
Abstract
Studies of family nursing interventions have shown positive results for the health of individuals and families. To increase the availability of instruments that evaluate the practice of family nursing, this research adapted and validated the Family Nursing Practice Scale (FNPS) for use in Brazil with a sample of 144 hospital nurses using a cross-sectional design. The adaptation process involved back-translation, validation by a committee of experts, and semantic analysis. Content validity was analyzed through the content validity coefficient (CVC); construct validity was analyzed by exploratory factor analysis (EFA), confirmatory factor analysis (CFA), and convergent and discriminant validation through average variance extracted (AVE). The reliability of the measure was evaluated using Cronbach’s alpha index and composite reliability (CR). The results indicate that the adapted version of FNPS is recommended for family nursing research, education, or clinical practice with Brazilian nurses.
Influenced by General Systems Theory, family nursing recognizes that illness or risk to health affects all the family members and, reciprocally, that family relationships influence the health and well-being of the family. The recognition of this interaction and reciprocity invites nurses to investigate changes in thinking and practice, turning from a model of caring only for the individual patient to considering the family as the focus of care (Wright & Leahey, 2013).
Over the past 40 years, nurses have been investigating a variety of approaches to involve the family in care. Nursing has sought to advance knowledge about care approaches in different contexts and with measures that evaluate the phenomena present in family care (Dorell & Sundin, 2016; Sawin, 2016; Svavarsdottir & Sigurdardottir, 2013; Sveinbjarnardottir et al., 2012). The literature suggests that nurses’ beliefs about the benefits of family inclusion in care may be both a barrier and a facilitator for translating knowledge into practice (Duhamel et al., 2015). If nurses maintain constraining beliefs about families and lack pro-family attitudes, they tend not to include the family in their practice (Duhamel et al., 2015). Therefore, the study of nurses’ beliefs and attitudes about family nursing is essential for the practice and promotion of patients’ and families’ health.
Nurses’ attitudes about the inclusion of the family in care reflect the importance given to the family in the care process and define the type and quality of the relationship that will be developed between professionals and the family (Díaz et al., 2019). Hence, developing and improving measurement instruments that enable the assessment of nurses’ attitudes toward the inclusion of family in care can be helpful in the practice of family nursing evaluation (Benzein et al., 2008; Meiers et al., 2007; Sawin, 2016; Simpson & Tarrant, 2006). Instruments that are easy to apply, useful for research and capable of providing good qualitative and/or quantitative measures can contribute to knowledge production and the translation of knowledge to practice.
Several instruments have been developed in various countries (Benzein et al., 2008; Bruce & Ritchie, 1997; Meiers et al., 2007; Simpson & Tarrant, 2006; Toyama et al., 2017). In Brazil, we have two instruments: Self-efficacy Scale for the Establishment of Good Relationships with Families in Neonatal and Pediatric Hospital Settings, developed by (Cruz et al., 2017) and the Families’ Importance in Nursing Care: Nurses’ Attitudes, developed in Sweden by Benzin et al. (2008), adapted and validated for Portuguese by Oliveira et al. (2011). However, both instruments have some limitations. The first instrument was designed for neonatal and pediatric contexts only, and its size (39 items) can make its application difficult. The second instrument measures only nurses’ attitudes concerning families, but not their involvement with families in nursing practice (Oliveira et al., 2011).
Among the English-language scales, the Family Nursing Practice Scale (FNPS) developed by Simpson and Tarrant (2006) presents one of the best measurements of the nurses’ attitudes regarding the importance of involving families in their clinical practice (Díaz et al., 2019). This scale is economical (13 items) and examines the practice of family nursing and nurses’ attitudes toward working with families, family nursing, and reflections on the nurse–family relationship. Although the instrument was developed in a psychiatric nursing context, the FNPS has no specificity and is recommended to be tested in general nursing contexts (Simpson & Tarrant, 2006). This scale has been used in research examining family nursing practice in acute hospitalized older patients (Misto, 2018) and inpatient hospital units in Germany (Naef et al., 2021). As suggested by Díaz et al. (2019), cross-cultural studies are essential to strengthening the psychometric properties of a scale. Given the importance of understanding nurses’ attitudes and practices about working with families and the possibility of obtaining essential data from the use of the evaluation tools already developed, this study proposed to translate the FNPS to Brazilian Portuguese and evaluate the content, construct validities, and reliability measures.
Method
The purpose of this study was to translate the FNPS to Brazilian Portuguese and assess the psychometric properties of the adapted version. This methodological study involved two main phases: a cultural adaptation phase and a testing psychometric properties phase.
Ethical Considerations
This study was approved by the Research Ethics Committee of the University of São Paulo at Ribeirão Preto College of Nursing on November 21, 2017 (CAAE: 77821317.1.0000.5393) and by the Research Ethics Committee of the Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto on November 29, 2017 (CAAE: 77821317.1.3001.5440). All participants were informed of their rights regarding the research and gave their written consent. Anonymity of the collected data was guaranteed throughout the research.
