
Abstract
Children’s experiences of information and family communication when a parent has a life-threatening illness have been sparsely studied, though such information is important for the child’s wellbeing. The aim of this study was to explore children’s reports of illness-related information and family communication when living with a parent with a life-threatening illness. Forty-eight children, aged 7 to 19 years, were recruited from four specialized palliative home care units in Stockholm, Sweden. All but one child reported that someone had told them about the parent’s life-threatening illness; however, two thirds wanted more information. A quarter of the teenagers reported that they had questions about the illness that they did not dare to ask. Half of the children, aged 8 to 12, reported that they felt partially or completely unable to talk about how they felt or show their feelings to someone in the family. Interventions are needed that promote greater family communication and family–professional communication.
Children in families where a parent has a life-threatening illness report distress and concerns related to a lack of information about the parent’s illness and death, their own feelings of guilt, and fear of getting the illness themselves or that their other parent will also fall ill (Christ et al., 1993; Dehlin & Mårtensson, 2009; Kennedy & Lloyd-Williams, 2009a; Melcher et al., 2015; Phillips, 2015; Spira & Kenemore, 2000). Dunning (2006) has argued that information about illness in the family prevents psychological ill-health among children. Previous research about bereaved children found that inadequate information and poor communication between the family and professionals during the illness trajectory increased the risk for long-term psychological distress years after the loss (Bylund-Grenklo et al., 2014; Eilegard Wallin et al., 2016; Lövgren et al., 2018). According to Swedish law (Swedish Healthcare Act [Hälso- och sjukvårdslag: HSL] (Svensk författningssamling [SFS] 2017:30) [Swedish Code of Statutes], 2017), it is the responsibility of health care professionals to acknowledge needs and provide support and information to children of parents with a life-threatening illness.
Communicating both verbally and nonverbally about thoughts and feelings when something traumatic occurs has been shown to be a key component in coping and finding meaning in stressful situations. Failure to communicate about traumatic events may increase psychosocial distress (Lepore et al., 2000; Pennebaker, 1993). Open and honest communication between parents and children when a parent has a life-threatening illness seems to be particularly important in helping the child manage everyday life (Ellis et al., 2017; Morris et al., 2016; Phillips, 2014), as well as increase psychosocial wellbeing (Lindqvist et al., 2007). Through communication, families can come together in shared understanding about existential concepts such as life and death (Keeley, 2016).
In palliative care, families face a life-changing situation and need to find ways to adapt and cope with these challenges (Mehta et al., 2009). From a theoretical family systems perspective, the whole is greater than the sum of its parts. The family is an integrated system where each individual influences other family members; a change in one part of the system affects the family as a whole. The family composition is self-defined; it is the family who defines who is included in the “family” not just those who are linked by blood, adoption, or marriage (Wright & Leahey, 2013).
Children’s experiences of information and family communication during a parent’s life-threatening illness have been explored in only a few studies, primarily involving teenagers (Ellis et al., 2017; Finch & Gibson, 2009; Morris et al., 2016). To the best of our knowledge, no study has focused on children’s perspectives when a parent is cared for in specialized palliative home care. The aim of this study was to explore children’s self-reports of illness-related information and family communication when living in a family where a parent has a life-threatening illness and is receiving specialized palliative home care.
Method
Study Design
This study used baseline survey data from an ongoing intervention study which had the goal of supporting families who were experiencing a life-threatening illness, with a focus on children’s needs (Eklund et al., 2018).
Participants and Data Collection
Families were recruited from four specialized palliative home care units in Stockholm, Sweden, between March 2017 and February 2018. The palliative care units provided 24-hr services, with multiprofessional teams. Families at two of the units had previously been asked to participate in an ongoing intervention study, whereas the families on the other two units were used as a comparison group. For this study, all families from all four palliative home care units were included.
To participate in this study, families needed to speak and write Swedish and have at least one child aged 6 to 19 years. All children in the families were invited to participate in the intervention study, but children younger and older than 6 to 19 years were not included in the data collection for this study. In this study, the ill parent was asked to define the family composition. Families were contacted through mail and phone by the research group. All families were also given written information about the study. Age-adapted information regarding the study was given to all children, and informed consent was obtained from parents/guardians of children under 15 years. Children more than 15 years gave informed consent for their own participation. In accordance with Swedish law, children between 15 and 18 years must be informed and give consent for themselves, even though the parents give their consent. If the family gave verbal consent to participate, each family member was mailed a baseline questionnaire.
