-centered care.
Limitations and Strengths
Our cross-sectional analysis precludes any causal inferences. Generalizability of the findings may be limited to family members of veterans with TBI followed by the VA health system and who were willing to participate in an intervention study. Findings may be less generalizable to families of veterans with TBI who receive care outside the VA system. Future research should incorporate longitudinal designs and include family members of veterans with TBI from non-VHA settings as well as family members of civilians with TBI. Our one-item measure of perceived financial distress, although meaningful, could be augmented by objective measures of financial distress in future research. Another limitation is that our study did not collect data on caregiver services (VA or community) that family members were currently using beyond whether they were enrolled in the VA Program of Comprehensive Assistance for Family Caregivers; these additional data are important to include in future studies. Despite the acknowledged limitations, our study advances understanding of the mental health of family members of veterans with TBI, particularly those with mild to moderate TBI. Previous research has focused on families of civilians with primarily moderate to severe TBI, but the large majority of TBIs are mild, representing 82% cases of military TBIs (Defense and Veterans Brain Injury Center, 2014) and 80% of civilian TBIs (CDC, 2016; Warden, 2006).
Conclusion
Guided by the ecological model, this exploratory study illuminated three factors—caregiver burden, the presence of a veteran with a PTSD diagnosis, and financial difficulty—related to depressive symptoms in family members of veterans. These factors are clinically meaningful and can be easily assessed by family nurses and other health professionals during interactions with families in diverse clinical settings. Efforts to support families and decrease depression in family members should aim to reduce caregiver burden and financial stress and should recognize the additional risk that PTSD in the veteran poses to the caregiver. Family-inclusive interventions that provide strategies for veterans and family members to manage PTSD and TBI and that offer support for family members are key directions for clinical practice and future research. Given that TBI is a global public health problem, nurse investigators with a family focus should engage in international partnerships to develop and test family interventions for civilians, active service members, and military veterans.
Footnotes
Acknowledgements
The research team gratefully acknowledges the veterans with traumatic brain injury (TBI) and their family members who gave of themselves and their time to share their stories and take part in this study.
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by Award Number R21 HD068857-01 from the Eunice Kennedy Shriver National Institute of Child Health & Human Development, National Institutes of Health, USA. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Eunice Kennedy Shriver National Institute of Child Health & Human Development or the National Institutes of Health. This material is the result of work also supported with resources and the use of facilities at the Corporal Michael J. Crescenz VA Medical Center, Philadelphia, PA, USA.