The Family Nursing Practice Scale
The FNPS is a self-report questionnaire developed to assess changes in family nursing practice after the implementation of an educational program in Family Systems Nursing (FSN; Simpson & Tarrant, 2006). It measures nurses’ attitudes toward working with families, as well as their critical evaluation of the FSN practice and reflections on the nurse–family relationship (NFR). The instrument was constructed with 10 five-point inverted Likert-type scale items and three open questions about family nursing practices. The 10 items are divided into two different domains: practice assessment (PA) consisting of five items: 1, 2, 3, 4, and 5, and NFR consisting of five items: 6, 7, 8, 9, and 10. The potential FNPS score is between 10 and 50. As the scale of points is inverted, lower scores reflect high levels of family nursing practice. In the reliability tests, Cronbach’s alpha was .85 for the PA subscale and .73 for the FNR subscale. For the total scale, the coefficient was .84. Item-total correlation coefficients were all positive and ranged from .76 to .83 in the PA subscale and from .64 to .79 in the FNR subscale (Simpson & Tarrant, 2006).
Cultural Adaptation Phase
The process of cultural adaptation was directed by the recommendations of existing literature (Beaton et al., 2000; Borsa et al., 2012; Cassepp-Borges et al., 2010) that identifies the following steps appropriate to adapting instruments. The permission of the original author was first sought. A Brazilian Portuguese translation was developed by two Brazilian translators, both fluent in English and experienced in adaptation studies. They assessed the content validity coefficient (CVC) of the translated version, rating each item, using a 5-point Likert-type scale ranging from 1 (very low) to 5 (very high), based on the following criteria: theoretical relevance, practical relevance, and clarity of language. The CVC was calculated according to the literature (Cassepp-Borges et al., 2010; Hernández-Nieto, 2002). The overall CVC was .95, with .9 for the language clarity criterion, .97 for practical relevance, and .98 for theoretical relevance. These results indicate optimal content validity. This version of the FNPS was then back-translated. A consensus between back-translation versions was reached. To verify whether the items were understandable to the target population, the new version of the adapted FNPS was then subjected to semantic analysis by four newly graduated nurses. This included their impressions of the general instrument characteristics, and the relevance and understanding of the items. Both forms were adapted from the DISABKIDS® project (Fegadolli et al., 2010). The results of the semantic analysis were satisfactory, indicating that the adapted version presented no comprehension or application problems, and no further changes were necessary.
Testing of Psychometric Properties Phase
Pilot testing
A pilot study was conducted to refine the content and structure of the adapted FNPS, test the data collection method, and verify how the data would behave. This stage was performed with 60 practicing nurses who provided care in a general public health hospital in Brazil. Inclusion criteria were the following: nurses of any age or gender who worked directly to provide health care to patients treated in any ward of the hospital and who gave their consent for the study. The contact took place personally with all participants in their own workplace. Convenience sampling was used and collection was performed in all sectors of the hospital, in the morning, afternoon, and evening. The nurses received an envelope containing two copies of an informed consent form, a sociodemographic questionnaire, and the adapted FNPS. When the packets were returned, the researcher asked the nurse to comment on their perceptions about the scale at the time of receipt. Previous analyses of the reliability and factor structure of the instrument were performed using Cronbach’s alpha and exploratory factor analysis (EFA), respectively. The minimum sample for preliminary analysis is 50 participants, according to Terwee et al. (2007). Given that the results obtained were satisfactory and there were no problems in the collection procedure, the participants of the pilot study were included in the final sample.
Sample and Setting
The sample of the main study consisted of 144 practice nurses who provided care in a general public health hospital in Brazil. Inclusion criteria were the following: nurses of any age or gender who worked directly to provide health care to patients treated in any ward of the hospital and who gave their consent to participate in the study.
Data Collection
Data collection was performed from June to September 2018. Contact was made person to person with all participants in their work environment. The purpose of the research was explained. Each nurse received a packet containing two copies of a consent form, the adapted version of the FNPS, and a sociodemographic questionnaire which gathered information about age, gender, marital status, number of children, time since graduation, education in family care, mental health education, postgraduate work, current position, work shift, length of employment in the institution, number of employment links, weekly workload, and whether family nursing care was performed. The packet stayed with the nurse so that he or she could respond when his or her work routine allowed. The packets were received back at the day and time scheduled between the researcher and the participant. At the time of receipt, the researcher asked the nurse to comment on his or her perceptions about the scale.