Of the 78 eligible families, 30 families participated which included 48 children. Twenty-three of the 30 ill parents were diagnosed with cancer, the others with a neurological, pulmonary, cardiovascular, or gastrointestinal life-threatening illnesses.
Close cooperation with the social workers at the specialized palliative home care units was maintained throughout the study. They were aware of the families who agreed to participate in the research and were willing to support families who reported any distress during participation. Also, the two interventionists were available to the participating families if they experienced any distress.
This study was approved by the Regional Ethical Review Board in Stockholm, approval numbers 2016/664-31/5 and 2017/7-31/1.
Measurement
Due to a lack of standardized instruments that measure illness-related information and family communication for children in this specific context, study-specific questionnaires were developed using the method suggested by Charlton (2000). Questions from earlier nationwide surveys regarding the loss of a family member were used (Bylund-Grenklo et al., 2014; Kreicbergs et al., 2004; Lövgren et al., 2016), as well as questions from earlier intervention studies (Holm et al., 2016; Pihkala et al., 2010). To refine and improve the questions used in earlier studies and to generate new relevant questions adapted for the context of palliative care, interviews were conducted with seven family members. As recommended by Charlton (2000), the questionnaires were pilot-tested and sent to families for validation. Through pilot-testing, age-adapted questionnaires were developed for children 6 to 7 years old, children 8 to 12 years old, and teenagers 13 to 19 years old (Eklund et al., 2018). All families were informed that a researcher from the research group could help children fill out the questionnaires; two of 48 children requested such help.
Illness-related information
All children were asked whether someone had talked to them about their parent’s illness and whether they wanted to know more about it. These two questions were answered on a 3-point response scale from “no” to “yes, a lot” by children aged 6 to 12 years and on a 4-point response scale from “do not agree at all” to “agree completely” by teenagers. All of the children were also asked about what illness their parent had, and who had informed the child about their parent’s illness. These two questions were open-ended. Teenagers, but not younger children, were asked seven further questions concerning the information they had received regarding the parent’s illness, for example, about the parent’s prognosis and treatment. These questions were answered on a 3-point response scale from “have not received any information” to “have received enough information.” For each of the seven questions, the teenagers were asked whether they had received this information from health care professionals, someone in their family, or some other source.
Family communication
This area involved questions concerning communication within the family in the context of living with a parent with life-threatening illness. All children were asked whether they could talk to someone in the family about how they felt. This question was answered on a 3-point response scale from “no” to “yes, a lot” by children aged 6 to 12 years and on a 4-point response scale from “do not agree at all” to “agree completely” by teenagers. Children aged 8 to 19 years were also asked whether they wanted to talk more, whether they could show someone in the family how they felt, and whether they wanted to show this more. In two open-ended questions, they were asked to write about who in the family they could talk to and show their feelings to. The teenagers were asked five additional questions, such as whether they had any questions they did not dare ask and whether they were satisfied with the conversation within the family about the parent’s illness. These questions were answered on a 4-point response scale from “do not agree” to “agree completely.”
Data Analysis
Answers from closed-ended questions were analyzed with descriptive statistics, calculated as frequencies and percentages using IBM SPSS Statistics version 24. Answers to open-ended questions were analyzed based on similarity in content (Krippendorff, 2004). Children’s reports regarding who the child could talk to and show feelings to were sorted into different units based on what the child had written (e.g., “mother,” “father”) and then the amount in each unit was summed. The children’s reports about the parent’s illness were compared with the ill parents’ reports (baseline questionnaires) and then the amount in each unit was summarized.
Results
Demographic Characteristics of the Children
The age of the children in this study (N = 48) ranged from 7 to 19 years. Two of the children were 7-year-old girls; 20 were between 8 and 12 years, of whom 14 were boys; and 26 were teenagers, of whom half were girls. Most children lived in nuclear families and all but six had siblings (Table 1).
Demographic Characteristics of Participating Children.