Data Analysis
The data were analyzed using the Statistical Package for the Social Sciences software, IBM SPSS, version 25.0. The answers to the items were reversed to facilitate the interpretation of the data. Descriptive analyses were performed for all variables. Content validity was verified by the CVC during the cultural adaptation phase. The cutoff point was .8 (Alexandre & Coluci, 2011; Cassepp-Borges et al., 2010). The construct validity was evaluated by EFA, confirmatory factor analysis (CFA), and convergent and discriminant validation. The adequacy of the database for the application of factor analysis was evaluated by the Kaiser–Meyer–Olkin (KMO) test sample adequacy index, establishing a criterion above .7 and by the Bartlett Sphericity test with p < .05 (Damásio, 2012). For the extraction of factors in the EFA, principal axis factoring of the covariance matrix was used, and the eigenvalue criterion was greater than 1. The oblique oblimin direct method was used to test whether there was a correlation between the factors (Field, 2009; Laros, 2012). CFA was performed with the special module of SPSS Analysis of Moment Structures (AMOS), using the indexes χ2/gl < 3.0, confirmatory factor index (CFI) > .9, root mean square error of approximation (RMSEA) <.1, standardized root mean residual (SRMR) <.08, parsimonious normed fit index (PNFI) >.6 and parsimony comparative fit index (PCFI) >.6, as suggested in the literature (Hair et al., 2009; Hooper et al., 2007; Hu & Bentler, 1999). The covariance matrix was used, adopting the maximum likelihood estimation method.
Convergent validation was evaluated by the value of the average variance extracted (AVE) associated with the composite reliability (CR) value. Discriminant validation was evaluated by comparing the AVE and the square of the correlation between the RA and NFR factors of the adapted version of the FNPS. The AVE cutoff points >.4 with CR >.6 were adopted for convergent validation. Discriminant validation was determined by an AVE higher than the square of the correlation between PA and NFR factors (Fornell & Larcker, 1981; Huang et al., 2013).
The items were analyzed using the corrected item-total correlation for the scale and for the two subscales using the Pearson product-moment correlation coefficient. The reliability of adapted FNPS and its subscales was analyzed by Cronbach’s alpha index and CR, establishing values above .7 as acceptable (Hair et al., 2009; Pasquali, 2013).
Results
Sample
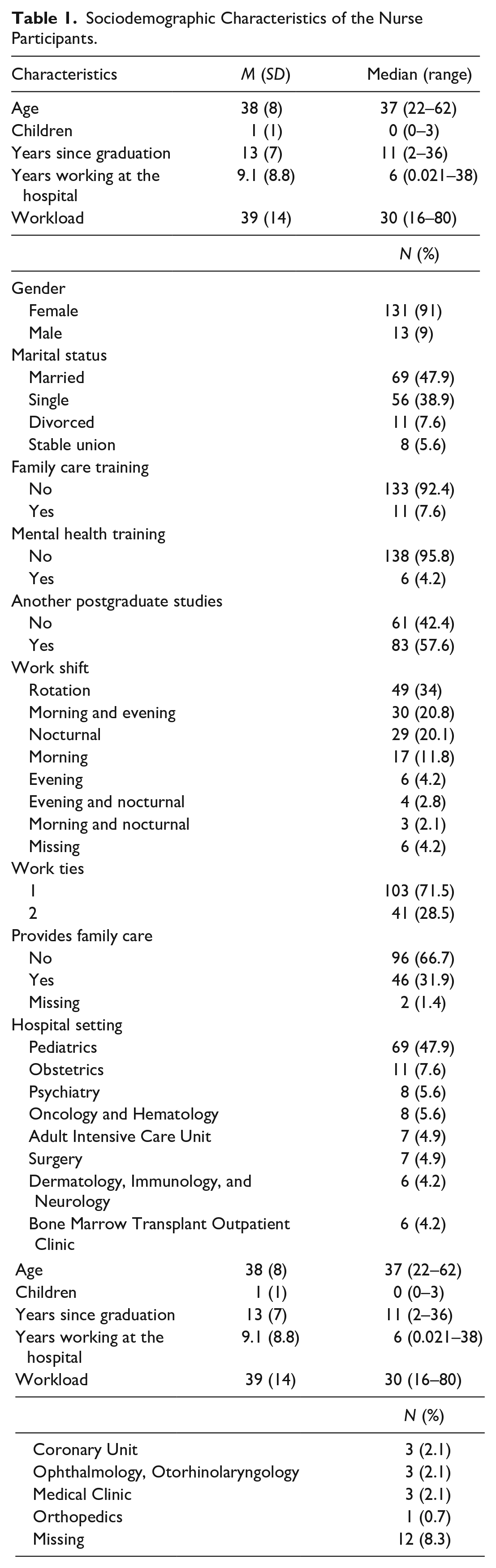
A total of 144 nurses responded to the questionnaire. The sociodemographic characteristics of the participants are shown in Table 1. Most were female (91%). The mean age was 38 years (SD = 8), and the average working time in the institution was 9.1 years (SD = 8.8), with an average workload of 39 hr per week (SD = 14). Of the respondents, 31.9% reported performing family care, 69% reported having some postgraduate work, 7.6% said they had a postgraduate degree in family care, and 48% came from some type of pediatric context.
Sociodemographic Characteristics of the Nurse Participants.