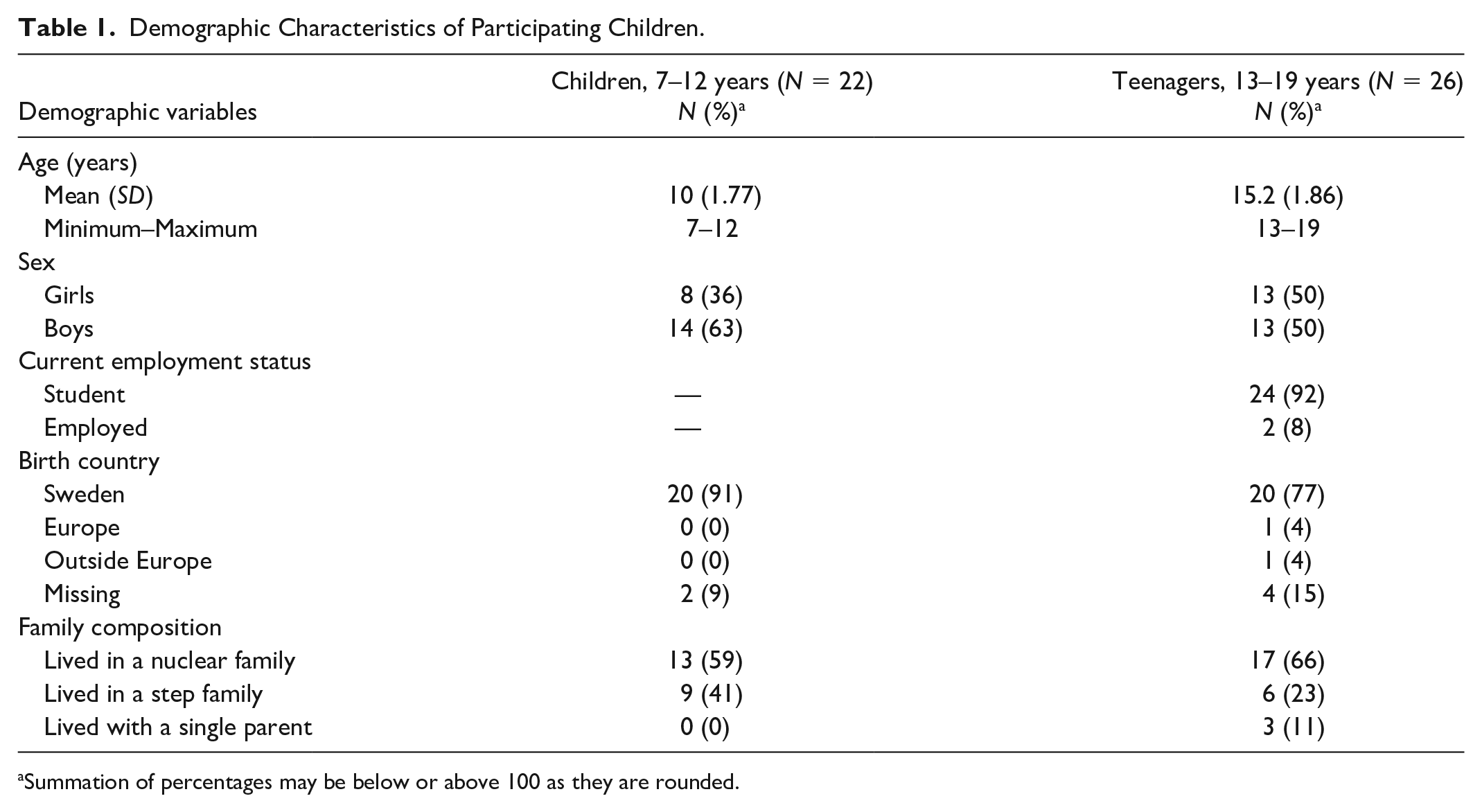
Summation of percentages may be below or above 100 as they are rounded.
Illness-Related Information
Reports from children aged 7 to 19 years
All but one child reported that someone had told them about the parent’s illness. Most children (42/48) received that information from their parent(s). Two children received the information from a sibling and three teenagers received information from a physician. Two thirds of the children (32/48) wanted to know more about their parent’s illness (Table 2). In most instances (40/48), the child’s and the ill parent’s reports of the illness agreed. The eight children who did not report the same illness as their parents had responded “I don’t know” or left the field blank. In two families, the parents had very rare diagnoses and the children had described the symptoms or treatment instead of naming the illness.
Children’s Reports of Illness-Related Information Received.
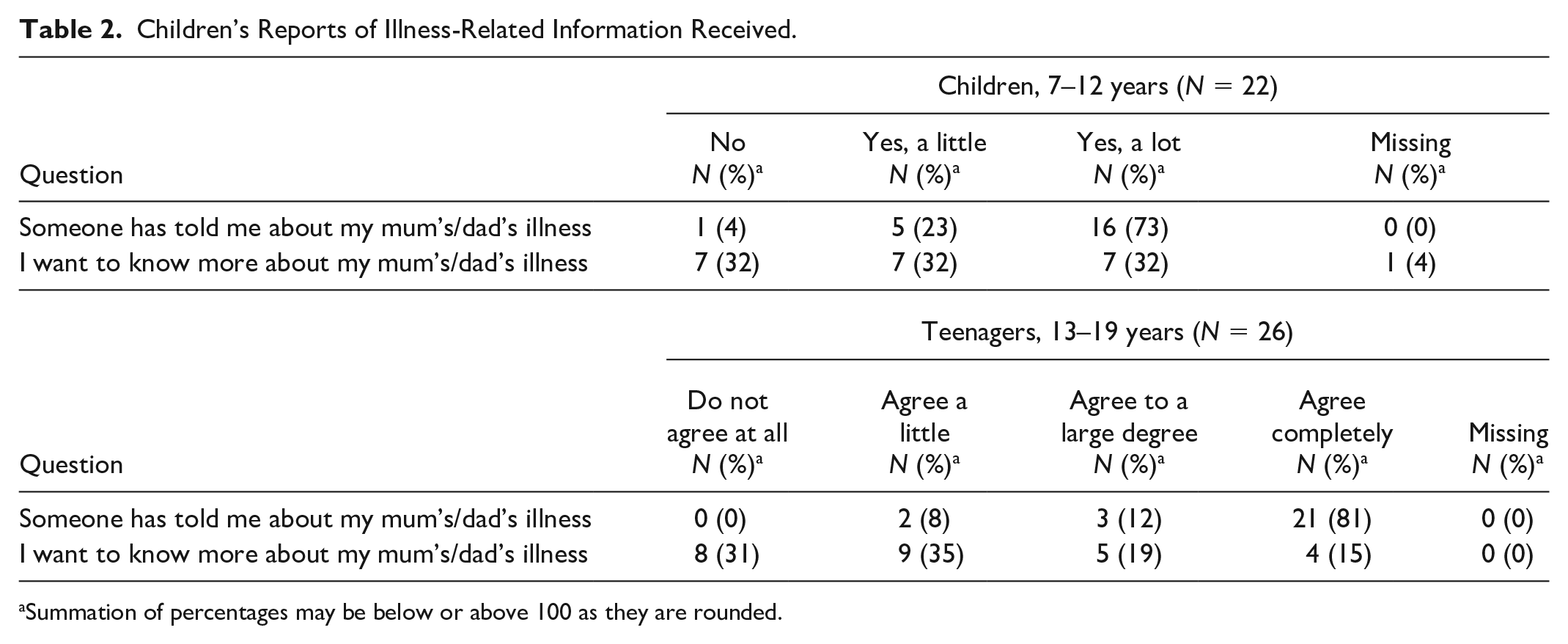
Summation of percentages may be below or above 100 as they are rounded.
Reports from teenagers
Almost all the teenagers (24/26) had received information about the illness progression. Around one-quarter reported that they received a little, but not enough, information about the parent’s treatment (6/26) and how the treatment could affect the parent’s physical health (7/26). Seven of 26 teenagers reported not having received any information at all about how the treatment could affect the parent’s mental health, and eight reported having received a little, but not enough, information about this. Almost three quarters (18/26) reported that they received little or no information about what they could do if an illness-related emergency occurred. Approximately one third (8/26) reported that they had received a little information about who they could contact if they had any questions about the parent’s illness; this information came from parents and/or health care professionals. However, five teenagers reported not having received any such information. Six of the teenagers reported having received some, but not enough, information about who to contact for their own support, while four had not received any such information. The teenagers mainly received illness-related information from someone in the family (Table 3).
Teenagers’ Reports of Illness-Related Information Received.