The distribution of participants’ frequency of responses to the 10 items of the adapted FNPS can be seen in Table 2. The median for the total score of the adapted version of the FNPS was 35, higher than the median of the possible range (30). The only item that did not show marking at the extreme end of the Likert-type scale was Item 3. There were no missing cases.
Response Frequencies to the Items of the Adapted Version of the FNPS.

Note. FNPS = Family Nursing Practice Scale.
Construct Validity
EFA
Bartlett’s sphericity test found the rejection of the null hypothesis (p = .000), so the R-matrix is not an identity matrix. The KMO test was also performed, which obtained an index ranging from “good” to “very good” (KMO = .805). Both results indicate that the collected data were adequate and sufficient for the application of EFA.
Based on the eigenvalue greater than 1, two factors were defined. The total variance explained was 58.5%, with 39.75% for the NFR factor and 18.7% for the PA factor. The two retained factors were left with five items each. As can be seen in Table 3, the factor loads of all items are above .4 in their respective factor. The comparison between the adapted version and the original version of the FNPS shows that both seem to have similar factorial structures. The matrix of factor correlations showed that both factors present a positive correlation of .39.
Adapted FNPS Factor Load Pattern Matrix.

Note. Extraction method: principal axis factorization; rotation method: oblimin with Kaiser normalization; the factor loading of the items is presented in descending order. FNPS = Family Nursing Practice Scale; NFR = nurse–family relationship; PA = practice appraisal.
CFA
The path diagram, Model 1, was constructed based on the factorial structure proposed by the original authors and the CFA conducted in this study (Figure 1). Although the factor loads were all above .5 and the adjustment indexes showed some good results, the RMSEA obtained a value not recommended. Analysis of the Modification Indexes was used to establish free parameters that would lead to an improved model. Establishment of a free parameter between the residuals of Items 6 and 8 showed an improvement to the fit, with all indexes within the recommended limit and all factorial loads above .5, as shown in Figure 2. The Fit Indexes details for Model 1 and Model 2 are presented in Table 4. The individual reliability of the items was above .25, and the factors presented a positive correlation of .44.
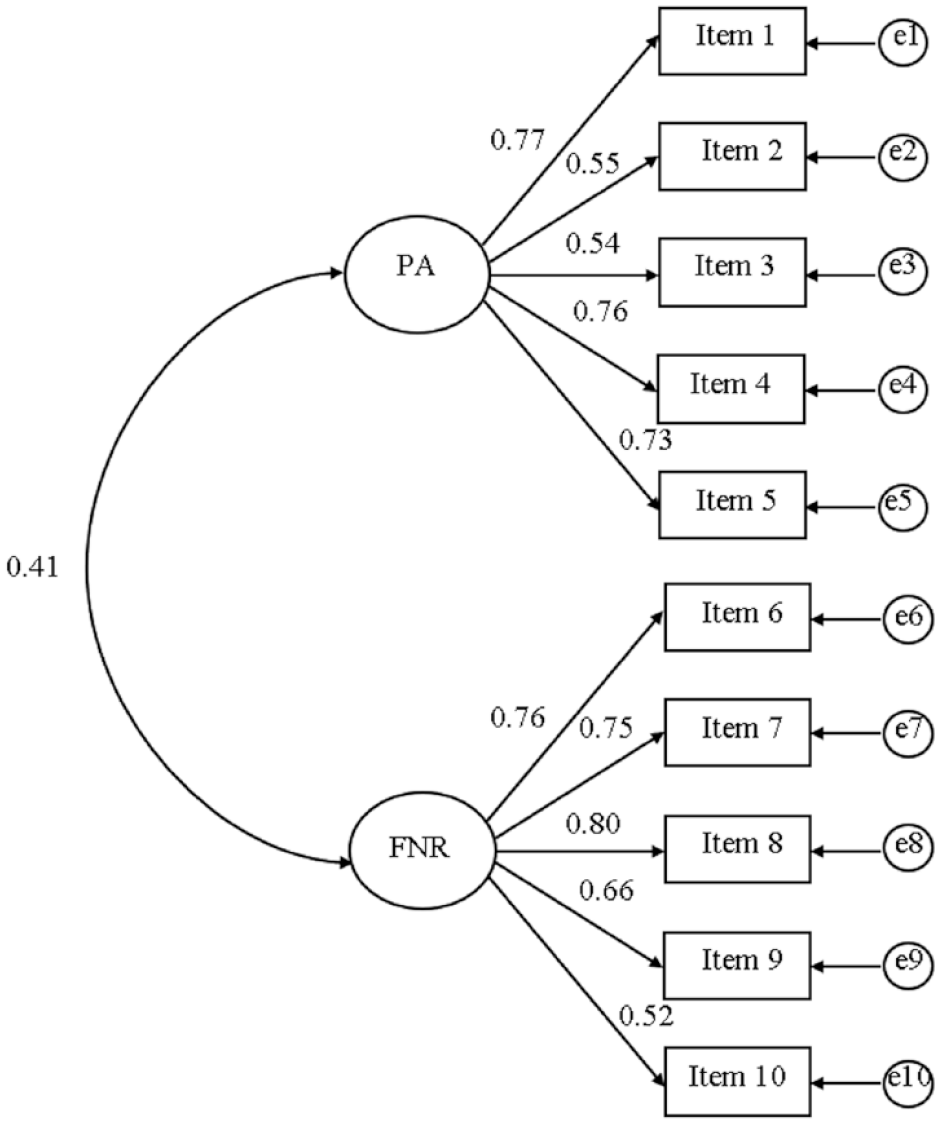
Path diagram—Model 1
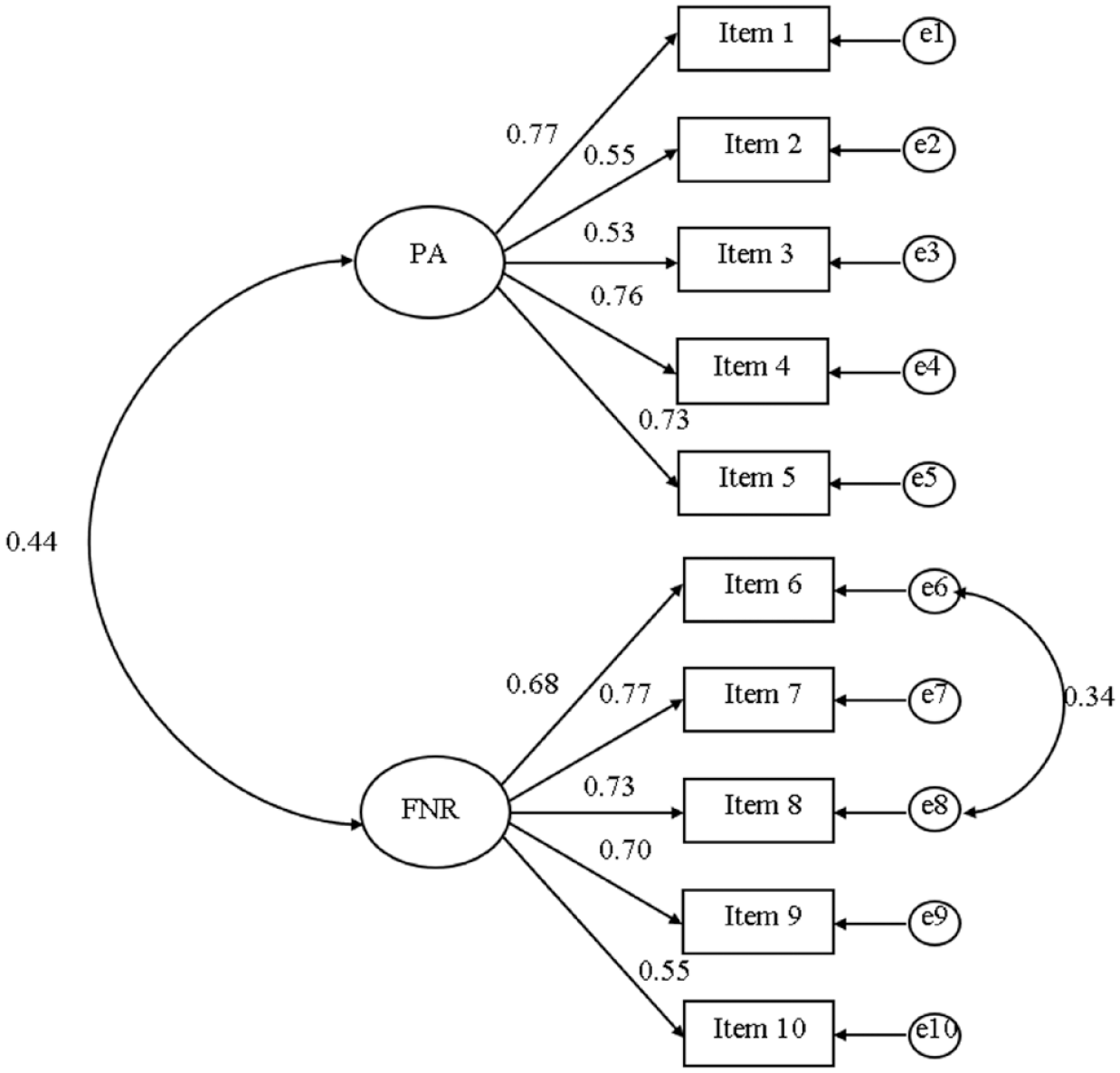
Path diagram—Model 2
Model Fit Indices for the Confirmatory Factor Analysis.