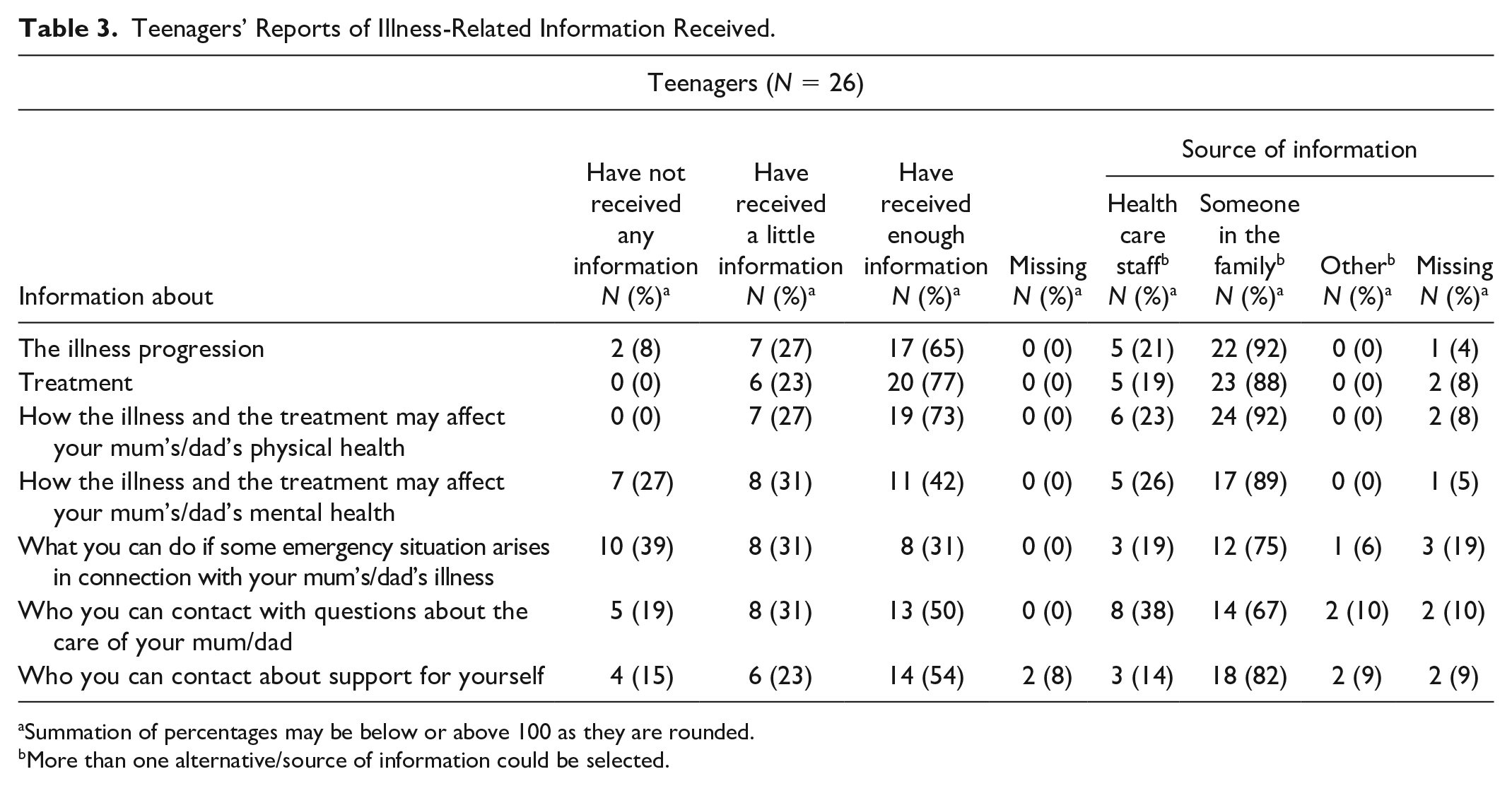
Summation of percentages may be below or above 100 as they are rounded.
More than one alternative/source of information could be selected.