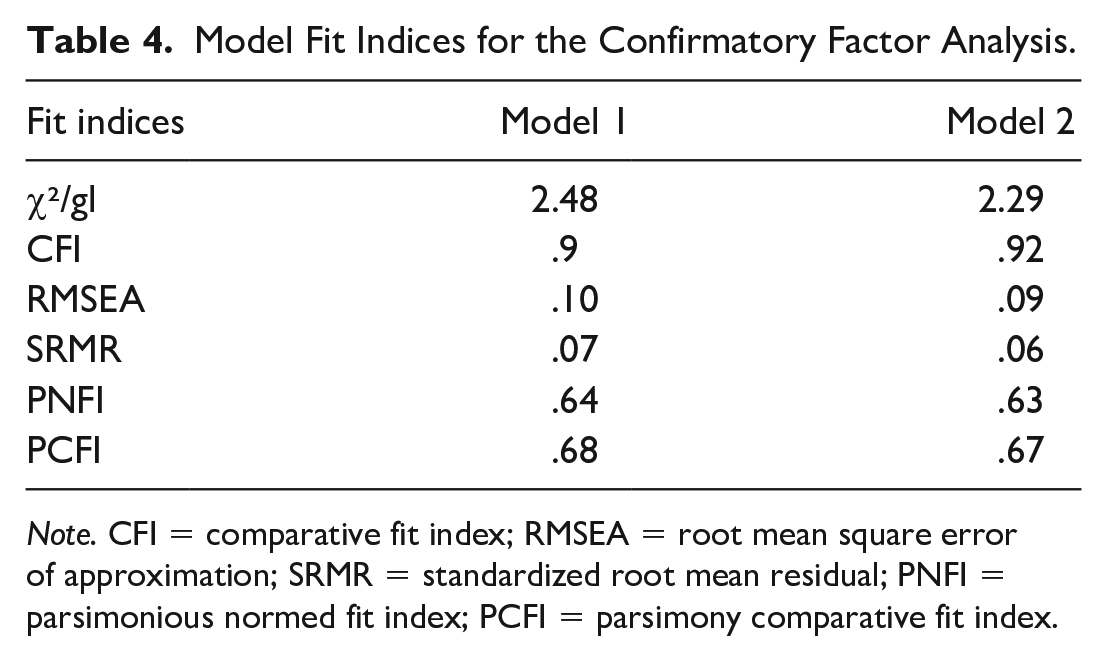
Note. CFI = comparative fit index; RMSEA = root mean square error of approximation; SRMR = standardized root mean residual; PNFI = parsimonious normed fit index; PCFI = parsimony comparative fit index.
Convergent and Discriminant Validation
Concerning convergent validation, the PA factor presented a value of .46 for the AVE and of .81 for the CR, whereas the NFR factor obtained the values AVE = .47 and CR = .82, reaching the established criteria. The AVE values for both factors were greater than the square of the correction between them, indicating discriminant construct validation. This information can be seen in Table 5, along with the standard factor loads and the items’ individual reliability for each factor.
Standardized Factor Loadings, Individual Reliability, Composite Reliability, Average Variance Extracted, and Square Correlation of PA and NFR Factors.

Note. PA = practice appraisal; NFR = nurse-family relationship; λ = standardized factor load; λ2 = individual reliability of the item; CR = composite reliability; AVE = average variance extracted; r = correlation between factors; r2 = correlation to the square of the factors.
Reliability Analysis Results
The Cronbach’s alpha coefficient was .82 for the total scale, .80 for the PA subscale, and .83 for the NFR subscale. The adopted confidence interval was 95%, ranging from .78 to .86 for the total scale, from .74 to .84 for the PA subscale, and from .78 to .87 for the FNR subscale. For both the full scale and the subscales separately, Cronbach’s alpha did not present higher values than the total alphas when an item was excluded. CRs were above .7 for both the full scale and the two domains. As for the corrected item-total correlation, the correlation strength of items with the scale total ranged from weak (Items 2, 3 and 10) to moderate (Items 1, 4, 5, 6, 7, 8, and 9) on the scale total, from weak (Items 3 and 5) and moderate (Items 2 and 4) to strong (Item 1) in the PA domain, and from weak (Item 10) to moderate (Items 6, 7, 8, and 9) in the NFR domain. All indexes were above .3, which indicates that the items present good consistency with the total score. These results can be seen in Tables 6 to 8.
Corrected Item-Total Correlation Coefficient Values for Cronbach’s Alpha If Any Item Is Excluded From Alpha and Composite Reliability for the Total Scale.

Corrected Item-Total Correlation Coefficient Values of Cronbach’s Alpha If Any Item Is Excluded From Alpha and Composite Reliability for the PA Domain.
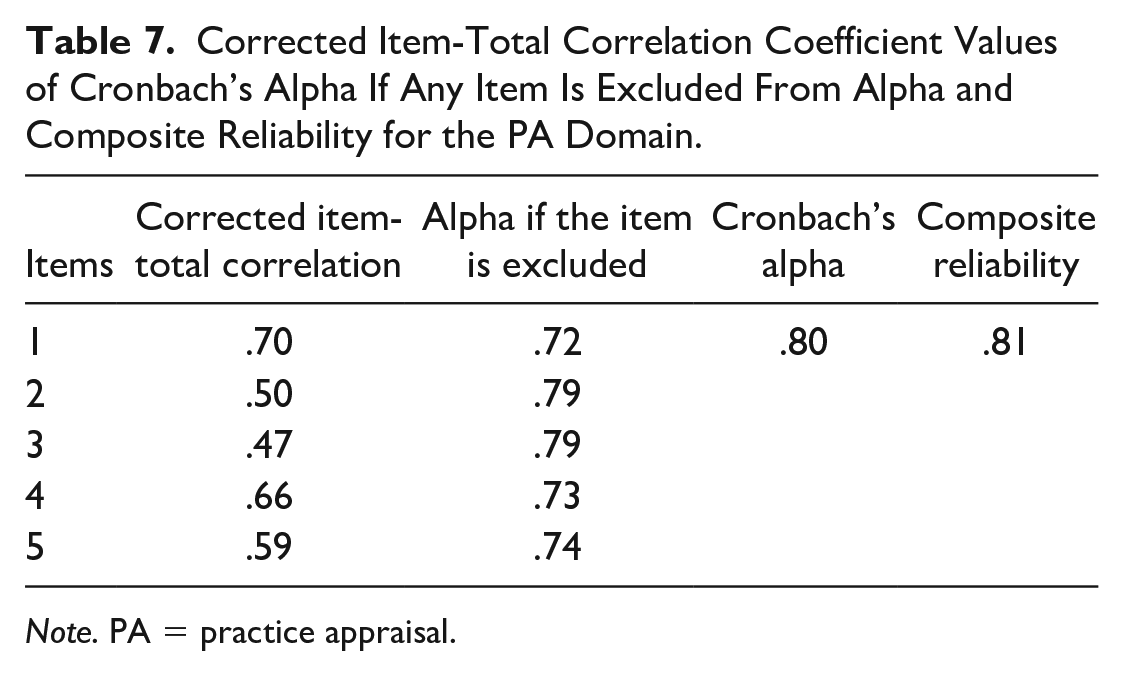
Note. PA = practice appraisal.
Corrected Item-Total Correlation Coefficient Values of Cronbach’s Alpha If Any Item Is Excluded From Alpha and Composite Reliability for the NFR Domain.
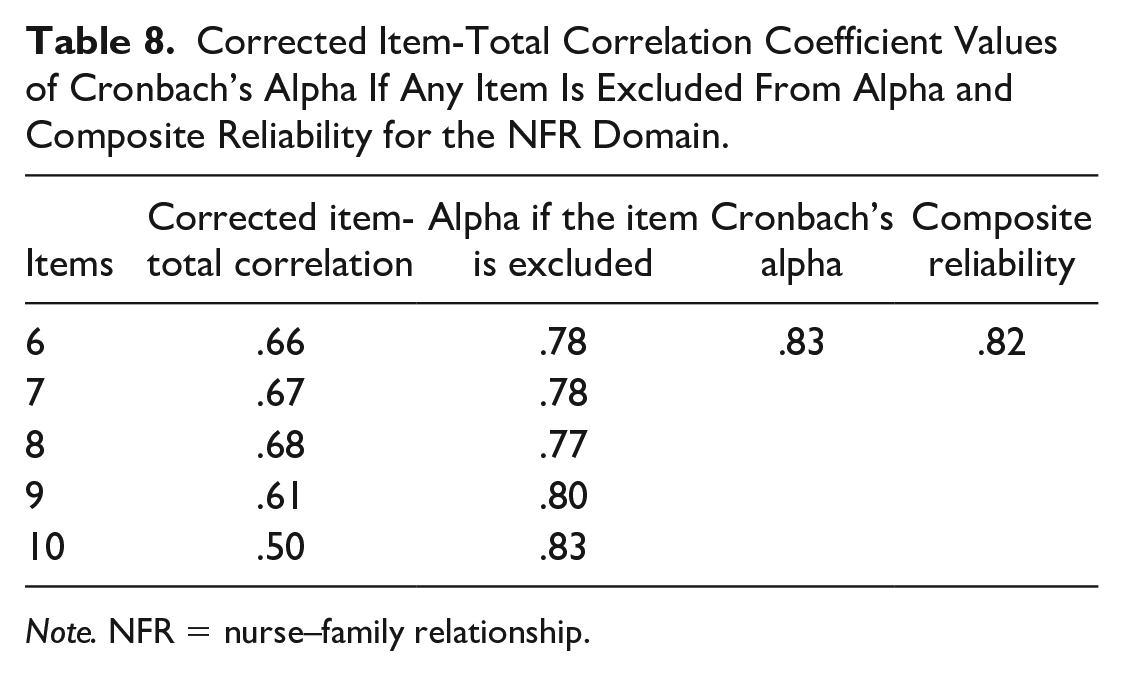
Note. NFR = nurse–family relationship.