Family Communication
Reports from children aged 7 to 12 years
Two girls were 7 years old: one reported that she could only talk a little to someone in her family and the other girl reported that she could talk a lot (Table 4). Eight of the 20 children aged 8 to 12 years reported that they could not talk at all about how they felt, or only a little, with someone in the family. Half of the children (10/20) wanted to talk more about how they felt with someone in their family (Table 4). Of the children who talked to someone in the family, half reported that they talked with their parent(s).
Children’s Reports of Communication Within the Family During the Last Week.
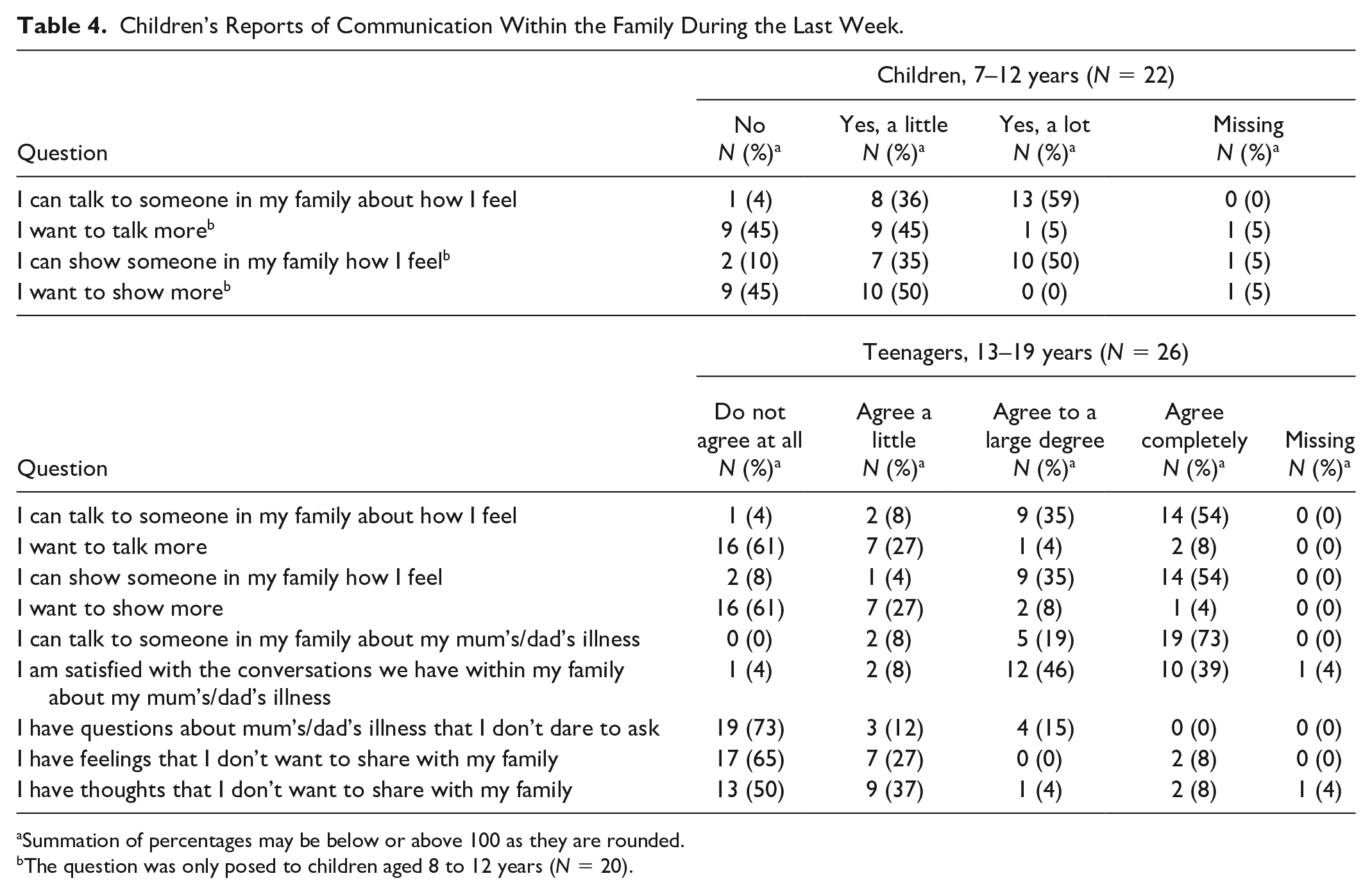
Summation of percentages may be below or above 100 as they are rounded.
The question was only posed to children aged 8 to 12 years (N = 20).
Nine of the 20 children aged 8 to 12 years reported that they could not show their feelings to anyone in the family or could show only a little. Half of the children (10/20) wanted to be able to show more (Table 4). Those who could show their feelings showed them exclusively to their mothers (3/20), to both parents (3/20), or to both parents and other relatives (3/20).
Reports from teenagers
All the teenagers reported that they could talk to someone in the family about their parent’s illness, but three reported not being satisfied with these conversations. All but one could talk to someone in the family about how they felt, but to different degrees. Nine reported being able to talk about how they felt to “everyone” and six of them talked to their mothers. Three teenagers from two families wanted to talk more about how they felt with someone in their family.
A few teenagers (3/26) reported that they could show their feelings only a little or not at all to someone in the family. Of those who could show their feelings, 11 reported in the open question that they showed them to “everyone” or “everyone in the family.” Three teenagers from two families wanted to be able to show more of how they felt to someone in the family. About one quarter of the teenagers (7/26) had questions about the illness that they did not dare ask (Table 4).
Discussion
Almost all children in this study reported that someone had told them about the parent’s life-threatening illness. However, two thirds wanted to know more about the illness. Almost three quarters of the teenagers did not receive any information about what they could do if an emergency occurred related to the parent’s illness. A family member was reported to be the source of illness-related information by almost all children. About half of the younger children reported that they could neither talk nor show how they felt to anyone in their family. Notably, half of all children aged 8 to 12 years wanted to be able to talk and/or show their feelings more to someone in their family.
According to Swedish law (Swedish Healthcare Act [Hälso- och sjukvårdslag: HSL] (Svensk författningssamling [SFS] 2017:30) [Swedish Code of Statutes], 2017), health care professionals should take into account a child’s need for information, advice, and support if the child’s parent, or any other adult the child lives with, has a life-threatening illness. Despite this, most children in the study received information from a family member. Many children in this study also wanted to know more about their parent’s illness. This is similar to previous interview studies which found that children want information, they want to be prepared, and be told the truth (Karlsson et al., 2013; Kennedy & Lloyd-Williams, 2009b; Maynard et al., 2013). Children want thorough, detailed information from health care professionals, throughout the illness trajectory, in order to prepare themselves for their parent’s illness and death (Alvariza et al., 2017). When children do not receive enough information regarding a parent’s illness or death, they often make things up to fill in the gaps. These imaginings are not always realistic and may exacerbate a child’s fear or worry (Bugge et al., 2008; Dunning, 2006; Fearnley, 2015). Children in situations like this are at increased risk of experiencing psychological issues (Morris et al., 2016). Another study found that giving adolescents too little information about a dying parent led to uncertainty and loneliness (Melcher et al., 2015). Moreover, Bylund-Grenklo et al. (2013) found that if adolescents had not been told about the parent’s illness, they were more likely to report a lack of trust in the health care provided to the dying parent, which further increased their risk of depression.
Previous literature shows that parents struggle with telling their children about serious illness, and that when the parents are ready to provide illness-related information, they reach out to health care professionals for support. Unfortunately, parents often report that health care professionals are unsupportive and unable to help them speak to and inform the children (Morris et al., 2016; Phillips, 2014; Semple & McCance, 2010). This lack of support may be related to research showing that health care professionals believed that the children of patients with a life-threatening illness were not their concern (Franklin et al., 2019). This was partly because the children were in school during daytime and partly because the health care professionals did not want to interfere with the family and the parents’ wishes. Even if the health care professionals wanted to include the children, they reported a lack of knowledge and feelings of insecurity about how to support the parents in talking to the children about illness and impending death. Another reason could be that the health care professionals needed the parents’ permission to talk to the children, and if the parents were not ready to give it, they simply had no chance to inform the children properly (Franklin et al., 2019).
It is possible that societal and cultural norms in Sweden, about how to talk about death, may have contributed to the study findings regarding family communication. Sweden today is a secular society with many different perspectives on what are desirable values in life and regarding death (af Burén, 2015; Zuckerman, 2009). Health care professionals require knowledge and skills in working with families to understand each family member’s beliefs and preferences regarding communication about illness and impending death (Ternestedt et al., 2017). The uniqueness of the Swedish context is that children living in Sweden are raised to become independent social actors, citizens with their own rights. For example, the convention of the rights of the child will be incorporated within the Swedish law in January 2020 (Socialdepartementet, 2017), which will create even more demand for health care professionals to include and be responsive to each child’s perspective.