Discussion
This study adapted and validated the FNPS for the Brazilian Portuguese language and context. Content validity was achieved based on qualitative and quantitative evaluations, obtaining optimal values for CVC.
To test its psychometric properties, the instrument was completed by a sample of 144 nurses working in a hospital context. The difference in context between the nurses in the original study and the nurses in this validation study was not observed as a problem because none of the items were formulated with specific content or concepts related to psychiatric nursing alone.
An analysis of the frequency of responses to the items found that only Item 3 did not obtain any point at the maximum level, showing a range between 1 and 4. In addition, it was the item that obtained the highest concentration of responses at the lower midpoint of the scale (2 and 3). Analyzing the frequency table published by the original authors, it was noticed that the same phenomenon occurred during the development study of the original FNPS. This indicates that the respondents had a low level of knowledge about the FSN model. This result is understandable, as only 7.6% of the survey participants reported having received some FSN education.
Items 7, 9, and 10 had the highest number of responses in the upper portion of the scale (4–5). The responses to Item 7 suggest that the work context requires nurses to contact the patients’ relatives. The answers to Items 9 and 10 indicate that, for most participants, this contact is gratifying.
Concerning EFA, the results identified two factors, adding a total explained variance of 58.5%, of which the NFR factor represents 39.75% and the PA factor represents 18.75%. In the original study, the total variance explained was 56.4%, with the difference that the majority of the variance belonged to the PA factor (41.9%), while NFR was the lower factor (14.5%). With a factorial structure similar to that of the original study, Items 1, 2, 3, 4, and 5 carried the PA factor, with all factorial loads above .4, whereas Items 6, 7, 8, 9, and 10 carried the NFR factor, with all loads above .5. The correlation between the factors was confirmed with a value of .39.
In the model specified for CFA, all factorial loads of observable variables were above .5, a value recommended for CFAs (Souza et al., 2017). The correlation between the factors was confirmed with a value of .44. Fit indexes less affected by sample size were chosen (Hooper et al., 2007).
A correlation was established between the residues of Items 6 and 8. Both belong to the NFR factor with high factor loads. Observing the content of the two items, unlike the others loaded in this factor, both also refer to the nurse’s tendency to act proactively to include the patient and the family in the health care decision-making processes. This content seems to be related not only to the relationship between nurses and families, but also to the proactive practice of family nursing. In this way, the content of the two items seems to justify this correlation. Regarding the fit indexes, all showed values within the acceptable cutoff point, indicating that the model fit the data and that, therefore, there was construct validity.
Another way used to assess convergent and discriminant validation in CFA studies is through the AVE. To convergent validation, the literature recommends the combined analysis of AVE and CR, adopting cutoff points of AVE >.4 with CR >.6. To discriminant validation, the AVE should be higher than the square of the correlation between instrument factors (Fornell & Larcker, 1981; Huang et al., 2013). Considering the low availability in Brazil of instruments that assess nurses’ attitudes toward working with families in general work contexts, this study chose to adopt the method of evaluating the convergent and discriminant construct validities through AVE.
The analyses showed convergent construct validity for both the PA factor and the NFR factor, with AVE values of .46 and .47 and CR of .81 and .82, respectively, corresponding to the recommendations in the literature. Similarly, the comparison of AVEs with the square of the correlation between the two factors showed that there is discriminant construct validity between them (Fornell & Larcker, 1981; Huang et al., 2013).
The results showed alpha values above .8 for the total scale and for the two domains. The analysis of CR, more adequate in confirmatory studies, showed indexes of .9 for the total scale and above .8 for the domains. As the cutoff point indicative of good reliability for both indexes is .7 (Hair et al., 2009), the adapted version of the FNPS presents measurement reliability, based on the principles of internal consistency.
Conclusion
This report increases knowledge about the psychometric properties of the FNPS with nurses in the general hospital context. The process of cultural adaptation to Brazilian Portuguese and FNPS validation achieved the criteria of content validity, construct validity, and reliability measure.
This study presents limitations such as the noncomparison of the measures obtained with others from similar instruments. The correlation between the sociodemographic data and the responses to the items did not show any significant relationship, and this could be explained due to the size and characteristics of the sample used. Further studies should compare the measures of the adapted version of the FNPS with others that are available at the appropriate time. Similarly, larger samples than those used in this work could provide even more in-depth results for the understanding of the constructs evaluated here.
Footnotes
Acknowledgements
The authors would like to express their sincere appreciation to Dr. Peggy Simpson, co-author of the Family Nursing Practice Scale, for her collaboration and advice during the development of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received partial financial support for the research, authorship, and/or publication of this article: Project—Strengthening the family nursing in mental health context. CNPq PQ 2018 Category/Level: 2- Process nº 307797/2018-0