Other potential reasons why many children in this study reported being unable to talk or show their feelings to someone in the family might be related to them being reluctant to disturb, upset, or burden their parents with their own emotional needs (Christ et al., 1993; Dehlin & Mårtensson, 2009; Kennedy & Lloyd-Williams, 2009a; Melcher et al., 2015; Phillips & Lewis, 2015). Previous research has found that even when children wanted to talk to their parents, broaching the topic of the illness could be scary, and the conversations would focus more on practical than emotional issues (Phillips & Lewis, 2015). Parents frequently also have difficulty knowing what to say to their children, or when, and the situation can be experienced as stressful. Parents have reported fear of being unable to manage their feelings and of breaking down in front of the children. They often try to protect their children by hiding facts about the illness and the risk of death. This hinders communication and can reduce the family’s possibilities of preparing emotionally for the impending death (Morris et al., 2016; Phillips, 2014; Semple & McCance, 2010).
Study Strengths and Limitations
As far as we know, this is the first study where children living in a family with a parent with a life-threatening illness have provided self-reports in a survey measuring illness-related information and family communication. Our small sample included families from four specialized home care units in a large city in a welfare society with the inclusion criteria of speaking and writing Swedish and having a child aged 6 to 19 years. The results can therefore not be generalized to other contexts, but confirms that children experienced a lack of information and communication. As our data was derived from an ongoing intervention study that primarily aims to increase illness-related information and family communication, there was a risk of selection bias. Participating in such an intervention takes time, energy, and courage. It is also conceivable that families choosing to participate in this study already communicated relatively well and were well functioning. Some of the families who chose not to participate in this study declined because the children had not yet been informed that the parent was ill.
Implications for Family Nursing Practice
The results of this study provide valuable insight and understanding about what children need in terms of illness-related information and family communication when a parent has a life-threatening illness. It is of utmost importance for health care professionals to provide such information, in accordance with the Swedish Healthcare Act, to offer useful support to these children and their families. Previous research shows that health care professionals, for example, nurses, could benefit from more guidance in working with these families (Franklin et al., 2019). One way of doing that could be to gather the whole family in a family nursing conversation intervention before the loss. Previous research (Bylund-Grenklo et al., 2014) has shown that children who have lost a parent have an increased risk for long-term psychological distress if they lacked medical information prior to the parent’s death. The findings from this study show that children want to know more about their parent’s illness and often do not have the ability to communicate their own thoughts and feelings with a family member to the extent they want. Taken together, these findings suggest that a preventive family-focused intervention starting early in the illness trajectory could be helpful for the whole family. Family-focused interventions offered by health care professionals may help both children and parents to talk and learn more about the illness, and communicate their feelings, thus helping the family come to a shared understanding of their situation (Mehta et al., 2009; Wright & Leahey, 2013).
Conclusion
The findings of study offer valuable information regarding a lack of communication both within and outside families when a parent has a life-threatening illness. Despite legislation in Sweden that regulates health care professionals to address children’s need for information, advice, and support when a child’s parent has a life-threatening illness, children in this study wanted to know more about their parent’s illness. They reported not been given enough information, and many of the children in this study reported having no family member with whom they could show or talk about their own feelings. As communication within the family about the parent’s life-threatening illness is still unexplored in the research from the children’s perspective, this study adds valuable knowledge in that area. To support these children, and to encourage parents to talk to their children, family-focused interventions to promote family communication and improve communication between family members and health care professionals are needed. Such interventions might be particularly beneficial if initiated shortly after the parent’s diagnosis or early in the illness trajectory and offered by skilled and courageous clinicians who believe that “illness is a family affair” (Wright & Leahey, 2013).
Footnotes
Acknowledgements
We are very grateful to all the children who participated in this study. We want to acknowledge the two interventionists who suggested the idea of evaluating the support program in palliative care settings. We also thank the specialized palliative home care units that helped with the recruitment process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Erling-Persson Family Foundation (grant number 545 02).